Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Narrative Review: Pathogenesis of the Inflammatory Response and Intestinal Flora in Depression
Authors Zeng JW ![]() , Zhao JL, Han ZJ, Duan YJ, Lin L
, Zhao JL, Han ZJ, Duan YJ, Lin L ![]()
Received 13 July 2023
Accepted for publication 26 October 2023
Published 16 November 2023 Volume 2023:19 Pages 2469—2483
DOI https://doi.org/10.2147/NDT.S430444
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Roger Pinder
Jia-Wei Zeng,1,2 Juan-Li Zhao,1 Zhen-Jie Han,1 Yan-Jun Duan,2 Li Lin1
1Laboratory of Medical Molecular and Cellular Biology, College of Basic Medical Sciences, Hubei University of Chinese Medicine, Wuhan, 430065, People’s Republic of China; 2Department of Anatomy Teaching and Research, College of Basic Medical sciences, Hubei University of Chinese Medicine, Wuhan, 430065, People’s Republic of China
Correspondence: Li Lin, Laboratory of Medical Molecular and Cellular Biology, College of Basic Medical sciences, Hubei University of Chinese Medicine, No. 16 of Huangjia Lake Western Road, HongShan District, Wuhan, 430065, People’s Republic of China, Tel +86 27 68890123, Fax +86 27 68890029, Email [email protected] Yan-Jun Duan, Department of Anatomy Teaching and Research, College of Basic Medical sciences, Hubei University of Chinese Medicine, No. 16 of Huangjia Lake Western Road, HongShan District, Wuhan, 430065, People’s Republic of China, Tel +86 27 68890047, Fax +86 27 68890029, Email [email protected]
Abstract: Depression, as a common mental illness that is often accompanied by suicidal and homicidal behaviors, is one of the most important diseases in the medical field that requires urgent attention. The pathogenesis of depression is complex, and the current therapeutic drugs such as tricyclic antidepressants (TCAs), monoamine oxidase inhibitors, and secondary serotonin reuptake inhibitors have certain shortcomings. The inflammatory factor hypothesis, one of the pathogenesis of depression, suggests that inflammatory response is a key factor leading to the occurrence and development of depression, and that overactivation of inflammatory factors such as NLRP3, Toll-like receptor 4, and IDO leads to immune-system dysfunction and depression. The other pathogenic hypothesis, the gut flora hypothesis, has also been the focus of recent research. The gut flora may work together with inflammatory factors to cause depression. The approach to treating depression has been by altering the gut flora through drugs or probiotics. However, effective and clear treatment methods are lacking. In this study, by exploring the involvement of intestinal flora and inflammatory factors in the pathogenesis of depression, we found that improving the intestinal flora can affect inflammatory factors and, therefore, provide research ideas for the development of novel drugs to treat depression.
Keywords: depression, pathogenesis, inflammation, inflammatory factors, intestinal flora, therapeutic drugs
Introduction
Depression is a common mental disorder that clinically manifests in patients as low mood, negative and pessimistic emotions, inability to concentrate, gradual decline in memory, slow thinking, slow response, high alertness, cognitive distortion, and sleep disorders, as well as fatigue and other physical symptoms. Of late, the incidence of depression has been increasing annually and has affected 10% of the global population.1 According to the Global Burden of Disease, there has been a 27.6% increase in anxiety and depression worldwide since the COVID-19 outbreak in 2020.2 In 2019, 280 million people worldwide suffered from depression; an additional 70 million people were diagnosed in 2022. More than 350 million people worldwide currently suffering from depression. In China, the incidence of depression is as high as 6% and the lifetime prevalence rate is 6.8%. The number of people affected by depression is as high as 95 million,3 and the disease is expected to result in the highest disease burden globally by the year 2030. Depression is characterized by high rates of morbidity, recurrence, suicide, and disability, as well as high costs.4 Although many scholars are committed to the study of depression, its pathogenesis and causes are still unclear. Research data indicate that the pathogenesis of depression is related to many factors, such as biological factors, mainly including genetic (mostly depression-related genes5), neurobiochemical, regeneration, and other aspects. Another example is social and psychological factors, which mainly include social and cultural environment, economic conditions, and the impact of negative emotions. These factors often do not lead to the occurrence of depression alone, but rather interact with each other and play an important role in the occurrence and development of depression. Depression affects the health of patients and reduces their quality of life. In serious cases, dangerous behaviors such as suicide and homicide are possible, which pose a serious threat to patients’ as well as others’ life and safety, resulting in a great burden to the family and society. Recent research on the causes of depression involves numerous scholars elucidating the relationship between the inflammatory response and the pathogenesis of depression, namely, the inflammatory mechanism hypothesis of depression. The study of depression based on the relationship between intestinal flora and inflammation is now a current hotspot and the specific response mechanism has not yet been thoroughly studied.6 Taking the inflammation hypothesis as a starting point, this review briefly elaborates on the mechanism of inflammation affecting the onset of depression and presents the relationship between inflammation and other hypotheses, focusing on the relationship between inflammatory response, intestinal flora, and depression, thereby providing a reference for the early prevention, diagnosis, and treatment of depression.
Pathogenesis of Depression
Based on the above-mentioned factors related to the pathogenesis of depression, the possible pathogeneses mediated by numerous hypotheses related to the onset of depression have been widely studied by scholars worldwide. A common hypothesis includes that of monoamine neurotransmitters and their receptors, which suggests that depression is related to the depletion of neurotransmitters such as 5-hydroxytryptamine (5-HT), dopamine (DA), and norepinephrine.7 This hypothesis has received considerable support, but it attempts to provide a pathophysiological explanation for the action of antidepressants and does not provide a complete explanation for the action of antidepressants. Moreover, the pathophysiology of depression itself is still unknown; thus, the key questions have not been resolved for many years.8 The hypothalamus–pituitary–adrenal (HPA) axis dysfunction hypothesis was proposed, and hyperfunction of the HPA axis was indicated to cause depression.9–11 Although this hypothesis articulates the possible mechanism and pathways of depression, the mechanism of action of the HPA axis is complex and it is often difficult to determine whether the overactivity of the HPA axis is a cause or a consequence of the disease.9 The neuroplasticity and neurotrophic factor hypothesis suggests that depression is associated with neuroplasticity disorder and reduced levels of neurotrophic factors.12 This hypothesis stipulates disrupted neurotrophic support as the key mechanism underlying major depressive disorder (MDD)-related synaptic and brain-related alterations.13 According to the inflammatory and cytokine hypothesis, the immune inflammatory response plays an important role in the pathogenesis of depression; thus, a close relationship between them is proposed. As early as in the 90s, Maes et al examined the relationship between inflammation and depression, which now provides evidence for the inflammatory and cytokine hypothesis.14 The intestinal flora–imbalance hypothesis holds that changes in the intestinal flora may lead to the occurrence of depression.15 The gut flora also influences other factors in the development of depression, such as the HPA axis, neurotrophic factor, and inflammation. The pathogenesis of depression is extremely complex. Although several hypotheses have been proposed, the elucidation of its pathogenesis varies, and the mechanism underlying its pathogenesis is still inconclusive.
Inflammatory Cytokine Hypothesis
Depression is often accompanied by inflammation during its occurrence and development, and immune-inflammatory reactions play an important role in its pathogenesis. The inflammatory hypothesis holds that the body releases inflammatory cytokines to activate peripheral immunity, causing overactivation of neuroendocrine and immune systems and further dysfunction, ultimately leading to depression.16 Inflammatory cytokines, also known as inflammatory factors, include all cytokines involved in the inflammatory response, including interleukins (ILs), interferon (IFN), colony-stimulating factor, and tumor necrosis factor (TNF). Cytokines can be divided into pro-inflammatory and anti-inflammatory cytokines according to their roles. The former acts on the body, inducing the production of pro-inflammatory cytokines and promoting cellular immune response, such as by increasing the levels of IL-1, IL-2, IFN-α, TNF-α, and TNF-β. The latter protects against immune responses by inhibiting cell activation and regulating the production of inflammatory cytokines including IL-4, IL-10, and IL-13.
As for the mechanism of the influence of inflammatory response on the onset of depression, many studies have focused on activation of the NLRP3 inflammasome, influence of the Toll-like receptor (TLR)4 receptor on neuroinflammation, and overexpression of indoleamine-2,3-dioxygenase (IDO). Currently, the antidepressant effect of different drugs with anti-inflammatory effects strengthens the current knowledge of the implication of inflammation in the pathogenesis of depression. For example, depression is accompanied by peripheral immunization, which, in turn, causes structural and functional changes in the brain.17,18 It is clear that treatment of inflammation is important in treating depression.
