Back to Journals » International Journal of Nanomedicine » Volume 21
Nanotechnology-Driven Cancer Therapies for Precision Oncology: Advances and Clinical Outlook
Authors Gupta V, Kumar D ![]() , Gupta S, Tanwar R, Jaiswal NK
, Gupta S, Tanwar R, Jaiswal NK ![]() , Islam MM
, Islam MM ![]() , Singh S, Choudhary N, Gowri S, Webster TJ
, Singh S, Choudhary N, Gowri S, Webster TJ ![]() , Faiyazuddin M
, Faiyazuddin M ![]()
Received 17 September 2025
Accepted for publication 6 December 2025
Published 23 January 2026 Volume 2026:21 568254
DOI https://doi.org/10.2147/IJN.S568254
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Eng San Thian
Vrinda Gupta,1 Dinesh Kumar,2 Sonia Gupta,3 Rajni Tanwar,4 Nicky Kumar Jaiswal,5 Md Moidul Islam,5 Shivani Singh,6 Neeraj Choudhary,7 S Gowri,8 Thomas J Webster,9– 12 Md Faiyazuddin13
1The ICFAI University, Baddi, Himachal Pradesh, 174103, India; 2Department of Pharmaceutics, GNA School of Pharmacy, GNA University, Phagwara, Punjab, India; 3Department of Pharmaceutics, Swami Devi Dyal Group of Professional Institute, Barwala, Panchkula, India; 4Department of Pharmaceutics, Department of Pharmaceutical Sciences, Guru Jambeshwar University, Hisar, Haryana, India; 5Department of Pharmaceutical Science, School of Pharmacy, Desh Bhagat University, Fatehgarh Sahib, Punjab, India; 6Department of Pharmacology, School of Pharmaceutical Sciences, Jaipur National University, Jaipur, Rajasthan, India; 7Department of Pharmacognosy, GNA School of Pharmacy, GNA University, Phagwara, Punjab, India; 8PG & Research Department of Physics, Cauvery College for Women, Affiliated to Bharathidasan University, Tiruchirappalli, Tamil Nadu, 600018, India; 9School of Health Sciences and Biomedical Engineering, Hebei University of Technology, Tianjin, People’s Republic of China; 10School of Engineering, Saveetha University, Chennai, Tamil Nadu, India; 11Program in Materials, UFPI, Teresina, Brazil; 12Division of Pre-College and Undergraduate Studies, Brown University, Providence, RI, USA; 13Centre for Global Health Research, Saveetha Institute of Medical and Technical Sciences, Chennai, Tamil Nadu, India
Correspondence: Md Faiyazuddin, Email [email protected] Thomas J Webster, Email [email protected]
Abstract: Cancer continues to pose a global health challenge, with conventional therapies often limited by non-specific toxicity, drug resistance, and an inadequate therapeutic index. Nanotechnology offers transformative opportunities by enabling targeted drug delivery, improved pharmacokinetics, and integrated diagnostic-therapeutic platforms (termed nanotheranostics). This review highlights key nanocarrier systems including liposomes, polymeric nanoparticles, dendrimers, inorganic nanostructures, carbon-based materials, extracellular vesicles, and hybrid platforms with a focus on human studies and clinical translation. Design strategies (such as passive and active tumor targeting, biomimicry, and stimuli-responsive release mechanisms) are discussed in the context of improving tumor selectivity and minimizing systemic toxicity. Recent innovations, including AI-supported nanomedicine design, smart nanorobots, and cell-mediated delivery systems, are also examined. Although multiple nano-formulations such as Doxil®, Abraxane®, and Vyxeos® have reached clinical use, challenges remain including large-scale manufacturing, regulatory pathways, long-term safety evaluation, and cost-effective global accessibility. This review provides a critical appraisal of current evidence, translational bottlenecks, and emerging opportunities to guide future nanomedicine development. Nanotechnology is poised to become a cornerstone of precision oncology, enabling personalized, safe, and effective cancer treatment paradigms.
Keywords: cancer immunotherapy, drug delivery, nanocarriers, nanotheranostics, oncology, precision medicine
Introduction
Cancer is still one of the most serious global health problems of the 21st century, and this disease kills almost 10 million people each year. GLOBOCAN 2024 indicates that there were approximately 20 million new cancer cases and 9.7 million cancer deaths in 2022 alone.1 The most frequent cancers include lung, breast, colorectal, prostate, and stomach, but the most frequent single type of cancer is lung cancer, causing approximately 1.8 million fatalities annually.2 By 2050, the number of cancer cases might top 35 million, for a total rise of 77%, with the sharpest rate of acceleration in low- and middle-income countries. Simultaneously, the nanomedicine oncology market is growing. Specifically, the nanomedicine market is expected to grow at a CAGR of ~11 to 12%, with the largest application in oncology.3 Today, cancer is the second most frequent cause of death in the world.4 The World Health Organization has estimated that by 2040, the global cancer burden could increase to 28.4 million new cases or 47% more new cases by the year 2020, which will largely be due to aging populations, lifestyle factors, environmental exposures and the emerging prevalence of oncogenic infections in some parts of the world.5 Cancer continues to cause high global mortality, and despite major advances in chemotherapy, radiotherapy, targeted therapy, and immunotherapy, many patients still experience limited benefits due to toxicity, resistance, tumor heterogeneity, and inconsistent treatment responses.6 Several FDA-approved nano-formulations, including Doxil®, Abraxane®, Vyxeos®, and NBTXR3, have already demonstrated advantages such as improved drug delivery, reduced systemic side-effects, and enhanced efficacy compared with conventional agents.7 These clinical outcomes highlight the growing role of nanotechnology in addressing unmet needs in cancer treatment and support its potential to advance safer, more precise, and personalized oncology care.8
Although decades of considerable scientific effort has taken place, traditional treatment practices, such as surgery, chemotherapy, radiotherapy, and immunotherapy, remain rather monumental tasks to overcome and eradicate cancer entirely and permanently.9 Although effective at killing rapidly dividing cells, conventional chemotherapeutic agents are widely non-specific and produce acute systemic and collateral damage to healthy tissues.10 The repeated use of such drugs can cause multidrug resistance (MDR) in many different ways, such as the overexpression of cancer cell efflux pumps, genomic mutation, and drug target variation, which considerably decrease the therapeutic effect over time.11 In a similar way, radiotherapy, despite a wide range of applications, can only be applied accurately when it comes to separating malignant tissues and the surrounding normal tissues, invariably leading to off-target treatment and permanent side effects.11 Although the recent introduction of immunotherapies, specifically using the patient’s own immune system, has revolutionized the way in which certain cancers are managed, issues like immune system evasion by cancer cells, patient heterogeneity in treatment response, high costs, and immune-related adverse events continue to serve as high barriers to their universal success. This enduring disparity between benchside to bedside has pushed the oncology community to reconsider the diagnosis, treatment, and vital surveillance of cancers.12 In recent years, precision oncology has created a paradigm shift, the grand objective of which is to match interventions with the genetic microenvironment and molecular traits of the patient-specific tumor. Bioimplants and more personalized therapies have been enabled by technological developments in high-throughput sequencing, multi-omics technology, and biomarker discovery.13 Nevertheless, these insights concerning precise drug delivery and real-time monitoring have yet to be translated to patients effectively, representing a considerable scientific and technical challenge.
For this transitioning field, the paradigm of nanotechnology has become a game changer to tackle most of these age-old challenges. Engineering nanoscale materials (usually less than 100 nm in at least one direction) allows researchers to develop multi-functional nanocarriers, not only protecting therapeutic agents against premature wear, but also increasing their delivery to the tumor destination via passive and/or active targeting. As an example, the enhanced permeability and retention (EPR) phenomenon, which indicates that leaky tumor vasculature permits nanoparticle (NP) entry and retention more easily than that of free small molecules, has been heavily applied for passive targeting.14 In the interim, active targeting schemes allow ligands with antibodies, peptides, and aptamers site-specific tumor-associated cell receptor binding, and offer better targeting to tumor cells, diminishing overall systemic toxicity.15 Nanotechnology platforms applicable to oncological processes have been developed broadly, and include liposomes, polymeric NPs, dendrimers, inorganic nanostructures (eg, gold NPs and iron oxide NPs), carbon-based nanomaterials (eg, carbon nanotubes and graphene materials), and biologically derived nanocarriers such as extracellular vesicles and exosomes.16 Most of these structures can be additionally designed to react to internal (pH, redox, enzymatic, etc.) or external (temperature, magnetic fields, light, etc.) cues, enabling the release of drugs in the tumor microenvironment (TME) in a time and controlled, on-demand fashion.17 In addition to drug delivery, loading diagnostic agents in nanocarriers has given rise to a new field, nanotheranostics, which has provided opportunities to both image and monitor cancer treatment, adaptively adjusting to a therapeutic response living in tandem with precision medicine. Promisingly, some nanomedicine preparations have already been used in clinical settings enhancing pharmacokinetics, minimizing side effects, and enhancing patient outcomes over conventional treatment methods. Among them, examples that one may recall are liposomal doxorubicin (Doxil-R) and albumin-bound paclitaxel (Abraxane-R).18
Nevertheless, despite such developments, serious impediments still exist that have to be overcome prior to the wide availability of nanotechnology-based cancer drugs for humans.19 Problematic questions of mass production, replicability, batch-to-batch variation, regulatory clearance routes, and long-term safety, as well as availability and fair accessibility, are also burning questions that demand cross-disciplinary cooperation and comprehensive translational approaches.20 The purpose of this review is to offer a critical and full overview of the existing and future perspectives of nanotechnology-based cancer treatments. We start by outlining key nanotechnology platforms being studied, with specific features, benefits, and drawbacks of each platform. Various tumor-targeting approaches are discussed next, such as passive accumulation, ligand-based active targeting, stimuli-responsive, and cell-mediated delivery platforms.21 Following this, we proceed to discuss therapeutic applications as diverse as traditional chemotherapy, radiotherapy adjuvants, photothermal therapy, photo dynamic therapy, immunotherapy, gene therapy, and multifaceted synergistic therapies. The convergence of precision and personalized oncology with nanotechnology is described, including omics-based design, biomarker-responsive systems, and newer directions, emphasizing nano-bioinformatics and artificial intelligence (AI)-aided formulation development.22 Additionally, we look at bridging preclinical validation to clinical use, emphasizing success stories, their current clinical trial status, regulatory parameters, consideration of good morals, and the pitfalls that should not be avoided when introducing safe and efficient applications. We conclude by providing a prospective outlook of the developments that are most likely to define the future of nanotechnology in cancer, with the notable mention of smart nanorobots, bioresponsive hydrogels, and adaptive AI-guided nanoplasts.23 Through a holistic and progressive view of the subject, this review aims to make researchers, clinicians, industry stakeholders, and policymakers aware of the paradigm-changing aspects of nanotechnology in the context of redefining cancer care over the decades to come.24
Nanotechnology Platforms in Oncology
Nanotechnology has introduced numerous platforms to overcome the shortcomings of traditional cancer treatment.25 All of these nanocarriers are different in terms of their constitution, plasticity in use, and method of enhancing anti-cancer drug delivery, targeting, and therapeutic effect. This section provides a description of the most notable nanotechnology platforms that are currently at the forefront of enhancing cancer diagnosis and treatment.26
Liposomes
Liposomes have been one of the most clinically proven nanoplatforms, yet recent developments have pushed them much even further than lipid vesicles. The next generation liposomes incorporate active targeting, duplex-purposed payloads, and active real-time imaging (making them smart theranostic platforms).27 The traditional clinical gold standard is liposomal doxorubicin (Doxil®/Caelyx®), which has been approved to treat multiple malignancies with a demonstrable usefulness in reducing cardiotoxicity. In addition to these new liposomal preparations, others are being tested to overcome multi-drug resistance (MDR) and tumor heterogeneity.28 As an example, ThermoDox® (NCT02181075) is a doxorubicin-loaded temperature-sensitive liposome that delivers its drug cargo upon exposure to mild hyperthermia and is in clinical trials to treat breast cancer in recurrent chest walls and hepatocellular carcinoma. On the same note, Marqibo® (Liposomal Vincristine) has been approved by the FDA to treat Philadelphia chromosome-negative ALL, and it is quite evident that drugs with poor pharmacokinetics (PK) can be rescued using liposomes.29 These state-of-the-art designs deploy stimuli-responsive shells that can degrade in acidic or enzymatic environments of the tumor microenvironment (TME). Other research groups are mixing liposomes and immune adjuvants to use as a nano vaccine platform to boost tumor immunogenicity. As an example, personalized neoantigen vaccines (n.b., BNT111, NCT04526899) are being tested as cationic liposome-based mRNA carriers. Moreover, the integration of liposomes with diagnostic agents (eg, gadolinium or fluorophores) and associated methodologies that allow image-guided drug administration are under development.30 There is also an effort to use biomimetic liposomes (such as liposomes coated in cell membranes, eg, cancer cell membranes or platelet membranes) to avoid being detected by the immune system and allow for a more sustained circulation in the body, which has been shown to be effective in preclinical experiments. Liposomes are, in general, incorporating more multi-stimuli, multi-functional smart vesicles, positioning themselves between conventional chemotherapy and more effective targeted, personalized, and image-guided oncology.31
Polymeric NPs
Polymeric NPs no longer merely provide a reservoir for a drug, but instead they are becoming much more advanced platforms that can co-deliver many therapeutics, and conquer chemotherapeutic-resistant cancer cells, even functioning as programmable micro-reactors within tumors.32 They are extremely versatile towards delivering a precision cancer therapy because of their tunable size, surface chemistry, and degradation profiles. Generally, such polymers are FDA-approved including PLGA (poly(lactic-co-glycolic acid)) and PEGylated or stainless-steel natural polymers such as chitosan or hyaluronic acid.33 Due to their predictability in terms of release kinetics and biocompatibility, these biodegradable materials have been developed into a number of polymeric NPs which have moved into clinical evaluation. Among them is BIND-014, which is a docetaxel-loaded, prostate-specific membrane antigen (PSMA)-directed PLGA NP, that has entered Phase II trials (NCT01812746).34 Despite the commercial failure of the original company that developed these materials, clinical results demonstrated increased tumor localization with diminished systemic toxicity, confirming the idea of ligand-targeted polymeric NPs. Further, there has been a new trend to concentrate on dual-delivery techniques. An example is the preclinical testing of PLGA NPs co-encapsulating paclitaxel with MDR1 siRNA in an attempt to silence multiple drug-efflux genes to induce chemo-sensitivity in chemo-resistant tumors. Another trend includes pH/redox dual-responsive polymeric micelles that remain intact when exposed to acidic tumor vicinities and conditions of high glutathione concentrations but will release a drug in a site-specific manner.35
Recently, there have been bioresponsive polymers that can change according to the TME stimulus. As an example, the overexpression of CD44 by cancer cells may be used to actively target hyaluronic acid-coated NPs, as was done in early-stage studies of breast and lung cancers. In addition to delivery, polymeric NPs are increasingly finding use as nanoreactors, loaded with catalytic payloads, which produce cytotoxic reactive oxygen species within cancer cells, a developing line of research in nanocatalytic cancer therapy.36 Polymer design based on AI is also being researched to simulate the ideal architecture to implement multi-agent loading situations and an accurate release profile. Seen cumulatively, polymeric NPs have not only existed as passive carriers, but they are also becoming smart and bioresponsive, programmable platforms that can carry drugs, genes, or immunomodulators and target multiple hallmarks of cancer.37
Dendrimers
Dendrimers can be distinguished by their accurate tree-like branched geometry that provides extraordinary control over size, shape, and surface functionality. Such structural specificity enables dendrimers as not just high-capacity reservoirs of drugs, but also versatile vehicles of genes, imaging probes, and therapeutic adjuvants, making them excellent candidates as truly multifunctional theranostic platforms. PAMAM (polyamidoamine) is the most well-defined dendrimer system to date and has thus been extensively studied as an agent useful in cancer therapy in light of its biocompatibility and functional groups on the surface (namely, amine groups) that can be used to allow for multi-site functionalization.38,39 Although there is still no FDA-approved dendrimer-based anticancer drug, a number of translational studies are underway at the preclinical, early human stage. AZD0466, or an inhibitor of BCL-2/xL, is one of these hopeful candidates since it was delivered within a dendrimer-based scaffold to enhance solubility and ligand release. AZD0466 entered into a clinical trial for hematological malignancies (NCT04214093), demonstrating the possibility to rescue poorly soluble, otherwise complex small molecules with dendrimers.40 Dendrimers have also been considered for gene delivery . The fourth-generation PAMAM dendrimer-siRNA and CRISPR/Cas9 elements were delivered successfully and showed powerful gene downregulation in preclinical solid cancer experiments, treating MDR and overexpression of oncogenes through improved intracellular uptake over naked nucleic acids.
