")
Back to Journals » Infection and Drug Resistance » Volume 15
National Early Warning Score and New-Onset Atrial Fibrillation for Predicting In-Hospital Mortality or Transfer to the Intensive Care Unit in Emergency Department Patients with Suspected Bacterial Infections
Authors Nielsen FE , Stæhr CS, Sørensen RH , Schmidt TA, Abdullah SMOB
Received 24 January 2022
Accepted for publication 5 July 2022
Published 26 July 2022 Volume 2022:15 Pages 3967—3979
DOI https://doi.org/10.2147/IDR.S358544
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Finn Erland Nielsen,1,2 Christina Seefeldt Stæhr,1 Rune Husås Sørensen,2 Thomas Andersen Schmidt,3,4 S M Osama Bin Abdullah2,5
1Department of Emergency Medicine, Copenhagen University Hospital, Bispebjerg and Frederiksberg, Copenhagen, Denmark; 2Department of Emergency Medicine, Slagelse Hospital, Slagelse, Denmark; 3Department of Emergency Medicine, Nordsjaellands Hospital, Hilleroed, Denmark; 4Institute of Clinical Medicine, Faculty of Health Sciences, University of Copenhagen, Copenhagen, Denmark; 5Department of Internal Medicine, Copenhagen University Hospital, Amager and Hvidovre, Copenhagen, Denmark
Correspondence: Finn Erland Nielsen, Department of Emergency Medicine, Bispebjerg and Frederiksberg Hospital, Copenhagen, Denmark, Tel +45 26822753, Fax +45 38639863, Email [email protected]
Purpose: There are conflicting data regarding the role of the National Early Warning Score 2 (NEWS2) in predicting adverse outcomes in patients with infectious diseases. New-onset atrial fibrillation (NO-AF) has been suggested as a sepsis-defining sign of organ dysfunction. This study aimed to examine the prognostic accuracy of NEWS2 and whether NO-AF can provide prognostic information in emergency department (ED) patients with suspected bacterial infections.
Patients and Methods: Secondary analyses of data from a prospective observational cohort study of adults admitted in a 6-month period with suspected bacterial infections. We used the composite endpoint of in-hospital mortality or transfer to the intensive care unit as the primary outcome. The prognostic accuracy of NEWS2 and quick sequential organ failure assessment (qSOFA) and covariate-adjusted area under the receiver operating curves (AAUROC) were used to describe the performance of the scores. Logistic regression analysis was used to examine the association between NO-AF and the composite endpoint.
Results: A total of 2055 patients were included in this study. The composite endpoint was achieved in 198 (9.6%) patients. NO-AF was observed in 80 (3.9%) patients. The sensitivity and specificity for NEWS2 ≥ 5 were 70.2% (63.3– 76.5) and 60.2% (57.9– 62.4), respectively, and those for qSOFA ≥ 2 were 26.3% (20.3– 33.0) and 91.0% (89.6– 92.3), respectively. AAUROC for NEWS2 and qSOFA were 0.68 (0.65– 0.73) and 0.63 (0.59– 0.68), respectively. The adjusted odds ratio for achieving the composite endpoint in 48 patients with NO-AF who fulfilled the NEWS2 ≥ 5 criteria was 2.71 (1.35– 5.44).
Conclusion: NEWS2 had higher sensitivity but lower specificity and better, albeit poor, discriminative ability to predict the composite endpoint compared to qSOFA. NO-AF can provide important prognostic information.
Keywords: infectious disease, sepsis, predictive ability, National Early Warning Score 2, NEWS2, quick sequential organ failure assessment, qSOFA, new-onset atrial fibrillation
Introduction
Sepsis is a potentially life-threatening condition with organ failure.1
Unfortunately, we do not have a robust diagnostic tool for identifying patients with sepsis. The previously used systemic inflammatory response syndrome (SIRS) criteria to identify patients with sepsis are obsolete due to the low specificity.1
A Sepsis-3 task force replaced the SIRS criteria in 2016 with clinical criteria based on the Sequential Organ Failure Assessment (SOFA) score.1 A parsimonious method of SOFA, the quick SOFA (qSOFA) score, was proposed for rapid risk stratification of patients with suspected infection.1 qSOFA was designed as a prognostic and not a diagnostic tool. However, qSOFA is not a sensitive tool for early identification of infection-induced organ dysfunction and has poor discriminative performance to predict a serious outcome.2,3 Therefore, a more accurate scoring system than qSOFA for detecting organ dysfunction and adverse outcomes is needed.
The National Early Warning Score (NEWS) determines the severity of disease and prompts critical care intervention.4 The UK Royal College of Physicians Early Warning Score version 2 (NEWS2) provides an updated early warning score (EWS) for identifying acutely ill patients in hospitals in England.5 However, data on the predictive validity of EWS in patients with sepsis are conflicting, and the methodology and quality of validation studies of early warning systems have been criticized.6,7 Therefore, further studies based on prospectively collected and multiple recorded data in ED settings compared to other bedside scoring systems are needed to assess the role of early warning systems in patients with suspected sepsis.6
It may also be interesting to study whether signs of disease severity and cardiac dysfunction other than those included in the different screening tools can contribute more prognostic information. New-onset atrial fibrillation (NO-AF) has been associated with increased mortality in patients with and without sepsis.8–19 There is uncertainty whether NO-AF independently affects the outcome or rather is a marker of disease severity.11,13,15,19 However, it has been suggested that NO-AF should be investigated as a potentially sepsis-defining sign of cardiac dysfunction.20
The primary aim of this study was to examine the prognostic accuracy of NEWS2 compared to qSOFA in predicting a composite endpoint of in-hospital mortality or admission to the intensive care unit (ICU) using ED admission clinical variables and worst clinical values within the first 4 h after presentation at the ED in adults with suspected bacterial infection. The secondary aim was to examine whether NO-AF on admission to the ED can provide more prognostic information in ED patients with suspected sepsis.
Materials and Methods
Setting
This study was performed as a secondary analysis of a single-center prospective observational cohort study of the prognostic ability of qSOFA, SOFA, and SIRS criteria in adult patients (age ≥18 years) with suspected bacterial infection admitted to the ED at Slagelse Hospital, Denmark, from October 1, 2017 to March 31, 2018.2,21 Slagelse Hospital is a tertiary care center with acute medical, surgical, and trauma care. The uptake area comprised 198,000 adult inhabitants, with 26,500 annual visits. The Danish healthcare system is universal and based on free and equal access to healthcare for all citizens. Privately funded Danish hospitals have no acute patient intake.22
Patients with Infections
During the study period, all patients with either documented or suspected infection diagnosed by a senior ED physician based on clinical presentation, laboratory test results, radiological findings, and if delivery of either intravenous or peroral antibiotics within 24 h from arrival were prospectively registered in a database as patients with suspected infectious disease.21 Initially, all patients were considered suffering from suspected bacterial diseases.
Sepsis Treatment Protocol
A standard sepsis treatment protocol based on Danish and international guidelines for the management of sepsis23,24 guided the staff in the early identification of ED patients with sepsis and treatment during the study period, independently of the present study. The treatment of patients with sepsis has been previously described in detail.2,21 A combination of clinical judgment, SIRS criteria, and qSOFA score was used to identify patients with suspected sepsis. The NEWS2 score was not used as a routine screening tool during the study period.
