Back to Journals » International Journal of Nanomedicine » Volume 21
Advances in Nanotechnology-Based Immunomodulatory Strategies for the Treatment of Allergic Rhinitis
Received 26 April 2026
Accepted for publication 15 June 2026
Published 22 June 2026 Volume 2026:21 620098
DOI https://doi.org/10.2147/IJN.S620098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Dong Wang
Xiaona Liu, Wei Zhao
Department of Otolaryngology, Baoding NO.1 Central Hospital, Hebei, 071000, People’s Republic of China
Correspondence: Wei Zhao, Email [email protected]
Abstract: Allergic rhinitis is a prevalent, chronic airway inflammatory disorder that poses growing public health, clinical, and socioeconomic challenges on a global scale. Allergen immunotherapy (AIT) is currently the only etiological therapy that can modify the natural course of allergic rhinitis. However, conventional AIT has limitations such as significant individual differences in efficacy, long treatment duration, and local adverse effects. The above bottlenecks highlight the urgent need to develop precise, efficient, and more secure immune-targeted intervention strategies. In recent years, nanodurgs have opened a new avenue for allergic rhinitis immunotherapy by leveraging unique advantages such as precise drug release control, targeted delivery, and enhanced immunomodulation. This article systematically reviews the recent advances in nanotechnology-based immunotherapeutic strategies for allergic rhinitis, with particular emphasis on two innovative strategies: nanovaccines and nanobodies. We further discusses the utility of diverse nanocarrier platforms, including polymeric nanoparticles, liposomes, and exosomes, which as immunomodulatory adjuvants and precision delivery systems. In addition, we elucidate the design principles and mechanistic underpinnings of intelligent responsive nanosystems, highlighting their potential to concurrently improve therapeutic efficacy and safety through synergistic immunoregulation. Collectively, this review provides a scientific foundation for the future development of novel, clinically translatable interventions for immune-mediated diseases, including allergic rhinitis.
Keywords: allergic rhinitis, nanodurg, allergen immunotherapy, targeted delivery, immunomodulation
Introduction
Allergic rhinitis is a chronic inflammatory airway disease that affects 10–40% of the global population and is characterized by sneezing, nasal congestion, and a reduced quality of life.1 Currently employed treatment approaches, including pharmacotherapy, immunotherapy and surgery, provide symptomatic relief but face limitations such as drug dependence, long treatment cycles, and tissue damage. Although these interventions have been introduced, about 10%–20% of the patients are still unsatisfactory, thus, immuno-adjuvant therapy is required.
The pathogenesis of allergic rhinitis is an abnormal immune response mediated by allergens. After dendritic cells (DCs) take in allergens, they induce the differentiation of naïve CD4⁺ T cells into Th2 cells. The Th2 cells secrete cytokines such as IL-4, IL-5, and IL-13, which promote B cells to produce allergen‑specific IgE. These IgE molecules will bind to the high-affinity FcεRI receptors on the surface of mast cells and basophils. When the allergen re-enters the body, it cross-links with the specific IgE bound to the cell surface, thereby triggering the release of granules from the cells and the release of bioactive mediators such as histamine and leukotrienes, thereby mediating type I hypersensitivity reactions. The treatment approaches for allergic rhinitis mainly include drug therapy and allergen immunotherapy (AIT).2 Currently, the drugs used in clinical treatment of allergic rhinitis, such as oral or nasal administration of antihistamine drugs, corticosteroids, leukotriene inhibitors, and mast cell stabilizers, can alleviate allergic symptoms. However, relapse is common after drug discontinuation, and long-term use carries risks of side effects such as nasal mucosal damage. AIT induces immune tolerance by regularly administering pathogenic allergens to patients, and is currently the only etiological therapy that can potentially alter the natural course of allergic rhinitis. AIT mainly includes subcutaneous immunotherapy (SCIT) and sublingual immunotherapy (SLIT), and is the only potential treatment for allergies.3,4 Compared with pharmacotherapy, AIT has a slower onset of action, taking several years to achieve clinical symptom relief. Patient acceptance is relatively low, and the efficacy of immunotherapy varies from person to person.
Nanodrugs are novel pharmaceutical formulations that utilize nanoscale (1–100 nm) materials as carriers or active ingredients. Their unique physicochemical properties including high specific surface area, tunable surface modification, controlled and sustained drug release capabilities, and targeted delivery characteristics, enable more precise control over drug release, preservation of drug stability, reduction of systemic side effects, and enhanced immunomodulatory efficacy. In the field of allergic rhinitis immunotherapy, nanoparticles can either function directly as immunomodulators to intervene in immune responses or serve as carriers for proteins, peptides, or DNA molecules to achieve targeted delivery.5 Therefore, nanodrugs are expected to break through the limitations of traditional clinical medication and AIT, providing new strategies for the treatment of allergic rhinitis.
Here, we systematically reviewed the research progress of recent years on the use of nanodrugs through immunomodulatory strategies to treat allergic rhinitis. We focused on elaborating the application strategies of various nanodrugs in allergic rhinitis immunotherapy, the molecular mechanisms of immunomodulation, and the key challenges faced in this field, laying a scientific foundation for the development of new therapy strategies for immunological diseases including allergic rhinitis in the future.
Immunomodulatory Mechanisms of Nanodrugs
The core mechanism of nanodrug treatment for allergic rhinitis lies in its ability to regulate the immune response, prompting it to shift from the pathogenic Th2 type to the protective Th1/Treg type, thereby restoring immune tolerance. The essence of allergic rhinitis is that the immune system of the body generates abnormal and excessive immune responses to harmless allergens in the environment (such as dust mites, pollen, pet dander, etc), mainly triggered by IgE-mediated type I allergic reactions, leading to type 2 inflammatory responses in the nasal mucosa. During this process, antigen-presenting cells present the allergens to the naive CD4⁺ T cells, and the T cells polarize towards the Th2 lineage and secrete cytokines such as IL-4, IL-5, and IL-13, thereby driving B cells to undergo IgE class conversion. When the allergen is exposed again, the specific IgE on the surface of mast cells (MC) and basophils cross-link with the allergen, triggering degranulation reactions and releasing inflammatory mediators such as histamine and leukotrienes, causing acute allergic symptoms. Therefore, the core mechanism of allergic rhinitis immunotherapy lies in restoring the body’s immune tolerance - that is, inducing the immune system to recognize the allergen as a harmless substance rather than an attack target.
The establishment of immune tolerance relies on the synergy of multiple mechanisms, and nanodrugs demonstrate unique advantages in these key steps. Firstly, nanodrugs can effectively induce immune deviation of allergen-specific T cells, that is, drive the Th2 dominant response to transform into the Th1 type. Studies have shown that nasal administration of nanodrugs can strongly inhibit allergen-specific Th2 cell immunity, thereby inhibiting Th2/IgE-mediated allergic reactions. The molecular basis of this immune deviation lies in the fact that nanoparticles can influence the way antigen-presenting cells take up and process allergens through their unique physical and chemical properties (such as surface charge, particle size, hydrophobicity, etc), thereby regulating the differentiation direction of T cells.6 Secondly, the induction of regulatory T cells is a crucial step in the establishment of immune tolerance. Tregs exert negative regulatory effects on the excessive activation of effector T cells by secreting inhibitory cytokines such as IL-10 and TGF-β. In this regard, nanodrugs offer a feasible strategy to enhance the efficiency of Treg induction. Nanocarriers not only serve as “delivery tools” for allergens but also can work in synergy with immunomodulatory molecules to precisely restore immune balance. Furthermore, nanodrugs also demonstrate unique value in regulating mucosal immune responses. The nasal mucosa is not only the main entry point for allergens into the body but also an ideal site for inducing mucosal immune tolerance. Nanodrugs administered via the nasal route can cross the mucosal barrier through microfold cells (M cells) or DCs and induce specific immune responses in local lymph nodes.7 In summary, nanodrugs systematically reconfigure the abnormal immune response of allergic rhinitis through the synergistic effects of multiple immunomodulatory mechanisms, such as inducing Th1/Th2 immune imbalance, promoting the expansion of Treg cells, and regulating the balance of mucosal IgA/IgE. These mechanisms not only provide a solid theoretical basis for the immunotherapy of allergic rhinitis, but also guide the material design and optimization of various nanodrugs.
Novel Immunotherapy for Allergic Rhinitis Therapy
Immunotherapy is a therapeutic strategy that modulates the host immune system to prevent and treat various diseases, including cancer, autoimmune disorders, and infectious diseases. With respect to allergic rhinitis, emerging immunological interventions are primarily categorized into two mechanistically distinct approaches: (i) active immunotherapy utilizing nanovaccine platforms, designed to elicit durable, antigen-specific immune tolerance; and (ii) passive immunotherapy employing nanobodies, which enable rapid, precise, and controllable biological effects through high-affinity targeting and neutralization of allergens or critical inflammatory mediators.
Nanovaccines-Based Active Immunotherapy
Tolerogenic nanovaccines represent the latest development direction in allergic rhinitis immunotherapy. These vaccines are designed to treat IgE-mediated type I hypersensitivity by inducing allergen-specific immune tolerance rather than merely alleviating symptoms. The key to their design lies in precisely regulating the co-delivery of antigens and immunomodulators, thereby achieving reprogramming of the immune system. Currently, research on tolerance vaccines based on nanoparticles mainly focuses on three core areas: optimization of existing nanoparticle platforms, screening and design of biomaterials, and integration of multi-functional engineering strategies.8 Among various nanovaccine platforms, nucleic acid–based approaches currently represent the most advanced and actively pursued strategy.
DNA-Based Nanovaccines
DNA-based nanovaccines represent an emerging immunotherapeutic platform that integrates plasmid DNA encoding allergen antigens with engineered nanocarrier systems. By selectively promoting Th1-polarized immune responses and suppressing allergen-specific IgE production, they offer a promising and mechanistically grounded approach for the immunomodulatory treatment of allergic rhinitis.