Role of NLRP3 Inflammatory Corpuscles in Depression
The NLRP3 inflammasome is a multidomain protein complex derived from NLR, which is an important factor involved in innate immunity. It is also a mediator of inflammatory factors in the IL-1β–associated central nervous system (CNS) and includes the NLRP3 protein, adaptor protein apoptosis–associated spot-like protein ASC, and effector protein Caspase-1. NLRP3 activation plays an important role in the pathogenesis of depression,19–21 and NLRP3 bodies are considered to be one of the potential inflammatory indicators of depression.22 The activation of NLRP3 promotes pro-Caspase-1 cleavage, activates the effector protein Caspase-1, cleaves and activates IL-1β and IL-18, and then activates the downstream signal transduction pathway to produce numerous inflammatory mediators. The activation of NLRP3 also induces microglia to synthesize and release inflammatory mediators and mediate inflammatory responses, eventually leading to changes in neurotransmitters, followed by the occurrence of depression-like behaviors in the brain.23,24 (Please see the blue line in Figure 1) Several years ago, it was found that the levels of inflammatory factors, such as IL-1β, in the cerebrospinal fluid25 and serum26 of patients with depression were significantly increased and positively correlated with the severity of depression. Alcocer Gomez et al27 analyzed the peripheral blood mononuclear cells in patients with severe depression and found that the mRNA expression of NLRP3 and Caspase-1 in these patients were significantly higher than those in normal people, and their levels were significantly higher than those of healthy individuals. Wang et al28 and Zhou et al29 confirmed that IL levels as well as the levels of other inflammatory cytokines such as TNF-α were elevated in the serum of patients with depression through the induction of IL-1β or IL-18 autocrine or parasecreted mechanisms. More than a decade ago, the severity of depressive symptoms was found30 to be closely related to the level of plasma cytokines. In conclusion, neuroinflammatory response is an important link in the pathogenesis of depression and the NLRP3 inflammasome plays a key role in the neuroinflammatory response.
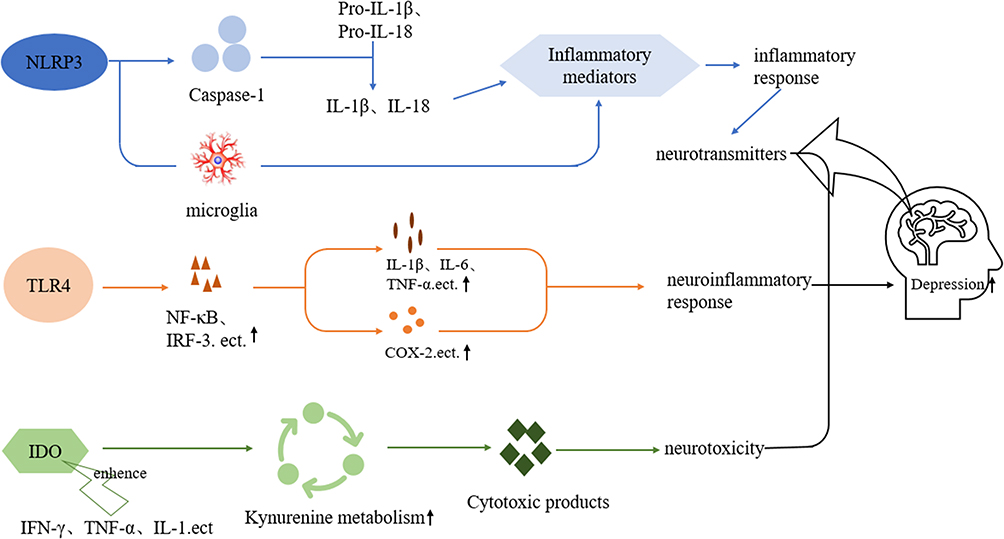 |
Figure 1 NLRP3 activation induces the cleavage of pro-Caspase-1, activates the effector protein Caspase-1, shears and activates interleukin (IL)-1β and IL-18, and activates the downstream signaling pathways to produce inflammatory mediators; NLRP3 activation induces microglia to synthesize and release inflammatory mediators, which induce inflammatory responses and ultimately lead to neurotransmitter changes in the brain and depressive-like behaviors. (Blue line) TLR4 is ultimately involved in the neuroinflammatory response by promoting the expression of transcription factors such as nuclear transcription factor-kappa-B (NF-κB) and interferon regulatory factor 3, which, in turn, induce the production and release of inflammatory factors such as IL-1β, IL-6, and tumor necrosis factor (TNF)-α, and also upregulate the expression of proteins such as cyclooxygenase-2. (Orange line) IDO is overactivated and the kynurenine metabolic pathway is enhanced, producing several cytotoxic products that cause neurotoxicity and ultimately lead to neurological disorders such as depression. Inflammatory factors such as interferon-γ, TNF-α, and IL-1 also augment the overexpression of IDO. (Green line). |
Role of the TLR4 Receptor in Depression
TLR4 is an autoimmune pattern recognition receptor present on the surface of cell membranes and is capable of recognizing various extracellular endogenous damage-related molecular patterns, microbial-related molecular patterns, and pathogen-related molecular patterns. It can affect the onset of depression through neuroinflammatory signaling pathways. Studies31 have found that TLR4 expression in the peripheral blood mononuclear cells of individuals who are depressed is significantly higher and that its expression is reduced significantly after treatment compared with that in healthy individuals, indicating the role of TLR4 in the pathogenesis of depression. TLR4 also affects the neuroinflammatory response and plays an important role in the neuropathic process of certain neurodegenerative diseases. With the proposed inflammatory hypothesis of depression, Li et al32 confirmed that TLR4 was fully involved in the pathogenesis of depression. TLR4 induces the generation and release of inflammatory factors such as IL-1β, IL-6, and TNF-α by promoting the expression of transcription factors including nuclear transcription factor-kappa B (NF-κB) and interferon regulatory factor 3, and also upregulates the expression of proteins such as cyclooxygenase-2 (COX-2), ultimately participating in the neuroinflammatory response.33,34 (Please see the orange line in Figure 1) Li et al35 found through animal experiments that stimulating the TLR4 receptors by lipopolysaccharides in animals leads to depression-like behaviors such as low interest, anhedonia, and loss of appetite. Hung et al36 found that the expression of TLR3, TLR4, TLR5, TLR7, and TLR9 increases in the peripheral blood of patients with depression and returns to normal levels after effective treatment; however, TLR4 and TLR6 levels decrease to lower than normal levels. Moreover, the activation of TLR4 in the brain is involved in the pathogenesis of depression. Studies also have found that TLR4 is overexpressed in the brains of depressed rats.37,38 Using positron emission computed tomography, Huang et al34 found that microglia were overactivated in the hippocampi of patients who were depressed, and TLR4 was mainly expressed in these cells in the brain. In conclusion, TLR4 is involved in the occurrence and development of depression by participating in the inflammatory response.
Role of IDO in Depression
IDO, as a rate-limiting enzyme, is widely present in human tissues, where it promotes the metabolism and decomposition of tryptophan (TRP) and kynurenine. Recent studies have found that IDO is closely related to cytokines, neuronal plasticity, and other factors, and plays an important role in the pathogenesis and treatment of depression.39 The overexpression of IDO is a key mechanism of inflammation that leads to depression.40 When IDO is overactivated, the metabolic pathway of uric acid in canines is enhanced and cytotoxic products such as kynurenine and quinolinic acid are produced, which result in neurotoxicity and, eventually, neurological diseases.39,40 Pro-inflammatory factors such as IFN-γ, TNF-α, and IL-1 can enhance the overexpression of IDO. (Please see the green line in Figure 1) IFN-γ is one of the most powerful induction factors. The induction ability of IFN-γ can be enhanced by TNF-α, IFN-α, IL-1, and other pro-inflammatory factors.40–42 Studies have shown that IDO levels are the highest in the prefrontal lobe, hippocampus, and other regions of the brain, and pro-inflammatory factors can increase the expression of IDO mRNA in the microglia in these regions.43,44 IDO activation can be partially blocked by the action of pro-inflammatory factor antagonists, such as TNF-α antagonists. Some receptor genes of pro-inflammatory factors can also be knocked out to block IDO overactivation, thus blocking the generation of depression-like behaviors.45 Animal experiments reveal that anti-inflammatory factors such as IL-1046 can protect nerves by inhibiting the activation of IDO mRNA. In summary, IDO overexpression can be reduced by inhibiting the activity of pro-inflammatory factors or promoting the activation of anti-inflammatory factors, which ultimately reduce the onset of depression-like behaviors.
Correlation Between Depression-Related Inflammatory Factors and Other Hypotheses
The inflammatory response is accompanied by the occurrence and development of depression and continues throughout. Inflammatory factors can affect neurons, eg, neuronal degeneration (especially in the hippocampus) and play an important role in the process of neurogenesis. As an important cause of depression, inflammation also contributes to the occurrence of depression by participating in the other hypothesized mechanisms.
