Back to Journals » Journal of Pain Research » Volume 19
Musculoskeletal Ultrasound-Guided Micro-Needle-Knife Intervention at the Deep Fascial versus Superficial Fascial Layers in Lateral Epicondylitis Patients: A Randomized Controlled Trial
Authors Zhang W, Zhang J, Hu J, Song J, Feng Y, Ruan C, Du J, Feng P, Liu H ![]()
Received 17 March 2026
Accepted for publication 3 June 2026
Published 12 June 2026 Volume 2026:19 608269
DOI https://doi.org/10.2147/JPR.S608269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Wentao Zhang, Jiaqi Zhang, Jun Hu, Jiacheng Song, Yongjie Feng, Chen Ruan, Jia Du, Peipei Feng, Hao Liu
Department of Acupuncture, Tongde Hospital of Zhejiang Province Affiliated to Zhejiang Chinese Medical University (College of Integrated Traditional Chinese and Western Medicine Clinical Medicine), Hangzhou, People’s Republic of China
Correspondence: Hao Liu, Department of Acupuncture, Tongde Hospital of Zhejiang Province Affiliated to Zhejiang Chinese Medical University (College of Integrated Traditional Chinese and Western Medicine Clinical Medicine), No. 234, Gucui Road, Xihu District, Hangzhou, Zhejiang, People’s Republic of China, Tel +8615868814927, Email [email protected]
Background: Lateral epicondylitis (LE) is a prevalent musculoskeletal disorder causing persistent elbow pain and upper-limb dysfunction. While micro-needle-knife (MNK) therapy has shown promise for musculoskeletal pain, its optimal anatomical target and intervention depth remain poorly defined.
Patients and Methods: 70 participants with unilateral lateral epicondylitis (mean age, 39.91± 12.41 years; 40 women, 57.1%) were randomized 1:1 to receive musculoskeletal ultrasound (MU)-guided micro-needle-knife intervention targeting either the deep fascial (DF) layer or superficial fascial (SF) layer at two anatomically defined forearm interfaces corresponding to LI10 and TE9. Both groups underwent 12 treatment sessions over 4 weeks. The primary outcomes were Visual Analog Scale (VAS) for pain and Pressure Pain Threshold (PPT) assessed at baseline, week 1, 2, 3, 4, and 8. Secondary outcomes included Pain-Free Grip Strength (PFG) and Mayo Elbow Performance Score (MEPS).
Results: The DF group demonstrated significantly greater and earlier reductions in pain compared with the SF group. At week 1, 42.9% of participants in the DF group achieved mild pain levels (VAS ≤ 3), compared with 8.6% in the SF group (P < 0.001). The odds of achieving over 50% pain reduction in VAS pain score were higher in the DF group at both week 4 (OR 3.25, 95% CI: 1.72 to 6.19) and week 8 (OR 2.50, 95% CI: 1.67 to 3.75). Improvements in PPT, PFG, and MEPS were consistently greater in the DF group across all post-treatment time points (all P < 0.001). Specifically, the DF group achieved a median VAS reduction of 3 (2, 4) at week 4, which was significantly larger than the 2 (1, 3) observed in the SF group (P < 0.001) and exceeded the established minimal clinically important difference (MCID) of 1.5 points for LE. No serious adverse events were observed.
Conclusion: Over 8-week follow-up period, musculoskeletal ultrasound-guided MNK targeting the deep fascial layer demonstrated superior efficacy and comparable safety to superficial fascial intervention for LE, supporting anatomically targeted, MU-guided fascial interventions as a promising short-term rehabilitation strategy.
Clinical Trial Registration Number: ITMCTR2025001055.
Keywords: ultrasound imaging, micro-needle-knife, tennis elbow, fascia, randomized controlled trial
Introduction
Lateral epicondylitis (LE) is a common load-related musculoskeletal disorder characterized by lateral elbow pain, reduced grip strength, and impaired upper-limb function.1,2 It affects approximately 1–3% of the general population.3 This condition predominantly affects individuals aged 40–50 years, with an equal gender distribution, and severely impairs patients’ quality of life and work capacity, thereby imposing a substantial social and economic burden.4,5 Although historically described as an inflammatory condition, accumulating evidence indicates that LE is more accurately understood as a degenerative and mechanical disorder.6–9 Repetitive mechanical loading leads to pain-related motor inhibition, reduced load tolerance, and functional limitation, resulting in substantial occupational disability and socioeconomic burden.1,10–13
Non-surgical strategies represent the first-line approach for LE management, typically starting with patient education, activity modification, eccentric exercise training, and bracing.14,15 For patients who fail to respond to these initial measures, second-line options include physical therapy modalities, acupuncture, non-steroidal anti-inflammatory drugs (NSAIDs), and corticosteroid injections.15–17 Among complementary therapies, acupuncture has shown the advantages to effectively alleviate short-term pain,18 providing a safer profile with fewer adverse effects compared to autologous blood injection or NSAIDs.19,20 The small needle knife has also demonstrated promising efficacy in the management of musculoskeletal pain disorders.21,22
Micro-Needle-Knife (MNK) therapy, minimally invasive intervention to deliver anatomically targeted fascial release,23 featuring a diameter that is smaller than the small needle knife, offers a theoretical solution by physically disrupting these adhesions, thereby offering improved safety and precision.24
However, its clinical application lacks standardization, particularly regarding the depth of intervention. Blind needle insertion poses risks to the radial nerve and fails to guarantee precise release of the targeted inter-muscular septa.
To address these gaps, this study integrates Musculoskeletal ultrasound (MU)-guided MNK therapy, aiming to visualize and treat specific anatomical interfaces.25–27 We focus on two strategic coordinates: Shousanli (LI10): Anatomically targeting the inter-muscular septum between the Brachioradialis and the extensor carpi radialis brevis (ECRB). Release here aims to restore independent muscle gliding.28 Sidu (TE9): Anatomically targeting the fascia overlying the Extensor Digiti Minimi (EDM) and Extensor Carpi Ulnaris (ECU). Addressing this often-overlooked ulnar compartment is critical for restoring rotational stability.29
This randomized controlled trial (RCT) compares the efficacy of MU-guided MNK targeting the deep fascial (DF) versus superficial fascial (SF) layer in patients with LE. We hypothesized that MU-guided MNK targeting the deep fascial layer would result in significantly greater and earlier improvements in pain, pressure pain threshold, grip strength, and elbow function compared with superficial fascial intervention in patients with LE.
Materials and Methods
Study Protocol
This single-center, parallel-controlled randomized controlled trial was conducted at Tongde Hospital of Zhejiang Province Affiliated to Zhejiang Chinese Medical University between December 1, 2024, and September 21, 2025. The protocol adhered to the CONSORT guidelines, and written informed consent was obtained from all participants prior to enrollment. Inclusion criteria included: 1) For the diagnosis of LE, two out of the five clinical provocation tests should be provocative on the lateral side of the elbow.30–32 (a) Pain on palpation over lateral epicondylar, (b) pain with stretching or contraction of the wrist extensor muscles, (c) pain during power grip, (d) The Maudsley test is positive: Pain on resisted extension of the third digit; (e)Mills sign is positive: pain upon passive elbow extension with the forearm pronated and wrist flexed; 2) Be aged between 18 and 65 years; 3) Experience elbow pain for a duration of less than six months; 4) Present a tenderness Visual Analogue Scale (VAS) score of ≥ 4 at the lateral humeral epicondyle; 5) Exhibit unilateral elbow involvement; 6) Be capable of cooperating with various examinations related to lateral epicondylitis of the humerus and diligently complete the subjective survey information form; 7) Willingly participate in this trial and provide informed consent. Exclusion criteria included the following: 1) Presence of severe tumorous lesions in vital organs, such as the heart, liver, or kidneys; 2) Pregnancy or breastfeeding; 3) Receipt of physical therapy, acupuncture, needle knife treatment, or non-steroidal anti-inflammatory drug treatment within the past week; 4) Aversion to acupuncture or a tendency to faint during acupuncture; 5) Presence of skin damage or infection in the elbow joint area, history of elbow joint surgery, upper limb deformities, or other neuromusculoskeletal conditions that may affect grip strength; 6) Patients exhibiting poor compliance or unable to complete the entire trial process; 7) With other serious comorbidities, such as heart disease, hypertension, or cerebral infarction.
Randomization and Blinding
This study adopted an single-blind randomized controlled design. A random number table was generated using SPSS 25.0 statistical software, and 70 eligible participants were randomly assigned to either the deep fascia group or the superficial fascia group in a 1: 1 ratio, with 35 participants in each group. To ensure randomization and concealment, project team members developed random allocation cards and sealed them in opaque envelopes. The researchers responsible for recruitment and outcome assessment were blinded to the random sequence allocation. Blinding of participants, outcome assessors, and statisticians was strictly implemented. Due to the specific nature of MNK treatment, blinding the acupuncturists were not feasible, but participants were blinded to the specific intervention depth, and outcome assessors as well as statisticians were blinded to group allocation.
