Back to Journals » OncoTargets and Therapy » Volume 12
Mutations In Thirty Hotspot Genes In Newly Diagnosed Chinese Multiple Myeloma Patients
Received 19 May 2019
Accepted for publication 24 October 2019
Published 21 November 2019 Volume 2019:12 Pages 9999—10010
DOI https://doi.org/10.2147/OTT.S216289
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Takuya Aoki
Ying Hu,1 Wenming Chen,2 Jingbo Wang1
1Department of Hematology, Aerospace Center Hospital, Beijing 100049, People’s Republic of China; 2Department of Hematology, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Wenming Chen
Department of Hematology, Beijing Chao-Yang Hospital, Capital Medical University, No. 8 GongTi South Road, Beijing, People’s Republic of China
Tel +86 139 1010 7759
Email [email protected]
Objective: In recent years, whole-genome sequencing and whole-exon sequencing have revealed the spectrum of gene mutations in multiple myeloma (MM). Gene mutations may play an important role in the pathogenesis, progression, and prognosis of this disease. On the basis of these studies, we established a box of mutations in 30 hotspot genes and analyzed the characteristics in newly diagnosed MM patients in China.
Methods: Bone marrow samples were collected. Mononuclear cells were isolated and plasma cells were separated using CD138 magnetic beads. Gene mutations were detected by PCR and Sanger sequencing. Fluorescence in situ hybridization (FISH) was used to analyze 1q21, 17p13.1, 14q32/16q23, 14q32/4p16, and 14q32/11q13.3. In the first part of this study, characterization of 30 genes and FISH analysis were performed in 40 patients. For economic reasons, in the second part of this study, 12 of 30 genes were characterized in another 46 patients.
Results: In the 40 patients of the first part of this study, single nucleotide polymorphisms (SNPs) were detected in 7 genes (CRBN, ATM, FAT4, FAM46C, RB1, NR3C1, and SPEN), while 16 genes were mutated (ATM, CUL4B, IRF4, CCND1, KRAS, DIS3, CRBN, TP53, FAT4, NR3C1, VCAN, RB1, SP140, NRAS, EGR1, and BRAF). Overall, 83 mutations of 30 genes were identified, including 54 intronic mutations, 18 missense mutations, 6 synonymous mutations, 3 5′/3′-UTR mutations, and 2 deletions mutations. Cytogenetic abnormalities were also screened in the 40 patients assayed, with 50% of the patients having 1q21+, 12.5% having 17p−, 15% having t(4;14), and 17.5% having t(11;14). DIS3 was mutated in 4/40, three of which involved t(4;14) or t(11;14). TP53 was mutated in two non-17p− patients, one of whom survived only 7 months, while the other survived 13 months. Three genes (ATM, CUL4B, and IRF4) with a high mutation rate were analyzed for an association with survival. There was no statistically significant difference in 2-year PFS (progress free survival) and 2-year OS (overall survival) between patients with or without ATM or CUL4B mutation (P>0.05). This finding was also obtained for IFR4 mutation, but patients with IFR4 mutation did show trends for longer PFS and OS.
Conclusion: SNPs and other types of gene mutations are common in newly diagnosed Chinese multiple myeloma patients. The genes most commonly featuring SNPs are CRBN, ATM, FAT4, and FAM46C, while the genes most commonly featuring other mutation types are ATM, CUL4B, and IRF4. There were differences in the profiles of genes affected by SNPs and by other mutation types. Intronic mutations were the most common mutation type. Gene mutations may differ among patients with different cytogenetic abnormalities. Genetic mutations may be associated with prognosis.
Keywords: multiple myeloma, gene mutation, single nucleotide polymorphism
Introduction
Multiple myeloma (MM) is an incurable malignancy of plasma cells. Its pathogenesis is only partially understood. Almost all patients harbor chromosomal aberrations; however, these alone are unlikely to be sufficient for malignant transformation. Risk assessment based on individual cytogenetics has already been established in MM. However, the prognostic indices used in such assessment do not evaluate patients’ genomic profiles accurately and comprehensively to guide precision therapy.1 Recently, large sequencing studies have defined the mutation landscape of multiple myeloma.2,3 Therefore, we generated a mutation box for 30 hotspot genes based on previous research to explore the characteristics and clinical significance of gene mutations in newly diagnosed Chinese MM patients.
