Back to Journals » International Journal of Nanomedicine » Volume 21
Natural Compound–Loaded PLGA Nanocarriers for Infected Wound Management: A Review
Authors Norouzi E, Hemmati J, Chehelgerdi M ![]() , Arabestani MR
, Arabestani MR
Received 13 February 2026
Accepted for publication 15 May 2026
Published 22 May 2026 Volume 2026:21 603447
DOI https://doi.org/10.2147/IJN.S603447
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kamakhya Misra
Elahe Norouzi,1 Jaber Hemmati,2 Mohammad Chehelgerdi,3 Mohammad Reza Arabestani1
1Department of Microbiology, School of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran; 2Department of Microbiology, Faculty of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran; 3Young Researchers and Elite Club, Shahrekord Branch, Islamic Azad University, Shahrekord, Iran
Correspondence: Mohammad Chehelgerdi, Young Researchers and Elite Club, Shahrekord Branch, Islamic Azad University, Shahrekord, Iran, Email [email protected] Mohammad Reza Arabestani, Department of Microbiology, School of Medicine, Hamadan University of Medical Sciences, Hamadan, IR, Iran, Tel +98-8118380755, Fax +98-8118380130, Email [email protected]
Abstract: Infected wounds remain a significant clinical challenge due to persistent microbial colonization, biofilm formation, delayed tissue regeneration, and prolonged healing processes. Poly (lactic-co-glycolic acid) (PLGA), a biodegradable and biocompatible polymer approved by the FDA, has gained increasing attention as a carrier for natural compounds because of its ability to provide controlled and sustained drug release, improve compound stability, and enhance therapeutic efficacy. This review summarizes recent advances in PLGA-based formulations loaded with natural compounds for the treatment of infected wounds. Findings from various studies demonstrate that these nanostructures promote wound healing through antimicrobial and anti-biofilm activities, antioxidant and anti-inflammatory effects, stimulation of angiogenesis, collagen deposition, and re-epithelialization. In addition, this review discusses different aspects of PLGA-based nanostructures, including fabrication and synthesis strategies, drug release behaviors, and bacterial biofilm-targeting mechanisms, which may play an important role in the development of novel nanoparticle-based therapeutic approaches for overcoming current challenges associated with infected wound management. Overall, the delivery of natural compounds through PLGA-based systems represents a promising strategy for the effective treatment of infected wounds and the advancement of next-generation wound care therapies. This review, with a focus on PLGA–natural compound systems for the treatment of infected wounds, provides a coherent synthesis of dispersed studies and, by emphasizing antibiofilm mechanisms and controlled drug release, offers an integrated perspective for a better understanding of the therapeutic potential of these nanoplatforms.
Keywords: PLGA, natural compounds, antioxidant, anti-inflammatory, wound
Introduction
The skin is the largest and outermost organ of the human body, covering its entire surface. Its primary function is to protect the muscles, bones, ligaments, and internal organs from environmental hazards and serves as the body’s first line of defense against external insults.1 However, the structure and function of the skin can be compromised by various factors, including cuts, burns, surgical incisions, exposure to radiation, contact with chemical agents, and underlying conditions such as diabetes.2 Following skin injury, the wound healing process initiates almost immediately to restore barrier integrity and prevent microbial invasion and infection.3 Wounds are generally categorized into two main types based on their healing duration and physiological progression: acute and chronic (Figure 1). Acute wounds, such as cuts, burns, insect bites, and surgical incisions, typically heal within a predictable timeframe. In contrast, chronic wounds are including diabetic foot ulcers, vascular ulcers, and non-healing surgical wounds are often the result of underlying pathologies like diabetes, obesity, immune deficiencies, or aging, which interfere with the normal healing process.4 Wounds that fail to heal within 8 to 12 weeks are usually classified as chronic.5,6 The open wound environment, particularly in chronic cases, provides a favorable niche for microbial colonization.6 Most infected wounds are polymicrobial in nature, comprising both endogenous microorganisms from mucosal surfaces and exogenous microbes from adjacent skin flora. In the early stages of chronic wounds, gram-positive bacteria such as Staphylococcus aureus and Streptococcus pyogenes are predominant. As the wound progresses, gram-negative pathogens such as Escherichia coli and Pseudomonas aeruginosa become more prevalent, invading deeper tissues and causing extensive damage. These pathogens often form biofilms, which disrupt healing and contribute to high levels of antimicrobial resistance.6 In immunocompetent individuals, the innate and adaptive immune responses typically control microbial growth and prevent systemic infection. However, in immunocompromised patients, these pathogens can penetrate into deeper dermal layers, reach the lymphatic system or bloodstream, and lead to sepsis.2 Sepsis represents the most severe clinical manifestation of wound infection and poses a significant risk, particularly in burn unit patients. Pathogens such as P. aeruginosa and Acinetobacter baumannii are particularly dangerous due to the presence of toxic lipopolysaccharides in their outer membranes, which trigger exaggerated inflammatory responses and increase the likelihood of mortality.2 The management of chronic wounds and severe burns is not only time-consuming and costly but often requires repeated surgical debridement and prolonged antimicrobial therapy. On the other hand, the primary challenges in managing acute wounds involve preventing excessive scarring, contraction, and secondary infection.5 Despite the availability of various antibiotics, including carbapenems, aminoglycosides, colistin, and β-lactam/β-lactamase inhibitors, their frequent and improper use has led to the emergence of multidrug-resistant (MDR), extensively drug-resistant (XDR), and pandrug-resistant (PDR) pathogens.2,7 This issue has become a global threat to human health, with projections indicating that such infections could cause up to 10 million deaths annually by 2050.8,9 Resistant pathogens such as methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant enterococci (VRE) are particularly common in wound infections and are notoriously difficult to treat.2 Moreover, systemic antibiotic therapies, such as intravenous administration, are often ineffective in deep wounds due to barriers like necrotic tissue, granulation, fibrosis, and hyper perfusion, which hinder drug penetration.10 Topical antibiotic treatments may also be inadequate, as they can be diluted by wound exudates or inactivated by enzymes and inflammatory mediators.10,11 Additionally, the presence of bacterial biofilms within wounds further protects pathogens from antimicrobial agents and significantly complicates treatment. To overcome these challenges, researchers have turned to innovative approaches, including the use of nanoparticles, natural products, probiotics, phototherapy, and bacteriophage therapy.12,13
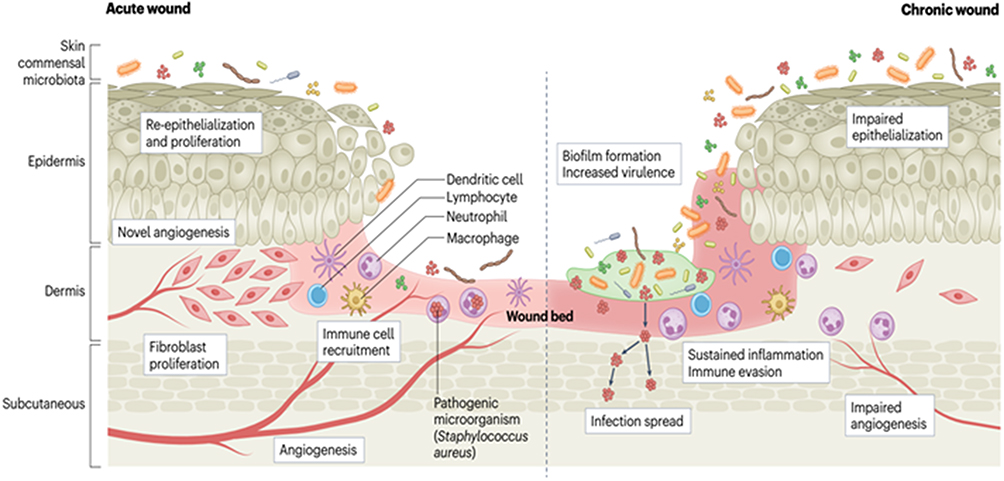 |
Figure 1 Progression of acute and chronic wound healing. Acute wound healing proceeds through a regulated series of biological events beginning with coagulation and hemostasis, followed by infiltration of inflammatory cells such as neutrophils and macrophages. As inflammation resolves, dermal fibroblasts proliferate to form granulation tissue and deposit extracellular matrix, while angiogenesis and keratinocyte proliferation occur to restore the epidermal layer. Typically, these wounds close within 3–14 days, with tissue remodeling continuing for several months. In contrast, chronic wounds like diabetic foot ulcers fail to progress through these stages, often resulting in persistent inflammation, infection, and impaired healing. This chronicity is driven by non-migratory keratinocytes, dysregulated immune activity, abnormal protease expression, defective angiogenesis, and fibroblast senescence. Reprinted from14 with permission from Springer Nature. |
Among these, nanoparticles are especially promising due to their intrinsic antimicrobial properties, selective targeting capability, reduced side effects, and lower potential for inducing bacterial resistance, making them a viable alternative to traditional antibiotics.15 Nanoparticles have enhanced their role as drug carriers in the topical treatment of chronic infected wounds. In such wounds, systemic antibiotic therapy is often ineffective due to insufficient tissue perfusion, which leads to low drug concentrations at the site of infection.15 Similarly, conventional topical treatments are frequently inadequate because of poor drug penetration into the deeper layers of the wound or the inability of the drug to cross the bacterial biofilm.15 In this context, nanotechnology offers novel opportunities to enhance drug delivery systems by utilizing materials at the nanoscale.16 The substantial increase in surface-to-volume ratio in nanoparticles leads to enhanced physicochemical reactivity, which is highly advantageous for medical applications.17 Nanoparticles can encapsulate unstable or toxic drugs, thereby preserve their stability and minimize side effects. This capability allows for targeted and precise drug delivery to the wound site, significantly improving therapeutic efficacy. This characteristic positions nanoparticles as a promising alternative for the treatment of antibiotic-resistant wound infections, while also reducing the likelihood of developing new microbial resistance.18
Poly (lactic-co-glycolic acid) (PLGA) is a biocompatible and biodegradable polymer that is widely recognized as a gold standard in drug delivery systems.19,20 Due to its ability to provide sustained and controlled drug release, high safety profile, and tunable degradation rate, PLGA enables the design of targeted and patient-specific therapeutic strategies.19 PLGA is particularly valuable in the fabrication of drug-loaded nanoparticles and has gained attention as a carrier in wound healing formulations.18 These nanoparticles release the drug locally at the site of injury, promoting tissue regeneration and accelerating wound healing.21 Owing to its amphipathic nature, PLGA nanoparticles possess hydrophobic cores and relatively hydrophilic surfaces, allowing them to encapsulate and transport poorly water-soluble drugs effectively.22 The well-documented clinical success, capacity to carry a wide range of therapeutic agents, and excellent safety of PLGA have established it as one of the most reliable and extensively used polymers in the field of drug delivery and biomedical applications.23
Medicinal plants contain a wide range of bioactive compounds, including flavonoids, alkaloids, phenolic acids, tannins, terpenoids, fatty acids, essential oils, and polyphenols, which exhibit antioxidant, antibacterial, antifungal, anti-inflammatory, and wound-healing properties.24,25 These compounds can enhance the effectiveness of antibiotics, thereby contributing to the revival of older drugs for clinical use and preventing the development of antimicrobial resistance. One promising approach to improve the efficacy of these compounds is through nanotechnology and the process of nanosizing. Nanoparticles, due to their high surface-area-to-volume ratio and ability to modify the physical and chemical properties of substances, can facilitate controlled release and enhanced penetration of plant-based compounds into wound tissues. The use of nanocarriers not only improves the bioavailability and therapeutic efficiency of these agents but also promotes faster wound healing, reduces wound-related complications, and enhances patient compliance.26
Chronic wounds are characterized by impaired angiogenesis, persistent inflammation, and fibroblast senescence, all of which contribute to delayed tissue regeneration. Advanced delivery systems such as poly (lactic-co-glycolic acid) (PLGA) nanoparticles have been widely explored to overcome these pathological barriers by enabling sustained and targeted release of bioactive natural compounds. For instance, curcumin and quercetin have been shown to modulate oxidative stress and inflammatory signaling pathways, thereby restoring fibroblast function and reducing cellular senescence. When encapsulated in PLGA carriers, these compounds exhibit improved stability, bioavailability, and controlled release, which enhances their therapeutic efficacy in chronic wound environments. Furthermore, PLGA-based delivery systems can promote angiogenesis by facilitating prolonged exposure of endothelial cells to pro-healing phytochemicals, ultimately improving neovascularization and tissue remodeling. Thus, integrating natural compounds into PLGA formulations provides a mechanistically driven strategy to specifically target key pathological features of chronic wounds, including defective angiogenesis and fibroblast dysfunction, thereby offering a rational framework for wound healing formulation design.27–29
This review aims to comprehensively discuss the recent progress of PLGA-based delivery systems loaded with natural compounds for the treatment of infected wounds, with particular emphasis on fabrication strategies, controlled and sustained drug release behaviors, and biofilm-targeting mechanisms. Since biofilm-associated infections represent one of the major causes of chronic wound persistence and antimicrobial resistance, PLGA nanocarriers have attracted considerable attention due to their ability to enhance drug penetration into the extracellular polymeric substance (EPS), maintain therapeutic drug concentrations for prolonged periods, and improve the stability and bioavailability of natural bioactive compounds. Furthermore, the sustained release properties of PLGA formulations may provide therapeutic advantages during different stages of wound infection and healing. In this context, Figure 1 clearly contrasts the biological processes underlying acute and chronic wound healing. It is essential to link the pathological differences, such as impaired epithelialization, sustained inflammation, immune evasion, biofilm formation, and increased virulence of pathogens, directly to the targeted effects of PLGA-based natural compound formulations. Specific natural compounds delivered by PLGA nanocarriers can reverse impaired epithelialization and fibroblast senescence, reduce chronic inflammation, and overcome biofilm-mediated immune evasion. Despite these promising findings, several translational challenges still limit the clinical application of PLGA-based systems, including large-scale manufacturing complexity, formulation stability, reproducibility, sterilization, regulatory approval, and insufficient clinical studies. Therefore, further investigations are required to optimize these nanostructures and facilitate their successful translation into clinical wound management applications.
