Back to Journals » International Journal of Nanomedicine » Volume 21
Nanotechnology-Driven Drug-Delivery Systems: Mechanistic Insights for Pediatric Autism Treatment in 2026
Authors Atashgahi M, Madani F ![]() , Webster TJ
, Webster TJ ![]()
Received 28 January 2026
Accepted for publication 17 April 2026
Published 9 June 2026 Volume 2026:21 599496
DOI https://doi.org/10.2147/IJN.S599496
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Anderson Oliveira Lobo
Mahboubeh Atashgahi,1 Fatemeh Madani,2 Thomas J Webster3– 5
1Department of Surgery, Royal Children’s Hospital, Melbourne, VIC, Australia; 2Department of Medical Nanotechnology, Tehran University of Medical Sciences, Tehran, Iran; 3Division of Pre-College and Undergraduate Studies, Brown University, Providence, RI, USA; 4School of Engineering, Saveetha University, Chennai, India; 5School of Health Sciences and Biomedical Engineering, Hebei University of Technology, Tianjin, People’s Republic of China
Correspondence: Thomas J Webster, Email [email protected]
Abstract: Autism spectrum disorder (ASD) is a diverse neurodevelopmental disorder that commences in early childhood, characterized by enduring social-communication challenges, limited interests, and behavioral rigidity. The management of ASD continues to pose significant difficulties in pediatric practice. Converging evidence implicates abnormalities in synaptic scaffolding and transmission, excitation–inhibition imbalance, mTOR/PI3K–AKT signaling, neuroinflammation, gut–brain axis, and metabolic disturbances, highlighting multiple cellular and molecular targets for potential therapeutic development. Nonetheless, contemporary care is primarily characterized by non-pharmacological interventions and symptomatic pharmacological treatments, with a scarcity of strategies that alter fundamental mechanisms. The blood-brain barrier (BBB) is a significant hurdle to overcome - its structure, transport routes, and context-specific dysfunction in ASD both limit and create opportunities for central nervous system (CNS) drug delivery at the same time. In this context, nanomedicine presents novel opportunities and nanoparticles are currently emerging for various neurological applications in preclinical and clinical studies. They can be designed for targeted drug delivery to the brain, for the development of sophisticated ASD models and for diagnostic and theranostic purposes. This review incorporates the clinical manifestations, mechanistic pathways, BBB biology, and nanoparticle-based methodologies to provide a developmentally informed framework for nano-enabled interventions in ASD.
Keywords: autism spectrum disorder, nanomedicine, blood–brain barrier, targeted delivery, gut–brain axis
Introduction
It is frequently asserted that the brain is the most intricate structure in the body. This is due not only to its regulation of thinking, behavior, and emotion, but also to its susceptibility to various neurological and psychiatric illnesses.1,2 Neuroscience has advanced significantly over recent decades; nonetheless, the treatment of central nervous system (CNS) illnesses remains exceedingly challenging. Both the complexity of the CNS regarding its architecture and function, along with biological protective mechanisms, such as the blood-brain barrier (BBB) which complicate drug penetration and frequently diminish their specificity and safety, are significant hurdles to be overcome.3
ASD is a distinct neurodevelopmental disease marked by persistent difficulties in social communication and restricted or repetitive behaviors. Over the past two decades, the worldwide prevalence of ASD has increased markedly. While improved diagnostic awareness substantially influences this tendency, various environmental factors impacting early neurodevelopment have also been investigated. The World Health Organization (WHO, 2021) estimates that roughly 1 in 127 individuals worldwide are on the autism spectrum, representing approximately 0.8% of the global population.4,5 The Global Burden of Disease (GBD 2021) research validates these findings, revealing an age-standardized prevalence of 0.788% and an incidence rate of 9.3 per 100,000 individuals.6 Significant regional variance exists. The U.S. Centers for Disease Control and Prevention (CDC, 2024) indicate that approximately 1 in 36 children are affected by the condition; nevertheless, most low- and middle-income countries continue to record lower prevalence rates, albeit with gradual increases.7,8 These disparities are likely attributable to variations in diagnostic practices, healthcare systems efficacies, and public awareness of the issue, rather than genuine biological differences. Nonetheless, the rising incidence of ASD diagnoses globally indicates an urgent need for interventions that can immediately target the fundamental neurological processes of the illness.9
Since Leo Kanner’s 1943 characterization of ASD,10 scientific views on ASD have changed. Once thought to merely psychogenic, it is now recognized as a complex condition impacted by genetic, neurological, and environmental factors.11,12 ASD patients often have comorbidities like epilepsy, anxiety, depression, and ADHD, which complicate diagnosis and treatment.10 Although behavioral evaluation tools have improved, clinical observation is still the main way to diagnose ASD. Due to individual heterogeneity, no reliable biochemical or neuroimaging biomarkers have been found.10 Current interventions, such as Early Intensive Behavioral Intervention (EIBI), Applied Behavior Analysis (ABA) speech and occupational therapy, and other behavioral supports, aim to improve communication and daily tasks. Drugs usually address ASD symptoms like irritability and hyperactivity, not the illness itself. Modern treatments rarely address the disorder’s neurobiology.13
Nanotechnology has attracted considerable attention as a prospective approach in this setting.2,14 Nanoparticles (NPs) exhibit considerable potential in drug delivery systems. Their diminutive size, customizable surface characteristics, and overall superior biocompatibility render them more effective than conventional delivery systems. They can traverse the BBB more effectively and enhance medication stability, bioavailability, and overall therapeutic efficacy.15 As a result, nanotechnology-based methods are increasingly being explored for neurological and neurodevelopmental problems, such as Autism Spectrum Disorder (ASD).16
This review summarizes ASD knowledge and examines the potential of nanotechnology to diagnose and treat ASD in preclinical studies as of 2026. Interest is in NP-mediated drug delivery systems and nanoscale diagnostic technologies that potentially improve ASD and other neurodevelopmental disorder treatment, and finally pave the way for future clinical studies.
Clinical Manifestations of ASD
ASD is marked by persistent challenges in social communication and interaction, alongside constrained and repetitive behavioral patterns, interests, or activities. The diagnostic framework now encompasses atypical sensory reactivity, including hyper-responsiveness, hypo-responsiveness, or unusual sensory interests, which have been acknowledged as a fundamental aspect of the phenotype. Symptoms generally appear in early development and endure throughout life, although their manifestation and the requisite level of support can vary significantly among individuals.17 A defining characteristic of ASD is its heterogeneity. Language and cognitive skills cover a wide range, from very low levels of intelligence to very high levels of intelligence or anywhere in between.2 Motor coordination difficulties and variations in sensory processing are frequently noted and may affect daily functioning in nuanced yet significant manners.18 ASD seldom manifests as a singular condition. Neurological comorbidities are especially important to note. Epilepsy affects about 2–60% of people with ASD, and this is especially true for those who also have an intellectual disability.19 This shows that ASD is more than just a problem with social-cognitive circuits; it also affects other neural systems.20 Systemic conditions are also common such as sleep disturbances, encompassing insomnia, circadian rhythm irregularities, and parasomnias, manifesting at elevated frequencies, and can markedly intensify diurnal behavioral and emotional difficulties. Multiple meta-analyses20 have shown that autistic children are more likely than non-autistic children to have gastrointestinal problems like constipation, diarrhea, stomach pain, and reflux.21 Psychiatric comorbidities, such as ADHD, anxiety disorders, and mood disturbances, are also common and frequently lead to significant functional impairment. These multisystem characteristics collectively highlight the necessity for evaluation and intervention strategies that transcend a solely neurocentric paradigm, advocating for a more holistic biopsychosocial approach.18 Figure 1 demonstrates the clinical manifestations of ASD.
 |
Figure 1 Clinical features of ASD (Created with BioRender.com). |
Cellular and Molecular Pathophysiology of ASD: Implications for Nanomedicine Therapeutic Development
ASD originates from disruptions across multiple hierarchical biological levels, including genes, chemical processes, brain circuits, and extended networks. Although the complete causal architecture remains difficult to elucidate, numerous cellular and molecular pathways have been repeatedly associated with it. These pathways are becoming significant for discovering new treatments as they offer distinct biological targets that can potentially be modified through pharmaceuticals, genetics, or nanotechnology. The key mechanistic domains relevant to therapeutic innovation are outlined below.22,23
Synaptic Scaffolding and Transmission
Significant evidence suggests that synapse disruption is a fundamental element in ASD. Loss-of-function mutations and copy-number variants impacting synaptic scaffolding and adhesion proteins, particularly within the SHANK, neuroligin (NLGN), and neurexin (NRXN) families, alter the formation of excitatory synapses and reduce synaptic plasticity. These abnormalities undermine the integrity of glutamatergic synapses, affecting both microcircuit stability and long-range connectivity.24,25 In particular syndromic variations of ASD, namely Phelan–McDermid syndrome caused by SHANK3 haploinsufficiency, preclinical studies suggest that restoring SHANK3 expression can restore synaptic function and reverse core behavioral abnormalities. The results offer compelling evidence for a direct gene → circuit → behavior link and highlight the potential of gene-targeted therapies for specific genetic subgroups.26,27
Excitation–Inhibition (E/I) Imbalance
A further significant mechanistic topic pertains to alterations in the equilibrium between excitatory and inhibitory transmission between cortical and subcortical networks. Disruptions in GABAergic interneurons and alterations in glutamatergic transmission leads to network hyperexcitability and atypical oscillatory patterns. Many individuals believe that these issues are the underlying causes of sensory hypersensitivity, motor stereotypes, and repetitive behaviors.28,29 Whilst pharmacological treatments to restore excitatory/inhibitory balance show theoretical promise; in practice, systemic modulators often have adverse off-target effects. Such difficulties underscore the need for more precise delivery systems that can alter circuit dynamics with less systemic effects.30
Maternal Immune Activation and ASD
Maternal immune activation (MIA) is known as one of the causes of ASD. Various researchers indicate that inflammatory processes during pregnancy may enhance the risk of neurodevelopmental disorders in offspring which may trigger the release of pro‑inflammatory cytokines that can change the maternal–placental–fetal interface resulting in dysregulation of inflammatory cytokines like interleukin‑6 (IL‑6), tumor necrosis factor‑α (TNF‑α), and interleukin‑17A (IL‑17A). Finally, these changes in inflammatory pathways can leads to impaired cortical development and contribute to the emergence of behavioral phenotypes associated with ASD. Furthermore, maternal inflammation may lead to activation of microglia in the developing fetal brain and also lead to disruption of synaptic connectivity which is a key feature in ASD pathophysiology.31–33
mTOR/PI3K-AKT Signaling
Hyperactivation of the mTOR pathway has been documented in multiple ASD models and in human genetic variants linked to PTEN, TSC1/2, and associated signaling elements. Excessive mTOR activity disrupts the production of synaptic proteins, the morphology of dendrites, and neuronal development. Modulating mTOR signaling in animal models has shown the ability to rectify synaptic defects and enhance behavioral deficits, suggesting that targeted pathway inhibitors may be effective in ASD subgroups marked by discernible mTOR–PI3K–AKT dysregulation.34,35
Neuroinflammation and Immune Dysregulation
The participation of the neuroimmune system constitutes another substantial and reproducible discovery. Research consistently indicates microglial activation, increased levels of pro-inflammatory cytokines (such as IL-6 and TNF-α) and altered peripheral immunological profiles in both human ASD cohorts and animal models. Neuroinflammation can adversely affect synaptic pruning, activity-dependent maturation, and functional connectivity. These results provide a molecular rationale for exploring immune-modulating treatments, including anti-inflammatory drugs, targeted cytokine regulation, and, in experimental contexts, cell-based immunotherapies.36,37
Gut–Brain Axis and Metabolism
Increasing evidence indicates a bidirectional influence between the gut microbiome and neurodevelopment.32,33,38,39 Dysbiosis, in conjunction with alterations in microbial metabolites (such as short-chain fatty acids and tryptophan-derived substances), can influence the development of the CNS, neurotransmitter synthesis, and behavior. Clinical trials, though still limited, suggest improvements in gastrointestinal and behavioral symptoms following therapies that affect the gut microbiome, such as particular probiotics, dietary modifications, and fecal microbiota transplantation (FMT).33 These findings suggest a viable peripheral-to-CNS treatment route that may improve upon direct neuromodulatory approaches.
