Back to Journals » Nature and Science of Sleep » Volume 12
Music Therapy as a Potential Intervention for Sleep Improvement
Authors Loewy J
Received 26 August 2019
Accepted for publication 5 December 2019
Published 7 January 2020 Volume 2020:12 Pages 1—9
DOI https://doi.org/10.2147/NSS.S194938
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sutapa Mukherjee
Joanne Loewy
The Louis Armstrong Center for Music and Medicine, Mount Sinai Beth Israel, New York, NY 10003, USA
Correspondence: Joanne Loewy
The Louis Armstrong Center for Music and Medicine, Mount Sinai Beth Israel, 10 Union Square East, New York, NY 10003, USA
Tel +1 212 420-3484
Email [email protected]
Abstract: Sleep deficiency is linked to chronic health problems, such as heart disease, kidney disease, high blood pressure, diabetes, stroke, obesity, and depression. Healthcare practitioners are increasingly paying close attention to sleep and its impact on health and wellness as a measure of critical vitality. Sleep’s impact on neurologic function, and cognitive endurance affect capacity throughout the lifespan. This article will address recent findings related to the potential of music to induce sleep in illness and wellness. Music therapy research findings and its efficacy as a potent cost-effective intervention will be highlighted.
Keywords: music sedation, music therapy, sleep induction
Introduction
Healthcare practitioners are increasingly paying close attention to sleep and its impact on health and wellness as a measure of critical vitality. This is most particularly being focused upon in sleep’s impact related to neurologic function and cognitive endurance and capacity throughout the lifespan. A lack of sleep increases the likelihood of mortality and the risk of chronic diseases including stroke, hypertension, diabetes, obesity, heart disease, stroke, and depression. 1 This article will address findings related to the potential of music to impact sleep in neurologic function in illness, and wellness. Music therapy as a potent cost-effective intervention will be highlighted.
Sleep Deprivation as a Health Risk
The cost associated with poor work attendance due to insomnia is approximated at $63.2 billion per year in the United States, according to the American Association for Sleep Medicine. 2 Sleep loss alters the structural plasticity involved in neural signals of the brain where dendritic spine numbers and morphology are affected. The result poses threats to mood, cognitive performance and one’s capacity to sustain vigilance to activities.3 One survey suggested a 293% increase in the number of sleep-related prescriptions from 5.3 to 20.8 million prescriptions from 1999 to 2010.4
Sleep capacity comes into view as a distinct measure of health that can likely contribute to disease progression. It is considered to be a major influential factor reflected in how patients perceive pain5 and subsequent anxiety which risks impairing resiliency factors that potentially combat illness.
Ironically, in hospitalization, nighttime routine checks can disrupt sleep, as so often the busy and acoustically jarring environment experienced in in-patient care awakens patients. Exacerbated interruptions of sleep cycles and insomnia can be the result of too much or too little sleep. While there is a debate about the impact of over-stimulation or not enough stimulation, that can complicate the optimal care of neonates6 or adults7 who are housed in hospitals, and most particularly within communal units, there is no contesting amongst the medical community about the importance of sleep. “Sleep health” is instrumental toward one’s capacity to fight disease, and regular routine sleep habits can increase resilience in maintaining wellness.2
Noise as a Sleep Hazard
A recent study seeking to learn about the intensive care unit (ICU) environment and the potential sources of sounds patients may be exposed found that the mean ICU noise levels exceeded those recommended by the World Health Organization.8 In fact, the acoustic intensity was reportedly 193 times greater than what was recommended. Sleep disruption was the reported result of noise for fragile patients whether in a multi-bedded unit or in single-roomed units. The descriptions of the sources of noise were largely staff conversations-with unpredictable variability that resulted in substantial sleep disruption. The study represented a baseline cohort of 24 beds, and an effort on this research teams’ quest to develop effective sound abatement strategies. They first determined nocturnal noise levels and their variability and in turn then posited to strategize ways to address sound abatement.8
Environmental Music Therapy (EMT) is one such abatement strategy that has been utilized and researched in two hospital contexts, with subsequent results that will be described later in this article.9,10 EMT is inclusive of addressing and attending to not only patients, and their partners, but to staff as well. It substantiates a potential appeal to the body of literature that has revealed that the voices of professional caregivers can invasively pervade the sound environment.11–13 Additionally, where acoustic obtrusion compromises sleep health in the most fragile patient environments, such as geriatric wards,9 where incidents of falls and memory loss are often attributed to sleep impairment, EMT may offer a safe, viable, cost-effective option.
