Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 13
Necrotizing Enterocolitis and Its Predictors Among Preterm Neonates Admitted in Neonatal Intensive Care Units of Gurage Zone Public Hospitals, Southwest Ethiopia, 2021
Authors Chekole Temere B ![]() , Aynalem Mewahegn A
, Aynalem Mewahegn A ![]() , Tefera Zewudie B
, Tefera Zewudie B ![]() , Alebel GebreEyesus F
, Alebel GebreEyesus F ![]() , Kassaw A
, Kassaw A ![]() , Gelaw Walle B, Geze Tenaw S
, Gelaw Walle B, Geze Tenaw S ![]() , Mesfin Y
, Mesfin Y ![]() , Argaw M, Abebe H
, Argaw M, Abebe H ![]() , Tesfa S
, Tesfa S ![]() , Habte N, Birhanu R, Seid W
, Habte N, Birhanu R, Seid W
Received 12 December 2021
Accepted for publication 22 March 2022
Published 30 March 2022 Volume 2022:13 Pages 95—102
DOI https://doi.org/10.2147/PHMT.S353663
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Bogale Chekole Temere,1 Agerie Aynalem Mewahegn,1 Bitew Tefera Zewudie,1 Fisha Alebel GebreEyesus,1 Amare Kassaw,2 Belete Gelaw Walle,3 Shegaw Geze Tenaw,4 Yibeltal Mesfin,4 Muche Argaw,4 Haymanot Abebe,1 Shegaw Tesfa,1 Netsanet Habte,5 Robel Birhanu,5 Wesila Seid5
1Department of Nursing, College of Medicine and Health Science, Wolkite University, Wolkite, Ethiopia; 2Department of Pediatric Nursing, College of Medicine and Health Science, Debre Tabor University, Debre Tabor, Ethiopia; 3Pediatric Nursing, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 4Midwifery, Wolkite University, Wolkite, Ethiopia; 5Nursing, Wolkite University, Wolkite, Ethiopia
Correspondence: Bogale Chekole Temere, Department of Nursing, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia, Email [email protected]
Background: Necrotizing Enter colitis (NEC) is the most common multifactorial and devastating gastrointestinal emergency which primarily affects premature infants. The purpose of this study was to identify the prevalence of Necrotizing Enterocolitis and its associated factors among preterm neonates admitted to Neonatal Intensive Care Units in Gurage Zone hospitals.
Methods: Institution-based cross-sectional study design was employed. The simple Random Sampling Technique was applied to collect the data using a structured questionnaire. Data were cleaned, checked for inconsistencies, coded and entered via EPI data 3.1, and exported to Stata version 14 for further analysis. The data were processed by Stata 14 to estimate the prevalence of necrotizing enterocolitis.
Results: The prevalence of Necrotizing Enterocolitis among neonates was 28 (9.7%) 95% CI of 6. 8– 13.7%. Birth weight (AOR: 7.33 95% CI (2.04: 26.38)), presence of maternal infection (AOR: 6.09, 95% CI (1.31:28.26)), length of hospital stay (AOR: 3.28, 95% CI (1.20, 8.96)), and initiating trophic feeding (AOR: 5.89, 95% CI (2.27: 15.33)) were associated with neonatal necrotizing enterocolitis.
Conclusion: The prevalence of Necrotizing Enterocolitis among preterm neonates was significant and special attention is needed for premature neonates with low birth weight and born from mothers with infection during pregnancy. Minimizing the length of hospital stay will be very useful to prevent the occurrence of Necrotizing Enterocolitis.
Keywords: necrotizing enter colitis, low birth weight, trophic feeding
Introduction
Necrotizing enter colitis (NEC) is an inflammatory intestinal disorder primarily seen in premature infants, characterized by variable damage to the intestinal tract, ranging from mucosal injury to full-thickness necrosis and perforation.1 The global incidence of NEC was 7.0%.2 The incidence of NEC in India was 1.26%.3 In high-income countries, the incidence of NEC among preterm and low birth weight babies was 7% and 22% respectively.4 In one study, the prevalence of NEC among enteral Feed preterm and low birth weight neonates was 25.4%.5 The burden of NEC in 820 US centers was (7.6%).6 Early neonatal death was strongly associated with prematurity and NEC in different settings, including Ethiopia.7–14 The overall mortality in neonates with confirmed NEC was about 25%.15–17 Necrotizing enterocolitis in premature infants impacts morbidity, mortality, and septic complications in developing countries.18 Budgetary issues are the main challenge encountered during and after the commencement of neonatal units in developing countries.19 In sub-Saharan countries, inadequate facilities and a lack of trained personnel are the main obstacles to neonatal care.20
There are variations in the incidence of necrotizing enterocolitis between high and low-income countries.2 The rate of neonatal necrotizing enterocolitis in high-income countries was ranged from 2% to 7%.4 The Ethiopian government have been planning and prepared treatment guideline to strengthen the neonatal intensive care unit to give care for babies who are born early, and who have problems like NEC.21,22
There is limited evidence regarding the prevalence of Necrotizing Enterocolitis & its associated factors among premature infants. Therefore, The purpose of this study was to assess the prevalence and associated factors of Necrotizing Enterocolitis among preterm neonates admitted to Neonatal Intensive Care Units of Gurage Zone public hospitals.