PLGA
Nanoparticles (NPs) are solid, spherical structures ranging from 10 to 1000 nm in size, synthesized from either natural or synthetic polymers.30 They are capable of carrying diverse therapeutic agents, including hydrophilic and hydrophobic drugs, vaccines, and biological macromolecules, while enabling targeted delivery to specific tissues or cells and providing controlled release.31 Recent advances in therapy have highlighted the need for intelligent drug delivery systems with improved performance and efficiency.32 Controlled release of drugs remains a major challenge in pharmacology.33 Over the past decades, nanotechnology has significantly transformed various fields, including pharmaceuticals, where several nanomedicine products have already reached the market.34 In particular, the application of nanocarriers has been validated in both preclinical and clinical studies for enhancing the efficacy of many drugs, especially anticancer agents. Currently, multiple NP-based delivery systems are either established or under development, with the main objectives of minimizing drug degradation, reducing side effects, improving bioavailability, and promoting drug accumulation at the diseased site.35 In conventional drug administration, whether oral or injectable, the medication disperses throughout the body, leading to both therapeutic effects and systemic side effects.36 Achieving the desired outcome often requires large doses.37 To address this limitation, researchers have increasingly explored nanotechnology, which offers promising opportunities for targeted drug delivery.38
Polymeric particles have recently been widely investigated as drug carriers in cancer therapy and other pathological conditions, as their synthesis can be tailored to control physicochemical properties.39 Among biodegradable polymers, PLGA has attracted particular attention due to its biocompatibility and safe metabolic degradation into CO2 and water.40 Initially, developed in the 1970s for biodegradable sutures, PLGA has since been applied in implants, grafts, prosthetics, and, more recently, nanoscale drug delivery. It has been successfully used to encapsulate drugs such as paclitaxel, doxorubicin, cisplatin, docetaxel, and curcumin.41 PLGA particles provide several biomedical advantages: they can be functionalized with antibodies or targeting ligands, protect biomolecules from degradation, enhance immune responses, and maintain long-term stability in powder form.42 PLGA can be synthesized either by direct polycondensation, yielding low molecular weight polymers, or by ring-opening polymerization, producing higher molecular weight polymers with narrower molar mass distribution.43,44 Its molecular weight can be tuned from 4 to 240 kDa, and its degradation rate depends on polymer composition and microstructure.43,45 Notably, a 50:50 lactic-to-glycolic acid ratio results in the fastest degradation (~2 months in vivo) and the highest drug release rates.40 The solubility of PLGA varies with composition, ranging from chlorinated and water-miscible solvents to fluorinated solvents.46,47 Its glass transition temperature typically lies between 40–60 °C but decreases with lower molecular weight or reduced lactic acid content.40 While polymer characteristics determine basic particle properties, synthesis methods and encapsulated substances strongly influence particle size and distribution.40,46 Furthermore, surface modification with hydrophilic polymers such as polyethylene glycol (PEG) generates stealth particles that evade clearance by the reticuloendothelial system, prolong circulation time, and allow for more reproducible sustained-release profiles.48,49 PLGA is widely applied in drug delivery systems (DDSs) due to its excellent biocompatibility and biodegradability. It enables controlled drug release, protects active compounds from degradation, and maintains stability throughout the product life cycle.50,51 In aqueous environments, PLGA undergoes a four-stage degradation process: hydration, initial degradation, continuous degradation, and solubilization. This sequence involves water penetration, bond cleavage, autocatalysis, and eventual dissolution of polymer fragments.43,52 Serving both as a drug carrier and a structural matrix, PLGA has been the basis of several FDA-approved products that rank among the most successful complex therapeutics.20,53 Its advantages include high encapsulation efficiency, favorable biocompatibility, stable release behavior, and sufficient bioavailability. Moreover, nano-PLGA formulations improve aqueous solubility, enhance bioavailability, and increase the stability of active pharmaceutical ingredients (APIs).30
Preparation of PLGA-Based Particles
The production of PLGA particles with tailored characteristics, such as particle size or degradation rate, requires careful selection of the synthesis method, raw materials, and processing parameters. Particle size can be influenced by several factors, including polymer concentration, the type and amount of surfactant, the encapsulated compound, and the applied energy input (eg, sonication, homogenization, or shear stirring). Moreover, the efficiency of drug loading and release is strongly dependent on the chosen fabrication approach, the physicochemical properties of the therapeutic agent, and the intended route of administration.54 Table 1 outlines different techniques employed for the preparation of PLGA nanoparticles.
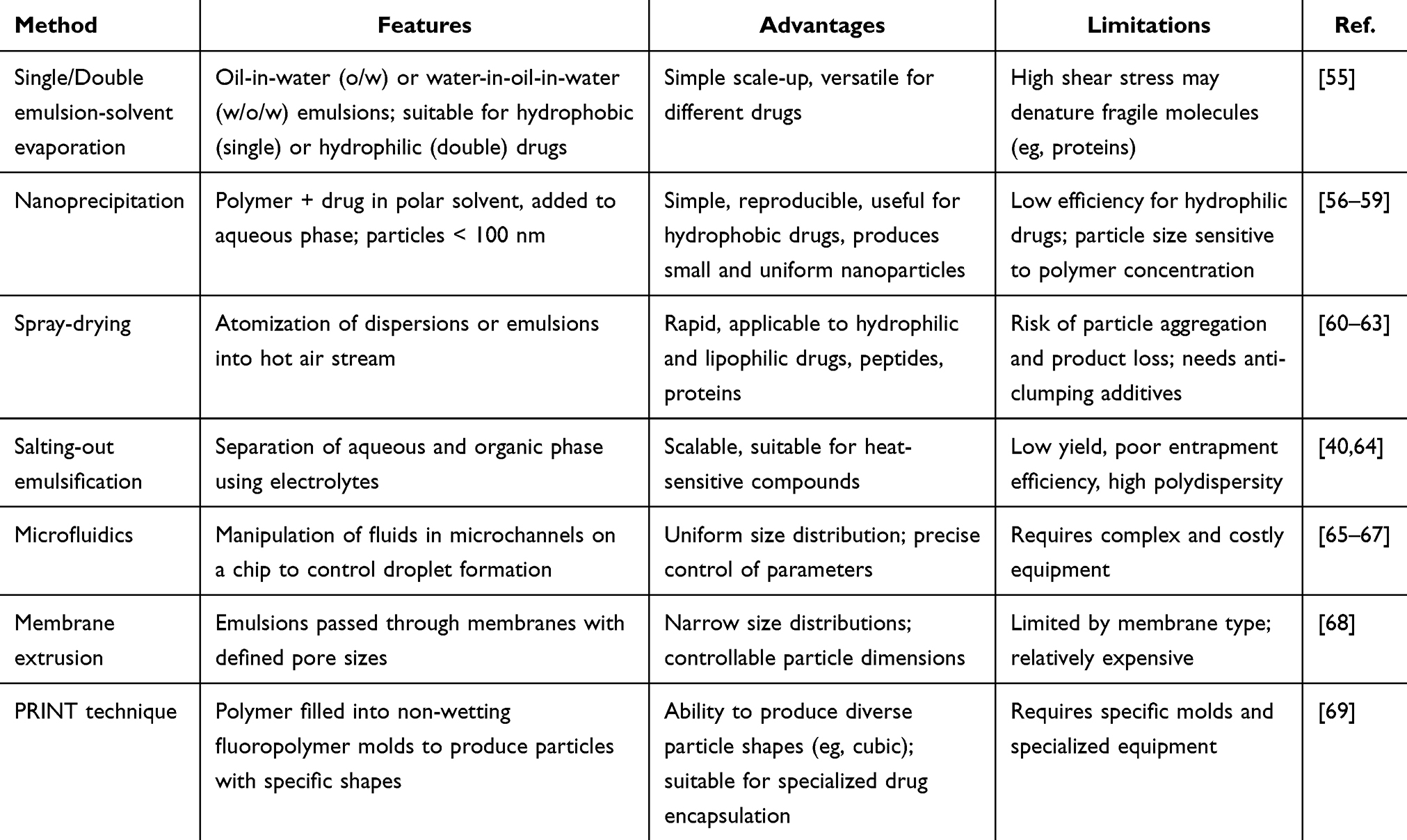 |
Table 1 Comprehensive Insights into PLGA Particle Synthesis Approaches |
Wound Healing Overview
A wound is defined as any disruption of tissue integrity, and given that the skin functions as the largest organ and the primary protective barrier against the external environment, maintaining its integrity is essential for survival and physiological homeostasis.70 Wound healing is therefore a highly regulated and dynamic biological process, yet it remains a major clinical and economic burden,71 particularly in chronic conditions such as diabetic foot ulcers (DFUs), which affect nearly one-quarter of diabetic patients and frequently lead to severe complications including amputation. The repair of injured tissue occurs through four temporally overlapping but functionally distinct phases: hemostasis, inflammation, proliferation, and remodeling.72 Immediately following injury, the hemostasis phase is initiated through vasoconstriction, platelet aggregation, and fibrin clot formation, which not only prevents blood loss but also establishes a provisional extracellular matrix (ECM) scaffold enriched with growth factors such as PDGF and TGF-β that guide subsequent cellular events. This is followed by the inflammatory phase, characterized by the infiltration of neutrophils and monocytes/macrophages that eliminate pathogens and cellular debris; however, excessive or prolonged inflammation—commonly observed in diabetic wounds—disrupts healing. A critical regulatory mechanism within this phase is the phenotypic transition of macrophages from the pro-inflammatory M1 state to the anti-inflammatory, tissue-repairing M2 phenotype, a shift that is often impaired under hyperglycemic, hypoxic, and oxidative stress conditions, leading to persistent inflammation and delayed healing. During the proliferative phase, fibroblasts, keratinocytes, and endothelial cells actively contribute to granulation tissue formation, re-epithelialization, and angiogenesis. Collagen type III deposition, along with the formation of new capillary networks mediated by VEGF, plays a central role in restoring tissue architecture. However, in DFUs, hypoxia and excessive reactive oxygen species (ROS) disrupt mitochondrial function, impair cell migration, and inhibit angiogenesis, thereby preventing effective progression to this stage. Finally, the remodeling phase involves the gradual replacement of collagen type III with collagen type I, matrix reorganization, and increased tensile strength of the repaired tissue, processes that may last for months and are frequently incomplete in chronic wounds.73 Recent advances in biomaterials, particularly hydrogel-based systems, have introduced promising strategies to overcome these pathological barriers by actively modulating the wound microenvironment. Hydrogels, composed of hydrophilic polymer networks that mimic the ECM, provide a moist and protective environment while enabling the controlled delivery of bioactive agents. Importantly, next-generation immunomodulatory hydrogels are designed not only to scavenge ROS but also to address hypoxia and immune dysregulation simultaneously. For instance, the engineered RGH2 hydrogel, incorporating Ru@allomelanin nanoparticles, GelMA-PBA, and HA-based components, demonstrates a dual function of oxygen generation and ROS neutralization, effectively disrupting the ROS–inflammation feedback loop and promoting macrophage polarization toward the M2 phenotype.73 This leads to reduced inflammation, enhanced collagen synthesis, and improved angiogenesis, ultimately accelerating wound closure.73 Similarly, advanced adhesive hydrogels such as SCE2, enriched with bioactive nanoparticles derived from natural sources like cuttlefish ink, provide strong tissue adhesion, antimicrobial activity, and antioxidative effects, facilitating the transition from inflammation to proliferation, particularly in challenging environments such as oral mucosa.74 Collectively, these findings highlight that successful wound healing depends on the precise coordination of all four phases and that disruption at any stage, especially due to hypoxia, oxidative stress, and immune imbalance, can lead to chronic non-healing wounds. Modern multifunctional biomaterials, by targeting these underlying mechanisms, offer a transformative approach to restoring the healing cascade, particularly in complex conditions such as diabetic wounds. Natural bioactive compounds and poly (lactic-co-glycolic acid) (PLGA) play complementary roles in enhancing the different phases of wound healing. Natural compounds such as polyphenols, terpenoids, and flavonoids exhibit potent antioxidant, anti-inflammatory, and antimicrobial activities, which are essential for modulating the inflammatory phase and preventing excessive reactive oxygen species (ROS)-induced tissue damage. These compounds can also stimulate key signaling pathways involved in angiogenesis, fibroblast proliferation, collagen deposition, and re-epithelialization, thereby accelerating the proliferative and remodeling phases of healing.75,76 In parallel, PLGA serves as a biodegradable and biocompatible polymeric carrier that enables controlled and sustained release of therapeutic agents, maintaining optimal local drug concentrations at the wound site. Moreover, PLGA-based scaffolds and nanocarriers support cell adhesion, migration, and tissue regeneration, while protecting encapsulated bioactive molecules from premature degradation.46,75 The synergistic integration of natural compounds with PLGA systems therefore provides a promising strategy to regulate the wound microenvironment and promote efficient, multi-stage tissue repair. Table 2 presents the stages of wound healing along with their underlying mechanisms.