Music’s Role in Sleep Induction
Neurologically, even as the body is seemingly resting, the mind is quite active during sleep. The mind unconsciously processes thoughts previously dismissed or, put aside as afterthoughts that occurred throughout the active, waked experience of the day.11
Typically, aspects related to the application of music and its use as a therapeutic tool have been documented from ancient to current times as a potent stimulator or sedative in bringing about optimal activation or sleep potential. One typically utilizes activating rhythms and strong beats to infuse an energetic state. Yet, this should not be confused with the neurological impact that repetition and predictability of rhythm, especially when combined with melody and harmony, can provide. Slow repetitive rhythms so often can imbue feelings of safety and familiarity that can prepare and induce the brain’s sleep response.
Accounts of music’s capacity to activate or sedate have been historically recorded throughout humankinds’ use of music. For instance, marching bands typically preceded wars in ground battle times, and currently, they precede events that seek to mark a prowess of strength, such as warming up for football games. The strong beat and accent on 1 (the downbeat), or 1 and 4, signal preparation prompting neurologic cues of wakefulness and attention.
At the same time, music has been used to soothe and sedate. In the Old Testament of the Bible, there were numerous accounts of spirits tormenting Saul, resulting in David playing the lyre and strumming a soothing tune. As a result, Saul was relieved from his terror, as the music prompted the evil spirits to leave his tormented body, so he could rest with ease.
One might question how music is used in our modern age to induce sleep. A recent review of 35 sleep apps on the worldwide web market revealed essential elements analyzed as “behavioral construct scores” related to sleep. These reflected the variety of uses that were perceived as central to devising sleep programs. They included realistic goal setting (86%), time management (77%), and self-monitoring (66%) as the most common sought contingencies in developing programs that were most suitable for sleep.12
The potential for successful use of music in therapeutic and clinical settings may present a viable, low-cost option, particularly appealing in our culture of pharmacologic addiction, as it is free from side effects.13 Yet, the majority of studies claiming to implement “music therapy” in numerous clinical trials do not involve music therapy, nor do they include consultation with a music therapist. Furthermore, while music may be instrumental as a sleep aid, there is surprisingly a dearth of research that has evaluated the music implemented in sleep studies, and the rationale involved in implementing the music selected for the study. No identified assessments, for instance, have scrutinized decision-making pertaining to the characteristics of elements utilized within music (melody, harmony, rhythm, meter, timbre, structure) that would lend investigators to hypothesize how these factors might impact the neural mechanisms involved in sleep.
These most basic essential music elements; melody, harmony, rhythm, meter, timbre might serve their integrated prowess – music, more effectively if each was first analyzed prior to being combined into a piece of music. As a result, programmers and musicians seeking to invoke sleep responses using music would likely include decisions related to content and genre within these combined elements. They could also consider the listening length of prep – prior to sleep. This would impact considerations of transitioning, with musical sensitivity to ease from wakefulness into sleep cycles-based on population, age, culture and context. Sleep-Wake cycle observations and patients’ history of sleep in the research pertaining to sleep disturbances include a quantified investigative measurement. The Pittsburgh Sleep Quality Index (PSQI) is a widely used instrument, inclusive of critical areas such as sleep quality, latency, duration, efficiency, disturbance and daytime function.
Polysomnographic measurements of sleep (PSG) are multi-parametric tests used in the study of sleep and as a diagnostic tool in sleep medicine. Polysomnographic measurements of sleep with music were compared to a tone and control group14 in a study that sought to uncover the most efficacious use of music by implementing a commercially available selection specifically designed to improve sleep. The rationale for implementing the selected music in this study was that the subjects had no previous exposure to it and therefore would preclude possible positive or negative associations to it. This begs to question why music with a positive association, particularly music that is familiar and deemed by a subject (within a music therapy evaluative context, for instance) as relaxing, would not be implemented as a resource worthy of implementation for study. The fact that “testable claims were made by the manufacturer” of the music used in this research that implemented a “Delta Sleep System” raises questions about the “tests” and how musical preferences were accounted for. Claims of superiority endorsing any “one size fits all” product, and in this case improvement of overall sleep quality based on slow-wave sleep increase, are not representative of personalized care in best practice music therapy standards.14
Music as a Viable Resource
If one is to study the impact of music as a sleep aid, analyses of the music implemented should be at the forefront and it may best be inclusive of a contingency analysis at the pre-institution stage. A recent Cochrane review15 on sleep revealed no analytic categorization for the best practice of selecting music. The supposable participant-selected music was most often labeled as a choice amongst researcher pre-selected music that is arguably indeed still music influenced by researchers’ biases. This does not reflect best practice essential to music decision-making in music therapy.16 To provide familiarity, predictability and most significantly, safety, the individualization of comfort, met within the music conditions will likely be enhanced when conditions of sleep are met with participant choice.17,18
Our team has been studying sleep and methods of music and music therapy interventions that induce a sleep response for many years. The following video clip shows an example of the author’s use of music therapy with a neonate where a musical instrument, the Remo Ocean disc and a vocal technique called “tonal vocal holding”17 induced a sleep response in less than 1 min (https://www.pbs.org/wnet/musicinstinct/video/interviews/music-and-medicine-music-therapy-for-infants/76/).