Dendrimer surface functionalization is also quickly moving beyond the state of the art where investigators are functionalizing dendrimer terminals with targeting ligands, eg, folic acid against ovarian cancer or RGD peptides against integrin-overexpressing solid tumors. Dual targeting dendrimers (eg, tumor cells and tumor vasculature at the same time) are now in preclinical testing. Stimuli-responsive dendrimers that break apart in acidic or reductive tumor micro conditions, provisionally guarantee on-demand release of drugs with minimum leakage into non-target environments, have also been a recent trend. Occasional dendrimer structures are under development as a co-delivery depot of MRI contrast agents, resulting in the real-time tracing of biodistribution and therapeutic effects, representing a step towards personalized adaptive dosing.41 A central concern of safety has been maintained because cationic dendrimers can cause membrane disruption at high levels. This is currently being overcome through PEG or zwitterionic coatings to cover surface charges. In general, dendrimers are no longer considered simple, immobile, drug-carrying systems but have been upgraded to intelligent, multi-use, and stimuli responsive transporters in which such drugs are delivered to locations that require them, and in which early-stage clinical trials, such as the AZD0466 (NCT04214093), act as precursors to their future integration into precision oncology.
Inorganic NPs (Gold, Iron Oxide, and Quantum Dots)
Inorganic NPs present unusual optical, magnetic, and catalytic features that allow them to transcend well beyond the realm of conventional drug delivery. These structural versatilities have made these materials multifunctional agents for targeted therapy, hyperthermia, imaging, and combined theranostics.42 One of these pillars include gold NPs (AuNPs) that have strong biocompatibility, tunable size and shape, and a unique surface plasmon resonance that permits photothermal and photodynamic applications. Silica-gold nanoshells, branded as AuroLase 650, were loaded with near-infrared light and used to merge into localized heat to destruct solid tumors in cancer, which entered a pivotal Phase I trial for head and neck cancers (NCT00848042).43 A newer generation of gold nanoshells are increasingly being hybridized with immunoadjuvants to achieve systemic anti-tumor immunity after ablation, turning local ablation into a systemic vaccine-like effect, but despite best-efforts of regulatory bodies to stay apace with progress, due to issues of scalability and control of heat-dosing, such materials have yet to be used clinically.
Some iron oxide NPs (IONPs) have been FDA certified as MRI contrast agents (eg, Ferumoxytol in iron deficiency anemia containing off-label utilization in imaging). They have the potential to be used in drug delivery-based image guidance and for magnetic hyperthermia, in which particles are heated by an alternating magnetic field to kill tumor cells.44 NanoTherm Planisilane-coated iron oxide NPs, bound to a localized magnetic hyperthermia therapy, have been approved by the European regulatory authority with recurrent glioblastoma therapy and prostate cancer and are still in clinical trials (eg, NCT02033447).45
Quantum dots (QDs) are novel semiconductor nanocrystals, which possess unique fluorescence emission, that have been recognized as next-generation imaging probes for the early detection of a tumor, during surgical intervention.46 In contrast, their translation to the clinic has lagged behind because of fears of heavy metal toxicity (eg, cadmium cores) with recent research focussing more on carbon and silicon-based cadmium-free QDs for enhanced biocompatibility. One such promise involves the use of carbon-dot hybrid systems which are a combination of tumor-specific imaging with drug loading and reactive oxygen species (ROS) based photodynamic therapy of triple negative breast cancer in preclinical studies.
More recent developments involve combining inorganic NPs with biomimetic coatings; eg coating gold NPs with cancer cell membranes to improve tumor homing and immune system evasion.47 The next upcoming approach to watch is the production of hybrid nanostructures, eg, gold-iron oxide corediff-shell particles, which integrate magnetic resonance imaging with plasmonic photothermal therapy in one platform. Difficulties persist with regard to bio persistence and routes of clearance of such inorganic materials over the long term. Researchers are overcoming this by engineering ultrasmall inorganic NPs (<10 nm) with the ability to be cleared through the kidneys by renal filtration, thereby reducing the possibility of buildup and development of chronic toxicity. Overall, inorganic NPs are good examples of how physical characteristics at the nanoscale can be used to achieve exact tumor destruction, imaging without needle and hybrid treatment, crossing the line between diagnosis and therapy.48 Current examples of ongoing clinical trials with AuroLase 106 (NCT00848042) and NanoTherm (NCT02033447), confirm their clinical relevance and the growing promise of nanotheranostics.
Carbon-Based Nanostructures (Carbon Nanotubes and Graphene)
Nanomaterials made especially of carbon (such as carbon nanotubes (CNTs) and graphene derivates) have received attention because of their large surface area and controllable functional groups, as well as having superior electrical and photothermal capabilities. Carbon nanostructures can carry biomolecules and contrast image in contrast to many fully dense organic nanocarriers. They make simultaneous delivery, imaging, and controlled external activation possible allowing them to be at the forefront of smart nanomedicine. CNTs refer to cylindrical graphene sheets of single (SWCNT) or multiple (MWCNT) walls.49 They are naturally shaped like needles enabling for efficient cell uptake and work as nanoneedles to inject therapeutic agents (drug, genes, or imaging agents) directly into the cytoplasm skipping the conventional endocytosis routes. Yet clean CNTs can be highly toxic because of hydrophobic agglomeration and remaining unreacted metal catalysts, thus, large bodies of research have been directed at CNT functionalization to decrease toxicity.50 Newer developments have centered on functionalizing CNTs with hydrophilic polymers (eg, PEGylation) or with targeting ligands to limit off-targeting and increase tumor specificity. As an illustration, folate-conjugated PEGylated SWCNTs were found to considerably accumulate in folate receptor-positive ovarian cancer cells. Although none of the CNT-based oncology drugs are in clinical trials presently, preclinical programs exhibit potent tumor ablation with a combination of CNTs and near-infrared (NIR) light in photothermal therapy.
Graphene oxide (GO) and reduced form (rGO) have plenty of oxygen-containing groups which provide high-capacity drug loading, surface modification, and stimulated release.51 GO-based nanosheets have shown synergy with chemotherapy and photothermal therapy: they can convert NIR light into heat (greatly enhancing cytotoxicity). As an example, PEGylated GO conjugated with doxorubicin possessed increased efficacy against breast cancer xenografts by avoiding efflux pumps and anytime release. Meanwhile, an important translational thrust has been focussed on hybrid carbon-based composites – combining GO or CNTs with metals (gold, iron oxide) or polymers – to form multifunctional constructs serving as combined therapeutic and imaging agents.52
A potentially interesting current research area involves synthesizing graphene-quantum dot hybrids to delineate tumor margins in real-time in an intraoperative setting. Their safety and clearance have been among the major bottlenecks for clinical translation. Recent research is overcoming this by designing ultrasmall carbon dots (<10 nm) capable of remaining highly photoluminescent while being eliminated renally. Further, biomimetic methods, ie, covering CNTs or GO with cancer cell membranes, have also been investigated to increase immune cell evasion, thus, extending circulation.53 NA is yet another innovation, under AI guidance. Functional group densities and aspect ratios are being optimized by machine learning, at a desirable drug-loading density and biocompatibility; a trend that promises rapid standardization for improving regulation. CNTs, along with other nanostructures based on graphene, are a potent family of multifunctional, externally trigger response carriers that are ready to address problems of drug resistance, tumor recidivism, and live tracking situations. They are not currently being tested for oncology but, with a strong preclinical pipeline, are virtually the next generation of precision nano-intervention platforms.54
Extracellular Vesicles / Exosomes
Extracellular vehicles (EVs) and especially exosomes have become nanocarriers of a natural origin, demonstrating distinct benefits impossible to achieve in synthetic systems. Formed as vesicles released by nearly all cell-types, exosomes (30–150 nm) are naturally involved in transporting proteins, lipids, and nucleic acids, thus crucial to cell-to-cell communication; a capability in recent years being introduced to bioinspired cancer nanotherapies. Exosomes possess labile biocompatibility, low immunogenicity and native homing skills that tend to recreate the molecular portrait of cells.4,55 This offers potential as tumor-specific delivery vehicles of both small molecules and nucleic acids, and even CRISPR/Cas9 gene-editing substrates. Their ability to penetrate biological barriers such as the blood-brain barrier (BBB) is one of their strongest potentials that make EVs good candidates for the treatment of brain cancer, such as glioblastoma. Among the clinical studies, a prominent EV example is ExoSTING that uses a STING agonist against cancerous immunity.56 ExoSTING is currently under Phase I development against advanced solid cancers or lymphoma (NCT04592484), which is one of the earliest clinical efforts to use exosomes to re-educate the immune system.57
Despite their strong therapeutic promise, exosomes and genetically engineered exosome-mimics (GEM) face practical barriers for clinical scale-up. Current limitations include low synthesis yield and the absence of standardized, high-throughput GMP-compliant isolation and purification platforms.58 Ultracentrifugation, precipitation, and size-exclusion methods often result in heterogeneous vesicle populations, variable purity, and inconsistent batch potency. Ensuring reproducible cargo loading and stable retention of bioactivity during storage and transport also remains challenging. In addition, exosomes carry endogenous biomolecules whose immunological effects and safety profiles require stringent quality control.59 Emerging solutions such as microfluidic purification, tangential-flow filtration, scalable cell-factory systems, synthetic exosome platforms, and defined-release assays aim to address these issues. However, regulatory clarity and robust manufacturing standards are still required before exosome-based nanotherapies achieve widespread clinical adoption.60
Plant Exosome-like Nanovesicles (ELNVs) which can be pre-potentiated by edible plants (eg ginger) have also shown promise and have been tested in their potential to alter the TME or failing to deliver chemotherapeutics with minimal side effects.61 The latest research includes “designer exosomes” engineered either after isolation or being biosynthetically produced using genetically modified donor cells to achieve tailored therapeutic functions. An example is using tumor-derived exosomes to encapsulate doxorubicin or paclitaxel and to target triple-negative breast cancer through active targeting (surface-engineering) in exosomes (EGFR antibodies). One of the most potential technological breakthroughs is the so-called hybrid exosome system in which natural exosomes are temporarily bound with synthetic liposomes or polymeric NPs to essentially harness the biocompatibility of the natural vesicles and the practical adaptability of the engineered nanocarriers.62 In some preclinical studies, such hybrids have shown increased circulation time, more evasion of the immune system, and increased drug payload. However, EVs and exosomes have major issues regarding clinical translation, such as difficulty in high-scale isolation, consistency of cargo loading or batch-to-batch consistency. As a solution to this, microfluidics and tangential flow filtration scale-up technologies are under development that will be able to scale to clinical-grade products under GMPs.63 Further, exosome mimetics, nanovesicles artificially secreted by cell membranes and having a higher yield than natural exosomes are being studied, although with similar targeting abilities. Taken together, exosomes are a natural example of nature-inspired nanocarriers that can address top challenges related to cancer therapy immune evasion to crossing biological barriers facilitating next-generation immunotherapy, gene editing, and adaptive combination regimens. First-in-human studies, such as ExoSTING (NCT04592484), are crucial to support the validation of exosomes as living smart nanocarriers to support precision oncology.64
Hybrid and Multifunctional Nanocarriers
Hybrid nanocarriers combine organic and inorganic components or multiple organic matrices to integrate targeting, imaging, and therapeutic functions; however, this multifunctionality comes with structural design trade-offs. Increased architectural complexity can influence colloidal stability, surface integrity, and degradation kinetics, potentially affecting release profiles.65 Rigid inorganic cores may enhance stability but slow biodegradation, whereas fully organic hybrids may degrade rapidly and compromise mechanical robustness.66 Current design strategies address this by using modular core-shell architectures, cleavable inorganic–organic linkers, degradable polymer shells, and stimuli-responsive shedding layers to ensure timely disassembly.65 Complementary approaches, such as design-of-experiments-guided optimization, microfluidic synthesis, and biodegradation-rate tuning, allow hybrid systems to balance stability, biodegradability, and control release while retaining clinical feasibility.67
Hybrid and multi-functional nanocarriers are the best of nano-oncology in the modern era in that they synthesize the properties of several materials or design principles into one smart platform that can address the multidimensional nature of cancer. These systems, through the combination of organic, inorganic, and biomimetic components, are capable of delivering, sensing, responding, and adapting at the same time and thus fulfilling the need between specific delivery and real-time theranostics.68 The most prominent ones are lipid polymer hybrid NPs (LPNPs), combining the biocompatibility as well as the long circulation times of liposomes with structure stability and controlled release of polymeric cores.69 LPNPs have demonstrated greater encapsulation efficiency of both hydrophilic as well as hydrophobic drug molecules. One has been the derivation of hybrid systems whereby Genexol-PM (polymeric micelle for paclitaxel; NCT01249293) is derived of micelles assembled with a liposomal shell in a way such that tumor retention is enhanced whilst limiting burst release.70 Another popular design is core-shell NPs. The more usual ones involve a core composed of a polymer or an inorganic material loaded with the drug, with a lipid or PEGylated shell giving stealth and active targeting.70 Examples are gold-liposome hybrids where the photothermal functionality of gold nanoshells and a drug delivery capability of liposomes freely combine to, in this case, exploit heating-activated drug release along with simultaneous imaging. This kind of material has been studied in early clinical trials for recurrent head and neck tumors. Multistage hybrid nanocarriers made in response to sequential tumor barriers represent a frontier innovation. As an example, a NP may first escape detection by immune systems via PEG and afterwards, release its stealth outer surface in the acidic TME to reveal a cell-penetrating peptide to penetrate deep tumors. In vitro models of PLGA cores, lipid layers, and pH-labile linkers have shown enhanced infiltration of hypoxic tumor areas.71 Another emerging family of hybrids iinclude metal-organic frameworks (MOFs) due to their high porosity, pore size that can be tailored, and high payload load capacity, such as proteins and genes.
Current MOF applications include the co-delivery of chemotherapeutics and siRNA or in the production of reactive oxygen species using nanocatalysts to increase tumor killing. There are preliminary studies that combine MOFs with targeting ligands or biomimetic coatings to highlight their potential as the next-generation of adaptive nanomedicine. A promising new route is that of the composite natural/synthetic module, eg, exosome-hybrid-polymer.72 They take advantage of the natural homing and biocompatibility of the exosomes and increase drug loading ability and structural factor with synthetic polymer cores. This hybridization is especially promising in crossing obstacles beyond current capabilities, such as the BBB in glioblastoma treatment, an area of fast preclinical development.73 To even promote multifunctionality further, they are incorporating actual-time diagnostic modules in the hybrid carriers. An example would be contrasting MRI or fluorescence probes co-delivered with therapeutics so clinicians can see not only where and how parts are spreading, but also drug release and response in time, ie a first step towards precision and adaptive dosing in the clinic. Anyhow, multifunctional hybrids are still hard to translate. Scale up, replication of batches, and regulatory approval may be a problem with complicated architectures. Artificial intelligence and high-throughput microfluidic fabrication methods to generate the most efficient hybrid formulation and manufacturing pipelines are emerging techniques to produce the most viable production pipelines.
