Back to Journals » Journal of Pain Research » Volume 19
Musculoskeletal Pain Among University Faculty: A Cross-Sectional Study of Prevalence, Determinants, and Associations with Work Performance and Occupational Stress
Authors Elkholi SM ![]() , Alqabbani S
, Alqabbani S ![]() , Hakami W, Althukair M, Aldhahi MI
, Hakami W, Althukair M, Aldhahi MI ![]()
Received 19 October 2025
Accepted for publication 6 February 2026
Published 21 February 2026 Volume 2026:19 575383
DOI https://doi.org/10.2147/JPR.S575383
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Safaa M Elkholi, Samiah Alqabbani, Wesal Hakami, Monirah Althukair, Monira I Aldhahi
Department of Rehabilitation Sciences, College of Health and Rehabilitation Sciences, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia
Correspondence: Safaa M Elkholi, Department of Rehabilitation Sciences, College of Health and Rehabilitation Sciences, Princess Nourah bint Abdulrahman University, P.O. Box 84428, Riyadh, 11671, Saudi Arabia, Email [email protected]; [email protected]
Background and Objectives: Faculty members are considered highly exposed to work-related injuries such as work-related stress (WRS) and work-related musculoskeletal disorders. This study aimed to investigate the prevalence of musculoskeletal pain (MSP) among faculty members and explore its association with work performance, occupational factors and WRS.
Methods: A cross-sectional study conducted between September 2023 and August 2024 and enrolled 369 faculty members from various universities who completed a self-administered online questionnaire. Musculoskeletal pain was evaluated with the Nordic Musculoskeletal Questionnaire (NMQ), psychological stress with the Workplace Stress Scale (WSS), and work performance—covering absenteeism, presenteeism, and functional capacity—with the WHO Health and Work Performance Questionnaire (WHO-HPQ). Binary logistic regression and multiple linear regression were used to identify predictors of pain and work performance outcomes.
Results: A total of 92.6% of participants reported experiencing pain in at least one body region annually, and 74% reported pain weekly, with 64.4% experiencing pain in three or more regions. The most commonly affected areas were the shoulders at 69.1%, the neck at 66.9%, and the lower back at 59.3%. Psychological stress levels were highest among those with lower limb pain and among participants with multisite involvement. MSP was associated with reduced work functioning and presenteeism, but not absenteeism. Higher stress, uncomfortable posture, female gender, obesity, and repetitive movements were significant predictors of MSP. Stress and lower limb pain predicted impaired work functioning.
Conclusion: Musculoskeletal pain and psychological stress were highly prevalent among academic faculty and were associated with reduced work functioning and productivity. These findings highlight the need for targeted ergonomic interventions and stress management strategies to promote health and maintain performance in academic work settings.
Keywords: musculoskeletal disorders, pain, psychological stress, productivity, academicians
Introduction
According to the International Classification of Functioning, Disability and Health framework, musculoskeletal pain (MSP) is identified as an impairment of body function that can be linked to activity limitations and participation restrictions.1 The MSP is a widespread medical condition and a predominant occupational health concern on a global scale, with lifetime prevalence estimates among academic personnel in developed countries ranging from 47% to 85%.2–5 Diminished work performance and career progression have been documented among individuals experiencing such pain and psychosocial factors may further amplify its severity and functional impact.3–5
Although the occupational burden of MSP among clinicians is well documented, academic faculty are exposed to a distinct constellation of risk factors.6–8 These include prolonged computer use during course preparation and research activities, sustained static postures while lecturing or supervising laboratory sessions, repetitive fine-motor tasks such as grading or data entry, and the psychosocial strain of simultaneously meeting teaching, clinical, and scholarly obligations.3–5 The mechanisms underlying musculoskeletal pain involve a cascade of biomechanical, physiological, and neuroplastic processes. Biomechanically, prolonged static postures and repetitive movements sustained during occupational tasks lead to continuous muscle contraction, impairing local blood flow and causing ischemia. This results in the accumulation of metabolic by-products such as lactic acid, which lower tissue pH and activate nociceptors—specialized sensory nerve endings sensitive to mechanical deformation, inflammation.4 Over time, these stressors induce muscle fatigue, microscopic tissue damage (microtrauma), and inflammation, sensitizing peripheral nociceptors and amplifying pain. In chronic cases, central sensitization occurs in the spinal cord and brain, where repeated nociceptive input lowers pain thresholds, expands receptive fields, and integrates psychosocial factors to perpetuate pain independently of ongoing tissue damage9,10 (Volcheck et al, 2023) (Ibrahim et al, 2024).