Themes Identified in Music Sleep Studies
It is no surprise that the abundance of articles examining sleep difficulties in adults have studied the elderly and often attribute incurring frequency of sleep difficulties to physical restrictions, lack of movement, disease progression and/or comorbidities, as well as changes in cognitive status related to aging and loss.9
Older patients present with safety issues often related to commonly prescribed daytime sedation (benzodiazepines). There are often increased risks of falls. As the importance of sleep in hospital recovery and the side effects of sleep medications are increasingly recognized, nonpharmacological alternatives, such as music, and music therapy are considered as safe options and may be cognitively and neurologically indicated.
A recent review of sleep studies in the medical field showed that the designs used for measuring sleep were relatively poor, and recommended that polysomnography19 and actigraphy be implemented to obtain more quantifiable outcomes. A recent review of actigraphy20 supports its use as a low cost, objective measure of sleep patterns and furthermore revealed that certain estimated sleep parameters in both children and adults, and across a wide range of sleep disorders, can be assessed most particularly when conducted using validated algorithms with attention to sensitivity settings and standardized scoring procedures. The review finds its use most effective when utilized in conjunction with sleep logs.20 Measurements over a 24 hr period were found to be most constructive and, perhaps most essentially, implementation of actigraphy has proven useful for assessing circadian dysrhythmia.
Insomnia and sleep difficulties associated with disease-related hospitalizations are common grounds for researching music and music therapy’s effect on sleep.21 There is evidence that there are measurements indicative of cerebrospinal fluid associated with Alzheimer’s disease pathology and sleep disturbances.22
A large concern is the link between insomnia and suicide that is apparently quite common in the US, in older adults. (Centers for Disease Control and Prevention, 2012, Web-based injury statistics query and reporting system. Retrieved July, 13, 2019, from http://www.cdc.gov/injury/wisqars/index.html.) One wonders why infants, children and teens23 are less commonly researched in sleep capacity.24,25
In a meta-analysis that viewed music “therapy” in acute and chronic sleep disorders,26 10 studies involving 557 participants were identified, but the pool of subjects studied did not show measured characteristics typically characterized as insomnia, rendering results that reveal a broadly mixed span of included trials.
Music has been shown to have an effect on the level of depression in the elderly, and this effect has been directly correlated with sleep.27,28 This is representative of another body of literature that stratifies how common comorbidities occur alongside irregular sleep patterns in the elderly29 In implementing music programs to induce sleep, 3 weeks of listening seem to be the recommended amount of “expectancy” time where a threshold of a comfort-effect time can take hold.
An overview of the themes broadly undertaken in the research15,25–28,30 views “music” as a general intervention and focuses more on the outcomes resulting from its use, rather than delineating how its decisions for use are implemented. This prompts the need to examine more distinctly the calming, tranquil elements of music. This will lead toward a more effective evaluation of the musical characteristics and conditions that enhance sleep capacity. In this way, distinctive criteria of implementation and maintenance of music will foster best practices for sleep health. Furthermore, the elements of consideration when utilizing music for inducing sleep should be provided. These are often mentioned in sleep article summaries but not as pertaining to music considerations related to age, diagnosis, the significance of awake activity-levels, past relationship with music, context, psychosocial contributing factors, etc.
An interesting study within recent literature took a broad view in a sleep investigation,30 where researchers surveyed 62% of responders inclusive of 651 people originally surveyed through the internet. In using questions that considered past and present relationships with music, and sleep habits, their analysis of the reported 14 musical genres of 545 artists showed trends related to sources of stress, age, and past and current music use as significant predictors of sleep quality (PSQI) scores.
This study found that younger people with higher musical engagement were significantly more likely to use music as a way to enhance sleep. The analysis of categorical themes taken from the open text responses revealed the beliefs of responders that were quite informative and relevant to the considerations of music utilized for sleep conditions. These included: music used as a provision, as a routine-habit, as a means of altering mental or physical state capacity; or as a blocking-of noise or thoughts that otherwise could keep someone awake.
Age range, level of musicality, past and present sleep habits and stress levels provided new insight into what the authors called “pathways of effect” which they defined as the elements involved in considering the choices people make when utilizing music as a sleep aide.30 In terms of the kind of music used, there were no typical trends or necessarily defining characteristics. The music selections were explained as “idiosyncratic preferences” and there were no overall general rules or musically identified sequences that the selected pieces’ content had in common. The deductions that the researchers noted were that the music that supports sleep health went far beyond physical/mental relaxation. They observed diversity in musical choices.
