")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Nationwide Trends of Modern Endodontic Practices Related to Working Length, Instrumentation, Magnification, and Obturation: A Comparative Cross-Sectional Survey Comparing Endodontic and Non-Endodontic Specialties Practicing Root Canal Treatment in India
Authors Mohanty A, Patro S , Das A, Miglani S, Luke AM, Pawar AM , Reda R , Zanza A, Testarelli L
Received 16 November 2022
Accepted for publication 20 March 2023
Published 2 April 2023 Volume 2023:16 Pages 865—873
DOI https://doi.org/10.2147/JMDH.S397778
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Ankita Mohanty,1 Swadheena Patro,1 Antarikshya Das,1 Sanjay Miglani,2 Alexander Maniangat Luke,3,4 Ajinkya M Pawar,5 Rodolfo Reda,6 Alessio Zanza,6 Luca Testarelli6
1Department of Conservative Dentistry and Endodontics, Kalinga Institute of Dental Sciences, KIIT University, Bhubaneswar, Odisha, 751024, India; 2Department of Conservative Dentistry and Endodontics, Faculty of Dentistry, Jamia Millia Islamia (A Central University), New Delhi, 110025, India; 3Department of Clinical Science, College of Dentistry, Ajman University, Al-Jurf, Ajman, 346, United Arab Emirates; 4Center of Medical and Bio-Allied Health Sciences Research, Ajman University, Al-Jurf, Ajman, 346, United Arab Emirates; 5Department of Conservative Dentistry and Enododntics, Nair Hospital Dental College, Mumbai, Maharashtra, 400008, India; 6Department of Oral and Maxillo-Facial Sciences, Sapienza University of Rome, Rome, 00161, Italy
Correspondence: Alexander Maniangat Luke, Department of Clinical Science, College of Dentistry, Ajman University, Al-Jurf, Ajman, 346, United Arab Emirates, Email [email protected] Ajinkya M Pawar, Department of Conservative Dentistry and Enododntics, Nair Hospital Dental College, Mumbai, Maharashtra, 400008, India, Email [email protected]
Aim: The present study was designed to assess trends in contemporary endodontic practice regarding the techniques and materials used in endodontic therapy among dental practitioners from various regions of India.
Methods: A cross-sectional questionnaire-based study was conducted amongst dentists who were pursuing postgraduates in endodontics (PG Endo) and other branches (PG-OB), specialists from other branches (MDS-OB) and specialists in endodontics (MDS-Endo) in various dental colleges representing East, West, North, South, and Central zones through an e-survey using Google forms. State-wise postgraduate dental college lists were obtained from the Dental Council of India (DCI) website. Using a multistage cluster random sampling method and considering the unanticipated response rate, emails were sent to 2100. A 29-item close-ended questionnaire, framed according to different aspects of endodontic treatment, was used to record the responses.
Results: When the distribution of the groups of dentists was compared, the central zone had the highest number of PG-OB (44.2%) and the lowest number of MDS-Endo (8.4%). The electronic apex locator (EAL) method of working length determination has been reported less among MDS-Endo than MDS-OB. The difference between the usage of various methods for working length determination was significant among the different groups in all the zones. (p < 0.0001) Most MDS-Endo preferred the rotary method of instrumentation over the combination method for different zones. The majority of dental practitioners preferred a combination method of instrumentation.
Conclusion: Zone-wise comparisons among dentists showed the majority of general dental practitioners preferred the combination method (radiographs and electronic apex locator) for working length determination. Most MDS-Endo preferred the rotary method of instrumentation over the combination method for different zones. All dental practitioners did not so commonly use magnification in all the zones. The single cone technique was the most opted by dental practitioners of all the zones.