Interventions
All ultrasound-guided procedures were performed using a SonoEye V2 handheld musculoskeletal ultrasound system (Chison Medical Technologies Co., Ltd., Wuxi, China). Both deep fascia group and superficial fascia group were performed by licensed acupuncturists with at least 3 years of treatment experience. During the 4-week treatment period, a total of 12 treatment sessions were carried out, with a treatment frequency of 3 times a week.
Deep Fascia Group
Patients assume either a supine or seated position to fully expose the affected limb. Following routine disinfection of the acupoints, the musculoskeletal ultrasound probe was horizontally positioned over the Shousanli (LI10) and Sidu (TE9) acupoints on the affected forearm. (Figure 1) Careful precautions were taken to avoid the radial artery, vein, and nerve branches. A 0.35×40 mm MNK was then employed for the intervention. At the LI10, the needle was inserted in the direction of the brachioradialis, and 2–3 longitudinal incisions were performed. (Figure 2) After penetrating the deep fascia of the muscle, the needle was retracted to the superficial fascia layer. Subsequently, the MNK orientation was adjusted towards the extensor carpi radialis longus (ECRL) and brevis (ECRB) muscles, and the previous procedure was replicated. Upon needle withdrawal, pressure was applied to achieve hemostasis. At the TE9, the extensor digiti minimi (EDM) and extensor carpi ulnaris (ECU) muscles were sequentially punctured using an identical technique.
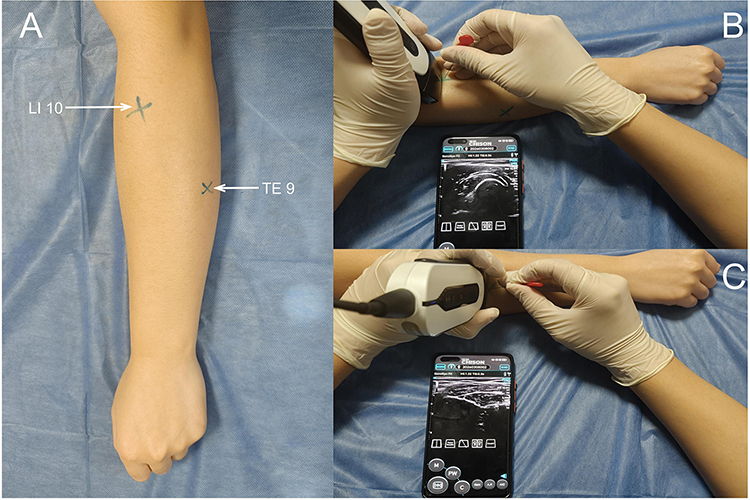 |
Figure 1 Locations of Acupoints and Schematic Diagram of MNK Therapy. (A) Anatomical locations of Shousanli (LI10) and Sidu (TE9) acupoints; (B) Schematic of MNK therapy at LI10; (C) Schematic of MNK therapy at TE9. Abbreviations: LI10, Shousanli; TE9, Sidu. Notes: LI10 is located on the dorsoradial aspect of the forearm, 2 cun below the cubital transverse crease, along the line connecting Yangxi (LI5) and Quchi (LI11). TE9 is located on the dorsal aspect of the forearm, 5 cun below the elbow tip, between the ulna and radius, along the line connecting Yangchi (TE4) and the elbow tip. |
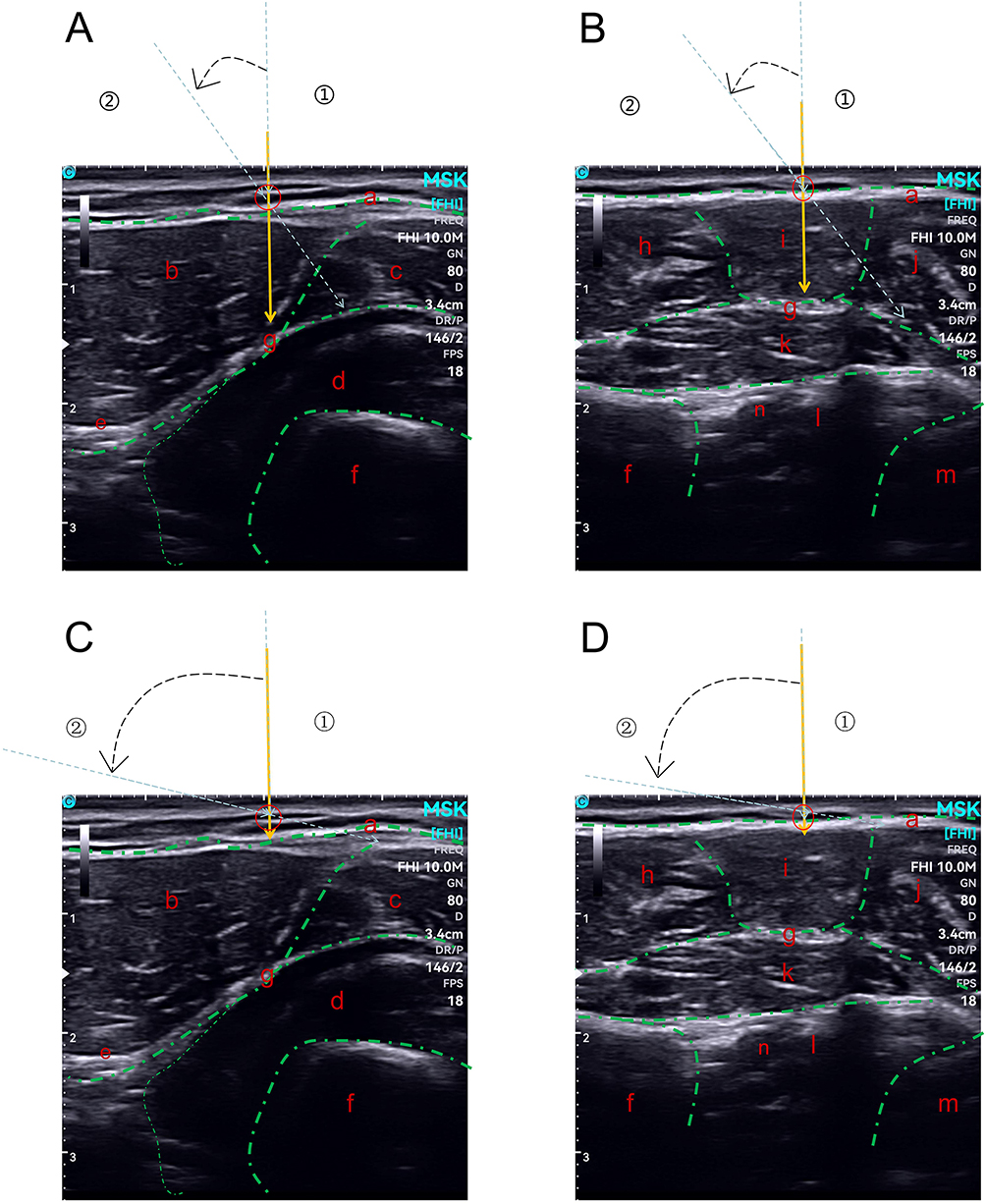 |
Figure 2 Musculoskeletal ultrasonographic images of anatomical structures and MNK intervention procedures. (A and B) LI10 & TE9; DF group: Needle insertion targets the deep fascia layer of the involved muscles; (C and D) LI10 & TE9; SF group: Needle insertion targets the superficial fascia layer without penetrating the deep fascia. Abbreviations: DF, Deep fascia; SF, Superficial Fascia; ECRB, Extensor Carpi Radialis Brevis; ECRL, Extensor Carpi Radialis Longus; MNK, Micro-Needle-Knife. Notes: (a) superficial fascia; (b) brachioradialis; (c) ERCB/ERCL; (d) supinator; (e) superficial branch of the radial nerve; (f) radius; (g) deep fascia; (h) extensor digitorum; (i) extensor digiti minimi; (j) extensor carpi ulnaris; (k) abductor pollicis longus; (l) interosseous membrane; (m) ulna; (n) posterior interosseous artery; ① indicates the initial vertical needle insertion direction (Step 1); ② indicates the adjusted needle insertion direction after angle adjustment (Step 2); Yellow arrows indicate the initial MNK insertion path and depth; blue arrows indicate the adjusted MNK insertion path and depth; black dashed lines between the arrows represent the path of MNK angle adjustment; green dashed lines indicate the muscle contours; red circles indicate the change point. |
Superficial Fascia Group
The operational protocol was consistent with that of the deep fascia group. At the LI10, the MNK was precisely oriented towards the brachioradialis. The MNK was then inserted into the superficial fascia of the brachioradialis, carefully avoiding penetrating the fascial layer and stimulating the deep fascia of the muscle.
