Back to Journals » Journal of Pain Research » Volume 14
Naldemedine Improves Patient-Reported Outcomes of Opioid-Induced Constipation in Patients with Chronic Non-Cancer Pain in the COMPOSE Phase 3 Studies
Authors Camilleri M ![]() , Hale M, Morlion B
, Hale M, Morlion B ![]() , Tack J, Webster L
, Tack J, Webster L ![]() , Wild J
, Wild J
Received 13 October 2020
Accepted for publication 16 June 2021
Published 16 July 2021 Volume 2021:14 Pages 2179—2189
DOI https://doi.org/10.2147/JPR.S282738
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Schatman
Michael Camilleri,1 Martin Hale,2 Bart Morlion,3 Jan Tack,4 Lynn Webster,5 James Wild6
1Clinical Enteric Neuroscience Translational and Epidemiological Research (CENTER), Mayo Clinic, Rochester, MN, USA; 2Gold Coast Research, LLC, Plantation, FL, USA; 3Leuven Center for Algology and Pain Management, University Hospital Leuven, University of Leuven, Leuven, Belgium; 4Translational Research Center for Gastrointestinal Disorders (TARGID), University of Leuven, Leuven, Belgium; 5PRA Health Sciences, Salt Lake City, UT, USA; 6Upstate Clinical Research Associates, Williamsville, NY, USA
Correspondence: Michael Camilleri
Clinical Enteric Neuroscience Translational and Epidemiological Research (CENTER), Mayo Clinic, 200 First St. S.W., Charlton Building, Rm. 8-110, Rochester, MN, 55905, USA
Tel +1 507-266-2305
Fax +1 507-538-5820
Email [email protected]
Objective: Opioid-induced constipation is among the most common side effects associated with opioid use in patients with chronic non-cancer pain, and it can have a significant negative impact on health-related quality of life (QOL). This analysis evaluated the effect of naldemedine 0.2 mg on patient-reported outcomes in three phase 3 clinical studies.
Methods: COMPOSE-1 and COMPOSE-2 were identical randomized, double-blind, placebo-controlled, parallel-group studies of 12 weeks’ duration, allowing data to be integrated (n=1095). COMPOSE-3 was similar in design, but of 52 weeks’ duration (n=1241). Patients were adults with chronic non-cancer pain who had been treated with opioid analgesics for ≥ 3 months and experiencing opioid-induced constipation. Patient-reported outcomes included Patient Assessment of Constipation Symptoms (PAC-SYM; 12 questions assessed on a 5-point Likert scale), PAC-QOL (28 questions assessed on a 5-point Likert scale), and Subject Global Satisfaction (measured on a 7-point Likert scale). The proportion of patients achieving a ≥ 1.5 improvement in PAC-SYM and PAC-QOL was calculated. The correlation between change in PAC-SYM and PAC-QOL scores and frequency of bowel movements was also explored.
Results: The proportion of PAC-SYM and PAC-QOL responders was significantly higher for naldemedine than for placebo at all assessed time points in COMPOSE-1/COMPOSE-2 (p< 0.005 for both) and COMPOSE-3 (p< 0.005 and p< 0.0001, respectively). There was a statistically significant correlation between improvement in PAC-SYM/PAC-QOL and frequency of bowel movements at all time points (p≤ 0.0002). The majority of patients treated with naldemedine reported markedly or moderately improved satisfaction with constipation and abdominal symptoms on the Subject Global Satisfaction questionnaire.
Discussion: Naldemedine treatment was associated with a rapid and sustained clinically relevant improvement in patient-reported outcomes, indicating improvement in opioid-induced constipation-related symptoms and QOL.
ClinicalTrials.gov Registration: NCT01965158, NCT01993940, NCT01965652.
Keywords: gastrointestinal tract, minimal clinically important difference, mu opioid receptor, patient satisfaction, quality of life
Plain Language Summary
Opioid analgesic therapy is one treatment option for chronic moderate-to-severe cancer and non-cancer pain in selected patients. However, treatment with opioids can result in opioid-induced constipation, which is characterized by symptoms such as straining to pass a bowel movement, small or hard bowel movements, bloating, gas or flatulence, and abdominal pain. These symptoms can have a significant negative impact on an individual’s quality of life. Naldemedine is approved in the United States, Japan, and the European Union for the treatment of opioid-induced constipation. This analysis determined whether improvements in bowel movement frequency after treatment with naldemedine also improved health-related symptoms and quality of life in non-cancer pain in 2336 patients with opioid-induced constipation based on an analysis of the COMPOSE-1, COMPOSE-2, and COMPOSE-3 studies. The results showed that naldemedine treatment increased the frequency of bowel movements in patients with chronic non-cancer pain and, based on patient questionnaires, improved health-related symptoms and quality of life. In addition, the results showed that the majority of patients treated with naldemedine reported improved satisfaction with constipation and abdominal symptoms.