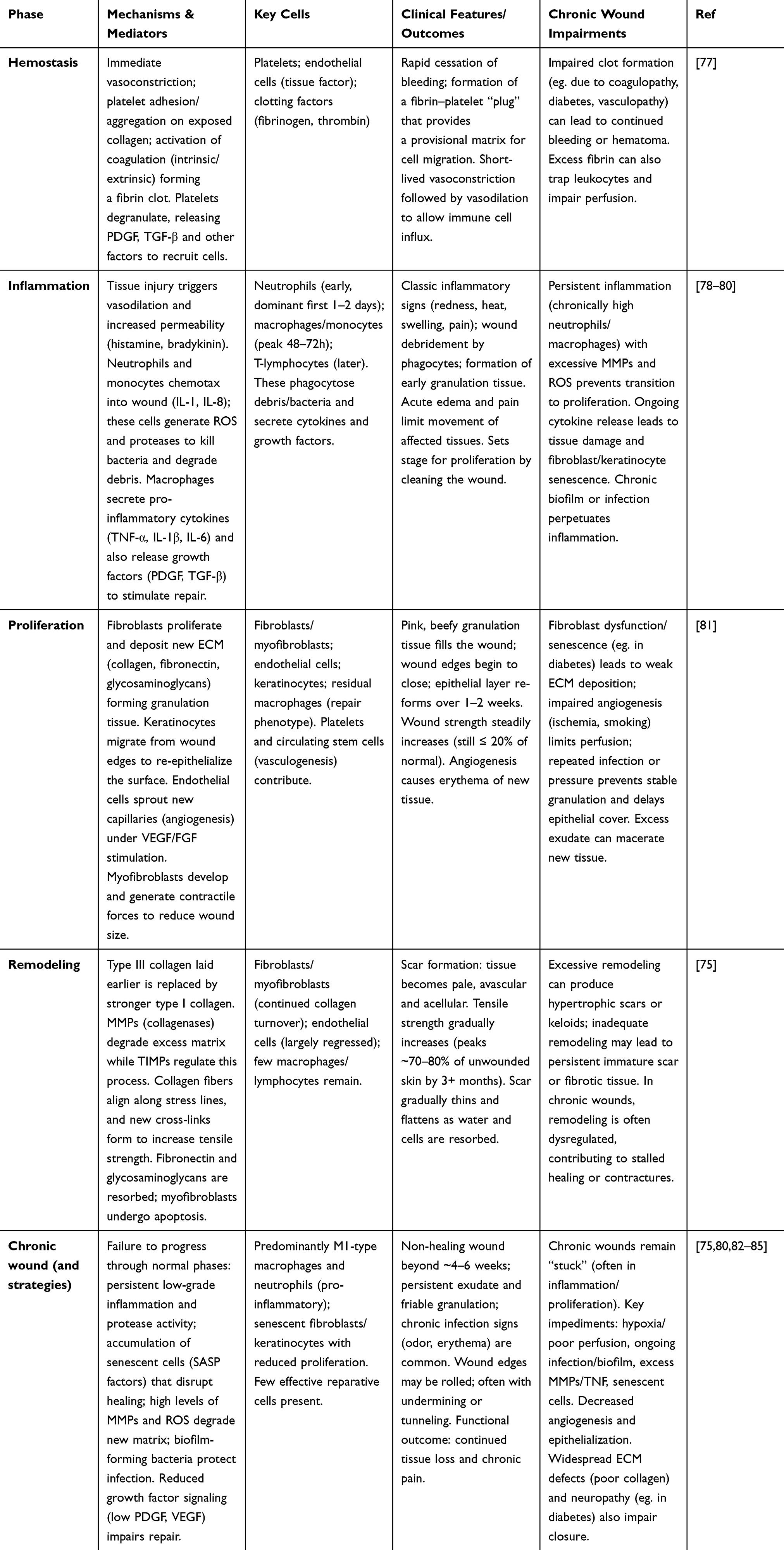 |
Table 2 Wound Healing Phases and Chronic Impairment Overview |
The Role of Biofilm in Wound Chronicity
Chronic wounds are defined as those that fail to achieve anatomical and functional integrity within one month.86 With the aging of the global population, these wounds represent an increasing healthcare burden.87 The major categories include diabetic ulcers, pressure injuries, and venous leg ulcers. Standard management typically involves debridement of necrotic tissue, application of carefully selected dressings, and administration of local or systemic antimicrobial agents, while specific therapies must address the underlying etiology of each ulcer type. In severe, life-threatening cases, distal limb amputation may be required. Despite diligent care, treatment frequently fails when secondary infection develops. A principal reason for this failure is biofilm formation, which remains a major barrier to effective healing in chronic wound infections.87,88 Biofilm development progresses through four stages: surface attachment, microcolony formation, maturation, and dispersal.88 Mature biofilms are predominantly composed of extracellular polymeric substances (EPS), which provide structural integrity, facilitate adhesion, and protect bacteria from environmental stress and host defenses (Figure 2).89 Moreover, EPS and its components, including polysaccharides and alginate, suppress pro-inflammatory cytokines, inhibit immune cell infiltration, and protect against complement-mediated killing.87 These immune-evasion strategies contribute to persistent inflammation. Elevated levels of cytokines and growth factors—including TNF-α, IL-6, and VEGF—are commonly observed in chronic wounds. In particular, excessive TNF-α production, linked to dysregulation of its converting enzyme (TACE), plays a central role in impaired healing and parallels other chronic inflammatory conditions.90,91 The most commonly isolated bacteria in chronic wounds are S. aureus and P. aeruginosa, which produce virulence factors and sustain persistent inflammation, thereby impairing wound healing.92 Clinical indicators of biofilm presence include a pale and edematous wound bed, fragile granulation tissue, excessive exudate, necrotic tissue, pain, and foul odor.93 Indirect signs of biofilm infection include poor response to antibiotics, delayed wound healing, recurrent infections, chronic inflammation, and abundant exudate.92 Biofilm detection in wounds can be performed using various methods, including standard microbial culture,82 electron and confocal microscopy,94,95 specialized EPS staining, molecular analysis via 16S rRNA sequencing, metabolomics, wound blotting, transcriptomics, and artificial intelligence–based approaches. Bacteria within biofilms are often in a viable-but-non-culturable (VBNC) state, contributing to antibiotic resistance and making detection difficult. Therefore, effective management of chronic wounds requires biofilm disruption, inhibition of bacterial cooperation, and control of bacterial dissemination to optimize the wound healing process. Debridement, which involves the removal of necrotic tissue, foreign bodies, and poorly healed tissue that serve as sites for bacterial colonization and biofilm formation, creates a clean wound environment conducive to healing and is considered the primary treatment for chronic wounds. Additionally, debridement temporarily disrupts mature biofilms, providing a window for wound repair. Antimicrobial Therapy Targeting Microbial Metabolic Processes: Phage Therapy, Nanotechnology, Blue Light Therapy, Population Effect Inhibitors, Aptamers, Peptide Nucleic Acids, Biodegradation-Related Enzymes, Antimicrobial Peptides, Catabolite Control Protein A.92
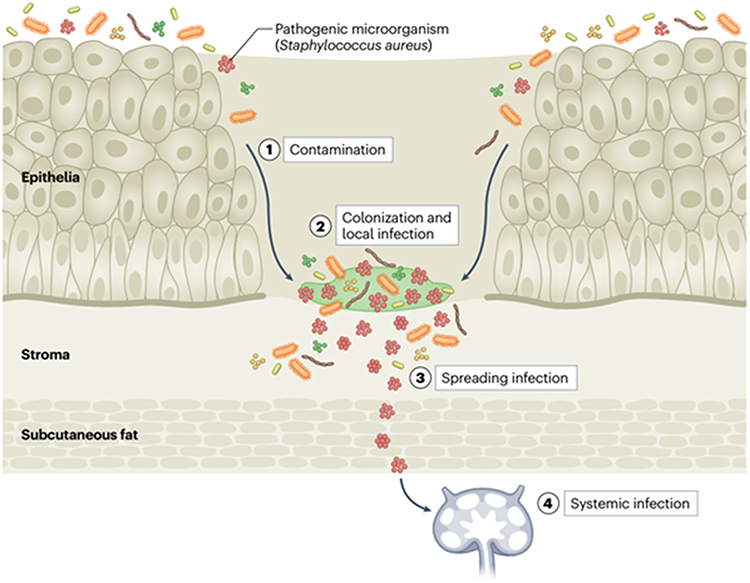 |
Figure 2 The wound infection continuum in chronic wounds. Chronic wounds, which fail to regain structural and functional integrity within one month, often progress along a wound infection continuum. Initially, microorganisms from the environment or skin contaminate the wound surface (phase 1). Nutrient-rich exposed tissue promotes microbial colonization (phase 2), which can advance to local infection or biofilm formation (phase 3). In chronic wounds such as diabetic, pressure, or venous ulcers, biofilms are key contributors to persistent infection and impaired healing. Mature biofilms protect bacteria through extracellular polymeric substances (EPS), enabling immune evasion and chronic inflammation. If unchecked, localized infection may spread to deeper tissues or become systemic (phase 4), further complicating management. Understanding this continuum clarifies how microbial progression, particularly biofilm development, underlies the chronicity and therapeutic resistance of these wounds. Reprinted from14 with permission from Springer Nature. |
The therapeutic efficacy of PLGA–natural compound formulations can be correlated with the temporal progression of chronic wound infection. During the contamination and early colonization stages, the initial burst release of encapsulated antimicrobial phytochemicals may rapidly reduce planktonic bacterial load and suppress early bacterial adhesion. As infection progresses toward mature biofilm formation, the sustained release behavior of PLGA-based systems becomes particularly advantageous by maintaining prolonged local therapeutic concentrations capable of penetrating the extracellular polymeric substance (EPS) matrix and disrupting biofilm stability. Several studies have demonstrated that PLGA nanoparticles enhance the penetration of antimicrobial agents into deeper biofilm layers while reducing rapid drug clearance and minimizing bacterial regrowth. Furthermore, prolonged release kinetics may help prevent recurrent infection and reduce selective pressure associated with repeated high-dose antibiotic exposure. In advanced or systemic infection stages, multifunctional PLGA formulations containing anti-inflammatory and antioxidant natural compounds may additionally modulate excessive inflammation, oxidative stress, and tissue damage, thereby supporting tissue regeneration alongside antimicrobial activity. Therefore, the release profile of PLGA-based delivery systems appears to align closely with the dynamic pathological stages of chronic wound infection and may provide stage-specific therapeutic benefits.31,96–98
Natural Products in Wound Healing
Natural compounds with medicinal properties play a beneficial role in the wound healing process. Numerous studies have demonstrated their therapeutic potential, highlighting activities such as anti-inflammatory, antioxidant, antibacterial, and collagen-stimulating effects. These healing properties are largely attributed to their bioactive phytochemicals, which belong to diverse chemical classes including alkaloids, essential oils, flavonoids, tannins, terpenoids, saponins, and phenolic compounds.83 Numerous studies have highlighted the potential of natural compounds to enhance wound healing, suggesting their applicability across different phases of the repair process.75,99 Compared to certain synthetic agents, these compounds are generally considered safer, better tolerated, and more cost-effective than conventional therapeutic approaches.75
In vitro Evaluation of Natural Products for Their Potential in Wound Healing
Natural products have been widely investigated as potential sources of bioactive compounds with wound-healing properties. Prior to in vivo validation, their effects are typically examined through in vitro assays, with keratinocyte and fibroblast cell lines serving as standard models for assessing regenerative activity.75
The genus Aloe comprises over 550 species, with leaves and roots rich in diverse bioactive phytochemicals.100 Species such as Aloe vera and Aloe arborescens are renowned for their medicinal properties, including antioxidant, anti-inflammatory, antibacterial, anti-aging, and anticancer activities. Among these, Aloe saponaria (syn. Aloe maculata) has been traditionally used in southern Brazil for burn treatment and contains flavonoids (rutin, quercetin, kaempferol) and phenolic acids (gallic and caffeic acids), which contribute to its anti-inflammatory, antioxidant, analgesic, and anticancer effects.101 In a study by Kim et al,102 extracellular vesicles derived from Aloe saponaria (AS-EVs) were isolated using an optimized polyethylene glycol (PEG)-based precipitation method. This approach allows for rapid, cost-effective, and scalable isolation of large quantities of vesicles from edible plants with low toxicity. AS-EVs demonstrated efficient cellular uptake in various mammalian cell types without causing significant cytotoxicity. Functionally, AS-EVs reduced the expression of pro-inflammatory cytokines in LPS-stimulated RAW264.7 macrophages, thereby mitigating the initial inflammatory phase of chronic wounds. They also enhanced proliferation and migration of human dermal fibroblasts and promoted angiogenesis in human umbilical vein endothelial cells, facilitating nutrient delivery to the wound site and accelerating tissue repair.
Propolis is a resinous substance rich in polyphenolic compounds and widely used in traditional medicine, cosmetics, and the food industry.103 It exhibits diverse pharmacological activities, including antioxidant, antimicrobial, anti-inflammatory, and anticancer effects.104–106 Its main bioactive constituents include caffeic acid phenethyl ester (CAPE) and flavonoids such as chrysin, drupanin, cardanol, pinobanksin, galangin, and pinocembrin.107 Composed primarily of resins, waxes, aromatic oils, bee saliva, pollen, and other minor components, propolis not only protects beehives but also plays a role in connective tissue regulation and collagen synthesis, highlighting its therapeutic potential.108 Necip et al,108 evaluated the wound-healing potential of propolis water extract (PWE) on oral mucosal fibroblast cells. The results demonstrated that PWE enhanced wound closure compared to untreated controls. Phenolic compounds such as fraxetin, apigenin, galangin, pinobanksin, and chrysin were isolated and structurally characterized, showing notable antioxidant capacity and acetylcholinesterase (AChE) inhibition with IC50 values between 0.45 ± 0.01 and 1.15 ± 0.03 mM. In vitro assays further revealed that human gingival fibroblasts (hGFs) treated with 62.5 µg/mL PWE exhibited the highest cell viability and significantly improved wound closure rates of 55.9% and 79.3% after 24 and 48 h, respectively, compared to 51% and 65% in controls. Collectively, these findings highlight the therapeutic promise of PWE, attributing its efficacy to antioxidant and bioactive phenolic compounds that support oral mucosal wound healing.
Curcumin, traditionally used for wound treatment, has recently gained scientific validation for its efficacy in both acute and chronic wounds.109 Beyond its antibacterial, antioxidant, and anti-inflammatory properties, curcumin contributes to all stages of wound healing.110 It regulates inflammation by suppressing IL-1 and TNF-α production, reduces oxidative stress, and enhances fibroblast migration, granulation tissue formation, collagen deposition, and re-epithelialization. Moreover, by stimulating TGF-β synthesis and fibroblast proliferation, curcumin facilitates tissue remodeling and wound contraction, establishing its role as a potent therapeutic agent in wound management.110 Quercetin, a natural polyhydroxy flavonoid, possesses strong antioxidant and anti-inflammatory properties that facilitate wound healing by regulating oxidative stress and inflammation.111 Studies have demonstrated that quercetin accelerates wound repair through modulation of inflammatory cells, enhancement of fibroblast proliferation, reduction of immune cell infiltration, suppression of fibrosis and scar formation, and regulation of fibrosis-associated signaling pathways.112 In diabetic wounds, it has also been shown to suppress inflammatory responses by modulating macrophage polarization, thereby promoting cutaneous wound healing through the regulation of cytokines, angiogenic growth factors, and antioxidant systems.113 Chittasupho et al,114 conducted a study to evaluate the effects of quercetin, curcuminoids, and their combinations on bacterial inhibition, antioxidant activity, cell proliferation, and migration in the wound healing process. Their findings revealed that the strongest antibacterial activity against S. aureus and P. aeruginosa was observed with the 1:1 quercetin/curcuminoid combination, whereas the individual compounds showed no such effect. In the cell migration assay, quercetin alone and the 3:1 quercetin/curcuminoid mixture exhibited the greatest potential in accelerating human dermal fibroblast migration. Regarding antioxidant capacity, quercetin outperformed curcuminoids, while their mixtures demonstrated intermediate activity. Overall, quercetin alone and the 3:1 quercetin/curcuminoid combination were identified as the most effective formulations for wound healing, owing to their antibacterial, antioxidant, and cell migration-enhancing properties. The biological activities of selected natural compounds effective in wound healing are summarized in Table 2.