ASD Treatment
The therapeutic management of ASD includes both non-pharmacological and pharmaceutical approaches, each customized to address the considerable heterogeneity characteristic of the illness. The main goals of these therapies are to improve adaptive functioning, promote communication and learning, reduce maladaptive or unpleasant behaviors, and eventually enhance the overall quality of life.25 Treatment strategies are typically customized for each individual, as symptoms vary among patients, necessitating a collaborative approach including a team of professionals which consider cognitive, behavioral, emotional, and physiological elements to build a comprehensive care plan. Growing data highlight the importance of the microbiota–gut–brain axis in ASD.40,41 Many autistic children experience gastrointestinal issues correlated with alterations in their gut microbiota composition that can be quantified. These alterations encompass modifications in the bacteroidetes/firmicutes ratio, genus-specific disturbances, and elevated concentrations of microbially produced metabolites, particularly short-chain fatty acids such as propionic acid. Biomarkers reflecting increased intestinal permeability and epithelial injury frequently correlate with the intensity of behavioral symptoms, reinforcing the concept that “leaky gut” physiology may affect symptom expression in specific individuals. Communication along the microbiota–gut–brain axis transpires through multiple mechanisms, including vagal and enteric nervous system signaling, immune and cytokine activity, endocrine modulation, and microbial metabolites that influence central nervous system circuits and the integrity of the BBB. These interconnected circuits offer a medically plausible method via which gut physiology may affect neurodevelopment and behavior. Preliminary clinical investigations provide initial validation for this approach. Research employing tailored probiotics or synbiotics suggests that these therapies may alleviate gastrointestinal symptoms and, in some cases, produce slight improvements in behaviors related to ASD. Nonetheless, considerable heterogeneity in microbial strains, dosage protocols, inclusion criteria, and study design has limited the ability to draw conclusive findings. Cristofori et al emphasize that the next advancements will require biomarker-stratified, adequately powered clinical trials to evaluate precision microbiome manipulation as a potential enhancement to multimodal ASD care.42
Non-Pharmacological ASD Treatment
Non-pharmacological therapies remain fundamental, emphasizing evidence-based behavioral, developmental, educational, and physical approaches.43,44 Behavioral therapies, particularly Applied Behavior Analysis (ABA), Discrete Trial Training (DTT), and Pivotal Response Training (PRT), represent the most rigorously tested methods in contemporary therapeutic practice.45
The Lovaas approach is a highly structured, therapist-directed intervention that integrates the principles of ABA and DTT. It focuses on deconstructing complex skills into smaller, educational components to enhance learning in communication, cognition, social interaction, and daily adaptive behaviors, while concurrently reducing maladaptive habits.46,47 Conversely, PRT is a form of Naturalistic Developmental Behavioral Intervention (NDBI) that emphasizes enhancing intrinsic motivation and fostering spontaneous, child-directed communication. Therapy is included into play and daily activities, connecting educational possibilities with the child’s inherent interests and routines. Despite the structural and philosophical differences between ABA/DTT and PRT, both methodologies have demonstrated substantial advancements in various developmental domains, including language acquisition, social engagement, and adaptive functioning. Their complementary strengths underscore the need for individualized treatment planning that aligns intervention tactics with each child’s unique behavioral traits, learning preferences, and developmental needs.48,49 Table 1 and Figure 2 summarize the common interventions in ASD treatment.
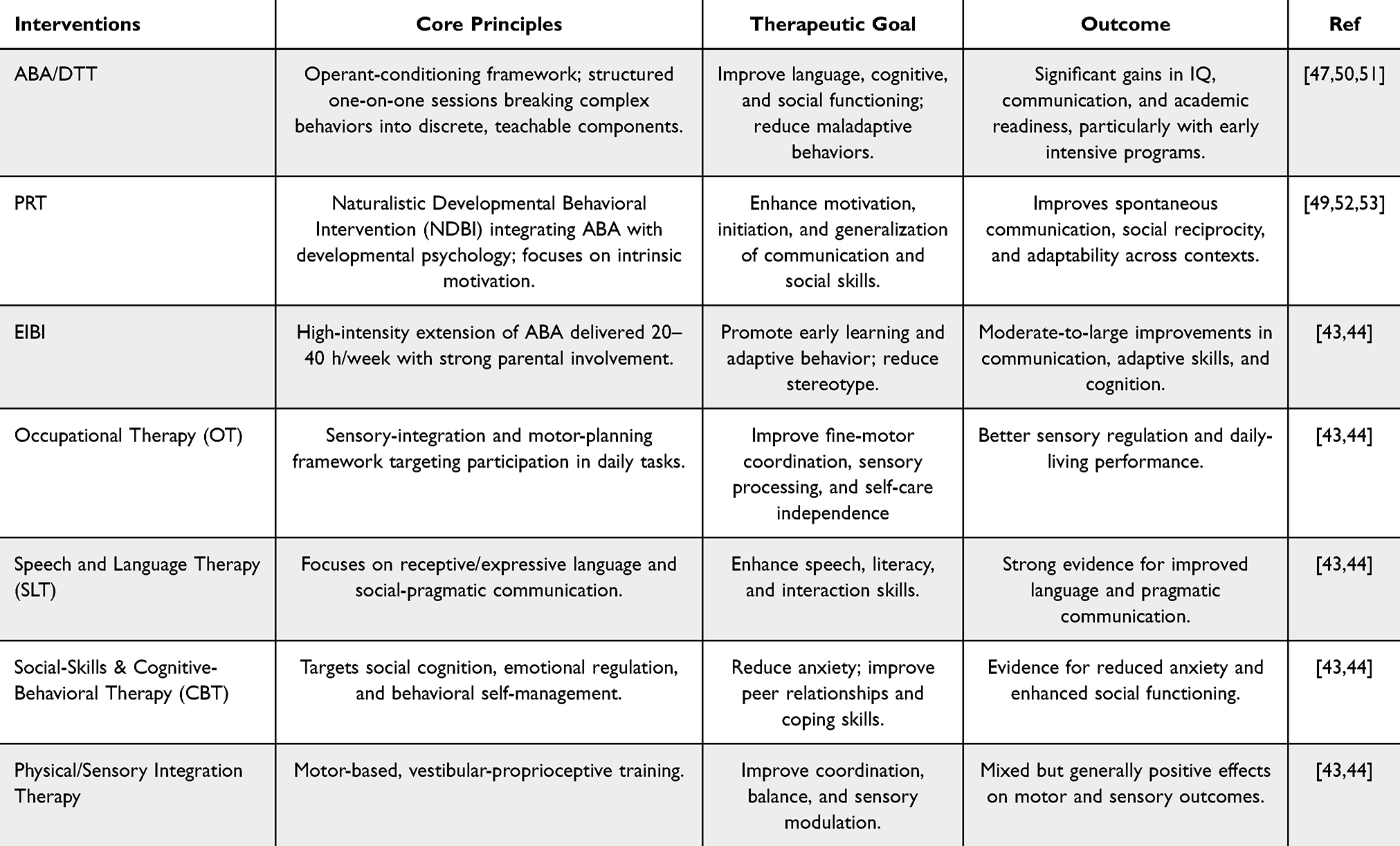 |
Table 1 Non Pharmacological Interventions for ASD |
 |
Figure 2 Common intervention strategies for ASD (Created with BioRender.com). Abbreviations: ABA, Applied Behavior Analysis; CBT, Social-Skills & Cognitive-Behavioral Therapy; DTT, Discrete Trial Training; EIBI, Early Intensive Behavioral Intervention; and PRT, Pivotal Response Training. |
Pharmacological Treatments
In addition to non-pharmacological methods, pharmacological treatments are an important part of treating the behavioral, emotional, and physical problems associated with ASD.54 These medications do not address the fundamental diagnostic characteristics of ASD; instead, they focus on alleviating concomitant symptoms such as irritability, aggression, anxiety, hyperactivity, or sleep disturbances - that can profoundly impact daily functioning and overall health.55 Table 2 provides a summary of the main drugs that are currently used to treat ASD, along with their uses and other important information.