Introduction
Opioid treatment can be effective for management of chronic non-cancer pain in select patients.1 However, the use of opioids is associated with a number of significant adverse events,2 of which the most frequent is constipation.3 Opioid-induced constipation (OIC), characterized by symptoms such as straining to pass a bowel movement (BM), small or hard BMs, bloating, gas or flatulence, and abdominal pain,4 can have a significant negative impact on health-related quality of life (QOL).5 These symptoms can cause patients to skip or reduce prescribed opioid doses, leading to inadequate pain relief and further decrements to QOL.4–6
Patient-reported outcome (PRO) instruments are critical for assessing the impact of disease and associated treatments on QOL; these instruments appraise the effects of treatment as clinically meaningful to patients in accordance with regulatory requirements. In the case of patients with OIC, PRO instruments extend measurement of the effects of treatment beyond improvements in the number of BMs over defined time periods. The Patient Assessment of Constipation Symptoms (PAC-SYM) and Patient Assessment of Constipation Quality of Life (PAC-QOL) are validated PRO instruments that measure health-related symptoms and QOL related to constipation.7,8 The PAC-SYM has been validated specifically in the context of OIC.9 These PRO instruments have been used in a range of studies, including clinical assessment of the peripherally acting µ-opioid receptor antagonist naldemedine and the 5-HT4 receptor agonist prucalopride in patients with OIC.10,11 Importantly, a number of studies have established the clinical utility of these PROs in constipation, including OIC, by determining the minimal clinically important difference (MCID).7,12,13
This analysis evaluates the effect of naldemedine on PAC-SYM and PAC-QOL scores in three phase 3 clinical studies in which naldemedine provided a significant improvement in the frequency of BMs over 12 weeks (in the COMPOSE-1 and COMPOSE-2 studies)14 and over 52 weeks (in COMPOSE-3).11 In COMPOSE-1 and COMPOSE-2, the proportion of patients who were responders (defined as at least 3 spontaneous BMs [SBMs] per week and an increase from baseline of at least 1 SBM per week for ≥9 weeks of the 12-week treatment period and 3 of the last 4 weeks) was 47.6% and 52.5% with naldemedine, respectively, compared with 34.6% and 33.6%, respectively, with placebo.14 The longer-duration COMPOSE-3 study demonstrated that this improvement in OIC was sustained for 52 weeks with no apparent loss of efficacy.11
The objective of the current study was to determine whether the improvements in BM frequency after treatment with naldemedine were clinically meaningful to patients when assessed by PAC-SYM and PAC-QOL, as well as by patient satisfaction with improvement in the symptoms of OIC.
Materials and Methods
Study Design
The designs of COMPOSE-1, COMPOSE-2, and COMPOSE-3 have been described in detail previously.11,14 All three studies were conducted in accordance with the Declaration of Helsinki and all applicable local Good Clinical Practice guidelines and regulations. All patients provided written informed consent. The Institutional Review Boards utilized in COMPOSE-1, -2, and -3 are shown in Supplementary Table 1.
COMPOSE-1 and COMPOSE-2 were randomized, double-blind, placebo-controlled, parallel-group, phase 3 studies of 12 weeks’ duration. For the purposes of this analysis, data from these 2 identically designed studies were integrated. Adults aged 18–80 years with chronic non-cancer pain who were treated with opioid analgesics for ≥3 months, were experiencing OIC, and were either not using laxatives or had agreed to discontinue laxative use at the time of enrollment were randomized 1:1 to naldemedine 0.2 mg or placebo once daily for 12 weeks. Exclusion criteria included the presence of significant structural gastrointestinal abnormalities that might have affected bowel transit, as well as other conditions or circumstances not related to opioid use that might have caused constipation. Patients who had no bowel movement for a period of 72 hours during screening and/or the treatment period could receive rescue laxatives; use of routine laxative regimens was not permitted in COMPOSE-1 and COMPOSE-2. The primary efficacy endpoint for these 2 studies was the proportion of responders, who were defined as having had at least 3 SBMs per week and an increase from baseline of at least 1 SBM per week for that week (a positive response week) for at least 9 out of 12 weeks in the study period and at least 3 of the final 4 weeks.
COMPOSE-3 was a randomized, double-blind, placebo-controlled, parallel-group, phase 3 clinical study that evaluated the long-term safety and efficacy of naldemedine 0.2 mg for 52 weeks. As with COMPOSE-1 and COMPOSE-2, patients had access to rescue laxatives, but could be on a background laxative regimen at baseline. The primary endpoints for this study were measures of treatment-emergent adverse events and assessments of opioid withdrawal. Efficacy endpoints were secondary and included the frequency of BMs at weeks 12, 24, 36, and 52.