Keywords: endodontic practices, endodontists, dental practitioners, survey
Introduction
Endodontics is a rapidly expanding branch of dentistry, including root canal therapy as a regular treatment option.1,2 Technological and material advances are carefully applied based on evidence-based approaches. Endodontic practise is effective when research-backed materials and procedures are used.3
Contemporary endodontics includes orofacial pain management, pulp therapy, root canal treatment and retreatment, post-treatment endodontic disease, surgical endodontics, internal tooth whitening, and coronal restorations with a post-core.4 New tools, techniques, and methodologies are always being developed, leading to increased success rates. Nevertheless, treatment outcome is determined by a number of factors, including canal complexity and endodontist-controlled variables such as canal preparation method and apical seal placement.5 As a result, dental practitioners performing root canal therapy now have a comprehensive selection of endodontic armamentarium.6
Endodontic practice surveys, previously conducted in several countries, aid in overcoming this dilemma by examining adaptation to novel techniques.7,8 Since these surveys were undertaken, the diagnostic modality of therapies has changed due to novel materials, efficient irrigation procedures, and the latest scientific evidence supporting clinical effectiveness and findings. For example, the precision of electronic apex locators has altered the practice of determining working length.9 Their study in India in 2022 demonstrated that the novel Root ZX mini Apex Locator (third-generation Electronic) had excellent precision in determining working length determination.10
The evidence-based technique in dentistry is being used to conduct continuing research and modification of root canal treatment guidelines. Unfortunately, adopting the most recent advancements cannot guarantee therapeutic effectiveness.11 Understanding the newest innovations in microscopes, rotary devices, and obturation procedures is critical, since they have a significant impact on endodontic treatment. Root canal therapy conducted by experts often has a greater success rate than that of regular dentists.12
One of the main reasons there is a dearth of knowledge on endodontic standards in India is that there is no centralised organisation that regulates endodontics there. As there is no centralised organisation to oversee and regulate the sector, there is no set standard for endodontic therapy. Patients may suffer injury as a consequence of variations in the quality of their therapies as a result of this. Moreover, there is a lack of funding for endodontic research in India. Because of this, it may be challenging to carry out the necessary research to develop precise standards and criteria for endodontic therapy. Therefore, there is a big problem that has to be remedied with the lack of knowledge about endodontic standards in India.
This study aims to assess the adaptability of Indian dental practitioners to new techniques and materials in contemporary endodontic practice with respect to working length, instrumentation, magnification, and obturation. It will identify gaps in everyday practice and standardize treatment for patients by examining whether current procedures and materials are being applied correctly or incorrectly. The study used a questionnaire-based survey to compare the trends in endodontic therapy among dental practitioners from various regions of India to those practicing root canal treatment in India.
Methods
The institutional review committee approved the study by Kalinga Institute of Dental Sciences (KIDS/RES/030/2022).
Study Setting
A cross-sectional questionnaire-based study was conducted amongst dentists who were pursuing postgraduates in endodontics (PG Endo) and other branches (PG-OB), specialists from other branches (MDS-OB) and specialists in endodontics (MDS-Endo) in various dental colleges representing East, West, North, South, and Central zones through an e-survey using Google forms. Any incomplete questionnaire was excluded from the current evaluation.
Study Population and Sampling Technique
State-wise postgraduate dental college lists were obtained from the Dental Council of India (DCI) website. There was uneven distribution of colleges in different zones, indicating a proportionate multistage cluster random sampling method. It was noted that the southern zone housed the greatest number of dental schools as compared to other zones. A list of the email addresses of all four groups of dentists was collected. A minimum of 1601 sample size was estimated using G*Power software (version 3.1.9.7.), and emails were sent to 2100, considering the unanticipated response rate.
Study Tools and Data Collection
The third part of the extensive 29-item close-ended questionnaire containing 4 items are included in the current study. The entire 29-item close-ended questionnaire was framed according to different aspects of endodontic treatment which include parameters or preferences like sterilization technique, using magnification, biomechanical radiographic technique used, preferred isolation technique, local anaesthesia administration technique, preferred rotary instrumentation, working length determination, choice of irrigating material, choice of sealant used, choice of obturation technique employed, etc. (Supplementary File 1). The third component comprising 4 questions (Supplementary File 2) of the 29-item close-ended questionnaire is reported here, which includes working length determination practice, instrumentation practice, magnification procedures, and obturation methods. The previous 2 parts of the survey have already been reported.11,13
Lawshe’s method14 was used for content validity using judgments from a panel of 15 subject matter experts. (SMEs) Cronbach’s alpha value was calculated for each subscale to know the reliability coefficient. A high internal consistency was indicated with α= 0.97.
Checkboxes were provided, and participants had to click on any one option for each question. Care was taken so that one person could answer the questionnaire only once, and all questions were mandatory. The responses were directly recorded through Google forms. Since this was an e-survey, the informed consent was included in the Google form.
Statistical Analysis
The online recorded information was converted into codes and analyzed using Statistical Package for Social Sciences (SPSS) for Windows, Version 28.0. (Armonk, NY: IBM Corp.) Confidence intervals were set at 95%, and a p-value ≤0.05 was considered statistically significant. The chi-square test was applied to compare four groups amongst various zones of India.
Results
All dentists who performed root canal treatments in clinic or college and are willing to participate in the study were enrolled. This study included 2000 dentists who were contacted by e-mail by the investigator to complete the questionnaire. The sample size of 1601 dentists (who successfully completed the entire questionnaire) in total was achieved with 80.05% response rate. The distribution of responses from different zones has been presented in Table 1.
 |
Table 1 Zone-Wise Distribution of the Responses |
The male and female ratio was almost at par in the eastern and southern zones. The percentage of females was double that of males in the western and northern zones. The ratio was thrice in the central zone. When the distribution of the groups of dentists was compared, the central zone had the highest number of postgraduates belonging to other specialities (44.2%) and the lowest number of endodontists (8.4%).