Methods and Materials
Study Design
A cross-sectional study was employed to assess the prevalence of Necrotizing Enterocolitis & its associated factors among neonates admitted to Neonatal Intensive Care Units of Gurage Zone public hospitals.
Study Setting and Period
The study sites were Gunchire primary hospital, Atat hospital, and Wolkite University specialized and teaching hospital from June 2019 to June 2021. The Wolkite University specialized and teaching hospital is located in Wolkite town, located 150 km away from Addis Ababa.
Study Participants and Eligibility
In this study, all preterm neonates admitted to NICU in the selected hospitals of the Gurage zone from June 2019 to June 2021 were included, and neonates with incomplete data were excluded.
Sample Size Determinations
The sample size was determined using a single population proportion using the proportion of NEC 25.4%.5 Assuming the Z α/2=critical value for normal distribution at 95% confidence level, 5% margin of error (W). After adding a 5% non-response rate, the final sample size was 288.
Sampling Technique and Procedure
Random sampling was applied to select the three hospitals from all the public hospitals in the Gurage zone. Participants that fulfilled the inclusion criteria were randomly selected using excel (computer-generated random sample). Allocation of the study subjects was applied based on the proportion of the number of medical records of the neonates.
Data Collection Tool
Data were collected by reviewing the patients’ cards using the pretested checklist. NEC was confirmed by referring to the neonates’ medical charts.
Data Quality Control
A proper data abstraction tool, which evaluated by experienced researchers, and it was pretested on 5% of the given sample size to identify problems with the checklist. Based on the pretest, variables which have had the potential of being incomplete were excluded from the tool. For the data collectors and supervisors’ training was given.