In allergic rhinitis research, the predominant allergenic targets are the major house dust mite (HDM) allergens Der p 1 and Der p 2. Epidemiological evidence indicates that more than 80% of individuals with HDM-induced allergic rhinitis exhibit allergen-specific IgE reactivity to both Der p 1 and Der p 2. Other clinically relevant allergens include Der p 7, Der p 23, Japanese cedar pollen allergens Cry j 1 and Cry j 2, and ragweed allergen Amb a 1. As a representative example, the Der p2–A20 nanovaccines formulated as PLGA-encapsulated pVAX1 plasmid DNA encoding Der p2 and the anti-inflammatory regulatory protein A20 (termed PpDA), which was prepared via emulsion-solvent evaporation. This nanovaccine exerts dual immunomodulatory effects which by reducing expression of A20 to suppress NF-κB–dependent proinflammatory signaling and expressing Der p 2 to promote antigen-specific Treg differentiation. In murine allergic rhinitis models, intranasal administration of PpDA significantly alleviated hallmark behavioral symptoms of nasal scratching and sneezing, and markedly reduced inflammatory cell infiltration in the nasal mucosa. Collectively, these findings demonstrate robust therapeutic efficacy of the PpDA nanovaccine in preclinical allergic rhinitis models.9 Shi et al constructed a chitosan nanovaccine (pVAX1-Der p1/CS) by loading the house dust mite major allergen Der p1 DNA into chitosan as a carrier. The pVAX1-Der p1/CS nanoparticles, using chitosan as a gene carrier, exhibited excellent DNA encapsulation efficiency and effectively protected the plasmid DNA from nuclease degradation. In an allergic rhinitis animal model, intranasal administration of the pVAX1-Der p1/CS nanovaccine resulted in significantly reduced serum total IgE and IL-4 levels, decreased eosinophil infiltration, and effective suppression of Th2-type inflammation. Using chitosan as a carrier promoted the local absorption of DNA vaccine nanoparticles in the nasal mucosa and enhanced their anti-inflammatory effects, restoration of the Th1/Th2 balance, and inhibition of Der p1-specific IgE. After intranasal immunization of an animal model with chitosan microsphere-encapsulated antigens, both antigen-specific nasal mucosal and systemic immune responses were induced. Chemical modification of chitosan microspheres further achieved a synergistic effect with the antigens on immune responses.10
mRNA-Based Nanovaccines
Nanovaccines based on mRNA-lipid nanoparticles (LNPs) have shown promising potential in immunotherapy, as they can alleviate allergic reactions by inducing allergen-specific IgG antibodies while maintaining low IgE levels. mRNA does not integrate into the host genome and exhibits transient expression in vivo, thereby minimizing long-term safety concerns. Furthermore, its nucleotide sequence can be rationally engineered and precisely encoded to represent any known allergen, including its immunodominant epitopes, which enabling the development of targeted therapeutic strategies with high antigenic specificity. For example, Rochman et al constructed a Der p1–mRNA–LNP nanovaccine by loading house dust mite allergen Der p1 mRNA into LNPs. The results showed that in an established mouse model of allergy, immunization with Der p1–mRNA–LNP attenuated the allergen-induced Th2 response, reduced levels of Th2-type cytokines (eg, IL-4, IL-5, IL-13), alleviated allergic symptoms, enhanced Th1 and CD8⁺ T cell responses, induced Treg expansion, and promoted the production of allergen-specific IgG2a antibodies (which competitively inhibit IgE), thereby achieving immune tolerance. Thus, by redirecting the Th2-type immune response toward a Th1/Treg-dominant tolerogenic state, allergen-specific mRNA-LNP therapy effectively prevents and treats experimental allergy in mice, offering a potential new nucleic acid vaccine strategy for allergic diseases such as asthma and allergic rhinitis (Figure 1 and Table 1).11
 |
Figure 1 Der p1–mRNA–LNP protects against allergic responses. (A) Allergen-specific mRNA-LNP therapy modulates immune responses, reducing allergy symptoms while enhancing protective immunity. (B) Box-and-whisker plot of Der p1–IgG1 antibody levels in the serum of naive, LNP, or Der p1–mRNA–LNP–vaccinated mice on day 26 (n = 9–20). (C) Quantification of cells in the BALF on day 2 after the last challenge. (D and F) The frequency of GATA3+ and cytokine-producing cells among CD4+ T cells in the lungs. (E) Representative PAS-stained sections in bronchi and bronchiole for mucus production. Arrows indicate goblet cells producing mucin. The box-and-whisker plot shows a mucus score pooled from 2 independent experiments (n = 6–8). Scale bar: 50 μm. (C, D, and F) Data are pooled from 2 or 3 independent experiments (n = 6–12), the dots represent individual mice, and the line represents the mean per group. *P ≤ 0.05, **P ≤ 0.01, ***P ≤ 0.001, ****P ≤ 0.0001 by 1-way ANOVA with Tukey correction. n.d., not detected. Adapted with permission from,11 copyright 2025, The American Society for Clinical Investigation. |
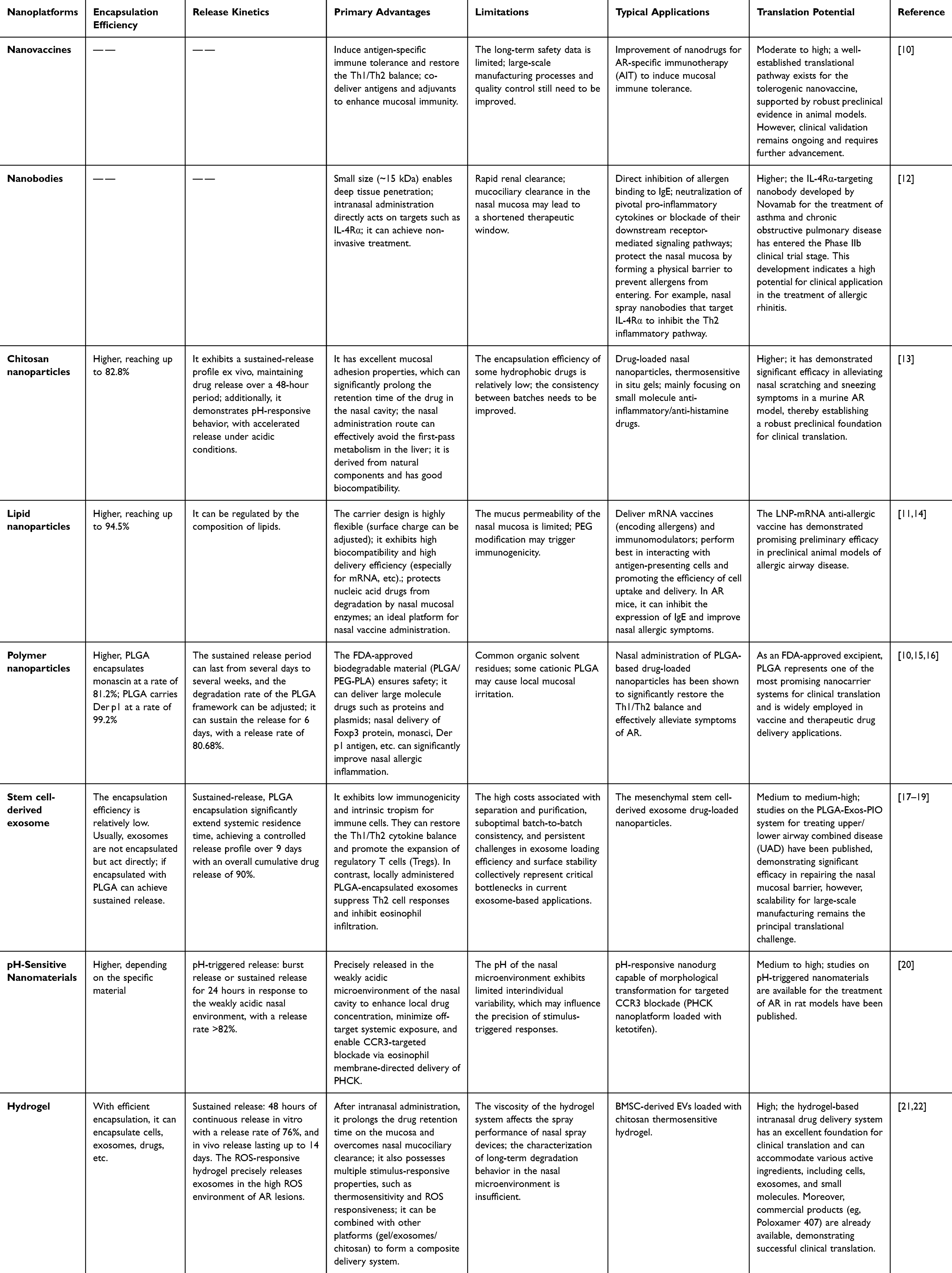 |
Table 1 Comparative Analysis of Different Types of Nanoplatforms |
Nanobody-Based Passive Immunotherapy
As a new generation of biologics, nanobodies have shown great promise in treating allergic diseases in recent years, owing to their unique advantages such as small molecular weight, high stability, strong affinity, and ease of engineering. Nanobodies are derived from naturally occurring heavy chain-only antibodies (HcAbs) found in camelids. Unlike conventional IgG antibodies, HcAbs lack light chains; their antigen-binding function is carried out by a single heavy-chain variable domain (VHH). Through genetic engineering, this VHH domain can be expressed alone to yield a nanobody with a molecular weight of only approximately 15 kDa. This structural feature endows nanobodies with a range of unique physicochemical and biological properties.23 Currently, nanobody-based therapeutic strategies for allergic rhinitis focus on three key aspects: (1) directly blocking allergen-IgE binding; (2) neutralizing key inflammatory cytokines or blocking their receptor signaling pathways; and (3) preventing allergen entry into the nasal mucosa via physical barrier protection.24
Nanobodies Targeting the IgE/FcεRI Pathway
IgE-mediated immune response is central to the pathogenesis of allergic rhinitis. Blocking the binding of IgE to FcεRI, or directly targeting the FcεRI receptor, can inhibit mast cell and basophil activation at the source, thereby preventing the onset of allergic reactions. Targeting IgE as a therapeutic strategy has already been exemplified—Omalizumab, the first approved anti-IgE humanized monoclonal antibody, has shown good efficacy in treating allergic asthma and chronic urticaria. However, its subcutaneous administration route and relatively limited affinity remain limiting factors.
In recent years, nanobody technology has brought new breakthroughs to anti-IgE therapy. For example, Aagaard et al immunized camels with Timothy grass pollen extract to construct an extract-specific immune nanobody library. Using phage display technology, they screened for nanobodies capable of recognizing the pollen extract and further engineered them into human IgE fusion proteins (nb-hIgE). These nb-hIgE specifically recognized the major Timothy grass pollen allergens Phl p 6 and Phl p 4 and exhibited significant cross-reactivity among pollen extracts from different grass species. This approach provides new tools for the specific diagnosis and treatment of pollen-induced allergic rhinitis.25
Bauernfeind et al engineered a trimeric form of the Bet v 1-specific nanobody, designated Nb32ILZ. This trimeric nanobody more efficiently competes with IgE for binding to Bet v 1 and its cross-reactive allergens (such as PR-10 family proteins from hazelnut, alder, etc.) than the monomeric form. Consequently, Nb32ILZ significantly inhibits the binding of patients’ IgE antibodies to Bet v 1 allergen and also suppresses allergen-induced mediator release, thereby effectively blocking the initiation mechanism of the allergic reaction.26
Nanobodies Targeting Type 2 Inflammatory Cytokines
Type 2 inflammation is a hallmark of the immunopathology of allergic rhinitis. Key cytokines such as IL-4, IL-13, and TNF-α play central role in the onset and maintenance of allergic rhinitis, making them important targets for nanobody intervention.
Nanobodies Targeting IL-4Rα
IL-4 and IL-13 are key cytokines that drive pathogenic responses in allergic airway diseases, both of which signal through the shared receptor subunit IL-4 receptor α chain (IL-4Rα). Currently, monoclonal antibodies targeting IL-4Rα (eg, Dupilumab) are administered subcutaneously for the treatment of eosinophilic sinusitis and allergic asthma; however, they have drawbacks such as inconvenient injection and the potential risk of systemic immunosuppression.
To address these challenges, Ahn et al developed a specific IL-4Rα nanobody (H5), which can effectively inhibit inflammatory signal transduction in human nasal epithelial cells through non-invasive intranasal administration, demonstrating the potential of this as a new non-invasive strategy for treating rhinitis. This study obtained H5 through screening from a synthetic nanobody library using ribosome display technology, and utilized AlphaFold2 and GROMACS for dimerization and computer-assisted affinity maturation, significantly enhancing its binding affinity. Functional experiments showed that H5 effectively controlled inflammatory markers such as MUC5AC, CCL26, and FOXJ1 in human nasal epithelial cells (HNEC) by inhibiting IL-4 and IL-13 signal transduction. Notably, the bivalent form of H5 exhibited good efficacy in easily accessible cells (such as ciliated cells), while the monovalent variant could target cells that are difficult to reach (such as the basal cells of HNEC). This study confirmed that H5 can effectively inhibit inflammatory signal transduction in HNEC through intranasal administration, demonstrating significant potential as a non-invasive treatment for rhinitis (Figure 2 and Table 1).12 This nanobody-based biological agent strategy overcomes the problems of large molecular weight and poor tissue permeability of traditional antibody drugs while maintaining high targeting efficiency, providing new ideas for precise biological treatment of allergic rhinitis.