Inclusion and Exclusion Criteria
We included patients with suspected bacterial infection who were treated with intravenous or peroral antibiotics within 24 h after ED presentation and continuing for at least 48 hours. Figure 1 shows the excluded patients.2,21
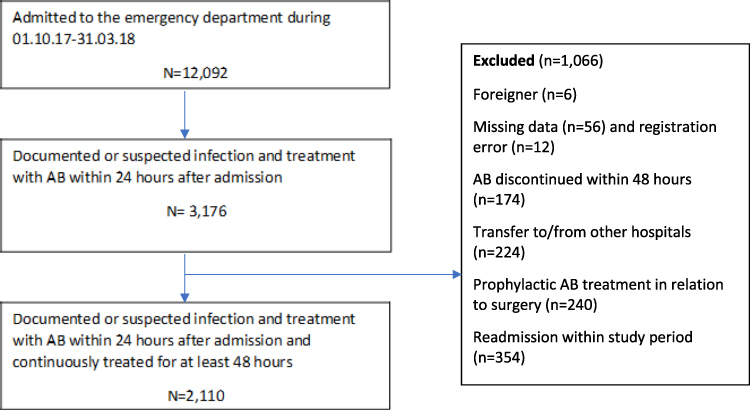 |
Figure 1 Flow-chart.Abbreviation: AB; antibiotics. |
Definitions
NEWS2 includes seven parameters with a score ranging from 0 to 20 (Table 1).5 The SpO2 Scale 2 was not included in the NEWs system.5 An altered mental state was assumed to be new unless confirmed to have other causes.
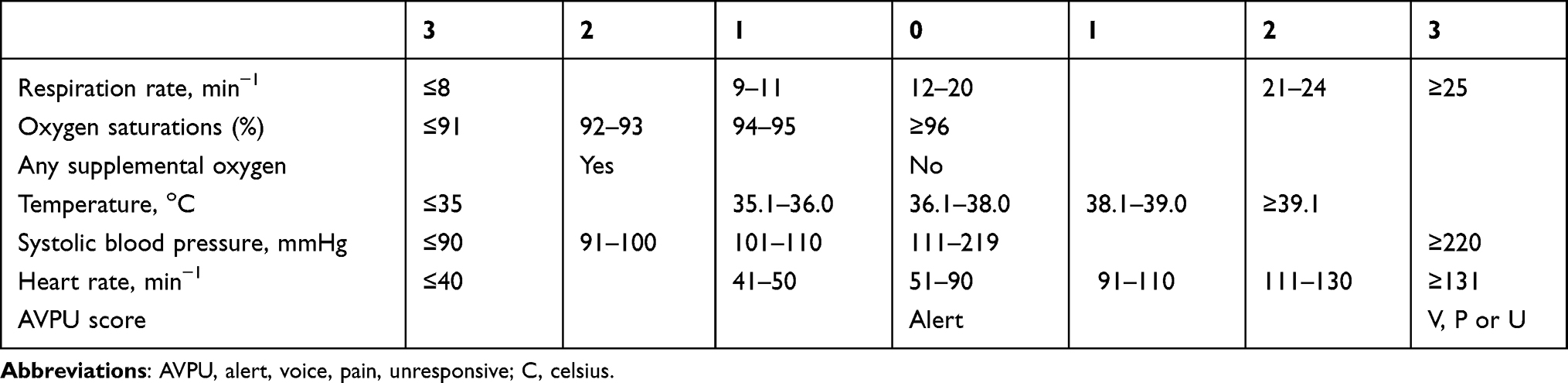 |
Table 1 National Early Warning Score (NEWS2) |
The definition of the qSOFA was based on the original guidelines.1 The total Sequential Organ Failure (SOFA) score included in the regression analyses was adjusted for chronic diseases with potential impact on the score. The method behind the SOFA adjustments has previously been described.2
A NEWS2 ≥5 score and qSOFA ≥2 score were used as the cutoff scores for positivity.1,5 However, both NEWS2 ≥5 and NEWS2 ≥7 were used as cutoff points in the analyses of prognostic accuracy.
We used the Charlson Comorbidity Index (CCI) to classify patients with chronic diseases.25 It was graded into three levels of severity: low (CCI score 0), moderate (CCI score 1–2), and high (CCI score ≥ 3).
Data Collection
All data in the present study were extracted from the research database constructed to conduct our previously published sepsis studies.2,21
We obtained information on the mental status (Glasgow Coma Scale or Alert Voice Pain Unresponsive), systolic blood pressure, respiratory rate, heart rate, body temperature, peripheral oxygen saturation, and any supplemental oxygen on admission to the ED. Furthermore, we obtained information on the single most abnormal or deranged value, if any, of the vital parameters within the first 4 h of stay, and was registered as the worst value within the first 4 h after ED admission. The authors calculated the NEWS2 and qSOFA scores based on the registered physiological parameters at admission and the worst values of the vital parameters within the first 4 h. The physiological parameters of NEWS2 are shown in Table 1. The qSOFA uses three criteria, assigning one point for low blood pressure (SBP ≤100 mmHg), high respiratory rate (≥22 breaths per min), or altered mental status (GCS<15).1
Information on comorbidities, results of admission laboratory tests, blood cultures, results of other examinations, transfer to the ICU, and treatment in the ICU were also obtained from the database.
Information on death was obtained from The Regional Zealand Patient Registration System, which is linked to the Danish Civil Registration System with updated daily information on the vital status of all Danish citizens.26
AF and ECG
The history of AF was obtained from the CCI classification of chronic diseases. The ECG at admission was analyzed to determine the occurrence of AF. NO-AF was defined as episodes of AF documented on a 12-lead electrocardiogram on admission without a history of AF.
Outcome
We used the composite endpoint of in-hospital mortality or transfer to the ICU as the primary outcome.
Statistical Analysis
Continuous data are presented as medians with interquartile ranges (IQR), assuming non-normality. Proportions are presented with 95% confidence intervals (CIs). Differences within medians with 95% CI and exact differences in proportions with 95% CI were used to compare the groups. Differences were considered significant if the 95% CI for the median difference or 95% CI for the difference in proportions did not include zero.
We used logistic regression analysis with adjustment for potential confounders (age, sex, CCI, and pulmonary infection) to examine the association between NEWS2, qSOFA, and the composite endpoint. The confounders were selected based on the judgment of pre-existing knowledge of factors associated with the outcome and analyses of the association between baseline characteristics and the composite endpoint.
We used univariate and multivariate logistic regression in an etiological study27 to analyze the association between NO-AF and the composite endpoint in patients with suspected sepsis (NEWS2 ≥5). The adjustment variables were age, sex, CCI, the SOFA score, and pulmonary infection status.
Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive and negative likelihood ratio (LR+/LR-) with NEWS2 ≥5,5 NEWS2 ≥7,5 and qSOFA ≥21 as cutoff points, and area under the receiver operating characteristic curve (AUROC with 95% CI) was used to assess the prognostic accuracy of the scores. The accuracy variables for the scores were calculated using admission and the worst clinical variables within the first 4 h after admission.
Both the unadjusted AUROC (UAUROC) and covariate-adjusted (age, sex, CCI) AUROC (AAUROC)28 values are presented. Pairwise comparisons of the UAUROCs were performed using the DeLong method with Bonferroni correction.
Stata 15.1 (StataCorp, College Station, Texas, USA) was used for all analyses.
Results
Population
A total of 12,092 patients were admitted, and 3176 patients were treated with antibiotics at arrival or within 24 h after arrival.21 A total of 1066 patients were excluded (Figure 1) leaving an infection cohort of 2110 patients. Furthermore, 55 (2.6%) patients were excluded due to missing values for score calculation, leaving 2055 patients (48.5% male) with a median age of 73.1 years (IQR 60.0–82.7) for further analyses. The numbers of patients with score positivity for NEWS2 and qSOFA at admission were 782 (38.1%) and 167 (8.1%), respectively (Table 2).