The Musical Choices That Induce Sleep
Music therapists are concerned with not only the actual music utilized to achieve sleep, but also the decisions made in creating the most clinically indicated programs for sleep. This results from a full music therapy assessment. In this way, the clinical considerations can lead to critical content evaluation31 inclusive of elements related to sequential analyses. The analysis of how distinct pieces of music should be layered into a consecutive program is critical. This implores that “music” should not include an arbitrary intervention that is necessarily researcher- or even solely patient-selected and then implemented without the discipline of the procedure. Sleep is one of the brains and body’s foremost activities whereby mechanisms of anxiety and trauma will necessarily impact its onset. It is, therefore, most advantageous to have a certified music therapist incorporate evaluated mechanisms of current psychological states with consideration of neurologic impostures to design easeful wake–sleep transitions.
Institution of a Music-Based Sleep Protocol
Best practice recommendations for inclusion of music in a treatment trajectory should consider essential elements that will inform the clinical advice of an individualized sleep program inclusive of the decisions that are made in rendering the music.
Conditions of Sleep Analysis:
- Past sleep history
- Issues of anxiety that may be perpetuating one’s capacity to relax
- Decisions involving the duration of the music intervention based on:
- Age, diagnosis, treatment recommendations inclusive of logged measurements defining:
- The time it takes one to typically go through the sleep cycle, and
- Analysis of depth and quality of sleep pre/post-intervention
- Age, diagnosis, treatment recommendations inclusive of logged measurements defining:
The critical decision-making that informs clinical inferences affecting the actual content of the music utilized in treatment planning involves careful consideration of culture. Music research hypotheses can succinctly address the decisions of how and why the music selected would likely be most potent for inducing sleep.
The music selected for implementation in sleep protocols might also warrant analysis by music therapists, who in turn can provide clinical inductions that will influence the music programming. Patient-selected music programs can be devised to alter tempo, meter, and intensity based on patient presentation. Attention to the design of how musical pieces are sequenced can be instituted to elicit gradual de-activation by manipulating the essential elements of music.31 In this way, music sleep regimens can be therapeutically and strategically rendered suitable for a sleep-informed plan of care.
Critical decisions related to how to structure music that can serve the unique needs of distinct clinical populations are missing from current literature. Focus on music’s unique characteristics will better address personalized programs that are central to sleep capacity in future planning. Furthermore, the involvement of music therapists as researchers, and/or consultants that is been noticeably void in the literature will influence the research and practice of sleep, likely leading toward better outcomes. The aforementioned review30 did relay that how one uses music – daily, prior to sleep – was an effective factor in music’s likelihood of improving overall sleep quality when used for sleep in adults. This finding is related to the everyday routine and habits of the participant and strongly considers exposure and familiarity of music in health and wellness conditions to be of central value.
Music Therapy Considerations as Best Practice: Decisions Involving Music Choice
Sedation & Sleep in Babies and Children
Nearly 2 decades ago, the American Academy of Pediatrics relayed the potential risks of pharmacological sedation for infant and young children in the following statement: “Although transient hypoxemia is unlikely to lead to long-term consequences, unrecognized or inadequately treated hypoxemia, especially when related to airway obstruction, may progress to more severe complications.”32
Having observed first hand, some of the complications of pharmacological sedatives, our integrative team, consisting of a pediatric neurologist, nurse, and music therapist, set out to formally compare what we had piloted in so many cases in helping children become sedated for EEG and other medical tests. We implemented a formal music therapy protocol instituting culturally selected, indicated “songs of kin” that music therapists and/or parents could sing in a therapeutically adapted way, to assist in the sedation of their children for medical testing.18 From this research, we refined a music sedation protocol (Figure 1) that has been in use ever since for patients requiring sedation for medical testing, and it has also been used to assist patients with sleep deprivation from anxiety.
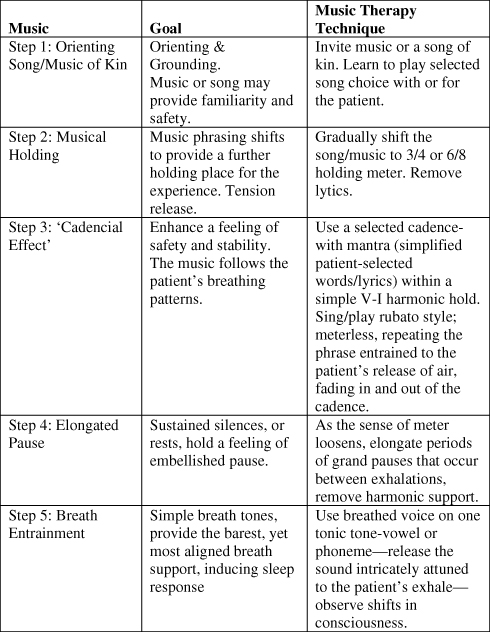 |
Figure 1 Music sedation protocol. Notes: Reprinted with permission from: Musical sedation: Mechanisms of breathing entrainment. In: Azoulay, R, Loewy JV (editors). Music, the breath and health: advances in integrative music therapy. New York, NY: Satchnote Press; 2009:228.33 |
Implementing aspects of the music itself, melodies that were familiar to the children and parents, (“song of kin”) proved to be the most critically clinically indicated part of this clinical trial. The sedation and “song of kin” protocol was also instituted in a subsequent clinical trial inclusive of 272 neonates in 11 NICUs in the US.17 The melodies utilized were strategically implemented with meter adaptations, to lullaby formats, and often removal of lyrics to accentuate the parents’ voices-conditions providing opportune circumstances for entrainment. The music therapy “song of kin” intervention was proven to be effective whether offered by a parent or by a music therapist. This was reflected in the amount of sedation that was required (less chloral hydrate), and reduced the length of time it took for the children to be sedated in order to complete the EEG.18 The live aspect of the music enabled opportunities for the music therapists to entrain to the breathing rhythm of each child in the moment, which prompted feelings of safety, thus enhancing sleep.
