Back to Journals » Journal of Pain Research » Volume 19
Myoelectric and Progressive Motor Training for Phantom Limb Pain in People with Amputations During War: A Feasibility Report
Authors Ksenchyna K, Huk Y, Kristoffersen MB, Buist M ![]() , McGowan E
, McGowan E ![]() , Limakatso K, Kovalenko S, Dmytriiev D
, Limakatso K, Kovalenko S, Dmytriiev D ![]() , Ortiz-Catalan M
, Ortiz-Catalan M ![]()
Received 15 November 2025
Accepted for publication 21 February 2026
Published 3 March 2026 Volume 2026:19 578370
DOI https://doi.org/10.2147/JPR.S578370
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Kateryna Ksenchyna,1,2 Yuliia Huk,3 Morten B Kristoffersen,4 Mirka Buist,5 Eithne McGowan,6 Katleho Limakatso,7 Serhii Kovalenko,8 Dmytro Dmytriiev,1,2,9 Max Ortiz-Catalan2,10
1National Pirogov Memorial Medical University, Vinnytsia, Ukraine; 2Prometi Pain Rehabilitation Center, Vinnytsia, Ukraine; 3Department of the Physical and Rehabilitation Medicine, Regional Pirogov Memorial Clinical Hospital, Vinnytsia, Ukraine; 4Department of Engineering Technology, Technical University of Denmark, Copenhagen, Denmark; 5Center for Bionics and Pain Research, Gothenburg, Sweden; 6Center for Advanced Reconstruction of Extremities, Sahlgrenska University Hospital, Gothenburg, Sweden; 7Pain Management Unit, Department of Anaesthesia and Perioperative Medicine, Neuroscience Institute, University of Cape Town, Cape Town, South Africa; 8Vinnytsia Clinical Emergency Hospital, Vinnytsia, Ukraine; 9Superhumans Center, Lviv, Ukraine; 10Center for Complex Endoprosthetics, Osseointegration, and Bionics, Kyiv, Ukraine
Correspondence: Max Ortiz-Catalan, Email [email protected]
Purpose: Phantom limb pain (PLP) is a common condition after limb amputation which is notoriously difficult to treat. The Russian full-scale invasion of Ukraine has resulted in over 100,000 people with amputated limbs and persistent PLP. This study reports on the feasibility of implementing two novel treatment approaches, Phantom Motor Execution (PME) and Progressive Motor Training (PMT), during the Russian war on Ukraine.
Methods: PME and PMT follow the principle of facilitating motor training of the phantom limb and are grounded on the Stochastic Entanglement hypothesis for the pathogenesis of PLP. PME employs myoelectric pattern recognition on residual limb muscles to control virtual and augmented reality environments (mixed reality). PMT uses mixed reality to guide patients to imagine or execute predefined movements according to their evolving motor skills, and it is suitable for patients where myoelectric signals are not viable. Nineteen participants with major limb amputation were treated with PME (N=8) and PMT (N=11).
Results: Participants who completed 9 sessions reported a reduction of PLP greater than 50%. Participants received half of the training time per session and less sessions than reported in previous studies, yet clinically meaningful pain reductions were observed.
Conclusion: This study demonstrates the feasibility of implementing PME and PMI for the treatment of PLP during war time and constraint resources. Ukrainian clinicians found the technologies and treatment approaches efficient and effective at reducing PLP and have introduced them as part of their clinical practice.