Relationship Between Inflammatory Factors and Monoamine Neurotransmitters
The decrease in the levels of monoamine neurotransmitters, such as 5-HT and DA, is an important factor in the onset of depression. 5-HT is generated from TRP; thus, the content of TRP is crucial in the synthesis of 5-HT. IDO is excessively activated during inflammation, leading to the decomposition of large amounts TRP; moreover, the reduction in 5-HT synthesis ultimately leads to a reduction of 5-HT content.40 DA synthesis is also affected by inflammatory factors. The rate-limiting enzyme in DA synthesis is phenylalanine hydroxylase, which catalyzes the reaction to yield DA. Animal experiments47 have shown that the cofactor of this enzyme, tetrahydrobiotrexate, is reduced by the inflammatory factor IFN-α, which results in reduced DA synthesis.
Relationship Between Inflammatory Factors and the HPA Axis
Neuroendocrine abnormalities of the HPA axis play a very important role in the pathogenesis of depression. Individuals suffering from depression who exhibit suicidal tendencies have elevated levels of hydroxycorticosteroids, which are major breakdown products of cortisol.10 In the HPA axis, the hypothalamus produces corticotropin-releasing hormone (CRH), which acts on the pituitary gland to secrete adrenocorticotropic hormone (ACTH) and ultimately affects the adrenocortical secretion of glucocorticoids. Long-term stress in humans leads to abnormal functioning of the glucocorticoid receptor (GR), resulting in reduced binding of hormones to receptors; the reduced expression of the receptor eventually overactivates the inflammatory response, which then aggravates the functional abnormality of GRs through certain signaling pathways after activation of the inflammatory response. Researchers40 injected the inflammatory factors IL-6 and TNF-α into the brains of depressed rats and found that they had an excitatory effect on the hypothalamus, could activate CRH neurons, promote ACTH release, and affect the release of glucocorticoids and activate the HPA axis.
Association of Inflammatory Cytokines with Brain-Derived Neurotrophic Factor (BDNF)
BDNF is synthesized in neurons and is widely present in the CNS, with the highest levels in the hippocampus and cortex. BDNF is involved in neuroplasticity and repair of stressed nerve injury. After binding with receptor tyrosine hydroxylase B (TrkB), BDNF plays a role in protecting and nourishing neurons. Studies48 have shown that long-term exposure to high stress can reduce BDNF levels in the brain and increase depression-like behaviors. Xiangang et al49 studied the correlation between BDNF and inflammatory factors in patients with depression and found that BDNF was negatively correlated with the inflammatory factors IL-6, IL-1β, and TNF-α, and positively correlated with IL-10. Inflammatory factors also affect TrkB phosphorylation, reduce binding to BDNF, and thus reduce BDNF expression. (Please see the yellow line in Figure 2).
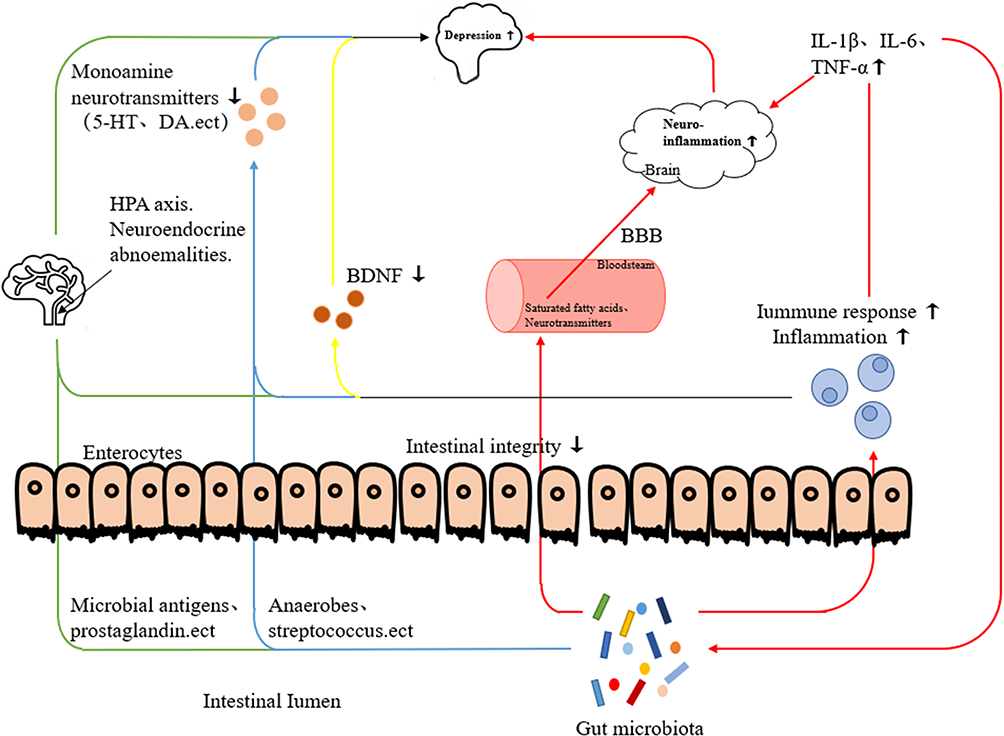 |
Figure 2 Schematic of the pathogenesis of inflammatory response in depression. Inflammatory response exacerbates abnormal HPA axis function; intestinal flora activates the HPA axis through microbial antigens, prostaglandins, and other mediators, all of which eventually lead to depression (Green line). Inflammatory response decreases the synthesis and thus the levels of monoamine neurotransmitters; some flora in the intestine (anaerobic bacteria, streptococci) can affect the metabolism or synthesis of monoamine neurotransmitters, all of which eventually lead to the onset of depression (Blue line). Inflammatory factors reduce the expression of BDNF and thus its levels, leading to depression (Yellow line). Metabolites of the intestinal flora (short-chain fatty acids, neurotransmitters) enter the brain via blood circulation to aggravate the neuroinflammatory response, and other metabolites activate inflammatory cells to produce inflammatory factors that aggravate the neuroinflammatory response in the brain. The inflammatory factors that are produced in turn lead to an imbalance of the intestinal flora and dysregulation of metabolites (Red line). |
Association of Inflammatory Cytokines with Intestinal Flora
In-depth studies reveal that intestinal flora is closely related to depression. An increasing number of studies are focusing on the role of intestinal flora in the pathogenesis of depression. Intestinal flora is the general term for the normal microorganisms inhabiting the human gut. There are about 100 trillion bacteria in the human gut, which are mutually beneficial to and symbiotic with the human body. They enhance digestive ability and reduce the risk of immune diseases, thereby playing an important role in maintaining human health. Studies4,50 suggest that depression is associated with an imbalance of the gut flora. Gut flora, as a key node of interaction between the “gut–brain axis” and the CNS, can be bidirectionally regulated between the “microbiota–gut–brain” (MGB) axis and the CNS. On the one hand, the CNS can directly or indirectly affect the composition and function of the intestinal flora. Gut flora, on the other hand, can in turn influence the development and function of the CNS.
Ke et al51 studied the relationship between human intestinal flora diversity and depression and found that the intestinal flora of patients with depression was disordered and its richness was significantly altered with either an increase or decrease in terms of phyla, family, genus, etc., compared with that in healthy individuals. Xiaomi et al52 found that there were significant differences in the diversity and evenness of intestinal flora in patients with depression compared with that in healthy individuals. For example, Actinomycetes was significantly increased in patients with major depression at the phylum level in intestinal flora. At the family level, the condition of depressed patients was negatively correlated with Prevotella.53 At the genus level, Coprobacillus and other bacteria in the intestinal tracts of patients with severe depression are reported to be lower than those in healthy individuals, whereas the abundance of Collinia, Lactobacillus, and other genera are higher in individuals with severe depression than those in healthy individuals.54 The role of the intestinal flora in the pathogenesis of depression is very complex and no clear mechanisms of action have been reported so far. Many scholars have found that the possible mechanisms may involve the HPA axis, CNS, intestinal nerve and immune inflammatory response, neurotransmitters, intestinal mucosa, and the blood–brain barrier.55 Overactivation of the HPA axis is an important reason leading to depression. Studies have shown that56 intestinal flora can activate the HPA axis through various mediators such as microbial antigens and prostaglandins, thereby leading to depression. (Please see the line green line in Figure 2) Moreover, high neurotransmitter levels in the brain play a role in improving depressive-like behaviors.57 Gut bacteria such as Klebsiella, Egeria, anaerobic bacteria, Streptococcus, etc.) can affect the metabolism or synthesis of one or more monoamine neurotransmitters. (Please see the blue line in Figure 2) For instance, the intestinal flora can activate IDO, reduce 5-HT levels through the canine uric acid metabolism pathway and ultimately lead to depression.58,59
The mechanism of intestinal flora in causing depression may involve the immune inflammatory response. Numerous detailed studies have been conducted to clarify the mechanism of the two causes of depression. The MGB axis is a signal-transduction network with intestinal flora as the core, and its function is closely related to the immune system, nerves, and other aspects.60 Metabolites of the intestinal flora (such as short-chain fatty acids, vitamins, and neurotransmitters) can enter the brain via the blood and have a certain regulatory effect on the human neural circuit. Some metabolites can directly activate inflammatory cells in the circulatory system and migrate to the CNS, thereby regulating the physiological functions of the brain.61 The microbial inflammasome brain axis is also thought to be a communication system associated with depression, linking depression-like stress responses, the immune system, and the gut flora.