Altogether, hybrid and multifunctional nanocarriers are the future of smart nanomedicine against cancer - multi-layered, multi-stimuli, multi-modal platforms implemented to outsmart tumor heterogeneities, resistance, and fluctuating micro-environments. In their approach, which includes therapy, imaging, and smart response into the same construct, they reconceptualize how cancer will be treated in the future by clinicians in real time.74
Real-Time Monitoring and Modeling of NP–TME Interactions
To better capture the dynamic nature of the tumor microenvironment, emerging experimental and computational platforms are enabling real-time visualization and prediction of hybrid nanoparticle behavior in vivo. Intravital multiphoton and light-sheet microscopy permit high-resolution monitoring of nanoparticle trafficking, vascular extravasation, and stromal penetration.75 Complementary non-invasive methods such as PET/MRI, photoacoustic imaging, Raman spectroscopy, and FRET-based nanosensors provide longitudinal insight into biodistribution, release kinetics, and TME biochemical changes. On the computational front, agent-based modelling, multiscale pharmacokinetic-pharmacodynamic simulations, spatial systems biology, and AI-driven digital-twin tumor models are increasingly being used to forecast nanoparticle transport, immune modulation, and adaptive TME responses.76 These integrative tools support the rational design and optimization of hybrid nanocarriers by predicting performance in heterogeneous and evolving tumor niches, accelerating the translation of precision nanomedicine.77 An overview comparison is provided in Table 1.
 |
Table 1 Verified Comparison of Nanocarriers in Oncology |
Tumor Targeting Strategies Using Nanotechnology
To address tumor heterogeneity, nanocarriers are increasingly engineered with multi-ligand surfaces (eg, dual targeting of integrins and EGFR), enabling recognition of diverse tumor cell subpopulations. Stimuli-responsive platforms tuned to the tumor microenvironment (pH, enzymes, hypoxia, etc.) allow for adaptive drug release across variable intratumoral niches.84 Biomimetic coatings (platelet, cancer-cell, or macrophage membranes) enhance immune evasion and broad tumor tropism, improving intratumoral penetration despite phenotypic variability.85 Integration of real-time imaging with nanotheranostics also supports adaptive treatment planning for evolving tumor profiles.86 These interactions are shown schematically in Figure 1.
 |
Figure 1 Schematic representation of the dynamic interaction pathways between engineered nanocarriers and the TME. Illustrated steps include: (1) Systemic circulation of nanocarriers, (2) Vascular extravasation via EPR, (3) Ligand-mediated active targeting of tumor-specific receptors, (4) Deep tumor penetration, (5) Navigation and diffusion through the dense extracellular matrix (ECM), (6) Receptor-mediated endocytosis and cellular internalization, (7) Stimuli-responsive drug release triggered by tumor-specific cues (eg, pH, enzymes, redox), (8) Modulation of immune components within the TME to overcome immunosuppression, and (9) Final therapeutic action for maximal antitumor efficacy. |
Passive Targeting and the Enhanced Permeability and Retention (EPR) Effect
Although EPR is an essential concept of tumor nanomedicine, its clinical application has been limited by considerable inter-patient variation and heterogeneity across tumor types. In an attempted revival of the passive delivery approach, most current investigations are swinging to TME priming, a mix of nanomedicines and stroma-corrective medicines that restore the contracted extracellular matrix and shrink tumor blood vessels.87 As a case in point, co-administration with losartan, an angiotensin receptor blocker, has been found promising in blood vessel decompression and NP penetration in desmoplastic malignancies such as pancreatic ductal adenocarcinoma, where Phase 1 data (NCT01821729) shows that perfusion of drugs is enhanced. There are also complementary methods: interstitial transport is additionally increased by enzyme degradation of hyaluronic acid (eg, PEGPH20) and low-dose metronomic chemotherapy.88 In addition to pharmacological preconditioning, patient stratification with advanced image-guided approaches is being developed with the potential to process the most effective patient stratification based on the dynamic contrast-enhanced MRI to detect patients with an already high EPR potential. On-demand delivery can also be achieved with physical methods (such as focused ultrasound and microbubble cavitation), temporarily rupturing tumor vasculature in order to enhance NP extravasation. All of these innovations represent a paradigm shift: rather than giving up on EPR, next-generation training to the TME can enable passive targeting to occur reliably in the clinic.89
While the EPR effect remains an important mechanistic foundation in nanomedicine, increasing clinical evidence confirms that its magnitude is highly variable among patients and tumor types due to vascular heterogeneity, stromal density, and immune pressure within the tumor microenvironment.90 Consequently, passive targeting alone may not guarantee sufficient therapeutic delivery in all clinical settings.91 Emerging approaches including ligand‐decorated active targeting systems, biomimetic nanoparticles (eg, cell membrane–coated carriers), and immune system or cell-mediated delivery (eg, macrophage- and MSC-based vectors) are being developed to complement or bypass EPR dependency. Together, these strategies provide more consistent tumor localization and represent a rational evolution toward hybrid targeting designs in clinical nano-oncology.87
Active Targeting, Ligand Engineering for Multi-Target and Immuno-Smart Nanocarriers
Active targeting has progressed well beyond the traditional ligand labeling with folate or transferrin. The potential of the current frontier entails multi-specific nanocarriers designed to target simultaneously multiple tumor hallmarks. As another instance, NPs with two ligands (ie, RGD peptides (integrins) and VEGFR2 antibodies) have been reported to show synergy when targeting tumors (both cancer cells and vasculature) and are beneficial in targeting heterogeneous tumors by enhancing payload delivery and retention. Immune checkpoint targeting is also being incorporated onto NP surfaces with cutting edge designs.92,93 One of the most promising trends in 2024–2025 was the synthesis of anti-PD-L1-functionalized nanogels that would deliver siRNA or CRISPR components to a tumor and also target the local tyrosine kinase pathway immunosuppressive components, making the tumor-associated macrophages change their phenotype from M2 to the tumoricidal M1.94 The given combinatorial targeting strategy increases specificity, reduces the risk of off-target effects, and resorts to the counteraction of tumor immune evasion decipherly. Furthermore, ligand clustering using multivalent ligands and DNA origami nanoarchitecture are providing the ability to tune ligand density and possess higher avidity with or without loss of stealth. These developments are indicative of an important shift: next-generation active targeting no longer will only serve as a delivery mechanism, but a multi-dimensional, immune-integrated precision-based strategy designed to overcome tumor adaptability.95
Stimuli-Responsive Systems, Logic-Gated Smart Release
Patients and clinical researchers have seen a rapid development in stimuli-responsive nanocarriers in the gradual progress of complex release governed by logic-gates having multi-stimuli control.96 Differential TME signals such as acidic pH, redox gradients, enzyme overexpression, or localized hyperthermia, are also used by these inputs to elicit immediate payload delivery (Figure 1). Some more recent concepts use AND-gate creation, with payloads only being activated in the presence of two or more activators, which greatly minimizes off-target leakage.97 As an example, pH-sensitive linkers and disulfide-bonded hybrids were functionalized on microtomes to be inert in circulation and disintegrate within tumors strongly presented with low-pH and glutathione, in order to guarantee the release of payloads at the appropriate site.98 Temperature-sensitive liposomal doxorubicin, ThermoDox 120microg/mL, showed the prospect of externally activated release in combination with radiofrequency ablation; however, as evidenced in its Phase III results (NCT02181075), thermal-dose specificity was required to achieve success. Innovative ideas in 2025 include nanogels activated by enzymes to break down selectively in tumor-overexpressed matrix metalloproteinases and NPs that can amplify the generation of ROS to enhance chemotherapeutic effects by chemical synergy. The next step is to combine several stimuli-responsive triggers, logic gate and real-time imaging, and this will turn stimuli-responsive systems into intelligent theranostic machines to eradicate the dynamic tumor.99
The physicochemical properties of nanocarriers strongly influence biodistribution and clearance. In general, particles sized ~50–120 nm with near-neutral or zwitterionic surfaces and hydrophilic coatings, such as dense PEG or POx layers, demonstrate prolonged circulation and reduced opsonization, whereas particles <6–8 nm undergo rapid renal clearance and positively charged surfaces are prone to protein adsorption and hepatic uptake.100 These mechanistic factors guide tumor delivery, protein corona interactions, immune recognition, and RES sequestration across platforms including liposomes, polymeric nanoparticles, inorganic systems, and extracellular vesicles.101 Meanwhile, advanced stimuli-responsive and logic-gated nanocarriers are being engineered to discriminate tumor tissue from healthy environments by responding to combinations of cues such as mildly acidic pH, elevated glutathione, hypoxia, or tumor-associated enzymes. Rather than relying on a single trigger, modern systems frequently use AND-logic (eg, pH AND redox) to ensure payload activation only under tumor-specific microenvironmental thresholds, thereby reducing false activation in inflamed or physiologically stressed tissues.102 Safety-interlock strategies, ratiometric sensing, and validated trigger windows help maintain selectivity amid physiological fluctuations, supporting more reliable differentiation between malignant and healthy tissues.103 Collectively, the rational tuning of particle size, charge, hydrophilicity, and logic-gated responsiveness enhances precision delivery and improves translational robustness in diverse tumor settings.104
Cell-Mediated Delivery, Living Taxis for Deep Tumor Penetration
Immune and stem cell-based nanoparticle delivery platforms show strong potential for targeted transport and deep tumor penetration; biosafety considerations are essential for clinical translation. Immune-cell carriers may trigger unintended immune activation or cytokine release if over-stimulated.105 In contrast, stem-cell-based carriers carry a theoretical risk of ectopic engraftment or tumorigenic transformation if proliferative capacity is not carefully controlled.106 To address these concerns, emerging strategies include pre-irradiation or genetic modification to limit cell division, use of apoptotic-switch circuits or drug-inducible kill switches, and thorough ex vivo quality control to ensure immunological compatibility and phenotypic stability. Continued refinement of cell engineering and safety screening is expected further to support the clinical development of living-cell-based nanoparticle delivery systems.107 One of the most revolutionary future tools in nanomedicine is the emergence of cell-based delivery, which would use living cells as a biological carrier to transport NPs past biological obstacles to directly go into the depths of the tumor.
Hitchhiking NPs (such as macrophage-hitchhiking NPs) take advantage of the natural tropism of macrophages to immunologically privileged hypoxic tumor sites.108 Glioblastoma and triple-negative breast cancer preclinical tumor models have demonstrated that macrophages loaded ex vivo with iron oxide or polymeric NPs may migrate into the tumor core past the thick tissue unit. This concept is being actively translated into early-phase clinical research studies such as the City of Hope “The Trojan Horse” cell delivery program. Similarly, nanotherapies with mesenchymal stem cells (MSC) is rising to breach the BBB and reach metastatic niches; GMP grade procedures are now being piloted in Asia in the case of glioma.109 There is also the area of engineered T-cell ferries where T-cells with chimeric antigen receptor (CAR)-T allow deliveries of two-pronged therapies with multiple functions directly into the TME, keeping the cytotoxic T-cell activity intact through attaching NP-based payloads (such as immunostimulatory nanogels or cytokine microcapsules). Cell therapy and nanomaterials represent a living nano-factory with a level of tumor penetration, accuracy, and modulation of immune cells, unequaled in otherwise untreatable cancers.110
Therapeutic Applications
Chemotherapy: Overcoming Multidrug Resistance
Conventional chemotherapy has been limited by the inability to selectively target tumors, toxicity to the whole body and induced MDR through efflux mechanisms such as P-glycoprotein. Nanotechnology is changing this paradigm by introducing smart drug delivery systems that overcome efflux mechanisms, co-deliver chemosensitizers and deliver locally. An example is polymeric micelles co-loaded with paclitaxel and P-glycoprotein inhibitors (including tariquidar) which exhibit impressive tumor retention in MDR models.111 Liposomal doxorubicin (Doxil) is still a landmark; however, more recent stimuli-responsive nano carriers such as pH/redox-sensitive dendrimer-drug conjugates show greater penetration into resistant tumor cores, and release cargoes in a controlled manner among acidic intracellular environments. Markedly, exosome-mimetic NPs constructed from patient cells are in Phase I discovery toward personalized chemo based on patient intrinsic immune system evasion overcoming MDR.112
Radiotherapy: Radiosensitizers
NPs have the ability to become strong generators of radiosensitizers by enhancing local radiation dose deposition and surpassing radioresistance. High-Z NPs are inorganic typically employed in cancer (AuNPs and NBTXR3; Phase III trial NCT04862455) by increasing the photoelectric effect in the tumor, thereby increasing DNA damage. Also, iron oxide NPs that target tumors are under investigation as potential combined hyperthermia-radiosensitizing agents.113 Other potential applications of multifunctional nanoplatforms are the co-delivery of DNA repair inhibitors (such as PARP inhibitors) with metal-based NPs to deliver synergistic effects on both radiosensitization and minimize normal tissue exposure. Trending materials are shape- and size-optimized gold nanorods and biodegradable cerium oxide NPs that scavenge reactive oxygen species in healthy tissues and increase oxidative stress within tumors.114
Photothermal and Photodynamic Therapy
Photothermal therapy (PTT) and photodynamic therapy (PDT) utilize light energy as a spatially selective cancer ablative modality. Nanotechnology takes these modalities a step higher by increasing tumor delivery of therapeutic agents (photothermal materials: Au NPs, CNTs) and photosensitizers (porphyrin-containing liposomes), as well as enhancing the delivery of other therapeutic agents (porphyrin-loaded liposomes).115 Irrespective of whether they convert light to heat (NIR) (as a potent inducer of apoptosis) or generate ROS, at near-infrared (NIR) irradiation, such nanoplatforms are confined to induce apoptosis.116 New developments of theranostic NPs are merging imaging features with PTT/PDT which allows for real time-monitoring. Recovery is new in the form of organic-inorganic hybrid nanogels characterized by dual mode photothermal/photodynamic behavior and exosome-coated graphene quantum dots, providing deep tissue penetration and low-off target damage.117
Nanocarrier Strategies to Modulate PD-1/PD-L1 and CTLA-4 Signaling
Rational nanocarrier design enables spatially and temporally controlled checkpoint modulation to better reverse tumor immune evasion. First, lymph-node–addressed carriers (eg, ~10–50 nm, albumin-hitchhiking or chemokine-decorated) can deliver anti-PD-1/anti-CTLA-4, agonists of co-stimulatory axes (CD40/OX40/4-1BB), or mRNA/siRNA that tune T-cell priming while limiting systemic exposure.118 Second, TME-restricted release via pH/redox/enzyme-responsive shells or photo/ultrasound triggers localize checkpoint blockades and dose-spares to reduce immune-related adverse events. Third, gene-level modulation of PD-L1 on tumor or myeloid cells (siRNA/ASO/CRISPR or miR-34a/miR-200 restoration) downshifts inhibitory signaling upstream of the receptor–ligand interaction.119 Fourth, combo nanotherapies co-deliver checkpoint agents with STING/TLR agonists, cytokines (eg, IL-12), or TAM-reprogramming cargos (CSF1R/PI3Kγ inhibitors) to convert “cold” TMEs to inflamed, checkpoint-responsive states.120 Fifth, logic-gated designs (eg, AND-gates requiring acidic pH and high GSH) and decoy/trap nanoparticles that sequester PD-L1 in the TME further increase on-target specificity. Together, these approaches enhance antigen presentation and effector T-cell function, mitigate systemic toxicity, and provide a tunable framework for synergizing PD-1/PD-L1 and CTLA-4 pathway intervention.121
Immunotherapy: Nanovaccines, mRNA Delivery, and Adjuvants
Nanocarriers (NCs) are transforming cancer immunotherapy by targeting dendritic cells and lymph nodes with the delivery of tumor antigens, immunostimulatory adjuvants or mRNA-based vaccines. The most modern nanovaccines at the clinical-level use lipid NPs (LNPs) to deliver mRNA payload encoding tumor neoantigen-specific vaccines, with success in patients confirmed by the personalized cancer mRNA vaccine platform of BioNTech (eg, BNT122, Phase II NCT03815058).122 Co-loading of STING agonists with checkpoint inhibitors in polymeric NPs has shown augmentation of T-cell activation and infiltration of the TME in malignant melanoma. Additionally, nanoadjuvants are under development based on dendrimers in order to cross-present antigens and re-educate immunosuppressive cancer-associated macrophages (TAMs) to an M1 phenotype in order to enhance the checkpoint blockade immunotherapy response.123
Gene Therapy: SiRNA and CRISPR/Cas9
Genome editing and gene silencing have massive potential for the correction of oncogenic drivers. The prominent barrier of naked nucleic acid instability and off-target delivery is surmounted through the use of NPs.124 Clinical validation of mRNA and siRNA options is demonstrated by the use of lipid NPs, and new-generation polymer and exosomal nanocarries have been tailored for exact gene knockdown and editing. The siRNA therapies developed by Alnylam thus opened up siRNA BCL2, KRAS, or MYC-focused anti-cancer siRNANO-based pipelines. At the same time, CRISPR/Cas9-loaded gold nanoclusters and lipid-based nano-formulations are accelerating towards clinical-grade GMP scale-up with first-in-human trials expected within the next 2–3 years.125
Combination Therapies: Multimodal Synergy
Complex and adaptive tumors are becoming resistant to single-modality therapy. Nano vehicles enhance the spatiotemporal concomitant use of chemo-, radio-, immuno-, and gene therapy, allowing one to harness strong synergistic effects into one platform. Specifically, siRNA to silence MDR genes is co-encapsulated with liposomes to show dramatic tumor regression under pre-clinical breast cancer conditions. Photosensitizers-plus-checkpoint inhibitor nanogels make it possible for both PTT/PDT and immune stimulation to be combined in a single treatment. Smart hybrid nanosystems combine image-guided delivery, logic-gated release and enhanced targeting, and established nanomedicine as the foundation for the next generation of combination oncology.126,127 Some approved and pipeline nanotechnology-based therapies are summarized in Table 2.