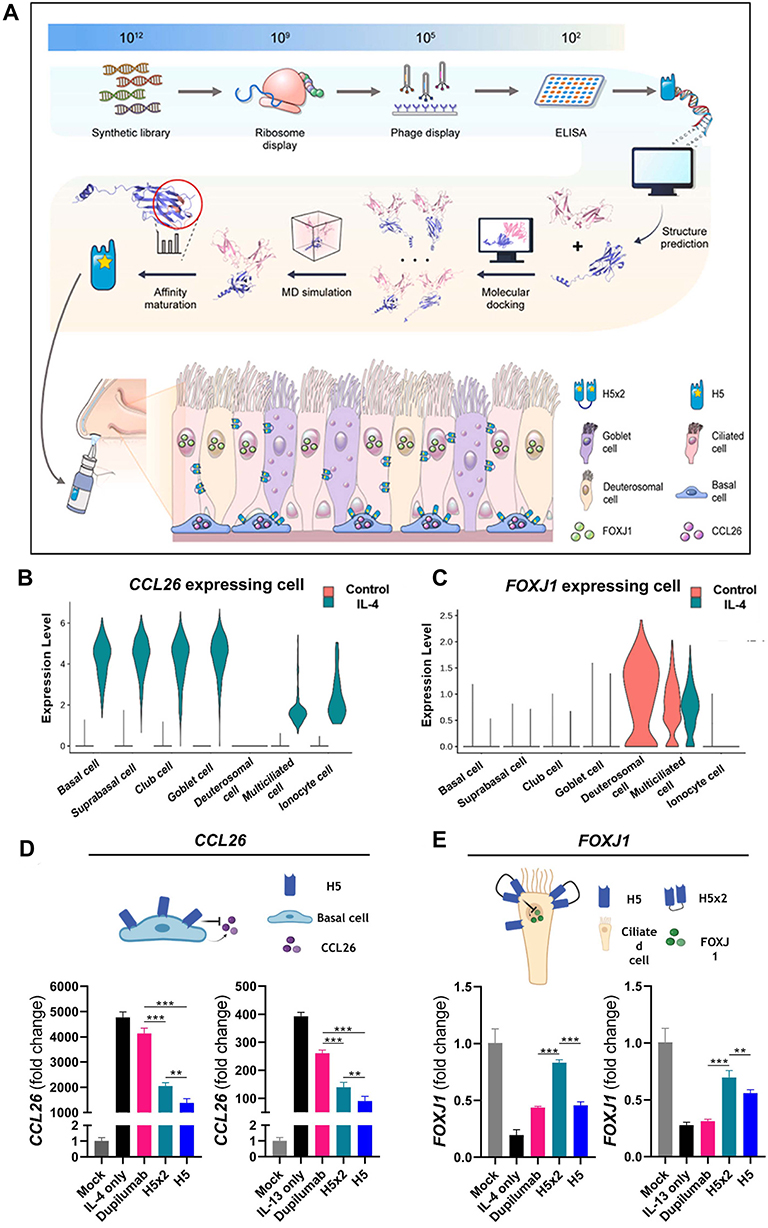 |
Figure 2 (A) Schematic representation of a topical IL-4Rα-specific nanobody for the treatment of allergic airway diseases. (B and C) Violin plots displaying the expression levels of CCL26 (B) and FOXJ1 (C) genes in distinct subsets of HNEC cells under normal and IL-4 treated conditions, as determined through single-cell sequencing analysis. (D and E) Expression of CCL26 (D) and FOXJ1 (E) with administration of the nanobody variants in IL-4 (D) and IL-13 (E) supplemented condition in HNEC detected by quantitative PCR. All data were plotted as mean ± SD, and statistical significance was assessed using Student’s unpaired t-test: **p < 0.01, ***p < 0.001. Adapted with permission from,12 copyright 2024, ELSEVIER. |
Nanobodies Targeting TNF-α
TNF-α is a pro-inflammatory cytokine that plays an important role in nasal mucosal inflammation and epithelial barrier dysfunction in allergic rhinitis. However, the precise role of TNF-α inhibitors in allergic rhinitis has remained unclear. Fu et al assembled an anti-TNF-α nanobody (V) with tannic acid (TA) to form V/TA nanoparticles and evaluated their efficacy in an ovalbumin (OVA)-induced mouse model of allergic rhinitis. The results showed that following V/TA treatment, the degree of inflammatory cell infiltration, as well as the numbers of mucus-secreting cells and mast cells in the nasal mucosa, returned to near-normal levels. Mechanistic studies revealed that the efficacy of V/TA was closely associated with the restoration of tight junction protein (ZO-1, occludin, claudin-1, claudin-5) expression levels, suggesting a therapeutic effect mediated by repair of the nasal epithelial barrier. Of note, this anti-TNF-α nanobody was superior to the commercial drug Infliximab in repairing the epithelial barrier defect induced by allergic rhinitis. Tannic acid-assisted assembly not only enhanced the therapeutic efficacy of the nanobody but also exhibited no obvious toxicity.27
Nanobodies Targeting Intercellular Adhesion Molecule-1 (ICAM-1)
The nasal cavity serves as a primary gateway for allergen entry into the body. Blocking allergen penetration across the epithelium and the subsequent IgE-mediated allergic inflammatory response at this stage could prevent the development of allergic rhinitis at its source. Intercellular adhesion molecule-1 (ICAM-1) is highly expressed on the respiratory epithelial cell surface in patients with allergic diseases and is considered an ideal target for anchoring antibody conjugates. Zettl et al successfully generated a high-affinity ICAM-1-specific nanobody (Nb44) by immunizing camels with ICAM-1 followed by phage display screening. Surface plasmon resonance (SPR) analysis revealed that Nb44 binds to ICAM-1 with an affinity as high as 10−10 M and is not internalized at the cell surface. Furthermore, Nb44 efficiently binds to ICAM-1-expressing cells, with a binding rate of over 96%. Therefore, Nb44 can be used in the future to design allergen/ICAM-1 specific heterodimers, in order to develop bispecific nanobodies for local treatment of allergic rhinitis. This strategy has the advantages of strong targeting, local efficacy and non-invasive administration, opening up new ideas for the prevention and treatment of allergic rhinitis.28
Nanobodies Targeting Thymic Stromal Lymphopoietin
Thymic stromal lymphopoietin (TSLP), a key cytokine derived from epithelial cells, is secreted by airway epithelial cells in response to allergens. It is a crucial initiating factor for regulating type 2 and non-type 2 immune responses. Although monoclonal antibodies targeting TSLP have shown promising clinical efficacy, the traditional injection administration method is unable to achieve high drug concentrations locally in the respiratory tract, and the high cost of biological agents also limits their wide application. To address these challenges, the researchers developed the bispecific nanobody LQ043. By screening four TSLP immunization libraries, they obtained humanized nanobody monomers, which were then dimerized to form the final structure. The half-maximal inhibitory concentration (IC50) of LQ043 against hTSLP is in the nanomolar range (3.2 nM), and it can effectively block the interaction between TSLP and TSLPR. In an OVA-induced mouse model of airway inflammation, inhaled LQ043 dose-dependently reduced eosinophil counts and IL-4 and IL-5 levels in bronchoalveolar lavage fluid. In non-human primates, nebulized administration achieved lung drug concentrations 20-fold higher than those in plasma, highlighting the local advantage of inhaled delivery. A Phase I clinical trial further confirmed favorable pharmacokinetics and safety of LQ043 in healthy subjects. Notably, LQ043 can be produced at low cost on a large scale using a yeast expression system, with a single-administration cost reduced by more than 80% compared with conventional mAbs. LQ043 is the first inhaled TSLP-targeting nanobody to enter clinical development, opening a new avenue for precision therapy of airway inflammatory diseases such as allergic rhinitis.29
The Nanocarriers with Immunomodulatory Effects
In addition to serving as delivery vehicles, certain nanomaterials exhibit intrinsic immunomodulatory properties, thereby serving dual roles as both antigen carriers and adjuvants, which collectively enhance the efficacy of AIT.
Chitosan Nanoparticles
Chitosan is a natural cationic polysaccharide obtained by deacetylation of chitin. Due to its excellent biocompatibility, biodegradability and inherent mucosal adhesion properties, it has attracted much attention in the nanodelivery system for allergic rhinitis immunotherapy.30 The cationic nature of chitosan enables it to form strong electrostatic interactions with the negatively charged nasal mucosa surface, prolonging the retention time of allergens in the nasal cavity and thereby enhancing the efficiency of local immune response.31 The immunomodulatory effect of chitosan nanoparticles not only stems from their delivery function, but also has intrinsic adjuvant activity on its own. Chitosan nanoparticles have been proven to promote the maturation of antigen-presenting cells and the bias towards Th1-type immune responses, thereby exerting a dual role in inhibiting Th2-mediated allergic reactions. Chitosan can enhance the activation of antigen-presenting cells by interacting with Toll-like receptors or activating the NLRP3 inflammasome, thereby promoting Th1-type immune responses. Moreover, the protective effect of chitosan nanoparticles against allergens is particularly prominent-in the enzyme-rich environment of nasal mucosa, protein-type allergens are easily degraded, while chitosan nanoparticles encapsulation can effectively resist the degradation effect of enzymes, ensuring that allergens are delivered to immune cells in their intact form (Table 1).32 Su et al loaded miRNA-146a into a chitosan hydrogel/PEG-PLA nanoparticle binary delivery system. The results showed that the prepared binary formulation could rapidly form a gel in the nasal cavity at a temperature of 34°C, had good mucosal adhesion, and could stably and continuously deliver nucleic acids to the nasal mucosa. The nasal symptoms (such as sneezing and rubbing the nose) of allergic rhinitis rats treated with the binary formulation were significantly improved, and the expressions of TLR4 and NF-κB in the nasal mucosa were significantly downregulated. Compared with the single formulation, the gel/NPs/miR-146a binary formulation performed better in terms of nucleic acid delivery capacity and efficacy.13 Moreover, a novel chitosan/oligochitosan/Tween 80 (CS-COS-T80) co-stabilized emulsion, used as a nasal vaccine adjuvant, significantly increased nasal secretory IgA (sIgA) levels—five times higher than those induced by the naked antigen and two times higher than those induced by the commercial adjuvant MF59. Compared with MF59, the CS-COS-T80 emulsion more effectively activated humoral immunity and T-cell memory differentiation, promoting the secretion of IL-4 and IFN-γ.33 Therefore, the CS-COS-T80 emulsion represents a promising nanovaccine adjuvant platform for the treatment of allergic rhinitis.
However, the clinical application of chitosan nanoparticles still faces several bottlenecks. Although chitosan has excellent biocompatibility, the structural differences among its batches (such as variations in molecular weight and deacetylation degree) may lead to significant differences in its biological distribution, degradation kinetics, and toxicity profile, thereby posing technical obstacles to standardized production and regulatory approval. Currently, the FDA has not approved any chitosan-based products for drug delivery, indicating that the application of chitosan nanoparticles in allergic rhinitis treatment is still in the preclinical exploration stage. A more systematic safety evaluation and quality control system is urgently needed.
Lipid Nanoparticles
Liposomes and lipid nanoparticles (LNPs) possess unique advantages in AR nasal administration due to their biomimetic membrane structure, high drug-loading capacity, and excellent mucosal penetration properties. Research on LNPs for allergic rhinitis treatment has grown rapidly in recent years. The surface charge state of engineered LNPs significantly influences their cellular targeting properties and immune regulatory functions in the body. Surface charge modification of LNPs represents an effective strategy to enhance the immunogenicity and efficacy of nanovaccines (Table 1). The research found that negatively charged LNPs performed the best in interacting with antigen-presenting cells, promoting cell uptake and delivery efficiency. The negatively charged LNPs could selectively deliver Bryostatin-1 to B cells, promoting IgA class switching and simultaneously inhibiting IgE expression. In the allergic rhinitis mouse model, a low intranasal dose of 0.5 ng of Bryostatin-1-LNPs was able to effectively increase the level of antigen-specific IgA in saliva secretions. This study demonstrates that by designing the surface charge of nanoparticles, precise delivery to specific B cell subsets can be achieved, thereby enhancing mucosal protective immunity while suppressing the sensitizing IgE response. This study proposes a novel “selective enhancement” strategy for the treatment of allergic rhinitis.14
Polymer Nanoparticles
Poly(lactic-co-glycolic acid) (PLGA) has been proven to be an excellent carrier for drugs and proteins, making it suitable to treat various diseases, and is known for its outstanding biodegradability and biocompatibility.34 Another potential advantage of PLGA-mediated delivery over intravenous administration is the ability of PLGA to induce humoral and mucosal immunity even with low doses of encapsulated allergens, potentially reducing the drug dose required to achieve equivalent therapeutic effects.