Rogers et al62 found that the NLRP3 inflammasome is heavily activated under emotional stimulation, and the inflammatory response that is dependent on this process helps transmit inflammatory signals via the production of IL-1β, IL-6, IL-18, and other inflammatory transcription factors. An imbalance in the metabolites of the intestinal flora can lead to changes in microbial function, and the inflammatory response caused by emotional stimulation is often one of the main reasons for this change. Moreover, the inflammatory response of the CNS, which depends on this process, is one of the possible mechanisms of depression. Huang et al63 proposed that stress-induced inflammatory response could change the composition of the intestinal flora and lead to an imbalance in its metabolites, thus strengthening systemic and central NLRP3-mediated pro-inflammatory signal transduction, affecting the function of the brain and aggravating depression-like behavior. In their review, Tengyun et al reported that the pathogenesis of depression is often accompanied by neuroinflammatory reactions caused by destruction of the blood–brain barrier, and the root cause of this pathological reaction is the inflammatory polarization of neuronal microglia caused by an imbalance in intestinal flora.64 The interaction mechanism between NLRP3 and intestinal flora plays a very important role in the pathogenesis of depression. Zhang et al65 proved the association between the NLRP3 inflammasome and the pathogenesis of depression and studied the flora of mice to determine the correlation between intestinal flora and emotional stimulation in mice. The results showed that mood changes had a significant effect on the changes in intestinal flora and that changes in intestinal flora may have a regulatory effect on brain function, especially during the onset of depression. NLRP3 plays a significant role in this regulatory process. Deletion of NLRP366 alters the normal regulatory function of the intestinal flora, which results in regulatory disorder and further affects brain function leading to neuroinflammation. This process is closely related to the possible causes of depression. Current studies show that changes in intestinal flora can activate the NLRP3 inflammasome pathway, thereby initiating the inflammatory response in the CNS and contributing to the pathogenesis of depression.67 Li et al68 detected the levels of inflammatory factors in the hippocampi of mice by evaluating the damage to the integrity of the intestinal barrier and the disturbance in intestinal flora to varying degrees. Li et al69 further confirmed that the disturbance in intestinal flora affects the expression of pro-inflammatory factors and exacerbates depressive behavior when the microbial population from chronically unpredictable mice with mild stress was injected into sterile mice. In summary, intestinal flora has a strong correlation with the inflammatory response. Inflammatory factors associated with depression, such as ILs, IFN, and TNF, can stimulate the intestine and affect the intestinal flora. The intestinal flora, in turn, aggravates inflammatory reactions through the NLRP3 pathway and ultimately exacerbates depression. (Please see the red line in Figure 2) However, the specific mechanisms of depression of both these approaches need further research.
Modern Medical Treatment of Depression
Modern medical treatment of depression follows certain principles of treatment, namely the development of individualized treatment plans to improve medication compliance. These include choosing a single drug to reduce interaction among different drugs; informing patients and their families about disease development prior to treatment; closely monitoring changes in patients’ conditions and in the occurrence of adverse reactions during treatment, and dealing with them in time. The ultimate goal is to improve the clinical cure rate, minimize disability and mortality rate, improve the quality of life of patients, assist patients in recovering their social function, and prevent the recurrence of depression. Antidepressants such as tricyclic antidepressants (TCAs), monoamine oxidase A inhibitors (MAOIs), selective serotonin reuptake inhibitors (SSRIs) have been developed based on the pathogenesis of depression.70
Tricyclic Antidepressants
Representative TCAs include amitriptyline, clomipramine, and doxepin, which can inhibit the reuptake of 5-HT and norepinephrine (NE) by the presynaptic membranes of nerve endings to increase the concentration of 5-HT and NE in the synaptic gap and promote neurotransmitter release to achieve antidepressant effects. TCAs, as first-generation antidepressants, are one of the first choices of drugs to treat depression in clinical practice since their approval. They are used to treat various types of depression and their effectiveness is as high as 70%–80%. Amitriptyline is commonly used clinically at a dose of 150–250 mg/d, whereas clomipramine and doxepin are used in a clinical setting at a dose of 50–75 mg/d. These drugs are administered as several slow doses.71 This drug family was primarily used to treat depression before 1980 and it monopolized the depression-related market for many years; however, with an increased use of this class of drugs, its shortcomings were apparent. Although TCAs are effective in alleviating depression, they can produce adverse reactions such as dry mouth, nausea, constipation, abnormal liver function, sleep disturbance, and fatigue,72 and even more serious reactions such as cardiotoxicity, which can lead to upright hypotension, tachycardia, and conduction block. These adverse reactions are widespread and severe, and poor drug tolerance results in poor drug compliance among patients.72 TCAs have an anti-inflammatory effect, and the process of treating depression also reduces the inflammatory response in the body. Mohamed et al73 found that the levels of the pro-inflammatory factor TNF-α in the hippocampi were reduced and the inflammatory response was mitigated compared with that in the model group after drug intervention while studying the effects of TNF-α and IDO in the hippocampus and frontal cortex in a rat model of promethazine-induced depression. The drug can be inhibited by the inhibition of pro-inflammatory factors, which reduces the inflammatory response in the treatment of depression.
Monoamine Oxidase A Inhibitors
MAOIs are selective inhibitors of monoamine oxidase and the representative drugs include moclobemide, isocarboxazid, and selegiline. These drugs catalyze the oxidation of monoamine neurotransmitters, inactivate them, and finally degrade them. MAOIs are another treatment option when TCAs are not indicated due to adverse effects. They are generally used as second-line drugs clinically when TCAs or other drugs are ineffective; they are effective in treating patients with atypical depression.72 However, they have a slow onset of action, poor safety and tolerability, and many side effects, including the high toxicity of traditional MAOIs and significant damage to the hematopoietic system and the liver.74 Symptoms such as hypertensive crisis and glutamine syndrome can occur in patients treated with MAOIs if they consume tyramine-containing foods. Studies have shown75 that post-stroke individuals suffering from depression who consume tyramine-containing foods (eg, cheese, fermented foods) while on medication can develop hypertensive crises or pentosidine syndrome, thereby adversely impacting their blood pressure. Side effects such as cardiovascular effects, weight gain, headache, dizziness, nausea, and sexual dysfunction limit the use of these drugs in clinical practice. This class of drugs also exerts an anti-inflammatory effect. Mosiołek et al76 found that patients with MDD had decreased levels of the pro-inflammatory factor IFN-γ and increased levels of anti-inflammatory factors, IL-6 and IL-1β, after treatment with antiphencyclidine. Thus, MAOIs analogs can reduce the levels of pro-inflammatory factors to achieve an anti-inflammatory effect in the treatment of depression.
Selective 5-Hydroxytryptamine Reuptake Inhibitors
As a new generation of antidepressant drugs, SSRIs have the advantages of an easily attainable effective dose, a small range of action, and few adverse reactions,74 which have led to it becoming the first choice in the treatment of depression and the most widely used antidepressant drug in clinical practice. The representative drugs include fluoxetine, paroxetine, sertraline, and escitalopram. The mechanism of action is the same as that of TCAs, which involves inhibition of the reuptake of 5-HT in the presynaptic membranes and an increase in 5-HT levels in the interstitial space to achieve antidepressant effects. In a clinical setting, SSRIs are used as first-line drugs as they are useful in treating several anxiety disorders in addition to exerting antidepressant effects. Paroxetine has the best effect followed by citalopram. Although these drugs are very effective in treating depression, they have certain disadvantages. Taking these drugs can cause adverse effects on the digestive system as diarrhea, dry mouth, nausea, and anorexia; nonspecific convulsions; nervous system presentations such as headaches and tremors; and sexual dysfunction. Nevertheless, SSRIs are safer and easier to use than traditional antidepressants. These drugs also have anti-inflammatory effects, and inflammatory factors are involved in the mechanism of action in treating depression. Fourrier et al77 studied the effect of vortioxetine on the inflammatory response and found that the levels of the inflammatory marker, C-reactive protein, were significantly reduced after drug therapy and that the inflammatory response was significantly reduced. Amitai et al78 studied the effect of fluoxetine and the effect of inflammatory factors in patients suffering from depression and found that the levels of anti-inflammatory factors such as IL-1, IL-6, and TNF-α were significantly higher in control patients than in healthy individuals and that IL-6 levels were reduced after 8 weeks of fluoxetine treatment. SSRIs alleviate depression by reducing the inflammatory response.