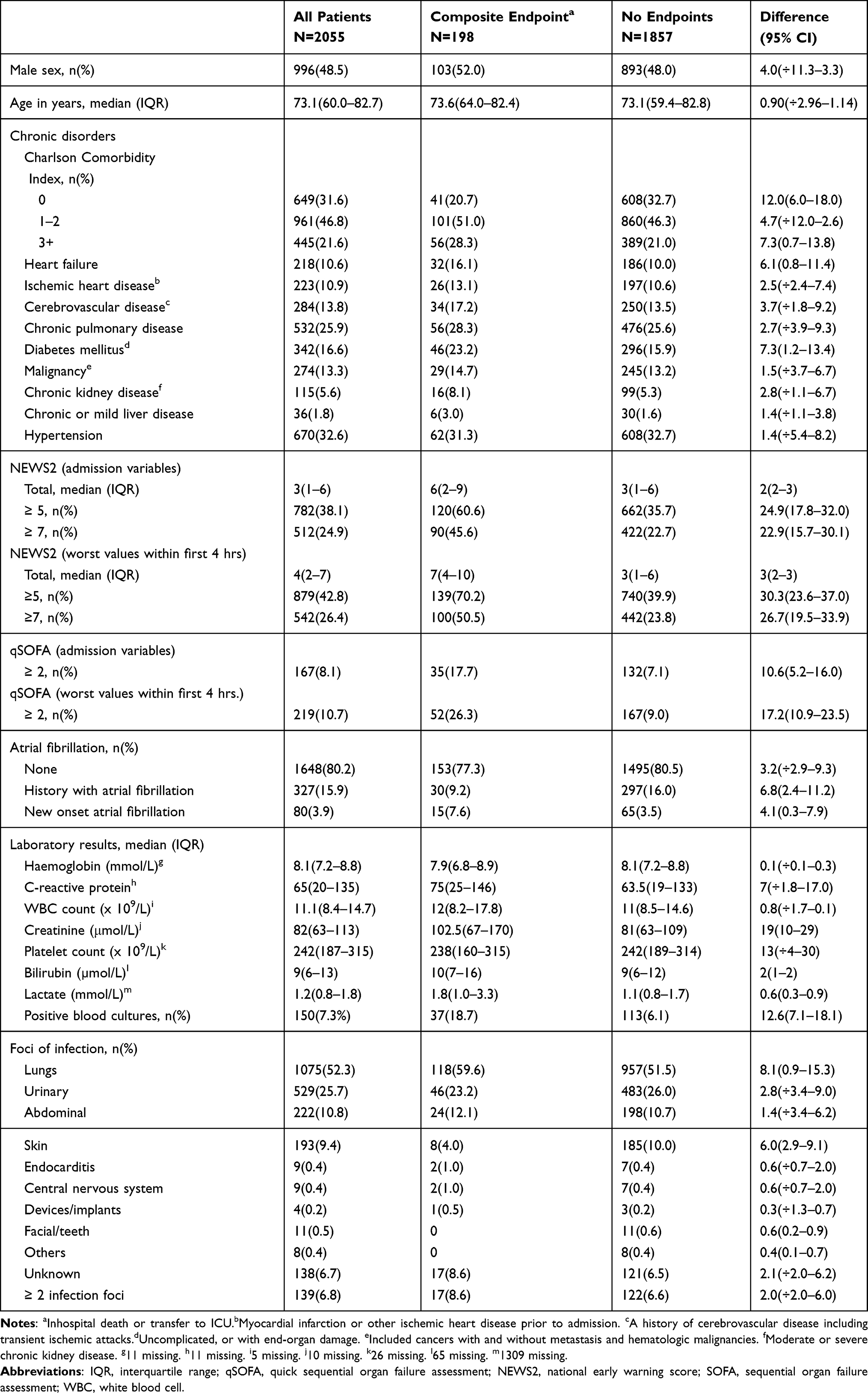 |
Table 2 Patient Characteristics According to the Composite Endpoint of In-Hospital Mortality or Transfer to the Intensive Care Unit |
Baseline Characteristics
The baseline characteristics according to the composite endpoint of in-hospital mortality or transfer to the ICU are shown in Table 2. The composite endpoint was achieved in 198 patients (9.6%; 8.4–11.0%). A total of 77 (3.8%; 3.0–4.7%) died during hospitalization, and 142 (6.9%; 5.9–8.1%) were transferred to the ICU. A total of 21 (1.0%; 0.6–1.6%) patients died during the ICU stay.
The proportion of patients who achieved the composite endpoint was significantly associated with CCI, sepsis score positivity, NO-AF, pulmonary infections, and positive blood culture results (Table 2). Several patients had missing laboratory values (Table 2); however, increased creatinine, bilirubin, and lactate levels were also associated with the composite endpoint (Table 2). Patients without a composite endpoint were more likely to have facial, tooth’s or skin infections (Table 2).
Composite Endpoint According to the Score Positivity
The proportion of patients who achieved the composite endpoint of in-hospital mortality or transfer to the ICU according to the positivity score of NEWS2 and qSOFA were 15.4% and 21.0%, respectively (Table 3). The odds of achieving the composite endpoint for positivity score were significantly increased for both admission scores after adjusting for potential confounding factors (Table 3). Adjusted odds ratio (OR) for the composite endpoint for NEWS2 ≥5 and qSOFA ≥2 using the worst clinical values within the first 4 h was 4.38 (2.24–8.54) and 4.63 (3.07–6.99), respectively (Table 3).