For instance, Shahzad et al previously demonstrated that exosome administration activates the peroxisome proliferator-activated receptor (PPAR) signaling pathway in nasal mucosal tissues, thereby implicating the PPAR-γ agonist pioglitazone (PIO) as a potential enhancer of exosome-mediated anti-inflammatory effects.35–37 However, systemic exosome delivery is limited by rapid clearance from circulation, whereas local (eg, intranasal) administration suffers from insufficient mucosal residence time and poor bioavailability. To overcome these pharmacokinetic challenges, they developed a rationally engineered “triple-component” nanocarrier system—PLGA-Exo-PIO—comprising PLGA co-loaded with exosome and PIO. In a murine model of uric acid-induced airway disease (UAD), intranasal administration of PLGA-Exo-PIO markedly alleviated clinical symptom scores and significantly suppressed eosinophil and basophil infiltration. Furthermore, this formulation restored Th1/Th2 immune homeostasis and modulated the frequencies of regulatory T cells (Tregs) and regulatory B cells (Bregs). Critically, the PLGA-based platform enabled sustained, synchronous release of both therapeutic agents following intranasal delivery, substantially extending their retention in nasal and pulmonary mucosa while facilitating dual-site targeting across the upper and lower airways. These findings provide a translational strategy for improving the efficacy of biologics in allergic rhinitis therapy.17 Wang et al encapsulated the natural anti-inflammatory component Monascin into PLGA nanoparticles. Through intranasal administration, they achieved sustained drug release, which significantly reduced inflammatory cell infiltration in the nasal tissues of allergic rhinitis mice, modulated IgE and histamine levels, decreased the numbers of helper T cell 2 (Th2) and helper T cell 17 (Th17) cells, while increasing the number of regulatory T cells (Tregs).15 Furthermore, Foxp3 protein, a key transcription factor for regulatory T (Treg) cells, demonstrated favorable anti-inflammatory efficacy after intranasal delivery via PLGA nanoparticles in a mouse model of allergic rhinitis. Foxp3 NP treatment significantly reduced serum levels of total IgE and OVA-specific IgE, as well as the expression levels of IL-4 and IL-13, and alleviated nasal allergic symptoms (Table 1).16
Therefore, the potential of biomaterial-assisted nanodelivery platforms in immunomodulatory therapy for allergic rhinitis represents a novel and promising strategy.
Stem Cell-Derived Exosomes
Mesenchymal stem cell-derived exosomes (MSC-Exos) have emerged in recent years as a cell-free therapeutic platform, combining the immunomodulatory advantages of stem cells with the low immunogenicity risk associated with cell-based preparations. Research has indicated that MSC-Exos exhibit immunomodulatory effects identical to those of the stem cells themselves in allergic airway diseases. Exosomes are involved in regulating both adaptive and innate immune responses. Notably, MSC-Exos play a crucial role in immunomodulation by inducing a shift from Th2 to Th1 responses, suppressing the differentiation of Th17 cells, and increasing the number of Tregs (Figure 3 and Table 1).18,38
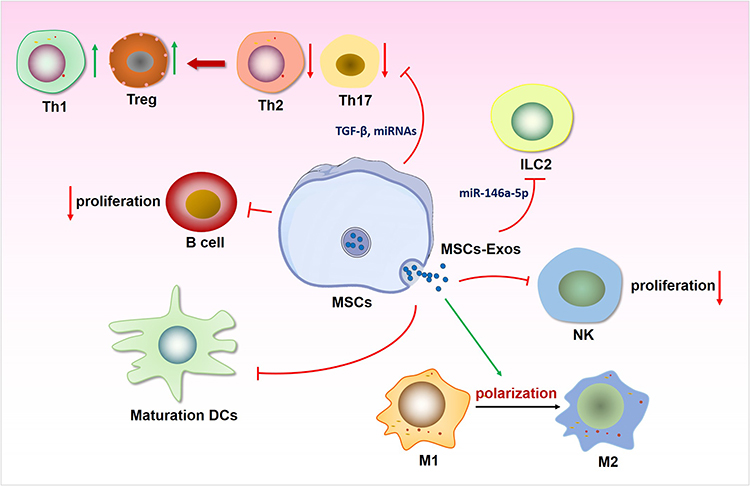 |
Figure 3 Mechanism of action of mesenchymal stem cell-derived exosomes (MSC-Exos) in the treatment of allergic rhinitis (AR). MSC-Exos alleviate AR by restoring the Th1/Th2 balance and regulating DCs differentiation. MSC-Exos could skew the balance of Th cells in favor of Th1 and Treg and suppress the function of Th2/Th17 cells by carrying miRNAs, TGF-β1 or HGF.19 Additionally, they also inhibited the proliferation of B cells and the maturation of DCs. MSC-Exos could inhibit the production of type 2 cytokines from ILC2 through the delivery of miR-146a-5p, affect the proliferation of NK cells, and the polarisation of macrophages.39 Abbreviations: DCs, dendritic cell; ILC2, group 2 innate lymphoid cell; M1/2, type 1/2 macrophage. |
For instance, Xu et al obtained exosomes from adipose-derived mesenchymal stem cells (AMSCs) and used them to treat mice with allergic rhinitis. Treatment with MSC-Exos effectively reduced the levels of inflammatory cytokines such as IL-4, IL-5, and interferon-gamma (IFN-γ); alleviated damage to and thickening of the mucosal layer; and decreased the numbers of goblet cells and eosinophils. These findings suggest that AMSC-Exos may ameliorate allergic symptoms and inflammation in allergic rhinitis model mice by correcting the Th1/Th2 imbalance.40 Similarly, Han et al treated peripheral blood mononuclear cells (MCs) from allergic rhinitis patients with AMSC-Exos and reported that AMSC-Exos can regulate the balance between Th2 cells and Treg cells in vitro through the PI3K/AKT/mTOR/p70S6K pathway.41 Park et al obtained palatine tonsil-derived stem cells (TMSCs) from palatine tonsil tissue and reported that these stem cells expressed more immunomodulatory proteins than stem cells derived from bone marrow and adipose tissue did.42,43 Treatment with TMSC-derived exosomes (TMSC-Exos) significantly alleviated allergic symptoms, reduced the infiltration of eosinophils and neutrophils in the nasal mucosa, and markedly decreased IL-4 expression in the induced allergic rhinitis mouse model. TMSC-Exos are rich in key immunomodulatory factors such as TGF-β1, PGE2, and HGF, which exert immunomodulatory effects on allergic inflammatory responses by inhibiting the phosphorylation of MAP kinase, the translocation of p65, and the activation of NFAT1, thereby inhibiting T-cell activation.19 Wang et al reported that treatment with human umbilical cord mesenchymal stem cell-derived exosomes (HUCMSC-Exos) increased the number of regulatory CD4+CD25+CD127− T cells. These cells release more IL-10 and TGF-β while inhibiting the production of the cytokine IL-17, thereby restoring the Treg/Th17 balance. Consequently, treatment with HUCMSC-Exos can modulate the Th1/Th2 cell balance and enhance the function of Tregs. Furthermore, the therapeutic effects of HUCMSC-Exos are associated with additional upstream molecular mechanisms. Significant changes in the expression of genes involved in the TGF-β signaling pathway and the Wnt signaling pathway and the transcription factor STAT5 were observed following HUCMSC-Exos treatment. These signaling pathways and transcription factors may represent important molecular mechanisms mediating the effects of exosomes therapy on allergic rhinitis and the Treg/Th17 balance.18
Furthermore, exosomes can block the differentiation of DCs from bone marrow progenitors and monocytes into mature DCs, promoting the generation of immunosuppressive cells and thus treating immune diseases (Figure 3). For example, Wu et al collected extracellular exosomes (Hy-Exos) from human umbilical cord mesenchymal stem cells (hUCMSCs) cultured under long-term hypoxic conditions (Hy-HUCMSCs) and reported that they were effective at treating allergic rhinitis. Hy-Exos can inhibit the maturation of DCs by reducing the expression of HLA-DR, CD80, CD40, and CD83 in DCs induced by OVA plus LPS. This inhibitory effect could be neutralized by an anti-VEGF antibody, confirming that the enrichment of VEGF in Hy-Exos plays a key role in inhibiting DC maturation. By suppressing DC maturation, Hy-Exos promote immune tolerance and reduce Th2-mediated inflammation in allergic rhinitis. Professor Fu Qingling’s team prepared exosomes from induced pluripotent stem cells (iPSC-Exos). They similarly confirmed that these iPSC-Exos inhibited the differentiation of iDCs into mature DCs by downregulating the expression of CD40, CD80, CD86, and HLA-DR. Concurrently, iPSC-Exos promoted the production of IL-10 by myeloid dendritic cells (mDCs), further suppressing the Th2 immune response and increasing Treg cell levels through the IL-10/IL-10Rα axis. These findings confirmed that iPSC-Exos can inhibit DC maturation, thereby demonstrating their potential therapeutic value in the treatment of allergic rhinitis.44
Furthermore, studies have revealed the presence of ILC2s, mDCs, and plasmacytoid dendritic cells (pDCs) in the nasal mucosa tissues of patients with allergic rhinitis. Among these, mDCs can activate ILC2s in patients via the IL-33/ST2 signaling pathway, prompting them to secrete Th2-type cytokines and thereby enhancing the immune response. Conversely, activated pDCs can inhibit the activation of ILC2s in allergic rhinitis patients by releasing IL-6.45 Therefore, the DC-ILC2 pathway may serve as an effective target for the treatment of allergic rhinitis. As demonstrated by Fu et al, the use of exosomes derived from iPSCs can inhibit the activation of ILC2s by mDCs in allergic rhinitis patients, thereby achieving immunotherapy for allergic rhinitis The expression levels of prostaglandin E synthase (PTGES) and IL-10 were elevated in DCs treated with exosomes (Exos-mDCs). These substances have inhibitory effects on ILC2 function. These findings indicate that the stimulatory effect of Exos-mDCs on ILC2 function is diminished, resulting in lower levels of IL-13 produced by ILC2s. The immunomodulatory mechanism primarily exerts immunosuppressive effects on ILC2s by increasing the binding of PGE2 to EP2/4 receptors.46 Therefore, the use of mesenchymal stem cell-derived exosomes to inhibit the interaction between DCs and ILC2s may represent a promising strategy for the treatment of allergic rhinitis.47 In summary, MSC-Exos have been shown to have potent therapeutic effects on allergic rhinitis (Figure 3).
Efficient Delivery Strategies for Allergic Rhinitis Therapy
In the treatment of allergic rhinitis, nanodurg-based delivery systems confront three interrelated challenges: (i) achieving precise targeting and immunomodulation of key immune effector cells—particularly DCs; (ii) enabling microenvironment-responsive drug release triggered by pathological cues in the nasal cavity, such as mildly acidic pH; and (iii) overcoming rapid mucociliary clearance to extend local drug residence time. A single delivery strategy is frequently insufficient to simultaneously address all three critical requirements. Consequently, integrating targeted delivery, environmentally responsive release, localized retention, and sustained-release mechanisms enables the development of a comprehensive therapeutic delivery system—one that progresses sequentially from “precise arrival” to “intelligent release” and ultimately to “prolonged therapeutic effect”—thereby offering an efficient, durable, and safe treatment modality for allergic rhinitis.