Working Length Determination Practices
Zone-wise variations showed the majority of specialists from MDS-OB preferred combination method for working length determination. The electronic apex locator (EAL) method of working length determination has been reported less among MDS-Endo specialists as compared to other dental practitioners. The difference between the usage of various methods for working length determination was significant among the different groups in all the zones. (p < 0.0001). Across the zones, the groups’ differences were statistically significant (p < 0.0001) (Table 2).
 |
Table 2 Zone-Wise Distribution and Comparison of Working Length Determination Practices |
Techniques of Instrumentation Practices
Most specialists from MDS-Endo preferred the rotary method of instrumentation over the combination method for different zones. The remaining dental practitioners preferred a combination method of instrumentation. The difference between the methods of instrumentation among the dentists of the various zones was significant (p < 0.0001). Across the zones, the difference among the groups was statistically significant (p < 0.0001) (Table 3).
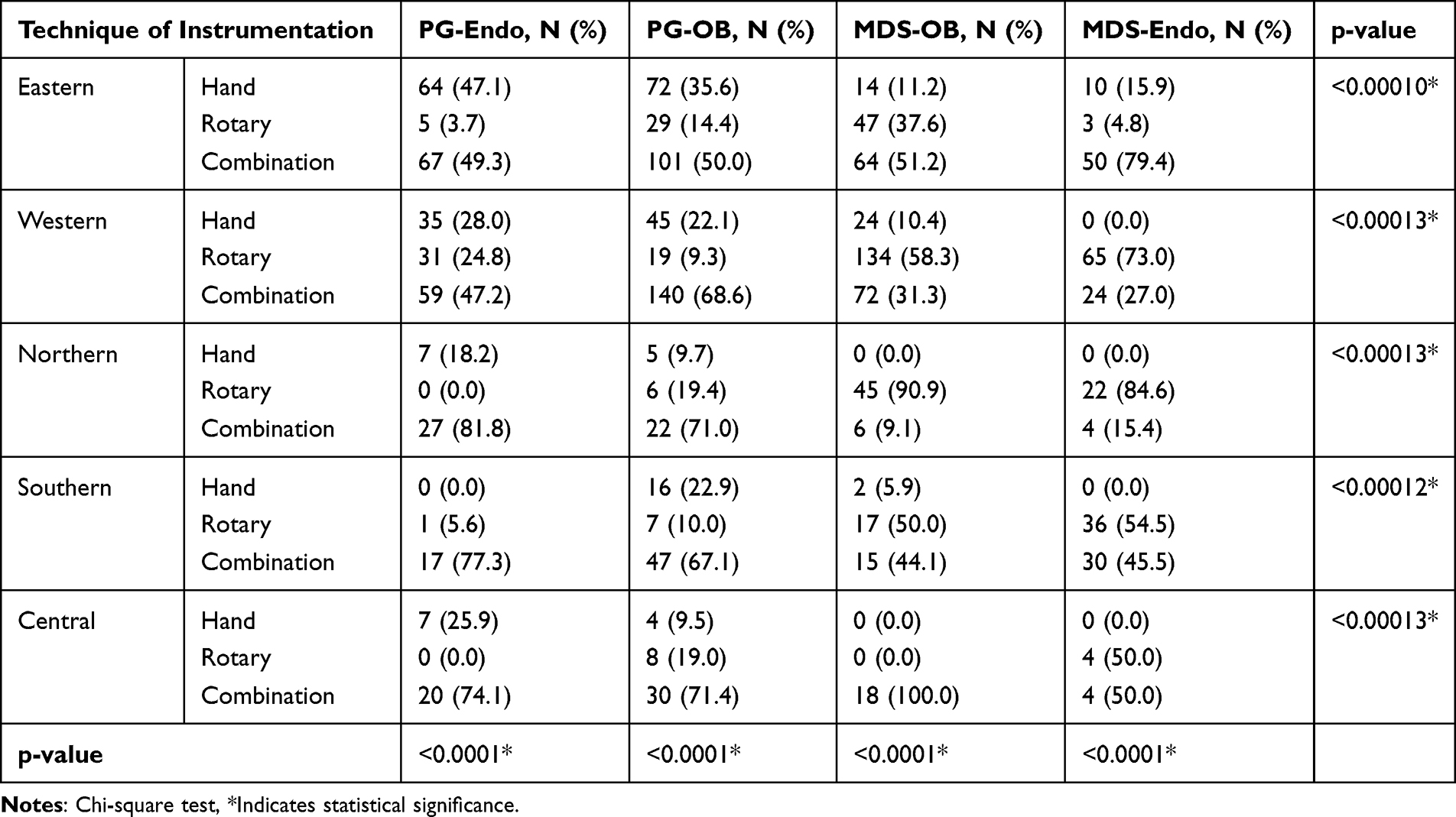 |
Table 3 Zone-Wise Distribution and Comparison of Techniques of Instrumentation Practices |
Methods of Magnification Practices
All dental practitioners did not so commonly use magnification in all the zones. MDS-OB most commonly used loupes in all the zones as compared to other dental practitioners. The difference between the magnification methods among the dentists of the various zones was significant (p < 0.0001). Across the zones, the difference among the groups was statistically significant (p < 0.0001) (Table 4).