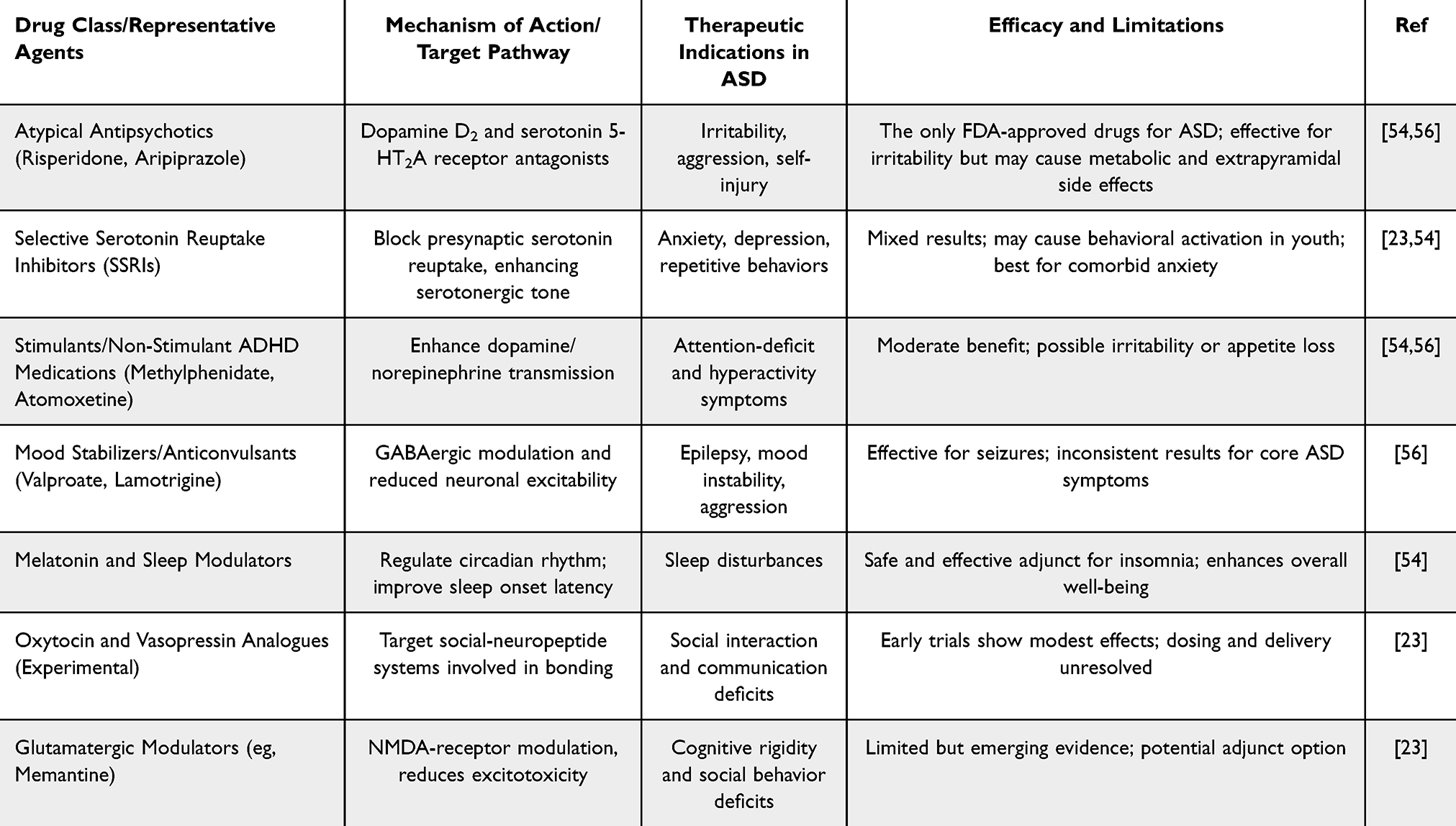 |
Table 2 Principal Pharmacological Interventions for ASD |
The BBB in ASD: Alterations and Design Opportunities
BBB Structure and Transport Routes
The BBB is the primary barrier regulating the exchange of chemicals between peripheral circulation and the central nervous system. Its primary characteristic is a highly selective permeability, allowing essential nutrients to enter the brain while excluding pathogens and poisons. The BBB neurovascular unit maintains vascular stability and neural equilibrium, and comprises of endothelial cells linked by tight junctions, pericytes tightly associated with the endothelial cells, and astrocytic endfeet.57
In the late 1800s, Paul Ehrlich’s dye tests showed that certain chemicals in the blood did not color brain tissue. This resulted in the hypothesis of a barrier separating the blood from the brain parenchyma.58 The selective shielding role remains crucial, as disruption to the BBB can lead to numerous neurological disorders, including inflammatory and viral diseases, meningitis, brain tumors, neurodegenerative syndromes such as Alzheimer’s disease, and traumatic brain injury.59,60 A network of tight junction proteins constitutes a fundamental component of the BBB’s architecture. These proteins constrict paracellular channels and maintain the low-permeability milieu characteristic of healthy cerebral vasculature. The effective pore size of healthy tight junctions is around 4 nm;61 however, when the barrier function is compromised, such as during inflammation or edema, these pores can significantly enlarge, occasionally reaching several hundred nanometers. The pathological BBB has increased permeability, detrimental to neural stability, offering prospects for NP-mediated drug delivery, enabling therapeutic NP medicines to penetrate brain tissue more readily than under normal conditions.62
Numerous strictly regulated mechanisms exist for drugs to traverse the BBB. This encompasses passive diffusion of small lipophilic molecules, restricted paracellular movement, carrier-mediated transport of glucose, amino acids, and other vital nutrients, ion-channel activity, adsorption-mediated transcytosis, receptor-mediated transcytosis via ligands such as transferrin or insulin, ATP-dependent efflux systems like P-glycoprotein, and diverse forms of endocytosis.58
Small, lipophilic compounds primarily cross the BBB through passive diffusion, enabled by their ability to incorporate into the lipid bilayer of the endothelial cell membrane. The capacity of a substance to diffuse in this manner is primarily influenced by three physicochemical properties: its capacity to establish hydrogen bonds, its molecular size, and its hydrophobic characteristics.58 Molecules under 500 Da with octanol-water partition coefficients favoring octanol by a factor of around 102–104 can readily traverse the BBB. Oxygen, carbon dioxide, caffeine, and ethanol exemplify typical substances. Conversely, ions and most tiny hydrophilic solutes can traverse other tissues via paracellular transport; however, the tight junctions of the brain capillaries effectively obstruct this pathway.58
Passive diffusion across the BBB relies on two primary transporter types: solute carrier (SLC) transporters and ATP-binding cassette (ABC) transporters. SLC proteins facilitate the transport of substances into and out of the cell, as well as the delivery of essential nutrients such as glucose and amino acids to the brain. Transmembrane proteins constitute ion channels, facilitating the movement of certain ions across the endothelium membrane.63 Seven subfamilies of ABC transporters predominantly reside on the luminal surface of BBB endothelial cells. Each transporter contains a transmembrane domain (TMD) and a cytosolic nucleotide-binding domain (NBD). P-glycoprotein (P-gp), encoded by ABCB1, is the most recognized of these. P-glycoprotein is present at several physiological barriers and functions as a potent efflux pump, aggressively eliminating xenobiotics and numerous therapeutic medicines from the central nervous system. The activity of P-glycoprotein presents a significant challenge for pharmaceuticals: even if a medicine penetrates endothelial cells, P-gp can inhibit its accumulation in the brain parenchyma.64,65 Larger molecules, including most NPs, typically depend on vesicular transport mechanisms to cross the BBB. These pathways include transcytosis, caveolae-mediated endocytosis, receptor-mediated endocytosis, macropinocytosis, and various forms of pinocytosis which are defined as:66,67
- Transcytosis is the process by which vesicles move from the luminal membrane to the abluminal membrane (or the other way around) through endothelial cells.68
- Caveolae-mediated endocytosis begins in lipid raft microdomains that are rich in caveolin, cholesterol, glycosphingolipids, sphingomyelin, and lipid-anchored glycoproteins. Caveolin (~22 kDa), characterized by cytosolic N- and C-termini, functions as a structural indicator of cellular integrity and is frequently dysregulated in cancer. Caveolae that have been internalized create vesicles that look like flasks. These vesicles then join together to form caveosomes, which then join together with lysosomes.69
- Clathrin-mediated endocytosis requires adaptor proteins, membrane receptors, phosphatidylinositol-4,5-bisphosphate (PIP2), GPCRs, and multiple accessory proteins that coordinate vesicle formation.70
- Macropinocytosis, on the other hand, makes big, uneven vesicles that take in fluid and matrix components from outside the cell. Actomyosin dynamics drive this process, and polypeptide growth factors usually speed it up.71
Even though these pathways work in many different types of cells, caveolae-mediated uptake, clathrin-coated pits, and micropinocytosis are some of the most important vesicular pathways in BBB endothelial cells. Their relative contributions are important for designing NPs that can deliver drugs to the CNS quickly and accurately.72
BBB Dysfunction in ASD
Alterations in the integrity and transport dynamics of the BBB may contribute to the neurobiological variability observed in ASD.73 Numerous documented issues, such as diminished levels of tight-junction proteins (eg, claudin-5), elevated concentrations of inflammatory mediators, and alterations in transporter expression, align with permeability and transport pathways previously discussed. The loss or impairment of tight junctions can transform the typical nm paracellular barrier into a significantly more porous interface, perhaps expanding to hundreds of nanometers. Although these conditions may temporarily promote the movement of NPs, they also allow the entry of unwanted solutes, microbial byproducts, and inflammatory mediators, hence worsening neuroinflammation and oxidative stress.74,75 Alterations in solute carrier (SLC) inflow mechanisms, ATP-binding cassette (ABC) efflux transporters, including P-glycoprotein (P-gp/ABCB1), and inflammation-responsive vesicular pathways, such as caveolae- and clathrin-mediated transcytosis, also modify the transendothelial transport of molecules. These alterations can either impede or facilitate the access of medications to the central nervous system, complicating the development of successful therapies. In this setting, BBB malfunction in ASD represents a “double-edged opportunity”: increased permeability may facilitate CNS entrance of therapeutic NPs, while also heightening the danger of off-target accumulation, immunological activation, and unpredictable pharmacokinetics.63,76,77
Consequently, the rational nanotechnological design for ASD should prioritize ligand-guided transcytosis over passive leakage. To mitigate cytokine-mediated inflammatory responses and protein corona formation, it is essential to tune the dimensions, surface charge, and chemical composition of NPs. Additional strategies to enhance safety and efficacy encompass the application of stealth coatings to circumvent efflux pumps, the engineering of NPs to evade recognition by P-glycoprotein, or the scheduling of doses to align with “windows” of transient permeability during regulated physiological or therapeutic conditions. However, these advantages must be evaluated meticulously to prevent exacerbating inflammation or damaging the BBB.78,79
One recent study by Ueno et al, provides a thorough review of BBB development, structure, and disease, with implications for ASD.80 The authors clarify the development of the BBB, comprising endothelial cells, pericytes, astrocytes, and basement membranes, via coordinated angiogenesis, cellular differentiation, and postnatal maturation. Cerebral microvascular endothelial cells display distinct features: robust tight and adherens junctions, limited basal pinocytosis, polarized transporter expression, and increased mitochondrial density. Astrocyte and pericyte signaling modulates vascular tone and BBB permeability, enhancing barrier stability.80
Additional research highlights a diverse range of BBB disruptors, encompassing genetic variants (eg, APOE4, SOD1, AQP4), oxidative stress, neuroinflammation, traumatic or hypoxic injury, and alterations in the gut and oral microbiome, which undermine tight junctions, dysregulate transporters, and potentially trigger microbleeds. The breakdown of the BBB appears to precede neuronal dysfunction or degeneration in multiple illnesses, including ASD, Alzheimer’s disease, Parkinson’s disease, and amyotrophic lateral sclerosis (ALS).81
Therapeutic approaches to address BBB dysfunction encompass neurosurgical delivery methods, chemical regulation of permeability, receptor-mediated “Trojan horse” systems, NP and exosome-based drug carriers, microbiome-targeted therapies, and stem cell techniques. Each possesses potential, yet, they must navigate trade-offs concerning specificity, safety, scalability, and translatability. The convergence of BBB processes in neurodevelopmental and neurodegenerative illnesses suggests the possibility of shared, biomarker-driven treatment methods, dependent on rigorous translational validation in future research.82,83
Nanoparticles (NPs) in ASD
NPs are materials that have at least one dimension between 1 and 100 nm and can be carefully designed to interact with biological systems at the molecular and cellular levels because they have a high surface-area-to-volume ratio, a tunable shape, and a surface chemistry that can be changed.84 These traits make it possible to control drug loading, deliver drugs to specific areas, make poorly bioavailable compounds more soluble, and improve pharmacokinetic behavior. In biomedical science, NPs include a wide range of platforms, such as polymeric NPs, liposomes, solid-lipid NPs, gold and magnetic nanostructures, dendrimers, and biomimetic or cell-membrane–coated vesicles. Each of these has its own benefits for use in therapy, diagnosis, and biosensing. NPs have become a revolutionary technology in modern drug delivery and neurotherapeutic research because they can cross physiological barriers, such as the BBB, and deliver active agents in a targeted, long-lasting, or stimulus-responsive way.85 In this article, we briefly talk about some of their new uses in ASD. The main focus is on how NPs can be used in drug-delivery systems, but we also mention other uses like biosensing and diagnostic platforms. Figure 3 depicts various applications of nanotechnology in ASD.
 |
Figure 3 Applications of nanotechnology in ASD (Created with BioRender.com). |
NP-Based Drug Delivery in ASD
A growing body of research demonstrates that nanocarriers can effectively deliver antioxidants, anti-inflammatory agents, neurotransmitter modulators, and gene-regulatory therapies, showing improved stability, bioavailability, and brain penetration.86 These methods are particularly advantageous for ASD87 since they circumvent significant challenges that diminish the efficacy of conventional small-molecule and biologic therapies, including inadequate solubility, rapid systemic clearance, and restricted transport across the BBB.88
Advancement by Lv et al involves microglia-targeted nanoformulated bumetanide. Bumetanide, an NKCC1 inhibitor, has produced variable outcomes in clinical trials; nevertheless, NP encapsulation may improve its therapeutic efficacy. They exhibited that PEG–PLA NPs administered into the medial prefrontal cortex (mPFC) of BTBR mice specifically modulated microglial reactivity and restored social novelty preference. The findings suggest that directing NPs precisely to microglia may rectify the limitations of systemic delivery and enhance the precision of existing ASD therapies.89
Nanocarriers composed of phytochemicals are increasingly gaining popularity. Naringenin and curcumin exemplify substances possessing antioxidant, anti-inflammatory, and neuroprotective properties. Nevertheless, when administered in free form, they exhibit poor solubility and rapidly degrade. Encapsulating NPs significantly enhances their pharmacokinetic characteristics. BBB entrance and concentration in the brain is an important factor for a NP in ASD treatment. As mentioned above, there are various routes for NP delivery via the BBB and dependent on their characteristics, NPs can use single or multiple approaches. However, the BBB transfer for pharmaceutical agents or macromolecules is extraordinarily meager - as low as just 1% of CNS drugs (out of 7000) can be transferred via the BBB and concentrate in the brain.90 Other research indicated that less than 5% of CNS-targeted candidate drugs progress from preclinical to clinical stage, because of in adequate brain penetration.91 Therefore, encapsulating a pharmaceutical agent within nanoplatforms leads to higher BBB entrance resulting in better efficiency.58 Scientists are designing various NP structures to improve their BBB entrance.88 For example, Chen et al designed a SPIO NP coated with PEG and insulin that were transferred via the BBB by 24.47% via intraperitoneal injection.92 In another study, it was observed that 60% of DNAzyme-loaded nanoliposomes with a median size of 68 nm were transferred via the BBB of female BALB/c mice (healthy model) via intravenous administration.93 Another investigation by Ohta et al revealed that the size of holes created via external energy in the BBB were about 15–120 nm in ICR mice.94 These improvements developed position NP-mediated drug delivery as one of the most rapidly evolving and mechanistically innovative domains for ASD treatment. Despite being in its nascent phase, the integration of improved BBB permeability, precise administration, and biological specificity highlights nanomedicine as a crucial frontier for the development of future treatments for ASD. Table 3 provides critical studies on using NPs for enhanced drug delivery for ASD.