A pre-procedure survey of the children’s parents helped us to learn the conditions of sleep at home, such as: does the child sleep in his/her own room, is the room quiet or noisy, is it dark or bright how long does it typically take the child to fall asleep. Knowing these conditions set the stage for how the music was administered.
Project Sleep
A second study, again involving music therapy, and a sleep-informed treatment plan was undertaken by a multidisciplinary core team including geriatricians, doctors, nurses, pharmacists, music therapists, and house staff. It took place with elderly adults in an inpatient medical unit. The study, entitled “Project Sleep” included the administration of a 5-question sleep survey to 125 patients8 that served as our pre-intervention group over a period of 10 months.
We aimed to strategize the use of non-pharmacological methods (inclusive of several music therapy interventions) to enhance inpatient quality of sleep with two explicit goals: to decrease falls and reduce zolpidem use. We also sought to improve patient experience. We piloted our protocol on a medical unit that had a history of low patient satisfaction scores resulting from what was reported on surveys as a “high volume noise” level, which had a direct impact on sleep. Interventions from former studies such as the HELP study (Hospital Elder Life Program) and a sleep pilot at one of our other hospitals34–39 provided baseline outcomes for the research protocol.
The Project Sleep protocol included evaluation of the optimal conditions necessary for each patient’s sleep through a pre-assessment that provided us with a means for understanding the hospital hindrances perceived by patients which were perceived to impair or interrupt their sleep. These questions included: patient-perceived quality and quantity of sleep, and pain/anxiety’s contribution to sleep. It also included the environmental conditions/obstructions such as noise, TVs, visitors, lighting, blood draws. Defining the sleep antagonists in this study was useful. So, too was our survey of what patients perceived would reportedly help them sleep-such as tea, melatonin, warm milk, etc. Individual and group music therapy sessions were also provided on the unit during the potentially noisiest time, and to patients who were referred by staff to be anxious on a twice-a-week basis.
The results of Project Sleep rendered from 125 patient surveys demonstrated a significant difference in the mean quality of sleep pre and post-intervention. A trend was also noted of decreased zolpidem orders. There was also a trend of improvement in several areas including an increased quietness of the environment.9
Environmental Music Therapy (EMT)
EMT was implemented into our study during the times slated as “noisiest” by patients and staff on the unit.9 EMT was first defined as an intervention of in-the-moment live music application for the purpose of modulating the experience of perceived noise.40 Whether induced by a beeping monitor, unexpected sounds (temperature, or blood pressure monitors, paper towel-automated machines, floor sanitizers, or staff or caregiver voices), the recurrence of a stress response caused by environmental noise can directly impact sleep, increase anxiety, and/or perpetuate irritation leading toward anger, annoyance, or depressive shut-down. EMT is an improvisatory process that relies on the agility and sensitivity of music therapists to gently incorporate the existing aural elements of ambient sounds into a purposeful soundscape/soundtrack of music.10,41–43 Familiar melodies (instrumental or song) reflective of the culture, age groups, and ethnicities through request and extension of requested eras, in a calculated arrangement based on the patient and staff recipients’ movement, discussion, and activity level ensue within each EMT application. In this way, secondary stressors of staff that may contribute to the noise of a unit can also be addressed.
In Project Sleep,9 we also incorporated “Caring for the Caregiver” groups for staff, to address their compassion fatigue. This is an understudied phenomenon in the literature. Although it is documented in studies44 that staff conversation is a high contributor to noise in the hospital setting, to date, few provisions have implemented mechanisms that have taken on staff stress. It is a complicated postulate to consider that the speaking voices of professional caregivers may escalate in pitch, tempo, and intensity, contributing to the perception of noise in the environment. However, we have found, that EMT and “Caring for the Caregiver” music groups for staff have improved their alacrity and eased their capacity to maintain calm in their caregiving. We observed this effect and reported it in our Project Sleep study.