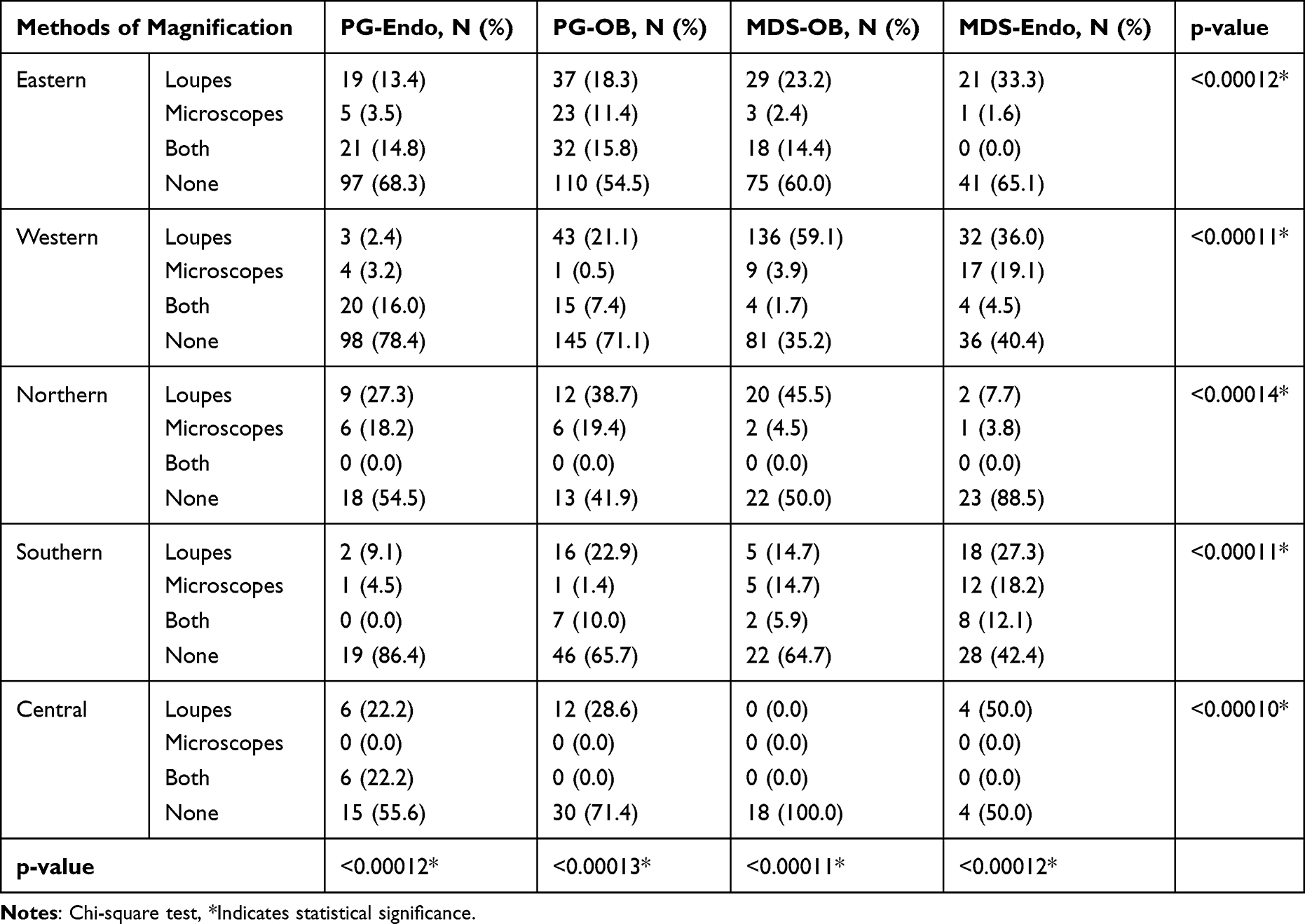 |
Table 4 Zone-Wise Distribution and Comparison of Methods of Magnification Practices |
Method of Obturation
The single cone technique was the most opted by all dental practitioners of all the zones. In the 1st and the 4th zone, MDS-Endo preferred the lateral cone technique over others. The difference in practice among the dental practitioners was seen to be statistically significant (p < 0.0001) among the groups in individual and across the zones (Table 5).