Materials And Methods
The Institutional Review Board of Beijing Chao-Yang Hospital, Capital Medical University, approved this study, which was conducted in accordance with the Declaration of Helsinki. On the basis of large sequencing studies, we established a box of mutations in 30 hotspot genes. We identified 40 patients (Box 1) (Table 1) and 46 patients (Box 2) (61 males, 25 females) newly diagnosed with MM. The median age was 61 years (42–79 years). The diagnostic criteria were those defined by the International Myeloma Working Group (IMWG). Bone marrow samples were collected from all of the patients. Mononuclear cells were isolated and plasma cells were separated by CD138 magnetic beads. DNA was extracted. Gene mutations were detected using PCR and Sanger sequencing (ABI 3500DX) by Kindstar Global Company in Beijing. Cytogenetic abnormalities, including 1q21, 17p13.1, 14q32/16q23, 14q32/4p16, and 14q32/11q13.3 were detected by FISH. SPSS 19 statistical software was used for survival analysis. When P<0.05, the difference was considered statistically significant.
 |
Box 1 (30 genes) |
 |
Box 2 (12 genes) |
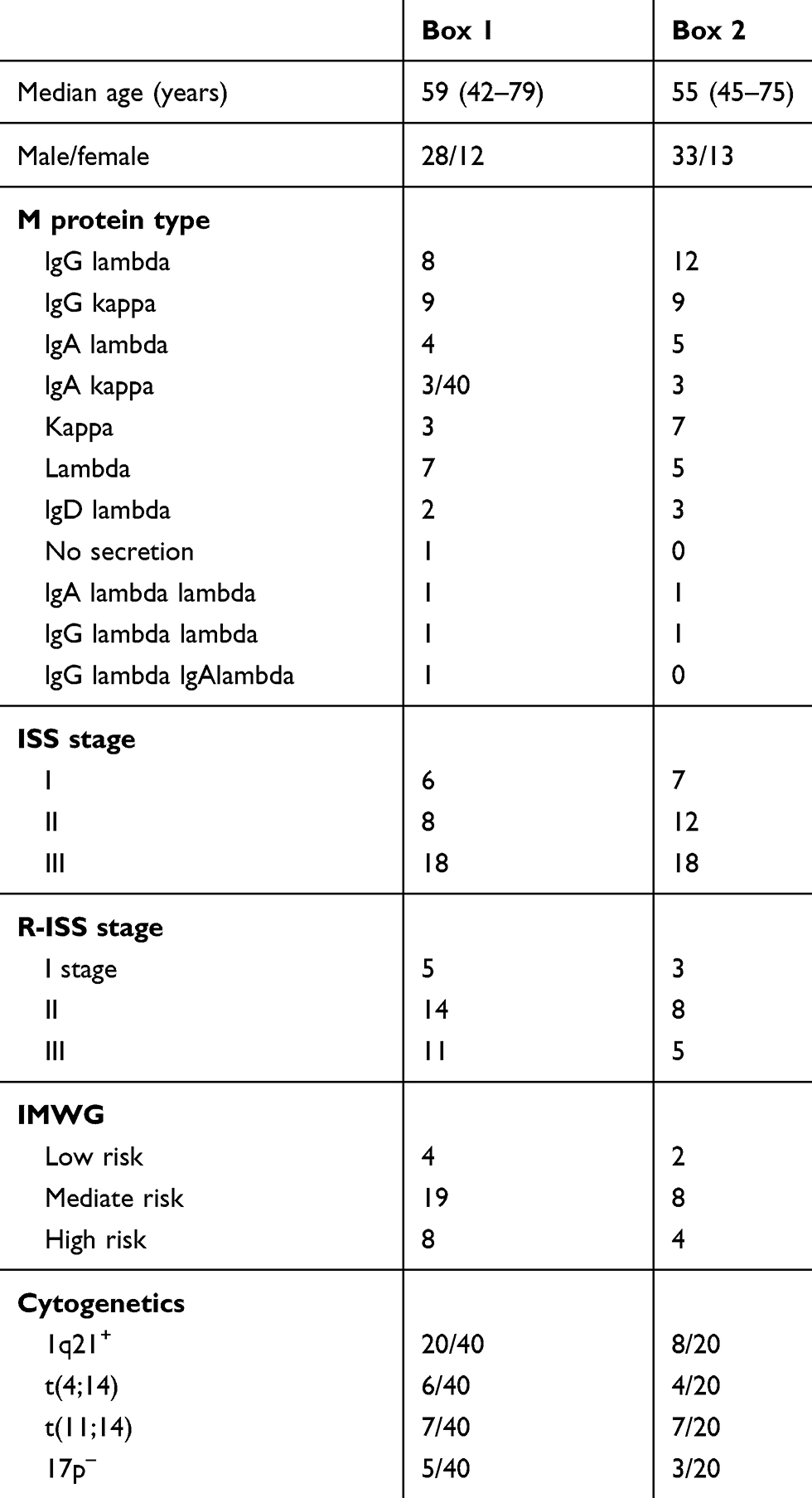 |
Table 1 Baseline Characteristics In Newly Diagnosed Patients |
Results
In the 40 patients who were assayed with Box 1, SNPs were detectable in all patients. In total, 230 missense/synonymous/intronic SNPs were detected. These SNPs were detected in seven genes: CRBN, ATM, FAT4, FAM46C, RB1, NR3C1, and SPEN. SNPs in CRBN were detected in 92.5% of the patients, those in ATM in 60%, those in FAT4 in 37.5%, those in FAM46C in 35%, those in RB1 in 20%, those in NR3C1 in 7.5%, and those in SPEN in 5% of the patients (Table 2). The numbers of patients with SNPs in 1, 2, 3, 4, and 5 genes were 7, 13, 12, 5, and 3, respectively. Mutated genes were detectable in 87.5% of the 40 patients assayed with Box 1. Sixteen mutated genes and 44 mutation sites were detected (Figure 1), including mutations in ATM in 57.5% of the patients, CUL4B in 27.5%, IRF4 in 25%, CCND1 in 12.5%, KRAS in 10%, DIS3 in 10%, CRBN in 7.5%, TP53 in 5%, FAT4 in 5%, NR3C1 in 5%, VCAN in 5%, RB1 in 2.5%, SP140 in 2.5%, NRAS in 2.5%, EGR1 in 2.5%, and BRAF in 2.5% of the patients (Figure 2). A total of 83 mutations were detected in the 40 patients who were assayed