Although the above-mentioned drugs are effective in treating depression, several drugs have to be taken for prolonged periods and are associated with slow onset of action, insignificant symptom relief, and obvious side effects. These are some of the challenges in treating depression that affect patients’ confidence and treatment adherence79 (Table 1). There is thus a need for new medications and the identification of new approaches to treat depression. Moreover, supplementation with existing medications could be an approach to treating the disease.
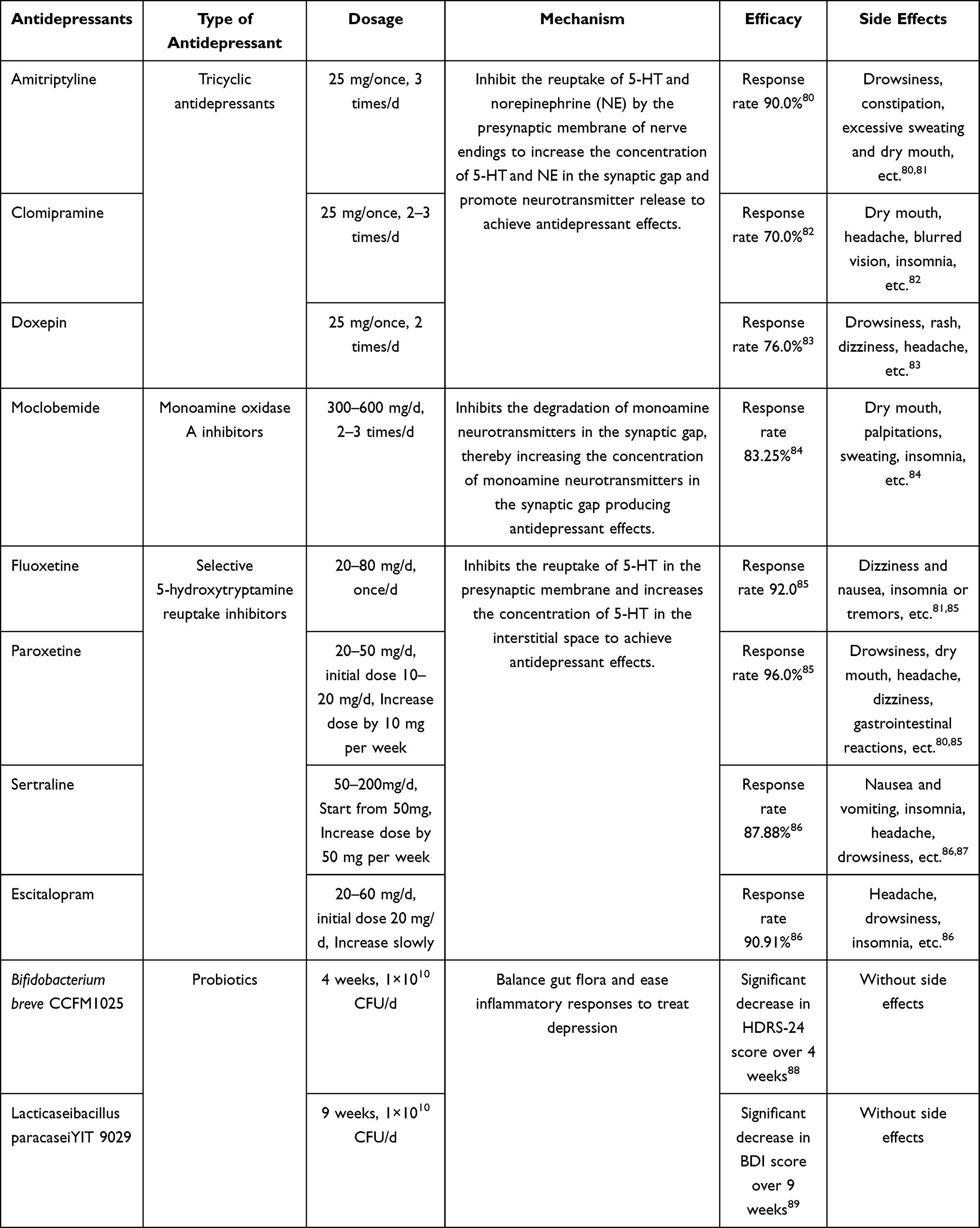 |
Table 1 Partial List of the Medications Available to Treat Depression |
Treating Depression Based on the Relationship Between Gut Flora and Inflammatory Responses
In recent years, some scholars have been studying the relationship between the pathogenesis of depression and inflammatory response due to an imbalance of the intestinal flora. From the theory of the “gut–brain” axis, it is known that depression is accompanied by an inflammatory response. The inflammatory response is generated in the brain and body of patients, and the inflammatory signal enters the intestine via blood circulation to cause disorders in the intestinal microbiota. Disruption of the intestinal flora balance will further aggravate the inflammatory response. Currently, most of these drugs are used to treat depression by restoring the balance of the intestinal flora and alleviating the inflammatory response in the brain.
Minocycline, a highly liposoluble tetracycline has been used for many years to treat Gram-negative bacterial infections and is known to exert anti-inflammatory effects. Yang et al90 treated mice with CUMS-induced depression and found that the drug could correct tight-junction proteins (occludin, ZO-1) of the intestinal mucosa that were disrupted by CUMS to restore intestinal wall integrity, restore the intestinal flora balance, improve intestinal flora metabolism, block the infiltration of intestinal inflammatory factors into the periphery, and reduce the levels of inflammatory factors (IL-6, IL-1β, TNF-α) in the brain, ultimately improving depression-like behavior. In addition, it inhibits specific pathways involved in the inflammatory mechanisms of depression, such as the kynurenine and p-38 pathways.91 The antidepressant effect of minocycline is also associated with the inhibition of microglia activation, which is closely related to neuroinflammation.92 Although there are many drugs to treat depression, approximately 30% of patients are noncompliant due to the side effects of the drugs; thus, there is an urgent need for new therapeutic drugs or treatments. The N-methyl-D-aspartic acid receptor (NMDAR) antagonist, ketamine, has anti-inflammatory and antibacterial effects. Alina Wilkowska et al investigated the specific mechanism of action of ketamine in treating depression and found that it acts through the “gut–brain” axis to alleviate depression, in which, γ-aminobutyric acid, a component of ketamine, can inhibit NMDAR in the protruding anterior and posterior membranes, activate the BDNF/TrkB signaling pathway, and increase BDNF levels in the brain to achieve rapid antidepressant effects.
In recent years, some researchers and scholars have also treated depression using nonpharmaceutical approaches and eventually achieved better results. Yoo et al93 treated depressed mice with oral anti-inflammatory probiotics using a gavage of Lactobacillus plantarum NK151, Bifidobacterium longum NK173, and B. bifidum NK175. As the intestinal flora and brain communicate bidirectionally through the MGB and HPA axes, after a period of treatment with probiotics, it was found that the inflammation caused by immunoglobulins in the hippocampi of depressed mice was suppressed, and the expression of BDNF and claudin-5 in the hippocampus was also reduced. Moreover, this approach also reduced the levels of inflammatory factors, endotoxins, and corticosterone in the blood, and the levels of these indicators were lower in the stools of treated animals versus those in the model group. These findings indicate improvement in the integrity of the intestinal mucosa and abundance of intestinal flora. Dogaru et al17 have reported that probiotics have anti-inflammatory effects in the gut and also at a broader level owing to their ability to reduce the levels of systemic pro-inflammatory cytokines including IL-1β, TNF-α, and IL-6. Therefore, anti-inflammatory probiotics can be used to treat depression. Indirectly treating depression using probiotics can avoid many side effects and likely become an important approach in treating depression (Please see Table 1).
Summary
Depression, as a common disorder of the nervous system, is a challenging research topic in the medical field globally. So far, there are no suitable drugs to treat depression completely based on the complexity of its pathogenesis. The inflammatory response not only directly participates in the pathogenesis of depression through inflammatory factors but also influences other proposed hypothesis mechanisms. Of late, several studies have been conducted to establish the role and mechanism of intestinal flora in depression, making this topic a research hotspot. However, the specific mechanisms are still unclear. Previous studies state that the balance of intestinal flora, including diversity and evenness, is damaged, which affects the levels of inflammatory factors and monoamine neurotransmitters, as well as the HPA axis, all of which culminate in depression (Figure 2). Researchers have reported encouraging findings of pharmacological interventions in influencing the abundance of intestinal flora and alleviating the inflammatory response to produce antidepressant effects. Promising results have been found by knocking out relevant genes and improving the diet to improve the composition of the intestinal flora.65,94,95 However, none of these approaches are clear or suitable for treating depression. Studies have found that inflammatory factors are closely related to intestinal flora in the pathogenesis of depression. For example, inflammation-related factors can stimulate the intestine and affect the intestinal flora, which, in turn, aggravates the inflammatory response and ultimately worsens the symptoms of depression. The mechanisms of action of existing pharmacologic approaches to treat depression have all been linked to inflammatory factors. In the future, if the composition of the intestinal flora is improved through the study of relevant treatment programs and the relevant mechanisms affecting inflammatory factors to treat depression are clarified, the findings will certainly provide a scientific and molecular basis for the treatment of depression by targeting the intestinal flora.