In vivo Evaluation of Natural Products for Their Potential in Wound Healing
The study by Kapare et al,115 was conducted with the aim of developing and optimizing a polyvinyl alcohol (PVA)-based hydrogel containing Indian propolis extract for wound healing applications. The hydrogel formulation was optimized using a design of experiments (DOE) approach, while FTIR and DSC analyses confirmed the uniform distribution of propolis within the hydrogel matrix. Animal models of burn, excision, and incision wounds demonstrated that the propolis hydrogel induced significant wound contraction (over 90% within 21 days) and accelerated epithelial regeneration, with outcomes comparable to the standard 5% povidone-iodine ointment. Moreover, acute toxicity studies confirmed the safety of the formulation. Overall, the findings indicate that the Indian propolis-loaded hydrogel is a safe and effective formulation that can reduce inflammation, stimulate collagen expression, and promote epithelialization, making it a promising natural drug delivery system for wound healing.
Cinnamon essential oil, owing to its antioxidant and antibacterial properties, has the potential to accelerate wound healing. In the study conducted by Seyed Ahmadi et al,116 the effects of an ointment containing Cinnamomum verum essential oil were evaluated in an infected wound model in mice. Circular wounds (5 mm in diameter) were created and infected with S. aureus and P. aeruginosa. The animals were divided into three groups and topically treated with control (soft paraffin), 2% ointment, and 4% ointment. The results indicated that topical application of cinnamon, particularly at the 2% concentration, shortened the inflammatory phase, enhanced fibroblast proliferation, collagen deposition, epithelial regeneration, and keratin synthesis. Moreover, the expression of IGF-1, FGF-2, and VEGF was significantly upregulated in the treated groups, while tissue antioxidant capacity increased and malondialdehyde (MDA) levels decreased. Overall, cinnamon promoted granulation tissue formation, balanced inflammatory cell infiltration, and facilitated a faster transition from the inflammatory to the proliferative phase through the upregulation of growth factors, ultimately accelerating wound repair. However, further investigations are required to clarify its precise anti-inflammatory mechanisms.
In the study by Khurshid et al,117 cinnamon oil (CO) and aloe vera (AV), both traditionally recognized for their antibacterial properties, were combined into a novel gel formulation (COVA) and evaluated through in vitro and in vivo experiments. Antibacterial activity was assessed against P. aeruginosa and S. aureus using disk diffusion and agar dilution methods, while wound healing potential was tested in a diabetic rat excision model. Key indicators, including wound closure, contraction, hydroxyproline content, total antioxidant capacity (TAC), and malondialdehyde (MDA) levels, were measured. Results showed that COVA achieved 79% wound contraction after 14 days, significantly enhanced collagen deposition and antioxidant activity (P<0.05), and reduced MDA levels compared to controls. Histopathological analysis further confirmed improved tissue regeneration, with a marked increase in hydroxyproline concentration in the COVA-treated group. Overall, the results suggest that the combination of cinnamon oil and Aloe vera in the COVA gel produces a notable synergistic effect in wound healing, as each component contributes through distinct yet complementary mechanisms. Cinnamon oil primarily reduces bacterial load via membrane disruption, while Aloe vera supports tissue repair by providing anti-inflammatory and regenerative effects. The interaction between these two agents enhances key healing parameters, including increased hydroxyproline levels as a marker of collagen synthesis, improved antioxidant status, and decreased oxidative stress, reflected by lower MDA levels. These combined effects lead to faster wound contraction and more efficient re-epithelialization. Consequently, this formulation not only strengthens antimicrobial activity but also facilitates multiple aspects of the healing process, suggesting its potential as a practical and cost-effective approach for managing chronic wounds, particularly those associated with diabetes.
Commiphora gileadensis (CG), a small shrub traditionally used in the Middle East for perfumes and in Saudi Arabia for treating wounds, burns, and scorpion stings, was investigated by Alhazmi et al,118 for its antimicrobial and wound healing properties. A methanolic extract of CG, characterized by LC–MS, revealed high levels of ceramide, hexosylceramide, and phosphatidylethanolamine. In a murine excision wound model, both infected and non-infected wounds treated with CG extract showed significantly greater wound contraction, reduced bacterial load, and improved histopathological parameters, including lower inflammatory cell infiltration, enhanced collagen deposition, granulation tissue formation, and re-epithelialization compared with controls (p < 0.01). These findings indicate that CG possesses antibacterial and anti-inflammatory effects that accelerate wound repair. The study suggests further evaluation of its efficacy in diabetic wounds and recommends isolation and characterization of its active bioactive compounds for potential antimicrobial applications. Table 3 presents the biological activities of various natural compounds with proven efficacy in wound healing.
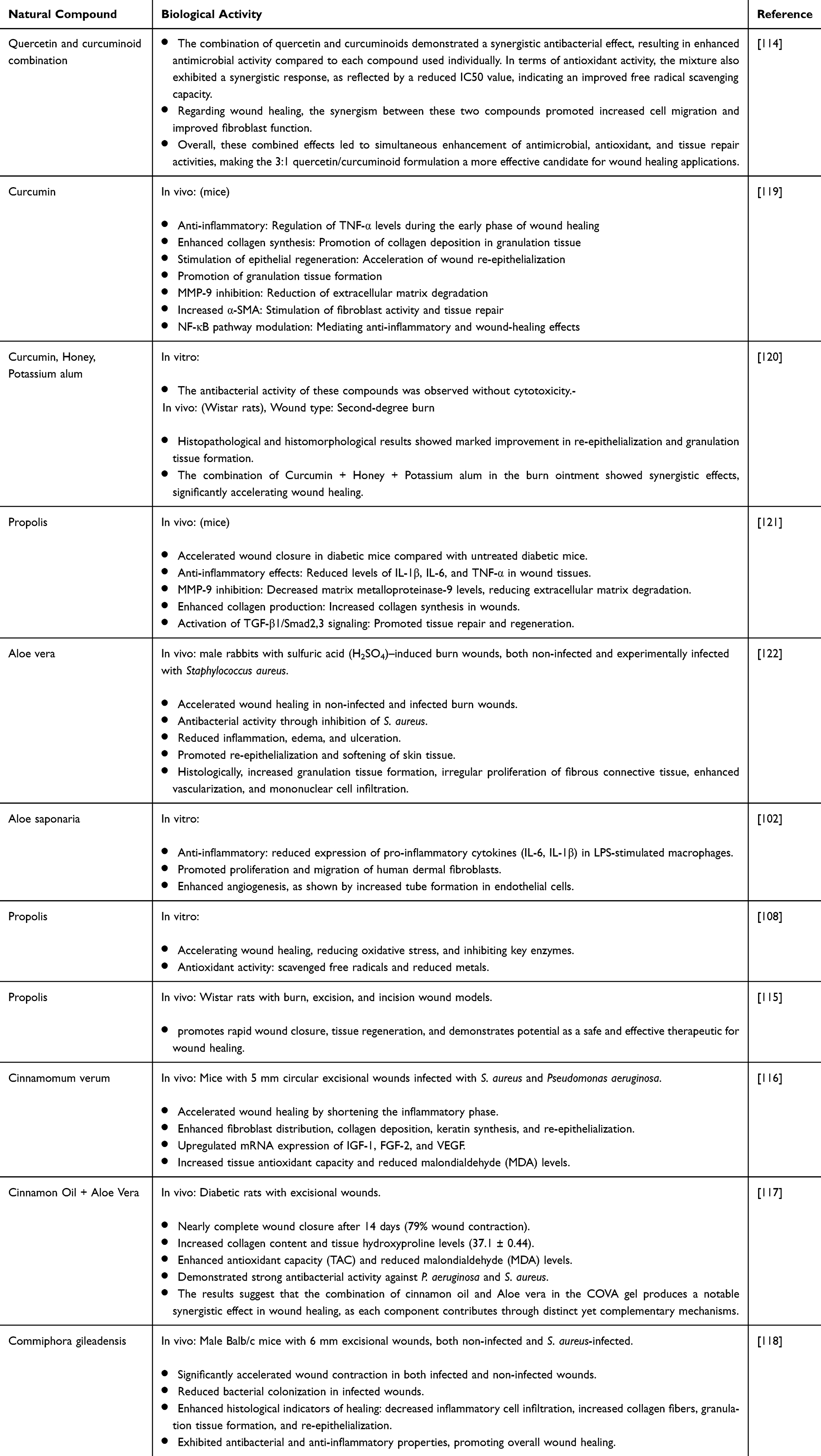 |
Table 3 Overview of the Bioactivities of Natural Compounds Involved in Wound Healing |
Encapsulation of Natural Compounds in PLGA
Various methods have been employed in studies for loading natural compounds into PLGA nanoparticles. In the study by Kizilbey et al,123 the loading of rutin (a natural flavonoid with important bioactivities but poor solubility and low bioavailability) into PLGA nanoparticles was investigated. The method applied was a single oil-in-water emulsion followed by solvent evaporation. To overcome rutin’s low solubility, propylene glycol was used as a solvent. During nanoparticle synthesis, different amounts of rutin and PLGA, varying PVA concentrations, and different aqueous-to-organic phase ratios were tested to determine optimal formulation conditions. The results demonstrated that nanoparticle NP4, with an average size of approximately 252 nm, a reaction yield of 47%, and an encapsulation efficiency of 81%, exhibited the most favorable characteristics. In vitro release studies showed that at a concentration of 0.5 mg/mL, rutin-loaded NP4 achieved complete release (100%) within five days (120 h). SEM imaging further confirmed the uniform spherical morphology of the nanoparticles. Overall, the findings indicate that encapsulation of rutin into PLGA nanoparticles offers an effective strategy to improve the solubility, bioavailability, and biological activities of poorly soluble natural compounds. Moreover, this approach provides a useful model for the encapsulation of other therapeutic or natural agents with potential clinical applications. In the study by Alam et al,124 curcumin-loaded PLGA nanoparticles (CUR-NPs) were synthesized with the aim of enhancing the bioavailability and therapeutic potential of curcumin, a natural compound with well-documented anticancer and antibacterial properties. The nanoparticles were prepared using a single oil-in-water emulsion solvent evaporation method. Polyvinyl alcohol was employed as a stabilizer, and following sonication and centrifugation, the resulting nanoparticles were washed and lyophilized. The findings demonstrated that encapsulating curcumin within PLGA nanoparticles is an effective strategy to improve its solubility, bioavailability, and biological activities, particularly its anticancer and antibacterial effects. This nanoformulation shows promise as a potential therapeutic option for the treatment of gastric cancer and Helicobacter pylori infection, although further in vivo studies are required to validate these results. In the study by Leung et al,125 curcumin, a natural compound with therapeutic properties, was encapsulated into PLGA nanoparticles using a microfluidic-assisted nanoprecipitation method. This innovative approach enabled the synthesis of nanoparticles without surfactants, with controllable sizes ranging from 30 to 70 nm and a narrow size distribution (PDI < 0.2). The resulting nanoparticles exhibited high colloidal stability and effectively prevented curcumin degradation.
Biological evaluations demonstrated a dose-dependent cytotoxic effect of curcumin-loaded PLGA nanoparticles (Cur-PLGA NPs) against Jurkat leukemia cells, while no significant effect was observed on normal NIH3T3 fibroblasts. Empty PLGA nanoparticles showed no cytotoxicity, confirming the safety of PLGA as a carrier. Confocal microscopy further revealed that PLGA did not interfere with curcumin uptake by cells. These findings highlight microfluidic nanoprecipitation as an efficient strategy for curcumin encapsulation in PLGA, offering improved stability, controlled particle size, and a safe, selective drug delivery system. This method holds promise for encapsulating other natural bioactive compounds in biomedical applications. In study of Roshan et al,126 PLGA nanoparticles loaded with curcumin (CUR), a natural bioactive compound, were prepared using two different synthesis methods: nanoprecipitation and electrospray. In the nanoprecipitation method, an organic solution of PLGA and curcumin was added dropwise into an aqueous PVA solution to form nanoparticles, which were then washed and lyophilized. In the electrospray method, the PLGA-curcumin solution in DMF/chloroform was sprayed under high voltage, and the resulting particles were collected and dried. Various parameters, including PLGA and PVA concentrations and applied voltage, were optimized to control particle size and polydispersity index (PDI). The results indicated that both methods successfully encapsulated curcumin; however, electrosprayed nanoparticles exhibited smaller size, lower PDI, higher encapsulation efficiency, and greater drug loading, with a slower and more controlled drug release. In vitro release studies demonstrated that both types of nanoparticles maintained sustained release for over 300 hours, following a biphasic pattern described by the Weibull model. Biological assays further showed that CUR-loaded PLGA nanoparticles possess significant antibacterial activity and could serve as a drug delivery system to prevent biofilm formation and dental plaque accumulation. Overall, the study demonstrates that the choice of synthesis method (nanoprecipitation or electrospray) substantially affects particle size, stability, encapsulation efficiency, and drug release profile. Optimizing these parameters enables the development of more effective and controlled drug delivery systems.