with Box 1, including 54 intronic mutations, 18 missense mutations, 6 synonymous mutations, 3 5′/3′-UTR mutations, and 2 deletion mutations (Figure 3). In this group, the numbers of patients with mutations in 1, 2, 3, 4, or 5 genes were 13, 11, 4, 4, and 2, respectively. No mutated genes were detected in six patients. Multiple mutations in a single gene, namely, CCND1, NR3C1, and IRF4, were detected in one patient each. Cytogenetic abnormalities were also screened in the 40 patients assayed with Box 1, with 50% (20/40) of them having 1q21+, 12.5% (5/40) having 17p−, 15% (6/40) having t(4;14), and 17.5% (7/40) having t(11;14). ATM, CCND1, CUL4B, DIS3, BRAF, IRF4, KRAS, EGR1, VCAN, and CRBN mutations were characterized in patients with 1q21+. ATM, CUL4B, IRF4, CCND1, and DIS3 were detected in patients with t(4;14). ATM, CUL4B, DIS3, CCND1, BRAF, KRAS, IRF4, VCAN, and RB1 were detected in patients with t(11;14). In addition, ATM, IRF4, CCND1, and CRBN were detected in patients with 17p−. DIS3 was mutated in 4 of 40 patients, three of whom had t(4;14) or t(11;14). TP53 was mutated in two non-17p− patients, one of whom survived only 7 months while the other survived 13 months. For economic reasons, a further 46 newly diagnosed patients were analyzed only with Box 2 (12 of 30 genes) (Figure 4). NRAS and KRAS were mutated in 7 and 9 of the total of 86 patients, respectively. All patients received bortezomib-based induction chemotherapy. Next, patients younger than 65 received autologous hematopoietic stem cell transplants (ASCT). An analysis of associations with survival was performed on genes with a high mutation frequency, namely, ATM, CUL4B, and IRF4. For this, all 86 patients were followed for 11 to 35 months. There was no significant difference in 2-year PFS between patients with or without ATM (data from 40 patients), CUL4B (data from 86 patients), and IRF4 (data from 86 patients) mutations (P>0.05). However, patients with IRF4 mutations had a tendency toward longer PFS (Figure 5). There was also no significant difference in 2-year OS between patients with or without ATM (data from 40 patients), CUL4B (data from 86 patients), and IRF4 (data from 86 patients) mutations (P>0.05). However, patients with IRF4 mutations had a tendency toward a longer OS time (Figure 6).