Keywords: phantom limb pain, progressive motor training, phantom motor execution, amputations, neuropathic pain, motor imagery, motor execution, virtual reality
Introduction
Approximately over 100,000 people have suffered major limb loss due to the Russian full-scale invasion of Ukraine since February 2022. The prevalence of PLP elsewhere has been estimated at 64%.1 Although official statistics are unavailable due to ongoing conflict, anecdotal reports suggest that the incidence of PLP in Ukraine exceeds that commonly reported in the literature. Several factors may account for the higher incidence of PLP among war victims, including prolonged duration between injury, evacuation, and the final amputation procedure;2 the psychological adverse factors of an ongoing war;3 and unprioritized nerve treatment during amputation due to time and resource constraints. From the beginning of the Russo-Ukrainian War in 2014, and prior to the full-scale invasion, PLP had already been identified as a major difficulty in the rehabilitation of war-injured veterans.4
Treatments for PLP, ranging from surgical to plasticity-guided interventions, have been employed clinically worldwide.5 Notably, pharmacological approaches serving as a pain management strategy, rather than treatment, are often considered unsuitable as long-term solutions but indispensable in acute pain.6 After failing to find effective and efficient treatments for PLP for our clinics in Ukraine, we sought to implement novel approaches that could remain feasible during wartime. We implemented Phantom Motor Execution (PME) as employed previously with positive results.7 PME relies on the possibility to record myoelectric signals from muscles in the residual limb, which are used to infer motor intent in the missing (phantom) limb. The resulting phantom motor volition can then be visualized using virtual and augmented reality (VR/AR) environments, which allows for the implementation of serious gaming.8 A consequence of the Stochastic Entanglement hypothesis for the pathogenesis of PLP is that re-engaging the neural resources of the affected limb would drive plastic neural changes throughout the neural axis disassociating pathologic pain processing, and this is hypothesized as the working mechanism of PME.9
A key challenge with utilizing myoelectric pattern recognition for treatment is the reliance on residual limb muscles, which are often compromised.10 In addition, war injuries are often complex and require extended healing periods extending for several months, during which conventional rehabilitation cannot be provided, despite the development of PLP. In consideration of this, we implemented Progressive Motor Training (PMT) to provide timely treatment for patients in whom residual limb electromyography is not feasible.11 PMT guides the patient to imagine and then execute movements shown in VR/AR environments. Previous work has shown that VR/AR guided motor imagery can achieve similar alleviation of PLP as PME using myoelectric pattern recognition.12,13 As derived by the Stochastic Entanglement hypothesis, this could be explained by the larger cortical neural resources employed when imagining complex movements, which can be comparable in proportion to that required for the execution of simpler movements in which circuits in sub-cortical areas and the spinal cord are involved.9,11 Ideally, most neural resources related to the affected limb should be recruited in the execution of complex movements. However, the execution of complex movements is difficult when attempted with phantom limbs that are often perceived as paralyzed.14 PMT takes advantage of motor imagery to facilitate execution, thus allowing training with simple and complex movements from the first intervention.11
Here, we report on the first implementation PME and PMT under constraint resources and during war. PMT was provided in cases where PME was not feasible due to the unavailability of myoelectric signals.
Methods
Participants
This study was approved by the ethical committee at the National Pirogov Memorial Medical University (7/072025). Participants were treated at the Regional Pirogov Memorial Clinical Hospital and Prometei Pain Rehabilitation Center, both in Vinnytsia, Ukraine, and provided written informed consent prior treatment. Participants were older than 18 years, could read and communicate in Ukrainian, suffer from PLP, and underwent limb amputation more than three months prior treatment. We did not consider individuals with addictive disorders; severe psychiatric disorders; significant cognitive impairment due to memory problems and brain disorders.
Phantom Motor Execution
The PME protocol consisted of 30-minute treatment sessions conducted every other day for up to 9 sessions. The technology to conduct PME and training protocol has been described extensively in prior studies.7,8,13 Briefly, a training session involved placement of electrodes, recording of myoelectric signals associated with the execution of a set of predefined movements, and then training in VR and AR environments performing the recorded movements now reflected in the movement of a virtual limb (Figure 1), or to control games. The set of movements was made progressively more difficult over time according to the ability of the participant and at the discretion of the therapist.
 |
Figure 1 Example of a treatment session with Phantom Motor Execution (PME). |
Progressive Motor Training
The PMT protocol consisted of 30-minute treatment sessions conducted every other day for up to 9 sessions. The guiding movements were provided in VR or AR environments as preferred by the participants (Figure 2). Participants were asked to execute a movement with their phantom limb three times. If they were unable due to feeling their phantom limb locked or frozen in place, they were instructed to imagine performing the movement three times, with progression to motor execution when possible.
 |
Figure 2 Example of a treatment session with Progressive Motor Training (PMT). |
Outcomes
Participants completed a pain questionnaire consisting of numeric rating scales (NRS) at baseline and after every third training session, for phantom and residual limb pain intensity, as well as PLP interference with activities of daily living (ADL) and sleep.