Subsequently, the MNK was retracted to the subcutaneous level. After reorienting, the MNK was inserted into the superficial fascia of the extensor carpi radialis longus. At the TE9, the superficial fascia of the extensor digiti minimi and extensor carpi ulnaris muscles were punctured in a sequential manner following the same approach as described previously.
Outcome Measurements
Primary Outcomes
The primary outcomes were patient-reported pain intensity and pressure pain threshold (PPT) at the lateral epicondyle. Visual Analog Scale (VAS): A 10-point horizontal scale where 0 indicates no pain and 10 indicates the worst imaginable pain. The minimally clinically important difference (MCID) for VAS in lateral epicondylitis was defined as 1.5 points.33 Pressure Pain Threshold (PPT): An objective measure of peripheral sensitization. Using a digital algometer (FDX-25), force was applied vertically to the lateral epicondyle until the first sensation of pain. The measurement was repeated three times, and the average value was taken. Assessed at Baseline, Week 1, 2, 3, 4, and Week 8.
Secondary Outcomes
Secondary outcomes included Mayo Elbow Performance Score (MEPS) and Pain-Free Grip Strength (PFG) on baseline, week 4 (post-treatment), and week 8 (follow-up). MEPS: A comprehensive 100-point scale evaluating pain (45 pts), motion (20 pts), stability (10 pts), and daily function (25 pts). Clinical outcomes were graded according to standard categories: excellent (90–100 pts), good (75–89 ps), fair (60–74 pts), and poor (0–59 pts).34 The MCID for MEPS was defined as 15 points.35 PFG: A direct biomechanical indicator of ECRB tendon integrity. Measured with a Jamar® Plus+ dynamometer. The measurement was repeated three times after short rests, and the average value was taken.
For outcome analysis, clinically meaningful improvement was defined as ≥30%, ≥50% reduction in VAS pain score and ≥30%, ≥50% increase in PPT, MEPS and PFG value from baseline.
Adverse Events
Adverse events (AEs) were monitored and recorded at each treatment session and follow-up visit. Meanwhile, any serious adverse events (SAEs) were required to be reported to the principal investigator within 24 hours of occurrence. All adverse events were reviewed by an independent clinician.
Statistical Analysis
Sample size was calculated based on detecting a clinically meaningful between-group difference of 1.5 points in VAS score reduction at week 4, which corresponds to the established MCID for LE.33 Using a two-sided significance level of α = 0.05 and 80% statistical power, a total of 62 participants (31 per group) were required. Accounting for a 10% dropout rate, the final sample size was set at 70 participants (35 per group). All analyses were done according to the intention-to-treat principle.
Data analysis was conducted using SPSS version 25.0. The data were analyzed by two researchers who were not involved in the patients’ treatment and blinded to the grouping allocation. All randomized participants were included in the primary intention-to-treat analysis regardless of treatment completion or follow-up status. Little’s Missing Completely at Random (MCAR) test was used to formally determine the missing data pattern. For data confirmed to be Missing Completely at Random, Multiple Imputation by Chained Equations (MICE) was