Delivery Strategies Targeting DCs
Modifying DC-Targeting Aptamers
To meet the demand for targeted therapy, artificial oligonucleotides known as “chemical antibodies”—namely, aptamers—have been employed as novel targeting ligands to construct aptamer–drug conjugates (ApDCs), enabling them to bind to DCs with high specificity.48,49 Aptamers are a class of short, single-stranded DNA or RNA oligonucleotides selected through systematic evolution of ligands by exponential enrichment (SELEX) technology. They bind to target molecules with high specificity via their unique three-dimensional conformations and are characterized by high stability, low synthesis cost, and nonimmunogenicity. Aptamers offer several advantages over monoclonal antibodies, such as nontoxicity, lack of immunogenicity, excellent thermal stability, and ease of modification and production. These superior properties of aptamers have led to their increased use in enhancing the efficacy of immunotherapies (Figure 4).50 Mahvash Sadeghi et al modified adipose-derived mesenchymal stem cell exosomes with aptamers and loaded OVA into these aptamer-modified exosomes to create exosome-based nanoparticles (Apt-OVA-Exos) capable of targeting DCs for the treatment of allergic rhinitis via SLIT. SLIT represents an effective and injection-free route for allergen-specific immunotherapy (AIT) that modulates immune responses, leading to sustained symptom relief and improved quality of life.51,52 Their study demonstrated that Apt-OVA-Exos shifted the immune response from a Th2-type to a Th1-type response by increasing the concentrations of TGF-β and IFN-γ and decreasing the concentration of IL-4, inducing an immunomodulatory response in Tregs, and reducing the infiltration of inflammatory cells and eosinophils. Exosomes and aptamers were utilized as nanocarriers and delivery systems, respectively, effectively enhancing the efficacy of SLIT in an allergic animal model.53
 |
Figure 4 The mechanism of targeting dendritic cell modification strategies in the treatment of allergic rhinitis. Adaptor modification strategy: Artificially synthesized oligonucleotide adaptors are employed to functionalize exosomes and facilitate the efficient loading of ovalbumin (OVA) antigen. This approach promotes a Th1-polarized immune response, which evidenced by upregulation of TGF-β and IFN-γ and concurrent downregulation of IL-4, while also modulating the activity and frequency of regulatory T (Treg) cells. P-D2 targeting peptide strategy: The P-D2 peptide selectively binds to CD11c expressed on dendritic cells (DCs), thereby inhibiting the Fut1/ICAM-1 signaling axis and the p38 MAPK pathway. This dual inhibition enhances IL-10 production and suppresses both Th2 cell differentiation and group 2 innate lymphoid cell (ILC2) activation. NGR peptide-based targeting strategy: A cyclic NGR peptide is employed to specifically bind the CD13 receptor expressed on DCs, enabling targeted delivery of xanthatin (XT) encapsulated in biodegradable polymer microspheres. This approach inhibits the COX-2/PGE2 signaling axis, resulting in the downregulation of co-stimulatory molecules (CD80, CD86, I-A/I-E), restoration of Th1/Th2 immune balance, expansion of Tregs, and significant reduction in allergy-associated mediators, including IgE, histamine, and IL-4. |
Modification of P-D2 Targeting Peptides
The P-D2 peptide (amino acid sequence: GGVTLTYQFAAGPRDK) has been reported as a synthetic targeting peptide with binding affinity for CD11c (integrin αX). It is primarily used in the development of drug delivery systems targeting CD11c⁺ DC/macrophage subsets. Studies have shown that nanoparticles modified with the P-D2 peptide can increase DC phagocytosis and significantly improve the antigen presentation ability of DCs in vitro (Figure 4).54,55 Liu et al isolated exosomes from hUCMSCs using ultracentrifugation and modified them with the P-D2 peptide via lipid hybridization technology, successfully preparing modified P-D2 exosomes (P-D2-Exos) capable of specifically targeting DCs and offering advantages for allergic rhinitis treatment. Owing to their specific immunomodulatory properties, compared with conventional drugs, P-D2-Exos may achieve superior targeting effects, thereby reducing unnecessary systemic side effects.56 Their research findings revealed that P-D2-Exos could reduce the expression of Fut1, thereby inhibiting the glycosylation of dendritic cells, suppressing the activation of the P38 MAPK signaling pathway, and increasing IL-10 metabolism in DCs. This subsequently inhibited Th2 cell differentiation and ILC2 activation. In an allergic rhinitis mouse model, treatment with P-D2-Exos was able to remodel the metabolic processes of DCs, inhibit Th2 cell differentiation, and further suppress ILC2 activation and alleviate allergic rhinitis symptoms by inhibiting the Fut1/ICAM1/P38 MAPK signaling pathway.57
Modification of NGR Peptide
NGR (GGCNGRC) is a disulfide-constrained cyclic peptide that specifically recognizes the CD13 receptor highly expressed on the surface of DCs, thereby enabling selective targeting of DCs (Figure 4). Zheng et al developed NGR cyclic peptide fragment-based polymeric micelles (NGR-XT-PM) loaded with the anti-inflammatory compound Xanthatin for the treatment of refractory allergic rhinitis. In a mouse model of allergic rhinitis, intranasal administration of NGR-XT-PM exhibited significant and sustained anti-allergic effects, whereas relapse occurred in all animals treated with budesonide, a commercially available control drug. The study revealed that NGR-XT-PM effectively reversed the Th1/Th2 immune imbalance by reducing serum levels of IgE, histamine, and IL-4, downregulating the expression of costimulatory molecules CD80, CD86, and I-A/I-E on DCs, while upregulating Treg cell levels and reducing the proportions of Th2, Th9, and Th17 cells to promote immune tolerance. Further mechanistic studies indicated that Xanthatin exerts its immunomodulatory effects by blocking the COX-2/PGE2 signaling pathway. Therefore, the NGR peptide-based DC-targeted delivery system significantly enhances the anti-allergic rhinitis efficacy of natural products and exhibits superior long-term immunomodulatory advantages over conventional glucocorticoids.58
pH-Responsive Intelligent Delivery Nanosystem
pH-responsive intelligent delivery systems represent another important direction. The pH-responsive targeted nanodelivery system can trigger drug release by taking advantage of the weak acidity of the nasal mucosa microenvironment in the allergic rhinitis nasal cavity, achieving spatiotemporal controlled therapy. The nasal mucosa in allergic rhinitis exhibits an acidic microenvironment. Studies have shown that pH can drop below 7.03 under allergic rhinitis conditions, and pH 5.0 is commonly used as the trigger condition in in vitro studies that simulate the allergic rhinitis environment. This shift from physiological neutrality (normal nasal pH ~7.1) to pathological acidity provides an ideal endogenous trigger for constructing pH-responsive nanoplatforms (Table 1).
Chitosan can serve as a pH-sensitive nanocarrier that triggers drug release within the mildly acidic microenvironment characteristic of nasal pathologies. For instance, Chen et al encapsulated the antibiotic cefminox into chitosan nanogels to create a pH-responsive drug delivery system, termed CEF@CS nanogels, for treating rhinitis caused by methicillin-resistant Staphylococcus aureus (MRSA). The results showed that the chitosan polymer shell of CEF@CS nanogels degraded under acidic conditions, effectively releasing cefminox at the bacterial infection site and inhibiting both MRSA growth and biofilm formation. Thus, CEF@CS nanogels represent an effective pH-responsive drug delivery platform for MRSA-associated rhinitis.59
Diatomite biosilica (DB), a natural nanostructured silica material, has recently gained attention in drug delivery due to its high specific surface area, favorable biocompatibility, and low cost. Peng et al loaded the anti-inflammatory model drug budesonide onto DB nanoparticles and modified the surface with polydopamine and carboxymethyl chitosan to develop a novel pH-responsive nasal drug delivery nanosystem. The resulting nanosystem exhibited significant mucin-binding capacity and antibacterial activity against Staphylococcus aureus, along with pH-responsive release under simulated allergic reaction conditions (pH 5.0, 35°C), as well as high biocompatibility.60
Teng et al conjugated a CCR3-blocking peptide (C) to pH-responsive polyethylene glycol (H) and encapsulated ketotifen (KT) to develop a “nasal in situ assembly” polymer–peptide nanodrug (PHCK). Under acidic nasal conditions, PHCK reassembles into nanofibers that attach to the cell surface, thereby avoiding phagocytosis, enhancing surface retention, improving blockade of eosinophil (EOS) chemotaxis, and inhibiting the late-phase inflammatory response of allergic rhinitis. In a rat model of allergic rhinitis, PHCK treatment significantly and sustainably alleviated allergic symptoms while also markedly reducing the levels of OVA-specific IgE antibody, histamine, IL-4, IL-5, and TNF-α Therefore, this pH-responsive “nasal in situ assembly” nanosystem, which undergoes morphological transformation triggered by pH changes in the nasal cavity, enhances drug delivery efficiency and offers an exploratory strategy for developing nasal drug delivery platforms and improving therapeutic efficacy in allergic rhinitis (Figure 5).20
 |
Figure 5 (A) Synthetic route of PHCK and schematic illustration of long-term treatment of allergic rhinitis. Experimental procedures and therapeutic effects of different treatment groups in rat models. (B) Establishment of a rat model of allergic rhinitis and the process of nasal administration. (C) Weight, (D) rubbing, and (E) sneezing times of rats in different treatment groups after administration. (F) OVA-sIgE, (G) histamine, (H) TNF-α, (I) IL-4, (J) IL-5, and (K) ECP in serum after administration in different treatment groups. Data denote mean ± S.D.; n = 5. Statistics: *** p <0.001, ** p < 0.01, * p<0.05. Adapted with permission from,20 copyright 2023, American Chemical Society. |
Stimuli-Responsive Nanohydrogel
The immunomodulatory properties of nanodurg offer a promising therapeutic strategy for allergic rhinitis. However, challenges such as low bioavailability and short retention time must be addressed before in vivo application. Conventional intranasal administration of nanodurg faces two primary obstacles: the rapid clearance by nasal mucociliary mechanisms, which severely limits drugs retention at the target site; and the complex nasal anatomy, which makes it difficult to retain liquid formulations. For effective delivery of nanodurgs, a biocompatible carrier system is essential to sustain high local drug concentrations. Among emerging candidate platforms, hydrogel nanocomposites have attracted increasing attention due to their excellent plasticity and the potential for precise and efficient release of nanodurgs in clinical applications. Hydrogels are high-hydrated materials composed of cross-linked polymers, possessing suitable mechanical properties, anti-infection capabilities, injectability, and the ability to provide sustained local delivery of various therapeutic agents.61,62 Their use as carriers has demonstrated clear advantages in the treatment of allergic rhinitis. Specifically, certain thermoresponsive hydrogels—such as poloxamer 407 and chitosan-based hydrogels—remain liquid at room temperature and undergo rapid sol-gel transition upon nasal administration at body temperature (37 °C), forming a semi-solid reservoir. This change in physical condition can achieve a stable attachment on the nasal mucosa, avoid mucus-cleaning failure, and enhance local persistence of drugs (Table 1).21 In addition, the three-dimensional network structure of hydrogels provides a sustained-release carrier for drugs. It can be released continuously and stably through diffusion or hydrogel degradation. The above-mentioned method can reduce the risk of cytokine storm due to a single high dose of drugs and maintain stable, long-lasting levels of treatment substances in the local microenvironment through reduced frequency of use compared to traditional treatments.
Wang’s group synthesised a thermoresponsive chitosan-based hydrogel (CHI-hydrogel), prepared using ionic cross-linking, and applied it as a nasal delivery system for BMSC-Exos (BMSC-EVs@CHI hydrogel). At a normal body-temperature sol-gel transformation occurs in this type of hydrogel, thus it can adhere well to the inner surface of the nose and sustain-release by virtue of being porous. In an animal model of allergic rhinitis, treatment with BMSC-EVs@CHI hydrogel promoted continuous release of BMSC-Exos to suppress submucosal eosinophil infiltration, lower the frequency of sneezing and nasal rubbing episodes, decrease peripheral blood Ig level, and restore the Th1/Th2 balance, therefore to rebalance T cell-related cytokine expression both in the nose and systemically. The hydrogel can extend the retention time of BMSC-Exos in the nose, enhance their biocompatibility for use locally, thus improving the treatment outcome of allergic rhinitis through this modification process. An excellent carrier platform to realise the application of active immunotherapy based on MSC-exosomes.63 Wang’s team also designed an MXene-modified gelatinated alginate hydrogel containing hypoxia-inducible MSC-Exo-hEVs@M-GelMA system as a sustained-release system of exosomes. Because hypoxia-induced MSC-Exos show stronger angiogenic and immune-modulating functions than others, thus, they have been used in treating allergic rhinitis.64,65 The obtained hEVs@M-GelMA hydrogel had good properties, including an adhesion rate with the nasal mucosa that met standard requirements and a sustained delivery mechanism for hEVs. Therefore, it could be retained longer at sites within the nose and have improved bioavailability. In addition, the hEVs@M-GelMA hydrogel also had strong ROS-scavenging ability and reduced allergic inflammation in allergic rhinitis via inhibition of oxidative stress. In mice with allergic rhinitis, when the hEVs@M-GelMA hydrogel was used as treatment for relief of allergic rhinitis symptoms, reduction of local eosinophils, inhibition of oxidative stress in nasal tissues. It also suppressed the production of OVA-sIgE in plasma, reduced IL-4 secretion and promoted the upregulation of IL-10 and IFN-γ expression compared to untreated controls or other therapies. As an initial groundwork to support the clinical translation of cell-free therapeutic methods for allergic rhinitis, as outlined by this study.22
Challenges and Opportunities for Clinical Translation
Although nanodrugs have demonstrated substantial progress in preclinical studies of allergen-specific immunotherapy for allergic rhinitis, their clinical translation is still impeded by several critical challenges.