Data Analysis
Data were analyzed using “R” version 4.5.1. The primary outcome is PLP severity, with a minimal clinically important within-group difference in pain reduction (50%) from baseline used to classify the treatment as successful.15,16 Given the small sample size in this study, all outcomes are presented using descriptive statistics.17
Results
Nineteen males with a median age of 37 (IQR: 30–42) were treated. All participants had undergone amputations due to trauma: 13 transfemoral, four transhumeral, one transradial, and one transtibial. All participants had previously received Mirror Therapy and medications for acute pain. At baseline, two participants were receiving Pregabalin (225 mg and 300 mg daily, respectively), while one additional participant was receiving Diclofenac (100 mg daily) as part of their ongoing analgesic management. Two participants presented with symptomatic neuromas, identified clinically during the initial assessment. In PME, four participants (50%) completed nine sessions and the other half six sessions. In PMT, six participants completed nine sessions (55%), then three and two participants completed six and three sessions, respectively. The participants were unable to complete all sessions due to transfer to other hospitals.
PLP Severity
The PME group had a median baseline PLP score of 70 (IQR: 35–85), which was significantly lower after the last treatment session [30 (IQR: 25–35)] (Figure 3). Within-group difference between baseline and end of treatment scores was 40 [95% CI (8.45–71.55)]. Further improvements were seen at 1-month follow-up [25 (IQR: 20–35)].
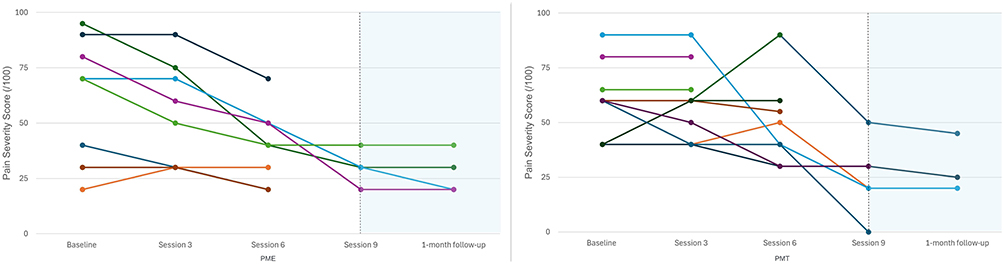 |
Figure 3 The effect of PME and PMT on PLP severity. |
The PMT group had a median baseline PLP score of 60 (IQR: 40–65), which was significantly lower after the last treatment session [25 (IQR: 20–30)] (Figure 3). Within-group difference between baseline and end of treatment scores was 35 [95% CI (21.53–48.47)]. Further improvements were seen at 1-month follow-up [22.5 (IQR: 20–35)].
PLP Interference with ADL
The PME group had a median baseline pain interference score of 70 (IQR: 50–70), which was significantly lower after the last treatment session [25 (IQR: 10–40)] (Figure 4). Within-group difference between baseline and end of treatment scores was 45 [95% CI (22.63–67.37)].
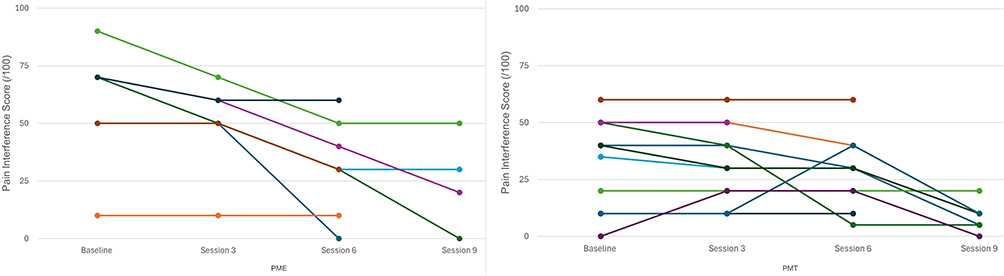 |
Figure 4 The effect of PME and PMT on pain interference with ADL. |
The PMT group had a median baseline pain interference score of 40 (IQR: 20–50), which was significantly lower after the last treatment session [10 (IQR: 5–15)] (Figure 4). Within-group difference between baseline and end of treatment scores was 30 [95% CI (14.25–45.75)].