Assessments
PAC-SYM, PAC-QOL, and Subject Global Satisfaction (SGS) with constipation and abdominal symptoms questionnaires were exploratory endpoints for COMPOSE-1 and COMPOSE-2 and secondary endpoints for COMPOSE-3. PAC-SYM is composed of 12 questions across 3 domains, including abdominal, rectal, and stool symptoms,7 and PAC-QOL includes 28 questions across 4 domains, including physical discomfort, psychosocial discomfort, constipation-related worries and concerns, and satisfaction.8 Questions for both PAC-SYM and PAC-QOL were rated on a 5-point Likert scale (0=absence of symptoms, 1=mild, 2=moderate, 3=severe, and 4=very severe), with lower scores reflecting better QOL; total scores on each questionnaire were averaged to give a final score out of 5. In COMPOSE-1 and COMPOSE-2, PAC-QOL and PAC-SYM were assessed on day 1 (predose), week 2, week 4, and week 12 or at early termination, and in COMPOSE-3, PAC-QOL and PAC-SYM were assessed on day 1 (predose), week 2, week 12, week 24, week 36, and week 52 or at early termination.
The SGS score was based on a 7-point scale, ranging from a score of 1 (markedly worsened) to 7 (markedly improved). In the SGS evaluation, patients rated their degree of satisfaction with constipation and abdominal symptoms relative to the beginning of the study. This evaluation was administered at the end of the study (week 12 for COMPOSE-1 and COMPOSE-2 and week 52 for COMPOSE-3) or at early termination.
In all 3 studies, participants completed the PAC-SYM, PAC-QOL, and SGS questionnaires.
Statistical Analysis
All efficacy analyses used the intent-to-treat analysis population, which included all randomized patients. The mean of the changes in the overall score for PAC-SYM and PAC-QOL from baseline was compared at each visit between naldemedine and placebo. A recent analysis identified that an improvement in PAC-SYM and PAC-QOL >1 was the MCID in OIC.12 For the purposes of this post hoc analysis, a PAC-SYM/PAC-QOL responder was defined more conservatively as having an improvement ≥1.5 (based on 5-point Likert scales). The correlation between the change from baseline in the frequency of BMs and PAC-SYM/PAC-QOL scores was also calculated. For SGS, the frequency distribution across the 7-point scale was calculated in the different treatment groups. The difference in SGS scores between naldemedine and placebo was analyzed using the Wilcoxon rank sum test. All analyses were performed using SAS version 9.2 (SAS Institute Inc, Cary, NC, USA).
Results
Patient demographics and baseline characteristics for the integrated populations from COMPOSE-1 and COMPOSE-2 (COMPOSE-1/COMPOSE-2; n=1095) and for COMPOSE-3 (n=1241), are shown in Table 1. The populations enrolled across the 3 studies were similar. Patients randomized to naldemedine or placebo were predominantly female (59.4% to 64.8%) and white (79.2% to 81.9%), with mean age ranging from 52.7 to 53.7 years in the different treatment arms. Other baseline demographics and characteristics including the distribution of opioid doses were also similar across the 3 studies and between naldemedine and placebo arms, with mean morphine-equivalent doses ranging from 121 mg/day to 132 mg/day. Supplementary Table 2 presents the factors used to convert opioid analgesic doses to morphine equivalents. The baseline frequency of SBMs per week was slightly higher in COMPOSE-3 at 1.6 per week, compared with 1.2 per week in COMPOSE-1/COMPOSE-2.
 |
Table 1 Demographic and Baseline Characteristics |
In COMPOSE-1/COMPOSE-2, bisacodyl was the most frequently used rescue laxative, accounting for 92.4% of all rescue laxative use during screening and 92.9% during the treatment period. Rescue laxative use in the naldemedine arms was decreased by 26.3% relative to placebo. In COMPOSE-3, the proportion of patients requiring rescue laxatives was reduced with naldemedine compared with placebo from 14.0% to 8.0% in patients on a routine laxative regimen and from 13.1% to 7.0% in patients not on a routine laxative regimen.
The proportions of patients who met the responder definition of ≥1.5 improvement in overall PAC-SYM scores for COMPOSE-1/COMPOSE-2 and COMPOSE-3 are shown in Figure 1. The proportion of PAC-SYM responders for patients treated with naldemedine was significantly higher than the proportion of responders treated with placebo at all assessed time points in COMPOSE-1/COMPOSE-2 (p<0.005; Figure 1A) and COMPOSE-3 (p<0.005; Figure 1B). Of note, the change from baseline in overall PAC-SYM was significantly correlated with the frequency of BM in COMPOSE-1/COMPOSE-2 and in COMPOSE-3 for patients treated with naldemedine at all time points assessed (p<0.0001; Table 2). The correlations between overall PAC-SYM and frequency of BMs were also statistically significant at all time points in patients who received placebo (p≤0.0002).