Data was cleaned, checked for inconsistencies, coded and entered via EPI data 3.1, and exported to Stata version 14 for further analysis. The data were processed by Stata 14 to estimate the prevalence of necrotizing enterocolitis. The data were processed by state 14 to estimate the prevalence of necrotizing enterocolitis. The results of this study are displayed using tables, figures, and charts.
Definition of Terms
Necrotizing enterocolitis: an acute disorder of the gastrointestinal system which could affect every part of the bowel with a partial or diffuse intestinal necrosis.
Trophic feeding: The first minimum enteral feeding to initiate the neonate gut regardless of method or volume.22
Early trophic feeding: indicates when the neonate starts trophic feeding within 24 hours of birth.22,23
Delayed trophic feeding: indicates when the neonates start trophic feeding after 24 hours of birth.22,23
Result
Socio-Demographic Characteristics
Of 288 neonates admitted to NICU selected for this study, about half (51.7%) were males (see Table 1).
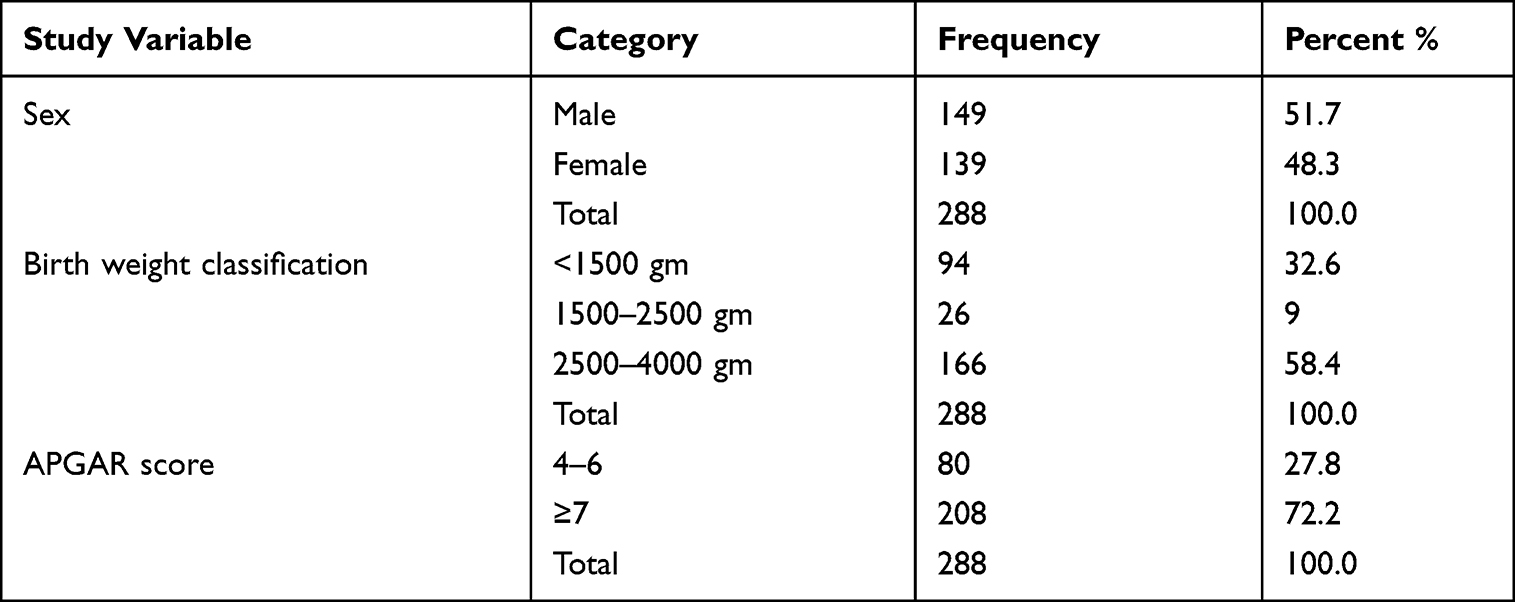 |
Table 1 Socio-Demographic Characteristics of Neonates Attending NICU of Gurage Zone Public Hospital, Southwest Ethiopia, August 2021 (n=288) |
Maternal Intra and antepartum Characteristics
More than half (58.3%) of neonates were born from multiparous mothers. About 134 (46.5%) neonates had a birth-related complication. Regarding the mode of delivery, 52.4% of neonates were via spontaneous vaginal delivery. (See Table 2).
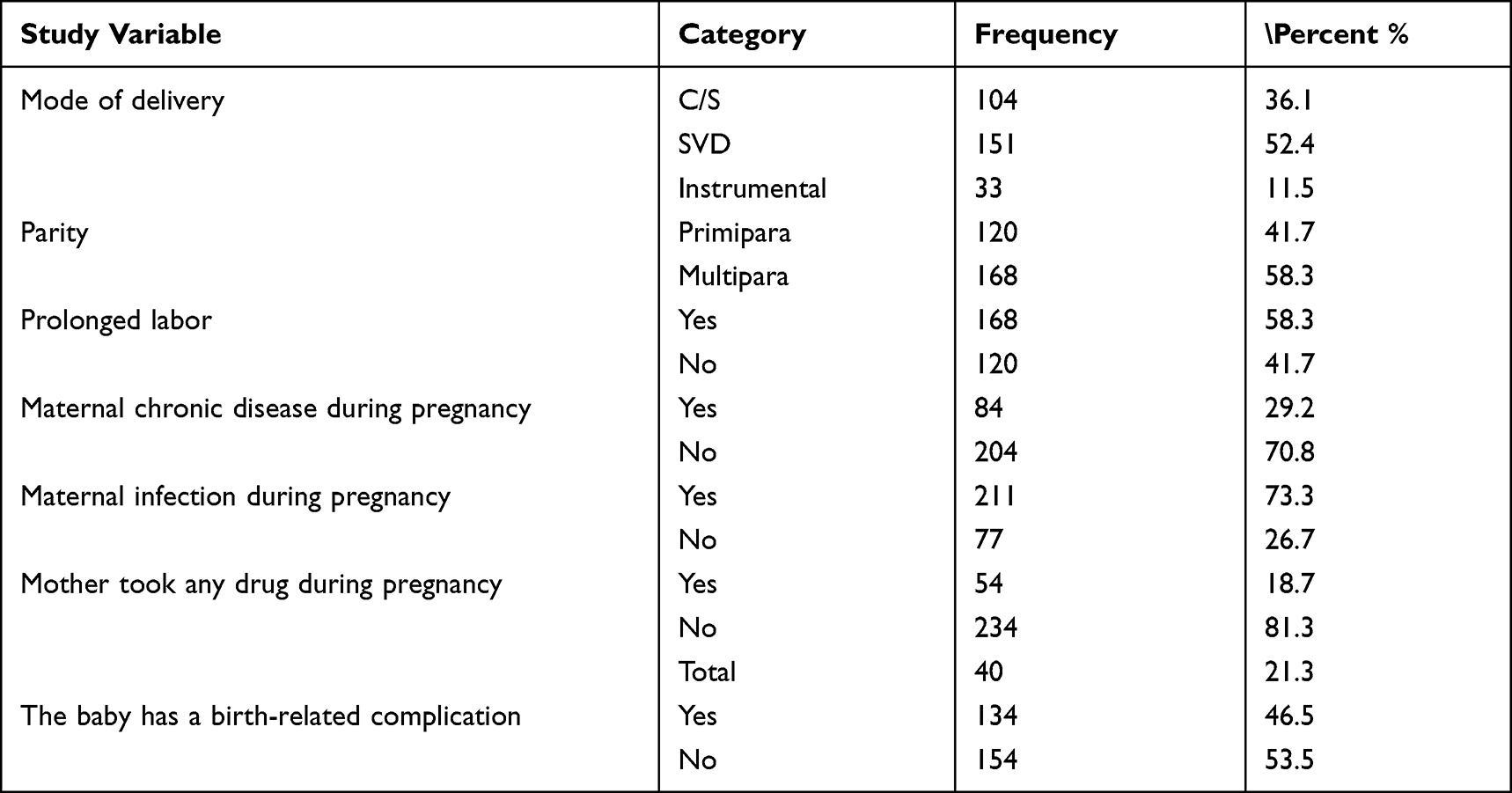 |
Table 2 Maternal Intra and Antepartum Characteristics of Neonates Attending NICU of Gurage Zone Public Hospital, Southwest Ethiopia, August 2021 (n=288) |
Clinical and Feeding Characteristics
Among the study participants, 10 (3.5%) babies had congenital anomalies, 181 (62.9%) of the babies had developed failure to breathe, 155 (53.8%) babies had respiratory distress, 237 (82.3%) babies had received antibiotics, and 90 (68. %) had received trophic feeding (see Table 3).