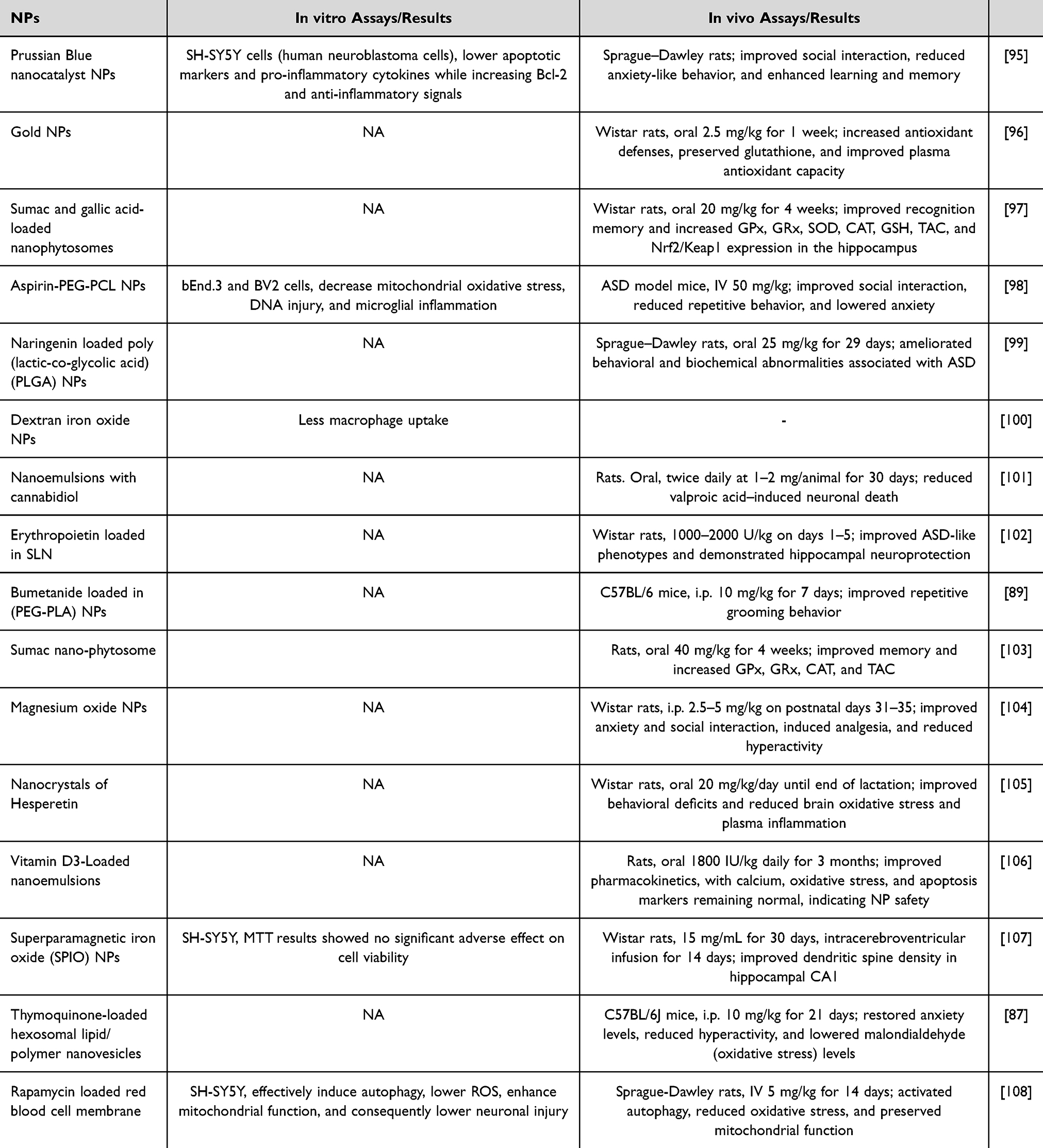 |
Table 3 Studies on NPs for Drug Delivery for ASD |
Nanoparticles as Tools for ASD Model Creation
Growing evidence suggests that NPs can influence neurodevelopmental pathways, leading to behavioral and biochemical alterations linked to ASD and ADHD.109–111 Besides their therapeutic use, NPs are emerging as experimental instruments for developing environmental, epigenetic, and transgenerational models of ASD.112,113 Ishido et al developed a silver NP (AgNP)-primed hyperactivity model, which is among the most intriguing findings today. In their study, pregnant mothers received a single oral dose of AgNPs on gestational day 7. For four successive generations, offspring were selectively bred for increased spontaneous motor activity levels. In the fourth generation, AgNP-primed rats exhibited a 1.8-fold increase in hyperactivity, indicating that a single prenatal exposure was sufficient to induce a persistent, heritable alteration in behavior. Conversely, early postnatal injection of valproic acid (VPA) - a conventional neurodevelopmental model of ASD/ADHD - resulted in a similar but less dramatic phenotype (1.4-fold increase in hyperactivity). Genome-wide DNA methylation analysis revealed convergent epigenetic patterns in the mesencephalon of hyperactive rats primed with AgNPs and treated with VPA. The fingerprints encompassed genes critical for neural maturation, synaptic function, transcriptional control, ubiquitination, DNA binding, and histone modification. Examples include Pax6 and Mecp2. The analogous epigenomic patterns suggest that NPs may act as environmental toxicants inducing ASD- and ADHD-like behaviors, as well as tools for modeling transgenerational, epigenetically mediated neurobehavioral syndromes - an investigative avenue that offers unique opportunities to examine heritable mechanisms in neurodevelopmental disorders.113
Another pertinent example is the research conducted by Notter et al which investigated whether prenatal exposure to titanium dioxide NPs (TiO2 NPs) alters brain development in mice.112 On gestational day 9, a critical period for fetal brain development, expectant dams received a single intravenous injection of either low-dose or high-dose TiO2 NPs. The progeny displayed dose-dependent behavioral abnormalities, marked by reduced neonatal ultrasonic vocalizations, compromised juvenile sociability, and heightened prepulse inhibition. These findings indicate essential and interconnected traits of ASD - difficulties in early communication, altered social behavior, and impairments in sensory-motor gating.112
The researchers observed no indications of maternal toxicity, complications during pregnancy, or significant fetal deformities. This indicates that TiO2 NPs may subtly disrupt neurodevelopment in manners that conventional teratological assessments cannot detect. This study provides substantial preliminary evidence that NPs often employed in consumer, industrial, and biomedical contexts may influence neurodevelopment and create environmentally linked ASD phenotypes.112 Moreover, TiO2 NPs offer a controlled and reproducible experimental paradigm for examining the impact of ambient nanomaterials on the risk of ASD.112 These findings collectively demonstrate that NPs can operate as model-inducing agents, enabling the exploration of environmental, epigenetic, and transgenerational factors affecting neurodevelopmental diseases. This dual function - therapeutic and pathogenic - underscores the imperative of rigorously assessing NP safety while harnessing their mechanistic promise for model advancement.112,113
NPs in ASD Diagnostics
Besides their therapeutic applications, NPs are increasingly significant in the development of advanced biosensing platforms for ASD. Their unique electrical, optical, and catalytic properties enable the precise detection of molecular biomarkers, advancing ASD assessment towards more objective, rapid, and physiologically pertinent methods. Nanomaterials (such as gold NPs, silicon nanowires, metal-organic frameworks (MOFs), and various carbon-based nanostructures) have proven highly beneficial due to their capacity to enhance signal amplification, improve surface-to-volume ratios, and significantly reduce detection limits.114
These nano-enabled biosensors have been employed to measure several biomarkers associated with ASD, including microRNAs (eg, miR-23a-3p, miR-146a, miR-132), inflammatory cytokines, and peptide markers such as β-casomorphin-7.115,116 Photoelectrochemical platforms utilizing gold NPs included in two-dimensional MOFs enable the detection of microRNAs associated with ASD without the need for labels. Likewise, silicon-on-insulator (SOI) nanowire devices enable the real-time measurement of circulating miRNA profiles associated with neurodevelopmental diseases.117,118 These technologies collectively potentially facilitate the identification of biomarkers with few or no adverse effects, enable early detection, and monitor the efficacy of treatments for each individual.117,118
Ivanov et al developed an ultrasensitive silicon-on-insulator nanowire nanosensor (SOI-NS) for the detection of microRNAs in ASD.119 The device comprises a CMOS-compatible array of nanowire sensing elements fabricated by gas-phase etching and sophisticated nanolithography techniques. Subsequently, sequence-specific oligonucleotide probes were introduced to facilitate their functionality. The authors employed this approach to directly quantify microRNAs associated with ASD from human plasma. The application of synthetic miRNA analogues in a buffer yielded an exceptionally low detection limit of 10−17 M. This research demonstrates that nanostructured semiconductor sensors can detect biomarkers with great precision and without the necessity for labeling. This represents a viable avenue for objective ASD diagnostics.119 Alosaimi et al developed an environmentally sustainable fluorescent nanosensing probe for the quantification of atomoxetine, a medication commonly utilized to alleviate ADHD symptoms in individuals with ASD.120 This serves as an additional exemplary instance. The researchers synthesized carbon quantum dots (CQDs) from black-eyed pea beans and subsequently included an atomoxetine–tetraphenylborate combination. The resultant nano-probe enabled rapid and highly specific detection of atomoxetine through fluorescence quenching in both pharmaceutical formulations and human plasma. The platform demonstrated exceptional analytical performance, according to all ICH validation standards, and was utilized in a pharmacokinetic study including autistic children with ADHD. This research highlights the therapeutic relevance of carbon-based nanomaterials as sensitive, sustainable, and scalable sensors for drug monitoring in neurodevelopmental care. These advancements indicate that NP-based diagnostics could improve behavioral evaluation, enabling earlier identification, biological stratification, and individualized monitoring of ASD.120
Other Nanotechnology Applications in ASD
NP systems have been adapted for gene-regulatory therapies, including siRNA- and microRNA-based approaches. Polymeric and lipid NPs can facilitate the delivery of nucleic acids to dysregulated pathways such as SHANK3 and MECP2; these applications remain predominantly experimental121,122 however they do introduce a non-viral, ultrasound-facilitated BDNF gene delivery method in a valproic acid (VPA) rat model of ASD. Shen et al designed brain-derived neurotrophic factor plasmid-loaded cationic microbubbles (BDNFp-CMBs), showcasing their significant plasmid loading efficiency and adequate in vivo durability. CMBs exhibited an average particle size of 1.33 ± 0.24 µm with a surface zeta potential of 29.8 mV. During treatment, BDNFp-CMBs were administered intravenously, while focused ultrasound (FUS) was applied transcranially to the prefrontal cortex (PFC) to transiently disrupt the BBB and facilitate local plasmid uptake (sonoporation). Ultrasound in combination with lipid microbubbles effectively and non-invasively opened the BBB, enabling enhanced delivery of BDNF to the brain. Evans blue staining revealed BBB disruption in the ultrasound-irradiated prefrontal cortex, while non-sonicated regions showed no staining. Consistently, fluorescence imaging demonstrated strong signals only in ultrasound-treated areas, confirming localized BBB opening. This technique enhanced BDNF production in the PFC, improved stereotyped, exploratory, and social behaviors, and partially restored neuronal morphology and synaptic ultrastructure upon electron microscopy compared to untreated VPA mice.123
Furthermore, nanomedicine establishes a conceptual connection between the beneficial effects of fever/hyperthermia on ASD symptoms and targeted, controllable therapies. Clinical and preclinical evidence suggests that temporary elevations in body or brain temperature may briefly improve social behavior and reduce repetitive symptoms in individuals or animal models with ASD, likely by influencing neuroinflammation, synaptic function, and neuromodulatory systems.124,125 Magnetically responsive or thermosensitive nanocarriers may replicate this “fever-like” condition in a spatially and temporally regulated manner - either by inducing mild, localized hyperthermia in specific brain regions or by associating heat generation with the controlled release and solubility enhancement of ASD-relevant pharmaceuticals.124 Ansari et al demonstrated that superparamagnetic nanoparticles can generate localized heat under an alternating magnetic field to induce in situ drug amorphization within oral solid dosage forms, thereby enhancing drug dissolution and bioavailability without compromising dosage form integrity. TEM analysis with log-normal distribution fitting revealed primary particle sizes of 17.6 nm and 17.3 nm for zinc ferrite and manganese ferrite nanoparticles, respectively, indicating a narrow size distribution suitable for effective magnetic hyperthermia.124