Through time-sensitively scheduled short periods of music respite designed specifically for staff, the expression of care and safety may have provided some direct trickle-down effect for patients. In designing groups for staff that incorporated breath work, music visualization, tension release, and vocalization, a higher degree of mental acuity seemed to be maintained and was reported in our surveys.9
Conclusion: Recommendations Involving Applications of Music for Optimal Sleep Health
The topic of sleep is of growing interest to physicians and healthcare providers in general. Specialty clinics are increasingly investigating issues related to sleep, as persistent lack of sleep is so frequently associated with other physical and mental disturbances. A recent article supported by the National Sleep Foundation as well as the National Heart, Lung, and Blood Institute and the National Institute of Environmental Health Science noted how diagnostic and treatment parameters are notably influenced by sleep outcomes. The detection and treatment of sleep disorders, the authors assert, can lead to a decrease of exacerbated problems seen in the context of other diseases:
In psychiatry (to aid diagnosis of anxiety disorders), neurology (in diagnosis, treatment planning), cardiology (to improve prognosis in heart failure/hypertension), rheumatology/pain (to improve quality of life and aid treatment), oncology (to address insomnia/fatigue), obstetrics (evaluate risk for complications)…and other specialties.45
This article opened with a review of how music has been utilized as a sleep intervention. With a plethora of articles that sought to answer questions about whether or not music was effective and how sleep was best measured, the context, conditions, and the music decision-making considerations were omitted from most of these studies.
Through the examination of the themes identified in former sleep studies, the development of a music-based sleep protocol has been highlighted. In particular, it is recommended that future studies necessarily include a Conditions of Sleep Analysis prior to the institution of a sleep protocol. It is likely most efficacious to include a music therapist who can identify the clinical decisions that are most relevant to the rendering of music that will be implemented.
Two studies described in this article, one with infants and toddlers18 that compared pharmacologic sedation versus music therapy for medical testing, and a second involving a music protocol inclusive of patients, staff and the environment,9 provide clear examples of how music can improve sleep. Variables to be considered as integral should include diagnosis, age, population, cultural background, and the characterization of the music itself (“playlist” or program).
Sound masking has been recommended as an effective technique for improving sleep in the hospital and one study highlighted the recommendation that “future research should (have) close collaboration between medical researchers and acousticians”.44 The second study described, in this article, “Project Sleep”9 provides a novel contribution, addressing the environmental factors of music, music therapy and medicine and the conditions that affect sleep. These are presented as correlates to assessing the most essential treatment conditions developed for patients during critical times.
Music, in and of itself, may or may not improve sleep. If skillfully selected, and when music can be part of a protocol informed by music therapists, the likelihood of its contributing to sleep health will increase. In this way, analysis of the music and clinical decision-making, along with integrative practice considerations, will provide an informed foundation.
Familiar music that is patient-selected accompanies the idea that cultural relevance can be individualized and catered within music interventions. Such adaptations toward meeting patient needs can easily be implemented to address patient comfort. Assessing a patient’s point of trauma, whether disease-related or mentally infused by anxiety is a necessary component to consider in sleep evaluation. Prescribing music and instituting specific aspects of musical elements requires knowledge and consultation with professionals that have analyzed genre, complexity and musical idioms.9
The recognition that music can increase comfort and decrease anxiety impeding sleep capacity is important. As sleep is considered to be a vital sign, viewing the conditions whereby music is instituted most efficaciously can lead toward optimal outcomes.
Disclosure
The author reports no conflicts of interest in this work.
References
1. National Center for Chronic Disease Prevention and Health Promotion. Sleep and Sleep Disorders. March 2015. Available from: https://www.cdc.gov/sleep/index.html.
2. Kessler, R Berglund, P, Coulouvrat, C, et al. Insomnia and the Performance of US Workers: Results from the America Insomnia Survey. Sleep. 2011;34(9):1161–1171.
3. Ford ES, Wheaton AG, Cunningham TJ, Giles WH, Chapman DP, Croft JB. Trends in outpatient visits for insomnia, sleep apnea, and prescriptions for sleep medications among US adults: findings from the national ambulatory medical care survey 1999–2010. Sleep. 2014;37(8):1283–1293. doi:10.5665/sleep.3914
4. Raven F, van der Zee E, Meerlo P, Havekes R. The role of sleep in regulating structural plasticity and synaptic strength: implications for memory and cognitive function. Sleep Med Rev. 2018;39:3–11. doi:10.1016/j.smrv.2017.05.002
5. Mondanaro J, Homel P, Lonner B, Lichtensztejn M, Shepp J, Loewy J. Music therapy increases comfort and reduces pain in patients recovering from spine surgery. Am J Orthoped. 2017;46(1):E13–E22.