The Toxic of Nanomaterials
The lack of many clinical applications for nanotherapeutics is likely due to a number of related reasons: low therapeutic effectiveness, poor safety, difficulties in reproducibility between production lots, problems in scaling up manufacturing, and complicated regulatory approval procedures. Several biological mechanisms of nanotoxicity include oxidative stress, direct cytotoxicity and pro-inflammatory responses. Notably, some nanomaterials that are at or below the threshold for traditional toxicity have been linked to possible long-term harm in recent years, and thus their safety has not been prioritized by nanosafety experts for a long time.66 The problems of preclinical models in predicting human-relevant nanotoxicity results have also been identified. Most of the traditional animal models have failed to reproduce the relevant physiological changes in humans under the presence of nanomaterials, such as haemotoxicity and genotoxicity. Collectively, the above results show that nanocarriers are not to be regarded as inherently inert or safe delivery systems. Clinically, it has been found that 79% of the failures in Phase II are due to a lack of efficacy rather than safety issues; thus, the design of nanodurgs should be optimized to improve target engagement, pharmacokinetic-pharmacodynamic coupling and disease-specific biological effects.67
The Challenges of Nasal Drug Delivery
Nanodurgs in nasal drug delivery need to overcome many physiological and biochemical barriers sequentially before reaching the top of the nasal epithelial cells, such as mucus trapping, enzymatic degradation and mucociliary clearance. First, nanocarriers should not be too tightly bound by the viscoelastic mucus network and need to be able to move more freely to reach the epithelial surface; secondly, they need to protect the contents of therapeutic agents from degradation by nasal metabolic enzymes (such as peptidases and esterases) during transit; finally, they must be resistant to continuous changes in mucus and mechanical removal caused by coordinated ciliary beating. Together, these factors present difficult design problems for the nasal nanocarriers. Therefore, monofunctional strategies are generally unable to meet all the current demands; thus, rational multimodal engineering of both physicochemical and biological optimisation needs to be adopted. Therefore, an ideal nasal nanodurg delivery system should have the following attributes: (i) It should be customised with various surface modifications, such as dense PEGylation or mucoadhesive ligands, to either enhance mucus penetration or extend the residence time on the mucosa according to the desired pharmacokinetic profile; (ii) Strong nanoencapsulation is required to improve the stability of the drug against enzymatic hydrolysis; (iii) Optimisation of the core physicochemical properties of the particles is necessary, such as a particle size in the range of 10–200 nm, a near-neutral zeta potential, and an optimal aspect ratio, to reduce ciliary clearance while maintaining interaction with epithelial cells; and (iv) The structural and functional design choices must be aligned with the specific aims of treatment (eg, direct nose-to-brain delivery, improved systemic bioavailability, or localised treatment in the nasal cavity).68,69 Although nasal nanodelivery systems have shown good efficacy and safety in preclinical trials so far, many serious problems still need to be resolved before they can be used in people. The problems include: (a) difficulties in large-scale, reproducible and GMP-compliant production of nanodurgs; (b) an incomplete understanding of long-term mucosal biocompatibility, such as the risk of chronic irritation, inflammation and immunogenicity; (c) uncertainty about the pharmacokinetic and toxicological effects of repeated or prolonged dosing; and (d) an unclear regulatory system for nanoscale nasal products, particularly regarding standards for characterisation, quality-by-design (QbD) requirements, and non-clinical to clinical bridging strategies. To address the above deficiencies, integrated, cross-disciplinary cooperation among nanomaterials science, pharmaceutical technology, translational toxicology and clinical development is needed.
The Heterogeneity of Allergic Rhinitis
The substantial heterogeneity of allergic rhinitis—including diverse allergen sensitization patterns, variable inflammatory endotypes (eg, eosinophilic vs. neutrophilic), and differing clinical phenotypes—necessitates precision-tailored nanotherapeutic approaches; however, current platforms predominantly adopt a one-size-fits-all design, limiting their therapeutic relevance across patient subpopulations.70–72 Therefore, immunotype stratification of allergic rhinitis—guided by established biomarkers including peripheral blood eosinophil count, total serum IgE level, and component-resolved allergen-specific IgE profiling—enables the rational design of precision nanodurgs. For the Th2-high endotype, characterized by elevated eosinophil counts and dominant sensitization to house dust mite (HDM) allergens, mucosal-adherent nanoparticles co-loaded with glucocorticoids or siRNA targeting IL-4/IL-13 may be engineered. Surface functionalization with HDM-derived allergenic peptides facilitates nasal administration and active targeting of dendritic cells and mast cells in the nasal mucosa, thereby promoting localized immune tolerance. On the other hand, for patients with a complex poly-sensitized phenotype characterized by significantly elevated total IgE and multiple allergen responses, bio-inspired nanovaccines encapsulating anti-IgE oligonucleotides or rapamycin have been proposed. Nanocarriers are used to target high-affinity IgE receptor (FcεRI)-mediated endocytosis pathways for selective inhibition of mast cell and basophil activation. Component-resolved IgE profiling serves as the basis for personalised nanovaccine strategies; allergen-specific peptides and immunomodulatory adjuvants (such as CpG oligodeoxynucleotides or rapamycin) can be co-encapsulated in biodegradable PLGA nanoparticles and delivered via intranasal or sublingual routes to stimulate antigen-specific regulatory T cell expansion. Together, this biomarker- and immunotype-informed nanotherapeutic system will change the way we treat allergic rhinitis by offering personalised medicine that improves treatment effectiveness and reduces off-target effects and systemic toxicity.
Limitations of Manufacturing Processes and Evaluation Systems
Most of the current studies have been conducted on animals; therefore, large-scale, long-term and carefully controlled clinical trials in humans to verify both safety and effectiveness are still lacking. Therefore, organised preclinical safety tests of the immunogenicity of nanodurg need to be carried out before commencing human trials. In addition to a general anti-drug antibody (ADA) test, other tests for nanomaterial-induced complement system activation will be performed. Measuring the terminal complement complex SC5b-9 alongside the key anaphylatoxins C3a and C5a can serve as reliable indicators of complement activation. Complement-mediated hypersensitivity reactions have been identified as one of the main causes of clinical failure for nanodurg development programmes. Dynamically monitor the level of the main cytokines involved in cytokine release syndrome (such as IL-6, TNF-α and IFN-γ) at the same time as the above. In conjunction with functional degranulation assays for mast cells and basophils, such monitoring can be used to conduct a detailed, mechanism-based study of nanoparticle-induced aberrant activation of these effector cells and thus support the early detection and prevention of severe immune toxicity, such as anaphylactic shock.73,74
Second, through organised experiments and standardised rules, the health risks posed by nanoparticles to humans will be investigated further, such as immune system disorders, damage to organs and protracted toxicity. Given that nanodurgs have a tendency to accumulate in the mononuclear phagocyte system (MPS), such as the liver, spleen and bone marrow, repeated-dose toxicity studies of at least 3–6 months are necessary. The subjects of these studies should be haematopoietic tissue, liver function and immune organs such as the thymus and lymph nodes. Further research is needed on the long-term biodegradation of various classes of nanomaterials (eg, lipid-based, polymeric, and metal-core formulations) to determine their in vivo clearance kinetics and half-lives, as well as to assess the toxicity of degradation products. Additional safety evaluations of intranasally administered nanodurgs need to be conducted, such as assessing nasal mucociliary function (eg, with ex vivo frog palate models), potential olfactory neurotoxicity and local inflammatory responses, as well as eosinophilic infiltration.
Manufacturing nanodelivery systems is also technically demanding and there is currently no harmonised quality-by-design system, so there are significant batch-to-batch variations and a lack of reproducibility; thus, it presents a serious risk to regulatory approval and large-scale production.
The Complex of Regulatory Barriers
In order to establish a complete regulatory system, scientific and standardised assessment and approval standards for nanotherapy drugs need to be set. Therefore, in the early stages of research and development, it is proposed that forward-looking communication be established with leading regulatory authorities, such as the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA), to reach an agreement on the technical requirements, quality attributes and review expectations for different kinds of nanomaterials in the process of clinical translation, thereby enhancing the scientific basis and compliance of the research and development plan and reducing risks during later stages of development.75 Multiple technical guidelines have been issued by the FDA that increase the demands for physical and chemical characterisation of liposomes and other nanodurg formulations, and the key quality attributes now under strict control include particle size distribution, surface charge (Zeta potential), microscopic morphology, structural integrity, and batch-to-batch consistency. EMA has established more cautious and stringent technical standards for the comparability assessment of nanodurgs (especially bridging studies in the event of process changes or site transfers) and long-term safety evaluation (such as tissue accumulation, immune persistence and delayed toxicity).76,77 At the same time, a unified and scalable quality-and-safety assessment system for nanocapsules should be built, and this system needs to include sub-modules for immunogenicity testing and systemic toxicity studies. Standardised application of this system will help to produce high-quality, reproducible and cross-study-comparable data sets, and improve the efficiency and consistency of regulatory review.78
Opportunities Arising from Artificial Intelligence
Conventional drug delivery systems have the following deficiencies: suboptimal bioavailability, uncontrolled drug release kinetics, high inter-individual pharmacokinetic variability, and insufficient target-site specificity. Although nanodurg is expected to solve these problems, it must be designed to rationally select the components of nanocarriers, ensure stability in a colloidal state, and achieve targeted release. Integration of artificial intelligence (AI) and nanodurg has introduced new concepts for research in drug discovery and delivery. AI-driven methods can be used to optimise the design of nanocarriers based on data and precisely predict their in vivo distribution and pharmacokinetics, etc, to improve both the accuracy and effectiveness of therapy.
In recent years, AI and machine learning (ML) have been incorporated into all parts of the design process for nanodurg to improve the efficiency of translation and increase scientific rigor. Drug encapsulation prediction is one of the earliest and well-known applications of AI in this area. Gaussian process regression (GPR), convolutional neural networks (CNNs) and artificial neural networks (ANNs) are employed as AI algorithms to quantify the drug-loading efficiency of nanocarriers. These models can map various kinds of input features, such as nanocarrier composition, physicochemical properties of therapeutic molecules, and important parameters in fabrication, to encapsulation performance with high accuracy and reproducibility; thus, a large number of empirical trial-and-error experiments can be reduced significantly, and preclinical development can be accelerated.79 AI has also found growing use in fine-tuning drug release kinetics. Many interconnected factors determine how nanodurgs are released; these include the composition of carrier materials, physicochemical characteristics of the drug inside, external environments such as pH and temperature, and thus, the underlying kinetic processes are generally complicated and non-linear. To deal with this problem, many machine learning (ML) approaches have been used in conjunction with design of experiments (DoE) to build models, fit these models and predict time-resolved drug release profiles, including XGBoost and Support Vector Machines (SVM), as well as Differential Evolution (DE). Empirical studies have shown that these ML models can effectively capture pH-dependent release dynamics and thus enable quantitative, data-driven design of stimuli-responsive nanocarriers for pH- or temperature-triggered drug release.80,81 Random Forest, XGBoost, k-nearest neighbors (k-NN) and Support Vector Machines (SVM) are ML models that have been widely used to predict endpoints of nanomaterial-induced toxicity, especially oxidative stress. This computational method has great prospects for promoting the long-term safety assessment of intranasally administered nanodurgs in the treatment of allergic rhinitis and thus guiding the development of safer candidate formulations in preclinical research.80 Microfluidic systems and AI algorithms have been integrated to improve the efficiency of process optimisation for nanomaterial synthesis. Real-time monitoring of key process parameters is realised, and in conjunction with generative AI models, such as Time-series Generative Adversarial Networks (TGAN), a hybrid system for data augmentation and intelligent inference can be used to systematically optimise nanoparticle fabrication conditions and improve the reproducibility of various batches.
Integration of AI and nanodelivery technology provides a strong technical basis for improving the therapeutic effect and reducing the side effects of drugs; at the same time, it is expected to help build a new era of intelligent, integrated diagnostic and treatment based on prediction, prevention and precise intervention.