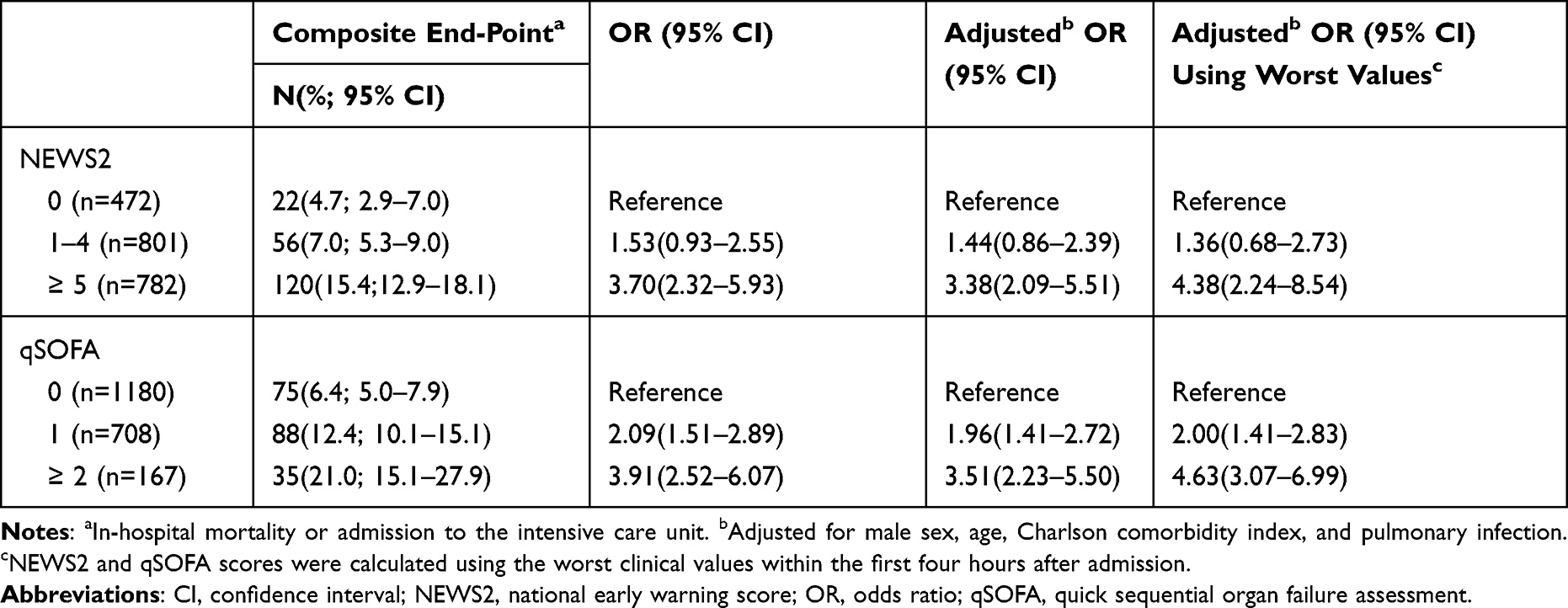 |
Table 3 Odds Ratio for the Composite Endpoint of In-Hospital Mortality or Transfer to the Intensive Care Unit According to Different Sepsis Scores |
Prognostic Accuracy of the Scores Using Clinical Admission Values
The sensitivity and specificity of NEWS2 ≥5 for predicting the composite endpoint of in-hospital mortality or transfer to the ICU were 60.6% and 64.4%, respectively (Table 4). The sensitivity decreased and the specificity increased using seven as the cutoff point (Table 4). The sensitivity of NEWS2 ≥5 was much higher than that of qSOFA ≥2 (60.6% vs. 17.7%); however, the specificity was lower than that of qSOFA ≥2 (64.4 vs 92.9%) (Table 4). Predictive values and likelihood ratios are also presented in Table 4.
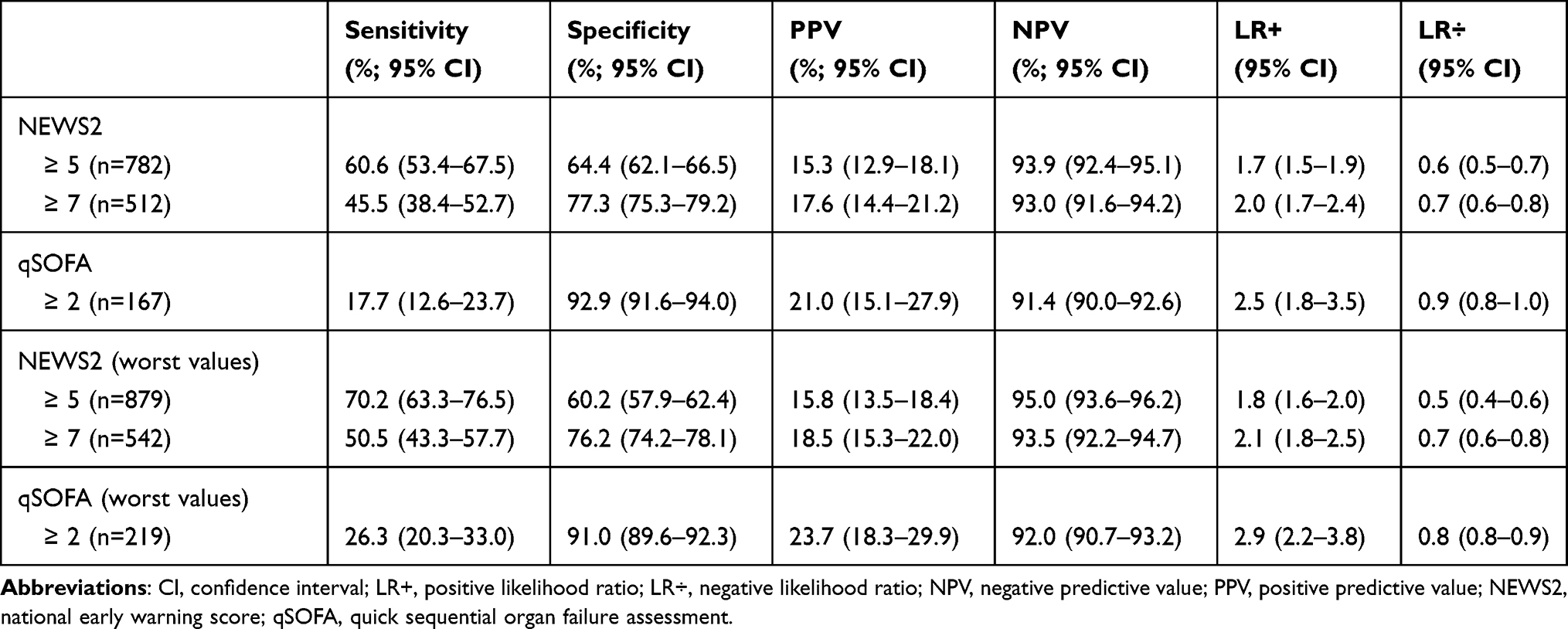 |
Table 4 Prognostic Accuracy of Different Sepsis Scores for a Composite Endpoint of In-Hospital Mortality or Transfer to Intensive Care Unit Using Baseline Clinical Values or Worst Clinical Values Within First Four Hours |
AUROC values were only slightly reduced after covariate adjustment (Table 5). The AUROC for NEWS2 (0.66; 0.62–0.70) was significantly higher than that for qSOFA (0.62; 0.58–0.66) (p=0.009).
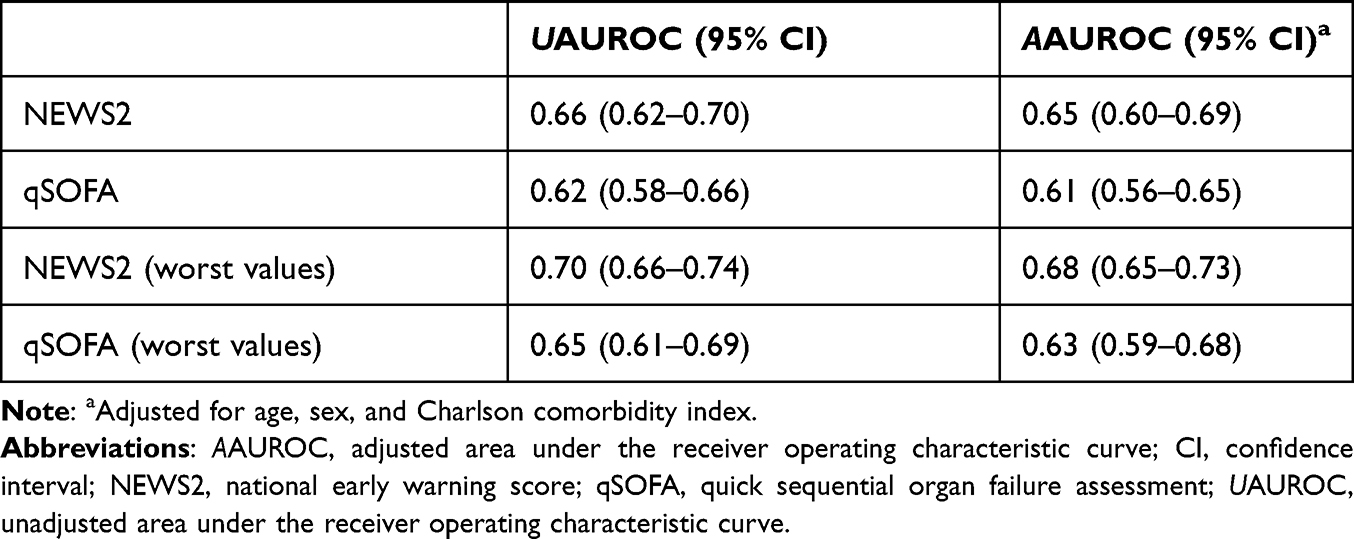 |
Table 5 Unadjusted and Adjusted Area Under Receiver Operating Characteristic Curves in Predicting the Composite Endpoint of In-Hospital Mortality or Transfer to Intensive Care Unit Using Baseline Clinical Values or Worst Clinical Values Within First Four Hours |
Prognostic Accuracy of the Scores Using Worst Clinical Values
The sensitivity for NEWS2 ≥5 and qSOFA ≥2 increased to 70.2% and 26.3%, respectively, when using the worst clinical variables (Table 4). The UAUROC (0.66) value for NEWS2 using admission variables significantly increased to 0.70 (0.66–0.74) (p<0.001) using the worst clinical values (Table 5). Similarly, the UAUROC value for qSOFA significantly increased from 0.62 to 0.65 (0.61–0.69) (p<0.001). The corresponding UAUROC curves are presented in Figure 2.