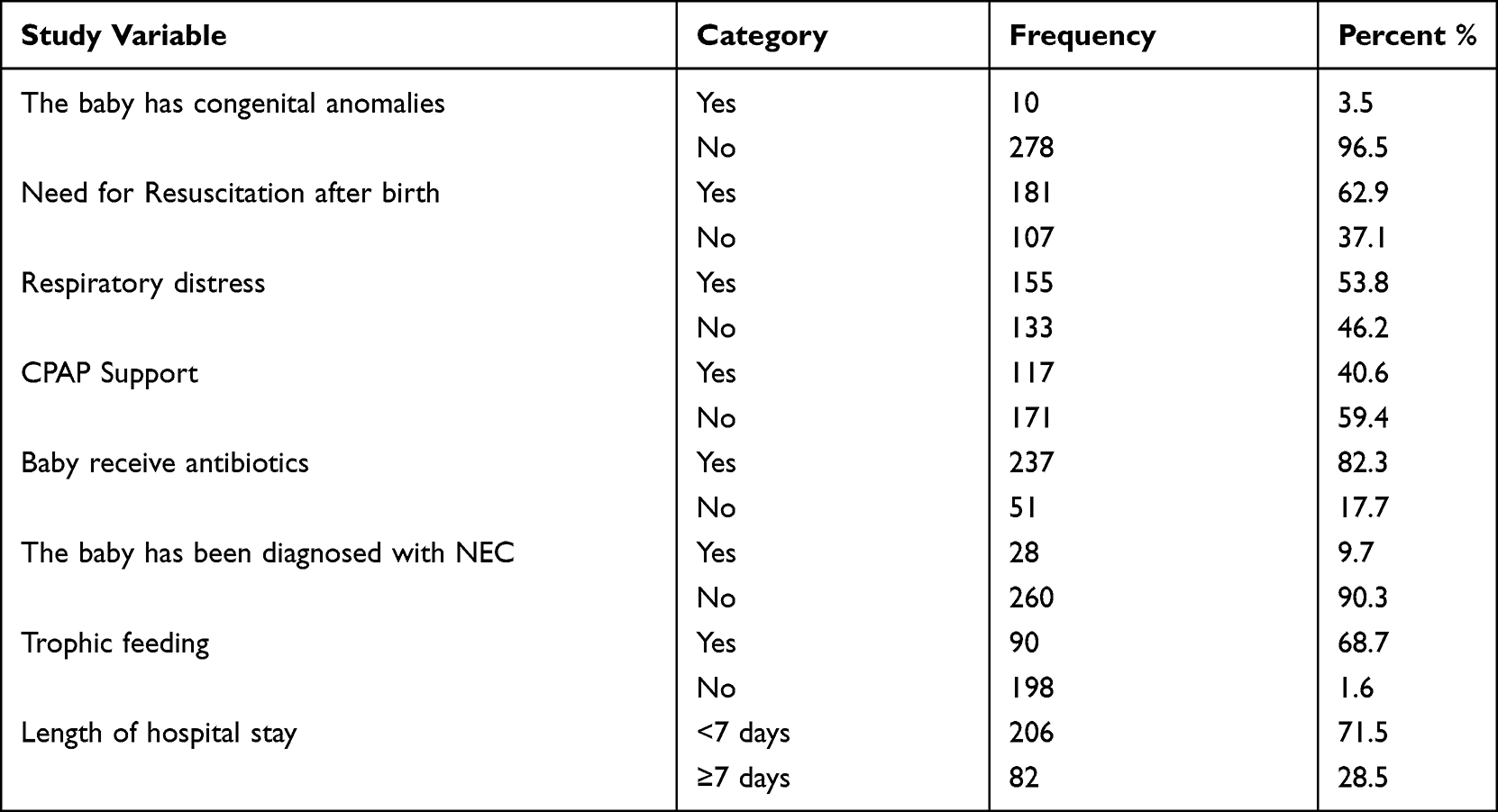 |
Table 3 Clinical and Feeding Characteristics of Neonates Attending NICU of Gurage Zone Public Hospital, Southwest Ethiopia, August 2021 (n=288) |
Prevalence of Necrotizing Enterocolitis
The prevalence of Necrotizing Enterocolitis among 288 study participants was 28 (9.7%) with a CI of 6.8–13.7% (Figure 1).