 |
Table 2 Correlation (R) Between the Change in Frequency of Bowel Movements and PAC-SYM and PAC-QOL. Negative Values Reflect an Inverse Relationship Between Frequency of Bowel Movements and PAC-SYM/PAC-QOL Scores |
 |
Figure 1 Proportion of patients achieving ≥1.5-point decrease in PAC-SYM scores from (A) integrated COMPOSE-1 and COMPOSE-2 data; (B) COMPOSE-3 data. ap<0.0001 for naldemedine vs placebo; bp<0.005 for naldemedine vs placebo. Abbreviation: PAC-SYM, Patient Assessment of Constipation Symptoms. Note: Data show mean and 95% confidence intervals. |
Similar results were observed for PAC-QOL. The proportions of patients meeting the responder definition of ≥1.5 improvement in overall PAC-QOL scores for COMPOSE-1/COMPOSE-2 and COMPOSE-3 are shown in Figure 2. The proportion of PAC-QOL responders for patients treated with naldemedine was significantly higher than for placebo at all assessed time points in COMPOSE-1/COMPOSE-2 (p<0.005; Figure 2A) and COMPOSE-3 (p<0.0001; Figure 2B). The change from baseline in overall PAC-QOL was significantly correlated with the frequency of BMs in COMPOSE-1/COMPOSE-2 and in COMPOSE-3 for patients treated with both naldemedine and placebo at all time points assessed (p<0.0001; Table 2). The negative correlation values for change in frequency of BMs and change from baseline in overall PAC-SYM and PAC-QOL reflect an inverse relationship of these variables. Specifically, the frequency of BMs increases as the PAC-SYM and PAC-QOL scores decrease (ie, show improvement in domains).
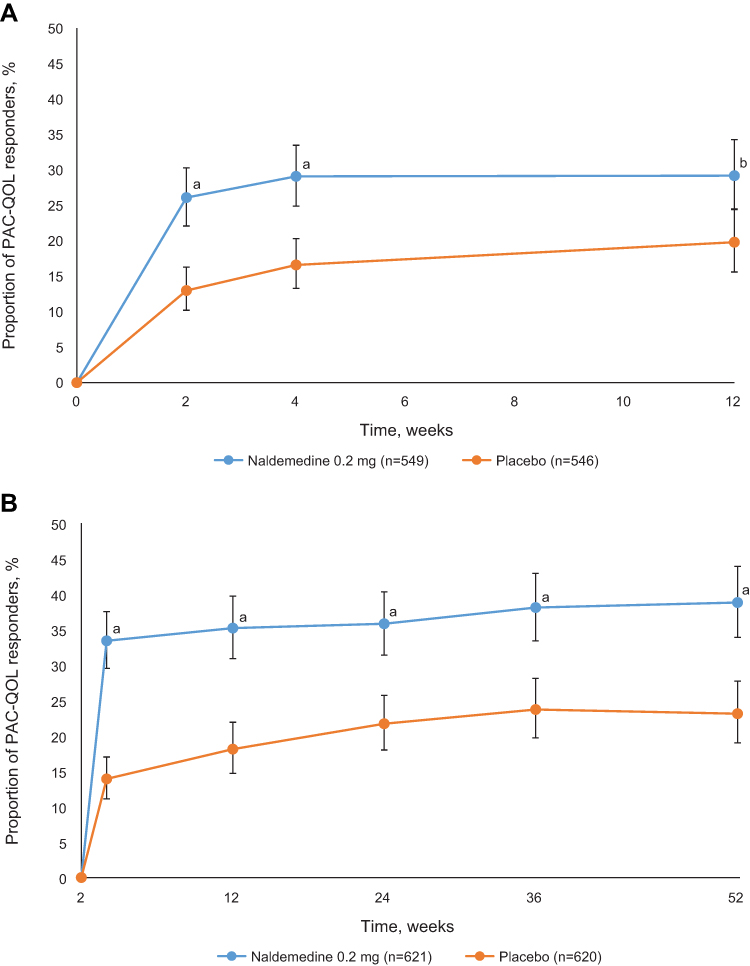 |
Figure 2 Proportion of patients achieving ≥1.5-point decrease in PAC-QOL scores from (A) integrated COMPOSE-1 and COMPOSE-2 data; (B) COMPOSE-3 data. ap<0.0001 for naldemedine vs placebo; bp<0.005 for naldemedine vs placebo. Abbreviation: PAC-QOL, Patient Assessment of Constipation Quality of Life. Note: Data show mean and 95% confidence intervals. |
The mean (SD) SGS scores at the end of the 12-week COMPOSE-1/COMPOSE-2 studies were 1.5 (1.5) and 0.9 (1.5) in the naldemedine and placebo arms, respectively (p<0.0001). Following the 52-week COMPOSE-3 study, the mean (SD) SGS score was higher in the naldemedine arm than in the placebo arm (1.7 [1.4] vs 1.0 [1.4]; p<0.0001). Overall, a greater proportion of patients had an improved SGS score with naldemedine than with placebo. Specifically, in COMPOSE-1/COMPOSE-2, 216 patients (55.5%) in the naldemedine group had moderately or markedly improved SGS, compared with only 140 (36.9%) in the placebo group (Figure 3A). In the naldemedine group of COMPOSE-3, 303 patients (61.0%) reported moderately or markedly improved SGS, compared with 184 patients (36.5%) who received placebo (Figure 3B).