PLGA Nanoparticles Loaded with Natural Compounds for Wound Infection Management
In the study by Amirthalingam et al,127 a novel chitosan scaffold embedded with PLGA–curcumin microparticles was designed and fabricated for wound-healing applications. The curcumin microparticles were incorporated into the scaffold using an optimization approach based on design of experiments, and the porous structure of the scaffold was confirmed by scanning electron microscopy. The scaffold demonstrated sustained release of curcumin, with a maximum release of 14% observed at the 12th hour. Antimicrobial evaluation showed that the scaffold significantly (p < 0.05) inhibited the growth of S. aureus. In vivo wound-healing studies in a murine model revealed that over 50% of the wounds healed within 4 days, with an epithelialization period of 18 days, which was faster compared to the control group. Overall, the PLGA–curcumin microparticle-embedded scaffold provides a combination of sustained drug release and microbial protection, making it a promising multifunctional drug delivery system for the treatment of severe and chronic wounds. Moreover, the scaffold system allows for integration with cell culture techniques, such as mesenchymal stem cells, enabling a comprehensive platform for simultaneous drug delivery and tissue regeneration. In the study by Almukainzi et al,128 gentiopicroside (GPS), a natural compound with antioxidant and antimicrobial properties, was investigated for its potential to enhance wound healing. Due to its poor aqueous solubility and low bioavailability, GPS was encapsulated in PLGA nanospheres (PLGA NSs). The nanoparticles were synthesized and optimized using a single oil-in-water (O/W) emulsion solvent evaporation method, and the effects of polymer (PLGA) and stabilizer (PVA) concentrations on the physicochemical properties were evaluated. The optimized formulation (F5) exhibited a controlled particle size (~250 nm), high encapsulation efficiency (83.35%), and sustained release (~85% over 3 days). The PLGA-loaded GPS nanoparticles demonstrated superior antimicrobial activity against S. aureus compared to free GPS. Furthermore, in vivo studies in diabetic rat showed that GPS-PLGA NSs significantly improved wound healing, promoting re-epithelialization, granulation tissue formation, and collagen synthesis. Overall, this study demonstrated that encapsulating GPS in PLGA nanospheres is an effective strategy to enhance stability, achieve controlled drug release, and improve the therapeutic efficacy of this natural compound in wound healing applications. In study of Azzazy et al,129 a harmala alkaloid-rich fraction (HARF), a natural compound with antibacterial and wound-healing properties, was loaded into PLGA nanoparticles coated with chitosan (H/CS/PLGA NPs). The nanoparticles were prepared using the emulsion–solvent evaporation method and optimized through a Box–Behnken experimental design. The resulting nanoparticles had an average particle size of 202 nm, a polydispersity index (PDI) of 0.23, a zeta potential of 9.22 mV, and an encapsulation efficiency of 86.77%. Drug release studies demonstrated a biphasic pattern, with an initial burst release of 82.5% within the first 2 hours, followed by a gradual release reaching 87.5% over 72 hours. Antibacterial activity results showed that H/CS/PLGA NPs exhibited superior inhibitory effects against S. aureus and E. coli (MICs of 0.125 and 0.06 mg/mL, respectively) compared to free HARF (MIC = 0.5 mg/mL). The nanoparticles were found to be biocompatible, and wound-healing assays revealed that 24 hours after application, wound closure with H/CS/PLGA NPs reached approximately 94.4%, compared to 68.2% with free HARF and 50.5% with unloaded nanoparticles. These findings indicate a synergistic effect of PLGA, chitosan, and HARF in enhancing both antibacterial activity and wound healing. In the study by Abdelazimet et al,130 electrospun nanofibers incorporating Syzygium cumini leaf extract (SCLE) along with PLGA, PMMA, collagen, and glycine were developed as wound dressing scaffolds for topical wound healing. Electrospinning conditions were optimized to produce uniform nanosized fibers with smooth surfaces. The nanofibers were evaluated for morphology, swelling behavior, and antibacterial activity against multidrug-resistant and pathogenic bacteria. Results demonstrated that nanofibers containing 0.5% and 1% w/v SCLE exhibited significantly higher antibacterial activity compared to equivalent concentrations of the free extract. In vivo studies in Wistar rats showed that SCLE- and collagen-loaded nanofibers substantially enhanced wound healing over two weeks compared to the untreated control group. These findings highlight the potential of the fabricated nanofibers to accelerate acute wound healing and manage local infections effectively. Table 4 presents a summary of natural compounds loaded into PLGA particles and their roles in infected wound healing.
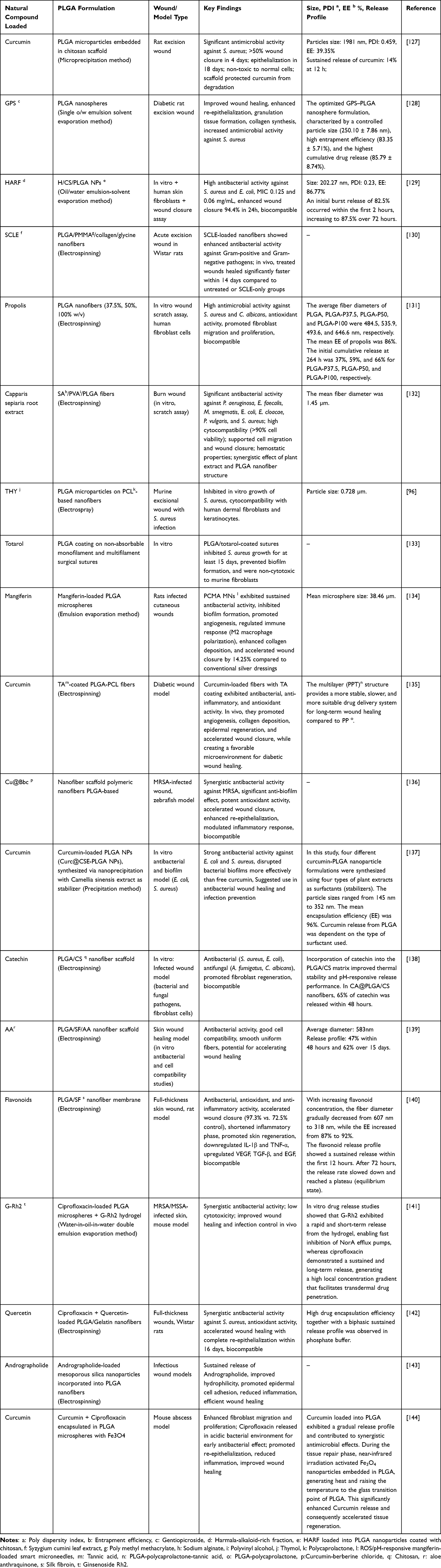 |
Table 4 An Overview of PLGA Particles Loaded with Natural Compounds and Their Roles in the Healing of Infected Wounds |
Several mechanisms have been proposed to explain the antibiofilm activity of PLGA nanoparticles: (1) modulation of quorum sensing systems and disruption of intercellular signaling pathways that are essential for the initiation and maturation of biofilms; (2) enhanced penetration into the extracellular polymeric substance (EPS) matrix due to their nanoscale size and high surface area, enabling improved drug delivery to deeper biofilm layers; (3) reduction of selective pressure through controlled drug release, thereby limiting the rapid emergence of bacterial resistance; (4) sustained and prolonged release of encapsulated agents, which maintains inhibitory concentrations at the infection site and enhances antimicrobial efficacy; (5) gradual degradation of PLGA into lactic and glycolic acids, leading to a localized decrease in pH that can destabilize the biofilm structure and impair bacterial metabolic activity; (6) targeted delivery of antimicrobial and antibiofilm agents (such as antibiotics, polyphenols, and quorum sensing inhibitors), resulting in interference with cell–cell communication and inhibition of biofilm formation; and (7) the potential for surface functionalization with cationic polymers, such as chitosan, which enhances electrostatic interactions with negatively charged biofilm surfaces, thereby improving adhesion, penetration, and antibacterial activity. In addition, PLGA nanoparticles have been reported to disrupt bacterial membrane integrity, increase cellular permeability, and, when loaded with active compounds, induce oxidative stress, all of which contribute to biofilm eradication. Collectively, these properties highlight PLGA nanoparticles as a versatile and effective platform for targeting bacterial biofilms and improving the efficacy of antimicrobial therapies.46,145 Figure 3 summarizes the fabrication, morphological characterization, cytocompatibility, antibacterial activity, and wound-healing performance of PLGA-based electrospun nanofibrous scaffolds loaded with dual bioactive agents.
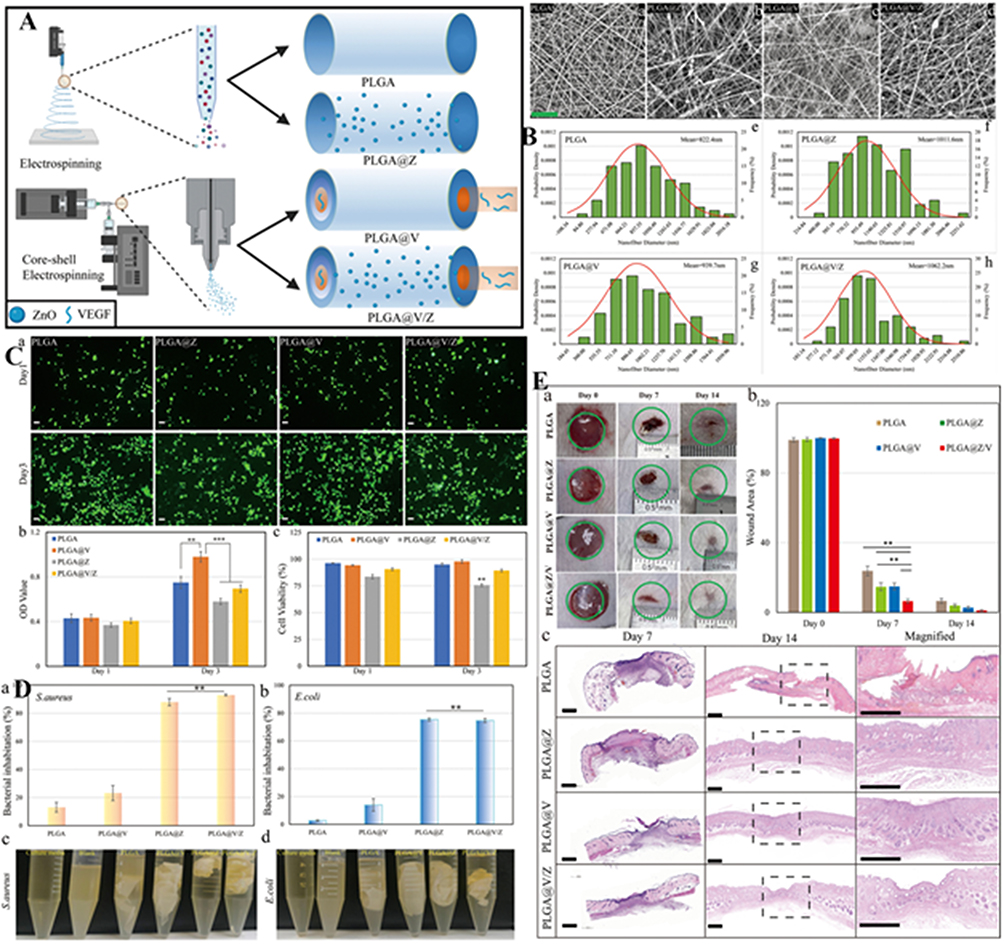 |
Figure 3 PLGA-based electrospun nanofibrous scaffolds incorporating dual bioactive agents as potential wound dressing materials. (A) Schematic representation of the fabrication of PLGA, PLGA@Z by electrospinning, and PLGA@V and PLGA@V/Z by core–shell electrospinning. (B) Morphological characterization of the fabricated membranes: a–d, SEM images of the membranes; e–h, average nanofiber diameter of each membrane. (C) Cytotoxicity evaluation of the different membranes: a, live/dead staining of cells cultured on the membranes; b and c, OD values and cell viability, respectively. (D) Antibacterial activity of the tested groups: a, inhibition against S. aureus; b, inhibition against E. coli; c and d, turbidity measurements for both bacterial strains. (E) Wound contraction assessment: a, representative wound images at different time points; b, wound contraction percentage; c, representative H&E-stained tissue sections collected from the wound bed at different time points. Reprinted from146 with permission from Elsevier Publisher. |
Release Profile of Natural Compounds
In the study by Kizilbey et al,123 rutin-loaded PLGA optimum nanoparticles (NP4) at concentrations of 0.5 and 1 mg/mL were investigated. The release profiles of both nanoparticle samples exhibited similar patterns; however, the numerical release values differed due to the variation in concentration. Initially, an abrupt release was observed after 24 hours. In the first stage, the rapid release reached 30% and 55% for the 1 and 0.5 mg/mL concentrations, respectively. In the second stage, with continued polymer chain degradation and drug diffusion, the release reached 95% for the 0.5 mg/mL NP4 and 47% for the 1 mg/mL NP4. In the final stages (4–14 days), the release percentage remained nearly constant at these levels. The NP4 formulation at 0.5 mg/mL achieved complete release (100%) by day 5 (120 h), whereas the 1 mg/mL formulation reached only 50% release at the same time point. Consistent with previous studies, the cumulative release of rutin was higher at lower nanoparticle concentrations. This can be attributed to the greater interaction of low-concentration nanoparticles with water molecules in PBS, leading to faster water uptake and accelerated degradation. Based on these findings, longer evaluation periods are recommended for higher-concentration nanoparticle formulations.
In the study by Amirthalingam et al,127 analysis of curcumin release from PLGA scaffolds showed that 14% of curcumin was released within the first 12 hours. The release was initially burst-like, with approximately 10% released during the first 5 hours.
In the study by Almukainziet al,128 the release profile of gentiopicroside (GPS) exhibited a biphasic behavior, characterized by an initial burst release after 4 hours followed by a sustained release phase lasting up to 72 hours. Free GPS was released almost immediately (approximately 94% within a short time), indicating an uncontrolled release behavior. These findings highlight two key points: (1) biphasic release behavior, consisting of an initial burst attributed to surface-associated or weakly bound drug followed by a controlled and sustained release from the PLGA matrix; and (2) the free form of GPS lacks controlled release properties.
In the study by Azzazy et al,129 in vitro drug release assays demonstrated a biphasic release profile, with an initial burst release of 82.5% occurring within the first 2 hours, which increased to 87.5% over 72 hours. The sustained release behavior was attributed to the gradual diffusion of encapsulated HARF from the polymeric matrix following erosion and hydrolytic degradation of PLGA. In addition, chitosan coating on the surface of PLGA nanoparticles played a crucial role in prolonging the release profile, thereby enhancing the therapeutic effect of HARF on wound sites through extended interaction with skin cells.