Conclusion and Prospects
Nanodurgs based on immune regulation have opened up new avenues for the therapy of allergic rhinitis. The rapid advancement of various nanodelivery systems has made it possible to precisely deliver immune regulators such as allergens, nucleic acids, and cytokines. At the same time, the inherent immune regulatory activity of nanoparticles also provides a unique advantage for the therapy of allergic rhinitis.5,82 Innovative strategies such as tolerogenic nanovaccines, targeted nanobodies, exosome-based immunotherapy, and intelligent nanodeivery systems produce synergistic therapeutic effects through multiple mechanisms, including regulating the Th1/Th2 balance, inducing Treg expansion, and controlling the ratio of IgA/IgE. Nanodurgs are catalyzing a paradigm shift in the management of allergic rhinitis: transitioning from conventional symptom-oriented therapy to etiology-directed restoration of immune tolerance; advancing from nonspecific drug delivery to cell- and molecule-level precision targeting; and progressing from frequent dosing regimens to long-acting, sustained-release formulations. Although challenges such as large-scale production, safety evaluation, and regulatory approval persist, with the continuous advancement of interdisciplinary research in nanomaterials science, immunology, and pharmaceutical sciences, as well as the gradual introduction of artificial intelligence-assisted design, nano-immunotherapy holds the promise of offering safer, more effective, and more convenient treatment options for patients with allergic rhinitis. Collectively, nanotechnology is transforming all critical dimensions of allergic rhinitis therapeutics.
Disclosure
The authors declare that they have no competing financial interests.
References
1. Cheng X, Zhou Y, Hao Y, et al. Recent studies and prospects of biologics in allergic rhinitis treatment. Int J Mol Sci. 2025;26(10):4509. doi:10.3390/ijms26104509
2. Creticos PS, Gunaydin FE, Nolte H, Damask C, Durham SR. Allergen immunotherapy: the evidence supporting the efficacy and safety of subcutaneous immunotherapy and sublingual forms of immunotherapy for allergic rhinitis/conjunctivitis and asthma. J Allergy Clin Immunol Pract. 2024;12(6):1415–24. doi:10.1016/j.jaip.2024.04.034
3. Yang J, Lei S. Efficacy and safety of sublingual versus subcutaneous immunotherapy in children with allergic rhinitis: a systematic review and meta-analysis. Front Immunol. 2023;14:1274241. doi:10.3389/fimmu.2023.1274241
4. Epstein T, Bernstein DI. Immunotherapy in allergic and mixed rhinitis. Immunol Allergy Clin North Am. 2026;46(1):111–124. doi:10.1016/j.iac.2025.09.008
5. Li K, Jin J, Yang Y, et al. Application of nanoparticles for immunotherapy of allergic rhinitis. Int J Nanomed. 2024;19:12015–12037. doi:10.2147/IJN.S484327
6. Zhao L, Gao Z, Yuan Z, et al. DC-CD4 bispecific tolerogenic nanovesicles induce antigen-specific regulatory T cells and ameliorate collagen-induced arthritis in mice. Nat Commun. 2026.
7. Kiyono H, Ernst PB. Nasal vaccines for respiratory infections. Nature. 2025;641(8062):321–330. doi:10.1038/s41586-025-08910-6
8. Ren Y, Yao D, Wu F, et al. Tolerogenic nanovaccines for the treatment of type I allergic diseases. J Controlled Release. 2025;380:664–685. doi:10.1016/j.jconrel.2025.02.029
9. Hu W, Ma L, Yang G, et al. Der p2‑A20 DNA vaccine attenuates allergic inflammation in mice with allergic rhinitis. Mol Med Rep. 2019;20(6):4925–4932. doi:10.3892/mmr.2019.10760
10. Shi WD, Cao W, Liu Y, Xu Y, Tao ZZ, Dai Q. Construction of recombinant house dust mite group 1 allergen vaccine and study on immune response induced by nasal immunization. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2013;48(1):26–31.
11. Rochman Y, Kotliar M, Klingler AM, et al. Allergen-specific mRNA-lipid nanoparticle therapy for prevention and treatment of experimental allergy in mice. J Clin Invest. 2025;135(21). doi:10.1172/JCI194080
12. Ahn T, Lee DH, Kim G, et al. Non-invasive strategy: developing a topical IL-4Rα-specific nanobody for the treatment of allergic airway diseases. Mater Today Bio. 2024;27:101148. doi:10.1016/j.mtbio.2024.101148
13. Su Y, Sun B, Gao X, Liu S, Hao R, Han B. Chitosan hydrogel doped with PEG-PLA nanoparticles for the local delivery of miRNA-146a to treat allergic rhinitis. Pharmaceutics. 2020;12(10):907. doi:10.3390/pharmaceutics12100907
14. Li J, Morita N, Miura R, Kimura Y, Shinkura R, Kondo T. Intranasal delivery of bryostatin-1 using surface charge-engineered lipid nanoparticles to modulate mucosal defense for allergic rhinitis treatment. Sci Rep. 2026.
15. Wang Z, Shahzad KA, Li D, et al. PLGA-loaded monascin intranasal delivery system: sustained-release and immunomodulatory effect for treatment of allergic rhinitis by improving regulatory T cell function. ACS Appl Bio Mater. 2025;8(7):5718–5731. doi:10.1021/acsabm.5c00387
16. Han SC, Yeon S, Kim H, Park S. Intranasal application of Foxp3 introduced with Poly(d,l-lactic-co-glycolic acid) (PLGA) nanoparticles (Foxp3 NPs) attenuates allergic inflammation in a mouse model of allergic rhinitis. Pharmaceutics. 2025;17(5):575. doi:10.3390/pharmaceutics17050575
17. Shahzad KA, Wang Z, Cai B, et al. Novel pharmaco-exosomal immunotherapy for united airway diseases: PLGA-encapsulated, mesenchymal stem cell-derived exosomes with PPAR-γ agonist for allergic rhinitis and asthma. Stem Cell Res Ther. 2025;16(1):488. doi:10.1186/s13287-025-04624-8
18. Wang Z, Shahzad KA, Li X, et al. Immunomodulatory effect of mesenchymal stem cells-derived extracellular vesicles to modulate the regulatory T cells and Th1/Th2 imbalance in peripheral blood mononuclear cells of patients with allergic rhinitis. Scand J Immunol. 2024;100(6):e13416. doi:10.1111/sji.13416
19. Park IS, Kim JH, Bae JS, Kim DK, Mo JH. The supernatant of tonsil-derived mesenchymal stem cell has antiallergic effects in allergic rhinitis mouse model. Mediators Inflammation. 2020;2020:6982438. doi:10.1155/2020/6982438
20. Teng Z, Yang J, Chen X, Liu Y. Intranasal morphology transformation nanomedicines for long-term intervention of allergic rhinitis. ACS Nano. 2023;17(24):25322–25334. doi:10.1021/acsnano.3c08752
21. Chu K, Chen L, Xu W, et al. Preparation of a paeonol-containing temperature-sensitive in situ gel and its preliminary efficacy on allergic rhinitis. Int J Mol Sci. 2013;14(3):6499–6515. doi:10.3390/ijms14036499
22. Wen X, Zhao C, Zhao Y, Yang J, Cheng J, Wang Z. Multifunctional MXene-modified GelMA hydrogel loaded with hypoxia-induced mesenchymal stem cells derived extracellular vesicles alleviates allergic rhinitis in mice. Int J Biol Macromol. 2024;281(Pt 3):136485. doi:10.1016/j.ijbiomac.2024.136485
23. Koch-Nolte F. Nanobody-based heavy chain antibodies and chimeric antibodies. Immunol Rev. 2024;328(1):466–472. doi:10.1111/imr.13385
24. Wu Y. Trends in nanobody technology in industrialization. Discov Nano. 2025;20(1):23. doi:10.1186/s11671-025-04200-2
25. Aagaard JB, Fischer M, Lober J, et al. Extract-shaped immune repertoires as source for nanobody-based human IgE in grass pollen allergy. Mol Biotechnol. 2023;65(9):1518–1527. doi:10.1007/s12033-023-00664-8
26. Bauernfeind C, Zettl I, Ivanova T, et al. Trimeric Bet v 1-specific nanobodies cause strong suppression of IgE binding. Front Immunol. 2024;15:1343024. doi:10.3389/fimmu.2024.1343024
27. Fu S, Cao Z, Huang B, et al. Tannic acid assisted anti-TNF-α nanobody assembly modulating the epithelial barrier dysregulation of allergic rhinitis. Nano Res. 2023;16(7):9781–9791. doi:10.1007/s12274-023-5646-6
28. Zettl I, Ivanova T, Zghaebi M, et al. Generation of high affinity ICAM-1-specific nanobodies and evaluation of their suitability for allergy treatment. Front Immunol. 2022;13:1022418. doi:10.3389/fimmu.2022.1022418
29. Zhu M, Ma L, Gai J, et al. Preclinical and Phase I randomized study of a potent inhalable nanobody targeting TSLP for the treatment of airway inflammation. J Allergy Clin Immunol. 2025;156(5):1314–1327.e1317. doi:10.1016/j.jaci.2025.06.024
30. Guadarrama-Escobar OR, Serrano-Castañeda P, Anguiano-Almazán E, et al. Chitosan nanoparticles as oral drug carriers. Int J Mol Sci. 2023;24(5):4289. doi:10.3390/ijms24054289
31. Reay SL, Marina Ferreira A, Hilkens CMU, Novakovic K. The paradoxical immunomodulatory effects of chitosan in biomedicine. Polymers. 2024;17(1):19. doi:10.3390/polym17010019
32. Sadeghi M, Asadirad A, Koushki K, Keshavarz Shahbaz S, Dehnavi S. Recent advances in improving intranasal allergen-specific immunotherapy; focus on delivery systems and adjuvants. Int Immunopharmacol. 2022;113(Pt A):109327. doi:10.1016/j.intimp.2022.109327
33. Li D, Li W, Li S, et al. Fabrication of chitosan-based emulsion as an adjuvant to enhance nasal mucosal immune responses. Int J Biol Macromol. 2024;272(Pt 2):132913. doi:10.1016/j.ijbiomac.2024.132913
34. Mo J, Da X, Li Q, Huang J, Lu L, Lu H. The study of exosomes-encapsulated mPEG-PLGA polymer drug-loaded particles for targeted therapy of liver cancer. J Oncol. 2022;2022:4234116. doi:10.1155/2022/4234116
35. Zhang Y, Li X, Fang S, et al. Peroxisome proliferator-activated receptor γ agonist suppresses mast cell maturation and induces apoptosis. Mol Med Rep. 2017;16(2):1793–1800. doi:10.3892/mmr.2017.6802
36. Lakshmi SP, Reddy AT, Banno A, Reddy RC. Airway epithelial cell peroxisome proliferator-activated receptor γ regulates inflammation and mucin expression in allergic airway disease. J Immunol. 2018;201(6):1775–1783. doi:10.4049/jimmunol.1800649
37. Shahzad KA, Wang Z, Li X, Li J, Xu M, Tan F. Immunomodulatory effect of PLGA-encapsulated mesenchymal stem cells-derived exosomes for the treatment of allergic rhinitis. Front Immunol. 2024;15:1429442. doi:10.3389/fimmu.2024.1429442
38. Zhu X, Wang X, Wang Y, Zhao Y. Exosomal long non-coding RNA GAS5 suppresses Th1 differentiation and promotes Th2 differentiation via downregulating EZH2 and T-bet in allergic rhinitis. Mol Immunol. 2020;118:30–39. doi:10.1016/j.molimm.2019.11.009
39. Zhou J, Lu Y, Wu W, Feng Y. HMSC-derived exosome inhibited Th2 cell differentiation via regulating miR-146a-5p/SERPINB2 pathway. J Immunol Res. 2021;2021:6696525. doi:10.1155/2021/6696525
40. Xu X, Li C, Qin Q, Han F, Wang Y. Effect of adipose mesenchymal stem cell-derived exosomes on allergic rhinitis in mice. Heliyon. 2025;11(1):e41340. doi:10.1016/j.heliyon.2024.e41340
41. Han F, Xu X, Wang Y. Influence of adipose mesenchymal stem cell-derived exosomes on the Th2/Treg cells in peripheral blood of the patients with allergic rhinitis and its mechanism. Am J Rhinol Allergy. 2025;19458924251401732.