performed to generate 5 imputed datasets, and pooled statistical estimates were calculated using Rubin’s rules. For all repeated-measures outcome measures, a 2 (group: deep fascia [DF] vs superficial fascia [SF]) × k (time point) mixed-design repeated-measures analysis of variance (RM-ANOVA) was first conducted. Mauchly’s test of sphericity was used to assess the assumption of sphericity for RM-ANOVA. If sphericity was violated, the Greenhouse-Geisser correction was applied, for repeated measures, the Friedman M test, was employed to assess the overall within-group time effect across all assessment points. For comparisons of baseline characteristics and inter-group differences (Tables 1 and 2), categorical data were presented as frequencies and compared using the chi-square test. For continuous data, normality was assessed with the Shapiro–Wilk’s test, followed by evaluation of variance homogeneity via Levene’s test: normally distributed continuous data were reported as mean ± standard deviation (SD) and compared using the independent-samples t-test; for data with unequal variances (including PPT data at baseline), the Welch-corrected t-test was applied; non-normally distributed continuous data were presented as median, interquartile range (IQR) and compared using the Mann–Whitney U-test. Within-group comparisons (Table 3) were performed using the paired-samples t-test for normally distributed paired differences or the Wilcoxon signed-rank test for non-normally distributed data. The Bonferroni correction was applied to all post-hoc pairwise comparisons following significant RM-ANOVA effects, for VAS and PPT (6 time points: baseline, week 1, 2, 3, 4, and 8), significance was adjusted for 5 comparisons (adjusted α = 0.01); for MEPS and PFG (3 time points: baseline, week 4, and 8), significance was adjusted for 2 comparisons (adjusted α = 0.025). Effect sizes were estimated using odds ratios (ORs) with 95% confidence intervals (CIs) for categorical outcomes. All statistical tests were two-sided, with P < 0.05 for unadjusted baseline comparisons and adjusted P less than the corresponding α threshold considered statistically significant.
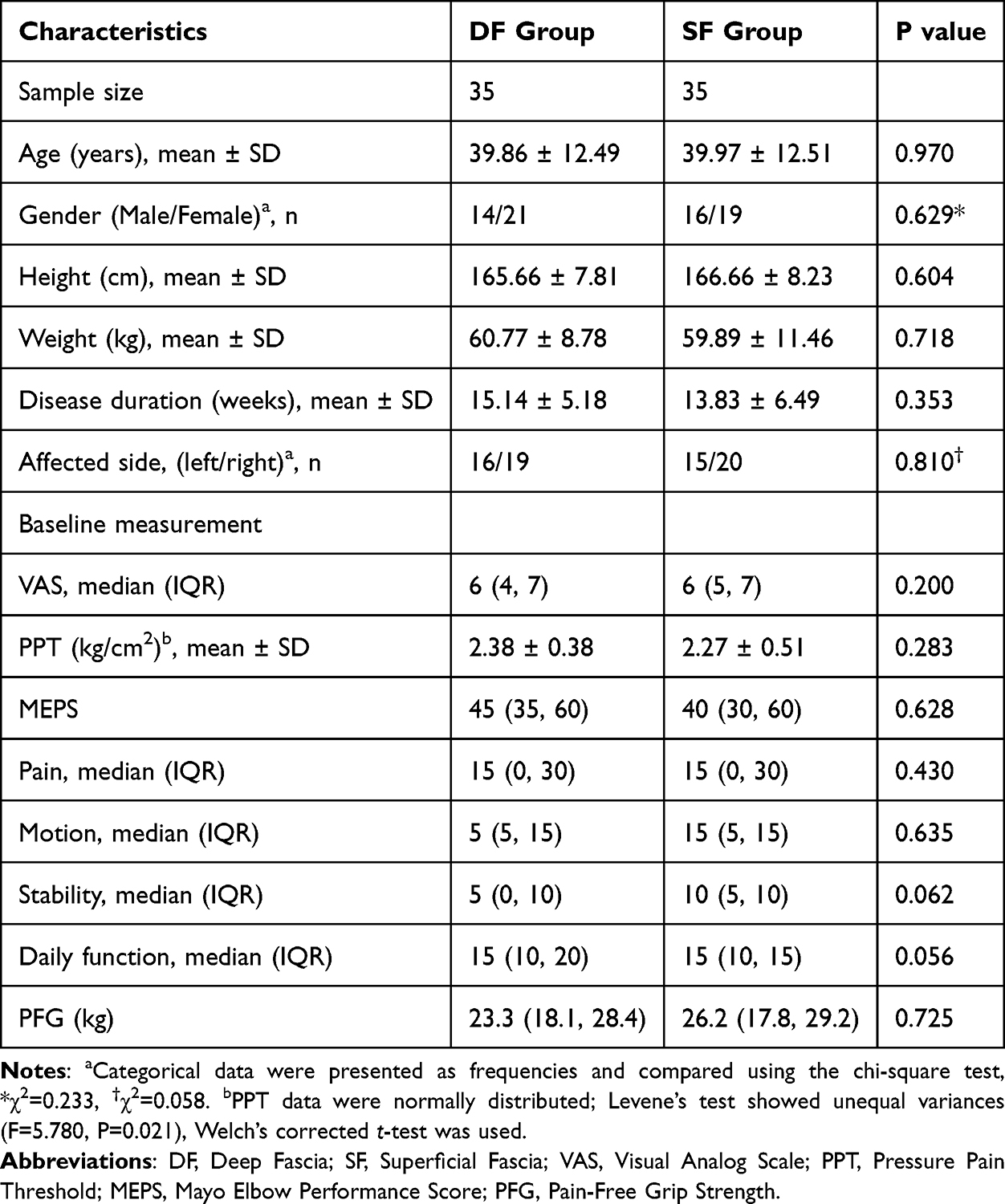 |
Table 1 Baseline Demographic and Clinical Characteristics of Participants |
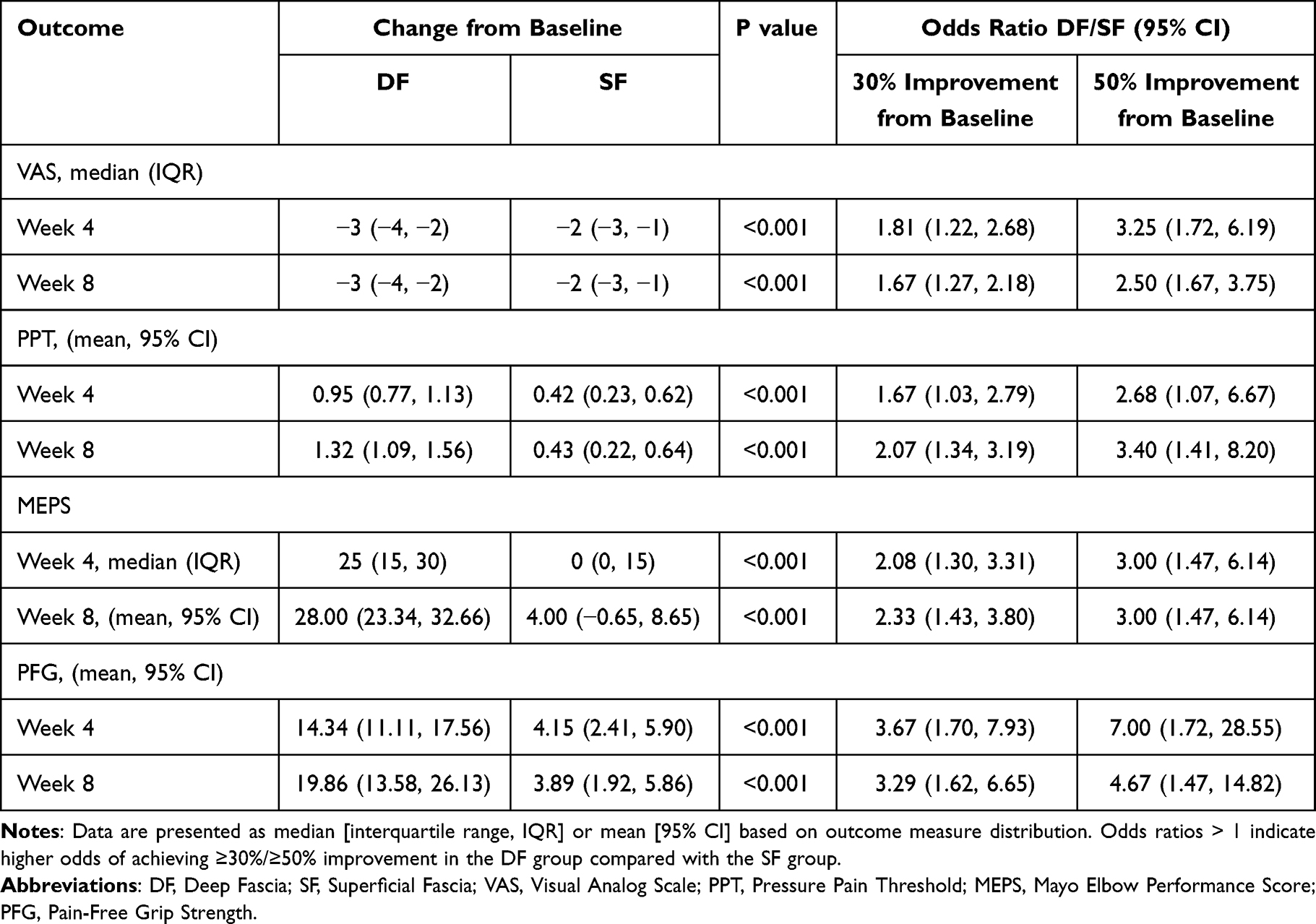 |
Table 2 Baseline-to-Time Point Changes and ORs for ≥30% and ≥50% Clinical Improvement at Post-Treatment and Follow-Up |
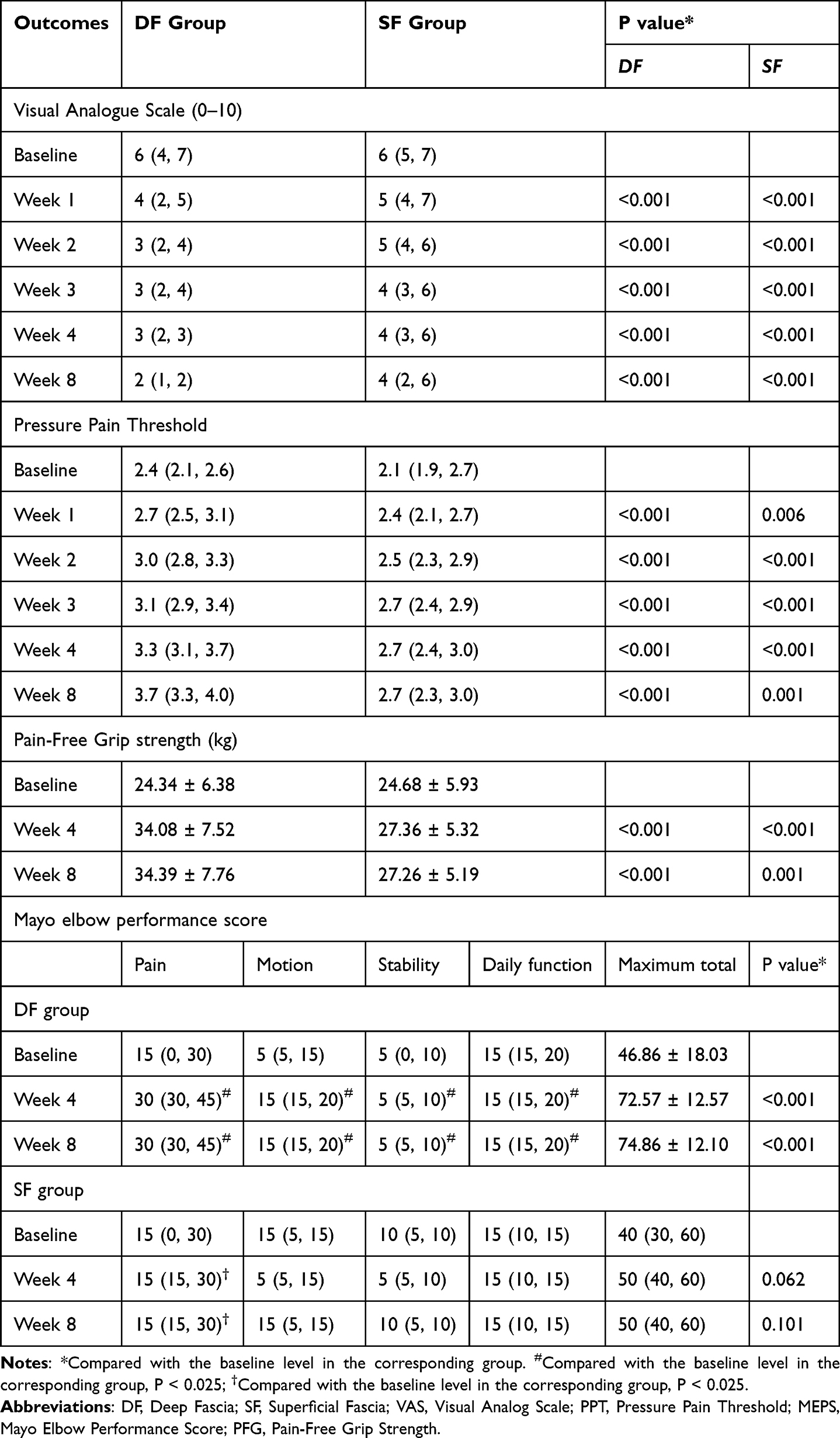 |
Table 3 Within-Group Comparisons of Primary and Secondary Outcomes Over Time |
Results
Patients
A total of 113 qualified individuals were screened between December 1, 2024, and September 21, 2025, and 70 were randomized 1:1 to the DF group (n = 35) or the SF group (n = 35). All 70 participants (age, 39.91±12.41 years; 40 women [57.1%]) completed the intervention protocol, 97.1% (68/70) completed the 8-week follow-up. One participant in the DF group completed the 4-week treatment but was lost to follow-up during the subsequent follow-up period, and one participant in the SF group withdrew from the study due to work schedule after completing 2 weeks of treatment. (Figure 3) There were no significant differences in demographic and clinical characteristics between the two groups at baseline (all P > 0.05), as shown in Table 1.