In the study by Li et al,135 curcumin release from PLGA-PCL and PLGA-PCL-TA systems was investigated and divided into three stages:
In the first stage (first two days), a burst release occurred due to incomplete encapsulation of curcumin in the PLGA core caused by instability of the Taylor cone during electrospinning. Surface-associated curcumin was rapidly released, generating an initial burst. In the PLGA-PCL-TA (PPT) system, the tannic acid (TA) coating reduced the release rate. In the second stage (days 2–4), the initially released curcumin gradually diminished. In the PP system, degradation of PCL began, exposing the PLGA core and maintaining a relatively constant release rate. In contrast, the TA coating in PPT limited interaction with the environment, slowing down curcumin diffusion. In the third stage (after day 4), a stable and slow-release phase was observed. In PP, remaining PCL had minimal encapsulating effect, leading to freer diffusion from PLGA. However, in PPT, the multilayer structure further slowed degradation, ensuring continued controlled release. Overall, the multilayer PPT system provided a more stable, slower, and long-term release profile suitable for chronic wound healing applications.
In the study by Kumari et al,137 PLGA nanoparticles loaded with curcumin were synthesized using four different plant extracts as surfactants (stabilizers). The results indicated that curcumin release was strongly dependent on the type of surfactant used. Among all formulations, only curc@CSF-PLGA nanoparticles exhibited a desirable release profile, with approximately 10% of curcumin released within the first 0–0.5 hours and about 45% released within 8 hours.
Collectively, these studies demonstrate that natural compound-loaded PLGA-based delivery systems consistently exhibit predominantly biphasic release behavior, characterized by an initial burst release followed by a sustained release phase. The burst phase is generally attributed to surface-associated drug molecules or incomplete encapsulation, while the sustained phase is governed by diffusion through and degradation of the PLGA matrix. Across different systems, including curcumin, gentiopicroside, and HARF, the release kinetics are strongly influenced by formulation parameters, such as polymer composition (PLGA, PCL), surface coatings (chitosan, tannic acid), and external stabilizers (plant extracts). For example, hydrophilic coatings (eg, chitosan) and multilayer architectures significantly prolong drug release, whereas unmodified systems or free drugs exhibit rapid and uncontrolled release. Importantly, multilayer and composite systems (eg, PLGA-PCL-TA) provide more controlled, prolonged, and therapeutically relevant release profiles, making them particularly suitable for long-term applications such as wound healing, where sequential phases of antimicrobial activity and tissue regeneration are required.
Conclusion
Infected wounds remain a significant clinical challenge due to persistent microbial colonization, biofilm formation, and impaired tissue regeneration. PLGA has emerged as a promising FDA-approved biodegradable carrier for natural compounds, enabling controlled and sustained release with demonstrated antimicrobial, anti-biofilm, antioxidant, and anti-inflammatory effects. Preclinical evidence indicates that PLGA–natural compound systems can accelerate wound healing by promoting angiogenesis, collagen deposition, and re-epithelialization, highlighting their dual role in infection control and tissue regeneration.
However, most studies are still confined to in vitro and in vivo models, with limited clinical translation. Key limitations include variability in formulation parameters, burst release behavior, lack of standardized fabrication protocols, and insufficient replication of the complex polymicrobial and hypoxic wound microenvironment. In addition, challenges related to large-scale production, long-term safety, and regulatory approval remain unresolved. Further studies are required to confirm the antibiofilm and therapeutic properties of PLGA for its further clinical development. In addition, the application of advanced statistical methods could significantly contribute to the optimization of synthesized nanoparticle formulations.
Overall, PLGA-based delivery of natural compounds represents a promising strategy for infected wound management, but future progress depends on standardized formulation approaches, clinically relevant biofilm models, and scalable translational frameworks to bridge the gap between laboratory research and clinical application.
Acknowledgments
The authors of this paper would like to express their gratitude to Hamadan University of Medical Sciences.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this study.
References
1. Chua AWC, Khoo YC, Tan BK, Tan KC, Foo CL, Chong SJ. Skin tissue engineering advances in severe burns: review and therapeutic applications. Burns Trauma. 2016;4. doi:10.1186/s41038-016-0027-y
2. Taati Moghadam M, Khoshbayan A, Chegini Z, Farahani I, Shariati A. Bacteriophages, a new therapeutic solution for inhibiting multidrug-resistant bacteria causing wound infection: lesson from animal models and clinical trials. Drug Des Devel Ther. 2020;Volume 14:1867–26. doi:10.2147/DDDT.S251171
3. Simões D, Miguel SP, Ribeiro MP, Coutinho P, Mendonça AG, Correia IJ. Recent advances on antimicrobial wound dressing: a review. Eur J Pharm Biopharm. 2018;127:130–141. doi:10.1016/j.ejpb.2018.02.022
4. Bowler P, Duerden B, Armstrong DG. Wound microbiology and associated approaches to wound management. Clin Microbiol Rev. 2001;14(2):244–269. doi:10.1128/CMR.14.2.244-269.2001
5. Saghazadeh S, Rinoldi C, Schot M, et al. Drug delivery systems and materials for wound healing applications. Adv Drug Delivery Rev. 2018;127:138–166. doi:10.1016/j.addr.2018.04.008
6. Sarheed O, Ahmed A, Shouqair D, Boateng J. Antimicrobial Dressings for Improving Wound Healing. Wound Healing-New Insights into Ancient Challenges. 2016;374–398.
7. Karaiskos I, Giamarellou H. Multidrug-resistant and extensively drug-resistant Gram-negative pathogens: current and emerging therapeutic approaches. Expert Opinion Pharmacother. 2014;15(10):1351–1370. doi:10.1517/14656566.2014.914172
8. Shafiq M, Huang J, Ur Rahman S, et al. High incidence of multidrug-resistant Escherichia coli coharboring mcr-1 and bla CTX-M-15 recovered from pigs. Infect Drug Resist. 2019;Volume 12:2135–2149. doi:10.2147/IDR.S209473
9. Abat C, Fournier P-E, Jimeno M-T, Rolain J-M, Raoult D. Extremely and pandrug-resistant bacteria extra-deaths: myth or reality? Eur J Clin Microbiol Infect Dis. 2018;37(9):1687–1697. doi:10.1007/s10096-018-3300-0
10. Kwiatek M, Parasion S, Nakonieczna A. Therapeutic bacteriophages as a rescue treatment for drug‐resistant infections–an in vivo studies overview. J Appl Microbiol. 2020;128(4):985–1002. doi:10.1111/jam.14535
11. Kutter E, Kuhl S, Alavidze Z, Blasdel B. Phage therapy: Bacteriophages as Natural, Self-Limiting Antibiotics. Textbook of Natural Medicine. 2005;112:945–956.
12. Cooper R, Kirketerp-Møller K. Non-antibiotic antimicrobial interventions and antimicrobial stewardship in wound care. J Wound Care. 2018;27(6):355–377. doi:10.12968/jowc.2018.27.6.355
13. Tsiouris CG, Kelesi M, Vasilopoulos G, Kalemikerakis I, Papageorgiou EG. The efficacy of probiotics as pharmacological treatment of cutaneous wounds: meta-analysis of animal studies. Eur J Pharm Sci. 2017;104:230–239. doi:10.1016/j.ejps.2017.04.002
14. Uberoi A, McCready-Vangi A, Grice EA. The wound microbiota: microbial mechanisms of impaired wound healing and infection. Nat Rev Microbiol. 2024;22(8):507–521. doi:10.1038/s41579-024-01035-z
15. Singh R, Sahore S, Kaur P, Rani A, Ray P. Penetration barrier contributes to bacterial biofilm-associated resistance against only select antibiotics, and exhibits genus-, strain-and antibiotic-specific differences. FEMS Pathogens Dis. 2016;74(6):ftw056. doi:10.1093/femspd/ftw056
16. Rajendran NK, Kumar SSD, Houreld NN, Abrahamse H. A review on nanoparticle based treatment for wound healing. J Drug Delivery Sci Technol. 2018;44:421–430. doi:10.1016/j.jddst.2018.01.009
17. Negut I, Grumezescu V, Grumezescu AM. Treatment strategies for infected wounds. Molecules. 2018;23(9):2392. doi:10.3390/molecules23092392
18. De Soricellis C, Laigle C, Spinelli L, et al. Lipidized LL37-loaded PLGA nanocarriers: bioengineered peptide delivery systems for enhanced wound healing. Int J Pharm. 2025;677:125668. doi:10.1016/j.ijpharm.2025.125668
19. Singhal M, Seaton CC, Surtees A, Katsikogianni MG. Formulation, characterisation, and biocompatibility assessment of rifampicin-loaded poly (d, l-lactide-co-glycolide) composites for local treatment of orthopaedic and wound infections. Pharmaceutics. 2024;16(11):1467. doi:10.3390/pharmaceutics16111467
20. Loureiro JA, Pereira MC. PLGA based drug carrier and pharmaceutical applications: the most recent advances. Pharmaceutics. 2020;12:903.
21. Huang K, Jinzhong Z, Zhu T, et al. Exploration of the antibacterial and wound healing potential of a PLGA/silk fibroin based electrospun membrane loaded with zinc oxide nanoparticles. J Mat Chem B. 2021;9(5):1452–1465. doi:10.1039/D0TB02822C
22. Rancan F, Jurisch J, Günday C, et al. Screening of surfactants for improved delivery of antimicrobials and poly-lactic-co-glycolic acid particles in wound tissue. Pharmaceutics. 2021;13(7):1093. doi:10.3390/pharmaceutics13071093
23. Martins C, Sousa F, Araújo F, Sarmento B. Functionalizing PLGA and PLGA derivatives for drug delivery and tissue regeneration applications. Adv Healthcare Mater. 2018;7(1):1701035. doi:10.1002/adhm.201701035
24. Shakya AK, Al-Sulaibi M, Naik RR, Nsairat H, Suboh S, Abulaila A. Review on PLGA polymer based nanoparticles with antimicrobial properties and their application in various medical conditions or infections. Polymers. 2023;15(17):3597. doi:10.3390/polym15173597
25. Tamilarasi GP, Krishnan M, Sabarees G, Gouthaman S, Alagarsamy V, Solomon VR. Emerging trends in curcumin embedded electrospun nanofibers for impaired diabetic wound healing. Appl Nano. 2022;3(4):202–232. doi:10.3390/applnano3040015
26. Lv Y, Li W, Liao W, et al. Nano-drug delivery systems based on natural products. Int J Nanomed. 2024;Volume 19:541–569. doi:10.2147/IJN.S443692
27. Tottoli EM, Dorati R, Genta I, Chiesa E, Pisani S, Conti B. Skin wound healing process and new emerging technologies for skin wound care and regeneration. Pharmaceutics. 2020;12(8):735. doi:10.3390/pharmaceutics12080735
28. Hubner A, Sobreira F, Vetore Neto A, et al. The synergistic behavior of antioxidant phenolic compounds obtained from winemaking waste’s valorization, increased the efficacy of a sunscreen system. Antioxidants. 2019;8(11):530. doi:10.3390/antiox8110530
29. Kant V, Gopal A, Kumar D, et al. Curcumin-induced angiogenesis hastens wound healing in diabetic rats. J Surg Res. 2015;193(2):978–988. doi:10.1016/j.jss.2014.10.019
30. Ding D, Zhu Q. Recent advances of PLGA micro/nanoparticles for the delivery of biomacromolecular therapeutics. Mater Sci Eng C. 2018;92:1041–1060. doi:10.1016/j.msec.2017.12.036
31. Shariati A, Chegini Z, Ghaznavi-Rad E, Zare EN, Hosseini SM. PLGA-based nanoplatforms in drug delivery for inhibition and destruction of microbial biofilm. Front Cell Infect Microbiol. 2022;12:926363. doi:10.3389/fcimb.2022.926363
32. Hosseini SM, Taheri M, Nouri F, Farmani A, Moez NM, Arabestani MR. Nano drug delivery in intracellular bacterial infection treatments. Biomed Pharmacother. 2022;146:112609. doi:10.1016/j.biopha.2021.112609
33. Patra JK, Das G, Fraceto LF, et al. Nano based drug delivery systems: recent developments and future prospects. J Nanobiotechnol. 2018;16(1):71. doi:10.1186/s12951-018-0392-8
34. Wang B, Kostarelos K, Nelson BJ, Zhang L. Trends in micro‐/nanorobotics: materials development, actuation, localization, and system integration for biomedical applications. Adv Mater. 2021;33(4):2002047. doi:10.1002/adma.202002047
35. Nasrollahzadeh M, Sajadi SM, Sajjadi M, Issaabadi Z. An introduction to nanotechnology. In: Interface Science and Technology. Elsevier; 2019:1–27.