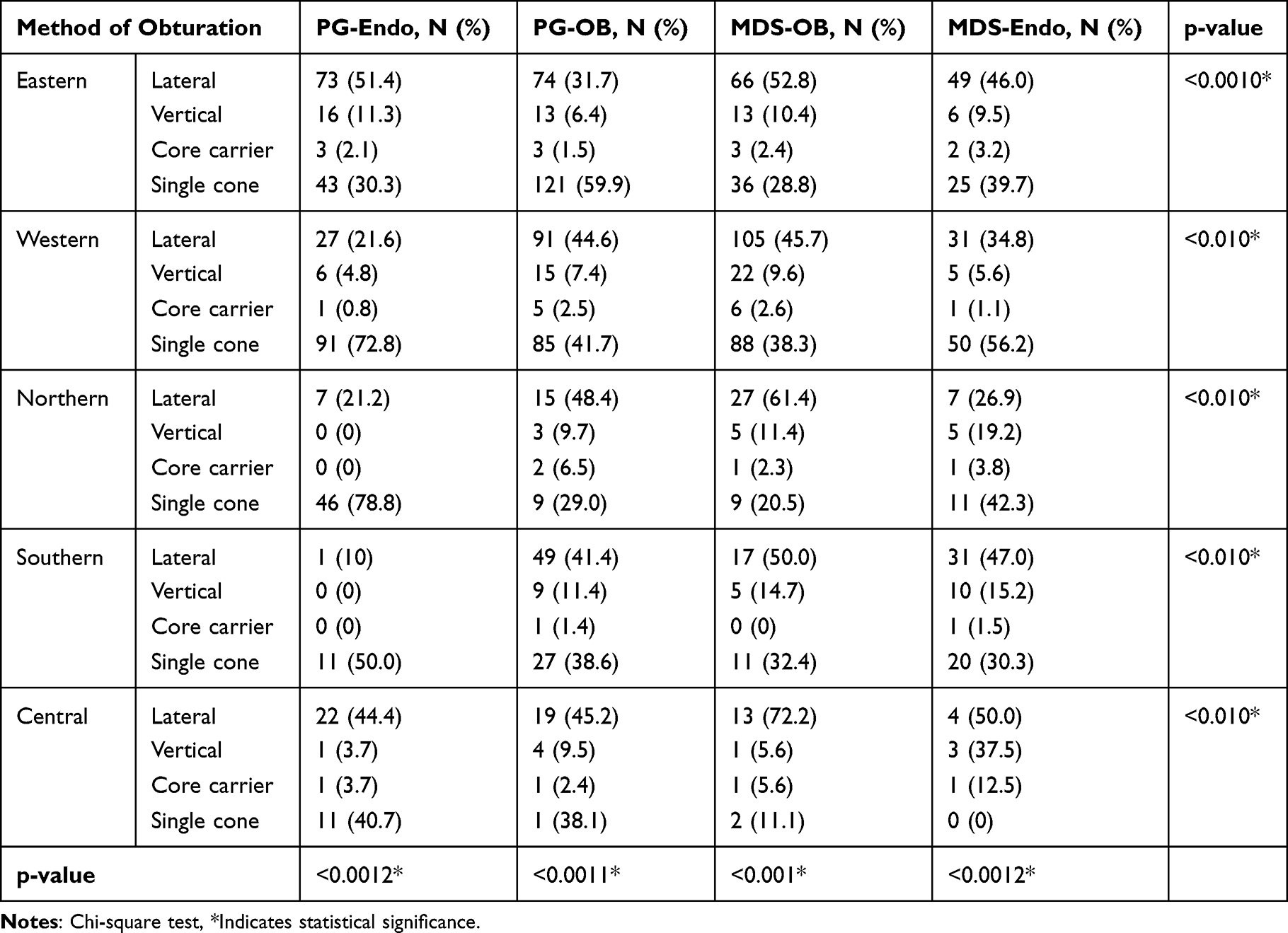 |
Table 5 Zone-Wise Distribution and Comparison of Method of Obturation |
Discussion
Endodontics is a vigorous, enormously expanding field that has undergone significant advancements in endodontic procedures and material advancements over the past ten years.15 This has evaluated the trends in contemporary endodontics and has significantly evaluated various endodontic procedures.16,17 Thus, over the years, the majority of endodontic research has concentrated on effectively treating apical periodontitis. Dentists who perform RCTs have been compelled to make clinical decisions in the face of substantial uncertainty.18 While clinicians place a high value on radiographic healing of periapical tissues, this outcome measure may be irrelevant for asymptomatic patients who seek long-term tooth survival. This has also led to the evolution of the underlying principles and treatment regimens of the endodontic procedure.19–21
Thus, the goal of the present study is to use a questionnaire-based survey to assess trends in contemporary endodontic practice regarding the techniques and materials utilized in endodontic therapy among diverse dental practitioners from different zones (North, South, East, West, and Central zones) of India. The rationale for selecting these groups, ie, MDS in endodontics, MDS in another branch, postgraduate students in endodontics, and postgraduate students in another branch, was advantageous, as all participants were exposed to the Masters in Dentistry curriculum and were well versed in the fundamentals of conducting a successful root canal procedure. Also, as the endodontic specialty is known as the foundation of dentistry, every dental graduate aspires to work in this field. Non-MDS endodontic experts might not hold a formal master’s degree in endodontics, but they nevertheless have a lot of practical endodontic treatment expertise. Non-MDS endodontic experts undertake a number of continuing dental education (CDE) courses all the time to keep their knowledge and abilities current. To ensure that patients receive the finest treatment possible, these professionals also employ the most recent tools and methods.