Additionally, nanozymes (that is, catalytic nanomaterials with enzyme-mimetic antioxidant capabilities) have been studied for their ability to alleviate oxidative stress and neuroinflammation, both acknowledged contributors to the pathogenesis of ASD. A restricted but growing body of research has examined NP-mediated hyperthermia and photothermal therapy, particularly gold and carbon nanomaterials, as potential regulators of neuroinflammatory responses; nonetheless, these approaches remain predominantly experimental concerning neurodevelopmental disorders. These exploratory applications illustrate the considerable therapeutic and mechanistic potential of nanotechnology in ASD research; nonetheless, most remain in the conceptual or early preclinical stages and require substantial validation before clinical application.126,127 Feng et al reported the development of a calcium hexacyanoferrate (III) (CaH) nanocatalyst designed to restore redox homeostasis as a therapeutic strategy for autism spectrum disorder. The study demonstrated that CaH nanocrystals effectively regulated oxidative stress and neuroinflammation, leading to a significant improvement in neurobehavioral outcomes. TEM images revealed the near-spherical morphology of CaH nanocrystals with an average size of 2.6 nm, while zeta potential measurements showed values of −9.4 mV in water, −21.0 mV in phosphate-buffered saline, and −9.8 mV in Dulbecco’s modified Eagle medium, indicating medium-dependent surface charge behavior and good colloidal stability.127
Gong et al present a detailed example by engineering Prussian blue NPs (PB NPs) to serve as multi-enzyme-mimetic nanozymes for ASD therapy. These PB NPs are designed to function as superoxide dismutase, glutathione peroxidase, catalase, and peroxidase, rendering them broad-spectrum antioxidants in the brain. In preclinical ASD models, systemic injection of PB NPs leads to substantial scavenging of reactive oxygen species and the re-establishment of redox equilibrium. TEM images showed that Prussian blue nanoparticles (PB NPs) exhibited a cubic morphology with an average size of approximately 30 nm. Confocal laser scanning microscopy (CLSM) following live/dead staining confirmed that PB NPs effectively preserved cell viability. Furthermore, flow cytometry analysis demonstrated that PB NP treatment markedly reduced apoptosis induced by H2O2 and VPA, with apoptosis rates decreasing from 26.3% to 10.9% and from 24.5% to 7.3%, respectively.95 This molecular alteration is evidenced by the diminished activation of apoptotic markers, such as cleaved caspase-3 and Bcl-2–associated X protein, along with an elevation in the anti-apoptotic protein Bcl-2. Simultaneously, PB NPs mitigate neuroinflammation by decreasing pro-inflammatory cytokines and increasing anti-inflammatory cytokines, so preventing glial overactivation. These synergistic antioxidant, anti-apoptotic, and anti-inflammatory properties enhance social interaction, reduce anxiety-like behavior, and elevate cognitive performance in ASD-like animals, illustrating the therapeutic potential of nanozymes in recalibrating oxidative and inflammatory pathways associated with ASD pathology.95
Toxicity Issues of NPs
Paying attention to NP distribution and their side effects are essential matters when designing a nanoplatform. Nanoplatforms can induce toxicity issues due to their interactions within other cellular structures and also because of their loaded agent.128 Various factors determine NP toxicity such as mean diameter, zeta potential, use of targeting agents and their components.129 To clearly define nanoformulation safety, various steps should be completed which are the same as ones for drug screening and to make them ready for commercialization. According to the regulatory guidelines for drug screening, ADME (Absorption, Distribution, Metabolism, and Excretion) and QSAR (Quantitative Structure–Activity Relationship) should be performed followed by in vitro cytotoxicity assays and preclinical examination. After complete fulfilment of preclinical assays from acute to chronic trials, clinical trials can be started.130,131 It is stated that NP toxicity management contains eight steps including: foundation of safety issues just for the nanoformulation, identification of NPs with biological moiety interactions, identification of their permeability within barriers such as the BBB, accurate dose escalation of NPs, determining standards for NP bio-fate, extension of data regarding NP biodistribution, determination of international standards, and modification of regulatory issues.129
Clinical Trials and Future Directions
To date in 2026, NP-based therapies for ASD have had limited applications in clinical environments. One recent comprehensive analysis concluded that “there is currently no established nanomedicine treatment specifically designed for ASD”.132 An examination of prominent clinical-trial registries identified a study concerning a nano-encapsulated probiotic formulation (K11-TMAX) intended to mitigate gut-brain axis inflammation in children with ASD (ClinicalTrials.gov identifier NCT06382909); nonetheless, this intervention is categorized as a nutraceutical rather than a brain-targeted nanotherapeutic. This was a randomized, double-blind Phase III clinical trial (NCT06382909) evaluating a probiotic-based, partly nano-encapsulated intervention in children aged 3 to 11 years with ASD. The researchers analyzed three groups: (1) a placebo, (2) K11-T probiotic alone, and (3) K11-Tmax, which is the same probiotic supplemented with amino acids, fatty acids, and vitamins. The primary objective was to evaluate whether K11-T and K11-Tmax improve neuropsychiatric, sociopedagogical, and inflammatory outcomes in ASD.
Sociodemographic and clinical characteristics characterized the children, thereafter assessed using three validated scales: Vineland-3 (adaptive behavior; parent report), ADOS (core autistic symptoms; clinician evaluation), and CARS (severity; teacher report). The study concurrently assessed serum biomarkers (insulin, C-reactive protein, prolactin, cortisol) and fecal calprotectin to examine inflammatory and metabolic impacts. Finally, it evaluated the impact of the enhanced K11-Tmax formulation on behavior, cognition, education, and inflammation in comparison to K11-T alone. This suggested gut-brain-microbiota manipulation as a potential supplementary approach for controlling ASD.
Unfortunately, no further registered trials have been located for NPs particularly designed for drug transport across the BBB, nano-enabled imaging, or nano-therapies in ASD populations. This highlights a significant disparity between promising preclinical research and human studies, indicating the necessity for rigorous clinical trials to ascertain the safety, efficacy, and feasibility of NP-based methods for individuals with ASD.132
Future advances in nanotechnology may enable more effective therapeutic strategies for ASD, particularly through the development of combinational NP-based drug delivery systems that address the disorder’s multifactorial pathophysiology. By co-delivering multiple therapeutic agents, nanocarriers may simultaneously modulate neuroinflammation, synaptic dysfunction, and immune dysregulation, thereby improving treatment outcomes compared with conventional monotherapies.133 Moreover, the design of more sophisticated nanoparticles, including surface-modified and multifunctional platforms, holds promise for enhancing BBB penetration targeting specific neural or immune cell populations, and achieving controlled drug release within the brain microenvironment.134 Although these approaches remain largely preclinical, rigorous safety assessments, standardized characterization, and well-designed clinical trials will be essential to translate advanced nanomedicine strategies into effective and personalized therapies for ASD.135 Figure 4 shows the completed Phase III clinical trial for ASD, highlighting the applied nanoformulation and eligibility criteria, as well as future perspectives on the use of innovative nanodrug-based strategies in ASD.
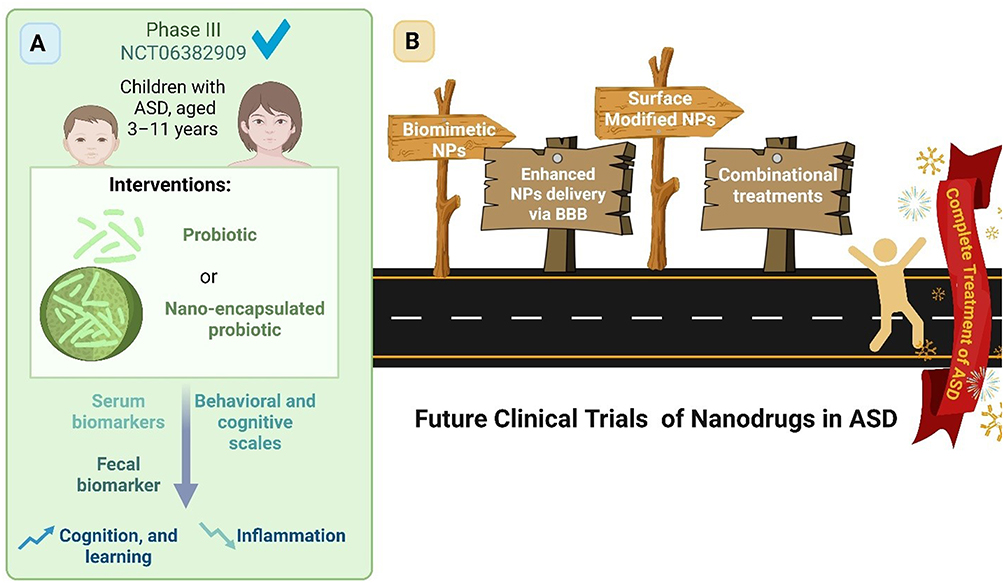 |
Figure 4 Clinical trials of ASD. (A) The completed Phase III clinical trial, including the criteria and nanoformulation applied. (B) Future perspectives on the use of innovative nanodrugs in ASD. |
Conclusions
ASD is a multifactorial neurodevelopmental condition involving dysregulation of molecular signaling pathways, synaptic function, immune responses, and large-scale brain connectivity, for which current therapeutic strategies remain largely limited to symptomatic management. Nanomedicine expresses a promising approach in ASD treatment, diagnosis and model creation. Nanoparticles enable the rational design of advanced formulations with enhanced stability, controlled release profiles, and improved penetration across the BBB, thereby increasing therapeutic efficacy while minimizing systemic adverse effects. However, despite encouraging preclinical outcomes, the clinical translation of NP-based therapies for ASD remains limited, highlighting a substantial gap between experimental research and human studies. Addressing this gap will require rigorously designed clinical trials to establish safety, efficacy, and feasibility, as well as continued interdisciplinary collaboration integrating nanotechnology, neuroscience, and clinical research. Collectively, these efforts may enable nanomedicine-based strategies to advance ASD treatment beyond symptom control toward mechanism-driven and personalized therapeutic interventions.