 |
Table 2 Approved and Pipeline Nanotechnology-Based Cancer Therapies |
Role in Precision and Personalized Oncology
Advances in multi-omics (genomics, proteomics, metabolomics, etc.) now enable patient-specific nanocarrier design by identifying actionable molecular signatures and dysregulated pathways.128 Tumor-specific biomarkers (such as HER2, EGFR, PD-L1, or KRAS mutations) can guide ligand-functionalization of nanoparticles for targeted delivery. Additionally, transcriptomic profiles can inform co-delivery strategies (eg, siRNA + chemotherapy) to down regulate resistance pathways.129 AI-driven nano-architectures further support personalization by predicting optimal nanoparticle size, surface chemistry, and drug combinations based on patient-specific datasets, thereby aligning nano-therapy with precision oncology frameworks.130 The integrated process is illustrated in Figure 2.
 |
Figure 2 Schematic workflow of personalized nano-oncology, integrating patient-specific omics profiling, biomarker identification, rational NC design, functionalization, real-time imaging, adaptive dosing, and outcome monitoring for precision treatment. The workflow further incorporates real-time imaging and diagnostic feedback for tracking biodistribution and therapeutic response. Adaptive dosing strategies are employed based on dynamic patient data, culminating in continuous outcome monitoring and treatment optimization. This integrated approach aims to enhance therapeutic efficacy, reduce off-target effects, and enable fully personalized cancer nanomedicine. |
Omics-Guided Nanotherapy Design
Omics-guided nanotherapy design takes advantage of the current observed achievements in next-generation sequencing technologies, single-cell RNA profiling, and spatial transcriptomics to unscramble the distinct mutational and molecular characteristics of the tumor of every patient. Such information allows engineered NCs with exclusively customized drug mixtures to be rationally designed – eg simultaneously incorporating a silencing siRNA targeting a patient-specific oncogenic driver coupled with chemotherapeutics within the same platform. Others are also trying to generate “nano-libraries” of narrowly tailored modular carriers that could possibly be quickly reconfigured according to the ever-shifting resistance pattern of a tumor setting the stage of adaptive nanotherapy in real time.131,132
Biomarker-Based Responsive Nanoplatforms
Responsive nanoplatforms based on biomarkers take personalization one step forward. These intelligent systems are able to respond dynamically to tumor-specific signals (ie, like overexpressed enzymes, characteristic pH gradients, redox, or discharge the drugs at the right site at the right time in patients with the right biomarkers). A recent illustration involves matrix metalloproteinase (MMP)-sensitive polymeric micelles, which degrade only in MMP-enriched TMEs, leading to a decreased off-target toxicity.133
Theranostics
Precision treatment is redefining cancer monitoring with theranostics, which fuse imaging and treatment into a single nanoplatform. Theranostic NPs have made it possible to visualize biodistribution, non-invasively monitor a response to treatment, and administer the dosing on the fly by including therapeutic payloads with the real-time imaging agents. To prove this dual role, radiolabeled liposomes, and gold NPs conjugated with PET or MRI contrast agents have already entered early trials.134,135 However, there are design trade-offs in theranostic nanocarriers. Combining imaging and therapeutic functions within one carrier can introduce inherent compromises. First, payload competition for core volume or binding sites may lower drug-loading capacity and entrapment efficiency, while fluorophores or radiolabel chelators can alter surface charge/hydrophilicity, shifting protein-corona composition and increasing RES uptake.136 Second, cargo–cargo interactions (eg, π–π stacking, FRET/quencher effects) can perturb release profiles or attenuate signal-to-noise ratio.137 Third, adding targeting ligands and imaging labels consumes the surface-area budget, sometimes reducing stealth polymer density and colloidal stability (higher PDI/aggregation) or changing zeta potential. These effects may manifest as modified PK/BD, faster clearance, or delayed drug release. To mitigate these trade-offs, designs increasingly use orthogonal compartments (core–shell, liposome-in-polymer, MOF cores, etc.) to segregate imaging and drug domains; ratiometric loading guided by DoE/AI to balance signal and dose; cleavable/activatable linkers (pH/redox/enzymatic) to decouple imaging and therapeutic timing; spacer chemistry to minimize dye-induced quenching; and microfluidic manufacturing to tighten size/PDI and reproducibility.138 Reporting EE%, DL%, PDI, zeta potential, serum stability, release kinetics (tumor-mimetic vs physiological), imaging SNR, and in vivo PK/BD before and after imaging conjugation is also important. In indications where compromises remain unacceptable, a companion diagnostic (separate imaging agent) co-administered with a therapeutic nanoparticle can retain clinical flexibility without overburdening a single construct.139
Nano-Bioinformatics Integration
A nano-bioinformatics interface is becoming an essential factor in precise nano-oncology. Through high-level gender computational modelling and AI algorithms, researchers are able to predict the outcome of interactions between NCs and biological systems, generate reliable NP patient-specific pharmacokinetics, and prescribe improved dosing schedules. Machine learning frameworks are now trained with large multi-omics data to find predictive biomarkers of NP performance, to enable the rational co-design of both carrier and therapeutic payload faster than ever.140,141
Combined, these overlapping approaches give nanotechnology the prospect to no longer be viewed as a tool to deliver drugs but rather as a key tenet to the next generation of precision oncology, whereby treatments are personalized dynamically based on the distinct molecular and microenvironmental signatures of the individual patient’s cancer. Key nanomedicine products and their regulatory pathways are listed in Table 3.
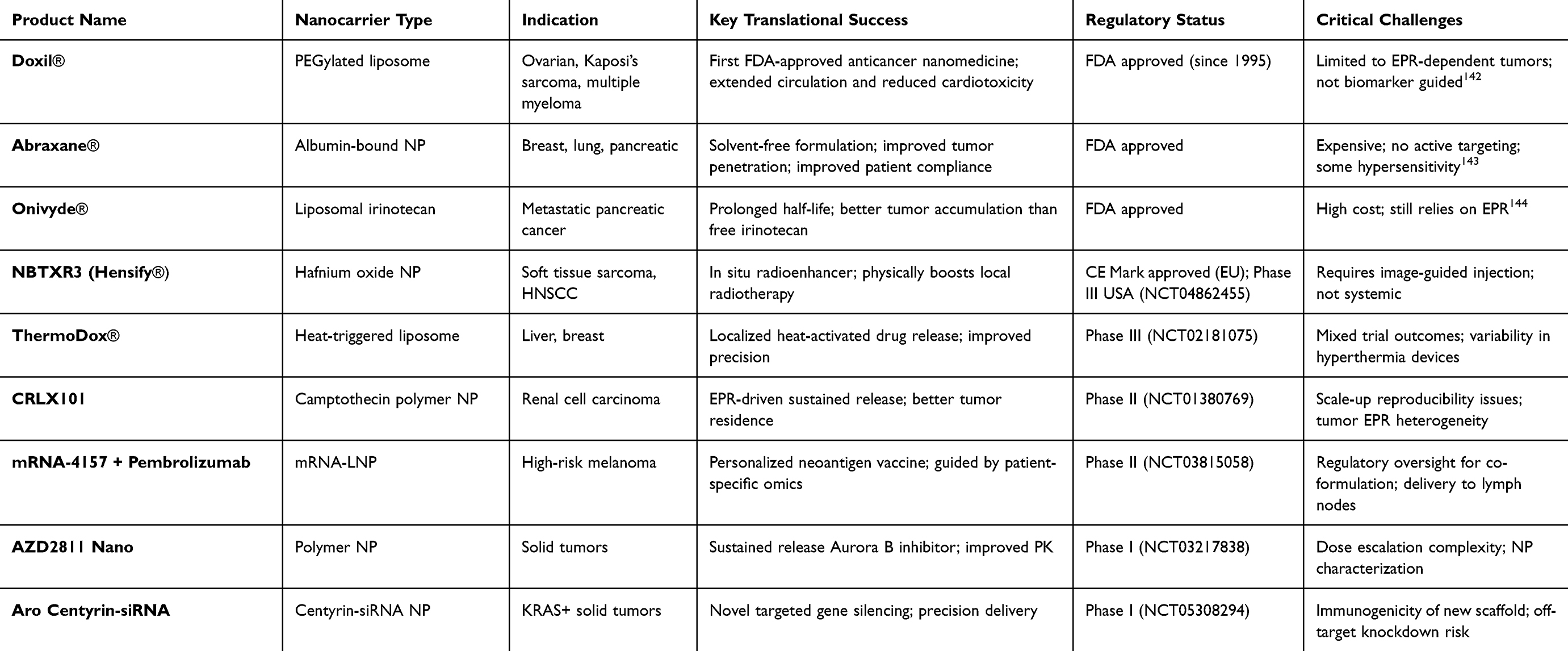 |
Table 3 Selected Nanomedicine Products: Preclinical to Clinical Translation and Regulatory Status |
Case Studies in Nanotechnology-Driven Cancer Therapies
Doxil® (PEGylated Liposomal Doxorubicin)
Doxil® is the first FDA-approved nanomedicine and has transformed the clinical use of doxorubicin by reducing its dose-limiting cardiotoxicity and enhancing tumor targeting through the enhanced permeability and retention (EPR) effect. Its established efficacy in breast and ovarian cancers has made it a benchmark liposomal formulation, with several clinical case studies confirming improved safety, prolonged circulation, and meaningful therapeutic outcomes. Building on this foundation, a mitochondria-targeted liposomal system, SS-02-Doxil®, was developed to further amplify anticancer activity.145 In vitro studies using TUBO breast cancer cells demonstrated that SS-02-Doxil induced significantly greater cytotoxicity compared to conventional Doxil®, driven by enhanced cellular uptake and elevated caspase-3 and caspase-9 activity indicative of stronger apoptosis induction. In vivo BALB/c mice bearing TUBO tumors showed that SS-02-Doxil, particularly with 200 ligand conjugates, produced superior therapeutic benefits by markedly delaying tumor growth (80.86% vs 68.34% for Doxil®), extending median survival (71.25 vs 66.44 days), and improving overall lifespan while maintaining body weight and minimizing systemic toxicity relative to free doxorubicin.146 Biodistribution analysis indicated that while both Doxil and SS-02-Doxil exhibited comparable pharmacokinetics without drastic differences in tumor accumulation versus free drug, SS-02-Doxil demonstrated a modest preferential distribution to tumor and vital organs (liver, kidney, lung, spleen, etc.). Together, these findings highlight that mitochondrial redirection of PEGylated liposomal doxorubicin through SS-02 peptide conjugation meaningfully strengthens its therapeutic profile, building upon the cardioprotective, tumor-targeting advantages already established in the clinical landscape of Doxil®, as summarized in Figure 3.
 |
Figure 3 Antitumor efficacy and histopathological evaluation of different treatment groups. (A) Gross images of excised tumors from each treatment group (Control, Liposome, Doxorubicin [Doxo], Doxil, Apigenin [Ap], AP+Doxo, and AP+Doxil) with antitumor activity (tumor weight (left graph) and tumor size/growth (right graph)) (***P<0.001 Compared with CO, ++P<0.01 Compared with Doxil, ^^P<0.01 Compared with AP, #P<0.01 Compared with all others, and ###P<0.001 Compared with all others). (B) Histopathological analysis of tumor sections by H&E staining at 10× and 40× magnifications showing reduced tumor cell density/necrosis in AP+Doxo and AP+Doxil groups. (C) H&E staining of heart and liver tissues indicating cardiotoxic/hepatotoxic changes with free Doxo, whereas Ap and liposomal formulations reduced systemic toxicity.147. |
Abraxane® (Albumin-Bound Paclitaxel)
Abraxane® represents a major advancement in chemotherapeutic drug delivery by leveraging endogenous albumin transport pathways to enhance intratumoral drug concentration, thereby optimizing paclitaxel bioavailability at the tumor site. The use of albumin NPs enables effective delivery without the need for Cremophor EL, a toxic solvent associated with hypersensitivity reactions in conventional paclitaxel formulations, resulting in improved safety and tolerability profiles in clinical practice. In metastatic breast cancer, Abraxane® has demonstrated favorable response rates, manageable tolerability, and prolonged overall survival, with clinical trials showing a median overall survival of up to 13.6 months and satisfactory safety across diverse patient subgroups. Notably, Abraxane® has also been approved in combination with gemcitabine for metastatic pancreatic cancer, where it achieved a significant increase in median overall survival (8.5 versus 6.7 months) and a substantial improvement in one-year survival rates when compared to standard treatments. These clinical insights highlight that albumin-bound paclitaxel not only enables greater tumor penetration and effective drug concentrations through albumin-mediated pathways but also addresses long-standing safety concerns, making it a valuable therapeutic option for patients facing difficult-to-treat cancers (Figure 4).148
 |
Figure 4 Data mining process and demographic distribution of adverse event reports related to Abraxane. The workflow (top panel) illustrates the extraction and filtering of adverse event reports from pharmacovigilance databases, followed by the application of signal detection algorithms including reporting odds ratio (ROR), proportional reporting ratio (PRR), Bayesian confidence propagation neural network (BCPNN), and empirical Bayesian geometric mean (EBGM). Analyses focused on indications, outcome events and incidence, onset time, and clinical characteristics. Pie charts (bottom panels) represent (A) gender distribution of cases, (B) age distribution of cases, (C) reporter occupation, (D) geographic distribution, (E) routes, and (F) outcomes of reported cases.148 |
NBTXR3 (Hafnium Oxide Radio Enhancer)
In a pivotal phase II/III clinical trial (Act.In.Sarc), NBTXR3, a hafnium oxide NP-based radioenhancer, was evaluated for its ability to improve radiotherapy outcomes in patients with locally advanced soft tissue sarcoma. Administered as a single intratumoral injection before radiotherapy, NBTXR3 acts by amplifying the local energy deposition of radiation, thereby increasing tumor cell death without additional toxicity to surrounding healthy tissues. The study demonstrated a statistically significant improvement in pathological complete response (pCR) rates, with 16% of patients treated with NBTXR3 plus radiotherapy achieving pCR compared to 8% with radiotherapy alone (p=0.044). Moreover, the NBTXR3 group experienced a higher rate of R0 surgical resections (81% vs 66%, p=0.030), indicating better tumor control and resectability. Importantly, the safety profile of NBTXR3 was comparable to radiotherapy alone, with no increase in serious adverse events or negative impact on long-term quality of life. Similar rates of treatment-emergent adverse events and wound complications between groups corroborated this. Mechanistically, NBTXR3 NPs are taken up by tumor cells and, upon radiotherapy activation, generate a higher quantity of electrons that induce amplified DNA damage and reactive oxygen species, resulting in enhanced tumor cell death. Beyond direct cytotoxic effects, emerging research suggests that NBTXR3 may also stimulate immune responses, making it a promising adjunct in combination with immunotherapy. These results position NBTXR3 as a novel and effective nano-radiotherapy agent that enhances the efficacy of standard radiotherapy, leading to improved pathological responses and surgical outcomes in soft tissue sarcoma patients without added toxicity.147
Vyxeos® (Liposomal Cytarabine/Daunorubicin)
Vyxeos® (CPX-351) is a novel liposomal formulation that co-encapsulates cytarabine and daunorubicin in a fixed 5:1 molar ratio designed to optimize the synergistic chemotherapy effect against acute myeloid leukaemia (AML), particularly therapy-related AML (t-AML) and AML with myelodysplasia-related changes (AML-MRC). This lipid NP delivery system provides controlled and sustained release of both drugs, enhances preferential uptake by leukemia cells in the bone marrow, and protects the drugs from rapid metabolism and systemic clearance, thereby overcoming pharmacokinetic differences between the two agents. In a pivotal phase III randomized clinical trial comparing Vyxeos® with conventional 7+3 cytarabine/daunorubicin chemotherapy in older adults (aged 60–75) with newly diagnosed high-risk AML, Vyxeos® significantly improved overall survival (median OS 9.56 vs 5.95 months; hazard ratio 0.69; p=0.003) and increased rates of complete remission (48% vs 33%). The safety profile was manageable and largely consistent with standard chemotherapy, with common side effects including febrile neutropenia, gastrointestinal symptoms, and fatigue. Mechanistically, the liposomal carrier enhances intracellular delivery and retention of the drugs in malignant myeloblasts, which may circumvent drug resistance mechanisms such as P-glycoprotein efflux pumps. Real-world experiences also support its efficacy and tolerability in high-risk AML populations (Figure 5). Thus, Vyxeos® exemplifies how dual-drug liposomal NP co-delivery can optimize chemotherapy regimens to improve therapeutic outcomes in aggressive hematological malignancies without substantially increasing toxicity.149