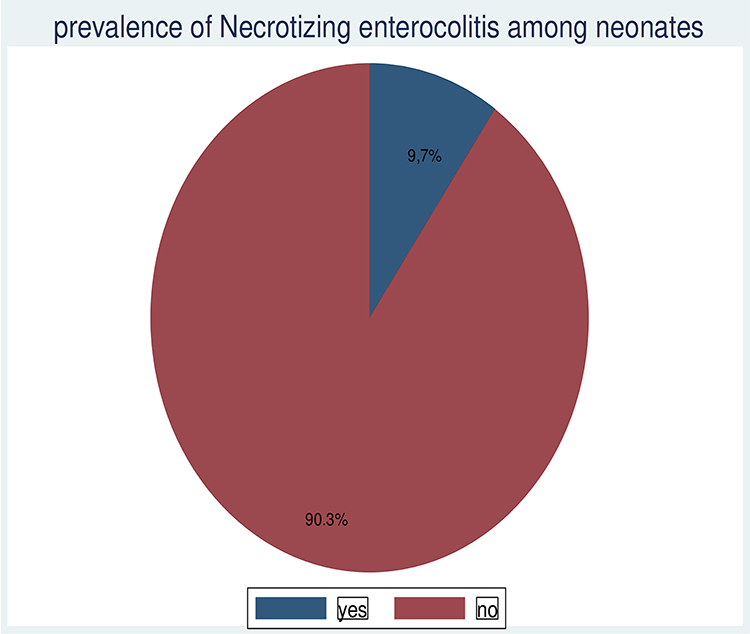 |
Figure 1 Prevalence of NEC among preterm neonates attending NICU of Gurage zone public hospital, South west Ethiopia, August 2021 (n=288). |
Factors Associated with Necrotizing Enterocolitis among those Neonates
Birth weight, maternal infection, length of hospital stay, and initiating trophic feeding were found to be significant factors for the development of Necrotizing enterocolitis among preterm neonates. The odds of neonates necrotizing enterocolitis among neonates who wait more than a week in NICU were 3.28 times higher than those who wait less than a week (AOR: 3.28, 95% CI (1.20, 8.96)).The odds of neonates with birth weight <1500 gm were 7.33 times more likely to develop NEC than those with a birth weight of 2500 gm–4000 gm (AOR: 7.33 95% CI (2.04: 26.38)). The odds of necrotizing enterocolitis among neonates from mothers with maternal infection were 6.09 times higher (AOR: 6.09, 95% CI (1.31:28.26)). The odds of necrotizing enterocolitis among neonates who start trophic feeding were 5.89 times higher (AOR: 5.89, 95% CI (2.27: 15.33)) (Table 4).
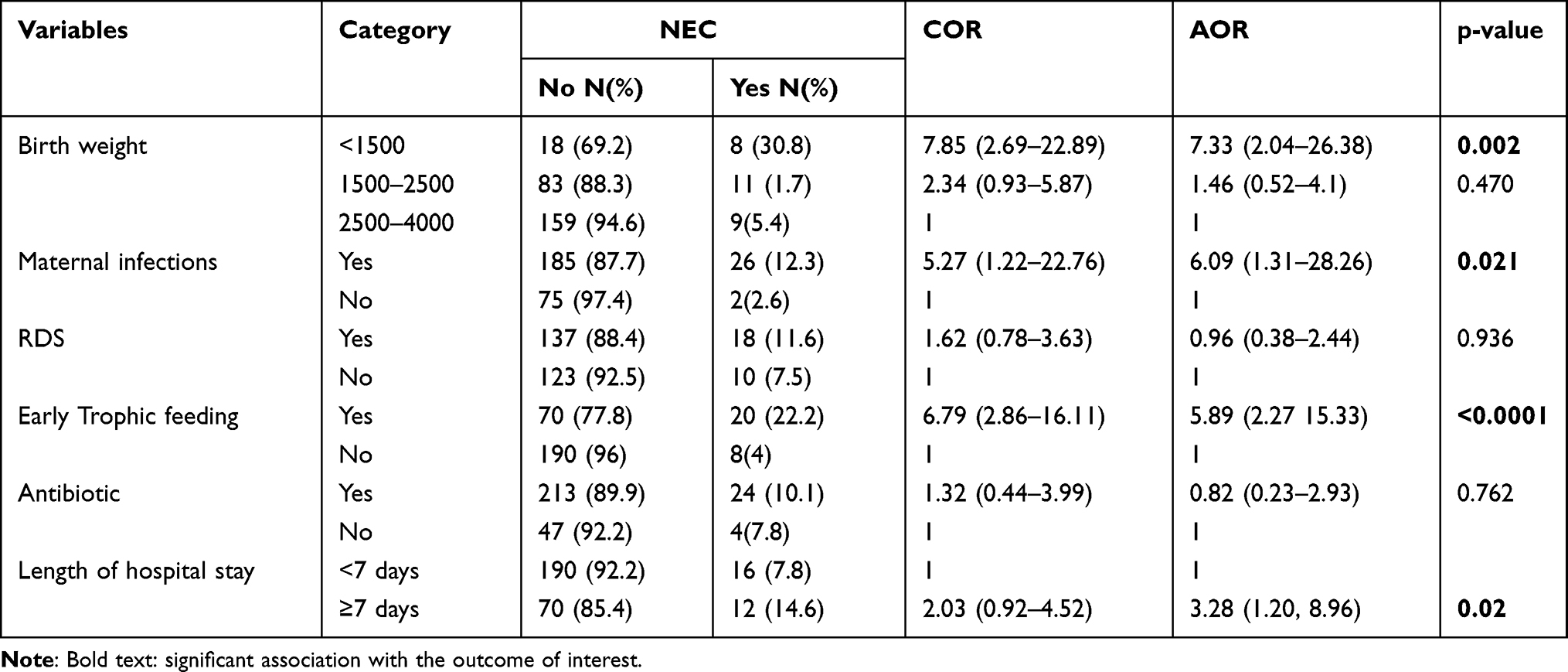 |
Table 4 Bivariable and Multivariable Logistic Regression Among Neonates Attending NICU Gurage Zone Public Hospital, Southwest Ethiopia, August 2021 (n=288) |
Discussion
The prevalence of necrotizing enterocolitis was 9.7% (95% CI: 6.8%- 13.7). The figure was consistent with studies conducted in Seoul National University Bundang Hospital, Seongnam, Korea (7.3%),24 US centers, in which the prevalence of NEC (7.6%),6 in Duke intensive care nursery in which the incidence of NEC as 10.7%.25 The finding is higher than studies conducted in several setting,14 in which the prevalence was 3.2%, United Kingdom, reported the prevalence as 1.8% for the winter season and 2.1% for the summer season.26 This difference may be due to the disparities in healthcare. But, the finding was lower than studies conducted in Addis Ababa, Ethiopia (25.4%).5 This difference might be due to the differences in population segment, as the study in Addis Ababa includes low birth weight infants as an inclusion criterion.
Birth weight was a significant factor for NEC. There is evidence that low birth weight increases the morbidity and mortality of neonates with NEC,27–29 Sweden,30 recent advance evidence,31 systemic review evidence,32,33 Seoul National University Bundang Hospital, Seongnam, Korea,24 Mexico.34