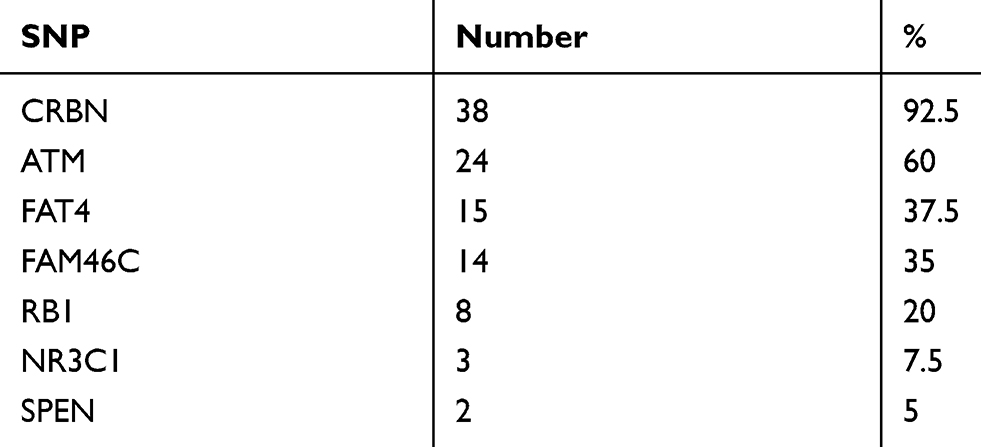 |
Table 2 SNPs In 40 Newly Diagnosed Patients |
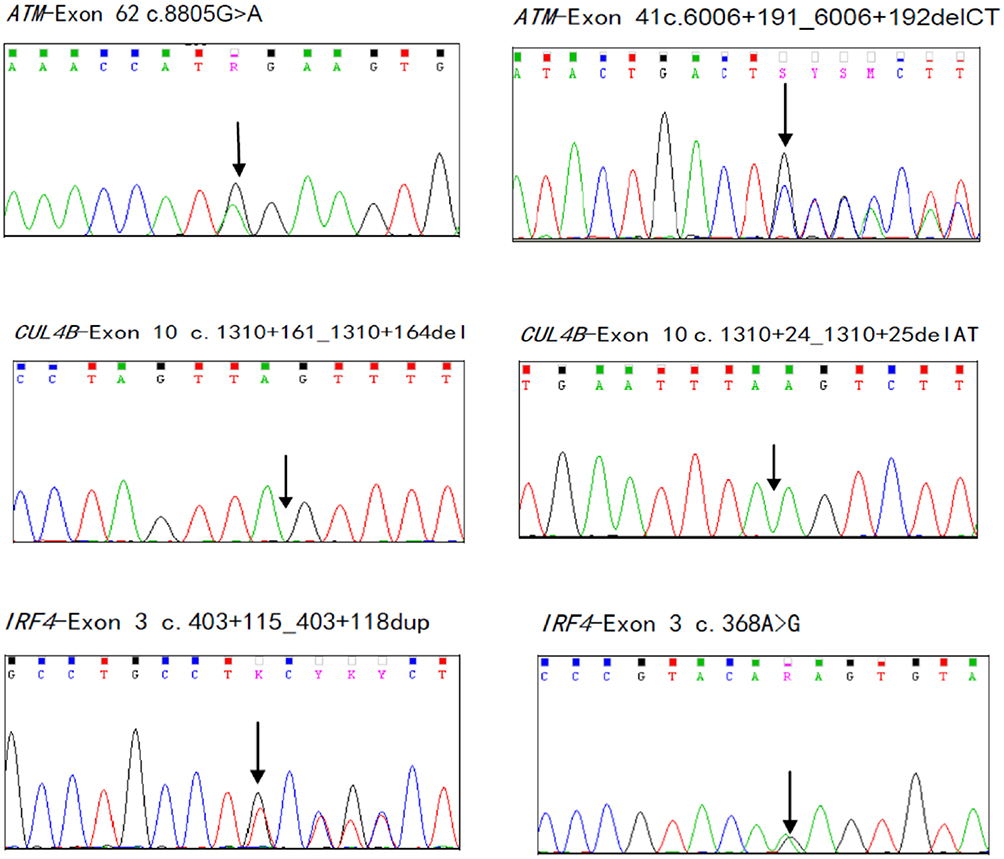 |
Figure 1 (Continued). |
 |
Figure 1 (Continued). |
 |
Figure 1 (Continued). |
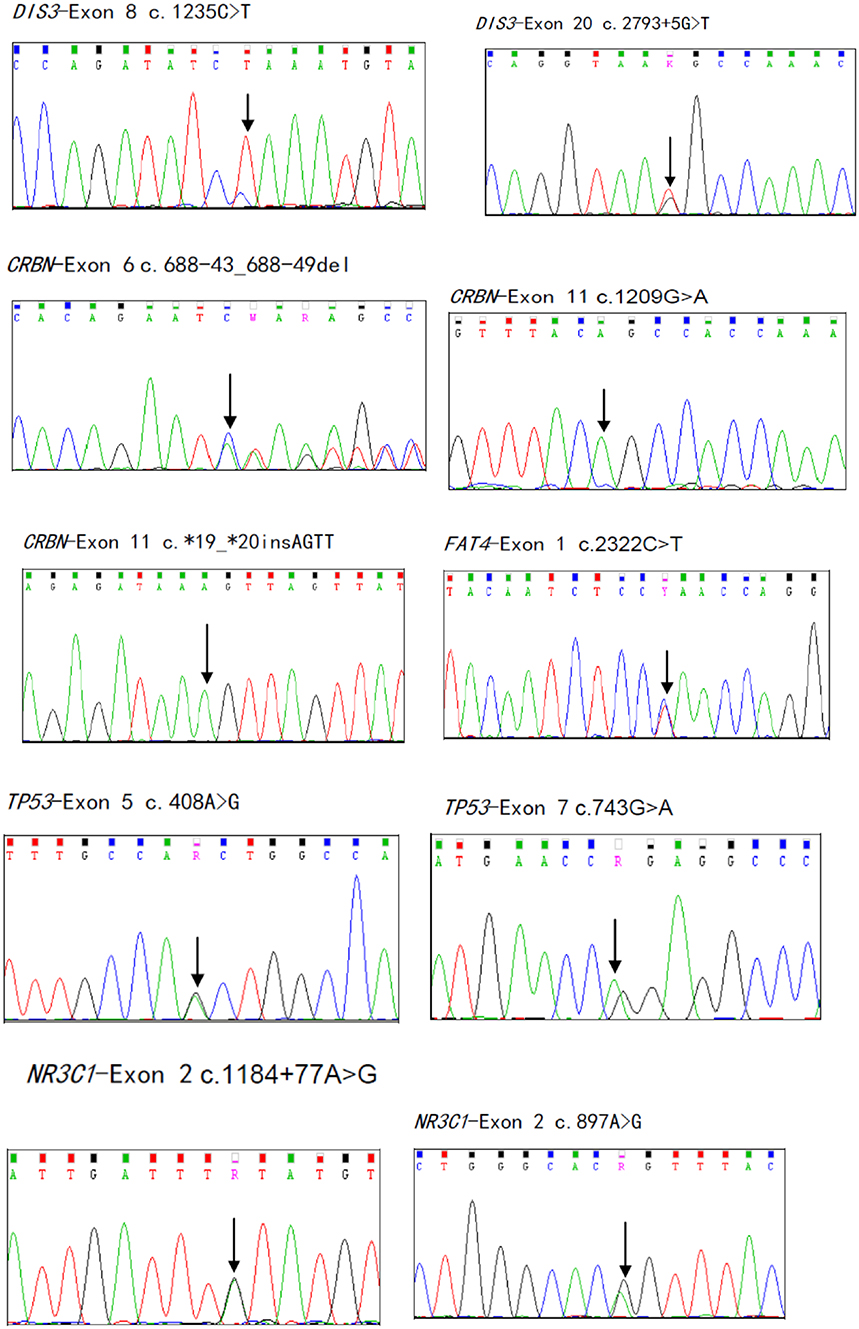 |
Figure 1 (Continued). |
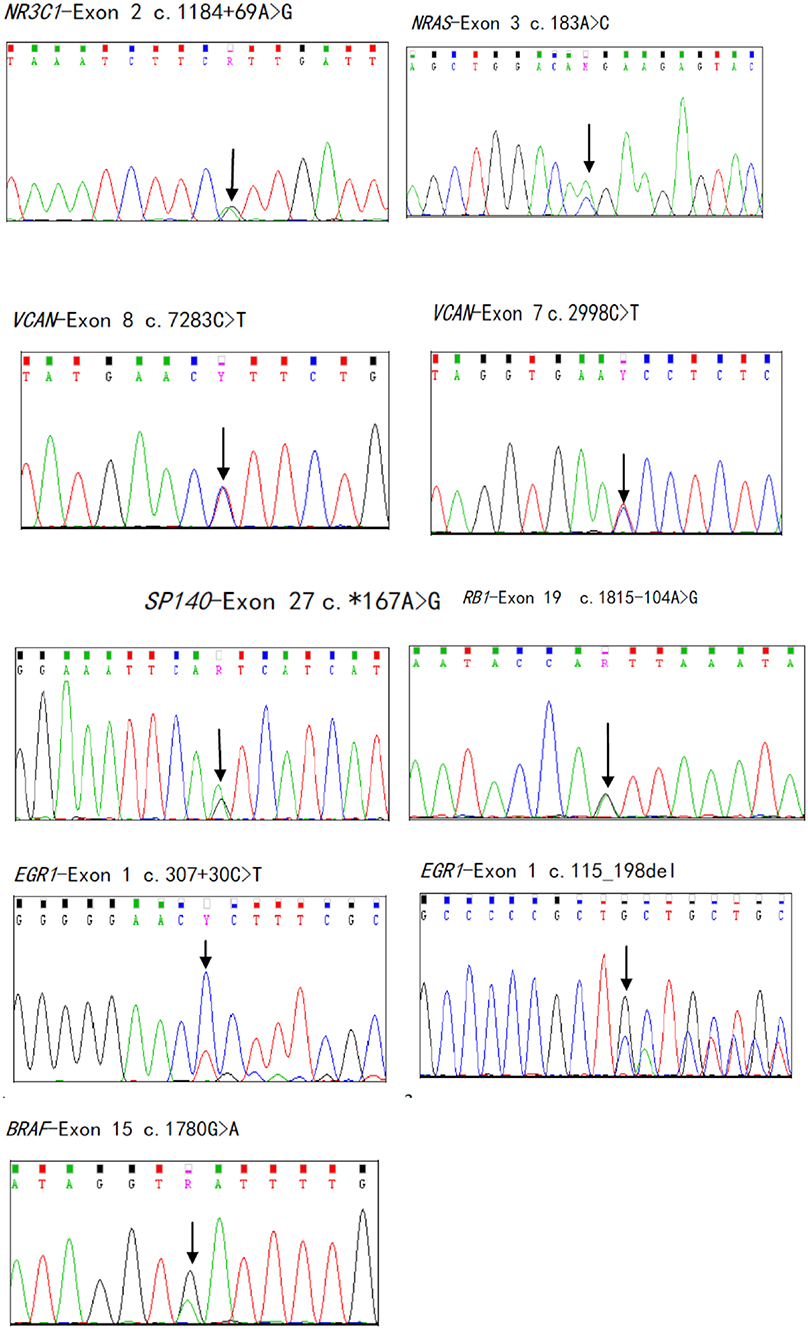 |
Figure 1 Mutation sites of 16 genes in 40 newly diagnosed multiple myeloma patients. Arrows indicate mutation sites. |
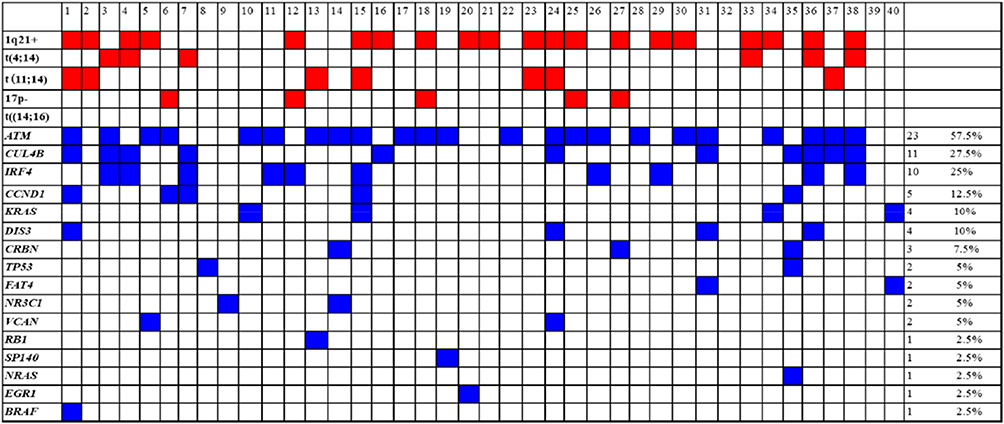 |
Figure 2 Gene mutations in 40 newly diagnosed multiple myeloma patients with Box 1. |
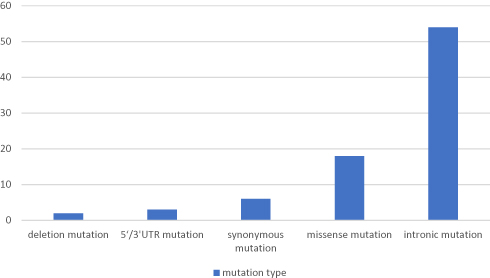 |