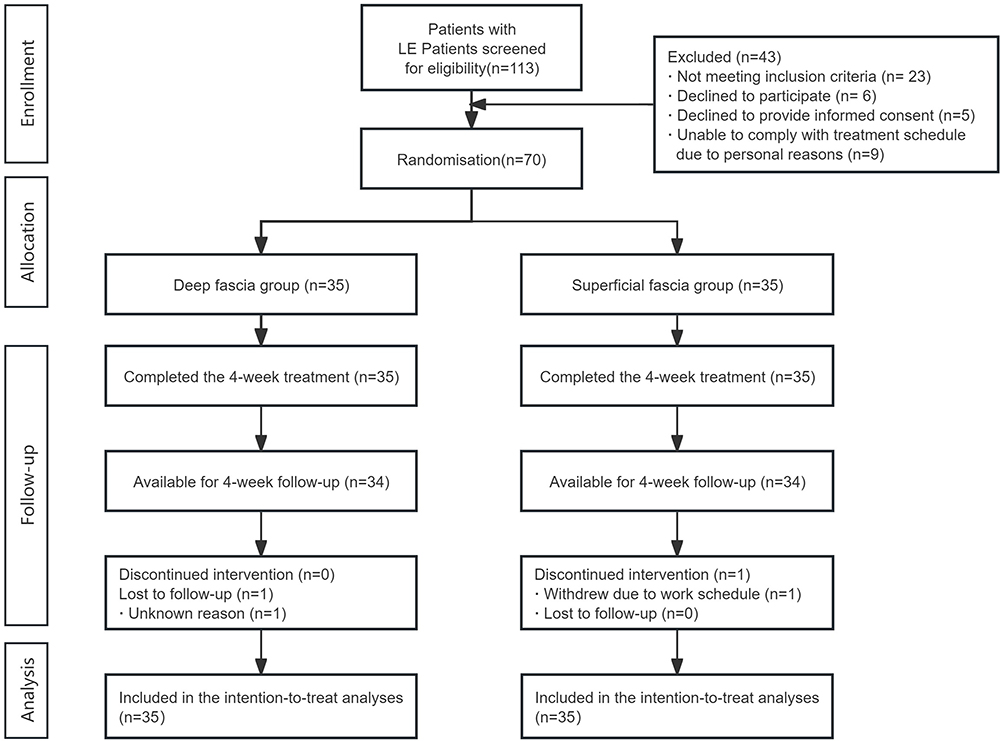 |
Figure 3 Trial flow chart. Abbreviation: LE, Lateral epicondylitis. |
Primary Outcomes
Compared with the baseline levels, the pain intensity of patients in both groups decreased at week 4 and week 8, with a significantly greater reduction in the DF group than in the SF group (Table 3). According to the VAS scores, the DF group showed a median decrease of 3 from the baseline level to post-treatment, while the SF group showed a median decrease of 2, with a statistically significant difference (P < 0.001). The odds of achieving clinically meaningful pain relief (≥50% reduction in VAS) were 3.25-fold higher (95% CI, 1.72 to 6.19) in the DF group at Week 4 compared to the SF group (Table 2). Moreover, 42.86% of patients in the DF group achieved a VAS score of 3 points (mild pain) after 1 week of treatment, which was significantly higher than the 8.57% in the SF group. (Figure 4) At the end of the follow-up, 94.29% of patients in the DF group had mild pain, compared with 42.86% in the SF group.
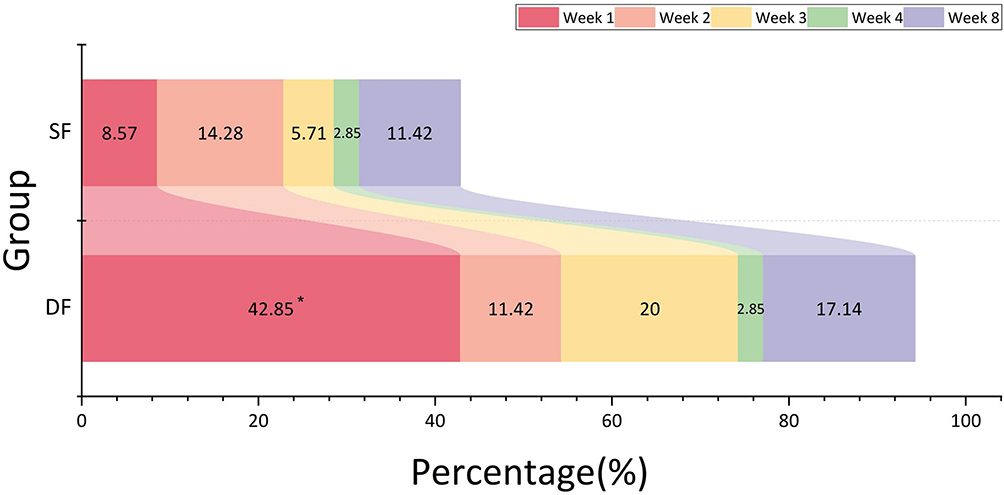 |
Figure 4 Proportion of Participants Achieving Mild Pain or Below (VAS ≤ 3) Across Treatment Week 1, 2, 3, 4, and 8 by Group. Statistical comparisons between groups were performed using Pearson’s chi-square test for weeks 1 and 8, continuity-corrected chi-square test for weeks 2 and 3, and Fisher’s exact test for week 4. *p < 0.05 indicates a statistically significant difference between groups. Abbreviations: DF, Deep Fascia; SF, Superficial Fascia; VAS, Visual Analog Scale. |
At baseline, there was no significant difference in PPT between the DF group and the SF group (P = 0.283). Throughout the treatment and follow-up periods, the DF group maintained a consistent upward trend in PPT, with significant increases relative to baseline observed at both Week 1 to 4 and Week 8. (Figure 5) In contrast, while the SF group also showed modest improvements in PPT, compared with the baseline, the PPT values only increased by 0.42 (95% CI: 0.23 to 0.62) kg/cm2 and 0.43 (95% CI: 0.22 to 0.64) kg/cm2 at week 4 and week 8, while the DF group increased by 0.95 kg/cm2 and 1.32 kg/cm2. For the proportion of patients achieving 30% improvement in PFG from baseline, the odds ratio (DF/SF) was 2.68 (95% CI: 1.07 to 6.67) at Week 4 and 3.40 (95% CI: 1.41 to 8.20) at week 8 for 50% improvement in PPT from baseline.
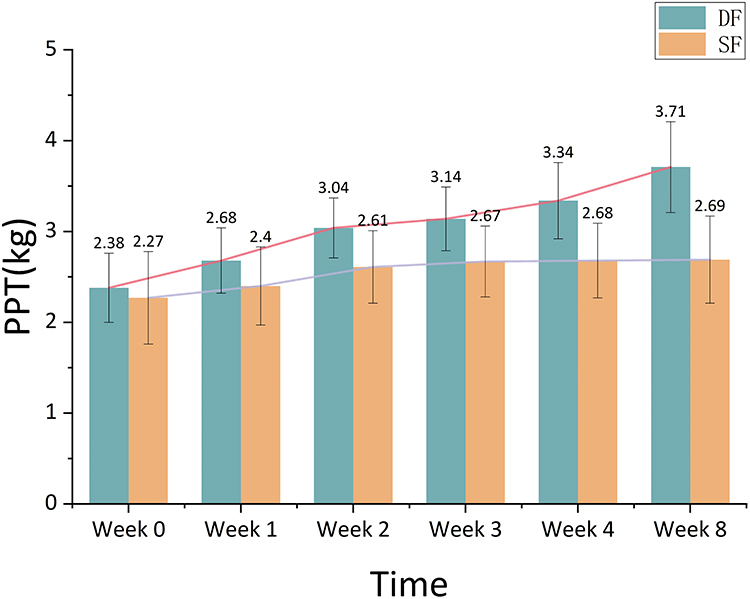 |
Figure 5 Measurements of PPT Values at Different Time Points in the Two Groups During the Study Period; Data are Presented as Mean ± SD. Abbreviations: DF, Deep Fascia; SF, Superficial Fascia; PPT, Pressure Pain Threshold. |
Secondary Outcomes
Compared with baseline, the MEPS in the DF group increased significantly at both week 4 and week 8, with scores consistently higher than those in the SF group. In contrast, the SF group showed no significant change in MEPS throughout the treatment period (P = 0.062). Notably, the DF group demonstrated improvements in both pain relief and motor function. At week 4, the DF group exhibited a mean increase of 25 in MEPS compared with baseline. Clinical grading of MEPS revealed that 17% of patients in the DF group achieved “excellent” outcomes (scores 90–100) at week 4, with 46% of patients in this group attaining overall “good” (75–89) or better results, which were significantly higher than the corresponding proportions in the SF group (Figure 6).