Maternal infection was found to be a significant factor in developing NEC. This finding was supported by studies done in Sweden,30,33 Seoul National University Bundang Hospital, Seongnam, Korea, and other countries in which chorioamnionitis was significantly associated with the development of NEC.24,31,35,36
Initiation of trophic feeding was associated with an increase in the risk of developing NEC, and it was evidenced by findings from a referral and training center in East Azerbaijan Province of Islamic Republic of Iran,37,38 in which delaying initiation was associated with less NEC and NEC associated death.
Length of hospital stay was significantly associated with NEC. This finding was evidenced by other studies in Iran.37 This present study does have some limitations. Since, the data were from medical records, socioeconomic factors, and some basic information was not possible to access.
Conclusion and Recommendation
The prevalence of Necrotizing Enterocolitis among neonates was significant and special attention is needed for premature neonates with low birth weight and born from mothers with infection during pregnancy. Minimizing the length of hospital stay will be very useful to prevent the occurrence of Necrotizing Enterocolitis.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request and will be attached to the editorial office when requested at any time.
Ethical Consideration
This study was approved by the Wolikite University College of Health science ethical review committee. After having the clearance, a permission letter was obtained from the managers of selected hospitals in the Gurage zone. The responsible bodies of pediatric inpatient care were tolled about the purpose of this study. Written informed consent was not sought from the legally authorized representatives of the patients directly since we used a medical record. When the data was recorded from their medical chart’s identification numbers were used for each individual patient so as to make it easy to identify the individuals’ profile while keeping patient’s medical secret. This study was conducted in accordance with the declaration of Helsinki.
Acknowledgments
Our gratitude goes to supervisors, the data collectors, and the staff of the selected hospitals for their cordial collaboration.
Disclosure
The authors have declared that there is no conflicts of interest in this work.