 |
Figure 5 Demographic and clinical characteristics of adverse event reports associated with Vyxeos®. (A) Geographic distribution of reported cases (world map) and annual distribution of Vyxeos-related adverse event reports. (B) Summary of report characteristics including age, gender, indication/route category, outcomes, reporting country, and reporter type. (C) Time-to-onset distribution stratified by sex.150 |
CRLX101 (Cyclodextrin-Polymer Camptothecin Conjugate)
In a first-in-human phase 1/2a clinical study, CRLX101 (a cyclodextrin-polymer conjugate of camptothecin) designed as a NP approximately 30–40 nm in diameter was evaluated for safety, pharmacokinetics, and preliminary efficacy in patients with advanced solid tumors. The NP formulation improves camptothecin’s solubility and stability at physiological pH, prolonging its plasma half-life and enabling preferential accumulation in tumor tissue through enhanced permeability and retention within tumor vasculature. CRLX101 was administered intravenously using a bi-weekly dosing schedule at a maximum tolerated dose of 15 mg/m2. The treatment was generally well tolerated, with myelosuppression (notably neutropenia) and fatigue being the most common dose-limiting toxicities. Pharmacokinetic analysis revealed prolonged systemic exposure to both polymer-conjugated and unconjugated camptothecin, with dose-proportional plasma concentrations. Clinically, stable disease was the best overall response in 64% of patients treated at the recommended dose, including 73% of a non-small cell lung cancer subgroup, with median progression-free survival of 3.7 months overall and 4.4 months in that subgroup. Preclinical data support CRLX101’s enhanced anticancer activity via sustained topoisomerase I inhibition and downregulation of HIF-1α, leading to anti-angiogenic effects and increased tumor cell death. The cyclodextrin polymer backbone mitigates the typical toxicities associated with camptothecin and facilitates sustained tumor-targeted drug delivery, underscoring CRLX101’s promise as a novel nano-radiotherapy agent for solid tumors with improved pharmacokinetic and toxicity profiles compared to conventional camptothecin.151
ThermoDox® (Thermosensitive Liposomal Doxorubicin)
In a Phase III randomized, double-masked clinical trial (HEAT Study), ThermoDox®, a thermosensitive liposomal formulation of doxorubicin, was evaluated in combination with radiofrequency ablation (RFA) for the treatment of unresectable hepatocellular carcinoma (HCC) lesions measuring 3 to 7 cm. ThermoDox® is engineered to release doxorubicin locally upon exposure to heat (≥40°C), enabling site-specific drug delivery when administered intravenously before RFA-induced tumor hyperthermia. The heat triggers rapid drug release from the liposomes specifically in the heated tumor area, significantly increasing intratumoral drug concentration while minimizing systemic exposure and toxicity. Although the overall trial did not meet its primary endpoints for progression-free and overall survival in the entire study population, a subgroup analysis showed that patients with solitary HCC lesions treated with RFA dwell times of 45 minutes or longer experienced improved overall survival with the combination therapy versus RFA alone. The safety profile was favorable with manageable, reversible myelosuppression similar to free doxorubicin. Subsequent drug development studies highlight the importance of adequate thermal dosing and timing to maximize ThermoDox® efficacy. The thermosensitive liposomal design, combined with hyperthermia for controlled spatial drug release, exemplifies a promising approach for targeted chemotherapy delivery in HCC and other solid tumors, although milestones suggest that NCs can enhance pharmacokinetics.150
CALAA-01 (siRNA-Loaded Polymeric NPs)
CALAA-01 was the first tumor-targeted, cyclodextrin-based siRNA nanotherapeutic evaluated in humans, designed for transferrin-receptor-mediated delivery of RRM2-targeting siRNA. Although early Phase I data confirmed nanoparticle tumor accumulation and RNAi-mediated gene silencing, the trial was ultimately terminated due to dose-dependent immune activation and delivery-related safety concerns. Despite discontinuation, CALAA-01 provided critical insight into the pharmacokinetics, immune interactions, and stability requirements for RNA nanoparticle systems, informing the design of next-generation RNA nanomedicines and highlighting the need for improved biocompatible carriers and controlled delivery strategies.152
Talimogene Laherparepvec (T-VEC, Oncolytic Virus)
A recent case study reported the use of intralesional Talimogene laherparepvec (T-VEC) immunotherapy in a patient with advanced melanoma. The patient, who had multiple cutaneous and subcutaneous melanoma lesions, received T-VEC injections directly into tumors, leveraging its mechanism to selectively replicate in melanoma cells and stimulate localized tumor cell lysis along with an immune response. Over the course of treatment, a significant reduction in tumor size was observed, with some lesions achieving complete remission. The case demonstrated not only the local efficacy of T-VEC in controlling injected tumors but also highlighted systemic immune activation, as some untreated lesions showed regression, indicating an abscopal effect. This clinical experience corroborates outcomes from larger trials and underscores T-VEC’s role as a valuable oncolytic NP therapy option for melanoma patients, particularly those with accessible lesions for intratumoral administration. The patient tolerated the treatment well, experiencing mainly mild flu-like symptoms and manageable injection site reactions, which was consistent.
Regulatory and Translational Perspectives in Nanomedicine
Among nanotechnologies, lipid-based systems (liposomes, LNPs) and albumin-bound platforms currently demonstrate the highest translational maturity due to biocompatibility, established manufacturing workflows, and predictable pharmacokinetics.153 Successful cases such as Doxil®, Abraxane®, Vyxeos®, and mRNA-LNP cancer vaccines show that clinical success correlates with scalable formulation, reproducible quality, and regulatory clarity. Emerging hybrid biomimetic systems and exosome-based carriers show promise, but maturation requires optimized isolation, payload consistency, and FDA-aligned GMP processes. Therefore, translation depends on balancing innovation with manufacturability, safety, and clinical utility.154
Ensuring large-scale reproducibility and batch-to-batch uniformity remains a critical requirement for clinical translation of nanocarriers. Current manufacturing control relies on GMP-compliant processes supported by Quality-by-Design (QbD) frameworks, where critical quality attributes (CQAs) including particle size, PDI, zeta potential, encapsulation efficiency, release kinetics, sterility, and endotoxin levels are continuously monitored.155 Technologies such as microfluidic and continuous-flow synthesis platforms enable precise control over mixing, flow rate, and temperature, significantly improving reproducibility compared to traditional bulk-mixing approaches. In-process analytical tools (eg, DLS, nanoparticle tracking analysis, chromatography, LC-MS, etc.) and real-time process analytical technology (PAT) ensure early detection of deviation and enable corrective adjustments.156 Additionally, predefined release criteria, validated raw-material sourcing, and rigorous documentation further contribute to consistent nanoparticle quality. These advances help minimize batch variability, support regulatory compliance, and enhance scalability for clinical and commercial production.157
FDA Approved Nanomedicines
The clinical translation of nanomedicine in the context of oncology is directly correlated with the development of regulatory factors and desirable product approvals in various jurisdictions. In America, the Food and Drug Administration (FDA) has licensed many nanomedicines that can be used in treating cancer.158 The most remarkable ones are Doxil (1995) (pegylated liposomal doxorubicin), the first nanodrug to be approved by the FDA against ovarian cancer, Kaposi sarcoma, and multiple myeloma, and Abraxane (2005) (albumin-bound paclitaxel) that has been widely used in breast, pancreatic, and non-small-cell lung cancer due to the absence of a solvent and enhanced tumor uptake.159 Approved more recently are Onivyde (liposomal irinotecan, 2015), as a treatment for metastatic pancreatic cancer, and Vyxeos (CPX-351, 2017), a fixed-ratio liposomal combination of daunorubicin and cytarabine for acute myeloid leukaemia. These milestones suggest that NPs can enhance pharmacokinetics, decrease side effects, and allow combination therapies.160 While several nanomedicines (such as Doxil®, Abraxane®, Vyxeos®, and NBTXR3) have demonstrated clinical efficacy and regulatory approval, others have faced challenges in translation.161 For example, CALAA-01, the first polymeric siRNA nanomedicine, was discontinued in Phase I due to immune activation, and ThermoDox® did not meet endpoints in advanced HCC despite promising mechanistic rationale, largely due to challenges in thermal-dose precision and patient selection.162 These examples illustrate that beyond innovative design, clinical success requires optimized delivery conditions, biomarker-guided patient stratification, robust manufacturing, and well-controlled trial execution. Balanced evaluation of successes and failures helps identify translational bottlenecks and guide the development of next-generation nanotherapies.158
EMA/CE Mark Approvals
In Europe, the European Medicines Agency (EMA) and CE Mark have also progressed nanomedicine approvals. One of the first EU clinical nanotechnology applications under the Advanced Therapy Medicinal Products (ATMP) mechanistic framework was NanoTherm (2010) (iron oxide NPs, CE mark 2010) which was authorized to be used for the localized magnetic hyperthermia of recurrent glioblastoma.163 Likewise, NBTXR3 (Hensify, hafnium oxide NP, CE mark 2019) has been approved to enhance radiotherapy in soft tissue sarcoma; an evaluation of this agent in head and neck squamous cell carcinoma is in phase III (NCT04862455). As compared to the US, Europe has actually been rather proactive in the application of nanotechnology to the field of oncology, and there are a couple of products that are currently in clinical use under regional approval systems.164
WHO and ISO Nanotoxicology Frameworks
In addition to regional regulatory bodies, harmonization initiatives are underway in international bodies. According to the WHO, the safety of nanomaterials, accessible and inclusive nanomedicine in essential health strategies should be evaluated. To internationalize regulations, the ISO Technical Committee 229 (Nanotechnologies) will establish uniform definitions and testing protocols to determine the toxicity of the nanoproducts and related risks, after which partner countries could implement them. Simultaneously, the EU Nanomedicine Characterisation Laboratory (EU-NCL) is developing standard characterization protocols on toxicology, pharmacokinetics and biodistribution studies, to be used as a reference by regulatory submissions.165 Collectively, these frameworks will serve to decrease the number of translational barriers, tackle the issue of biosafety, as well as speed up the safe widespread implementation of nanomedicines into the field of oncology.166
Chronic Biosafety and Ethical Considerations
Long-term biosafety remains a pivotal component for the responsible adoption of nanomedicine. While short-term tolerability may be demonstrated in early trials, chronic exposure could lead to delayed immunotoxicity, organ deposition, metabolic dysregulation, or unforeseen genetic or inflammatory effects, especially for non-biodegradable platforms.167 Ethical frameworks, therefore, emphasize robust pre-clinical chronic toxicity testing, along with post-approval pharmacovigilance. Increasingly, real-world evidence strategies such as patient registries, electronic health record monitoring, and structured long-term follow-ups are being implemented to detect potential silent or late-onset toxicities.168 Transparent patient consent processes, safety governance committees, and equitable access considerations also form part of ethical best practices in advancing nanomedicine toward clinical maturity and public trust.
Challenges and Future Outlook
With decades of development so far, the clinical translation of nanotechnology in oncology has continued to experience emerging and dynamic issues, which require programmed scientific, regulatory, and industrial innovation as shown in Table 4.19
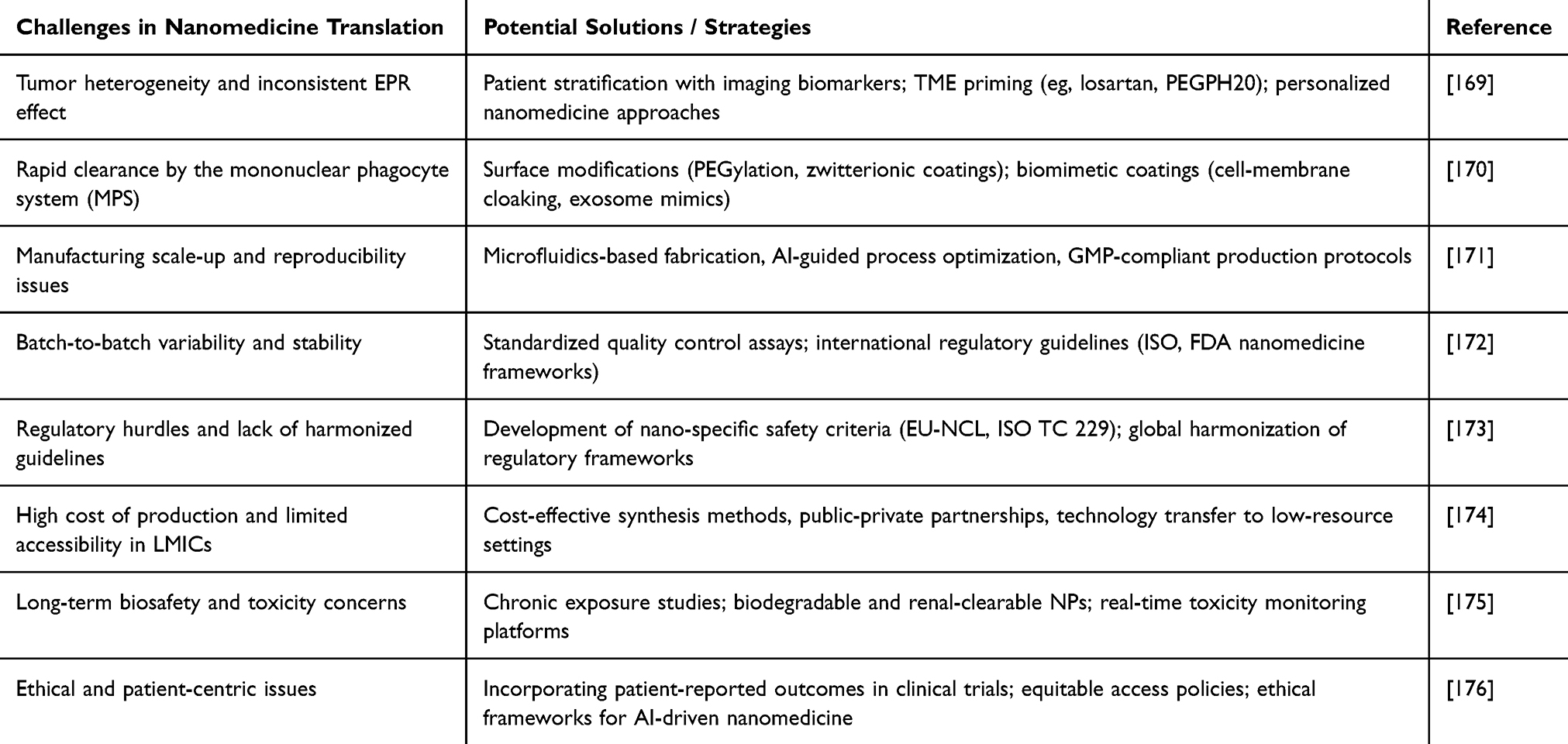 |
Table 4 Challenges vs Potential Solutions in Nanomedicine Translation |
Among the most serious obstacles is tumor heterogeneity, which challenges the consistency of the EPR effect and restricts the reliability of passive targeting among population groups. Tumors in the real world differ widely in vascular permeability, density of stroma, and the immune microenvironment, which can have a significant effect on the accumulation and therapeutic effect of NPs. Immune evasion and clearance are issues of concern.177 The mononuclear phagocyte system (MPS) effectively removes a large number of NPs, especially in the liver and the spleen, thus lowering tumor uptake. Other promising strategies like biomimetic coatings, stealth polymers or cell-derived exosome mimics bring in more complexity when it comes to scale-up and regulatory clearances.178 The other central pump is the manufacturing and cost hurdle. Precise synthesis and surface functionalization result in high batch-to-batch variability and cost of production, which further restricts access to many patients in low-resource healthcare systems, as advanced nanotherapies naturally become inaccessible. There is also inadequate biosafety and long-term toxicity. Although some approved nanodrugs have an established short-term tolerability, further longitudinal investigations are still required to develop chronic exposure risks, off-target build up in organs and immunologic responses.