Methods
The review used the following databases: PubMed, ScienceDirect, Springer, Taylor & Francis, China Knowledge Network, and China Wanfang. In the Introduction section, keywords such as “Depression”, “Pathogenesis”, and “Epidemiological research”, were input in the PubMed, CNKI, and ScienceDirect databases. In the Pathogenesis of depression section, keywords such as “Pathogenesis”, “Depression”, “Inflammatory factors”, “NLRP3”, “TLR4”, “IDO”, “Neurotransmitters”, “HPA axis”, “BDNF”, “Intestinal flora”, and “MGB”, were input in the PubMed, Taylor & Francis, CNKI, and Wanfang databases. Other keywords in the Modern medical treatment of depression section were searched in the Springer, PubMed, and CNKI databases, utilizing keywords such as “Treatment”, “Depression”, “TCAs”, “MAOIs”, “SSRIs”, “Adverse reaction”, “Inflammation”, “Intestinal flora”, “Treatment”, “BV2”, and “Anti-inflammatory probiotics”. In the final Summary section, the keywords were searched mainly in the PubMed and CNKI databases and included keywords such as “Improve”, “Depression”, “Intestinal flora”, and “Inflammatory factors”. The articles published in the last 5 years were screened and retrieved using these methods, except for some older articles that were useful for this review.
Meaning Statement
Depression, a serious psychiatric disorder, is a prevalent worldwide condition that requires urgent attention. Studies have reported a link between the gut flora pathogenesis hypothesis and the inflammatory factor pathogenesis hypothesis, but the mechanism of action is still unclear. This narrative review addresses and elaborates both these hypotheses and attempts to clarify the relationship between inflammatory factors, gut flora, and depression to provide a reference for the prevention, diagnosis, and treatment of depression.
Acknowledgments
This work was funded in part by grants from the China Postdoctoral Science Foundation (2016M592319, 2017T100542).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that the study was conducted without any relationship that could be considered a potential conflict of interest.
References
1. Siu AL, Bibbins-Domingo K, Grossman DC, et al; Force USPST. Screening for depression in adults: US preventive services task force recommendation statement. JAMA. 2016;315(4):380–387. doi:10.1001/jama.2015.18392
2. Santomauro DF, Mantilla Herrera AM, Shadid J. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700–1712. doi:10.1016/S0140-6736(21)02143-7
3. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
4. Xiahong Y. Research progress on the mechanism of depression regulation by intestinal flora and its prevention and treatment by Chinese medicine. Chin J Trad Chin Med. 2022;40(09):167–170.
5. Bijun C, Ming T. Advances in the etiology of depression: a focus on genes and gene-environment interactions. General Med Clin Educ. 2020;18(03):250–252.
6. Ng Q, Lim Y, Yaow C, Ng W, Thumboo J, Liew TJN. Effect of probiotic supplementation on gut microbiota in patients with major depressive disorders: a systematic review. Nutrients. 2023;15(6). doi:10.3390/nu15061351
7. Nedic Erjavec G, Sagud M, Nikolac Perkovic M, et al. Depression: biological markers and treatment. Prog Neuropsychopharmacol Biol Psychiatry. 2021;105:110139. doi:10.1016/j.pnpbp.2020.110139
8. Hirschfeld RM. History and evolution of the monoamine hypothesis of depression. J Clin Psychiatry. 2000;61(Suppl 6):4–6.
9. Mikulska J, Juszczyk G, Gawrońska-Grzywacz M, Herbet M. HPA axis in the pathomechanism of depression and schizophrenia: new therapeutic strategies based on its participation. Brain Sci. 2021;11(10):1298. doi:10.3390/brainsci11101298
10. Pitsillou E, Bresnehan SM, Kagarakis EA, et al. The cellular and molecular basis of major depressive disorder: towards a unified model for understanding clinical depression. Mol Biol Rep. 2020;47(1):753–770. doi:10.1007/s11033-019-05129-3
11. Ayoub D, Ahmed S, Moussa F, Moustafa A. Cortisol level in depressed patients and its relation with suicidal risk and anhedonia. Egypt J Neurol Psychiatry Neurosurg. 2016;53(4):193. doi:10.4103/1110-1083.202375
12. Carniel BP, da Rocha NS. Brain-derived neurotrophic factor (BDNF) and inflammatory markers: perspectives for the management of depression. Prog Neuropsychopharmacol Biol Psychiatry. 2021;108:110151. doi:10.1016/j.pnpbp.2020.110151
13. Fries GR, Saldana VA, Finnstein J, Rein T. Molecular pathways of major depressive disorder converge on the synapse. Mol Psychiatry. 2023;28(1):284–297.
14. Maes M, Van der Planken M, Stevens WJ, et al. Leukocytosis, monocytosis and neutrophilia: hallmarks of severe depression. J Psychiatr Res. 1992;26(2):125–134. doi:10.1016/0022-3956(92)90004-8
15. Yishu Y, Junlian L, Jiaping W, et al. Advances in research on the pathogenesis of depression-related disorders. Med Over. 2022;28(12):2368–2372.
16. MingHui H, YaQiong L, Hao Z, et al. Advances in research based on inflammatory mechanisms in animal models of depression. Med Over. 2019;25(12):2294–2298.
17. Dogaru IA, Puiu MG, Manea M, Dionisie V. Current Perspectives on Pharmacological and Non-Pharmacological Interventions for the Inflammatory Mechanism of Unipolar Depression. Brain Sci. 2022;12(10):1403. doi:10.3390/brainsci12101403
18. Han KM, Ham BJ. How inflammation affects the brain in depression: a review of functional and structural MRI studies. J Clin Neurol. 2021;17(4):503–515.
19. Li Y, Song W, Tong Y, et al. Isoliquiritin ameliorates depression by suppressing NLRP3-mediated pyroptosis via miRNA-27a/SYK/NF-κB axis. J Neuroinflam. 2021;18(1):1.
20. Chai Y, Cai Y, Fu Y, et al. viaSalidroside ameliorates depression by suppressing NLRP3-mediated pyroptosis P2X7/NF-κB/NLRP3 signaling pathway. Front Pharmacol. 2022;13:812362. doi:10.3389/fphar.2022.812362
21. Kaufmann FN, Costa AP, Ghisleni G, et al. NLRP3 inflammasome-driven pathways in depression: clinical and preclinical findings. Brain Behav Immun. 2017;64:367–383. doi:10.1016/j.bbi.2017.03.002
22. Hongmei W, LiC L, Li X-Y, et al. Effect of acupuncture on the NOD-like receptor protein 3 inflammatory vesicle signaling pathway in the prefrontal cortex of depressed rats. Acupunct Res. 2020;45(10):806–811. doi:10.13702/j.1000-0607.200063
23. Nan Z, Chen YL. The relationship between NLRP3 inflammatory vesicles and depression and the role of Chinese medicine intervention. Chin J Experimental Formulary. 2023;29(03):186–193.
24. Li DX, Wang CN, Wang Y, et al. NLRP3 inflammasome-dependent pyroptosis and apoptosis in hippocampus neurons mediates depressive-like behavior in diabetic mice. Behav Brain Res. 2020;391:112684. doi:10.1016/j.bbr.2020.112684
25. Levine J, Barak Y, Chengappa KN, Rapoport A, Rebey M, Barak V. Cerebrospinal cytokine levels in patients with acute depression. Neuropsychobiology. 1999;40(4):171–176. doi:10.1159/000026615
26. Thomas AJ, Davis S, Morris C, Jackson E, Harrison R, O’Brien JT. Increase in interleukin-1beta in late-life depression. Am J Psychiatry. 2005;162(1):175–177. doi:10.1176/appi.ajp.162.1.175
27. Alcocer-Gomez E, Cordero MD. NLRP3 inflammasome: a new target in major depressive disorder. CNS Neurosci Ther. 2014;20(3):294–295. doi:10.1111/cns.12230
28. Wang Q, Zeng L, Hong W, et al. Inflammatory cytokines changed in patients with depression before and after repetitive transcranial magnetic stimulation treatment. Front Psychiatry. 2022;13:925007. doi:10.3389/fpsyt.2022.925007
29. Zhou Y, Wang C, Lan X, Li H, Chao Z, Ning Y. Plasma inflammatory cytokines and treatment-resistant depression with comorbid pain: improvement by ketamine. J Neuroinflammation. 2021;18(1):200.