Savani et al16 conducted a national survey in the United States addressing current endodontic trends among general practitioners and discovered that 84% of general practitioners had adopted newer technologies such as digital radiography, magnification, electronic apex locators, and NiTi rotary instruments. Another study by Mohanty et al in 202011 compared rubber dams, preferred methods of instrumentation, obturation, and pre- and post-drug regimens. Thus, we conducted a nationwide cross-sectional survey adding various novel endodontic techniques like working length determination, instrumentation methods, magnification practices, and obturation techniques.11
In our study, the zone-wise variations showed dentists to prefer the combination method (radiographs and electronic apex locator) for working length determination. Combining traditional radiography techniques with contemporary electronic apex locators may determine an appropriate working length.22,23 Also, in our study, electronic apex locator (EAL) method of working length determination has been reported less among MDS-Endo as compared to MDS-OB. Our results were in accordance with a study conducted by Kohli et al in 20146 and Patrol et al in 2021,13 wherein the majority of dental professionals used a combination method for working length determination. This finding was contrary to that of Sedani et al in 2020.24 Joseph et al in 2022,25 wherein using apex locators to calculate working length was the most widely used method for determining working length and was also contrary to that of the study done by Bandaranayake et al in 2021 wherein majority of the respondents used tactile sensation in working length determination.4 Thus, the efficacy of endodontic therapy depends on a clinically accurate evaluation of working length.
Endodontic therapy aims to form and clean the root canal system so the entire space can be filled with a three-dimensional impermeable material. In our study, most endodontists preferred the rotary method of instrumentation over the combination method of different zones, which was similar to the study done by Anwer et al in 2018.26 In the present study, the remaining dental practitioners preferred a combination (hand and rotary) method of instrumentation. This finding was similar to that of Kishen et al in 2016,27 Mohanty et al in 202011 and Patrol et al in 202113 wherein dental practitioners preferred the combined method of instrumentation as compared to a single method. Kohli et al6 also reported similar findings wherein 71% of the dental practitioners preferred combined methods of instrumentation. However, these findings were contrary to those of Bandaranayake et al,4 as the most popular instrument in root canal preparation among dental practitioners was K files followed by H files.27 Raoof et al3 also reported extensive use of hand files by the dental practitioners in his study.
Magnification has been shown to significantly raise performance standards and technical precision and enhance ergonomics in endodontic clinical practice.18 However, magnification was not so commonly used by dental practitioners in all the zones. Additionally, loupes were mostly used by MDS-OB in all the zones as compared to other groups of dental practitioners. This finding was in accordance with the study done by Penmetsa et al, in 2017, wherein magnification is not commonly used in endodontic practice by less than 50% of practitioners.28,29 Magnification may not be used for several reasons, including its significant expense and somewhat steep learning curve. Elrashid et al30 also demonstrated similar findings which was conducted in Riyadh city in 2020 and stated that loupes were chosen above microscopes as a magnification tool in endodontic practice. However, a study conducted by Shah et al, in 2021,9 suggested contrary findings that board certified endodontists seemed to be more likely to always utilize microscope than non-board-certified endodontists.9 Low use of magnification methods was also reported amongst the dental practitioners of India.31 This could be linked to a shortage of equipment in dental colleges as well as a lack of training amongst several other branch postgraduates besides endodontists, which leads to an inadequate assurance to practice on a regular basis.28,29,32
Significantly contributing to the overall success of endodontic treatment is the quality of the root canal filling. Thus, in our study, single cone technique was most opted by dental practitioners of all the zones. This was contrary to the findings of Bandaranayake et al,4 wherein Single cone greater taper GP obturation was used by fewer practitioners. Additionally, in our study, it was seen that in the 1st and the 4th zone MDS-Endo preferred lateral cone technique over others. Cold lateral compaction of gutta-percha with a root canal sealer is largely recognized as the most prevalent obturation method. It is a straightforward and adaptable method that does not require expensive equipment.4 This finding was similar to previous studies, wherein they preferred lateral condensation techniques over other obturation techniques.6,25,26
Strengths and Limitations
The study was carried out meticulously, taking the entire country into account. This is the first study enlisting postgraduate students and specialists from various zones to enhance the generalization of the results thereby making comparisons between different levels of dental practitioners including PG-OB. However, this study could have been influenced by reporting bias. Additional limitations may be to keep the survey relatively quick, limit the quantity of in-depth data gathered from respondents, and restrict the survey to a certain cohort that is conversant with technology and has access to the internet. It would have been favourable to consider the endodontic expertise of specialists who were not MDS in endodontics. An improved study design would include an analytical element on endodontic treatment that would aid in precisely determining the causes for the effective practice.