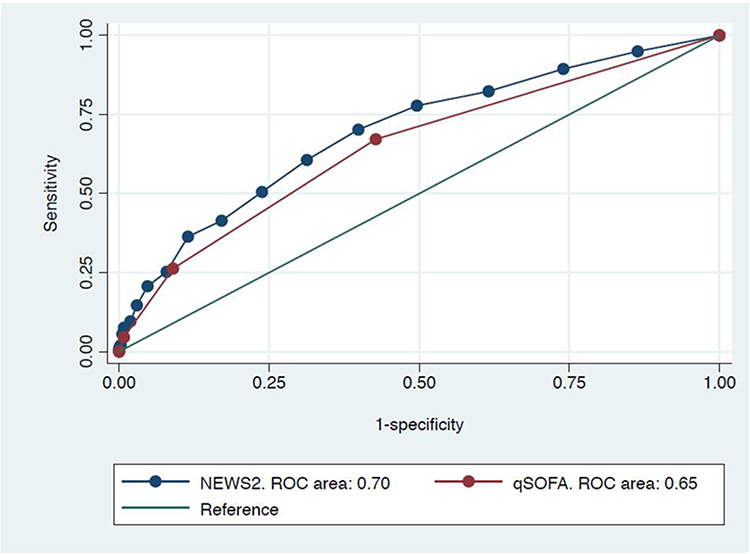 |
Figure 2 The area under the receiver operating characteristics (AUROC) curves. Abbreviations: NEWS2, national early warning score; qSOFA, quick sequential organ failure assessment; ROC, receiver operating characteristics. |
NO-AF
A total of 107 (5.2%) patients did not have ECG data. Patients without ECG data had a shorter length of stay than patients with admission ECG data (2.0 vs 4.6 days), and only two (1.9%) patients with missing ECG data achieved the composite endpoint.
A total of 80 (3.9%; 3.1–4.8%) patients developed NO-AF, and 38 (4.9%;3.5–6.6%) patients with suspected sepsis (NEWS2 ≥5) on admission had NO-AF upon ED arrival (Table 6). The number of patients with NO-AF was increased to 48 (5.5%; 4.1–7.2%) among all patients fulfilling the NEWS2 ≥5 criteria within the first 4 h. A total of 14 (29.2%; 16.6–44.1%) patients with NO-AF fulfilling the NEWS2 ≥5 criteria within the first 4 h had reached the composite endpoint; seven (14.6%; 6.1–27.8%) were transferred to the ICU, of whom one (14.3%; 0.4–57.9%) died. A total of seven (17.1%; 7.2–32.1%) non-ICU patients with NO-AF who fulfilled the NEWS2 ≥5 criteria within the first 4 h died during their stay.
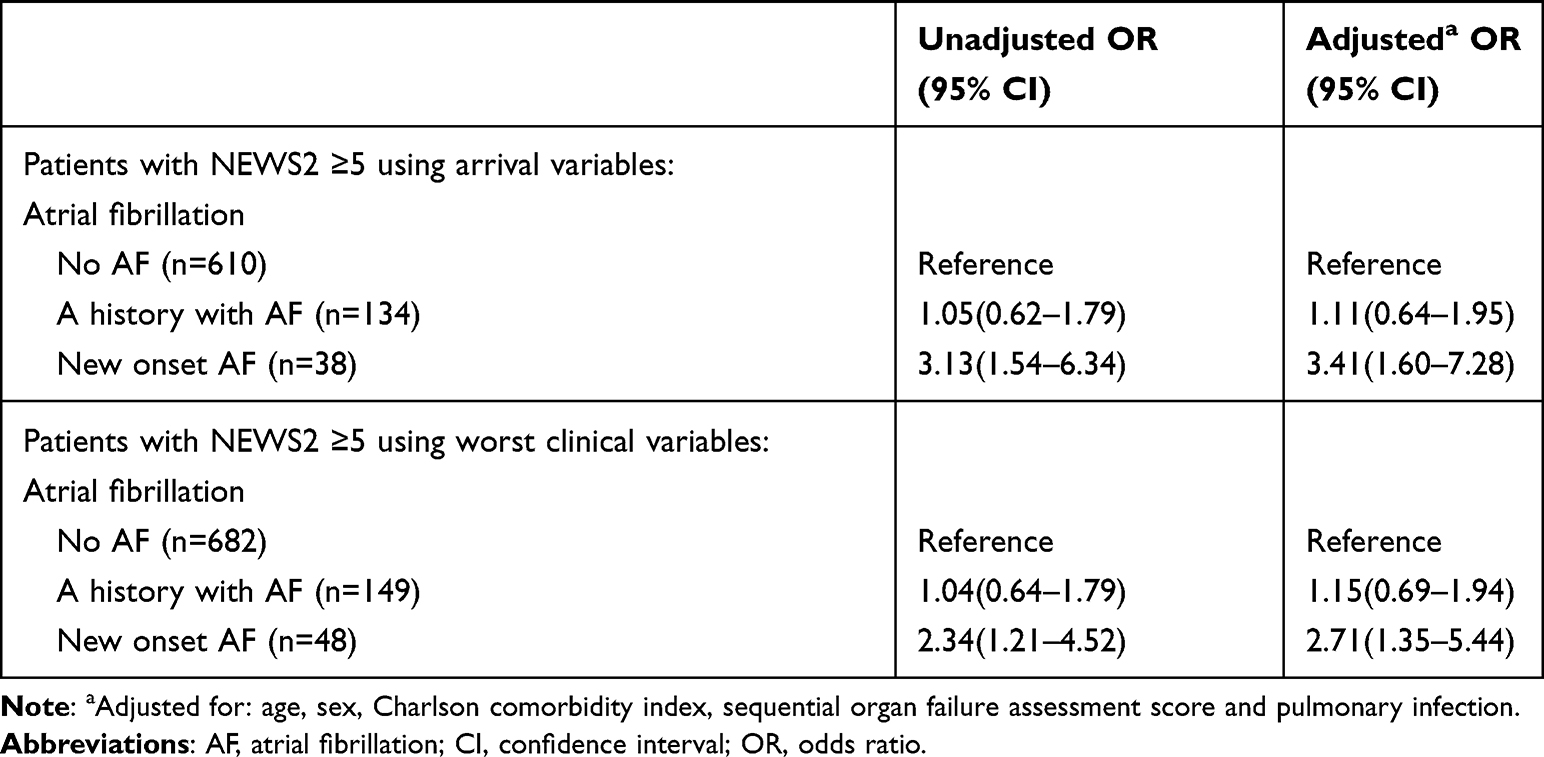 |
Table 6 Unadjusted and Adjusted Odds Ratios for the Composite Endpoint of In-Hospital Mortality or Transfer to the ICU in Patients with Suspected Sepsis (NEWS2 ≥5) Using Baseline Clinical Values or Worst Clinical Values Within First Four Hours to Identify Patients with Suspected Sepsis |
The adjusted ORs for achieving the composite endpoint of in-hospital mortality or transfer to the ICU in patients with NO-AF were 3.41 (1.60–7.28) and 2.71 (1.35–5.44) in patients fulfilling the NEWS2 ≥5 criteria on admission or within the first 4 h after admission, respectively (Table 6). A history of AF did not significantly increase the odds of the composite endpoint (Table 6).