PLP Interference with Sleep
The PME group had a median baseline pain interference score of 25 (IQR: 10–25), which was lower after the last treatment session [10 (IQR: 0–25)] (Figure 5). Within-group difference between baseline and end of treatment scores was 15 [95% CI (−3.04–33.04)].
 |
Figure 5 The effect of PME and PMT on pain interference with sleep. |
The PMT group had a median baseline pain interference score of 65 (IQR: 10–80), which was lower after the last treatment session [40 (IQR: 10–50)] (Figure 5). Within-group difference between baseline and end of treatment scores was 25 [95% CI (−15.12–65.12)].
Medication, Neuroma Pain, and Residual Limb Pain
The two participants on Pregabalin reduced the intake from 225 mg to 150 mg (33%) and from 300 mg to 100 mg (67%) by the end of the treatment. Notably, the two participants who presented with symptomatic neuromas did not report any reduction in PLP during the intervention period. The distribution of residual limb pain (RLP) throughout the study is shown in Figure 6.
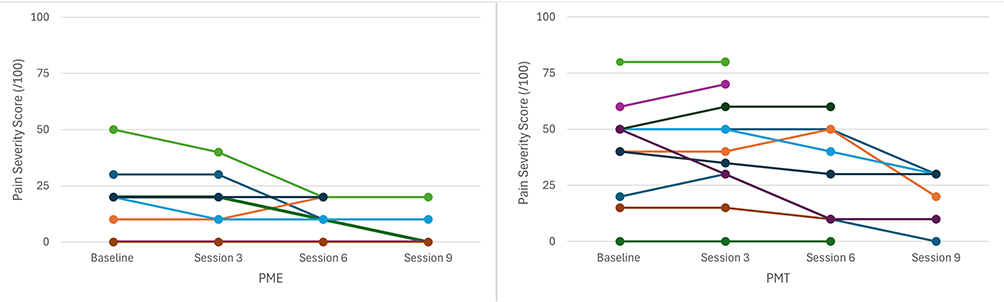 |
Figure 6 Distribution of RLP during PME and PMT interventions. |
Discussion
The current study was conducted during the war on a population that appears to show a higher incidence of PLP than previously reported. Due to current restrictions, it is not possible to conduct epidemiological studies on war casualties; however, the experience of clinicians treating these participants indicates that most, if not all, report enduring PLP. The participants in this study had been treated with Mirror Therapy and medications with unsatisfactory results. This study aimed to evaluate the feasibility of using modern treatments based on digital technologies, and with defined working mechanisms,9,11 in our current, demanding clinical practice. The number of war injuries has overwhelmed the Ukrainian healthcare system, with limited resources to attend to all patients who need treatment. The use of digital technologies represents a potential solution to satisfy the growing demand for PLP treatment. Moreover, these approaches can also be used to restore function in severe motor impairments such as after stroke18 or arm replantation.19 Here, we extend their application to a cohort of participants with war-related amputations, demonstrating its feasibility in highly resource-constrained and unstable clinical environments.
Despite constrained resources, in this study, we found similar results as previously reported in other studies (>50% reduction of PLP),7,8,13 with an important difference in that here, participants received 30 minutes of treatment per session, as opposed to 90 to 120 minutes as previously employed. The maximum number of sessions here was nine, whereas in previous work it was more than 12.7,8,13 The optimal length of treatment sessions has yet to be properly studied, as well as the adequate number of treatment sessions. A rule of thumb now adopted in our clinical practice is to provide 30 to 60 minutes of treatment, and as many sessions as necessary, as long as the patient reports progress, considering a minimum of nine sessions to determine if further benefits can be achieved.
We observed a general lack of knowledge regarding PLP among participants and clinicians. Participants seemed not to be sufficiently aware of the possibility of experiencing PLP, which diminished their psychological readiness for rehabilitation. On the other hand, clinicians felt unprepared to explain and address PLP once reported by their patients. We have now learned the importance of educating both patients and clinicians on PLP and treatment options, ranging from surgical to plasticity-guided interventions. We believe educating clinicians now helps them better diagnose the sources contributing to PLP, such as the presence of painful neuromas.20 Patients with complex amputations, comorbidities, and painful neuromas are unlikely to respond favorably to plasticity-guided treatments such as those employed here, if used in isolation.
A major challenge we identified was the participants’ state of mind. The trauma caused by war goes beyond the physical, and addressing it comprehensively is particularly challenging in resource-constrained environments.21 We could not provide psychological support during the PLP interventions, although this would have likely potentiated the therapeutic effects of the treatment. Comprehensive pain treatment remains a major challenge.