Internationally agreed nano-specific toxicology criteria, such as those currently promoted by the EU-NCL or the ISO Technical Committee 229, will be valuable for enabling sound clinical assessment. In the future, new technologies provide avenues through which these bottlenecks could be addressed. Advanced Smart, stimuli-responsive NPs, bioresponsive hydrogels, and logic-gated nanorobots hold the promise of more accurately targeted, on-demand drug delivery. Rapid rationalization of NPs will be conferred by incorporating AI-based design and nano-bioinformatics to identify new NC candidates, stratify patients, and continuously refine treatment in real-time patient care.179 Recent advances demonstrate the emerging role of AI in accelerating nanomedicine development. For example, machine-learning-guided polymer design has been used to identify optimal PEGylation density, surface charge, and hydrophobicity parameters for siRNA nanocarriers targeting KRAS-mutant tumors, resulting in improved transfection and tumor inhibition.180 Similarly, deep-learning models trained on nanoparticle physicochemical features have been shown to predict biodistribution profiles and cytotoxic outcomes, enabling rapid formulation screening with reduced laboratory experimentation. AI-assisted models have also been applied to optimize liposome composition for doxorubicin delivery, improving tumor accumulation while minimizing systemic toxicity. These studies highlight the potential of data-driven design in creating tailored, high-performance nanoplatforms for precision oncology.181
With the growing emphasis on precision oncology, emerging digital-twin frameworks and nano-bioinformatics tools offer new opportunities to simulate individualized nanotherapeutic behavior and optimize treatment regimens.182 Digital-twin models integrate patient-specific multi-omics, radiomics, immune profiles, and physiological parameters to forecast nanoparticle biodistribution, immune responses, and TME evolution in silico. These platforms, combined with multiscale nano-PK/PD models, can predict heterogeneous drug release, clearance dynamics, and therapeutic index across tumor sub-regions.183 Meanwhile, machine-learning-powered nano-bioinformatic pipelines analyze nanoparticle-cell interaction data, surface chemistry signatures, and protein-corona fingerprints to tailor carrier design for specific patient phenotypes. Together, these computational strategies enable rational dosing schedule design, adaptive therapy adjustments based on biological feedback, and informed patient stratification ultimately accelerating patient-tailored nanomedicine development and improving clinical outcomes.184
Multi-sensory approaches bringing nanomedicine together with immunotherapy, gene editing, and new imaging are already transforming the delivery of personal cancer care by oncologists. The complete potential of nanotechnology to treat and cure cancer patients may come after all, due to the implementation of interdisciplinary research, open regulations and manufacturing pathways, balanced manufacturing streams, and long-term financing of large-scale patient-based solutions. The philosophy of readily accessible, precision-medicine-oriented nano-oncology is likely to redefine the management of global cancer by 2030 and thereafter as these novel innovations converge.185
Conclusion
Nanotechnology has emerged as a powerful platform in oncology, offering targeted drug delivery, improved pharmacokinetics, and integrated diagnostic–therapeutic functions. This review highlights key nano-systems, including liposomes, polymeric nanoparticles, dendrimers, inorganic and carbon-based nanomaterials, extracellular vesicles, and hybrid nanoplatforms, that are advancing cancer therapy through enhanced tumor specificity, controlled release, and multi-modal treatment strategies. Clinical successes such as Doxil®, Abraxane®, Vyxeos®, and NBTXR3 demonstrate the growing clinical impact of nanomedicine. Despite encouraging progress, challenges remain in scalability, regulatory pathways, biosafety validation, and cost-effectiveness. Looking ahead, the convergence of nanotechnology with precision medicine, immuno-oncology, AI-assisted design, and bio-inspired systems is expected to accelerate translation and support patient-tailored therapies. Overall, nanotechnology is poised to play a central role in the future of precision oncology by delivering safer, more effective, and individualized cancer treatments.
Data Sharing Statement
No data was used for the research described in the article.
Acknowledgment
The authors acknowledge the contributions of colleagues, peers, and their respective institutes, whose insights and support have been valuable to this work.
Author Contributions
Vrinda Gupta and Dinesh Kumar are Joint First Authors. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received in preparing this manuscript.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–33. doi:10.3322/caac.21834
2. Li L, Shan T, Zhang D, et al. Nowcasting and forecasting global aging and cancer burden: analysis of data from the GLOBOCAN and global burden of disease study. J Nat Cancer Center. 2024;4(3):223–232. doi:10.1016/j.jncc.2024.05.002
3. Bizuayehu HM, Ahmed KY, Kibret GD, et al. Global disparities of cancer and its projected burden in 2050. JAMA Network Open. 2024;7(11):e2443198. doi:10.1001/jamanetworkopen.2024.43198
4. Harmanjot K, Islam MM, Kalita J, Chauhan A, Das HK, Singh A. Exosomes in oncology: advancing gene therapy and targeted drug delivery systems. Clin Cancer Drugs. 2025;11:1–14.
5. Ghufran MS, Soni P, Duddukuri GR. The global concern for cancer emergence and its prevention: a systematic unveiling of the present scenario. In: Bioprospecting of Tropical Medicinal Plants. Springer; 2023:1429–1455.
6. Zhang M, Liu C, Tu J, et al. Advances in cancer immunotherapy: historical perspectives, current developments, and future directions. Mol Cancer. 2025;24(1):136. doi:10.1186/s12943-025-02305-x
7. Zhou Y, Wei Y, Tian X, Wei X. Cancer vaccines: current status and future directions. J Hematol Oncol. 2025;18(1):18.
8. Minh Hoang CN, Nguyen SH, Tran MT. Nanoparticles in cancer therapy: strategies to penetrate and modulate the tumor microenvironment – a review. Smart Mater Med. 2025;6(2):270–284. doi:10.1016/j.smaim.2025.07.004
9. Liu B, Zhou H, Tan L, Siu KT, Guan XY. Exploring treatment options in cancer: tumor treatment strategies. Signal Trans Targeted Ther. 2024;9(1):175.
10. Lotfi-Jam K, Carey M, Jefford M, et al. Nonpharmacologic strategies for managing common chemotherapy adverse effects: a systematic review. J Clin Oncol. 2008;26(34):5618–5629. doi:10.1200/JCO.2007.15.9053
11. Catalano A, Iacopetta D, Ceramella J, et al. Multidrug resistance (MDR): a widespread phenomenon in pharmacological therapies. Molecules. 2022;27(3):616. doi:10.3390/molecules27030616
12. Said SS, Ibrahim WN. Cancer resistance to immunotherapy: comprehensive insights with future perspectives. Pharmaceutics. 2023;15(4):1143. doi:10.3390/pharmaceutics15041143
13. Rituraj, Pal RS, Wahlang J, et al. Precision oncology: transforming cancer care through personalized medicine. Med Oncol. 2025;42(7):246. doi:10.1007/s12032-025-02817-y
14. Hou Z, Liu Y, Xu J, et al. Surface engineering of magnetic iron oxide nanoparticles by polymer grafting: synthesis progress and biomedical applications. Nanoscale. 2020;12(28):14957–14975. doi:10.1039/D0NR03346D
15. Elumalai K, Srinivasan S, Shanmugam A. Review of the efficacy of nanoparticle-based drug delivery systems for cancer treatment. Biomed Technol. 2024;5:109–122. doi:10.1016/j.bmt.2023.09.001
16. Mosleh-Shirazi S, Abbasi M, Moaddeli MR, et al. Nanotechnology advances in the detection and treatment of cancer: an overview. Nanotheranostics. 2022;6(4):400. doi:10.7150/ntno.74613
17. Mi P. Stimuli-responsive nanocarriers for drug delivery, tumor imaging, therapy and theranostics. Theranostics. 2020;10(10):4557–4588. doi:10.7150/thno.38069
18. Yan L, Shen J, Wang J, et al. Nanoparticle-based drug delivery system: a patient-friendly chemotherapy for oncology. Dose-Response. 2020;18(3):1559325820936161. doi:10.1177/1559325820936161
19. Chehelgerdi M, Chehelgerdi M, Allela OQB, et al. Progressing nanotechnology to improve targeted cancer treatment: overcoming hurdles in its clinical implementation. Mol Cancer. 2023;22(1):169. doi:10.1186/s12943-023-01865-0
20. Gholami A, Mohkam M, Soleimanian S, et al. Bacterial nanotechnology as a paradigm in targeted cancer therapeutic delivery and immunotherapy. Microsys Nanoeng. 2024;10(1):113. doi:10.1038/s41378-024-00743-z
21. Kumar D, Kumar S, Gholap AD, et al. A comprehensive review on the biomass-mediated synthesis of silver nanoparticles: opportunities and challenges. J Environ Chem Eng. 2025;13(1):115133. doi:10.1016/j.jece.2024.115133
22. Deivayanai VC, Thamarai P, Karishma S, et al. Advances in nanoparticle-mediated cancer therapeutics: current research and future perspectives. Cancer Pathogenesis Ther. 2025;3(4):293–308. doi:10.1016/j.cpt.2024.11.002
23. Lottes AE, Cavanaugh KJ, Chan YY-F, et al. Navigating the regulatory pathway for medical Devices—a conversation with the FDA, clinicians, researchers, and industry experts. J Cardiovasc Transl Res. 2022;15(5):927–943. doi:10.1007/s12265-022-10232-1
24. Marques L, Costa B, Pereira M, et al. Advancing precision medicine: a review of innovative in silico approaches for drug development. Clin Pharmacol Personalized Healthc Pharmaceut. 2024;16(3):332.
25. Sabir S, Thani ASB, Abbas Q. Nanotechnology in cancer treatment: revolutionizing strategies against drug resistance. Front Bioeng Biotechnol. 2025;13:1548588. doi:10.3389/fbioe.2025.1548588
26. Zhu J, Lee H, Huang R, et al. Harnessing nanotechnology for cancer treatment. Front Bioeng Biotechnol. 2025;12. doi:10.3389/fbioe.2024.1514890
27. Cheng X, Gao J, Ding Y, et al. Multi‐functional liposome: a powerful theranostic nano‐platform enhancing photodynamic therapy. Adv Sci. 2021;8(16):2100876. doi:10.1002/advs.202100876
28. Jahangir MA, Mohanty D, Choudhury A, Imam SS. Theranostic applications of functionalized vesicular carriers: theranostic applications of functionalized vesicular carriers (liposomes, niosomes, virosomes, ethosomes, phytosomes). In: Multifunctional and Targeted Theranostic Nanomedicines: Formulation, Design and Applications. Springer; 2023:49–76.
29. Wang X. Preclinical efficacy of heat-activated drug delivery and radiotherapy in breast cancer. University of Toronto (Canada); 2024.
30. Chen W, Zhu Y, He J, et al. Path towards mRNA delivery for cancer immunotherapy from bench to bedside. Theranostics. 2024;14(1):96. doi:10.7150/thno.89247
31. Zhao X, Chen W, Wu J, et al. Application of biomimetic cell membrane-coated nanocarriers in cardiovascular diseases. Int J Nanomed. 2025;Volume 20:8249–8289. doi:10.2147/IJN.S531558
32. Eltaib L. Polymeric nanoparticles in targeted drug delivery: unveiling the impact of polymer characterization and fabrication. Polymers. 2025;17(7):833. doi:10.3390/polym17070833
33. Al Bostami RD, Abuwatfa WH, Husseini GA. Recent advances in nanoparticle-based co-delivery systems for cancer therapy. Nanomaterials. 2022;12(15):2672. doi:10.3390/nano12152672
34. Choksi AU, Khan AI, Lokeshwar SD, et al. Functionalized nanoparticles targeting biomarkers for prostate cancer imaging and therapy. Am J Clin Experim Urol. 2022;10(3):142.
35. Wei X, Song M, Li W, et al. Multifunctional nanoplatforms co-delivering combinatorial dual-drug for eliminating cancer multidrug resistance. Theranostics. 2021;11(13):6334. doi:10.7150/thno.59342
36. Raval H, Bhattacharya S. Exploring the potentials of hyaluronic acid-coated polymeric nanoparticles in enhanced cancer treatment by precision drug delivery, tackling drug resistance, and reshaping the tumour micro environment. Curr Med Chem. 2025;32(20):3960–3999. doi:10.2174/0109298673302510240328050115
37. Long T, Pang Q, Deng Y, et al. Recent progress of artificial intelligence application in polymer materials. Polymers. 2025;17(12):1667. doi:10.3390/polym17121667
38. Pérez-Ferreiro M, M. Abelairas A, Criado A, et al. Dendrimers: exploring their wide structural variety and applications. Polymers. 2023;15(22):4369. doi:10.3390/polym15224369
39. Fana M, Gallien J, Srinageshwar B, et al. PAMAM dendrimer nanomolecules utilized as drug delivery systems for potential treatment of glioblastoma: a systematic review. Int J Nanomed. 2020;Volume 15:2789–2808. doi:10.2147/IJN.S243155
40. Arslan S, Marconi G, Martinelli G, et al. Safety and tolerability of AZD0466 as monotherapy for patients with advanced hematologic malignancies. results from a Phase I/II trial. Blood. 2023;142(Supplement 1):5907. doi:10.1182/blood-2023-179168
41. He H, Li Y, Jia X-R, et al. PEGylated Poly(amidoamine) dendrimer-based dual-targeting carrier for treating brain tumors. Biomaterials. 2011;32(2):478–487. doi:10.1016/j.biomaterials.2010.09.002
42. Merupo V, Zarate JC, Abramova A, Arjona N, Herrera-Celis J, Arriaga LG. Inorganic nanoparticles. Nanochemistry. 2023;33.
43. Hoffmann C, Shen C, Le Tourneau C. Nanoparticle therapy for head and neck cancers. Curr Opin Oncol. 2022;34(3):177–184. doi:10.1097/CCO.0000000000000828
44. Huang Y, Hsu JC, Koo H, et al. Repurposing ferumoxytol: diagnostic and therapeutic applications of an FDA-approved nanoparticle. Theranostics. 2022;12(2):796. doi:10.7150/thno.67375
45. Sorrentino C, Ciummo SL, Fieni C, et al. Nanomedicine for cancer patient‐centered care. MedComm. 2024;5(11):e767. doi:10.1002/mco2.767
46. García de Arquer FP, Talapin DV, Klimov VI, et al. Semiconductor quantum dots: technological progress and future challenges. Science. 2021;373(6555):eaaz8541. doi:10.1126/science.aaz8541
47. Wang R, Yang H, Fu R, et al. Biomimetic upconversion nanoparticles and gold nanoparticles for novel simultaneous dual-modal imaging-guided photothermal therapy of cancer. Cancers. 2020;12(11):3136. doi:10.3390/cancers12113136
48. Khan S, Hossain MK. Classification and Properties of Nanoparticles, in Nanoparticle-Based Polymer Composites. Elsevier; 2022:15–54.