Acknowledgments
The authors would like to express their sincere gratitude to Christopher Brasher, FANZCA, from the Department of Anaesthesia and Pain Management, Royal Children’s Hospital, Melbourne, Australia, for his invaluable guidance, clinical insight, and constructive feedback during the development of this manuscript.
Disclosure
The authors declare no competing interest.
References
1. Abed M. A comprehensive examination of human brain disorders. J Biomed Sustain Healthc Applicat. 2023;3(2):141–20. doi:10.53759/0088/JBSHA202303014
2. Atashgahi M, Ghaemi B, Valizadeh A, Moshiri A, Nekoofar MH, Amani A. Epinephrine-entrapped chitosan nanoparticles covered by gelatin nanofibers: a bi-layer nano-biomaterial for rapid hemostasis. Int J Pharm. 2021;608:121074. doi:10.1016/j.ijpharm.2021.121074
3. Patel MM, Patel BM. Crossing the blood–brain barrier: recent advances in drug delivery to the brain. CNS Drugs. 2017;31(2):109–133. doi:10.1007/s40263-016-0405-9
4. Santomauro DF, Erskine HE, Herrera AMM, et al. The global epidemiology and health burden of the autism spectrum: findings from the global burden of disease study 2021. Lancet Psychiatry. 2025;12(2):111–121. doi:10.1016/S2215-0366(24)00363-8
5. Sacco R, Camilleri N, Eberhardt J, Umla-Runge K, Newbury-Birch D. The prevalence of autism spectrum disorder in Europe. In: Autism Spectrum Disorders-Recent Advances and New Perspectives. InTech – Open Access Publisher; 2022.
6. Li Y-A, Chen Z-J, Li X-D, et al. Epidemiology of autism spectrum disorders: global burden of disease 2019 and bibliometric analysis of risk factors. Front Pediat. 2022;10:972809. doi:10.3389/fped.2022.972809
7. Grosvenor LP, Croen LA, Lynch FL, et al. Autism diagnosis among US children and adults, 2011-2022. JAMA Network Open. 2024;7(10):e2442218. doi:10.1001/jamanetworkopen.2024.42218
8. McConkey R. Responding to autism in low and middle income countries (LMIC): what to do and what not to do. Brain Sci. 2022;12(11):1475. doi:10.3390/brainsci12111475
9. Ahsan K. Autism spectrum disorder: a global public health challenge. Mugda Med Coll J. 2025;8(1):1–2. doi:10.3329/mumcj.v8i1.82807
10. Kiogora N. Exploring common co-occurring conditions like ADHD, anxiety, depression and epilepsy in individuals with autism and how to manage these additional challenges. Int Acad J Health Med Nurs. 2025;2(2):39–49.
11. Kanner L. Autistic disturbances of affective contact. Nervous Child. 1943;2(3):217–250.
12. Havdahl A, Niarchou M, Starnawska A, Uddin M, van der Merwe C, Warrier V. Genetic contributions to autism spectrum disorder. Psychol Med. 2021;51(13):2260–2273. doi:10.1017/S0033291721000192
13. Chung K-M, Chung E, Lee H. Behavioral interventions for autism spectrum disorder: a brief review and guidelines with a specific focus on applied behavior analysis. J Korean Acad Child Adolesc Psychiatry. 2024;35(1):29. doi:10.5765/jkacap.230019
14. Ehterami A, Abbaszadeh-Goudarzi G, Haghi-Daredeh S, et al. Bone tissue engineering using 3-D polycaprolactone/gelatin nanofibrous scaffold containing berberine: in vivo and in vitro study. Polym Adv Technol. 2022;33(2):672–681. doi:10.1002/pat.5549
15. Ferraris C, Cavalli R, Panciani PP, Battaglia L. Overcoming the blood–brain barrier: successes and challenges in developing nanoparticle-mediated drug delivery systems for the treatment of brain tumours. In: International Journal of Nanomedicine. Taylor & Francis; 2020:2999–3022.
16. Al-Dujaili Z, Al Faraj A. Would nanoparticles give hope for the treatment of autism spectrum disorder? In: Review Journal of Autism and Developmental Disorders. Springer Nature; 2024:1–7.
17. Lord C, Elsabbagh M, Baird G, Veenstra-Vanderweele J. Autism spectrum disorder. Lancet. 2018;392(10146):508–520. doi:10.1016/S0140-6736(18)31129-2
18. Mukherjee SB. Identification, evaluation, and management of children with autism spectrum disorder: American academy of pediatrics 2020 clinical guidelines. Indian Pediatr. 2020;57(10):959–962. doi:10.1007/s13312-020-2003-7
19. Valaparambil KA, Sundaram S. Autism spectrum disorder and epilepsy: point of convergence or divergence. Int J Epilepsy. 2025;11(1) doi:10.1055/s-0045-1809042
20. Canitano R, Bozzi Y, Dhossche D. Autism Spectrum Disorders: Developmental Trajectories, Neurobiological Basis, Treatment Update, Volume 2. Vol. 11. Frontiers Media SA; 2020:589.
21. Lordan R, Storni C, De Benedictis CA. Autism spectrum disorders: diagnosis and treatment; 2021.
22. Li H, Zhang J. Advancements in nanotechnology for autism spectrum disorder: innovative strategies in pediatric neurology. Developl Neurobiol. 2025;85(3):e22989. doi:10.1002/dneu.22989
23. Jiang -C-C, Lin L-S, Long S, et al. Signalling pathways in autism spectrum disorder: mechanisms and therapeutic implications. Signal Transd Target Ther. 2022;7(1):229. doi:10.1038/s41392-022-01081-0
24. Sala C, Vicidomini C, Bigi I, Mossa A, Verpelli C. Shank synaptic scaffold proteins: keys to understanding the pathogenesis of autism and other synaptic disorders. J Neurochem. 2015;135(5):849–858. doi:10.1111/jnc.13232
25. Sun L. Computational analysis of autism-associated genetic mutation on the interaction between neurexin and neuroligin. Int J High School Res. 2024;6(1). doi:10.36838/v6i1.1
26. Huang C, Voglewede MM, Ozsen EN, Wang H, Zhang H. SHANK3 mutations associated with autism and schizophrenia lead to shared and distinct changes in dendritic spine dynamics in the developing mouse brain. Neuroscience. 2023;528:1–11. doi:10.1016/j.neuroscience.2023.07.024
27. Berg EL, Copping NA, Rivera JK, et al. Developmental social communication deficits in the Shank3 rat model of phelan-mcdermid syndrome and autism spectrum disorder. Autism Res. 2018;11(4):587–601. doi:10.1002/aur.1925
28. Port RG, Oberman LM, Roberts TP. Revisiting the excitation/inhibition imbalance hypothesis of ASD through a clinical lens. Br J Radiol. 2019;92(1101):20180944. doi:10.1259/bjr.20180944
29. Canitano R, Palumbi R. Excitation/inhibition modulators in autism spectrum disorder: current clinical research. Front Neurosci. 2021;15:753274. doi:10.3389/fnins.2021.753274
30. Pietropaolo S, Provenzano G. Targeting Excitation-Inhibition Imbalance in Neurodevelopmental and Autism Spectrum Disorders. Vol. 16. Frontiers Media SA; 2022:968115.
31. Ellul P, Maruani A, Vantalon V, et al. Maternal immune activation during pregnancy is associated with more difficulties in socio-adaptive behaviors in autism spectrum disorder. Sci Rep. 2023;13(1):17687. doi:10.1038/s41598-023-45060-z
32. Tang Q, Wang X, Yang F, et al. Pathophysiological associations between maternal immune activation and neurodevelopmental disorders in offspring: a comprehensive review. Front Endocrinol. 2025;16:1681190. doi:10.3389/fendo.2025.1681190
33. Woods RM, Lorusso JM, Fletcher J, et al. Maternal immune activation and role of placenta in the prenatal programming of neurodevelopmental disorders. Neuronal Signal. 2023;7(2):NS20220064. doi:10.1042/NS20220064
34. Thomas SD, Jha NK, Ojha S, Sadek B. mTOR signaling disruption and its association with the development of autism spectrum disorder. Molecules. 2023;28(4):1889. doi:10.3390/molecules28041889
35. Drehmer I, Santos-Terra J, Gottfried C, Deckmann I. mTOR signaling pathway as a pathophysiologic mechanism in preclinical models of autism spectrum disorder. Neuroscience. 2024;563:33–42. doi:10.1016/j.neuroscience.2024.10.050
36. Narzisi A, Halladay A, Masi G, Novarino G, Lord C. Tempering expectations: considerations on the current state of stem cells therapy for autism treatment. Frontiers in Psychiatry. 2023;14:1287879. doi:10.3389/fpsyt.2023.1287879
37. Abboud A-H, Abd D, Raheem AL-Gharrrawi SA. Evaluation of serum level of IL-6 and TNF-α in children with autism. Mag Al-Kufa Univ Biol. 2025;17(1). doi:10.36320/ajb/v17.i1.18142
38. Sellmann H, Williams JE, Udekwu K, et al. The relationship between infant feeding types, gut microbiome, intestinal inflammation, and neurodevelopment in a neonatal piglet model. J Parenteral Enteral Nutr. 2025;50(1):121–130.
39. Deady C, FitzGerard J, Kara N, et al. Maternal immune activation and antibiotics affect offspring neurodevelopment, behaviour, and microbiome. Brain Behav Immun Health. 2025;48:101065. doi:10.1016/j.bbih.2025.101065
40. Campanale A, Mir H-D, Dumais E, et al. Uncovering novel endocannabinoidome-gut microbiome-brain axis-based therapeutic targets in a fragile X syndrome mouse model. Prog Neuro Psychopharmacol Biol Psychiatry. 2025;144:111575. doi:10.1016/j.pnpbp.2025.111575
41. Novau-Ferré N, Papandreou C, Rojo-Marticella M, Canals-Sans J, Bulló M. Gut microbiome differences in children with attention deficit hyperactivity disorder and autism spectrum disorder and effects of probiotic supplementation: a randomized controlled trial. Res Develop Disabilit. 2025;161:105003. doi:10.1016/j.ridd.2025.105003
42. Dargenio VN, Dargenio C, Castellaneta S, et al. Intestinal barrier dysfunction and microbiota–gut–brain axis: possible implications in the pathogenesis and treatment of autism spectrum disorder. Nutrients. 2023;15(7):1620. doi:10.3390/nu15071620
43. Baribeau D, Vorstman J, Anagnostou E. Novel treatments in autism spectrum disorder. Curr Opin Psychiatry. 2022;35(2):101–110. doi:10.1097/YCO.0000000000000775
44. Tarver J, Palmer M, Webb S, et al. Child and parent outcomes following parent interventions for child emotional and behavioral problems in autism spectrum disorders: a systematic review and meta-analysis. Autism. 2019;23(7):1630–1644. doi:10.1177/1362361319830042
45. Girma DA, Hailu BH, Malle AY. Effects of parent and teacher mediated pivotal response treatment and discrete-trial training in improving communication skills of children with autism. Can J Fam Youth. 2024;16(3):1–21.