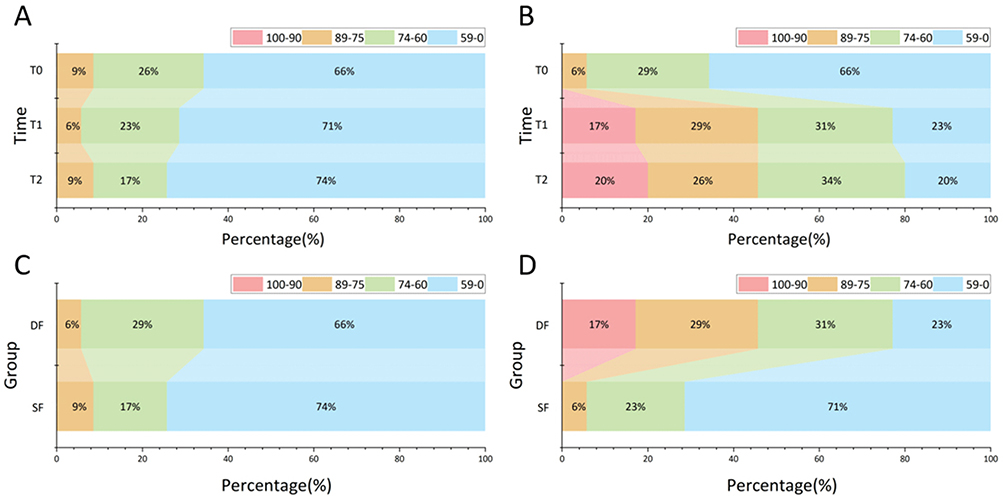 |
Figure 6 Distribution of MEPS Score Ranges Across Time and Groups. (A) Distribution of MEPS score ranges (90–100, 75–89, 60–74, 0–59) in the DF group at baseline (T0), post-treatment (T1, Week 4)`, and follow-up (T2, Week 8). (B) Distribution of MEPS score ranges in the SF group at T0, T1, and T2. (C) Baseline comparison of MEPS score ranges between DF and SF groups. (D) Week 4 comparison of MEPS score ranges between DF and SF groups. Abbreviations: DF, Deep Fascia; SF, Superficial Fascia; MEPS, Mayo Elbow Performance Score. |
The DF group exhibited a significant and statistically significant improvement in PFG from baseline to post-treatment and the follow-up. Specifically, PFG increased from 24.34 ± 6.38 kg at Week 0 to 34.08 ± 7.52 kg at Week 4 and 34.39 ± 7.76 kg at week 8 (P < 0.001). By contrast, the SF group exhibited only minimal alterations in PFG throughout the treatment course with values remaining at 24.68 ± 5.93 kg at Week 0, 27.36 ± 5.32 kg at Week 4 (P < 0.001), and 27.26 ± 5.19 kg at the follow-up (P = 0.001). The proportion of patients in the DF group achieving over 50% clinical improvement was higher than that in the SF group for both MEPS and PFG: For MEPS, the proportion in the DF group was 3.00-fold that of the SF group at both Week 4 and Week 8 (95% CI: 1.47 to 6.14); for PFG, the odds ratio (DF/SF) was 7.00 (95% CI: 1.72 to 28.55) at week 4 and 4.67 (95% CI: 1.47 to 14.82) at Week 8.
Adverse Event
AEs were monitored meticulously. The incidence of AEs was low and similar between groups (DF: 8.6%, SF: 5.7%), 2 in DF group and 2 in SF group were reported transient post-needling soreness, 1 in DF group was reported minor subcutaneous ecchymosis. No nerve injuries, infections, or tendon ruptures occurred, confirming the safety profile of the ultrasound-guided technique.
Discussion
LE is increasingly recognized as a degenerative and mechanical disorder characterized by impaired force transmission across the forearm extensor muscle compartments, rather than an isolated inflammatory condition of the common extensor tendon.36–38 In this randomized controlled trial, MU-guided MNK intervention targeting the deep fascial layer was associated with greater and earlier improvements in pain, pressure pain sensitivity, grip strength, and elbow function compared with superficially targeted intervention in patients with LE.
The median VAS reduction of 3 points in the DF group and 2 points in the SF group both exceeded the established MCID of 1.5 points for LE, confirming the clinical relevance of these pain relief effects. Deep fascia-targeted MNK therapy afforded rapid, clinically meaningful pain relief. A significantly higher proportion of patients in the DF group achieved mild pain (VAS ≤ 3) as early as week 1, and this advantage persisted through the 8-week follow-up, with far more DF patients maintaining mild pain at the final assessment. The superior analgesic effect of DF intervention cannot be attributed solely to adhesion release; it may instead reflect more effective modulation of mechanically sensitive nociceptors within deep fascial compartments and intermuscular septa.39,40 Deep fascia is richly innervated and plays a critical role in force transmission and proprioceptive signaling.41 Targeted mechanical stimulation at this level may therefore alter local nociceptive input and reduce pain-related movement inhibition, facilitating earlier functional engagement of the extensor musculature.42–44 The magnitude of VAS pain reduction at 8 weeks in our study was comparable to that reported by Seyed et al, who demonstrated similar analgesic efficacy with ultrasound-guided 1% ropivacaine injection for lateral epicondylitis.45
Improvements in PPT further confirmed the superiority of DF targeting. While both groups showed some increase in PPT over time, the DF group demonstrated significantly greater and sustained improvements from week 2 onward (Figure 5). The temporal dissociation observed—early reductions in subjective pain followed by delayed increases in PPT—may indicate that symptomatic relief precedes structural or neurophysiological adaptation within the involved tissues. This pattern aligns with current tendinopathy and myofascial pain models, where reductions in peripheral sensitization typically lag behind subjective pain relief.46,47 Beyond pain relief, DF-targeted MNK therapy promoted comprehensive recovery of elbow function and pain-free grip strength. These functional benefits likely stem from improved load distribution across extensor compartments after deep fascial release. The deep fascia serves as a critical interface for force transmission between muscle fibers and adjacent compartments,39 and mechanical dysfunction at this level amplifies strain on the extensor carpi radialis brevis during gripping and wrist extension.48,49 MU-guided DF intervention may therefore enhance force transfer efficiency and improve functional performance.50,51
Importantly, no activity restrictions were imposed during treatment, and participants continued their usual daily and occupational activities. This supports the clinical feasibility of this function-oriented intervention, which may facilitate earlier return to work for patients with lateral elbow tendinopathy. In contrast, SF intervention produced only modest and limited improvements in pain and grip strength. This partial benefit may relate to central pain modulation via the anterior cingulate cortex, but it failed to restore normal elbow biomechanics and thus did not yield significant functional improvement.52,53 MU guidance enhanced both the precision and safety of DF targeting by enabling real-time visualization of neurovascular structures at LI10 and TE9, allowing accurate needle placement while avoiding complications. Adverse events were mild, transient, and comparable between groups, with a safety profile similar to conventional acupuncture for LE.54
The findings of this study have important clinical implications. For patients with LE who fail to respond to first-line conservative treatments such as education and eccentric exercise, ultrasound-guided MNK targeting the deep fascial layer offers a safe and effective second-line intervention option. The rapid onset of analgesia allows patients to resume functional activities earlier, which may reduce the socioeconomic burden associated with this condition. Furthermore, the use of musculoskeletal ultrasound guidance enhances the precision of the intervention and minimizes the risk of complications, making it a valuable addition to the armamentarium of clinicians managing musculoskeletal pain disorders.
This study presents promising evidence from one of the first randomized controlled trials evaluating MU-guided MNK therapy targeting distinct superficial and deep fascial layers for LE. The integration of real-time sonographic visualization with layered fascial intervention supports the potential for precise anatomical targeting and provides preliminary mechanistic insights into soft tissue pathology, which may inform the development of tailored treatment approaches for clinical practice.
Limitations
This study has several limitations that should be acknowledged. First, this was a single-center trial with a relatively small sample size of 35 participants per group, which may overestimate the true treatment effect in broader clinical practice. Although the observed effect sizes were large and statistically significant, our findings should be interpreted with caution until validated in larger, multicenter cohorts. Second, the follow-up period was limited to 8 weeks, and the long-term sustainability of the observed pain relief and functional improvements remains unknown. Many interventions for lateral epicondylitis show early benefit that attenuates over months, so future studies with 6–12 month follow-up are needed to determine whether the benefits of deep fascial targeting persist over time. Third, due to the nature of the intervention, blinding of treating acupuncturists was not feasible, which may have introduced potential performance bias. However, we mitigated this risk by strictly blinding outcome assessors and statisticians to group allocation throughout the study period.