36. Hosseini SM, Abbasalipourkabir R, Jalilian FA, et al. Doxycycline-encapsulated solid lipid nanoparticles as promising tool against Brucella melitensis enclosed in macrophage: a pharmacodynamics study on J774A. 1 cell line. Antimicrob Resist Infect Control. 2019;8(1):62. doi:10.1186/s13756-019-0504-8
37. Singh AP, Biswas A, Shukla A, Maiti P. Targeted therapy in chronic diseases using nanomaterial-based drug delivery vehicles. Signal Transduction Targeted Ther. 2019;4(1):33. doi:10.1038/s41392-019-0068-3
38. Alphandéry E. Nano-therapies for glioblastoma treatment. Cancers. 2020;12(1):242. doi:10.3390/cancers12010242
39. Putnam D. Polymers for gene delivery across length scales. Nature Mater. 2006;5(6):439–451. doi:10.1038/nmat1645
40. Swider E, Koshkina O, Tel J, Cruz LJ, de Vries IJM, Srinivas M. Customizing poly (lactic-co-glycolic acid) particles for biomedical applications. Acta Biomater. 2018;73:38–51. doi:10.1016/j.actbio.2018.04.006
41. Dinarvand R, n S, Manoochehri S, Rouhani H, Atyabi F. Polylactide-co-glycolide nanoparticles for controlled delivery of anticancer agents. Int J Nanomed. 2011;877–895. doi:10.2147/IJN.S18905
42. Danhier F, Ansorena E, Silva JM, Coco R, Le Breton A, Préat V. PLGA-based nanoparticles: an overview of biomedical applications. J Control Release. 2012;161(2):505–522. doi:10.1016/j.jconrel.2012.01.043
43. Gentile P, Chiono V, Carmagnola I, Hatton PV. An overview of poly (lactic-co-glycolic) acid (PLGA)-based biomaterials for bone tissue engineering. Int J Mol Sci. 2014;15(3):3640–3659. doi:10.3390/ijms15033640
44. Pavurala N, Achenie LE. Identifying polymer structures for oral drug delivery–A molecular design approach. Comput Chem Eng. 2014;71:734–744. doi:10.1016/j.compchemeng.2014.07.015
45. Lü J-M, Wang X, Marin-Muller C, et al. Current advances in research and clinical applications of PLGA-based nanotechnology. Expert Rev Mol Diagn. 2009;9(4):325–341. doi:10.1586/erm.09.15
46. Makadia HK, Siegel SJ. Poly lactic-co-glycolic acid (PLGA) as biodegradable controlled drug delivery carrier. Polymers. 2011;3(3):1377–1397. doi:10.3390/polym3031377
47. Samavedi S, Poindexter LK, Van Dyke M, Goldstein AS. Synthetic biomaterials for regenerative medicine applications. In: Regenerative Medicine Applications in Organ Transplantation. Elsevier; 2014:81–99.
48. Salmaso S, Caliceti P. Stealth properties to improve therapeutic efficacy of drug nanocarriers. J Drug Delivery. 2013;2013(1):374252. doi:10.1155/2013/374252
49. Jain AK, Das M, Swarnakar NK, Jain S. Engineered PLGA nanoparticles: an emerging delivery tool in cancer therapeutics. Crit Rev Therapeut Drug Carrier Syst. 2011;28(1):1–45. doi:10.1615/critrevtherdrugcarriersyst.v28.i1.10
50. Ghitman J, Biru EI, Stan R, Iovu H. Review of hybrid PLGA nanoparticles: future of smart drug delivery and theranostics medicine. Mater Des. 2020;193:108805. doi:10.1016/j.matdes.2020.108805
51. Yang J, Zeng H, Luo Y, et al. Recent applications of PLGA in drug delivery systems. Polymers. 2024;16(18):2606. doi:10.3390/polym16182606
52. Samir A, Ashour FH, Hakim AA, Bassyouni M. Recent advances in biodegradable polymers for sustainable applications. NPJ Mater Degrad. 2022;6(1):68. doi:10.1038/s41529-022-00277-7
53. Giram PS, Wang JT-W, Walters AA, et al. Green synthesis of methoxy-poly (ethylene glycol)-block-poly (L-lactide-co-glycolide) copolymer using zinc proline as a biocompatible initiator for irinotecan delivery to colon cancer in vivo. Biomater Sci. 2021;9(3):795–806. doi:10.1039/D0BM01421D
54. Musyanovych A, Schmitz‐Wienke J, Mailänder V, Walther P, Landfester K. Preparation of biodegradable polymer nanoparticles by miniemulsion technique and their cell interactions. Macromol Biosci. 2008;8(2):127–139. doi:10.1002/mabi.200700241
55. Jain RA. The manufacturing techniques of various drug loaded biodegradable poly (lactide-co-glycolide)(PLGA) devices. Biomaterials. 2000;21(23):2475–2490. doi:10.1016/S0142-9612(00)00115-0
56. Xie H, Smith JW. Fabrication of PLGA nanoparticles with a fluidic nanoprecipitation system. J Nanobiotechnol. 2010;8(1):18. doi:10.1186/1477-3155-8-18
57. Govender T, Stolnik S, Garnett MC, Illum L, Davis SS. PLGA nanoparticles prepared by nanoprecipitation: drug loading and release studies of a water soluble drug. J Control Release. 1999;57(2):171–185. doi:10.1016/S0168-3659(98)00116-3
58. Choi J-S, Cao J, Naeem M, et al. Size-controlled biodegradable nanoparticles: preparation and size-dependent cellular uptake and tumor cell growth inhibition. Colloids Surf B. 2014;122:545–551. doi:10.1016/j.colsurfb.2014.07.030
59. Lalani J, Patil S, Kolate A, Lalani R, Misra A. Protein-functionalized PLGA nanoparticles of lamotrigine for neuropathic pain management. AAPS Pharm Sci Tech. 2015;16(2):413–427. doi:10.1208/s12249-014-0235-3
60. Wan F, Maltesen MJ, Andersen SK, et al. One-step production of protein-loaded PLGA microparticles via spray drying using 3-fluid nozzle. Pharm Res. 2014;31(8):1967. doi:10.1007/s11095-014-1299-1
61. Guo X, Zhang X, Ye L, et al. Inhalable microspheres embedding chitosan-coated PLGA nanoparticles for 2-methoxyestradiol. J Drug Targeting. 2014;22(5):421–427. doi:10.3109/1061186X.2013.878944
62. Hao Z. Preparation of PLGA ceftiofur hydrochlorate lungtargeted microsphere with spray drying process. J Wuhan Univ TechnolMater Sci Ed. 2013;28(6):1242–1245. doi:10.1007/s11595-013-0853-8
63. Takada S, Uda Y, Toguchi H, Ogawa Y. Application of a spray drying technique in the production of TRH-containing injectable sustained-release microparticles of biodegradable polymers. PDA J Pharmaceut Sci Technol. 1995;49(4):180–184.
64. Nagavarma B, Yadav HK, Ayaz A, Vasudha L, Shivakumar H. Different techniques for preparation of polymeric nanoparticles-a review. Asian J Pharm Clin Res. 2012;5(3):16–23.
65. Mahesh K, Vaidya S. Microfluidics: a boon for biological research. Current Sci. 2017;112:2021–2028. doi:10.18520/cs/v112/i10/2021-2028
66. Duncanson WJ, Lin T, Abate AR, Seiffert S, Shah RK, Weitz DA. Microfluidic synthesis of advanced microparticles for encapsulation and controlled release. Lab Chip. 2012;12(12):2135–2145. doi:10.1039/c2lc21164e
67. Karnik R, Gu F, Basto P, et al. Microfluidic platform for controlled synthesis of polymeric nanoparticles. Nano Lett. 2008;8(9):2906–2912. doi:10.1021/nl801736q
68. Vladisavljević GT, Williams RA. Recent developments in manufacturing emulsions and particulate products using membranes. Adv Colloid Interface Sci. 2005;113(1):1–20. doi:10.1016/j.cis.2004.10.002
69. Perry JL, Herlihy KP, Napier ME, DeSimone JM. PRINT: a novel platform toward shape and size specific nanoparticle theranostics. Acc Chem Res. 2011;44(10):990–998. doi:10.1021/ar2000315
70. Liang Y, He J, Guo B. Functional hydrogels as wound dressing to enhance wound healing. ACS Nano. 2021;15(8):12687–12722. doi:10.1021/acsnano.1c04206
71. Almadani YH, Vorstenbosch J, Davison PG, Murphy AM, editors. Wound healing: a comprehensive review. In: Seminars in Plastic Surgery. Thieme Medical Publishers, Inc; 2021.
72. Sun BK, Siprashvili Z, Khavari PA. Advances in skin grafting and treatment of cutaneous wounds. Science. 2014;346(6212):941–945. doi:10.1126/science.1253836
73. Qi X, Li Y, Xiang Y, et al. Hyperthermia-enhanced immunoregulation hydrogel for oxygenation and ROS neutralization in diabetic foot ulcers. Cell Biomat. 2025;1(3):100020. doi:10.1016/j.celbio.2025.100020
74. Xiang Y, Zhuge P, Qi X, et al. A cuttlefish ink nanoparticle-reinforced biopolymer hydrogel with robust adhesive and immunomodulatory features for treating oral ulcers in diabetes. Bioact Mater. 2024;39:562–581. doi:10.1016/j.bioactmat.2024.04.022
75. Criollo-Mendoza MS, Contreras-Angulo LA, Leyva-López N, Gutiérrez-Grijalva EP, Jiménez-Ortega LA, Heredia JB. Wound healing properties of natural products: mechanisms of action. Molecules. 2023;28(2):598. doi:10.3390/molecules28020598
76. Trinh X-T, Long N-V, Van Anh LT, et al. A comprehensive review of natural compounds for wound healing: targeting bioactivity perspective. Int J Mol Sci. 2022;23(17):9573. doi:10.3390/ijms23179573
77. Kondo T, Ishida Y. Molecular pathology of wound healing. Forensic Sci Int. 2010;203(1–3):93–98. doi:10.1016/j.forsciint.2010.07.004
78. Sorg H, Tilkorn DJ, Hager S, Hauser J, Mirastschijski U. Skin wound healing: an update on the current knowledge and concepts. Eur Surg Res. 2017;58(1–2):81–94. doi:10.1159/000454919
79. Barman PK, Koh TJ. Macrophage dysregulation and impaired skin wound healing in diabetes. Front Cell Develop Biol. 2020;8:528. doi:10.3389/fcell.2020.00528
80. Ibrahim NI, Wong SK, Mohamed IN, et al. Wound healing properties of selected natural products. Int J Environ Res Public Health. 2018;15(11):2360. doi:10.3390/ijerph15112360
81. Sinno H, Prakash S. Complements and the wound healing cascade: an updated review. Plastic Surg Int. 2013;2013(1):146764. doi:10.1155/2013/146764
82. Martin JM, Zenilman JM, Lazarus GS. Molecular microbiology: new dimensions for cutaneous biology and wound healing. J Invest Dermatol. 2010;130(1):38–48. doi:10.1038/jid.2009.221
83. Ramzan M, Rafiq A, Wahab A, et al. Natural products loaded with nanoparticles for wound healing. Complement Altern Med. 2024;2024:132–140
84. Deufert D, Graml R. Disease-specific, health-related quality of life (HRQoL) of people with chronic wounds—A descriptive cross-sectional study using the Wound-QoL. Wound Med. 2017;16:29–33. doi:10.1016/j.wndm.2017.01.006
85. Shedoeva A, Leavesley D, Upton Z, Fan C. Wound healing and the use of medicinal plants. Evidence-Based Complem Alternative Med. 2019;2019(1):2684108. doi:10.1155/2019/2684108
86. Clinton A, Carter T. Chronic wound biofilms: pathogenesis and potential therapies. Lab Med. 2015;46(4):277–284. doi:10.1309/LMBNSWKUI4JPN7SO
87. Wu Y-K, Cheng N-C, Cheng C-M. Biofilms in chronic wounds: pathogenesis and diagnosis. Trends Biotechnol. 2019;37(5):505–517. doi:10.1016/j.tibtech.2018.10.011
88. Bjarnsholt T. The role of bacterial biofilms in chronic infections. Apmis. 2013;121:1–58. doi:10.1111/apm.12099
89. Zogaj X, Nimtz M, Rohde M, Bokranz W, Römling U. The multicellular morphotypes of Salmonella typhimurium and Escherichia coli produce cellulose as the second component of the extracellular matrix. Mol Microbiol. 2001;39(6):1452–1463. doi:10.1046/j.1365-2958.2001.02337.x
90. Prabhakara R, Harro JM, Leid JG, Harris M, Shirtliff ME. Murine immune response to a chronic Staphylococcus aureus biofilm infection. Infect Immun. 2011;79(4):1789–1796. doi:10.1128/IAI.01386-10
91. Kalliolias GD, Ivashkiv LB. TNF biology, pathogenic mechanisms and emerging therapeutic strategies. Nat Rev Rheumatol. 2016;12(1):49–62. doi:10.1038/nrrheum.2015.169
92. Liu Y, Long S, Wang H, Wang Y. Biofilm therapy for chronic wounds. Int Wound J. 2024;21(2):e14667. doi:10.1111/iwj.14667
93. Hall-Stoodley L, Stoodley P, Kathju S, et al. Towards diagnostic guidelines for biofilm-associated infections. FEMS Immunol Med Microbiol. 2012;65(2):127–145. doi:10.1111/j.1574-695X.2012.00968.x
94. Høiby N, Bjarnsholt T, Moser C, et al. ESCMID guideline for the diagnosis and treatment of biofilm infections 2014. Clin Microbiol Infect. 2015;21:S1–S25. doi:10.1016/j.cmi.2014.10.024
95. Bjarnsholt T, Alhede M, Alhede M, et al. The in vivo biofilm. Trends Microbiol. 2013;21(9):466–474. doi:10.1016/j.tim.2013.06.002
96. Gámez-Herrera E, García-Salinas S, Salido S, et al. Drug-eluting wound dressings having sustained release of antimicrobial compounds. Eur J Pharm Biopharm. 2020;152:327–339. doi:10.1016/j.ejpb.2020.05.025
97. Thomas N, Thorn C, Richter K, Thierry B, Prestidge C. Efficacy of poly-lactic-co-glycolic acid micro-and nanoparticles of ciprofloxacin against bacterial biofilms. J Pharmaceut Sci. 2016;105(10):3115–3122. doi:10.1016/j.xphs.2016.06.022
98. Baek J-S, Tan CH, NKJ N, Yeo YP, Rice SA, Loo SCJ. A programmable lipid-polymer hybrid nanoparticle system for localized, sustained antibiotic delivery to Gram-positive and Gram-negative bacterial biofilms. Nanoscale Horiz. 2018;3(3):305–311. doi:10.1039/C7NH00167C
99. Melguizo-Rodríguez L, de Luna-Bertos E, Ramos-Torrecillas J, Illescas-Montesa R, Costela-Ruiz VJ, García-Martínez O. Potential effects of phenolic compounds that can be found in olive oil on wound healing. Foods. 2021;10(7):1642. doi:10.3390/foods10071642