46. Lovaas OI. Behavioral treatment and normal educational and intellectual functioning in young autistic children. J Consult Clin Psychol. 1987;55(1):3. doi:10.1037/0022-006X.55.1.3
47. Fard YA, Sadeghi EN, Pajoohesh Z, et al. Epigenetic underpinnings of the autistic mind: histone modifications and prefrontal excitation/inhibition imbalance. Am J Med Gene Part B. 2024;195(8):e32986. doi:10.1002/ajmg.b.32986
48. Lax L, Yanchik A, Vietze P, Vietze D. ABA curricula effects on toddler language, cognition and ASD symptoms. Autism. 2023;12:354.
49. Shayestehfar M, Nakhostin-Ansari A, Jahandideh P, Memari S, Geoffrey Louie W-Y, Memari A. Pivotal response treatment and applied behavior analysis interventions for autism spectrum disorder delivered by human vs robotic agents: a systematic review of literature. Disability Rehabil. 2025;20(2):286–297. doi:10.1080/17483107.2024.2382906
50. Wong C, Odom SL, Hume KA, et al. Evidence-based practices for children, youth, and young adults with autism spectrum disorder: a comprehensive review. J Autism Develop Disord. 2015;45(7):1951–1966. doi:10.1007/s10803-014-2351-z
51. Vivanti G. Autism and autism treatment: evolution of concepts and practices from Kanner to contemporary approaches. In: Clinical Guide to Early Interventions for Children with Autism. Springer; 2020:1–24.
52. Mohammadzaheri F, Koegel LK, Rezaee M, Rafiee SM. A randomized clinical trial comparison between pivotal response treatment (PRT) and structured applied behavior analysis (ABA) intervention for children with autism. J Autism Develop Disord. 2014;44(11):2769–2777. doi:10.1007/s10803-014-2137-3
53. Zanatta A, Siew J, Van der Paelt S, Warreyn P, Roeyers H. Developmental, behavioural and NDBI interventions in autistic children or at elevated likelihood of autism: a systematic review of neural outcomes. In: Review Journal of Autism and Developmental Disorders. Springer; 2024:1–23.
54. Yatawara C, Einfeld S, Hickie I, Davenport T, Guastella A. The effect of oxytocin nasal spray on social interaction deficits observed in young children with autism: a randomized clinical crossover trial. Mol Psychiatry. 2016;21(9):1225–1231. doi:10.1038/mp.2015.162
55. Hellings J. Pharmacotherapy in autism spectrum disorders, including promising older drugs warranting trials. World J Psychiatry. 2023;13(6):262. doi:10.5498/wjp.v13.i6.262
56. Stepanova E, Dowling S, Phelps M, Findling RL. Pharmacotherapy of emotional and behavioral symptoms associated with autism spectrum disorder in children and adolescents. Dialogues Clin Neurosci. 2017;19(4):395–402. doi:10.31887/DCNS.2017.19.4/rfindling
57. Moghe S. A double-edged sword: the blood-brain barrier. Berkeley Sci J. 2024;29(1). doi:10.5070/BS329164921
58. Madani F, Esnaashari SS, Webster TJ, Khosravani M, Adabi M. Polymeric nanoparticles for drug delivery in glioblastoma: state of the art and future perspectives. J Control Release. 2022;349:649–661. doi:10.1016/j.jconrel.2022.07.023
59. Wong AD, Ye M, Levy AF, Rothstein JD, Bergles DE, Searson PC. The blood-brain barrier: an engineering perspective. Front Neuroeng. 2013;6:7. doi:10.3389/fneng.2013.00007
60. Castro Dias M, Coisne C, Baden P, et al. Claudin-12 is not required for blood–brain barrier tight junction function. Fluids Barriers CNS. 2019;16(1):30. doi:10.1186/s12987-019-0150-9
61. Daneman R, Prat A. The blood–brain barrier. Cold Spring Harbor Perspect Biol. 2015;7(1):a020412. doi:10.1101/cshperspect.a020412
62. Jena L, McErlean E, McCarthy H. Delivery across the blood-brain barrier: nanomedicine for glioblastoma multiforme. Drug Delivery Transl Res. 2020;10(2):304–318. doi:10.1007/s13346-019-00679-2
63. Giacomini KM, Yee SW, Koleske ML, et al. New and emerging research on solute carrier and ATP binding cassette transporters in drug discovery and development: outlook from the international transporter consortium. Clin Pharmacol Ther. 2022;112(3):540–561. doi:10.1002/cpt.2627
64. Alam A, Locher KP. Structure and mechanism of human ABC transporters. Annu Rev Biophys. 2023;52(1):275–300. doi:10.1146/annurev-biophys-111622-091232
65. Shan Y, Cen Y, Zhang Y, et al. Acyclovir brain disposition: interactions with P-gp, Bcrp, Mrp2, and Oat3 at the blood–brain barrier. Eur J Drug Metabol Pharmacokinet. 2022;47(2):279–289. doi:10.1007/s13318-021-00733-w
66. Preston JE, Abbott NJ, Begley DJ. Transcytosis of macromolecules at the blood–brain barrier. Adv Pharmacol. 2014;71:147–163.
67. Tashima T. Smart strategies for therapeutic agent delivery into brain across the blood–brain barrier using receptor-mediated transcytosis. Chem Pharm Bull. 2020;68(4):316–325. doi:10.1248/cpb.c19-00854
68. Ayloo S, Gu C. Transcytosis at the blood–brain barrier. Curr Opin Neurobiol. 2019;57:32–38. doi:10.1016/j.conb.2018.12.014
69. Chen Z, DS Oliveira S, Zimnicka AM, et al. Reciprocal regulation of eNOS and caveolin-1 functions in endothelial cells. Mol Biol Cell. 2018;29(10):1190–1202. doi:10.1091/mbc.E17-01-0049
70. Selz B. Divergent Nuclear Signaling Pathways of Β-1 and Β-2 Adrenergic Receptors: Mechanisms and Functional Implications. Davis: University of California; 2025.
71. Salloum G, Bresnick AR, Backer JM. Macropinocytosis: mechanisms and regulation. Biochem J. 2023;480(5):335–362. doi:10.1042/BCJ20210584
72. Zhang C-L, Ma -J-J, Li X, et al. The role of transcytosis in the blood-retina barrier: from pathophysiological functions to drug delivery. Front Pharmacol. 2025;16:1565382. doi:10.3389/fphar.2025.1565382
73. Digonnet M, Chevin M, Alfaidy N, Raia-Barjat T, Giraud A, Sébire G. Restricted fetal blood brain barrier permeability in a preclinical model of autism induced by group B Streptococcus maternal immune activation. J Dev Orig Health Dis. 2025;16:e30. doi:10.1017/S2040174425100147
74. Wu D, Chen Q, Chen X, Han F, Chen Z, Wang Y. The blood–brain barrier: structure, regulation and drug delivery. Signal Trans Target the. 2023;8(1):217. doi:10.1038/s41392-023-01481-w
75. Ivashkin V, Poluektov Y, Kogan E, et al. Disruption of the pro-inflammatory, anti-inflammatory cytokines and tight junction proteins expression, associated with changes of the composition of the gut microbiota in patients with irritable bowel syndrome. PLoS One. 2021;16(6):e0252930. doi:10.1371/journal.pone.0252930
76. Deckmann I, Santos-Terra J, Fontes-Dutra M, et al. Resveratrol prevents brain edema, blood–brain barrier permeability, and altered aquaporin profile in autism animal model. Int J Dev Neurosci. 2021;81(7):579–604. doi:10.1002/jdn.10137
77. Gozal E, Jagadapillai R, Cai J, Barnes GN. Potential crosstalk between sonic hedgehog-wingless-related integration site signaling and neurovascular molecules: implications for blood brain barrier integrity in autism spectrum disorder. J Neurochem. 2021;159(1):15. doi:10.1111/jnc.15460
78. Bhandari R, Paliwal JK, Kuhad A. Enhanced bioavailability and higher uptake of brain-targeted surface engineered delivery system of naringenin developed as a therapeutic for autism spectrum disorder. Curr Drug Deliv. 2023;20(2):158–182. doi:10.2174/1567201819666220303101506
79. Bhor SD, Chaudhari VS, Lade SN, et al. Novel therapeutic strategies for neuropsychiatric treatments: targeted and controlled drug delivery approaches. In: Biomedical Materials & Devices. Springer; 2025:1–29.
80. Ueno M, Chiba Y, Murakami R, et al. Transporters, ion channels, and junctional proteins in choroid plexus epithelial cells. Biomedicines. 2024;12(4):708. doi:10.3390/biomedicines12040708
81. Merelli A, Repetto M, Lazarowski A, Auzmendi J. Hypoxia, oxidative stress, and inflammation: three faces of neurodegenerative diseases. J Alzheimers Dis. 2021;82(s1):S109–S126. doi:10.3233/JAD-201074
82. Aragón-González A, Shaw PJ, Ferraiuolo L. Blood–brain barrier disruption and its involvement in neurodevelopmental and neurodegenerative disorders. Int J Mol Sci. 2022;23(23):15271. doi:10.3390/ijms232315271
83. Ibarra LE. Cellular Trojan Horses for Delivery of Nanomedicines to Brain Tumors: Where Do We Stand and What Is Next? Vol. 16. Taylor & Francis; 2021:517–522.
84. Dolai J, Mandal K, Jana NR. Nanoparticle size effects in biomedical applications. ACS Appl Nano Mater. 2021;4(7):6471–6496. doi:10.1021/acsanm.1c00987
85. Madani F, Mujokoro B, Mohammadi S, Khosravani M, Adabi M. Chitosan/PVA nanofibers for implantable drug delivery systems. Nanomed Res J. 2022;7(2):150–155.