49. Zang Z, Chou S, Zhao Q, et al. A review of the production and application of mesoporous carbon and its potential as an excellent carrier for the adsorptive delivery of compounds. Biochar. 2025;7(1):1–26. doi:10.1007/s42773-025-00439-1
50. Chung JH, Hasyimah N, Hussein N. Application of carbon nanotubes (CNTs) for remediation of emerging pollutants-a review. Tropical Aquatic Soil Pollution. 2022;2(1):13–26. doi:10.53623/tasp.v2i1.27
51. Dubey R, Dutta D, Sarkar A, et al. Functionalized carbon nanotubes: synthesis, properties and applications in water purification, drug delivery, and material and biomedical sciences. Nanoscale Adv. 2021;3(20):5722–5744. doi:10.1039/D1NA00293G
52. Guo W, Chen Z, Feng X, et al. Graphene oxide (GO)-based nanosheets with combined chemo/photothermal/photodynamic therapy to overcome gastric cancer (GC) paclitaxel resistance by reducing mitochondria-derived adenosine-triphosphate (ATP). J Nanobiotechnol. 2021;19(1):146. doi:10.1186/s12951-021-00874-9
53. Gao P, Hui H, Guo C, et al. Renal clearing carbon dots-based near-infrared fluorescent super-small nanoprobe for renal imaging. Carbon. 2023;201:805–814. doi:10.1016/j.carbon.2022.09.052
54. Islam MH, Afroj S, Uddin MA, et al. Graphene and CNT‐based smart fiber‐reinforced composites: a review. Adv Funct Mater. 2022;32(40):2205723. doi:10.1002/adfm.202205723
55. Askenase PW. Ancient evolutionary origin and properties of universally produced natural exosomes contribute to their therapeutic superiority compared to artificial nanoparticles. Int J Mol Sci. 2021;22(3):1429. doi:10.3390/ijms22031429
56. He J, Biswas R, Bugde P, et al. Application of CRISPR-Cas9 System to study biological barriers to drug delivery. Pharmaceutics. 2022;14(5):894. doi:10.3390/pharmaceutics14050894
57. Wang B, Yu W, Jiang H, et al. Clinical applications of STING agonists in cancer immunotherapy: current progress and future prospects. Front Immunol. 2024;15:1485546. doi:10.3389/fimmu.2024.1485546
58. Sharma A, Yadav A, Nandy A, et al. Insight into the functional dynamics and challenges of exosomes in pharmaceutical innovation and precision medicine. Pharmaceutics. 2024;16(6):709. doi:10.3390/pharmaceutics16060709
59. Rezaie J, Feghhi M, Etemadi T. A review on exosomes application in clinical trials: perspective, questions, and challenges. Cell Commun Signal. 2022;20(1):145. doi:10.1186/s12964-022-00959-4
60. Lee KWA, Chan LKW, Hung LC, et al. Clinical applications of exosomes: a critical review. Int J Mol Sci. 2024;25(14):7794. doi:10.3390/ijms25147794
61. Dad HA, Gu T-W, Zhu A-Q, et al. Plant exosome-like nanovesicles: emerging therapeutics and drug delivery nanoplatforms. Mol Ther. 2021;29(1):13–31. doi:10.1016/j.ymthe.2020.11.030
62. Pagani A, Duscher D, Geis S, et al. The triple adipose-derived stem cell exosome technology as a potential tool for treating triple-negative breast cancer. Cells. 2024;13(7):614. doi:10.3390/cells13070614
63. Agrawal P, Wilkstein K, Guinn E, et al. A review of tangential flow filtration: process development and applications in the pharmaceutical industry. Org Process Res Dev. 2023;27(4):571–591. doi:10.1021/acs.oprd.2c00291
64. Mougenot MF, Pereira VS, Costa ALR, et al. Biomimetic nanovesicles—sources, design, production methods, and applications. Pharmaceutics. 2022;14(10):2008. doi:10.3390/pharmaceutics14102008
65. Abdullah M, Obayedullah M, Shariful islam shuvo M, et al. A review on multifunctional applications of nanoparticles: analyzing their multi-physical properties. Results Surfaces Interf. 2025;21:100635. doi:10.1016/j.rsurfi.2025.100635
66. Mishra R, Pal R, Khan Z, Sahoo S, Chawra HS, Kumar D. Solid lipid nanoparticles (SLNPs): a state-of-the-art formulation strategy and their applications against tuberculosis (TB) and analgesic effects. Nanosci Nanotechnol Asia. 2025;15(3):E22106812379362.
67. Zheng G, Zhang B, Yu H, et al. Therapeutic applications and potential biological barriers of nano-delivery systems in common gastrointestinal disorders: a comprehensive review. Adv Compos Hybrid Mater. 2025;8(2):227. doi:10.1007/s42114-025-01292-3
68. Singh P, Sahoo SK. Nano-oncology: clinical application for cancer therapy and future perspectives. In: Cancer Nanotheranostics. Vol. 2. Springer; 2021:49–95.
69. Sivadasan D, Sultan MH, Madkhali O, et al. Polymeric lipid hybrid nanoparticles (PLNs) as emerging drug delivery platform—A comprehensive review of their properties, preparation methods, and therapeutic applications. Pharmaceutics. 2021;13(8):1291. doi:10.3390/pharmaceutics13081291
70. Nam SH, Lee S-W, Lee Y-J, et al. Safety and tolerability of weekly Genexol-PM, a cremophor-free polymeric micelle formulation of paclitaxel, with carboplatin in gynecologic cancer: a phase I study. Cancer Res Treat. 2023;55(4):1346–1354. doi:10.4143/crt.2022.1436
71. Li Y, Sun H, Cao D, et al. Overcoming biological barriers in cancer therapy: cell membrane-based nanocarrier strategies for precision delivery. Int J Nanomed. 2025;Volume 20:3113–3145. doi:10.2147/IJN.S497510
72. Zhang Z-J, Hou Y-K, Chen M-W, et al. A pH-responsive metal-organic framework for the co-delivery of HIF-2α siRNA and curcumin for enhanced therapy of osteoarthritis. J Nanobiotechnol. 2023;21(1):18. doi:10.1186/s12951-022-01758-2
73. Zhang X, Zheng G, Zhou Z, Zhu M, Tang S. Co-delivery of siRNA and cisplatin via electrospun Nanofibrous membranes for synergistic treatment of malignant melanoma. Heliyon. 2024;10(17).
74. Yang D, Yu Z, Zheng M, et al. Artificial intelligence-accelerated high-throughput screening of antibiotic combinations on a microfluidic combinatorial droplet system. Lab on a Chip. 2023;23(18):3961–3977. doi:10.1039/D3LC00647F
75. Li S, Liu L, Shan J, et al. Visualizing cellular interactions: intravital imaging in tumor microenvironment. Front Immunol. 2025;16:1630658. doi:10.3389/fimmu.2025.1630658
76. Subhan MA, Parveen F, Filipczak N, et al. Approaches to improve EPR-based drug delivery for cancer therapy and diagnosis. J Personalized Med. 2023;13(3):389. doi:10.3390/jpm13030389
77. Huai Y, Hossen MN, Wilhelm S, et al. Nanoparticle Interactions with the Tumor Microenvironment. Bioconjug Chem. 2019;30(9):2247–2263. doi:10.1021/acs.bioconjchem.9b00448
78. Chelliah R, Rubab M, Vijayalakshmi S, et al. Liposomes for drug delivery: classification, therapeutic applications, and limitations. Next Nanotechnol. 2025;8:100209. doi:10.1016/j.nxnano.2025.100209
79. Autio KA, Dreicer R, Anderson J, et al. Safety and efficacy of BIND-014, a docetaxel nanoparticle targeting prostate-specific membrane antigen for patients with metastatic castration-resistant prostate cancer: a Phase 2 clinical trial. JAMA Oncol. 2018;4(10):1344–1351. doi:10.1001/jamaoncol.2018.2168
80. Patterson CM, Balachander SB, Grant I, et al. Design and optimisation of dendrimer-conjugated Bcl-2/x(L) inhibitor, AZD0466, with improved therapeutic index for cancer therapy. Commun Biol. 2021;4(1):112. doi:10.1038/s42003-020-01631-8
81. P NN, Mehla S, Begum A, et al. Smart nanozymes for cancer therapy: the next frontier in oncology. Adv Healthc Mater. 2023;12(25):e2300768. doi:10.1002/adhm.202300768
82. Eftekharifar M, Heidari R, Mohaghegh N, et al. Advances in photoactivated carbon-based nanostructured materials for targeted cancer therapy. Adv Drug Delivery Rev. 2025;222:115604. doi:10.1016/j.addr.2025.115604
83. Araujo-Abad S, Berna JM, Lloret-Lopez E, et al. Exosomes: from basic research to clinical diagnostic and therapeutic applications in cancer. Cell Oncol Dordr. 2025;48(2):269–293. doi:10.1007/s13402-024-00990-2
84. Shao X, Zhao X, Wang B, et al. Tumor microenvironment targeted nano-drug delivery systems for multidrug resistant tumor therapy. Theranostics. 2025;15(5):1689–1714. doi:10.7150/thno.103636
85. Kar NP, Lin J, HassankhaniRad A, et al. Smart polymeric nanoparticles for targeted delivery and microenvironment-responsive therapy in pancreatic cancer. Smart Mater Med. 2025;6(3):368–386. doi:10.1016/j.smaim.2025.09.003
86. de Lázaro I, Mooney DJ. Obstacles and opportunities in a forward vision for cancer nanomedicine. Nature Mater. 2021;20(11):1469–1479. doi:10.1038/s41563-021-01047-7
87. Wu J. The enhanced permeability and retention (EPR) effect: the significance of the concept and methods to enhance its application. J Personalized Med. 2021;11(8):771. doi:10.3390/jpm11080771
88. Chawla A, Qadan M, Castillo CF-D, et al. Prospective phase II trials validate the effect of neoadjuvant chemotherapy on pattern of recurrence in pancreatic adenocarcinoma. Ann Surg. 2022;276(5):e502–e509. doi:10.1097/SLA.0000000000004585
89. Takakusagi Y, Kobayashi R, Saito K, et al. EPR and related magnetic resonance imaging techniques in cancer research. Metabolites. 2023;13(1):69. doi:10.3390/metabo13010069
90. Belyaev IB, Griaznova OY, Yaremenko AV, et al. Beyond the EPR effect: intravital microscopy analysis of nanoparticle drug delivery to tumors. Adv Drug Delivery Rev. 2025;219:115550. doi:10.1016/j.addr.2025.115550
91. Izci M, Maksoudian C, Manshian BB, et al. The use of alternative strategies for enhanced nanoparticle delivery to solid tumors. Chem Rev. 2021;121(3):1746–1803. doi:10.1021/acs.chemrev.0c00779
92. Skubalova Z, Rex S, Sukupova M, et al. Passive diffusion vs active pH-dependent encapsulation of tyrosine kinase inhibitors vandetanib and lenvatinib into folate-targeted ferritin delivery system. Int J Nanomed. 2021;Volume 16:1–14. doi:10.2147/IJN.S275808
93. Bajracharya R, Song JG, Patil BR, et al. Functional ligands for improving anticancer drug therapy: current status and applications to drug delivery systems. Drug Delivery. 2022;29(1):1959–1970. doi:10.1080/10717544.2022.2089296
94. Gao J, Zhai Y, Lu W, et al. ROS-sensitive PD-L1 siRNA cationic selenide nanogels for self-inhibition of autophagy and prevention of immune escape. Bioact Mater. 2024;41:597–610. doi:10.1016/j.bioactmat.2024.08.013
95. Tseng CY, Wang WX, Douglas TR, et al. Engineering DNA nanostructures to manipulate immune receptor signaling and immune cell fates. Adv Healthc Mater. 2022;11(4):e2101844. doi:10.1002/adhm.202101844
96. Luo C, He L, Chen F, et al. Stimulus-responsive nanomaterials containing logic gates for biomedical applications. Cell Rep Phy Sci. 2021;2(2):100350. doi:10.1016/j.xcrp.2021.100350
97. Nolan-Stevaux O, Smith R. Logic-gated and contextual control of immunotherapy for solid tumors: contrasting multi-specific T cell engagers and CAR-T cell therapies. Front Immunol. 2024;15:1490911. doi:10.3389/fimmu.2024.1490911
98. Ruiz A, Ma G, Seitsonen J, et al. Encapsulated doxorubicin crystals influence lysolipid temperature-sensitive liposomes release and therapeutic efficacy in vitro and in vivo. J Control Release. 2020;328:665–678. doi:10.1016/j.jconrel.2020.09.032
99. Torres J, Valenzuela Oses JK, Rabasco-álvarez AM, et al. Innovations in cancer therapy: endogenous stimuli-responsive liposomes as advanced nanocarriers. Pharmaceutics. 2025;17(2):245. doi:10.3390/pharmaceutics17020245
100. Panico S, Capolla S, Bozzer S, et al. Biological features of nanoparticles: protein corona formation and interaction with the immune system. Pharmaceutics. 2022;14(12):2605. doi:10.3390/pharmaceutics14122605
101. Kumar D, Tanwar R. Nanoscience and the future: transforming technologies for sustainable development. Curr Engineer Letters Rev. 2025;2(1). doi:10.2174/012666948X386929250411055923
102. Zhang H, Barz M. Investigating the stability of RNA-lipid nanoparticles in biological fluids: unveiling its crucial role for understanding LNP performance. J Control Release. 2025;381:113559.
103. Kumar S, Tomar D, Kumar D, Kishore V. Applications of polymeric nanoparticle in nose to brain drug delivery. Res J Pharm Technol. 2023;16(12):6087–6094.
104. Zhang Y, Hu M, Xin R, et al. Enhanced hydrophilicity and antifouling performance of PEG with sulfoxide-containing side chains for nanomedicine applications. Polymer Sci Technol. 2025;1(7):640–650. doi:10.1021/polymscitech.5c00084
105. Hegde M, Mishra A, Banerjee R, et al. Bioresponsive engineered nanoparticles for immunomodulation. BMC Med. 2025;23(1):595.
106. Kumar D, Tanwar R. World’s first: stem cell therapy reverses diabetes. Stem Cell Res Ther. 2024;15(1):487. doi:10.1186/s13287-024-04036-0
107. Cheng R, Wang S. Cell-mediated nanoparticle delivery systems: towards precision nanomedicine. Drug Delivery Transl Res. 2024;14(11):3032–3054. doi:10.1007/s13346-024-01591-0
108. Wang Y, Sun S-K, Liu Y, et al. Advanced hitchhiking nanomaterials for biomedical applications. Theranostics. 2023;13(14):4781–4801. doi:10.7150/thno.88002
109. Haney MJ, Zhao Y, Jin YS, et al. Macrophage-derived extracellular vesicles as drug delivery systems for triple negative breast cancer (TNBC) therapy. J Neuroimmune Pharmacol. 2020;15(3):487–500. doi:10.1007/s11481-019-09884-9
110. Giorgioni L, Ambrosone A, Cometa MF, et al. Revolutionizing CAR T-cell therapies: innovations in genetic engineering and manufacturing to enhance efficacy and accessibility. Int J Mol Sci. 2024;25(19):10365. doi:10.3390/ijms251910365
111. Bukowski K, Kciuk M, Kontek R. Mechanisms of multidrug resistance in cancer chemotherapy. Int J Mol Sci. 2020;21(9):3233. doi:10.3390/ijms21093233
112. Majumder J, Minko T. Multifunctional and stimuli-responsive nanocarriers for targeted therapeutic delivery. Expert Opin Drug Deliv. 2021;18(2):205–227. doi:10.1080/17425247.2021.1828339
113. Liu X, Luo B, Wu X, Tang Z. Cuproptosis and cuproptosis-related genes: emerging potential therapeutic targets in breast cancer. Biochim Biophys Acta Rev Cancer. 2023;1878(6):189013.
114. Vlastou E, Kougioumtzopoulou A, Platoni K, Georgakopoulos I, Lagopati N, Kouloulias V, Zygogianni A. The emerging role of nanoparticles combined with either radiotherapy or hyperthermia in head and neck cancer: a current review. Cancers. 2025;17(5):899.
115. Salimi M, Mosca S, Gardner B, Palombo F, Matousek P, Stone N. Nanoparticle-mediated photothermal therapy limitation in clinical applications regarding pain management. Nanomaterials. 2022;12(6):922.
116. Luan X, Pan Y, Gao Y, Song Y. Recent near-infrared light-activated nanomedicine toward precision cancer therapy. J Mater Chem B. 2021;9(35):7076–7099.
117. Shang Y, Yi X, Xiang D, et al. Nanoagent-mediated photothermal therapy: from delivery system design to synergistic theranostic applications. Int J Nanomed. 2025;20:6891–6927. doi:10.2147/IJN.S522736
118. Liu D, Zhao T, Li Y, et al. Nanocarrier-based immunotherapy for viral diseases. Int J Pharm X. 2025;10:100408.
119. Tufail M, Jiang C-H, Li N. Immune evasion in cancer: mechanisms and cutting-edge therapeutic approaches. Signal Trans Targeted Ther. 2025;10(1):227. doi:10.1038/s41392-025-02280-1
120. Xiang G, Cui Y, Wang P, et al. Nanomedicine targeting the PD-1/PD-L1 axis in autoimmune diseases: breaking conventional barriers to restore immune tolerance. J Nanobiotechnol. 2025;23(1):664. doi:10.1186/s12951-025-03766-4
121. Yu L, Qiu Y, Liu B, et al. Engineered nano-bacteria hybrids for precision cancer immunotherapy. Mater Today Bio. 2025;35:102484. doi:10.1016/j.mtbio.2025.102484
122. Lorentzen CL, Haanen JB, Met Ö, et al. Clinical advances and ongoing trials on mRNA vaccines for cancer treatment. Lancet Oncol. 2022;23(10):e450–e458. doi:10.1016/S1470-2045(22)00372-2
123. Chen X, Xu Z, Li T, et al. Nanomaterial-encapsulated STING agonists for immune modulation in cancer therapy. Biomark Res. 2024;12(1):2. doi:10.1186/s40364-023-00551-z
124. Chien Y, Hsiao Y-J, Chou S-J, et al. Nanoparticles-mediated CRISPR-Cas9 gene therapy in inherited retinal diseases: applications, challenges, and emerging opportunities. J Nanobiotechnol. 2022;20(1):511. doi:10.1186/s12951-022-01717-x
125. Re F, Pelucchi S, Pettini F, et al. Emerging nanocarrier systems for the enhanced delivery of active pharmaceutical ingredients to the intestine. Nanomedicine. 2025;1–24.