100. Xiao J, Chen S, Chen Y, Su J. The potential health benefits of aloin from genus Aloe. Phytother Res. 2022;36(2):873–890. doi:10.1002/ptr.7371
101. Maan AA, Nazir A, Khan MKI, et al. The therapeutic properties and applications of Aloe vera: a review. J Herbal Med. 2018;12:1–10. doi:10.1016/j.hermed.2018.01.002
102. Kim M, Park JH. Isolation of aloe saponaria-derived extracellular vesicles and investigation of their potential for chronic wound healing. Pharmaceutics. 2022;14(9):1905. doi:10.3390/pharmaceutics14091905
103. Omer HH, Demirtas I, Ozen T. Investigation of phenolic contents and bioactivities of water-based extracts prepared from cryogenically pulverized Turkish propolis. J Food Measure Charact. 2023;17(2):1586–1601. doi:10.1007/s11694-022-01716-4
104. Ding Q, Sheikh AR, Gu X, et al. Chinese Propolis: ultrasound‐assisted enhanced ethanolic extraction, volatile components analysis, antioxidant and antibacterial activity comparison. Food Sci Nutr. 2021;9(1):313–330. doi:10.1002/fsn3.1997
105. El-Guendouz S, Al-Waili N, Aazza S, et al. Antioxidant and diuretic activity of co-administration of Capparis spinosa honey and propolis in comparison to furosemide. Asian Pac J Trop Med. 2017;10(10):974–980. doi:10.1016/j.apjtm.2017.09.009
106. Campoccia D, Ravaioli S, Santi S, et al. Exploring the anticancer effects of standardized extracts of poplar-type propolis: in vitro cytotoxicity toward cancer and normal cell lines. Biomed Pharmacother. 2021;141:111895. doi:10.1016/j.biopha.2021.111895
107. Yen C-H, Chiu H-F, Wu C-H, et al. Beneficial efficacy of various propolis extracts and their digestive products by in vitro simulated gastrointestinal digestion. Lwt. 2017;84:281–289. doi:10.1016/j.lwt.2017.05.074
108. Necip A, Demirtas I, Tayhan SE, et al. Isolation of phenolic compounds from eco‐friendly white bee propolis: antioxidant, wound‐healing, and anti‐Alzheimer effects. Food Sci Nutr. 2024;12(3):1928–1939. doi:10.1002/fsn3.3888
109. Salehi B, Rodrigues CF, Peron G, et al. Curcumin nanoformulations for antimicrobial and wound healing purposes. Phytother Res. 2021;35(5):2487–2499. doi:10.1002/ptr.6976
110. Farhat F, Sohail SS, Siddiqui F, Irshad RR, Madsen DØ. Curcumin in wound healing—a bibliometric analysis. Life. 2023;13(1):143. doi:10.3390/life13010143
111. Comino-Sanz IM, López-Franco MD, Castro B, Pancorbo-Hidalgo PL. The role of antioxidants on wound healing: a review of the current evidence. J Clin Med. 2021;10(16):3558. doi:10.3390/jcm10163558
112. Doersch KM, Newell-Rogers MK. The impact of quercetin on wound healing relates to changes in αV and β1 integrin expression. Exp Biol Med. 2017;242(14):1424–1431. doi:10.1177/1535370217712961
113. Fu J, Huang J, Lin M, Xie T, You T. Quercetin promotes diabetic wound healing via switching macrophages from M1 to M2 polarization. J Surg Res. 2020;246:213–223. doi:10.1016/j.jss.2019.09.011
114. Chittasupho C, Manthaisong A, Okonogi S, Tadtong S, Samee W. Effects of quercetin and curcumin combination on antibacterial, antioxidant, in vitro wound healing and migration of human dermal fibroblast cells. Int J Mol Sci. 2021;23(1):142. doi:10.3390/ijms23010142
115. Kapare HS, Giram PS, Raut SS, Gaikwad HK, Paiva-Santos AC. Formulation development and evaluation of Indian propolis hydrogel for wound healing. Gels. 2023;9(5):375. doi:10.3390/gels9050375
116. Seyed Ahmadi SG, Farahpour MR, Hamishehkar H. Topical application of Cinnamon verum essential oil accelerates infected wound healing process by increasing tissue antioxidant capacity and keratin biosynthesis. Kaohsiung J Med Sci. 2019;35(11):686–694. doi:10.1002/kjm2.12120
117. Khurshid S, Farwa U, Mazhar Z, Naeem H, Ishaq Y. Evaluation of aloe vera gel combined with cinnamon oil with antibacterial activity for wound healing application. Int J Lower Extremity Wounds. 2024;15347346241259102. doi:10.1177/15347346241259102
118. Alhazmi A, Aldairi AF, Alghamdi A, et al. Antibacterial effects of Commiphora gileadensis methanolic extract on wound healing. Molecules. 2022;27(10):3320. doi:10.3390/molecules27103320
119. Yen YH, Pu CM, Liu CW, et al. Curcumin accelerates cutaneous wound healing via multiple biological actions: the involvement of TNF‐α, MMP‐9, α‐SMA, and collagen. Int Wound J. 2018;15(4):605–617. doi:10.1111/iwj.12904
120. Shahbandeh M, Salehi MA, Soltanyzadeh M, et al. Evaluation of the antibacterial and wound healing properties of a burn ointment containing curcumin, honey, and potassium aluminium. Compar Immunol Microbiol Infect Dis. 2022. 81. arXiv preprint arXiv:221111939. doi:10.1016/j.cimid.2022.101747
121. Hozzein WN, Badr G, Al Ghamdi AA, Sayed A, Al-Waili NS, Garraud O. Topical application of propolis enhances cutaneous wound healing by promoting TGF-beta/Smad-mediated collagen production in a streptozotocin-induced type I diabetic mouse model. Cell Physiol Biochem. 2015;37(3):940–954. doi:10.1159/000430221
122. MJ A, Al-Ahbabi HH, Alhussani R, Hamad A. Study of the efficacy of aloe vera extracts in treatment of non-infected wounds induced by sulferric acid and infected wounds with Staphylococcus aureus. Int J. 2015;3(1):593–601.
123. Kızılbey K. Optimization of rutin-loaded PLGA nanoparticles synthesized by single-emulsion solvent evaporation method. Acs Omega. 2019;4(1):555–562. doi:10.1021/acsomega.8b02767
124. Alam J, Dilnawaz F, Sahoo SK, et al. Curcumin encapsulated into biocompatible co-polymer PLGA nanoparticle enhanced anti-gastric cancer and anti-Helicobacter Pylori effect. Asian Pac J Cancer Prev. 2022;23(1):61. doi:10.31557/APJCP.2022.23.1.61
125. Leung MH, Shen AQ. Microfluidic assisted nanoprecipitation of PLGA nanoparticles for curcumin delivery to leukemia jurkat cells. Langmuir. 2018;34(13):3961–3970. doi:10.1021/acs.langmuir.7b04335
126. Roshan Z, Haddadi‐Asl V, Ahmadi H, Moussaei M. Curcumin‐encapsulated poly (lactic‐co‐glycolic acid) nanoparticles: a comparison of drug release kinetics from particles prepared via electrospray and nanoprecipitation. Macromol Mater Eng. 2024;309(7):2400040. doi:10.1002/mame.202400040
127. Amirthalingam M, Kasinathan N, Amuthan A, Mutalik S, Sreenivasa Reddy M, Nayanabhirama U. Bioactive PLGA–curcumin microparticle-embedded chitosan scaffold: in vitro and in vivo evaluation. Artif Cells Nanomed Biotechnol. 2017;45(2):233–241. doi:10.3109/21691401.2016.1146727
128. Almukainzi M, A El-Masry T, A Negm W, et al. Gentiopicroside PLGA nanospheres: fabrication, in vitro characterization, antimicrobial action, and in vivo effect for enhancing wound healing in diabetic rats. Int J Nanomed. 2022;Volume 17:1203–1225. doi:10.2147/IJN.S358606
129. HME-S A, Fahmy SA, Mahdy NK, Meselhy MR, Bakowsky U. Chitosan-coated PLGA nanoparticles loaded with peganum harmala alkaloids with promising antibacterial and wound healing activities. Nanomaterials. 2021;11(9):2438. doi:10.3390/nano11092438
130. Abdelazim EB, Abed T, Goher SS, et al. In vitro and in vivo studies of Syzygium cumini-loaded electrospun PLGA/PMMA/collagen nanofibers for accelerating topical wound healing. RSC Adv. 2024;14(1):101–117. doi:10.1039/D3RA06355K
131. Geyik F, Kaya S, Yılmaz DE, et al. Propolis-loaded poly (lactic-co-glycolic acid) nanofibers: an in vitro study. ACS Omega. 2024;9(12):14054–14062. doi:10.1021/acsomega.3c09492
132. Ndlovu SP, Motaung KSM, Adeyemi SA, et al. Sodium alginate-based nanofibers loaded with Capparis sepiaria plant extract for wound healing. J Biomater Sci Poly Ed. 2024;35(15):2380–2401. doi:10.1080/09205063.2024.2381375
133. Reinbold J, Uhde AK, Müller I, et al. Preventing surgical site infections using a natural, biodegradable, antibacterial coating on surgical sutures. Molecules. 2017;22(9):1570. doi:10.3390/molecules22091570
134. Diao Z, Long J, Feng Y, et al. Dual ROS/pH-responsive mangiferin-loaded smart microneedles for precision therapy of wound infections. Mater Today Bio. 2025;35:102339. doi:10.1016/j.mtbio.2025.102339
135. Li Z, Guo Q, Chen R, et al. Tannic acid coated core-shell fibers with antibacterial and antioxidant properties for diabetic wound healing. Mater Des. 2025;253:113874. doi:10.1016/j.matdes.2025.113874
136. Kandaswamy K, Panda SP, Subramanian R, et al. Synergistic berberine chloride and Curcumin-Loaded nanofiber therapies against Methicillin-Resistant Staphylococcus aureus Infection: augmented immune and inflammatory responses in zebrafish wound healing. Int Immunopharmacol. 2024;140:112856. doi:10.1016/j.intimp.2024.112856
137. Kumari A, Guliani A, Shukla AK, Kumar S, Acharya A. Green surfactant based synthesis of curcumin loaded poly lactic-co-glycolic acid nanoparticles with enhanced solubility, photo-stability and anti-biofilm activity. J Drug Delivery Sci Technol. 2020;59:101884. doi:10.1016/j.jddst.2020.101884
138. Xu F, Zhang J, Wang H, Jiang L. Facile fabrication of catechin-loaded PLGA/chitosan nanofibers for effective nursing care of wound-infecting bacterial pathogens and healing. J Mater Res. 2025;40:1–15.
139. Ran R, Peng Y, Xiao L, et al. Fabrication of antimicrobial poly (lactic‐co‐glycolic acid)/silk fibroin/aloe anthraquinone fibrous membranes for potential application of wound healing. J Appl Polym Sci. 2022;139(25):e52394. doi:10.1002/app.52394
140. Chen X, Liu J, Lu Y, et al. A PLGA/silk fibroin nanofibre membrane loaded with natural flavonoid compounds extracted from green cocoons for wound healing. Int J Mol Sci. 2024;25(17):9263. doi:10.3390/ijms25179263
141. Sun M, Zhu C, Long J, Lu C, Pan X, Wu C. PLGA microsphere-based composite hydrogel for dual delivery of ciprofloxacin and ginsenoside Rh2 to treat Staphylococcus aureus-induced skin infections. Drug Delivery. 2020;27(1):632–641. doi:10.1080/10717544.2020.1756985
142. Ajmal G, Bonde GV, Mittal P, Pandey VK, Yadav N, Mishra B. PLGA/Gelatin-based electrospun nanofiber scaffold encapsulating antibacterial and antioxidant molecules for accelerated tissue regeneration. Mater Today Commun. 2023;35:105633. doi:10.1016/j.mtcomm.2023.105633
143. Jia Y, Zhang H, Yang S, et al. Electrospun PLGA membrane incorporated with andrographolide-loaded mesoporous silica nanoparticles for sustained antibacterial wound dressing. Nanomedicine. 2018;13(22):2881–2899. doi:10.2217/nnm-2018-0099
144. Wu Y, Wei G, Cao X, Wang R, Gou X. Stimuli-responsive dual-drug loaded microspheres with differential drug release for antibacterial and wound repair promotion. Colloids Surf B. 2025;248:114455. doi:10.1016/j.colsurfb.2024.114455
145. Koo H, Allan RN, Howlin RP, Stoodley P, Hall-Stoodley L. Targeting microbial biofilms: current and prospective therapeutic strategies. Nat Rev Microbiol. 2017;15(12):740–755. doi:10.1038/nrmicro.2017.99
146. Wang B, Lu G, Song K, et al. PLGA-based electrospun nanofibers loaded with dual bioactive agent loaded scaffold as a potential wound dressing material. Colloids Surf B. 2023;231:113570. doi:10.1016/j.colsurfb.2023.113570
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Gastroprotective Effect of Azilsartan Through Ameliorating Oxidative Stress, Inflammation, and Restoring Hydroxyproline, and Gastrin Levels in Ethanol-Induced Gastric Ulcer
Hama Amin RR, Aziz TA
Journal of Inflammation Research 2022, 15:2911-2923
Published Date: 11 May 2022
Blood Coral Polysaccharide Helps Prevent D-Gal/LPS-Induced Acute Liver Failure in Mice
Li C, Lai S, Yi R, Zhou X, Zhao X, Li Q
Journal of Inflammation Research 2022, 15:4499-4513
Published Date: 8 August 2022
Efficacy and Anti-Inflammatory Activity of Ashwagandha Sustained-Release Formulation on Depression and Anxiety Induced by Chronic Unpredictable Stress: in vivo and in vitro Studies
KrishnaRaju AV, Somepalli V, Thanawala S, Shah R
Journal of Experimental Pharmacology 2023, 15:291-305
Published Date: 25 July 2023
The NRF-2/HO-1 Signaling Pathway: A Promising Therapeutic Target for Metabolic Dysfunction-Associated Steatotic Liver Disease

Li N, Hao L, Li S, Deng J, Yu F, Zhang J, Nie A, Hu X
Journal of Inflammation Research 2024, 17:8061-8083
Published Date: 3 November 2024
From Citrus to Clinic: Limonene’s Journey Through Preclinical Research, Clinical Trials, and Formulation Innovations

S, Devi N, Bhattacharya B, Sharma A, Singh I, Kumar P, Huanbutta K, Sangnim T
International Journal of Nanomedicine 2025, 20:4433-4460
Published Date: 11 April 2025