30. Hestad KA, Tonseth S, Stoen CD, Ueland T, Aukrust P. Raised plasma levels of tumor necrosis factor alpha in patients with depression: normalization during electroconvulsive therapy. J ECT. 2003;19(4):183–188. doi:10.1097/00124509-200312000-00002
31. Keri S, Szabo C, Kelemen O. Expression of Toll-Like Receptors in peripheral blood mononuclear cells and response to cognitive-behavioral therapy in major depressive disorder. Brain Behav Immun. 2014;40:235–243. doi:10.1016/j.bbi.2014.03.020
32. Li S, Zhu Z, Lan T, et al. Levomilnacipran ameliorates lipopolysaccharide-induced depression-like behaviors and suppressed the TLR4/Ras signaling pathway. Int Immunopharmacol. 2023;122:110595. doi:10.1016/j.intimp.2023.110595
33. Zhang C, Wang X, Wang C, et al. Qingwenzhike prescription alleviates acute lung injury induced by LPS via inhibiting TLR4/NF-kB pathway and NLRP3 inflammasome activation. Front Pharmacol. 2021;12:790072. doi:10.3389/fphar.2021.790072
34. Huang X, Fei G, Liu W, et al. Adipose-derived mesenchymal stem cells protect against CMS-induced depression-like behaviors in mice via regulating the Nrf2/HO-1 and TLR4/NF-κB signaling pathways. Acta Pharmacol Sin. 2020;41(5):612–619. doi:10.1038/s41401-019-0317-6
35. Li M, Li C, Yu H, et al. Lentivirus-mediated interleukin-1beta (IL-1beta) knock-down in the hippocampus alleviates lipopolysaccharide (LPS)-induced memory deficits and anxiety- and depression-like behaviors in mice. J Neuroinflammation. 2017;14(1):190. doi:10.1186/s12974-017-0964-9
36. Hung YY, Huang KW, Kang HY, Huang GY, Huang TL. Antidepressants normalize elevated Toll-like receptor profile in major depressive disorder. Psychopharmacology. 2016;233(9):1707–1714. doi:10.1007/s00213-015-4087-7
37. C Z, X T, M H, Adilah A. Role of TLR4 signaling in sleep deprivation-induced depression in mice. J Brain Neurol Dis. 2023;31(01):1–7.
38. Y Z, W C, H M. Aerobic exercise and blackberry flavonoid intervention in depressed mice and tissue differential expression of factors related to TLR4/MyD88/NF-κB pathway. Chin J Cell Biol. 2018;40(11):1847–1857.
39. Chen LM, Bao CH, Wu Y, et al. Tryptophan-kynurenine metabolism: a link between the gut and brain for depression in inflammatory bowel disease. J Neuroinflammation. 2021;18(1):135. doi:10.1186/s12974-021-02175-2
40. Xiting Z, Yi W, Lin L, et al. Current status of research on the relationship between inflammatory factors and other depression-related factors. Chin J Clin Pharmacol. 2018;34(21):2568–2571.
41. Zhang K, Liu R, Gao Y, Ma W, Shen W. Electroacupuncture relieves LPS-induced depression-like behaviour in rats through IDO-mediated tryptophan-degrading pathway. Neuropsychiatr Dis Treat. 2020;16:2257–2266. doi:10.2147/NDT.S274778
42. Savonije K, Meek A, Weaver DF. Indoleamine 2,3-dioxygenase as a therapeutic target for Alzheimer’s disease and geriatric depression. Brain Sci. 2023;13(6):852. doi:10.3390/brainsci13060852
43. Mallik SB, Mudgal J, Kinra M, et al. Involvement of indoleamine 2, 3-dioxygenase (IDO) and brain-derived neurotrophic factor (BDNF) in the neuroprotective mechanisms of ferulic acid against depressive-like behaviour. Metab Brain Dis. 2023;38(7):2243–2254. doi:10.1007/s11011-023-01267-7
44. X F, H L, T C, Q J, H Q. Study on the relationship between IL-1β, IL-6 and downstream IDO activation and depressive behavior in rats. Chongqing Med. 2018;47(15):1986–1989.
45. Li H, Jian K. Advances in the involvement of indoleamine 2,3-dioxygenase (IDO) in the pathogenesis of depression. J Yichun Coll. 2016;38(09):24–28.
46. ZhuQing, L, LiPing, Y, ShanYin, Y et al. Effects of electroacupuncture “Xieyu Fang” on serum levels of indoleamine 2,3 dioxygenase, 5-hydroxytryptamine and interleukin 10 in rat models of depression. J Shanxi Univ Trad Chin Med. 2020;21(03):172–175.
47. Felger JC, Li L, Marvar PJ, et al. Tyrosine metabolism during interferon-alpha administration: association with fatigue and CSF dopamine concentrations. Brain Behav Immun. 2013;31:153–160.
48. Murawska-Ciałowicz E, Wiatr M, Ciałowicz M, et al. BDNF impact on biological markers of depression-role of physical exercise and training. Int J Environ Res Public Health. 2021;18(14):7553. doi:10.3390/ijerph18147553
49. Xiangang S, YuBo, H, GuoLiang, Z, et al. Effect of Huanglian Wenzhi Tang with addition and subtraction on the therapeutic effect and serum inflammatory response and levels of brain-derived neurotrophic factor, nuclear transcription factor-κB, 5-hydroxytryptamine and substance P in patients with coronary artery disease with anxiety and depressive states. World J Integr Chin Western Med. 2022;17(03):566–570.
50. Rui W, Shuming H. Advances in the study of the pathogenesis of depression. Graduate Med J. 2014;27(12):1332–1336.
51. Ke H, Tongtong Z, Kai, Z, GuoQiang, W, et al. Correlation between intestinal flora diversity and depressive symptoms in patients with first-episode depression. Microbiol Bull. 2023;50(03):1040–1051.
52. Xiaomi W, Yunxiao S, Xiaolan W, H SQ. Advances in research on the relevance of gut flora to depression. Mod Food Technol 2023 39 6,2. 331–341.
53. Chung YE, Chen HC, Chou HL, et al. Exploration of microbiota targets for major depressive disorder and mood related traits. J Psychiatr Res. 2019;111:74–82. doi:10.1016/j.jpsychires.2019.01.016
54. Chen JJ, Zheng P, Liu YY, et al. Sex differences in gut microbiota in patients with major depressive disorder. Neuropsychiatr Dis Treat. 2018;14:647–655. doi:10.2147/NDT.S159322
55. Kundu P, Blacher E, Elinav E, Pettersson SJC. Our gut microbiome: the evolving inner self. Cell. 2017;171(7):1481–1493. doi:10.1016/j.cell.2017.11.024
56. Misiak B, Łoniewski I, Marlicz W, et al. The HPA axis dysregulation in severe mental illness: can we shift the blame to gut microbiota? Prog Neuro Psychopharmacol Biol Psychiatry. 2020;102:109951. doi:10.1016/j.pnpbp.2020.109951
57. XiaoNa, C, YanShu, P, DongHui, W et al. Experimental study on the establishment of a novel rat model of depression based on the antagonistic relationship of neurotransmitter pairs in the brain. Chin J Pathophysiol. 2017;33(06):1141–1146.
58. Cheng D, Chang H, Ma S, et al. Tiansi liquid modulates gut microbiota composition and Tryptophan(-)Kynurenine metabolism in rats with hydrocortisone-induced depression. Molecules. 2018;23(11):2832. doi:10.3390/molecules23112832
59. Rogers GB, Keating DJ, Young RL, Wong ML, Licinio J, Wesselingh S. From gut dysbiosis to altered brain function and mental illness: mechanisms and pathways. Mol Psychiatry. 2016;21(6):738–748. doi:10.1038/mp.2016.50
60. Pellegrini C, Fornai M, Antonioli L, Blandizzi C, Calderone V. Phytochemicals as novel therapeutic strategies for NLRP3 inflammasome-related neurological. Metabol Inflam Dis. 2019;20(12):2876.
61. Pellegrini C, Antonioli L, Calderone V, Colucci R, Fornai M, Blandizzi CJ. Microbiota-gut-brain axis in health and disease: is NLRP3 inflammasome at the crossroads of microbiota-gut-brain communications? Prog Neurobiol. 2020;191:101806. doi:10.1016/j.pneurobio.2020.101806
62. Inserra A, Rogers G, Licinio J, Wong M. The microbiota-inflammasome hypothesis of major depression. BioEssays. 2018;40(9):e1800027. doi:10.1002/bies.201800027
63. Huang L, Ma Z, Ze X, et al. Gut microbiota decreased inflammation induced by chronic unpredictable mild stress through affecting NLRP3 inflammasome. Front Cell Infect Microbiol. 2023;13:1189008. doi:10.3389/fcimb.2023.1189008
64. Tengyun W, Huajun L, Chunlei J, W YX. Inflammatory response and depression due to disorders of intestinal flora. Adv Mod Biomed. 2014;14(36):7175–77+93.