126. Conte M, Cauda V. Multimodal therapies against pancreatic ductal adenocarcinoma: a review on synergistic approaches toward ultimate nanomedicine treatments. Adv Ther. 2022;5(11):2200079. doi:10.1002/adtp.202200079
127. Mousavi-Kiasary SMS, Senabreh A, Zandi A, et al. Synergistic cancer therapies enhanced by nanoparticles: advancing nanomedicine through multimodal strategies. Pharmaceutics. 2025;17(6):682. doi:10.3390/pharmaceutics17060682
128. Cardillo M, Katam K, Suravajhala P. Advancements in multi-omics research to address challenges in Alzheimer’s disease: a systems biology approach utilizing molecular biomarkers and innovative strategies. Front Aging Neurosci. 2025;17:1591796. doi:10.3389/fnagi.2025.1591796
129. Yang J, Na J, Shi T, et al. Advances in multi-omics research on biomarkers of intrahepatic cholangiocarcinoma. Curr Issues Mol Biol. 2025;47(11):905. doi:10.3390/cimb47110905
130. Liu J, Yang L, Liu D, Wu Q, Yu Y, Huang X, Li J, Liu S. The role of multi-omics in biomarker discovery, diagnosis, prognosis, and therapeutic monitoring of tissue repair and regeneration processes. J Orthop Translat. 2025;54:131–151.
131. John A, Qin B, Kalari KR, et al. Patient-specific multi-omics models and the application in personalized combination therapy. Future Oncol. 2020;16(23):1737–1750. doi:10.2217/fon-2020-0119
132. Shu M, Gao F, Yu C, et al. Dual-targeted therapy in HER2-positive breast cancer cells with the combination of carbon dots/HER3 siRNA and trastuzumab. Nanotechnology. 2020;31(33):335102. doi:10.1088/1361-6528/ab8a8a
133. Dadmehr M, Mortezaei M, Korouzhdehi B. Dual mode fluorometric and colorimetric detection of matrix metalloproteinase MMP-9 as a cancer biomarker based on AuNPs@gelatin/AuNCs nanocomposite. Biosens Bioelectron. 2023;220:114889. doi:10.1016/j.bios.2022.114889
134. Calatayud DG, Neophytou S, Nicodemou E, Giuffrida SG, Ge H, Pascu SI. Nano-theranostics for the sensing, imaging and therapy of prostate cancers. Front Chem. 2022;10:830133.
135. Farhadi A, Roxin Á, Wilson BC, Zheng G. Nano-enabled SERS reporting photosensitizers. Theranostics. 2015;5(5):469–476.
136. Sanadgol N, Abedi M, Hashemzaei M, et al. Exosomes as nanocarriers for brain-targeted delivery of therapeutic nucleic acids: advances and challenges. J Nanobiotechnol. 2025;23(1):453. doi:10.1186/s12951-025-03528-2
137. Zhang Z, He F, Li W, et al. Material-driven therapeutics: functional nanomaterial design paradigms revolutionizing osteosarcoma treatment. J Funct Biomat. 2025;16(6):213. doi:10.3390/jfb16060213
138. Gupta S, Chopra H, Singh Bajwa P, et al. Statistical formulation optimization of naproxen microsponges with eudragit RS100 for sustained drug release. J Pharm Innovation. 2025;20(4):117. doi:10.1007/s12247-025-09994-3
139. Sharma A, Verwilst P, Li M, et al. Theranostic fluorescent probes. Chem Rev. 2024;124(5):2699–2804. doi:10.1021/acs.chemrev.3c00778
140. Foroutan B, Abbasian Najafabadi AR. Capabilities of bioinformatics tools for optimizing physicochemical features of proteins used in Nano biosensors: a short overview of the tools related to bioinformatics. Biochem Biophys Rep. 2021;27:101094. doi:10.1016/j.bbrep.2021.101094
141. Panda PK, Verma SK, Suar M. Nanoparticle-biological interactions: the renaissance of bionomics in the myriad nanomedical technologies. Nanomedicine. 2021;16(25):2249–2254. doi:10.2217/nnm-2021-0174
142. Lee J, Choi MK, Song IS. Recent advances in doxorubicin formulation to enhance pharmacokinetics and tumor targeting. Pharmaceuticals. 2023;16(6):802. doi:10.3390/ph16060802
143. Ahire ED, Savaliya N, Makwana KV, et al. Protein-bound nano-injectable suspension: unveiling the promises and challenges. Applied Nano. 2025;6(2):9. doi:10.3390/applnano6020009
144. Milano G, Innocenti F, Minami H. Liposomal irinotecan (Onivyde): exemplifying the benefits of nanotherapeutic drugs. Cancer Sci. 2022;113(7):2224–2231. doi:10.1111/cas.15377
145. Aloss K, Hamar P. Recent preclinical and clinical progress in liposomal doxorubicin. Pharmaceutics. 2023;15(3):893. doi:10.3390/pharmaceutics15030893
146. Ghahremanloo A, Erfani B, Asgharzadeh F, et al. Reducing toxicity and enhancing efficacy of doxorubicin by liposomal doxorubicin and aprepitant in breast cancer. Sci Rep. 2025;15(1):9798. doi:10.1038/s41598-025-94291-9
147. Bonvalot S, Rutkowski PL, Thariat J, et al. Final safety and health-related quality of life results of the phase 2/3 Act.In.Sarc study with preoperative NBTXR3 plus radiation therapy versus radiation therapy in locally advanced soft-tissue sarcoma. Int J Radiation Oncol Biol Phys. 2022;114(3):422–432. doi:10.1016/j.ijrobp.2022.07.001
148. Zhao Y-C, Li X, Wang C-Q, et al. Unveiling the hidden risks: an update decade-long analysis of Abraxane-related adverse events from the FAERS database. Int J Nanomed. 2024;Volume 19:11847–11858. doi:10.2147/IJN.S490400
149. Liu Z, Fu Z, Liu Y, et al. Biomaterial-based drug delivery: evaluating the safety profiles of liposomal Vyxeos. Drug Delivery. 2025;32(1):2494781. doi:10.1080/10717544.2025.2494781
150. Tak WY, Lin S-M, Wang Y, et al. Phase III HEAT study adding lyso-thermosensitive liposomal doxorubicin to radiofrequency ablation in patients with unresectable hepatocellular carcinoma lesions. Clin Cancer Res. 2018;24(1):73–83. doi:10.1158/1078-0432.CCR-16-2433
151. Weiss GJ, Chao J, Neidhart JD, et al. First-in-human phase 1/2a trial of CRLX101, a cyclodextrin-containing polymer-camptothecin nanopharmaceutical in patients with advanced solid tumor malignancies. Invest New Drugs. 2013;31(4):986–1000. doi:10.1007/s10637-012-9921-8
152. Zuckerman JE, Gritli I, Tolcher A, et al. Correlating animal and human phase Ia/Ib clinical data with CALAA-01, a targeted, polymer-based nanoparticle containing siRNA. Proc Natl Acad Sci. 2014;111(31):11449–11454. doi:10.1073/pnas.1411393111
153. Wang H, Wu X, Wang J, et al. In vitro and in vivo correlation of injectable lipid-based nanomedicines: from dissolution to protein coronas. Mater Today Bio. 2025;35:102393. doi:10.1016/j.mtbio.2025.102393
154. Li F, Tang Z, Zheng Y, et al. Responsive nanomedicine strategies achieve pancreatic cancer precise theranostics. Bioact Mater. 2026;55:334–375. doi:10.1016/j.bioactmat.2025.08.012
155. Zagalo DM, Silva BMA, Silva C, et al. A quality by design (QbD) approach in pharmaceutical development of lipid-based nanosystems: a systematic review. J Drug Delivery Sci Technol. 2022;70:103207. doi:10.1016/j.jddst.2022.103207
156. Dass R, Rani P, Kumar D, et al. Quality by design approach for optimization, in-vitro and in-vivo evaluation of compression-spheronized itopride hydrochloride loaded gastroretentive pellets for the treatment of gastroesophageal reflux disease. Naunyn-Schmiedeberg’s Arch Pharmacol. 2025. doi:10.1007/s00210-025-04728-1
157. Herdiana Y. Bridging the gap: the role of advanced formulation strategies in the clinical translation of nanoparticle-based drug delivery systems. Int J Nanomed. 2025;Volume 20:13039–13053. doi:10.2147/IJN.S554821
158. Shan X, Gong X, Li J, et al. Current approaches of nanomedicines in the market and various stage of clinical translation. Acta Pharmaceutica Sinica B. 2022;12(7):3028–3048. doi:10.1016/j.apsb.2022.02.025
159. Gabizon AA, Patil Y, La-Beck NM. New insights and evolving role of pegylated liposomal doxorubicin in cancer therapy. Drug Resist Updat. 2016;29:90–106. doi:10.1016/j.drup.2016.10.003
160. Frampton JE. Liposomal irinotecan: a review in metastatic pancreatic adenocarcinoma. Drugs. 2020;80(10):1007–1018. doi:10.1007/s40265-020-01336-6
161. Kumar A, Shahvej SK, Yadav P, et al. Clinical applications of targeted nanomaterials. Pharmaceutics. 2025;17(3):379. doi:10.3390/pharmaceutics17030379
162. Germain M, He J, Xie S, et al. Delivering the power of nanomedicine to patients today. J Control Release. 2020;322:326. doi:10.1016/j.jconrel.2020.03.037
163. Pizevska M, Kaeda J, Fritsche E, Elazaly H, Reinke P, Amini L. Advanced therapy medicinal products’ translation in Europe: a developers’. Perspective Front Med. 2022;9:757647.
164. Zhang P, Marill J, Darmon A, et al. NBTXR3 radiotherapy-activated functionalized hafnium oxide nanoparticles show efficient antitumor effects across a large panel of human cancer models. Int J Nanomed. 2021;16:2761–2773. doi:10.2147/IJN.S301182
165. Rodríguez-Gómez F, Monferrer D, Penon O, Rivera-Gil P. Regulatory pathways and guidelines for nanotechnology-enabled health products: a comparative review of EU and US frameworks. Front Med. 2025;12:1544393.
166. Ramos D, Almeida L. Overview of standards related to the occupational risk and safety of nanotechnologies. Standards. 2022;2(1):83–89. doi:10.3390/standards2010007
167. Calé A, Elblová P, Andělová H, et al. Analyzing molecular determinants of nanodrugs. Cytotoxic Effects Int J Mol Sci. 2025;26(14):6687. doi:10.3390/ijms26146687
168. Loushambam B, Yanglem S, Krishnaswami V, et al. Nanomedicine: pioneering advances in neural disease, stroke and spinal cord injury treatment. Neuroglia. 2025;6(1):9. doi:10.3390/neuroglia6010009
169. Kim J, Cho H, Lim D-K, et al. Perspectives for improving the tumor targeting of nanomedicine via the EPR effect in clinical tumors. Int J Mol Sci. 2023;24(12):10082. doi:10.3390/ijms241210082
170. Qutub M, Tatode A, Iqbal Z, et al. Stimuli-responsive nanovesicles for spatiotemporal control of drug delivery in chronic cutaneous wounds: bridging molecular pathobiology to translational nanomedicine. J Drug Delivery Sci Technol. 2025;112:107238. doi:10.1016/j.jddst.2025.107238
171. Bi Y, Xie S, Li Z, et al. Precise nanoscale fabrication technologies, the “last mile” of medicinal development. Acta Pharmaceutica Sinica B. 2025;15(5):2372–2401. doi:10.1016/j.apsb.2025.03.040
172. Rodríguez-Gómez FD, Monferrer D, Penon O, et al. Regulatory pathways and guidelines for nanotechnology-enabled health products: a comparative review of EU and US frameworks. Front Med Lausanne. 2025;12:1544393. doi:10.3389/fmed.2025.1544393
173. Đorđević S, Gonzalez MM, Conejos-Sánchez I, et al. Current hurdles to the translation of nanomedicines from bench to the clinic. Drug Deliv Transl Res. 2022;12(3):500–525. doi:10.1007/s13346-021-01024-2
174. Salangwa C, Munthali R, Mfune L, et al. Public-private partnership (PPP) and health service delivery in Malawi: the case of Christian health association of Malawi (CHAM) facilities in Mzimba district. Health Policy OPEN. 2025;8:100139. doi:10.1016/j.hpopen.2025.100139
175. Kumar R, Kumar A, Bhardwaj S, et al. Nanotoxicity unveiled: evaluating exposure risks and assessing the impact of nanoparticles on human health. J Trace Elements Minerals. 2025;13:100252. doi:10.1016/j.jtemin.2025.100252
176. Weiner EB, Dankwa-Mullan I, Nelson WA, et al. Ethical challenges and evolving strategies in the integration of artificial intelligence into clinical practice. PLOS Digit Health. 2025;4(4):e0000810. doi:10.1371/journal.pdig.0000810
177. Wang B, Hu S, Teng Y, et al. Current advance of nanotechnology in diagnosis and treatment for malignant tumors. Signal Trans Targeted Ther. 2024;9(1):200. doi:10.1038/s41392-024-01889-y
178. Zelepukin IV, Shevchenko KG, Deyev SM. Rediscovery of mononuclear phagocyte system blockade for nanoparticle drug delivery. Nat Commun. 2024;15(1):4366. doi:10.1038/s41467-024-48838-5
179. Rodríguez-Gómez FD, Penon O, Monferrer D, et al. Classification system for nanotechnology-enabled health products with both scientific and regulatory application. Front Med Lausanne. 2023;10:1212949. doi:10.3389/fmed.2023.1212949
180. Chou WC, Canchola A, Zhang F, et al. Machine learning and artificial intelligence in nanomedicine. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2025;17(4):e70027. doi:10.1002/wnan.70027
181. Liu Y, Zhang Y, Li H, Hu TY. Recent advances in the bench-to-bedside translation of cancer nanomedicines. Acta Pharmaceutica Sinica B. 2025;15(1):97–122. doi:10.1016/j.apsb.2024.12.007
182. Ștefănigă SA, Cordoș AA, Ivascu T, et al. Advancing precision oncology with digital and virtual twins: a scoping review. Cancers. 2024;16(22):3817. doi:10.3390/cancers16223817
183. Shen S, Qi W, Liu X, et al. From virtual to reality: innovative practices of digital twins in tumor therapy. J Transl Med. 2025;23(1):348. doi:10.1186/s12967-025-06371-z
184. Giansanti D, Morelli S. Exploring the potential of digital twins in cancer treatment: a narrative review of reviews. J Clin Med. 2025;14(10):3574. doi:10.3390/jcm14103574
185. Venturini J, Chakraborty A, Baysal MA, Tsimberidou AM. Developments in nanotechnology approaches for the treatment of solid tumors. Exp Hematol Oncol. 2025;14(1):76.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Update on Novel Ocular Nanosystems with Possible Benefits in the Treatment of Corneal Neovascularization

Zhang C, Yin Y, Zhao J, Li Y, Wang Y, Zhang Z, Niu L, Zheng Y
International Journal of Nanomedicine 2022, 17:4911-4931
Published Date: 19 October 2022
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023
Drug Delivery System Targeting Cancer-Associated Fibroblast for Improving Immunotherapy
Zhang Z, Wang R, Chen L
International Journal of Nanomedicine 2025, 20:483-503
Published Date: 11 January 2025
Targeting Multiple Pathophysiological Axes in COPD: Nanomaterial Advances
Zhang Q, Xu S, Yang C, Wang X, Liu T, Zhang X, Qu C, Wu J, Yang J, Xing X
International Journal of Nanomedicine 2025, 20:11989-12007
Published Date: 1 October 2025
Nanomaterials for Theranostic Management of Oral Cancer: Advances in Imaging, Biosensing, Targeted Delivery, and Multimodal Synergistic Therapy
Zhu X, Chen J, Zhao J, Zhang Z, Wang C
International Journal of Nanomedicine 2025, 20:13689-13719
Published Date: 13 November 2025