Future research should address the limitations of this study by conducting larger, multicenter randomized controlled trials with longer follow-up periods to confirm the long-term efficacy of DF-targeted MNK therapy. Additional studies are also needed to compare the efficacy of MNK with other minimally invasive interventions such as platelet-rich plasma injections, to determine the optimal number of treatment sessions, and to identify patient subgroups that are most likely to benefit from this approach.
Conclusion
Within the context of this 8-week, single-center randomized controlled trial, our findings demonstrate that musculoskeletal ultrasound-guided MNK targeting the deep fascial layer is a similarly safe and significantly more effective treatment for lateral epicondylitis compared with superficial fascial intervention. The integration of real-time sonographic visualization provides precise anatomical targeting and preliminary mechanistic insights into soft tissue pathology, which may inform the development of tailored treatment approaches for clinical practice and potentially reduce the socioeconomic burden associated with LE, although this requires confirmation in future large-scale studies.
Abbreviations
LE, Lateral epicondylitis; MNK, Micro-Needle-Knife; MU, Musculoskeletal ultrasound; DF, Deep fascia; SF, Superficial fascia; VAS, Visual Analog Scale; PPT, Pressure Pain Threshold; PFG, Pain-Free Grip Strength; MEPS, Mayo Elbow Performance Score; MCID, Minimal clinically important difference; RCT, Randomized controlled trial; ECRB, Extensor carpi radialis brevis; EDM, Extensor Digiti Minimi; ECU, Extensor Carpi Ulnaris; ECRL, Extensor carpi radialis longus; RM-ANOVA, Repeated-measures analysis of variance; IQR, Interquartile range; OR, Odds ratio; CI, Confidence interval; SAE, Serious adverse event; LI10, Shousanli; TE9, Sidu.
Data Sharing Statement
The datasets generated and analysed during the current study are available from the corresponding author Hao Liu ([email protected]) on reasonable request.
Ethics Approval and Consent to Participate
This study protocol was formally approved on November 22, 2024, by the Medical Ethics Committee of Tongde Hospital of Zhejiang Province (Approval No.: 2024-254 (K)), all participants provided written informed consent prior to enrollment, and the entire study was conducted in strict accordance with the ethical principles of the Declaration of Helsinki. The trial was registered at the International Traditional Medicine Clinical Trial Registry (https://itmctr.ccebtcm.org.cn/, registration number: ITMCTR2025001055), with full registration completed on March 20, 2025. Of note, a brief pre-enrollment feasibility verification phase was conducted after ethical approval to standardize the MU-guided intervention procedure; participants in this phase were not included in the final statistical analysis. The full study protocol was locked before formal cohort enrollment, and the registered protocol was fully consistent with the implemented protocol, with no modifications made after formal recruitment.
Acknowledgments
We acknowledge all study personnel and participants for their contributions to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Department of State Administration of Traditional Chinese Medicine-Key Laboratory Project Co-constructed by Zhejiang Provincial Administration of Traditional Chinese Medicine (NO. GZY-ZJ-SY-2402); National Leading Medical Specialty Development Project-Department of Geriatrics, Tongde Hospital of Zhejiang Province (Project Number: [2024]90662); Zhejiang Provincial Alliance of Traditional Chinese Medicine Advantage Specialty for Geriatric Diseases (Project Number: [2024]10).
Disclosure
We declare that all authors have no financial or other conflicts of interest related to this article.
References
1. Perveen W, Anwar S, Hashmi R, et al. Effects of extracorporeal shockwave therapy versus ultrasonic therapy and deep friction massage in the management of lateral epicondylitis: a randomized clinical trial. Sci Rep. 2024;14(1):16535. doi:10.1038/s41598-024-67313-1
2. Cutts S, Gangoo S, Modi N, Pasapula C. Tennis elbow: a clinical review article. J Orthopaedics. 2020;17:203–15. doi:10.1016/j.jor.2019.08.005
3. Zhou Y, Guo Y, Zhou R, Wu P, Liang F, Yang Z. Effectiveness of acupuncture for lateral epicondylitis: a systematic review and meta-analysis of randomized controlled trials. Pain Res Manag. 2020;2020:8506591. doi:10.1155/2020/8506591
4. Speers CJ, Bhogal GS, Collins R. Lateral elbow tendinosis: a review of diagnosis and management in general practice. British J General Pract. 2018;68(676):548–549. doi:10.3399/bjgp18X699725
5. Dunning J, Mourad F, Bliton P, et al. Percutaneous tendon dry needling and thrust manipulation as an adjunct to multimodal physical therapy in patients with lateral elbow tendinopathy: a multicenter randomized clinical trial. Clin Rehab. 2024;38(8):1063–1079. doi:10.1177/02692155241249968
6. Ma KL, Wang HQ. Management of lateral epicondylitis: a narrative literature review. Pain Res Manag. 2020;2020:6965381. doi:10.1155/2020/6965381
7. Goislard de Monsabert B, Herbaut A, Cartier T, Vigouroux L. Electromyography-informed musculoskeletal modeling provides new insight into hand tendon forces during tennis forehand. Scand J Med Sci Sports. 2023;33(10):1958–1975. doi:10.1111/sms.14434
8. Bordachar D. Lateral epicondylalgia: a primary nervous system disorder. Med Hypotheses. 2019;123:101–109. doi:10.1016/j.mehy.2019.01.009
9. Stegink-Jansen CW, Bynum JG, Lambropoulos AL, Patterson RM, Cowan AC. Lateral epicondylosis: a literature review to link pathology and tendon function to tissue-level treatment and ergonomic interventions. J Hand Ther. 2021;34(2):263–297. doi:10.1016/j.jht.2021.05.005
10. Viswas R, Ramachandran R, Korde Anantkumar P. Comparison of effectiveness of supervised exercise program and Cyriax physiotherapy in patients with tennis elbow (lateral epicondylitis): a randomized clinical trial. Scientific World J. 2012;2012:939645. doi:10.1100/2012/939645
11. Akbar H, Akbar S, Saddique MN, Sarfraz MS. Prevalence of lateral epicondylitis among housewives in Lahore: a cross-sectional study. BMC Musculoskeletal Disord. 2024;25(1):815. doi:10.1186/s12891-024-07889-x
12. Cancela-Cilleruelo I, Rodríguez-Jiménez J, Fernández-de-Las-Peñas C, Cleland JA, Arias-Buría JL. Widespread pressure pain hyperalgesia is not associated with morphological changes of the wrist extensor tendon in unilateral lateral epicondylalgia: a case-control study. Phys Ther. 2024;104(9). doi:10.1093/ptj/pzae075
13. Bretschneider SF, Los FS, Eygendaal D, Kuijer P, van der Molen HF. Work-relatedness of lateral epicondylitis: systematic review including meta-analysis and GRADE work-relatedness of lateral epicondylitis. Am J Ind Med. 2022;65(1):41–50. doi:10.1002/ajim.23303
14. Uttamchandani SR, Phansopkar P. Efficacy of PowerBall versus mulligan mobilization with movement on pain and function in patients with lateral epicondylitis: a randomized clinical trial. Cureus. 2024;16(3):e56444. doi:10.7759/cureus.56444
15. Zhang Z, Zhang Z, Yao P. Advancements in physical factor therapy and traditional chinese physiotherapy for rehabilitation of tennis elbow. Physiotherapy Res Int. 2025;30(3):e70079. doi:10.1002/pri.70079
16. Ahmed AF, Rayyan R, Zikria BA, Salameh M. Lateral epicondylitis of the elbow: an up-to-date review of management. European J Orthopaedic Surg Traumatol. 2023;33(2):201–206. doi:10.1007/s00590-021-03181-z
17. Urits I, Markel M, Choi P, et al. Minimally invasive treatment of lateral epicondylitis. Best Pract Res Clin Anaesth. 2020;34(3):583–602. doi:10.1016/j.bpa.2020.08.004
18. Green S, Buchbinder R, Barnsley L, et al. Acupuncture for lateral elbow pain. Cochrane Database Syst Rev. 2002;2002(1):Cd003527. doi:10.1002/14651858.Cd003527