References
1. Neu J, Walker WA. Necrotizing enterocolitis. N Engl J Med. 2011;364(3):255–264. doi:10.1056/NEJMra1005408
2. Alsaied A, Islam N, Thalib L. Global incidence of necrotizing enterocolitis: a systematic review and meta-analysis. BMC Pediatr. 2020;20(1):1–15. doi:10.1186/s12887-020-02231-5
3. Adhisivam B, Vishnu Bhat B, Banupriya N, Poorna R, Plakkal N, Palanivel C. Impact of human milk banking on neonatal mortality, necrotizing enterocolitis, and exclusive breastfeeding–experience from a tertiary care teaching hospital, south India. J Matern Fetal Neonat Med. 2019;32(6):902–905. doi:10.1080/14767058.2017.1395012
4. Battersby C, Santhalingam T, Costeloe K, Modi N. Incidence of neonatal necrotising enterocolitis in high-income countries: a systematic review. Arch Dis Childhood. 2018;103(2):F182–F9. doi:10.1136/archdischild-2017-313880
5. Mekonnen SM, Bekele DM, Fenta FA, Wake AD. The prevalence of necrotizing enterocolitis and associated factors among enteral fed preterm and low birth weight neonates admitted in selected public hospitals in Addis Ababa, Ethiopia: a cross-sectional study. Glob Pediatr Health. 2021;8:2333794X211019695. doi:10.1177/2333794X211019695
6. Han SM, Hong CR, Knell J, et al. Trends in incidence and outcomes of necrotizing enterocolitis over the last 12 years: a multicenter cohort analysis. J Pediatr Surg. 2020;55(6):998–1001. doi:10.1016/j.jpedsurg.2020.02.046
7. Mengesha HG, Sahle BW. Cause of neonatal deaths in Northern Ethiopia: a prospective cohort study. BMC Public Health. 2017;17(1):1–8. doi:10.1186/s12889-016-3979-8
8. Yismaw AE, Tarekegn AA. Proportion and factors of death among preterm neonates admitted in University of Gondar comprehensive specialized hospital neonatal intensive care unit, Northwest Ethiopia. BMC Res Notes. 2018;11(1):1–7. doi:10.1186/s13104-018-3970-9
9. Yehuala S, Teka Z. Survival analysis of premature infants admitted to Neonatal Int ensive care unit (NICU) in Northwest Ethiopia using semi-parametric frailty model. J Biom Biostat. 2015;6(1):1.
10. Wesenu M, Kulkarni S, Tilahun T. Modeling determinants of time-to-death in premature infants admitted to neonatal intensive care unit in Jimma University Specialized Hospital. Ann Data Sci. 2017;4(3):361–381. doi:10.1007/s40745-017-0107-2
11. Muhe LM, McClure EM, Mekasha A, et al. A prospective study of causes of illness and death in preterm infants in Ethiopia: the SIP study protocol. Reprod Health. 2018;15(1):1–9. doi:10.1186/s12978-018-0555-y
12. Muhe LM, McClure EM, Nigussie AK, et al. Major causes of death in preterm infants in selected hospitals in Ethiopia (SIP): a prospective, cross-sectional, observational study. Lancet Glob Health. 2019;7(8):e1130–e8. doi:10.1016/S2214-109X(19)30220-7
13. Clark RH, Gordon P, Walker WM, Laughon M, Smith PB, Spitzer AR. Characteristics of patients who die of necrotizing enterocolitis. J Perinatol. 2012;32(3):199–204. doi:10.1038/jp.2011.65
14. Ree IM, Smits-Wintjens VE, Rijntjes-Jacobs EG, et al. Necrotizing enterocolitis in small-for-gestational-age neonates: a matched case-control study. Neonatology. 2014;105(1):74–78. doi:10.1159/000356033
15. Jones IH, Hall NJ. Contemporary outcomes for infants with necrotizing enterocolitis—a systematic review. J Pediatr. 2020;220:86–92. e3. doi:10.1016/j.jpeds.2019.11.011
16. Spinner JA, Morris SA, Nandi D, et al. Necrotizing enterocolitis and associated mortality in neonates with congenital heart disease: a multi-institutional study. Pediatr Crit Care Med. 2020;21(3):228–234. doi:10.1097/PCC.0000000000002133
17. Hull MA, Fisher JG, Gutierrez IM, et al. Mortality and management of surgical necrotizing enterocolitis in very low birth weight neonates: a prospective cohort study. J Am Coll Surg. 2014;218(6):1148–1155. doi:10.1016/j.jamcollsurg.2013.11.015
18. Arnold M, Moore S, Sidler D, Kirsten G. Long-term outcome of surgically managed necrotizing enterocolitis in a developing country. Pediatr Surg Int. 2010;26(4):355–360. doi:10.1007/s00383-010-2583-8
19. Basnet S, Adhikari N, Koirala J. Challenges in setting up pediatric and neonatal intensive care units in a resource-limited country. Pediatrics. 2011;128(4):e986–e92. doi:10.1542/peds.2010-3657
20. Ekenze SO, Ajuzieogu OV, Nwomeh BC. Challenges of management and outcome of neonatal surgery in Africa: a systematic review. Pediatr Surg Int. 2016;32(3):291–299. doi:10.1007/s00383-016-3861-x
21. Fedreal ministry of Health, Ethiopia: https://www.healthynewbornnetwork.org/hnn-content/uploads/nationalstrategy-for-newborn-and-child-survival-in-ethiopia-201516-201920.pdf.