6. Pineda R, Neil J, Dierker D, et al. Alterations in brain structure and neurodevelopmental outcome in preterm infants hospitalized in different neonatal intensive care unit environments. J Pediatr. 2014;164(1):52–60.e2. doi:10.1016/j.jpeds.2013.08.047
7. Elbaz M, Leger D, Sauvet F, et al. Sound intensity severely disrupts sleep in ventilated ICU patient throughout a 24-h period: a preliminary 24-h study of sleep stages and associated sound levels. Ann Intern Care. 2017;7:25. doi:10.1186/s13613-017-0248-7
8. Delaney L, Currie M, Huang HC, et al. The nocturnal acoustical intensity of the intensive care environment: an observational study. J Intensive Care. 2017;5:41. doi:10.1186/s40560-017-0237-9
9. Chang-Lit W, Loewy J, Fox J, Grabscheid E, Fogel J. Project sleep: the role and effect of a comprehensive, multidisciplinary music therapy quality improvement program. J Sleep Dis Res. 2018;1(2):26–41. doi:10.14302/issn.2574-4518.jsdr-17-1785
10. Canga B, Hahm CL, Luciso D, Grossbard ML, Loewy JV. Environmental music therapy: a pilot study on the effect of music therapy in a chemotherapy infusion suite. Mus Med. 2012;4(4):221–230.
11. Feld B, Born J. Sculpting memory during sleep: concurrent consolidation and forgetting. Curr Opin Neurobiol. 2017;44:20–27. doi:10.1016/j.conb.2017.02.012
12. Grigsby-Toussaint D, Shin JC, Reeves DM, Beattie A, Auguste E, Jean-Louis G. Sleep apps and behavioral constructs: a content analysis. Prev Med Rep. 2017;6:126–129. doi:10.1016/j.pmedr.2017.02.018
13. Stepanski EJ, Wyatt JK. Use of sleep hygiene in the treatment of insomnia. Sleep Med Rev. 2003;7:215–225. doi:10.1053/smrv.2001.0246
14. Lazic SE, Ogilvie RD. Lack of efficacy of music to improve sleep: a polysomnographic and quantitative EEG analysis. Int J Psychophysiol. 2007;63(3):232–239. doi:10.1016/j.ijpsycho.2006.10.004
15. Jespersen KV, Koenig J, Jennum P, Vuust P. Music for insomnia in adults. Cochrane Database Syst Rev. 2015;8. doi:10.1002/14651858.CD010459.pub2
16. Robb SL, Carpenter JS, Burns DS. Reporting guidelines for music-based interventions. J Health Psychol. 2011;16(2):342–352. doi:10.1177/1359105310374781
17. Loewy J, Stewart K, Dassler A-M, Telsey A, Homel P. The effects of music therapy on vital signs, feeding, and sleep in premature infants. Peds. 2013;131(5):902–918. doi:10.1542/peds.2012-1367
18. Loewy J, Hallan C, Friedman E, Martinez C. Sleep/sedation in children undergoing EEG testing: a comparison of chloral hydrate and music therapy. J Perianesth Nurs. 2005;20(5):323–331.
19. Chang ET, Lai HL, Chen PW, Hsieh YM, Lee LH. The effects of music on the sleep quality of adults with chronic insomnia using evidence from polysomnographic and self-reported analysis: a randomized control trial. Int J Nurs Stud. 2012;49(8):921. doi:10.1016/j.ijnurstu.2012.02.019
20. Smith M, McCrae C, Cheung J, et al. Use of actigraphy for the evaluation of sleep disorders and circadian rhythm sleep-wake disorders: an American academy of sleep medicine systematic review, meta-analysis, and GRADE assessment. J Clin Sleep Med. 2018;14(7):1209–1230. doi:10.5664/jcsm.7228
21. Hernández-Ruiz E. Effect of music therapy on the anxiety levels and sleep patterns of abused women in shelters. J Music Ther. 2005;42:140–158. doi:10.1093/jmt/42.2.140
22. Spira AP, Chen-Edinboro LP, Wu M, Yaffe K. Impact of sleep on the risk of cognitive decline and dementia. Current Opin Psych. 2014;27(6):478–483. doi:10.1097/YCO.0000000000000106
23. Nadorff MR, Nazem S, Fiske A. Insomnia symptoms, nightmares, and suicidal ideation in a college student sample. Sleep. 2011;34:93–98. doi:10.1093/sleep/34.1.93
24. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disor. 2011;135(1–3):10–19. doi:10.1016/j.jad.2011.01.011
25. Tan LP. The effects of background music on quality of sleep in elementary school children. J Mus Ther. 2004;41(2):128–150.
26. Wang C-F, Sun Y-L, Zang H-X. Music therapy improves sleep quality in acute and chronic sleep disorders: a meta-analysis of 10 randomized studies. Int J Nurs Stud. 2014;51(1):51–62. doi:10.1016/j.ijnurstu.2013.03.008
27. Chan MF, Chan EA, Mok E. Effects of music on depression and sleep quality in elderly people: a randomized controlled trial. Comp Med East West. 2010;18(3–4):150–159.