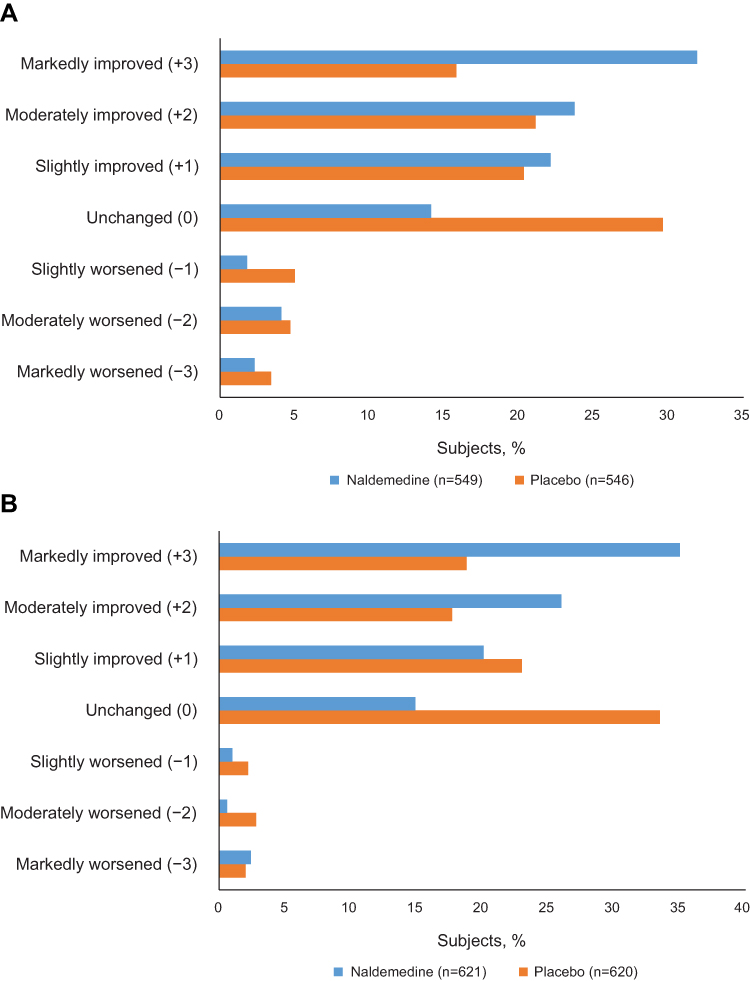 |
Figure 3 Frequency distribution of Subject Global Satisfaction scores for (A) integrated COMPOSE-1 and COMPOSE-2 data and (B) COMPOSE-3 data. |
Conversely, fewer patients had worse SGS scores. In COMPOSE-1/COMPOSE-2, a total of 25 patients (6.4%) in the naldemedine group and 31 (8.2%) in the placebo group had moderately or markedly worsened SGS (Figure 3A). In COMPOSE 3, 15 patients (3.0%) had moderately or markedly worsened SGS in the naldemedine group, compared with 24 patients (4.8%) who received placebo (Figure 3B).
The most commonly reported treatment-emergent adverse events across the three studies were diarrhea, abdominal pain, and nausea. Treatment-emergent adverse events occurring in ≥5% of patients in any treatment group are summarized in Supplementary Table 3. The number needed to harm for the two most common adverse events for COMPOSE -1/COMPOSE-2 and COMPOSE-3 was 18.9 and 17.5, respectively, for diarrhea and 23.8 and 20, respectively, for abdominal pain.