Conventional means of treating PLP, such as medication and Mirror Therapy have been ineffective at reducing the prevalence of PLP, which has remained over 60% for decades.22 The lack of standardized guidelines might be a contributor to sub-optimal pain outcomes.23 In this study, we found digital technologies useful to provide more standardized treatments, and we now emphasize the importance of pain science education,24 which we provide to patients as soon as possible. Randomized controlled trials are unfeasible during war time but must be conducted elsewhere to validate the efficacy of the clinical protocols employed here.
The limitations of this study are derived from the resource-constrained environment in which it took place. Although the participants received other treatment such as Mirror Therapy prior to the PME or PMI interventions, no additional control group was included in the study. A detailed characterization of PLP including quality, frequency, and duration was not investigated due to time constraints. Similarly, no in-depth or systematic psychological evaluations were conducted. Further studies are required to provide additional insights into the experience of PLP in this particular patient population.
Conclusion
In this study, we demonstrated the feasibility of conducting PLP treatment during wartime using digital technologies to facilitate motor training. Our results were clinically significant and comparable to those previously reported, despite being in a resource-constrained environment, which limited us to less than half of the treatment exposure used in prior studies. Given the cost-effectiveness of these treatments, we have incorporated them into our clinical practice. Additionally, we found educating both patients and clinicians to be a critical factor moving forward.
Abbreviations
PLP, phantom limb pain; PME, phantom motor execution; PMT, progressive motor training; RLP, residual limb pain.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This work complied with the Declaration of Helsinki and was approved by the ethical committee at the National Pirogov Memorial Medical University (7/072025), and participants provided informed consent.
Consent for Publication
The people in Figure 1 provided written informed consent for the image to be published.
Disclosure
MBK, MB, and MOC are shareholders of NeuroRehab Technologies OÜ. MB and MOC are inventors of a patent related to PMT. MB has a patent EP4291139A4 pending to NEUROREHAB TECHNOLOGIES OÜ, a patent US20240082533A1 pending to NEUROREHAB TECHNOLOGIES OÜ, a patent JP2024507172A pending to NEUROREHAB TECHNOLOGIES OÜ, a patent AU2022218905A1 pending to NEUROREHAB TECHNOLOGIES OÜ, a patent CN116829105A pending to NEUROREHAB TECHNOLOGIES OÜ, a patent KR20230146024A pending to NEUROREHAB TECHNOLOGIES OÜ, a patent PCT/EP2025/084676 pending to NEUROREHAB TECHNOLOGIES OÜ. MOC reports grants from Promobilia Foundation, during the conduct of the study; In addition, MOC has a patent 22753069.8 pending to NeuroRehab Technologies, a patent PCT/EP2025/084676 pending to NeuroRehab Technologies. The authors report no other conflicts of interest in this work.
References
1. Limakatso K, Bedwell GJ, Madden VJ, et al. The prevalence and risk factors for phantom limb pain in people with amputations: a systematic review and meta-analysis. PLoS One. 2020;15(10):e0240431. doi:10.1371/journal.pone.0240431
2. Edwards D, Guthrie HC, Yousaf S, et al. Trauma-related amputations in war and at a civilian major trauma centre—Comparison of care, outcome and the challenges ahead. Injury. 2016;47(8):1806–8. doi:10.1016/j.injury.2016.05.029
3. Fuchs X, Flor H, Bekrater-Bodmann R. Psychological factors associated with phantom limb pain: a review of recent findings. Pain Res Manag. 2018;2018:5080123. doi:10.1155/2018/5080123
4. Bespalenko А, Shchehlіuk OI, Kikh AY, et al. Algorithm for rehabilitation of combat-related patients with limb amputations based on multiprofessional and individual approach. Ukrainian J Military Med. 2020;1(1):64–72. doi:10.46847/ujmm.2020.1(1)-064
5. Limakatso K, Parker R. Treatment recommendations for phantom limb pain in people with amputations: an expert consensus delphi study. Pm r. 2021;13(11):1216–1226. doi:10.1002/pmrj.12556
6. Alviar MJ, Hale T, Dungca M. Pharmacologic interventions for treating phantom limb pain. Cochrane Database Syst Rev. 2016;10(10):Cd006380. doi:10.1002/14651858.CD006380.pub3
7. Ortiz-Catalan M, Guðmundsdóttir RA, Kristoffersen MB, et al. Phantom motor execution facilitated by machine learning and augmented reality as treatment for phantom limb pain: a single group, clinical trial in patients with chronic intractable phantom limb pain. Lancet. 2016;388(10062):2885–2894. doi:10.1016/S0140-6736(16)31598-7
8. Ortiz-Catalan M, et al. Treatment of phantom limb pain (PLP) based on augmented reality and gaming controlled by myoelectric pattern recognition: a case study of a chronic PLP patient. Front Neurosci. 2014;8:24.