28. Lestarini A, Putra KSP. Music therapy on sleep quality in elderly. IOP Conf Ser Mater Sci Eng. 2018;434:012143. doi:10.1088/1757899X/434/1/012143
29. Edinger JD, Means MK, Carney CE, Manber R. Psychological and behavioral treatments for insomnia II: implementation and specific populations. In: Kryger M, Roth T, Dement W, editors. Principles and Practice of Sleep Medicine.
30. Trahan T, Durrant SJ, Müllensiefen D. Williamson VJ. The music that helps people sleep and the reasons they believe it works: a mixed methods analysis of online survey reports. PLoS One. 2018;13(11):e0206531. doi:10.1371/journal.pone.0206531
31. Rossetti A. Towards prescribing music in clinical contexts: more than words. MusMed. 2014;6(2):70–77.
32. Polaner DM, Houck CS, Rockoff MA, et al. Sedation, risk, and safety: do we really have data at last? Pediatrics. 2001;108:1006–1008. doi:10.1542/peds.108.4.1006
33. Musical sedation: Mechanisms of breathing entrainment. In: Azoulay R, Loewy JV (editors). Music, the breath and health: advances in integrative music therapy. New York, NY: Satchnote Press; 2009:228.
34. Zaubler TS, Murphy K, Rizzuto L, et al. Quality improvement and cost savings with multicomponent delirium interventions: replication of the hospital elder life program in a community hospital. Acad Psychosomatic Med. 2013;54:1492–1499.
35. Inouye SK, Baker DI, Fugal P, Bradley EH. Dissemination of the hospital elder life program: implementation, adaptation, and successes. Amer Ger Soc. 2016;54:1492–1499. doi:10.1111/j.1532-5415.2006.00869.x
36. Nagel CL, Markie MB, Richards KC, Taylor JL. Sleep promotion in hospital elders. Med Surg Nurs. 2003;12(5):279–290.
37. LaReau R, Benson L, Watcharotone K. Examining the feasibility of implementing specific nursing interventions to promote sleep in hospitalized elderly patients. Geriatr Nurs (Minneap). 2008;29(3):197–206. doi:10.1016/j.gerinurse.2007.10.020
38. Rostata JR, Dunn M, Phelan G, Braun C, Chiu CT, Reld M. STY6 Rehab Staa. Implementing an Evidence-Based Sleep Protocol to Reduce Falls on an Inpatient Rehab Unit: An Interdisciplinary Approach. New York, NY: Department of Nursing & Patient Care Services Manual, Mount Sinai St. Luke’s; 2015.
39. Alessi CA, Martin JL, Webber AP, Kim EC, Harker JO, Josephson KR. Randomized, controlled trial of a nonpharmacological intervention to improve abnormal sleep/wake patterns in nursing home residents. J Am Geriatr Soc. 2005;53(5):803–810. doi:10.1111/j.1532-5415.2005.53251.x
40. Stewart K, Schneider S. The effect of music therapy on the sound environment in the neonatal intensive care unit: a pilot study. In: Loewy JV, editor. Music Therapy in the Neonatal Intensive Care Unit. New York, NY: Satchnote Press, The Louis Armstrong Center for Music and Medicine; 2000:85–100.
41. Zhang J, Doherty M, Mahoney J. Environmental music in a hospital setting: considerations of music therapists and performing musicians. Mus Med. 2018;10(2):71–79.
42. Rossetti A, Canga B. Environmental music therapy: rationale for ‘multi-individual’ music psychotherapy in modulation of the pain experience. In: Mondanaro JF, Sara AG, editors. Music and Medicine: Integrative Models in the Treatment of Pain. New York, NY: Satchnote Press, The Louis Armstrong Center for Music and Medicine; 2013:451–468.
43. Biglin T, Ma J, Lin Y. Confronting a different great wall: using environmental music therapy to provide psychoemotional support for Asian and Asian-American patients in a radiation oncology waiting room. In: Mondanaro JF, Sara AG, editors. Music and Medicine: Integrative Models in the Treatment of Pain. New York, NY: Satchnote Press, The Louis Armstrong Center for Music and Medicine; 2014:451–468.
44. Xie H, Kang J, Mills GH. Clinical review: the impact of noise on patients’ sleep and the effectiveness of noise reduction strategies in intensive care units. Crit Care. 2009;13(2):208–213. doi:10.1186/cc7154
45. Grandner M, Malhotra A. Sleep as a vital sign: why medical practitioners need to routinely ask their patients about sleep. Sleep Health. 2015;1(1):11–12. doi:10.1016/j.sleh.2014.12.011
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.