Recommendations
Professional bodies should implement continuous professional development programmes to improve practitioners’ knowledge and abilities. Continuing education programmes may be able to encourage and integrate new technologies into their regular practice. As a result, practitioners must raise the bar of their clinical practice by aggressively integrating the plethora of technology and materials available for endodontic practice based on research-based data. Our findings show that there remains a deficit in adaptability of many advanced endodontic techniques, recommending the inclusion of comprehensive endodontic practice training for postgraduate students.
Conclusion
The condition of endodontic practice among PG-Endo, PG-OB, MDS-OB, and MDS-Endo was reviewed and collated for our study. A wide range of dentists, most of whom adhere to the fundamental principles and methods used by professionals across the world. The majority of dental professionals prefer the combined approach (radiographs and electronic apex finder) for determining working length, according to zone-by-zone variations. Whereas the majority of MDS-Endo favoured the rotational instrumentation approach over the combination method of several zones. Our study’s key conclusion was that dental professionals did not utilise magnification all that frequently throughout the zones. When compared to other groups of dentists, MDS-OB employed loupes the most frequently in all the zones, and single cone method was the most frequently used by dental professionals.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abbott PV. Endodontics – current and future. J Conserv Dent. 2012;15(3):202–205. doi:10.4103/0972-0707.97935
2. Markowitz K, Roberts E, Strickland M. Dental products and evidence-based dentistry. Quintessence Int. 2019;50(5):402–411. doi:10.3290/j.qi.a42293
3. Raoof M, Zeini N, Haghani J, Sadr S, Mohammadalizadeh S. Preferred materials and methods employed for endodontic treatment by Iranian general practitioners. Iran Endod J. 2015;10(2):112–116.
4. Bandaranayake B, Wettasinghe KA, Fonseka M, Jayasinghe RD. Current trends in endodontic practice, adaptation to new technologies and attitude of dental practitioners towards endodontic standards in Sri Lanka. J Multidiscip Dent Res. 2021;7(1):17–23. doi:10.38138/jmdr/v7i1.2
5. Bhandi S, Mashyakhy M, Abumelha AS, et al. Complete obturation-cold lateral condensation vs. thermoplastic techniques: a systematic review of micro-CT studies. Materials. 2021;14(14):4013. doi:10.3390/ma14144013
6. Kohli A, Singh S, Podar R, Dadu S, Kulkarni G. A comparative evaluation of endodontic practice trends in India: the Mumbai study. Indian J Dent Res. 2014;25(6):729–736. doi:10.4103/0970-9290.152179
7. Jenkins SM, Hayes SJ, Dummer PM. A study of endodontic treatment carried out in dental practice within the UK: endodontic treatment in dental practice. Int Endod J. 2001;34(1):16–22. doi:10.1046/j.1365-2591.2001.00341.x
8. Slaus G, Bottenberg P. A survey of endodontic practice amongst Flemish dentists. Int Endod J. 2002;35(9):759–767. doi:10.1046/j.1365-2591.2002.00564.x