Figure 3 Mutation types of 16 genes in 40 newly diagnosed multiple myeloma patients. |
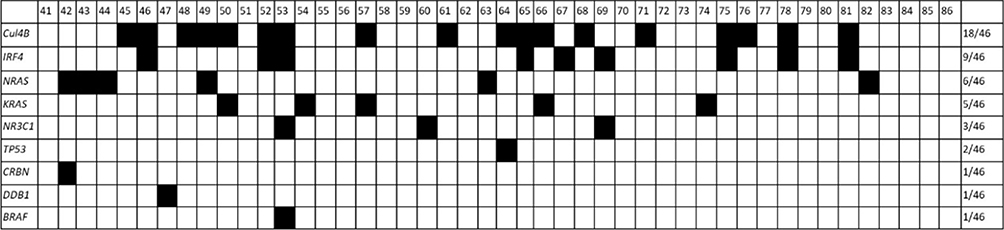 |
Figure 4 Gene mutations in 46 newly diagnosed multiple myeloma patients with Box 1. |
 |
Figure 5 Two-year PFS between patients with or without (A) ATM, (B) CUL4B, and (C) IRF4 mutations. |
 |
Figure 6 Two-year OS between patients with or without (A) ATM, (B) CUL4B, and (C) IRF4 mutations. |
In conclusion, SNPs and other types of mutation are common in newly diagnosed Chinese multiple myeloma patients. In the first part of this study, SNPs were detected in 100% of 40 patients. Genes with other types of mutation were found in 87.5% of 40 patients and such mutations were found in 53.3% of 30 analyzed genes. The genes most often containing SNPs were CRBN, ATM, FAM46C, and FAT4. The genes most often exhibiting other mutation types were ATM, CUL4B, and IRF4. TP53 was mutated in two non-17p− patients, who had very short survival times. In contrast, IRF4 mutations had a tendency to be associated with longer PFS and OS. However, there was no significant difference in PFS and OS in patients with or without mutations in ATM and CUL4B.