19. Güngör E, Karakuzu Güngör Z. Comparison of the efficacy of corticosteroid, dry needling, and PRP application in lateral epicondylitis. European J Orthopaedic Surg Traumatol. 2022;32(8):1569–1575. doi:10.1007/s00590-021-03138-2
20. Uygur E, Aktaş B, Özkut A, Erinç S, Yilmazoglu EG. Dry needling in lateral epicondylitis: a prospective controlled study. Int Orthopaedics. 2017;41(11):2321–2325. doi:10.1007/s00264-017-3604-1
21. Zhao Y, Fang W, Qin WK. [Thinking of therapeutic mechanism of small knife needle in treating closed myofascitis]. Zhongguo Zhen Jiu. 2014;34(9):907–909. Chinese
22. Zhu F, Chen Y, Zhu Y, Bai Z, Yan H. Acupuncture therapy for extremity musculoskeletal pain: a clinically focused evidence synthesis with therapeutic implications. J Pain Res. 2025;18:5541–5554. doi:10.2147/jpr.S551446
23. Feng C, Yao J, Xie Y, et al. Small needle-knife versus extracorporeal shock wave therapy for the treatment of plantar fasciitis: a systematic review and meta-analysis. Heliyon. 2024;10(1):e24229. doi:10.1016/j.heliyon.2024.e24229
24. Lu SW, Lang BX, Liu JN, et al. Comparative efficacy of micro-needle-knife therapy and acupuncture in acute ankle sprains: a randomized controlled trial. Med Sci Monitor. 2024;30:e944157. doi:10.12659/msm.944157
25. Wu YY, He FD, Chen K, Quan JR, Guo XY. Comparison of the clinical effectiveness of ultrasound-guided corticosteroid injection with and without needle release of the A1 pulley in treating trigger finger. J X-Ray Sci Technol. 2020;28(3):573–581. doi:10.3233/xst-190620
26. Wijntjes J, van Alfen N. Muscle ultrasound: present state and future opportunities. Muscle Nerve. 2021;63(4):455–466. doi:10.1002/mus.27081
27. Jiang L, Liu H, Li H, Jiang J, Liu X. Ultrasound-guided needle-knife for De Quervain’s disease: a protocol for systematic review and meta-analysis. Medicine. 2021;100(14):e24877. doi:10.1097/md.0000000000024877
28. Pirri C, Guidolin D, Fede C, Macchi V, De Caro R, Stecco C. Ultrasound imaging of brachial and antebrachial fasciae. Diagnostics. 2021;11(12):2261. doi:10.3390/diagnostics11122261
29. Besnard M, Marteau E, Laulan J, Bacle G. Tendon transfers for radial nerve palsy with extensor carpi ulnaris revival: technique and results. Orthopaedics Traumatol Surg Res. 2020;106(2):307–310. doi:10.1016/j.otsr.2019.11.026
30. Sveinall H, Brox JI, Engebretsen KB, Hoksrud AF, Røe C, Johnsen MB. Heavy slow resistance training, radial extracorporeal shock wave therapy or advice for patients with tennis elbow in the Norwegian secondary care: a randomised controlled feasibility trial. BMJ open. 2024;14(12):e085916. doi:10.1136/bmjopen-2024-085916
31. Lucado AM, Day JM, Vincent JI, et al. Lateral elbow pain and muscle function impairments. J Orthopaedic Sports Phys Ther. 2022;52(12):Cpg1–cpg111. doi:10.2519/jospt.2022.0302
32. Di Filippo L, Vincenzi S, Pennella D, Maselli F. Treatment, diagnostic criteria and variability of terminology for lateral elbow pain. Findings Overview System Rev Healthc. 2022;10(6):1095. doi:10.3390/healthcare10061095
33. Hao Q, Devji T, Zeraatkar D, et al. Minimal important differences for improvement in shoulder condition patient-reported outcomes: a systematic review to inform a BMJ rapid recommendation. BMJ Open. 2019;9(2):e028777. doi:10.1136/bmjopen-2018-028777
34. Ha C, Cho W, Hong IT, Park J, Ahn W, Han SH. Effect of repetitive corticosteroid injection on tennis elbow surgery. Am J Sports Med. 2023;51(7):1886–1894. doi:10.1177/03635465231166397
35. Sveinall H, Brox JI, Engebretsen KB, et al. Measurement properties of core outcomes in patients with tennis elbow. Shoulder Elbow. 2025:17585732251344264. doi:10.1177/17585732251344264
36. Landis J, Keselman I, Murphy CN. Comparison of electromyographic (EMG) activity of selected forearm muscles during low grade resistance therapeutic exercises in individuals diagnosed with lateral epicondylitis. Work. 2005;24(1):85–91.
37. Bal E, Cetin O. Demonstrating the relationship of ultrasonographic parameters with disease activity and pain in lateral epicondylitis. Medicine. 2023;102(40):e35499. doi:10.1097/md.0000000000035499
38. Bazancir Z, Fırat T. A potential factor in the pathophysiology of lateral epicondylitis: the long sarcomere length of the extensor carpi radialis brevis muscle and implications for physiotherapy. Med Hypotheses. 2019;130:109278. doi:10.1016/j.mehy.2019.109278
39. Caroccia B, Caputo I, Bertoldi G, et al. Angiotensin II activates yes-associated protein (YAP) in fibroblast promoting deep fascia remodeling. Int J Mol Sci. 2025;26(22):11105. doi:10.3390/ijms262211105
40. Pirri C, Petrelli L, Guidolin D, et al. Myofascial junction: emerging insights into the connection between deep/muscular fascia and muscle. Clin Anatomy. 2024;37(5):534–545. doi:10.1002/ca.24148
41. Slater AM, Barclay SJ, Granfar RMS, Pratt RL. Fascia as a regulatory system in health and disease. Front Neurol. 2024;15:1458385. doi:10.3389/fneur.2024.1458385
42. Guo S, Liu D, Yang Y, Hu Z. Clinical efficacy of small needle knife therapy on stage I-II frozen shoulder. J Visualized Experim. 2023;(201). doi:10.3791/65904
43. Zhu J, Zheng Z, Liu Y, et al. The effects of small-needle-knife therapy on pain and mobility from knee osteoarthritis: a pilot randomized-controlled study. Clin Rehab. 2020;34(12):1497–1505. doi:10.1177/0269215520938852
44. Schleip R, Gabbiani G, Wilke J, et al. Fascia is able to actively contract and may thereby influence musculoskeletal dynamics: a histochemical and mechanographic investigation. Front Physiol. 2019;10:336. doi:10.3389/fphys.2019.00336
45. Raeissadat SA, Khavari Ardestani D, Mousavikhah SE, et al. Ultrasound-guided injection strategies for lateral epicondylitis: a multicenter randomized comparison of corticosteroid, platelet-rich plasma, and ozone. Future Sci OA. 2026;12(1):2644326. doi:10.1080/20565623.2026.2644326
46. Cakar A, Gozlu OD. Comparing autologous blood, corticosteroid, and a combined injection of both for treating lateral epicondylitis: a randomized clinical trial. J Orthopaedics Traumatol. 2024;25(1):34. doi:10.1186/s10195-024-00772-4
47. Zhu P, Tang P, Su J, et al. Comparison of extracorporeal shockwave therapy, ultrasound therapy, and corticosteroid injections for treatment of lateral epicondylitis: an umbrella review of meta-analyses. J Orthopaedics Traumatol. 2025;26(1):55. doi:10.1186/s10195-025-00871-w
48. Shirato R, Aoki M, Iba K, et al. Effect of wrist and finger flexion in relation to strain on the tendon origin of the extensor carpi radialis brevis: a cadaveric study simulating stretching exercises. Clin Biomechanics. 2017;49:1–7. doi:10.1016/j.clinbiomech.2017.08.008
49. Meunier M. Lateral epicondylitis/extensor tendon injury. Clin Sports Med. 2020;39(3):657–660. doi:10.1016/j.csm.2020.03.001
50. Manickaraj N, Bisset LM, Kavanagh JJ. Lateral epicondylalgia exhibits adaptive muscle activation strategies based on wrist posture and levels of grip force: a case-control study. J Musculoskeletal Neuronal Interact. 2018;18(3):323–332.
51. Wilke J, Schleip R, Yucesoy CA, Banzer W. Not merely a protective packing organ? A review of fascia and its force transmission capacity. J Applied Physiol. 2018;124(1):234–244. doi:10.1152/japplphysiol.00565.2017
52. Wang Y, Xu J, Zhang Q, et al. Immediate analgesic effect of acupuncture in patients with primary dysmenorrhea: a fMRI study. Front Neurosci. 2021;15:647667. doi:10.3389/fnins.2021.647667
53. Journée SH, Mathis VP, Fillinger C, Veinante P, Yalcin I. Janus effect of the anterior cingulate cortex: pain and emotion. Neurosci Biobehav Rev. 2023;153:105362. doi:10.1016/j.neubiorev.2023.105362
54. Giovanardi CM, Gonzalez-Lorenzo M, Poini A, et al. Acupuncture as an alternative or in addition to conventional treatment for chronic non-specific low back pain: a systematic review and meta-analysis. Integrat Med Res. 2023;12(3):100972. doi:10.1016/j.imr.2023.100972
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.