Discussion
Naldemedine has been shown to increase the frequency of BMs and SBMs in patients with OIC and chronic non-cancer pain in three phase 3 randomized, controlled studies.11,14 The current data demonstrate that, in addition to improvements in the frequency of bowel movements, there were concomitant significant improvements in patients’ perception of meaningful change in bowel function and health-related QOL with naldemedine over the course of these studies. Consistent, statistically and clinically significant improvements compared with placebo were observed in overall PAC-SYM and PAC-QOL scores at all time points assessed. These improvements were realized rapidly, within 2 weeks of treatment initiation, and persisted with little change at up to 1 year of naldemedine treatment. This rapid improvement aligns with the improvement reported in BM frequency that has also been shown to significantly increase within 2 weeks; indeed, most patients have been shown to have a BM within 24 hours after the first dose.15
A recent receiver operator characteristic (ROC) analysis based on integrated data from COMPOSE-1 and COMPOSE-2 determined that the MCID for PAC-SYM and PAC-QOL was a change of approximately 1 unit on each scale.12 This result is in line with an analysis of data from a study with prucalopride that also found a 1-point improvement in PAC-QOL to be meaningful to patients with chronic constipation not related to opioid use.16 The conclusion was based on the fact that most patients who had a 1-point improvement in PAC-QOL also had an increased frequency of BMs; although statistically less rigorous than the ROC analysis, the results of the prucalopride study provide additional support for the clinical relevance of this 1-point change on the PAC-QOL scale. A study published in 1999 found the MCID for PAC-SYM to be 0.5 points and that a change of approximately 1 point corresponded to moderate clinical improvement.7 A more recent study suggested a decrease of 0.6 to be the MCID and that a cutoff of 0.75 should be used in placebo-controlled studies in chronic constipation.13 For the purposes of this analysis, a more conservative threshold of ≥1.5 unit improvement for both PAC-SYM and PAC-QOL was used to define a responder. Using this definition, significantly more patients who received naldemedine than received placebo were responders at all time points assessed. The proportion of patients with MCID >1.5 on naldemedine compared with placebo is consistent with the primary analyses of these studies in which the frequency of BMs/SBMs was previously shown to be significantly improved with naldemedine versus placebo.11,14 Furthermore, improvements in PAC-SYM and PAC-QOL were significantly correlated with the increase in frequency of BMs per week, indicating that the effects of naldemedine on OIC have a direct impact on OIC-associated symptoms and QOL. A significant correlation between BM frequency and change in PAC-SYM/PAC-QOL scores was also observed in the placebo arms of the studies described here. This correlation reflects the substantial placebo effect seen in studies of these agents for treatment of OIC14,17 and demonstrates the sensitivity of these health-related QOL measures to improvements in BM frequency.
The correlation between BMs and PAC-SYM and PAC-QOL scores observed in these analyses was comparable to the correlation identified in a previous post hoc analysis of pooled data from two phase 3 studies of naloxegol.18 Although these correlations were only moderate, they were statistically significant, in part due to the large numbers of patients in the included studies. The naloxegol studies found that an increase in frequency of 1 SBM per week was sufficient to cause improvements in PAC-SYM and PAC-QOL scores.18 The selective µ-opioid receptor antagonist methylnaltrexone has also demonstrated improvements in PAC-QOL in patients with chronic non-malignant pain and OIC.19
The 7-item SGS questionnaire measured patient satisfaction with constipation and abdominal symptoms. SGS scores indicated that most patients (55.5% and 61.0%; COMPOSE-1/COMPOSE-2 and COMPOSE-3, respectively) randomized to naldemedine had at least moderate or marked improvement in satisfaction with constipation and abdominal symptoms. By contrast, only 37% of patients randomized to placebo in COMPOSE-1/COMPOSE-2 and COMPOSE-3 had moderate or marked improvement. In addition, approximately twice as many patients who received placebo than received naldemedine had no change or worsened SGS scores. Although SGS is not a validated instrument, these results do provide independent support for the observed improvements in PAC-SYM and PAC-QOL.
The primary efficacy endpoint for COMPOSE-1 and -2 was based on SBMs and the secondary efficacy endpoints for COMPOSE-3 were based on BMs. For the sake of consistency, the analysis conducted here utilized number of BMs rather than number of SBMs. This is a potential limitation of the analysis, as overall BM was not a formal endpoint in COMPOSE-1 and -2. On the other hand, these data were prospectively collected and therefore lend themselves to this appraisal of data from the 3 trials in combination. Total BMs may be more meaningful to patients than SBMs and hence more relevant to measures of health-related QOL. Indeed, it has been shown that 83% of patients would prefer to have at least 1 BM per day, regardless of whether it is spontaneous or induced.4,20 A further limitation of this study is the fact that the correlation of PAC-SYM and PAC-QOL scores with improvement in the frequency of BMs per week was a post hoc analysis.
Naldemedine was generally well tolerated in these studies. As described previously, the most commonly reported treatment-related adverse events were related to gastrointestinal function, consistent with the mechanism of action of naldemedine (ie, the peripheral antagonism of effects of μ-opioid medications), and included abdominal pain, diarrhea, nausea, vomiting, and flatulence.11,14 However, the incidence of specific adverse events was low. The number needed to harm for diarrhea and abdominal pain in the COMPOSE studies was consistent with values obtained in a meta-analysis of randomized placebo-controlled trials in opioid-induced constipation.21 There were also no apparent symptoms of opioid withdrawal, change in pain intensity, or change in opioid dose, indicating that naldemedine had no effect on opioid activity outside the gastrointestinal tract, confirming its peripheral site of action.