9. Shah A. Current Trends in the Management of Endodontic Emergencies. West Virginia University Libraries; 2022.
10. Khan SA, Khanna R, Navit S, Jabeen S, Grover N, Pramanik S. Comparison of radiovisiography, an apex locator and an integrated endomotor-inbuilt apex locator in primary teeth endometrics. Int J Clin Pediatr Dent. 2022;15(Suppl 1):S18–S21. doi:10.5005/jp-journals-10005-2123
11. Mohanty A, Patro S, Barman D, Jnaneswar A. Modern endodontic practices among dentists in India: a comparative cross-sectional nation-based survey. J Conserv Dent. 2020;23(5):441–446. doi:10.4103/JCD.JCD_408_20
12. Alley BS, Kitchens GG, Alley LW, Eleazer PD. A comparison of survival of teeth following endodontic treatment performed by general dentists or by specialists. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98(1):115–118. doi:10.1016/j.tripleo.2004.01.004
13. Patro S, Mohanty A, Barman D. Comparative study of endodontic practices among dentists in India: a nation-wide cross-sectional survey. Int J Curr Res Rev. 2021;13(10):24–28. doi:10.31782/ijcrr.2021.131016
14. Lawshe CH. A quantitative approach to content validity. Pers Psychol. 1975;28(4):563–575. doi:10.1111/j.1744-6570.1975.tb01393.x
15. Silva EJNL, De-Deus G, Souza EM, et al. Present status and future directions – minimal endodontic access cavities. Int Endod J. 2022;55(S3):531–587. doi:10.1111/iej.13696
16. Savani GM, Sabbah W, Sedgley CM, Whitten B. Current trends in endodontic treatment by general dental practitioners: report of a United States national survey. J Endod. 2014;40(5):618–624. doi:10.1016/j.joen.2014.01.029
17. Malmberg J, Fincham O, Pijeira-Díaz HJ, Järvelä S, Gašević D. Revealing the hidden structure of physiological states during metacognitive monitoring in collaborative learning. J Comput Assist Learn. 2021;37(3):861–874. doi:10.1111/jcal.12529
18. Singh J, Goyal A, Kaur M, Fatima A, Sharma R, Sood P. Magnification in endodontics – the small is big enough – a review article. J Dent Panacea. 2022;4(1):10–20. doi:10.18231/j.jdp.2022.004
19. Mohamed A, Steier L. Uncertain decision-making in primary root canal treatment. J Evid Based Dent Pract. 2017;17(3):205–215. doi:10.1016/j.jebdp.2017.01.001
20. Ciobanu IE, Rusu D, Stratul SI, Didilescu AC, Cristache CM. Root canal stripping: malpractice or common procedural accident-an ethical dilemma in endodontics. Case Rep Dent. 2016;2016:4841090. doi:10.1155/2016/4841090
21. Nadeau B, Jung D, Vora V. Trends towards conservative endodontic treatment. Oral Health. 2019;109:30–45.
22. Smadi L. Comparison between two methods of working length determination and its effect on radiographic extent of root canal filling: a clinical study. BMC Oral Health. 2006;6(1):4. doi:10.1186/1472-6831-6-4
23. Dutta K, Desai PD, Das UK, Sarkar S. Comparative evaluation of three methods to measure working length – manual tactile sensation, digital radiograph, and multidetector computed tomography: an in vitro study. J Conserv Dent. 2017;20(2):76–80. doi:10.4103/JCD.JCD_4_16
24. Sedani S, Thakkar A, Nikhade P. Ongoing trends in endodontic practice. J Res Med Dent Sci. 2020;8(3):110–117.
25. Joseph A, Ramanarayanan V, Venugopal K, Prabath Singh VP, Dhruvan K, Sagar K. Standards of practice among endodontists in Kerala, India: an exploratory study. Amrita J Med. 2022;18(2):50. doi:10.4103/amjm.amjm_7_22
26. Bhatti UA, Qureshi B, Azam S. Trends in contemporary endodontic practice of Pakistan: a national survey. J Pak Dent Assoc. 2018;27(2):50–56. doi:10.25301/jpda.272.50
27. Kishen A, Peters OA, Zehnder M, Diogenes AR, Nair MK. Advances in endodontics: potential applications in clinical practice. J Conserv Dent. 2016;19(3):199–206. doi:10.4103/0972-0707.181925
28. Penmetsa GS, Mani LP, Praveen G, Dwarakanath CD, Suresh S. Awareness, attitude, and prevalence of usage of magnification devices among the dental practitioners in the state of andhra pradesh – a questionnaire-based study. J Indian Soc Periodontol. 2017;21(5):398–402. doi:10.4103/jisp.jisp_268_17
29. Basunbul GI. The use of magnifying loupes among dental professionals. J Contemp Dent Pract. 2018;19(12):1532–1538. doi:10.5005/jp-journals-10024-2461
30. Elrashid AH, Alderaa KJ, Alissa HA, et al. Perceived effectiveness about endodontic practice among private general dental practitioners in Riyadh city, Saudi Arabia. J Family Med Prim Care. 2020;9(5):2426–2430. doi:10.4103/jfmpc.jfmpc_129_20
31. Low JF, Dom TNM, Baharin SA. Magnification in endodontics: a review of its application and acceptance among dental practitioners. Eur J Dent. 2018;12(4):610–616. doi:10.4103/ejd.ejd_248_18
32. Krithikadatta J, Nawal RR, Amalavathy K, McLean W, Gopikrishna V. Endodontic and dental practice during COVID-19 pandemic: position statement from the Indian Endodontic Society, Indian Dental Association, and International Federation of Endodontic Associations. Endodontology. 2020;32(2):55–66.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.