9. Ortiz-Catalan M. The stochastic entanglement and phantom motor execution hypotheses: a theoretical framework for the origin and treatment of phantom limb pain. Front Neurol. 2018;9:9. Available from: https://www.frontiersin.org/journals/neurology/articles/10.3389/fneur.2018.00748/full.
10. Yadav D, Veer K. Recent trends and challenges of surface electromyography in prosthetic applications. Biomed. Eng. Lett. 2023;13(3):353–373. doi:10.1007/s13534-023-00281-z
11. Ortiz-Catalan M. Theoretical foundations of Progressive Motor Training (PMT) for Phantom Limb Pain. J Neuroeng Rehabil. 2026;23(1):5. doi:10.1186/s12984-025-01790-x
12. Munoz-Novoa M, van Veldhoven JE, Postema SG, et al. Regaining the intention to live after relief of intractable phantom limb pain: a case study. Scand J Pain. 2025;25(1). doi:10.1515/sjpain-2025-0006.
13. Lendaro E, Van der Sluis CK, Hermansson L, et al. Extended reality used in the treatment of phantom limb pain: a multicenter, double-blind, randomized controlled trial. Pain. 2025;166(3):571–586. doi:10.1097/j.pain.0000000000003384
14. Touillet A, Peultier-Celli L, Nicol C, et al. Characteristics of phantom upper limb mobility encourage phantom-mobility-based prosthesis control. Sci Rep. 2018;8(1):15459. doi:10.1038/s41598-018-33643-0
15. Farrar JT, Young JP, LaMoreaux L, et al. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/S0304-3959(01)00349-9
16. Laigaard J, Pedersen C, Rønsbo TN, et al. Minimal clinically important differences in randomised clinical trials on pain management after total Hip and knee arthroplasty: a systematic review. Br J Anaesth. 2021;126(5):1029–1037. doi:10.1016/j.bja.2021.01.021
17. Vaidyanathan AK. Basics in statistics: sample size calculation and descriptive data statistics. J Indian Prosthodont Soc. 2023;23(3):207–209. doi:10.4103/jips.jips_307_23
18. Munoz-Novoa M, Kristoffersen MB, Sunnerhagen KS, et al. Myoelectric pattern recognition with virtual reality and serious gaming improves upper limb function in chronic stroke: a single case experimental design study. J Neuroeng Rehabil. 2025;22(1):6. doi:10.1186/s12984-025-01541-y
19. Kristoffersen MB, Munoz-Novoa M, Buist M, et al. Myoelectric motor execution and sensory training to treat chronic pain and paralysis in a replanted arm: a case study. J Neuroeng Rehabil. 2024;21(1):204. doi:10.1186/s12984-024-01508-5
20. Lu C, Sun X, Wang C, et al. Mechanisms and treatment of painful neuromas. Rev Neurosci. 2018;29(5):557–566. doi:10.1515/revneuro-2017-0077
21. Koval V, Burlakova I, Sheviakov O, et al. Features of psychological education in ukraine during the war and post-war recovery. Pedagogy and Educ Manag Rev. 2024;4:76–86.
22. Sherman RA, Sherman CJ, Parker L. Chronic phantom and stump pain among American veterans: results of a survey. Pain. 1984;18(1):83–95. doi:10.1016/0304-3959(84)90128-3
23. Limakatso K, McGowan E, Ortiz-Catalan M. Evaluating mirror therapy protocols in phantom limb pain clinical trials: a scoping review. J Pain Res. 2025;18:619–629. doi:10.2147/JPR.S502541
24. Moseley GL, Leake HB, Beetsma AJ, et al. Teaching patients about pain: the emergence of pain science education, its learning frameworks and delivery strategies. J Pain. 2024;25(5):104425. doi:10.1016/j.jpain.2023.11.008
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.