65. Zhang Y, Huang R, Cheng M, et al. Gut microbiota from NLRP3-deficient mice ameliorates depressive-like behaviors by regulating astrocyte dysfunction via circHIPK2. Microbiome. 2019;7(1):116. doi:10.1186/s40168-019-0733-3
66. Yao H, Zhang D, Yu H, et al. Gut microbiota regulates chronic ethanol exposure-induced depressive-like behavior through hippocampal NLRP3-mediated neuroinflammation. Mol Psychiatry. 2023;28(2):919–930. doi:10.1038/s41380-022-01841-y
67. Hui Y. Mechanisms of Depressive-Like Behavior in Mice with Altered Intestinal Flora Composition Induced by Chronic Ethanol Exposure via Activation of Hippocampal NLRP3 Inflammatory Vesicles. China Medical University; 2022.
68. Li JM, Yu R, Zhang LP, et al. Dietary fructose-induced gut dysbiosis promotes mouse hippocampal neuroinflammation: a benefit of short-chain fatty acids. Microbiome. 2019;7(1):98. doi:10.1186/s40168-019-0713-7
69. Li N, Wang Q, Wang Y, et al. Fecal microbiota transplantation from chronic unpredictable mild stress mice donors affects anxiety-like and depression-like behavior in recipient mice via the gut microbiota-inflammation-brain axis. Stress. 2019;22(5):592–602. doi:10.1080/10253890.2019.1617267
70. Mu L, Sun J. Pathogenesis of depression and targets of antidepressant drug action. Int J Pharm Res. 2015;42(04):463–466.
71. Xiaodang W, Liyun H, Yanjiao L. Overview of research on antidepressants for depression. World’s Newest Med Inform Digest. 2018;18(06):50–53.
72. Gao Y. A review of research advances in the treatment of depression. Mod Trade Ind. 2019;40(05):78–80.
73. Mohamed BM, Aboul-Fotouh S, Ibrahim EA, et al. Effects of pentoxifylline, 7-nitroindazole, and imipramine on tumor necrosis factor-α and indoleamine 2,3-dioxygenase enzyme activity in the hippocampus and frontal cortex of chronic mild-stress-exposed rats. Neuropsychiatr Dis Treat. 2013;9:697–708. doi:10.2147/NDT.S41020
74. Shen R, Zhou H, Zhao Z. Advances in Western medical treatment of post-stroke depression. Med Rev. 2021;27(24):4883–4887.
75. Corbineau S, Breton M, Mialet-Perez J, Costemale-Lacoste J. Major depression and heart failure: interest of monoamine oxidase inhibitors. Int J Cardiol. 2017;247:1–6. doi:10.1016/j.ijcard.2017.07.005
76. Mosiołek A, Pięta A, Jakima S, Zborowska N, Mosiołek J, Szulc A. Effects of antidepressant treatment on peripheral biomarkers in patients with Major Depressive Disorder (MDD). J Clin Med. 2021;10(8):1706.
77. Fourrier C, Sampson E, Mills NT, Baune BT. Anti-inflammatory treatment of depression: study protocol for a randomised controlled trial of vortioxetine augmented with celecoxib or placebo. Trials. 2018;19(1):447. doi:10.1186/s13063-018-2829-7
78. Amitai M, Taler M, Ben-Baruch R, et al. Increased circulatory IL-6 during 8-week fluoxetine treatment is a risk factor for suicidal behaviors in youth. Brain Behav Immun. 2020;87:301–308. doi:10.1016/j.bbi.2019.12.017
79. Yang L, Wang Y, Hao L. Research progress of Chinese medicine in the treatment of depression. Chin Med Inform. 2022;39(07):86–89.
80. M J. Clinical efficacy of paroxetine in the treatment of depression Safety and prognostic analysis. Prim Care Forum. 2019;23(20):2833–2834.
81. X Z. Analysis of the efficacy and adverse effects of fluoxetine and amitriptyline in the treatment of depression. Electr J Clin Pharm Literat. 2019;6(95):
82. QiXin, Y, Bing, Y. Analysis of efficacy, adverse effects and patient compliance in the treatment of depression with mirtazapine and clomipramine. J Syst Med. 2021;6(17):145–147.
83. XiaoJing, L, YingYan, G, HaiXia, Z et al. The efficacy and safety of fluoxetine combined with doxepin in the treatment of childhood depression. Shandong Med. 2017;57(20):90–92.
84. Biao, D, Yang, D, Jie, Z et al. Systematic evaluation of moclobemide versus amitriptyline in the controlled treatment of depression. Chin Pharm Ind. 2015;24(20):21–23.
85. H L, Q Y, Y D, X H. Clinical efficacy and safety analysis of paroxetine and fluoxetine in the treatment of depression. J Clin Med Literat. 2018;5(73):
86. Yanping, Z, Yan, Z, Man, M. Comparison of the efficacy and safety of escitalopram and sertraline in depressed patients with anxiety symptoms. Int J Psychiatry. 2023;50(01):75–77+92.
87. Y L. Efficacy of sertraline combined with bupropion in adolescents with first-episode depression. Henan Med Res. 2023;32(18):3380–3383.
88. Tian P, Chen Y, Zhu H, et al. Bifidobacterium breve CCFM1025 attenuates major depression disorder via regulating gut microbiome and tryptophan metabolism: a randomized clinical trial. Brain Behav Immun. 2022;100:233–241. doi:10.1016/j.bbi.2021.11.023
89. Zhang X, Chen S, Zhang M, et al. Effects of fermented milk containing lacticaseibacillus paracasei strain shirota on constipation in patients with depression: a randomized, double-blind, placebo-controlled trial. Nutrients. 2021;13(7):2238.
90. Yang Q, Luo L, Sun T, et al. Chronic minocycline treatment exerts antidepressant effect, inhibits neuroinflammation, and modulates gut microbiota in mice. Psychopharmacology. 2020;237(10):3201–3213. doi:10.1007/s00213-020-05604-x
91. Nettis MA. Minocycline in major depressive disorder: and overview with considerations on treatment-resistance and comparisons with other psychiatric disorders. Brain Behav Immun Health. 2021;17:100335. doi:10.1016/j.bbih.2021.100335
92. Bassett B, Subramaniyam S, Fan Y, et al. Minocycline alleviates depression-like symptoms by rescuing decrease in neurogenesis in dorsal hippocampus via blocking microglia activation/phagocytosis. Brain Behav Immun. 2021;91:519–530. doi:10.1016/j.bbi.2020.11.009
93. Yoo J, Shin Y, Ma X, et al. The alleviation of gut microbiota-induced depression and colitis in mice by anti-inflammatory probiotics NK151, NK173, and NK175. Nutrients. 2022;14(10):2080.
94. Swann OG, Kilpatrick M, Breslin M, Oddy WH. Dietary fiber and its associations with depression and inflammation. Nutr Rev. 2020;78(5):394–411.
95. Wong ML, Inserra A, Lewis MD, et al. Inflammasome signaling affects anxiety- and depressive-like behavior and gut microbiome composition. Mol Psychiatry. 2016;21(6):797–805. doi:10.1038/mp.2016.46
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Associations of High-Sensitivity C-Reactive Protein and Interleukin-6 with Depression in a Sample of Italian Adolescents During COVID-19 Pandemic
Serra M, Presicci A, Quaranta L, Achille M, Caputo E, Medicamento S, Margari F, Croce F, Margari L
Neuropsychiatric Disease and Treatment 2022, 18:1287-1297
Published Date: 29 June 2022
The Role of Intestinal Flora and Its Metabolites in Heart Failure
Guan X, Sun Z
Infection and Drug Resistance 2023, 16:51-64
Published Date: 5 January 2023
Wenyang-Tianjing-Jieyu Decoction Improves Depression Rats of Kidney Yang Deficiency Pattern by Regulating T Cell Homeostasis and Inflammation Level
Zhang T, Wang J, Wang Y, He L, Lv S, Wang Y, Li W
Neuropsychiatric Disease and Treatment 2024, 20:631-647
Published Date: 22 March 2024
The Effect of Depression on Disease Activity and Treatment Response in Patients with Inflammatory Arthritis: Results from a Narrative Literature Review
Dagli A, Lee RR, Bluett J
Neuropsychiatric Disease and Treatment 2024, 20:1377-1386
Published Date: 5 July 2024
NMDAR Down-Regulation: Dual – Hit Molecular Target For COPD – Depression Comorbidity
Heresco-Levy U, Haviv J, Caine YG
Journal of Inflammation Research 2024, 17:7619-7625
Published Date: 23 October 2024