Discussion
In our study, 230 missense/synonymous/intronic SNPs were detected. The genes most often featuring SNPs were CRBN, ATM, FAM46C, and FAT4. Multiple SNPs were also found simultaneously in a single patient. In Kortüm et al‘s study, 123 nonsynonymous missense/nonsense SNPs were detected in newly diagnosed patients with 17p–1. SNPs are common in multiple myeloma, but few studies on their roles in this disease have been performed and their clinical significance remains to be determined. In our study, mutated genes were found in 87.5% of the patients and mutations were found in 53.3% of the 30 analyzed genes. Kortüm et al found gene mutations in 78% of newly diagnosed patients with 17p– and revealed mutations in 66% of the 47 analyzed genes.1 Moreover, in a study of genetic heterogeneity in multiple myeloma by Lohr et al, the most commonly mutated genes were KRAS, NRAS, FAM46C, DIS3, and TP53,2 while in our study the most commonly mutated genes were ATM, CUL4B, IRF4, KRAS, and NRAS. It is possible that the genes most commonly mutated in newly diagnosed Chinese MM differ from those in patients from other countries. In our study, NRAS and KRAS were commonly mutated in newly diagnosed patients, while Lohr et al instead reported that they were more often mutated in relapsed patients.2 TP53 has been reported to be the most frequently mutated gene in 17p− patients;1 however, in our study, TP53 was mutated in two non-17p− patients who survived for a very short period, suggesting that TP53 mutation may also occur in patients without 17p− and be predictive of a poor prognosis. Bolli et al also reported that TP53 mutation was associated with impaired EFS (event free survival) and OS.3 Moreover, DIS3 mutations have been reported to be exclusively present in t(4;14) and t(11;14) patients.4 In our study, DIS3 was mutated in four patients, three of whom had t(4;14) or t(11;14). These results suggest that certain gene mutations may be associated with specific cytogenetic changes. Genes that are members of the FAT family have been shown to have a significant number of mutations in chronic lymphocytic leukemia.5 FAT4 was mutated in two patients in our study, although the clinical significance of such mutations remains to be determined. FAM46C is often mutated in MM, but there is at present a very limited understanding of the function of this particular gene.6 Moreover, no FAM46C mutation was seen in our study. However, CUL4B and IRF4 were commonly mutated in our study. IRF4 has been reported to be a factor associated with the survival of MM.7 CUL4B and IRF4 both affect the CRBN pathway, a potential source of IMiD (immunomodulatory drug) resistance.1 CRBN SNPs were common in our patients, but CRBN gene mutations were found in only three patients. There are limited data available on the effects of CRBN gene mutations. One study identified a CRBN truncating mutation and a CRBN point mutation in 1 of 30 MM patients, and two CRBN SNPs in 24 newly diagnosed patients.8 Furthermore, EGR1 was found to be mutated in our study, which was also previously reported to play a role in resistance to MM therapy.9 SP140 has also recently been described as having a possible role as a tumor suppressor in MM.10 A single BRAF-mutant MM patient was recently reported to show a durable response to a BRAF inhibitor.11 So, the role of these mutations needs to be clarified by further research. In our study, multiple mutations of the same gene were detected in the same patient. In addition, mutations of different genes were detected in the same patient. In line with this, Lohr et al observed multiple significant mutations in the same tumor sample: some patients had mutations in two of three oncogenes (NRAS, BRAF, and KRAS) or had two mutations in KRAS.2 Moreover, Walker et al reported that FGFR3 was only mutated in the subgroup of patients with t(4;14), and that CCND1 was significantly more frequently mutated in the t(11;14) subgroup, while t(11;14) was also associated with KRAS and IRF4 mutations.12 However, in our study, no FGFR3 mutations were detected in the t(4;14) group, CCND1 was mutated in different groups with abnormal cytogenetics, and KRAS mutations were detected in the 1q21+ and t(11;14) groups. However, all of these issues require further study. In our study, ATM, CUL4B, and IFR4 were the most frequently mutated genes, so survival analyses of these three genes were carried out. Mutations in IRF4 were previously found to have a positive impact on survival, with a trend toward an improvement in OS (2-year OS, 100% vs 79%, P=0.05).12 In the current study, similar findings were obtained, in that patients with IRF4 mutations had a tendency toward longer PFS and OS. Mutations in ATM were also shown to be associated with a trend toward impaired OS (2-year OS, 50% vs 80.3%, P=0.01).12 However, in our study, there was no significant difference in ATM and OS between patients with and without ATM mutation.