Conclusions
In these three phase 3 studies, naldemedine was associated with a rapid and sustained improvement in PRO assessments, indicating improvement in OIC-related symptoms and QOL. The current data are consistent with a recent ROC analysis with anchors relating to bowel movement and constipation as well as patient satisfaction showing that changes in PAC-SYM and PAC-QOL are clinically relevant.12 Improvements in these PROs correlated with improvements in the frequency of BMs as early as 2 weeks after initiation of treatment that were sustained for up to 52 weeks. In addition, naldemedine was associated with improvements in patient satisfaction with constipation and abdominal symptoms, providing further confirmation of the clinical relevance of PAC-SYM and PAC-QOL. These observed improvements in health-related QOL may have positive implications for patients, such as encouraging increased adherence to opioid medications for pain management. Thus, this study shows that naldemedine 0.2 mg once daily provides not only an increased frequency of BMs in patients with chronic non-cancer pain but also clinically meaningful improvements in health-related QOL.
Abbreviations
BM, bowel movement; BMI, body mass index; MCID, minimal clinically important difference; OIC, opioid-induced constipation; PAC-QOL, Patient Assessment of Constipation Quality of Life; PAC-SYM, Patient Assessment of Constipation Symptoms; PRO, patient-reported outcome; QOL, quality of life; ROC, receiver operator characteristic; SBM, spontaneous bowel movement; SGS, Subject Global Satisfaction.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Acknowledgments
Editorial and writing support was provided by James Street, PhD, of Peloton Advantage, LLC, an OPEN Health company, and funded by Shionogi Inc.
Funding
These studies were sponsored by Shionogi Inc., Florham Park, NJ. BDSI owns full rights to commercialize Symproic® (naldemedine) tablets 0.2 mg in the US for opioid-induced constipation. The study sponsor was involved in the design, collection, and analysis of the data. The authors provided the interpretation of the results and made the decision to submit the manuscript for publication.
Disclosure
Michael Camilleri has provided scientific advice to Shionogi and has received a research grant from AstraZeneca in the field of opioid-induced constipation. Martin Hale was a clinical trial investigator, consultant to Shionogi Inc. and received a stipend for review of the clinical study report. Bart Morlion was a clinical trial site investigator for Shionogi Inc.; a consultant for Astellas Pharma Europe Ltd, Boehringer Ingelheim International, Boston Scientific, Bayer, Lilly, Reckitt Benckiser, Grünenthal, Mundipharma International, TEVA Pharmaceuticals Europe, GSK Consumer Healthcare, and Kyowa Kirin; and a speaker for Mundipharma International, Pfizer Inc, Shionogi Inc., Kyowa Kirin, and Procter and Gamble Company. Jan Tack has provided scientific advice to Allergan, Kyowa Kirin, Shionogi, and Shire, has been a speaker for Allergan and Kyowa Kirin, and has received a research grant from Kyowa Kirin related to opioid-induced constipation. Lynn Webster has provided scientific advice to Arbor Pharmaceuticals and BDSI; has worked on advisory boards for BDSI, Ensysce Biosciences, Neurana, and Salix; has received travel expenses from BDSI, Ensysce Biosciences, Elysium, Neurana, and Salix; has received personal fees for consultation from Bonti, Charleston Labs, Daiichi Sankyo, Depomed, Egalet, Elysium, Indivior, Insys Therapeutics, Inspirion Therapeutics, Kempharm, Mallinckrodt Pharmaceuticals, Merck, Pain Therapeutics, Pernix, Pfizer, Shionogi, Teva, Trevena, Trevi, and Vallon, outside the submitted work. James Wild received a stipend from Shionogi Inc. for review of the clinical study report. The authors report no other conflicts of interest in this work.
References
1. Noori SA, Aiyer R, Yu J, White RS, Mehta N, Gulati A. Nonopioid versus opioid agents for chronic neuropathic pain, rheumatoid arthritis pain, cancer pain and low back pain. Pain Manag. 2019;9(2):205–216. doi:10.2217/pmt-2018-0052
2. Els C, Jackson TD, Kunyk D, et al. Adverse events associated with medium- and long-term use of opioids for chronic non-cancer pain: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2017;10:CD012509.