Discussion
This study on the predictive performance of NEWS2 in predicting serious outcomes in unselected ED patients with suspected bacterial infectious diseases, found that almost 10% of patients achieved a composite endpoint of in-hospital mortality or transfer to the ICU. The sensitivity of NEWS2 ≥5 in predicting the composite endpoint was higher than that of qSOFA using clinical admission variables in the analyses. The sensitivity of NEWS2 and qSOFA increased using the worst clinical variables within the first 4 h after admission compared with admission variables. The discriminative ability of NEWS2 was better than that of qSOFA. However, the discriminative ability for both scores to predict the composite endpoint was poor.29 In patients with suspected sepsis (NEWS2 ≥5), the occurrence of NO-AF, in contrast to history with AF, was an independent determinant of transfer to the ICU or hospital death.
The available studies on vital signs in the ED mostly used single measurements only, mainly at triage. Vital signs may significantly change during the patient’s stay in the ED.30,31 Scoring systems based on a single registration of clinical parameters may have limited accuracy in predicting deterioration.32 Additionally, more than one in five patients presenting to the ED with suspected infection or sepsis deteriorate within 72 h from admission.31 Our data revealed that using clinical admission variables alone may result in flawed estimates of the prevalence of sepsis among ED patients and prognostic accuracy of the sepsis scores. Several patients without score positivity on admission deteriorated and achieved score positivity within the first 4 h of ED stay. Repeated vital sign measurements and sepsis scoring may potentially improve the scores and timely detection of sepsis.
NHS England has endorsed the updated NEWS2 to be the EWS used in acute care, including those with sepsis, in hospitals in England.5 The prognostic value of EW scores and quality of the available evidence have been discussed in reviews.6,7,33 A review by Nannan Panday et al showed that the NEWS was the best to predict mortality or ICU admission in the general ED population, and the modified EWS was the best in patients with suspected infection or sepsis.33 A meta-analysis and systematic review from 2018 of six studies on sepsis showed that EWSs have poor prognostic value in predicting mortality.6 However, it was also pointed out that the existing data have poor quality.6 A recent systematic review of universal EWS across all diseases and settings highlighted that the methodology and quality of validation studies of EWS are insufficient to recommend the use of EWS in all diseases and all clinical settings despite the good performance of EWS in some subgroups, such as patients with respiratory diseases.7 Studies of NEWS and qSOFA in sepsis have revealed a better predictive ability of NEWS.32,34–39 Notably, the studies have not shown a consistently high sensitivity, high specificity, and good discriminative performance for NEWS in predicting adverse outcomes. With lack of a superior method to determine deterioration and recognize sepsis, all hospitals and clinicians in England have been recommended the use of NEWS2 until a better EWS has been developed.40 The intermediary sensitivity and specificity value and the poor discriminative performance of NEWS2 in our study highlight the limitation of NEWS2 as a single clinical assessment scoring system for predicting adverse outcomes among ED patients with suspected bacterial infections. However, from our data, it is also clear that a single measurement of NEWS2 variables may have a limited value for predicting adverse outcomes. NEWS2 is easily calculable and suitable for automated computations. Electronic monitoring, computation, and calculation of NEWS2 during the the ED stay may be helpful to continuously flag clinically unstable patients with an increased risk of serious outcomes by allocating summed NEWS2 points to routine measurements of vital parameters.
NO-AF has been suggested as an additional sign of organ dysfunction in sepsis.20 A total of 5.5% of the patients in our study with NEWS2 ≥ 5 were diagnosed with NO-AF on admission. However, this is not the true incidence of NO-AF in patients with sepsis. We only examined the occurrence of NO-AF on ED admission. Several patients develop NO-AF during the following days after the admission.13 The incidence of the first episode of NO-AF has been described as 9%, 5%, and 4% on days 1, 2, and 3, respectively, and averaged < 1% thereafter in ICU patients with sepsis.13 The incidence of NO-AF in sepsis varies depending on the severity and is 8–10% in patients with sepsis,13,17 10–22% in patients with severe sepsis,13,17 and 23–46% in patients with septic shock,13,16,17 respectively. In a study based on administrative data, the incidence of NO-AF in discharged patients with sepsis was 7%.18
It is uncertain whether NO-AF independently has an impact on the outcome or is a marker of disease severity.11,13,15,19 Several studies have analyzed the association between sepsis and NO-AF.10,12,13,16,17,19 The studies were mainly performed among critically ill patients in ICU settings, using of old sepsis criteria, historical observational designs, and analyses based on administrative data, and many studies did not exclude patients with a known history of chronic or paroxysmal atrial fibrillation. Furthermore, the studies have been criticized for the lack of multivariate analyses to adjust for baseline differences.13,17,41 In our study, we adjusted for a wide range of potential confounders in an etiological study27 and found an independent association of NO-AF on ED admission, in contrast to a history of AF, and increased risk of achieving the composite endpoint of in-hospital mortality or transfer to the ICU. Our findings may indicate a causal effect27 of NO-AF on serious outcomes, and this information on NO-AF can contribute important information on the risk of adverse outcomes in patients with suspected bacterial infectious disease fulfilling the NEWS2 ≥5 criteria for sepsis.
Implications
Our study highlights the risk of erroneous conclusions regarding the utility of NEWS2 if studies on prognostic accuracy are based on few measurements, at worst only arrival variables. Future validation studies on NEWS2 should include an automated data-driven real-time alert system that is continuously able to identify patients with sepsis and the risk of adverse outcomes. ECG monitoring for the detection of NO-AF indicative of organ dysfunction should be included in the alert system and examined to determine if scoring for NO-AF added to the NEWS2 score can enhance the prognostic accuracy of the NEWS2 score.
The pathophysiological mechanism of NO-AF13,15–17,41 and how NO-AF may increase the risk of death13,17,19 is complex and not well defined. The role of NO-AF as a determinant of adverse outcomes in sepsis and interventional strategies with a potential effect on outcomes, should also be explored in further studies.
In the absence of a highly sensitive and specific diagnostic clinical test, it may also be relevant to examine the value of different biomarkers. Meta-analyses have examined more than 200 biomarkers for the early identification of patients with sepsis.42,43 However, the precise role of these biomarkers has not been defined. With rapid technological advancement within the point-of-care diagnostic tests, it may be interesting to examine whether the measurement of biomarkers, such as procalcitonin and mid-Regional pro-adrenomedullin, as point-of-care tests can improve the prognostic accuracy of the different bedside clinical scores.44 There is also promising research in the development of host-based molecular assays to detect sepsis at an early stage.45 A combination of clinical bedside scores, biomarkers, and assay techniques could be a direction for new clinical studies. This may be a potential way to increase the diagnostic test performance in the early identification of patients with sepsis.