86. Madani F, Khosravani M, Adabi M. PLGA nanoparticles loaded with cinnamon extract and coated with PVA/poloxamer188.
87. Eissa N, Alwattar JK, Jayaprakash P, et al. The effects of novel thymoquinone-loaded nanovesicles as a promising avenue to modulate autism associated dysregulation by restoring oxidative stress in autism in mice. Int J Nanomed. 2025;20:8041–8061. doi:10.2147/IJN.S509158
88. Madani F, Morovvati H, Webster TJ, et al. Combination chemotherapy via poloxamer 188 surface-modified PLGA nanoparticles that traverse the blood–brain–barrier in a glioblastoma model. Sci Rep. 2024;14(1):19516. doi:10.1038/s41598-024-69888-1
89. Lv H, Gu X, Shan X, et al. Nanoformulated bumetanide ameliorates social deficiency in BTBR mice model of autism spectrum disorder. Front Immunol. 2022;13:870577. doi:10.3389/fimmu.2022.870577
90. Thangudu S, Cheng F-Y, Su C-H. Advancements in the blood–brain barrier penetrating nanoplatforms for brain related disease diagnostics and therapeutic applications. Polymers. 2020;12(12):3055. doi:10.3390/polym12123055
91. Dong X. Current strategies for brain drug delivery. Theranostics. 2018;8(6):1481. doi:10.7150/thno.21254
92. Chen J, Yuan M, Madison CA, Eitan S, Wang Y. Blood-brain barrier crossing using magnetic stimulated nanoparticles. J Control Release. 2022;345:557–571. doi:10.1016/j.jconrel.2022.03.007
93. Hoseinifar MJ, Aghaz F, Asadi Z, et al. Facilitating DNAzyme transport across the blood-brain barrier with nanoliposome technology. Sci Rep. 2025;15(1):18914. doi:10.1038/s41598-025-04433-2
94. Ohta S, Kikuchi E, Ishijima A, Azuma T, Sakuma I, Ito T. Investigating the optimum size of nanoparticles for their delivery into the brain assisted by focused ultrasound-induced blood–brain barrier opening. Sci Rep. 2020;10(1):18220. doi:10.1038/s41598-020-75253-9
95. Gong Y, Yu L, Xia L, et al. Broad-spectrum antioxidant and neuroprotective Prussian blue nanocatalyst for therapeutic intervention in autism spectrum disorder. Redox Biol. 2025;84:103671. doi:10.1016/j.redox.2025.103671
96. Selim ME, Abd-Elhakim YM, Al-Ayadhi LY. Pancreatic response to gold nanoparticles includes decrease of oxidative stress and inflammation in autistic diabetic model. Cell Physiol Biochem. 2015;35(2):586–600. doi:10.1159/000369721
97. Abbasalipour H, Hajizadeh Moghaddam A, Ranjbar M. Sumac and gallic acid-loaded nanophytosomes ameliorate hippocampal oxidative stress via regulation of Nrf2/Keap1 pathway in autistic rats. J Biochem Mol Toxicol. 2022;36(6):e23035. doi:10.1002/jbt.23035
98. He X, Xie J, Zhang J, et al. Acid-responsive dual-targeted nanoparticles encapsulated aspirin rescue the immune activation and phenotype in autism Spectrum disorder. Adv Sci. 2022;9(14):2104286. doi:10.1002/advs.202104286
99. Bhandari R, Paliwal JK, Kuhad A. Naringenin and its nanocarriers as potential phytotherapy for autism spectrum disorders. J Funct Foods. 2018;47:361–375. doi:10.1016/j.jff.2018.05.065
100. Bolandparvaz A, Harriman R, Alvarez K, et al. Towards a nanoparticle-based prophylactic for maternal autoantibody-related autism. Nanomedicine. 2019;21:102067. doi:10.1016/j.nano.2019.102067
101. Silva MDFD, Santos-Magnabosco AR, Farias CKDS, et al. Nanoemulsions with cannabidiol reduced autistic-like behaviors and reversed decreased hippocampus viable cells and cerebral cortex neuronal death in a prenatal valproic acid rat model. Anais da Academia Brasileira de Ciências. 2025;97(1):e20240607. doi:10.1590/0001-3765202520240607
102. Haratizadeh S, Ranjbar M, Darvishzadeh-Mahani F, Basiri M, Nozari M. The effects of postnatal erythropoietin and nano-erythropoietin on behavioral alterations by mediating K-Cl co-transporter 2 in the valproic acid-induced rat model of autism. Develop Psychobiol. 2023;65(1):e22353. doi:10.1002/dev.22353
103. Hajizadeh Moghaddam A, Abbasalipour H, Ranjbar M, Khanjani Jelodar S. Effect of sumac nano-phytosome on memory and oxidative stress in valproic acid-induced rat model of autism spectrum disorder. J Guilan Univ Med Sci. 2021;29(4):102–113. doi:10.32598/JGUMS.29.4.950.1
104. Dastyar Z, Kesmati M, Dorostghoal M, Torabi M. Nanoparticles of magnesium oxide improve autistic-like behaviors induced by the maternal separation model without affecting gonads structure: nanoparticles of magnesium oxide improve autistic-like behaviors. Iran J Pharm Sci. 2024;20(2):130–142.
105. Khalaj R, Moghaddam AH, Zare M. Hesperetin and it nanocrystals ameliorate social behavior deficits and oxido-inflammatory stress in rat model of autism. Int J Dev Neurosci. 2018;69(1):80–87. doi:10.1016/j.ijdevneu.2018.06.009
106. Asfour MH, Abd El-Alim SH, Kassem AA, et al. Vitamin D3-loaded nanoemulsions as a potential drug delivery system for autistic children: formulation development, safety, and pharmacokinetic studies. AAPS Pharm Sci Tech. 2023;24(2):58. doi:10.1208/s12249-023-02501-2
107. Afshari M, Gharibzadeh S, Pouretemad H, Roghani M. Reversing valproic acid-induced autism-like behaviors through a combination of low-frequency repeated transcranial magnetic stimulation and superparamagnetic iron oxide nanoparticles. Sci Rep. 2024;14(1):8082. doi:10.1038/s41598-024-58871-5
108. Miao C, Shen Y, Lang Y, et al. Biomimetic nanoparticles with enhanced rapamycin delivery for autism spectrum disorder treatment via autophagy activation and oxidative stress modulation. Theranostics. 2024;14(11):4375. doi:10.7150/thno.95614
109. Adachi M, Takahashi M, Mori H. Positive childhood experiences reduce suicide risk in Japanese youth with ASD and ADHD traits: a population-based study. Frontiers in Psychiatry. 2025;16:1566098. doi:10.3389/fpsyt.2025.1566098
110. Pehlivanidis A, Kouklari E-C, Kalantzi E, Korobili K, Tagkouli E, Papanikolaou K. Self-reported symptoms of attention deficit hyperactivity disorder (ADHD), autism spectrum disorder (ASD), and affective lability in discriminating adult ADHD, ASD and their co-occurrence. BMC Psychiatry. 2025;25(1):391. doi:10.1186/s12888-025-06841-0
111. Verhagen C, Boekhorst M, Kupper N, Leeuwis F, Duijndam S. Associations between parental protective factors and child behavioral problems in children with ADHD and ASD. J Dev Phys Disabil. 2025;38(1):1–16.
112. Notter T, Aengenheister L, Weber-Stadlbauer U, et al. Prenatal exposure to TiO2 nanoparticles in mice causes behavioral deficits with relevance to autism spectrum disorder and beyond. Transl Psychiatry. 2018;8(1):193. doi:10.1038/s41398-018-0251-2
113. Ishido M, Higashi K, Mori H, Ueno M, Kurokawa K. DNA methylation profiles of transgenerational rat hyperactivity primed by silver nanoparticles: comparison with valproate model rats of autism. Behav Brain Res. 2025;477:115293. doi:10.1016/j.bbr.2024.115293
114. Ajibade PA, Oloyede SO. Synthesis of metal–organic frameworks quantum dots composites as sensors for endocrine-disrupting chemicals. Int J Mol Sci. 2022;23(14):7980. doi:10.3390/ijms23147980
115. Cieślińska A, Sienkiewicz-Szłapka E, Wasilewska J, et al. Influence of candidate polymorphisms on the dipeptidyl peptidase IV and μ-opioid receptor genes expression in aspect of the β-casomorphin-7 modulation functions in autism. Peptides. 2015;65:6–11. doi:10.1016/j.peptides.2014.11.012
116. Shahdost-fard F, Roushani M. Cu-In-S/ZnS quantum dots/silver nanoparticles nanocomposites-modified electrode as an electrochemical label-free aptasensor for the detection of β-casomorphin 7 in early distinguish of autism. Microchem J. 2020;159:105514. doi:10.1016/j.microc.2020.105514
117. Shan H-Y, Shen K-Y, Song -S-S, et al. In situ synthesis of Au nanoparticles confined in 2D sheet-like metal organic frameworks to construct competitive PEC biosensor for sensitive analysis of autism spectrum disorder miRNA. Sens Actuators B. 2023;375:132849. doi:10.1016/j.snb.2022.132849
118. Patil GC, Qureshi S. Asymmetric drain underlap schottky barrier SOI MOSFET for low-power high performance nanoscale CMOS circuits.
119. Ivanov YD, Malsagova KA, Goldaeva KV, et al. “Silicon-on-insulator”-based nanosensor for the revelation of microRNA markers of autism. Genes. 2022;13(2):199. doi:10.3390/genes13020199
120. Alosaimi ME, Abduljabbar MH, Alzhrani RM, Saeed S, Ramzy S, Almalki AH. Development of a fluorescent nano-sensing probe for atomoxetine analysis: additional clinical pharmacokinetic study. Spectrochimica Acta Part A. 2024;322:124793. doi:10.1016/j.saa.2024.124793
121. Pal A, Goel F, Garg VK. Zebrafish as a tool for autism research: unraveling the roles of Shank3, Cntnap2, Neuroligin3, and Arid1b in synaptic and behavioral abnormalities. Neurogenetics. 2025;26(1):48. doi:10.1007/s10048-025-00828-5
122. Zhou Q, Tian Y, Xu C, Wang J, Jin Y. Prenatal and postnatal traffic pollution exposure, DNA methylation in Shank3 and MeCP2 promoter regions, H3K4me3 and H3K27me3 and sociability in rats’ offspring. Clin Epigenetics. 2021;13(1):180. doi:10.1186/s13148-021-01170-x
123. Shen Y, Li N, Sun S, et al. Non-invasive, targeted, and non-viral ultrasound-mediated brain-derived neurotrophic factor plasmid delivery for treatment of autism in a rat model. Front Neurosci. 2022;16:986571. doi:10.3389/fnins.2022.986571
124. Ansari SR, Hempel N-J, Asad S, et al. Hyperthermia-induced in situ drug amorphization by superparamagnetic nanoparticles in oral dosage forms. ACS Appl Mater Interfaces. 2022;14(19):21978–21988. doi:10.1021/acsami.2c03556
125. Liu S, Yang Q, Zhu P, et al. Precise magnetic stimulation of the paraventricular nucleus improves sociability in a mouse model of ASD: s. Liu et al: PVN Stimulation Improves Sociability in ASD. Neurosci Bull. 2025;41(10):1711–1728. doi:10.1007/s12264-025-01444-x
126. Li M, Wang S, Chang L, et al. Mn 3 O 4 nanozymes as potential therapeutic agents for autism spectrum disorder: insights from behavioral and molecular studies. Nanoscale. 2025;17(34):19681–19694. doi:10.1039/D5NR01142F
127. Feng S, Gong Y, Xia L, et al. Calcium hexacyanoferrate (III) nanocatalyst enables redox homeostasis for autism spectrum disorder treatment. Adv Mater. 2024;36(39):2405655. doi:10.1002/adma.202405655
128. De Jong WH, Geertsma RE, Borchard G. Regulatory safety evaluation of nanomedical products: key issues to refine. Drug Delivery Transl Res. 2022;12(9):2042–2047. doi:10.1007/s13346-022-01208-4
129. Limaye V, Fortwengel G, Limaye D. Regulatory roadmap for nanotechnology based medicines. Int J Drug Regulatory Affairs. 2014;2(4):33–41.
130. Palit P. Evidence Based Validation of Traditional Medicines: A Comprehensive Approach. In: Mandal SC, Chakraborty R, Sen S, Eds. Berlin/Heidelberg, Germany: Springer; 2021.
131. Pirintsos S, Panagiotopoulos A, Bariotakis M, et al. From traditional ethnopharmacology to modern natural drug discovery: a methodology discussion and specific examples. Molecules. 2022;27(13):4060. doi:10.3390/molecules27134060
132. Jean-Baptiste Z, Pathak Y, Sneed KB. Nanomedicine-based drug delivery systems and the treatment of autism spectrum disorders: a review.
133. Madani F, Esnaashari SS, Bergonzi MC, et al. Paclitaxel/methotrexate co-loaded PLGA nanoparticles in glioblastoma treatment: formulation development and in vitro antitumor activity evaluation. Life Sci. 2020;256:117943. doi:10.1016/j.lfs.2020.117943
134. Madani F, Morovvati H, Khosravani M, Adabi M. progress in nanotechnology-enabled drug delivery for glioblastoma: reports since 2020. Nanomed Res J. 2025;10(2):139–147.
135. Đorđević S, Gonzalez MM, Conejos-Sánchez I, et al. Current hurdles to the translation of nanomedicines from bench to the clinic. Drug Delivery Transl Res. 2022;12(3):500–525. doi:10.1007/s13346-021-01024-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nanomedicine for Acute Kidney Injury: Precision Delivery Strategies, Therapeutic Breakthroughs, Challenges, and Future Perspectives
Wang Y, Wang N, Qu L, Jiao Y, Xiao Z
International Journal of Nanomedicine 2025, 20:14015-14031
Published Date: 22 November 2025
Advances in Nanotechnology-Based Immunomodulatory Strategies for the Treatment of Allergic Rhinitis
Liu X, Zhao W
International Journal of Nanomedicine 2026, 21:620098
Published Date: 22 June 2026