3. Kalso E, Edwards JE, Moore RA, McQuay HJ. Opioids in chronic non-cancer pain: systematic review of efficacy and safety. Pain. 2004;112(3):372–380. doi:10.1016/j.pain.2004.09.019
4. Coyne KS, Margolis MK, Yeomans K, et al. Opioid-induced constipation among patients with chronic noncancer pain in the United States, Canada, Germany, and the United Kingdom: laxative use, response, and symptom burden over time. Pain Med. 2015;16(8):1551–1565. doi:10.1111/pme.12724
5. Bell TJ, Panchal SJ, Miaskowski C, Bolge SC, Milanova T, Williamson R. The prevalence, severity, and impact of opioid-induced bowel dysfunction: results of a US and European patient survey (PROBE 1). Pain Med. 2009;10(1):35–42. doi:10.1111/j.1526-4637.2008.00495.x
6. Gupta S, Patel H, Scopel J, Mody RR. Impact of constipation on opioid therapy management among long-term opioid users, based on a patient survey. J Opioid Manag. 2015;11(4):325–338. doi:10.5055/jom.2015.0282
7. Frank L, Kleinman L, Farup C, Taylor L, Miner P
8. Marquis P, De La LC, Dubois D, McDermott A, Chassany O. Development and validation of the patient assessment of constipation quality of life questionnaire. Scand J Gastroenterol. 2005;40(5):540–551. doi:10.1080/00365520510012208
9. Slappendel R, Simpson K, Dubois D, Keininger DL. Validation of the PAC-SYM questionnaire for opioid-induced constipation in patients with chronic low back pain. Eur J Pain. 2006;10(3):209–217. doi:10.1016/j.ejpain.2005.03.008
10. Sloots CE, Rykx A, Cools M, Kerstens R, De Pauw M. Efficacy and safety of prucalopride in patients with chronic noncancer pain suffering from opioid-induced constipation. Dig Dis Sci. 2010;55(10):2912–2921. doi:10.1007/s10620-010-1229-y
11. Webster LR, Nalamachu S, Morlion B, et al. Long-term use of naldemedine in the treatment of opioid-induced constipation in patients with chronic non-cancer pain: a randomized, double-blind, placebo-controlled phase 3 study. Pain. 2018;159(5):987–994. doi:10.1097/j.pain.0000000000001174
12. Tack J, Camilleri M, Hale M, et al. Establishing minimal clinically important differences in quality of life measures in opioid-induced constipation. Clin Gastroenterol Hepatol. 2021:S1542-3565(21)00507-3.
13. Yiannakou Y, Tack J, Piessevaux H, et al. The PAC-SYM questionnaire for chronic constipation: defining the minimal important difference. Aliment Pharmacol Ther. 2017;46(11–12):1103–1111. doi:10.1111/apt.14349
14. Hale M, Wild J, Reddy J, Yamada T, Arjona Ferreira JC. Naldemedine versus placebo for opioid-induced constipation (COMPOSE-1 and COMPOSE-2): two multicentre, phase 3, double-blind, randomised, parallel-group trials. Lancet Gastroenterol Hepatol. 2017;2(8):555–564. doi:10.1016/S2468-1253(17)30105-X
15. Wild J, Yamada T, Arjona Ferreira JC, Hale M. Onset of action of naldemedine in the treatment of opioid-induced constipation in patients with chronic noncancer pain: results from 2 randomized, placebo-controlled, phase 3 trials. Pain. 2019;160(10):2358–2364. doi:10.1097/j.pain.0000000000001629
16. Dubois D, Gilet H, Viala-Danten M, Tack J. Psychometric performance and clinical meaningfulness of the patient assessment of constipation-quality of life questionnaire in prucalopride (RESOLOR) trials for chronic constipation. Neurogastroenterol Motil. 2010;22(2):e54–63. doi:10.1111/j.1365-2982.2009.01408.x
17. Chey WD, Webster L, Sostek M, Lappalainen J, Barker PN, Tack J. Naloxegol for opioid-induced constipation in patients with noncancer pain. N Engl J Med. 2014;370(25):2387–2396. doi:10.1056/NEJMoa1310246
18. Coyne KS, Poon JL, Thompson C, Hu Y, Datto CJ, Sostek M. Translating clinical findings into the patient’s perspective: post-hoc pooled analysis of bowel movement changes as a predictor of improvement in patients’ opioid-induced constipation symptoms and outcomes. Clin Ther. 2017;39(1):75–88. doi:10.1016/j.clinthera.2016.11.012
19. Michna E, Blonsky ER, Schulman S, et al. Subcutaneous methylnaltrexone for treatment of opioid-induced constipation in patients with chronic, nonmalignant pain: a randomized controlled study. J Pain. 2011;12(5):554–562. doi:10.1016/j.jpain.2010.11.008
20. LoCasale RJ, Datto CJ, Margolis MK, Tack J, Coyne KS. The impact of opioid-induced constipation among chronic pain patients with sufficient laxative use. Int J Clin Pract. 2015;69(12):1448–1556. doi:10.1111/ijcp.12718
21. Nee J, Zakari M, Sugarman MA, et al. Efficacy of treatments for opioid-induced constipation: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2018;16(10):1569–1584. doi:10.1016/j.cgh.2018.01.021
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.