22. FMoH. Neonatal Intensive Care Unit (NICU) Training, Participants’ Manual. 2014:194.
23. Nakubulwa C, Musiime V, Namiiro FB, et al. Delayed initiation of enteral feeds is associated with postnatal growth failure among preterm infants managed at a rural hospital in Uganda. BMC Pediatr. 2020;20(1):1–9. doi:10.1186/s12887-020-1986-5
24. Lee J-Y, Park K-H, Kim A, Yang H-R, Jung E-Y, Cho S-H. Maternal and placental risk factors for developing necrotizing enterocolitis in very preterm infants. Pediatr Neonatol. 2017;58(1):57–62. doi:10.1016/j.pedneo.2016.01.005
25. DeRienzo C, Smith PB, Tanaka D, et al. Feeding practices and other risk factors for developing transfusion-associated necrotizing enterocolitis. Early Hum Dev. 2014;90(5):237–240. doi:10.1016/j.earlhumdev.2014.02.003
26. Rees CM, Eaton S, Pierro A. National prospective surveillance study of necrotizing enterocolitis in neonatal intensive care units. J Pediatr Surg. 2010;45(7):1391–1397. doi:10.1016/j.jpedsurg.2009.12.002
27. Qian T, Zhang R, Zhu L, et al. Necrotizing enterocolitis in low birth weight infants in China: mortality risk factors expressed by birth weight categories. Pediatr Neonatol. 2017;58(6):509–515. doi:10.1016/j.pedneo.2016.10.004
28. Youn YA, Kim E-K, Kim SY. Necrotizing enterocolitis among very-low-birth-weight infants in Korea. J Korean Med Sci. 2015;30(Suppl 1):S75–S80. doi:10.3346/jkms.2015.30.S1.S75
29. March MI, Gupta M, Modest AM, et al. Maternal risk factors for neonatal necrotizing enterocolitis. J Matern Fetal Neonat Med. 2015;28(11):1285–1290. doi:10.3109/14767058.2014.951624
30. Ahle M, Drott P, Elfvin A, Andersson RE. Maternal, fetal and perinatal factors associated with necrotizing enterocolitis in Sweden. A national case-control study. PLoS One. 2018;13(3):e0194352. doi:10.1371/journal.pone.0194352
31. Alganabi M, Lee C, Bindi E, Li B, Pierro A. Recent advances in understanding necrotizing enterocolitis. F1000Research. 2019;8:107. doi:10.12688/f1000research.17228.1
32. Samuels N, van de Graaf RA, de Jonge RC, Reiss IK, Vermeulen MJ. Risk factors for necrotizing enterocolitis in neonates: a systematic review of prognostic studies. BMC Pediatr. 2017;17(1):1–9. doi:10.1186/s12887-017-0847-3
33. Rose AT, Patel RM. A Critical Analysis of Risk Factors for Necrotizing Enterocolitis. Seminars in Fetal and Neonatal Medicine. Elsevier; 2018.
34. Baños-Peláez M, Avila-Sosa V, Fernández-Carrocera LA, et al. Estimating neonatal necrotizing enterocolitis based on feeding practices. Children. 2021;8(4):253. doi:10.3390/children8040253
35. Duci M, Frigo AC, Visentin S, Verlato G, Gamba P, Fascetti-Leon F. Maternal and placental risk factors associated with the development of necrotizing enterocolitis (NEC) and its severity. J Pediatr Surg. 2019;54(10):2099–2102. doi:10.1016/j.jpedsurg.2019.04.018
36. Carter BM, Holditch-Davis D, Tanaka D, Schwartz TA. The relationship between black race, maternal infection and NEC in the preterm infant. Newborn Infant Nurs Rev. 2013;13(4):166–170. doi:10.1053/j.nainr.2013.09.002
37. Sallakh-Niknezhad A, Bashar-Hashemi F, Satarzadeh N, Ghojazadeh M, Sahnazarli G. Early versus late trophic feeding in very low birth weight preterm infants. Iran J Pediatr. 2012;22(2):171.
38. Masoli D, Dominguez A, Tapia JL, Uauy R, Fabres J. Enteral feeding and necrotizing enterocolitis: does time of first feeds and rate of advancement matter? J Pediatr Gastroenterol Nutr. 2021;72(5):763–768. doi:10.1097/MPG.0000000000003069
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.