In conclusion, SNPs and other mutation types are common in newly diagnosed Chinese multiple myeloma patients. The genes most commonly exhibiting SNPs and other types of mutation may differ between Chinese patients and those from other countries. It is not certain that gene mutations in newly diagnosed MM vary between patients with different cytogenetic abnormalities. Genetic mutations may be associated with prognosis. More cases need to be accumulated and longer follow-up is needed.
Acknowledgment
We thank Liwen Bianji, Edanz Group China for editing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kortüm KM, Langer C, Monge J, Bruins L. Targeted sequencing using a 47 gene multiple myeloma mutation panel (M3P) in −17p high risk disease). Br J Haematol. 2015;168(4):507–510. doi:10.1111/bjh.2015.168.issue-4
2. Lohr JG, Stojanov P, Carter SL. Widespread genetic heterogeneity in multiple myeloma: implications for targeted therapy. Cancer Cell. 2014;25(1):91–101. doi:10.1016/j.ccr.2013.12.015
3. Bolli N, Avet-Loiseau H, Wedge DC. Heterogeneity of genomic evolution and mutational profiles in multiple myeloma. Nat Commun. 2014;5:2997. doi:10.1038/ncomms3997
4. Walker BA, Wardell CP, Melchor L. Intraclonal heterogeneity and distinct molecular mechanisms characterize the development of t(4;14) and t(11;14) myeloma. Blood. 2012;120(5):1077–1086. doi:10.1182/blood-2012-03-412981
5. Messina M, Del Giudice I, Khiabanian H. Genetic lesions associated with chronic lymphocytic leukemia chemo-refractoriness. Blood. 2014;123(15):2378–2388. doi:10.1182/blood-2013-10-534271
6. Boyd KD, Ross FM, Walker BA. Mapping of chromosome 1p deletions in myeloma identifies FAM46C at 1p12 and CDKN2C at 1p32.3 as being genes in regions associated with adverse survival. Clin Cancer Res. 2011;17(24):7776–7784. doi:10.1158/1078-0432.CCR-11-1791
7. Shaffer AL, Emre NC, Lamy L. IRF4 addiction in multiple myeloma. Nature. 2008;454(7201):226–231. doi:10.1038/nature07064
8. Thakurta A, Gandhi AK, Waldman MF. Absence of mutations in cereblon (CRBN) and DNA damage-binding protein 1 (DDB1) genes and significance for IMiD therapy. Leukemia. 2014;28(5):1129–1131. doi:10.1038/leu.2013.315
9. Chen L, Wang S, Zhou Y. Novel target for JUN-induced apoptosis in multiple myeloma. Blood. 2010;115(1):61–70. doi:10.1182/blood-2009-03-210526
10. Di Bernardo MC, Crowther-Swanepoel D, Broderick P. A genome-wide association study identifies six susceptibility loci for chronic lymphocytic leukemia. Nat Genet. 2008;40(10):1204–1210. doi:10.1038/ng.219
11. Andrulis M, Lehners N, Capper D. Targeting the BRAF V600E mutation in Multiple Myeloma. Cancer Discov. 2013;3(8):862–869. Available from: https://www.dovepress.com/cr/email/compose_email.
12. Walker BA, Boyle EM, Wardell CP. Mutational spectrum, copy number changes, and outcome: results of a sequencing study of patients with newly diagnosed myeloma. J Clin Oncol. 2015;33(33):3911–3920. doi:10.1200/JCO.2014.59.1503
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.