42. Cho KA, Kim JY, Kim HS, Ryu KH, Woo SY. Tonsil-derived mesenchymal progenitor cells acquire a follicular dendritic cell phenotype under cytokine stimulation. Cytokine. 2012;59(2):211–214. doi:10.1016/j.cyto.2012.04.016
43. Cho KA, Park M, Kim YH, Woo SY, Ryu KH. RNA sequencing reveals a transcriptomic portrait of human mesenchymal stem cells from bone marrow, adipose tissue, and palatine tonsils. Sci Rep. 2017;7(1):17114. doi:10.1038/s41598-017-16788-2
44. Peng YQ, Wu ZC, Xu ZB, et al. Mesenchymal stromal cells-derived small extracellular vesicles modulate DC function to suppress Th2 responses via IL-10 in patients with allergic rhinitis. Eur J Immunol. 2022;52(7):1129–1140. doi:10.1002/eji.202149497
45. Peng YQ, Qin ZL, Fang SB, et al. Effects of myeloid and plasmacytoid dendritic cells on ILC2s in patients with allergic rhinitis. J Allergy Clin Immunol. 2020;145(3):855–867.e858. doi:10.1016/j.jaci.2019.11.029
46. Maric J, Ravindran A, Mazzurana L, et al. Prostaglandin E(2) suppresses human group 2 innate lymphoid cell function. J Allergy Clin Immunol. 2018;141(5):1761–1773.e1766. doi:10.1016/j.jaci.2017.09.050
47. Liu XQ, Peng YQ, Huang LX, et al. Dendritic cells mediated by small extracellular vesicles derived from MSCs attenuated the ILC2 activity via PGE2 in patients with allergic rhinitis. Stem Cell Res Ther. 2023;14(1):180. doi:10.1186/s13287-023-03408-2
48. Pordel S, Haghnavaz N, Rezaee M, et al. An epicutaneous therapeutic pollen-allergen extract delivery system in an allergic rhinitis mouse model: based on allergen loading on DC-specific aptamers conjugated nanogolds. Immunol Res. 2024;72(3):460–475. doi:10.1007/s12026-023-09445-6
49. Keshavarz Shahbaz S, Varasteh AR, Koushki K, et al. Sublingual dendritic cells targeting by aptamer: possible approach for improvement of sublingual immunotherapy efficacy. Int Immunopharmacol. 2020;85:106603. doi:10.1016/j.intimp.2020.106603
50. Chen K, Liu B, Yu B, et al. Advances in the development of aptamer drug conjugates for targeted drug delivery. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2017;9(3). doi:10.1002/wnan.1438
51. Durham SR, Shamji MH. Allergen immunotherapy: past, present and future. Nat Rev Immunol. 2023;23(5):317–328. doi:10.1038/s41577-022-00786-1
52. Boonpiyathad T, Lao-Araya M, Chiewchalermsri C, Sangkanjanavanich S, Morita H. Allergic rhinitis: what do we know about allergen-specific immunotherapy? Front Allergy. 2021;2:747323. doi:10.3389/falgy.2021.747323
53. Sadeghi M, Dehnavi S, Khodadadi A, et al. Immunomodulatory features of MSC-derived exosomes decorated with DC-specific aptamer for improving sublingual immunotherapy in allergic mouse model. Stem Cell Res Ther. 2024;15(1):481. doi:10.1186/s13287-024-04099-z
54. Lewis JS, Zaveri TD, Crooks CP, Keselowsky BG. Microparticle surface modifications targeting dendritic cells for non-activating applications. Biomaterials. 2012;33(29):7221–7232. doi:10.1016/j.biomaterials.2012.06.049
55. Yi S, Zhang X, Sangji H, et al. Surface engineered polymersomes for enhanced modulation of dendritic cells during cardiovascular immunotherapy. Adv Funct Mater. 2019;29(42). doi:10.1002/adfm.201904399
56. Yue J, Hao D, Liu S, et al. Research progress of traditional Chinese medicine in the treatment of allergic rhinitis. Heliyon. 2024;10(7):e29262. doi:10.1016/j.heliyon.2024.e29262
57. Liu J, Wang M, Tian X, et al. New insights into allergic rhinitis treatment: MSC nanovesicles targeting dendritic cells. J Nanobiotechnol. 2024;22(1):575. doi:10.1186/s12951-024-02748-2
58. Zheng X, Sun C, Yu R, et al. CD13-specific ligand facilitates Xanthatin nanomedicine targeting dendritic cells for therapy of refractory allergic rhinitis. Int J Pharm. 2020;577:119034. doi:10.1016/j.ijpharm.2020.119034
59. Chen H, Zhang C, Zhu Z, Shen N. Bioactive chitosan-coated cefminox nanogel as a pH-responsive drug delivery system of Methicillin-resistant Staphylococcus aureus leading to rhinitis and nursing care, an in vitro assessment. Part Sci Technol. 2026;44(1):71–82. doi:10.1080/02726351.2025.2565782
60. Peng G, Cai J, Wang Z, et al. Facile fabrication of diatomite biosilica-based nasal drug delivery vehicle for enhanced treatment of allergic rhinitis. Colloids Surf B. 2024;234:113715. doi:10.1016/j.colsurfb.2023.113715
61. Yuniarsih N, Chaerunisaa AY, Elamin KM, Wathoni N. Polymeric nanohydrogel in topical drug delivery system. Int J Nanomed. 2024;19:2733–2754. doi:10.2147/IJN.S442123
62. Ferozekhan S, Umashankar MS, Narayanasamy D. A comprehensive review of nanogel-based drug delivery systems. Cureus. 2024;16(9):e68633. doi:10.7759/cureus.68633
63. Zhao C, Wei X, Kong W, et al. Mesenchymal stem cell derived extracellular vesicles loaded thermosensitive chitosan-based hydrogel alleviates allergic rhinitis in mouse model. Mater Des. 2023;233:112271. doi:10.1016/j.matdes.2023.112271
64. Niazi V, Ghafouri-Fard S, Verdi J, et al. Hypoxia preconditioned mesenchymal stem cell-derived exosomes induce ex vivo expansion of umbilical cord blood hematopoietic stem cells CD133+ by stimulation of Notch signaling pathway. Biotechnol Prog. 2022;38(1):e3222. doi:10.1002/btpr.3222
65. Gupta S, Rawat S, Krishnakumar V, Rao EP, Mohanty S. Hypoxia preconditioning elicit differential response in tissue-specific MSCs via immunomodulation and exosomal secretion. Cell Tissue Res. 2022;388(3):535–548. doi:10.1007/s00441-022-03615-y
66. Alsaleh NB. Adverse responses of engineered nanomaterials at low and subtoxic exposure levels: current understanding and future perspectives. Nanotoxicology. 2025;19(4):453–473. doi:10.1080/17435390.2025.2516493
67. Herdiana Y. Bridging the gap: the role of advanced formulation strategies in the clinical translation of nanoparticle-based drug delivery systems. Int J Nanomed. 2025;20:13039–13053. doi:10.2147/IJN.S554821
68. Bandi SP, Bhatnagar S, Venuganti VVK. Advanced materials for drug delivery across mucosal barriers. Acta Biomater. 2021;119:13–29. doi:10.1016/j.actbio.2020.10.031
69. Abdulkarim M, Sharma PK, Gumbleton M. Self-emulsifying drug delivery system: mucus permeation and innovative quantification technologies. Adv Drug Delivery Rev. 2019;142:62–74. doi:10.1016/j.addr.2019.04.001
70. Skoner DP. Allergic rhinitis: definition, epidemiology, pathophysiology, detection, and diagnosis. J Allergy Clin Immunol. 2001;108(1 Suppl):S2–8. doi:10.1067/mai.2001.115569
71. Eifan AO, Durham SR. Pathogenesis of rhinitis. Clin Exp Allergy. 2016;46(9):1139–1151. doi:10.1111/cea.12780
72. Yuan Y, Wang C, Wang G, et al. Airway microbiome and serum metabolomics analysis identify differential candidate biomarkers in allergic rhinitis. Front Immunol. 2021;12:771136. doi:10.3389/fimmu.2021.771136
73. Giannakou C, Park M, Bosselaers IEM, et al. Nonclinical regulatory immunotoxicity testing of nanomedicinal products: proposed strategy and possible pitfalls. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2020;12(5):e1633. doi:10.1002/wnan.1633
74. Szebeni J, Storm G. Complement activation as a bioequivalence issue relevant to the development of generic liposomes and other nanoparticulate drugs. Biochem Biophys Res Commun. 2015;468(3):490–497. doi:10.1016/j.bbrc.2015.06.177
75. Velpurisiva P, Gad A, Piel B, Jadia R, Rai P. Nanoparticle design strategies for effective cancer immunotherapy. J Biomed. 2017;2(2):64–77. doi:10.7150/jbm.18877
76. Rodríguez-Gómez FD, Monferrer D, Penon O, Rivera-Gil P. Regulatory pathways and guidelines for nanotechnology-enabled health products: a comparative review of EU and US frameworks. Front Med Lausanne. 2025;12:1544393. doi:10.3389/fmed.2025.1544393
77. Stucchi F, Li M, Castellano G, Cellesi F. Regulatory framework for polymer-based nanotherapeutics in clinical translation. Front Bioeng Biotechnol. 2026;14:1735885. doi:10.3389/fbioe.2026.1735885
78. He J, Wei J, Chen J, Liu T, Long H, Wei W. Stimuli-responsive nasal in situ gel drug delivery systems: from material design to clinical translation. Int J Nanomed. 2026;21:602581. doi:10.2147/IJN.S602581
79. Vengateswaran HT, Habeeb M, Ahmed R, et al. Integrating artificial intelligence for design, optimization and pharmacokinetic prediction in nanoparticle based drug delivery. J Drug Delivery Sci Technol. 2026;115:107805. doi:10.1016/j.jddst.2025.107805
80. Zhang Z, Xiang Y, Laforet J, et al. TuNa-AI: a hybrid kernel machine to design tunable nanoparticles for drug delivery. ACS nano. 2025;19(37):33288–33296. doi:10.1021/acsnano.5c09066
81. Fathi-Karkan S, Rahdar A, Shirzad M. Integrating machine-learning and nanotechnology to quantify pH-modulated oxaliplatin release. Sci Rep. 2025;15(1):42190. doi:10.1038/s41598-025-26145-3
82. Wang Y, Zhou Y, Liang B, et al. Nanoparticle-based targeted drug delivery systems for allergic rhinitis: a comprehensive review. Int J Nanomed. 2026;21:581228. doi:10.2147/IJN.S581228
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Polyethylene Glycols Stimulate Ca2+ Signaling, Cytokine Production, and the Formation of Neutrophil Extracellular Traps
Hinz A, Stankiewicz S, Litewka JJ, Ferdek PE, Sochalska M, Bzowska M
International Journal of Nanomedicine 2024, 19:13165-13181
Published Date: 7 December 2024
Nanomedicine for Acute Kidney Injury: Precision Delivery Strategies, Therapeutic Breakthroughs, Challenges, and Future Perspectives
Wang Y, Wang N, Qu L, Jiao Y, Xiao Z
International Journal of Nanomedicine 2025, 20:14015-14031
Published Date: 22 November 2025
How Effective are Nanotechnology-Based Therapeutics to Treat Autoimmune Diseases
Barakat M, Abu Ershaid JM, Alzaghari LF, Abdulrazzaq SB, Raad D, Hasen E, Al-Qudah RA, Chellappan DK, Athamneh T, Al-Najjar MAA, Ashames A
International Journal of Nanomedicine 2026, 21:562959
Published Date: 20 January 2026
Systemic Immune Dysregulation in Allergic Rhinitis: Mechanisms, Comorbidities, and Implications for Targeted Therapy
Hui D, Shi C, Fan Y, Han M, Wang Y, Sun J, Xue Y, Li E
Journal of Asthma and Allergy 2026, 19:589195
Published Date: 9 March 2026
Nanotechnology-Driven Drug-Delivery Systems: Mechanistic Insights for Pediatric Autism Treatment in 2026
Atashgahi M, Madani F, Webster TJ
International Journal of Nanomedicine 2026, 21:599496
Published Date: 9 June 2026