Strengths and Limitations
The risks of selection and referral bias were minimized. This study was based on a prospective observational cohort study with the consecutive inclusion of all patients admitted with suspected bacterial infections. All patients admitted to the ED during the 6-month period were evaluated for inclusion. The study design ensured that patients fulfilling the inclusion criteria were included. All acute patients from the uptake area were referred to our ED.
This study has some limitations. First, data on deterioration in the ED after 4 h were not included in the analyses. An extension of the registration period and continuous automated registration of the parameters and EWS scoring could have identified more patients with sepsis and potentially enhanced the prognostic accuracy results. Second, the study was not designed to capture all patients with NO-AF because only the arrival ECG findings were analyzed for arrhythmias. Third, a few patients were excluded due to missing data. We believe that the amount of missingness was too small to have an impact on the estimates. However, ECG information was missing in 5% of the patients. These patients had a better prognosis than patients with ECGs’. Patients with missing ECG data were handled in the analyses as those without documented NO-AF. Bias due to misclassification of these patients may have distorted the estimates. Fourth, sepsis treatment was primarily guided by a sepsis treatment protocol for patients fulfilling the qSOFA ≥2 criteria, SIRS ≥2 criteria or if the patients were critically ill. Some patients with sepsis identified by the NEWS2 criteria in our study may not have fulfilled the qSOFA and SIRS criteria. Therefore, sepsis treatment may have been opted-out in patients only fulfilling the NEWS2 criteria. The extent to which this may have affected the outcomes in patients only fulfilling the NEWS2 criteria is challenging to clarify owing to the observational design and risk of bias. Fifth, following conflicting data on the usefulness of qSOFA identifying patients with sepsis and septic shock,3 it might have been relevant to compare NEWS2 with repeated measurements of SIRS and SOFA in the present study. However, laboratory tests were not routinely repeated during the first hour of the ED stay. Consequently, it was not possible to analyze changes in the SOFA and SIRS scores during the first 4 h stay in the ED for comparison purposes. Sixth, adding the NO-AF variable to the NEWS2 scoring system to examine whether a combination of variables could improve the prognostic value of NEWS2 was not tested and should be examined in future studies.
Finally, this was a single-center study, which may have affected the generalizability of the results.
Conclusion
NEWS2 had a higher sensitivity but lower specificity than qSOFA in predicting a composite endpoint of in-hospital mortality or transfer to the ICU in ED patients with suspected bacterial infection. However, the discriminative ability of NEWS2 in predicting adverse outcomes is poor. NO-AF, but not history of AF, contributed important prognostic information.
Abbreviations
AAUROC, adjusted area under receiver operating curve; AB, antibiotics; AF, atrial fibrillation; AUROC, area under receiver operating curve; CCI, Charlson comorbidity index; CI, confidence intervals; ECG, electrocradiogram; ED, emergency department; EWS, early warning score; GCS, Glasgow Coma Scale; ICU, intensive care unit; IQR, interquartile range; IV, intravenous; LR+, positive likelihood ratio; LR÷, negative likelihood ratio; NO-AF, new-onset atrial fibrillation; NPV, negative predictive value; OR, odds ratio; qSOFA, quick sequential organ failure assessment; NEWS, new early warning score; PPV, positive predictive value; SIRS, systemic inflammatory response syndrome; SOFA, sequential organ failure assessment; UAUROC, unadjusted area under receiver operating curve; WBC, white blood cell count.
Declarations
Data on new-onset atrial fibrillation have previously been presented (abstract) at Danish Emergency Medicine Conference 2019, Aarhus, Denmark. https://tidsskrift.dk/akut/article/view/112938.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was reported to The Danish Data Protection Agency (REG-105-2017). The data accessed complied with relevant data protection and privacy regulations. The study was on the 16th of May 2017 defined as a quality project by the Secretariat of the Committee on Health Research Ethics of Region Zealand. Therefore, it is not covered by the Committee Act and is not obligated to report for the ethics committee system. Administrative permission to access the data was acquired on September 25, 2018 from the head of the Slagelse Hospital Administration. The data were anonymized.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This project received financial support from the Region Zealand Health Research Foundation, Naestved, Slagelse and Ringsted Hospitals Research Fund, and the Department of Emergency Medicine, Bispebjerg and Frederiksberg Hospital, Denmark.
Disclosure
The authors declare that they have no competing interests.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
2. Abdullah SM, Sørensen RH, Nielsen FE. Prognostic accuracy of SOFA, qSOFA, and SIRS for mortality among emergency department patients with infections. Infect Drug Resist. 2021;14:2763–2775. doi:10.2147/IDR.S304952
3. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
4. Williams B, Alberti G, Ball C, et al. National Early Warning Score (NEWS): Standardizing the Assessment of Acute-Illness Severity in the NHS. London: Royal College of Physicians; 2012.
5. Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the Assessment of Acute-Illness Severity in the NHS. Updated Report of a Working Party. London: Royal College of Physicians; 2017.
6. Hamilton F, Arnold D, Baird A, Albur M, Whiting P. Early warning scores do not accurately predict mortality in sepsis: a meta-analysis and systematic review of the literature. J Infect. 2018;76(3):241–248. doi:10.1016/j.jinf.2018.01.002
7. Alhmoud B, Bonnici T, Patel R, Melley D, Williams B, Banerjee A. Performance of universal early warning scores in different patient subgroups and clinical settings: a systematic review. BMJ Open. 2021;11:e0458849. doi:10.1136/bmjopen-2020-045849
8. Xiao FP, Chen MY, Wang L, et al. Outcomes of new-onset atrial fibrillation in patients with sepsis: a systematic review and meta-analysis of 225,841 patients. Am J Emerg Med. 2021;42:23–30. doi:10.1016/j.ajem.2020.12.062
9. McIntyre WF, Um KJ, Cheung CC, et al. Atrial fibrillation detected initially during acute medical illness: a systematic review. Eur Heart J. 2019;8(2):130–141. doi:10.1177/2048872618799748
10. Bosch NA, Cohen DM, Walkey AJ. Risk factors for new-onset atrial fibrillation in patients with sepsis: a systematic review and meta-analysis. Crit Care Med. 2019;47:280–287. doi:10.1097/CCM.0000000000003560
11. Arrigo M, Ishihara S, Feliot E, et al. New-onset atrial fibrillation in critically ill patients and its association with mortality: a report from the FROG-ICU study. Int J Cardiol. 2018;266:95–99. doi:10.1016/j.ijcard.2018.03.051
12. Shahreyar S, Fahhoum R, Akinsey O, Bhandari S, Dang G, Khouzam RN. Severe sepsis and cardiac arrhythmias. Ann Transl Med. 2018;6(1):6. doi:10.21037/atm.2017.12.26
13. Klein Klouwenberg PMC, Frencken JF, Kipers S, et al. Incidence, predictors, and outcomes of new-onset atrial fibrillation in critically ill patients with sepsis. A cohort study. Am J Respir. 2017;195(2):1–22. doi:10.1164/rccm.201603-0618OC
14. Moss TJ, Calland JF, Enfield KB, et al. New-onset atrial fibrillation in the critically ill. Crit Care Med. 2017;45:790–797. doi:10.1097/CCM.0000000000002325
15. Shaver CM, Chen W, Janz DR, et al. Atrial fibrillation is an independent predictor of mortality in critically ill patients. Crit Care Med. 2015;43(10):2104–2111. doi:10.1097/CCM.0000000000001166
16. Meierhenrich R, Steinhilber E, Eggermann C, et al. Incidence and prognostic impact of new-onset atrial fibrillation in patients with septic shock: a prospective observational study. Critical Care. 2010;14:R108. doi:10.1186/cc9057
17. Kuipers S, Klein Klouwenberg PMC, Cremer OL. Incidence, risk factors and outcomes of new-onset atrial fibrillation in patients with sepsis: a systematic review. Critical Care. 2014;18(6):688. doi:10.1186/s13054-014-0688-5
18. Walkey AJ, Hammill BG, Curtis LH, Benjamin EJ. Long-term outcomes following development of new-onset atrial fibrillation during sepsis. Chest. 2014;146(5):1187–1195. doi:10.1378/chest.14-0003
19. Walkey AJ, Wiener RS, Ghobrial JM, Curtis LH, Benjamin EJ. Incident stroke and mortality associated with new-onset atrial fibrillation in patients hospitalized with severe sepsis. JAMA. 2011;306(20):2248–2254. doi:10.1001/jama.2011.1615
20. Bosch NA, Massaro JM, Winter MR. New-onset atrial fibrillation as a sepsis-defining organ failure. AnnalsATS. 2019;16(10):1332–1334. doi:10.1513/AnnalsATS.201902-176RL
21. Abdullah SM, Sørensen RH, Dessau R, Sattar SM, Wiese L, Nielsen FE. Prognostic accuracy of qSOFA in predicting 28-day mortality among infected patients in an emergency department: a prospective validation study. Emerg Med J. 2019;36(12):722–728. doi:10.1136/emermed-2019-208456
22. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;Volume 11:563–591. doi:10.2147/CLEP.S179083
23. The Danish Society for Patient Safety. The Danish Safer Hospital Programme. Early detection of sepsis/Patientsikkert Sygehus. Tidlig Opsporing Af Sepsis [In Danish]. Version 2013-06-10. Available from https://docplayer.dk/14119250-Tidlig-opsporing-af-sepsis-juni-2013.html.
24. Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. doi:10.1097/CCM.0b013e31827e83af
25. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
26. Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29:541–549. doi:10.1007/s10654-014-9930-3
27. van Diepen M, Ramspek CL, Jager KJ, Zoccali C, Dekker FW. Prediction versus aetiology: common pitfalls and how to avoid them. Nephrol Dial Transplant. 2017;32:ii1–ii5. doi:10.1093/ndt/gfw459
28. Janes H, Pepe MS. Adjusting for covariates in studies of diagnostic, screening, or prognostic markers: an old concept in a new setting. Am J Epidemiol. 2008;168:89–97. doi:10.1093/aje/kwn099
29. Fischer JE, Bachmann LM, Jaeschke R. A readers’ guide to the interpretation of diagnostic test properties: clinical example of sepsis. Intensive Care Med. 2003;29:1043–1051. doi:10.1007/s00134-003-1761-8
30. Quinten VM, van Meurs M, Ter Maaten JC, Ligtenberg JJ. Trends in vital signs and routine biomarkers in patients with sepsis during resuscitation in the emergency department: a prospective observational pilot study. BMJ Open. 2016;6(5):e009718. doi:10.1136/bmjopen-2015-009718
31. Quinten VM, van Meurs M, Olgers TJ, et al. Repeated vital sign measurements in the emergency department predict patient deterioration within 72 hours: a prospective observational study. Scand J Trauma Resusc Emerg Med. 2018;26:57. doi:10.1186/s13049-018-0525-y
32. Almutary A, Althunayyan S, Alenazi K, et al. National Early Warning Score (NEWS) as prognostic triage tool for septic patients. Infect Drug Resist. 2020;13:3843–3851. doi:10.2147/IDR.S275390
33. Nannan Panday RS, Minderhoud TC, Alam N, Nanayakkara PWB. Prognostic value of early warning scores in the emergency department (ED) and acute medical unit (AMU): a narrative review. Eur J Intern Med. 2017;45:20–31. doi:10.1016/j.ejim.2017.09.027
34. Kovach CP, Fletcher GS, Rudd KE, Grant RM, Carlbom DJ. Comparative prognostic accuracy of sepsis scores for hospital mortality in adults with suspected infection in non-ICU and ICU at an academic public hospital. PLoS One. 2019;14(10):e0224780. doi:10.1371/journal.pone.0224780
35. Mellhammar L, Linder A, Tverring J, et al. NEWS2 is superior to qSOFA in detecting sepsis with organ dysfunction in the emergency department. J Clin Med. 2019;8(8):1128. doi:10.3390/jcm8081128
36. Brink A, Alsma J, Verdonschot RJ, et al. Predicting mortality in patients with suspected sepsis at the Emergency Department; a retrospective cohort study comparing qSOFA, SIRS and National Early Warning Score. PLoS One. 2019;14(1):e0211133. doi:10.1371/journal.pone.0211133
37. Usman AO, Usman AA, Ward MA. Comparison of SIRS, qSOFA, and NEWS for the early identification of sepsis in the emergency department. Am J Emerg Med. 2019;37(8):1490–1497. doi:10.1016/j.ajem.2018.10.058
38. Goulden R, Hoyle M, Monis J, et al. qSOFA, SIRS and NEWS for predicting in-hospital mortality and ICU admission in emergency admissions treated as sepsis. Emerg Med J. 2018;35:345–349. doi:10.1136/emermed-2017-207120
39. Churpek MM, Snyder A, Han X, et al. Quick sepsis-related organ failure assessment, systemic inflammatory response syndrome, and early warning scores for detecting clinical deterioration in infected patients outside the intensive care unit. Am J Respir Crit Care Med. 2017;195(7):906–911. doi:10.1164/rccm.201604-0854OC
40. Inada-Kim NE, Nsutebu E. Views and reviews. NEWS 2: an opportunity to standardize the management of deterioration and sepsis. BMJ. 2018;360:k1260. doi:10.1136/bmj.k1260
41. Gandhi S, Litt D, Narula N. New-onset atrial fibrillation in sepsis is associated with increased morbidity and mortality. Neth Heart J. 2015;23:82–88. doi:10.1007/s12471-014-0641-x
42. Pierrakos C, Velissaris D, Bisdorff M, Marshall JC, Vincent JL. Biomarkers of sepsis: time for a reappraisal. Crit Care. 2020;24(1):287. doi:10.1186/s13054-020-02993-5
43. Liu Y, Hou JH, Li Q, Chen KJ, Wang SN, Wang JM. Biomarkers for diagnosis of sepsis in patients with systemic inflammatory response syndrome: a systematic review and meta-analysis. Springerplus. 2016;5(1):2091. doi:10.1186/s40064-016-3591-5
44. Spoto S, Nobile E, Carnà EPR, et al. Best diagnostic accuracy of sepsis combining. SIRS criteria or qSOFA score with Procalcitonin and Mid-Regional pro-Adrenomedullin outside ICU. Sci Rep. 2020;10(1). doi:10.1038/s41598-020-73676-y
45. Ullrich E, Heidinger P, Soh J, et al. Evaluation of host-based molecular markers for the early detection of human sepsis. J Biotechnol. 2020;310:80–88. doi:10.1016/j.jbiotec.2020.01.013
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.