The most frequently reported areas of musculoskeletal pain among university faculty include the neck (up to 41.5% in some studies).11 Followed by low back (up to 40.3%),3,4,12 then the shoulder and upper back,3,4 and wrist and hands, especially with increased computer use or repetitive tasks.13 These exposures, coupled with the psychosocial demands may create a vulnerability to MSP that is currently under-studied. Previous studies have identified MSP as a multifactorial condition;14 thus, there is a need to conduct exhaustive studies to shed light on its possible contributors. Although demographic factors have been frequently investigated, fewer studies expound upon occupational factors such as posture, physical workload, and administrative tasks, despite their presumed contribution to MSP. WRS has been shown to negatively impact the quality of life, and may exacerbate musculoskeletal symptoms, increasing the risk of functional limitations and long-term disabilities.6,15,16 Academic faculty can develop effective prevention and intervention strategies by having a comprehensive understanding of both occupational and psychosocial aspects.
Occupational epidemiology suggests that physical workload; years of professional experience, ergonomic setup, and perceived psychological stress each contribute independently to the development and persistence of MSP.6,8 Yet the relative weight of these factors within academic faculty settings, particularly in relation to productivity, presenteeism, and absenteeism, remains insufficiently explored. Understanding how pain in specific anatomical regions (eg, spine, lower limb, or upper limb) impairs day-to-day work performance is therefore essential for designing targeted preventive strategies. Although cross-sectional designs do not permit causal inference, it is necessary to estimate disease prevalence and patterns of association particularly in underrepresented occupational populations. Given the relatively scarce epidemiological data on musculoskeletal pain and its occupational correlates related to academic faculty, cross-sectional investigations are a necessary underpinning to guide longitudinal and interventional studies. Therefore, this study aimed to assess the prevalence and anatomical distribution of MSP among university faculty and to assess the predictive effect of occupational and psychological factors on pain presence and work performance outcomes. This study aims to bridge a significant gap in occupational health research, provide insights for evidence-based ergonomic and wellness strategies, and ultimately contribute to a healthier and more efficient academic workforce. Based on the existing literature and the objectives of the present study, it was hypothesized that musculoskeletal pain is highly prevalent among university faculty, with the neck, low back, and upper limb regions being the most frequently affected anatomical sites. It was hypothesized that musculoskeletal pain among university faculty is significantly associated with demographic characteristics and work-related variables, including years of professional experience, teaching, practical, and administrative workloads, as well as class size and prolonged or non-neutral working postures. It was further hypothesized that higher It is further hypothesized that increased perceived psychological stress is itself positively associated with the experience of musculoskeletal pain in general.
Materials and Methods
Study Design and Setting
This cross-sectional study was conducted among faculty members from various universities. Inclusion criteria require participants to have at least one year of experience in their current academic position or a comparable role, along with a self-reported history of work-related MSP, psychological stress, or both. Faculty were excluded if they, were currently pregnant, or had experienced a recent history of fractures or neuromuscular problems at the time of data collection.
Sample Size Calculation
A convenience sampling technique was employed, and the required sample size was estimated to be 323 participants using an online calculator, with parameters set at a 5% margin of error and a 95% confidence level. The population proportion was assumed to be 70%, based on previous literature reporting similar prevalence rates of MSP among university teaching staff.17
Data Collection Instrument
Data were collected using a self-administered questionnaire distributed electronically via Google Forms. The questionnaire comprised sections on demographics and occupational characteristics, commonly adopted work postures, and three standardized scales assessing musculoskeletal pain, psychological stress, and work performance.
Demographic, Occupational Characteristics and Work Positions
Participants reported their gender, age, Body Mass Index (BMI) which was calculated using self-reported height and weight, academic rank, years of experience, class size, teaching load, and whether they held administrative duties. They were also asked about routine work postures, including sitting, standing, trunk rotation, repetitive movements, lifting, and sustained uncomfortable positions.
Nordic Musculoskeletal Questionnaire (NMQ)
Musculoskeletal pain was evaluated using the Nordic Musculoskeletal Questionnaire (NMQ). Developed by Kuorinka et al under the guidance of the Nordic Council of Ministers, the NMQ is a standardized and validated tool widely used in occupational health research to assess the prevalence and impact of musculoskeletal disorders across various work environments.16 It includes a body diagram identifying nine anatomical regions: neck, shoulders, elbows, hands/wrists, upper back, lower back, hips/thighs, knees, and ankles/feet.18
The questionnaire captures the occurrence of pain or discomfort over both 12-month and 7-day recall periods, enabling the differentiation between chronic and acute symptoms. Additionally, it includes questions related to functional limitations, such as whether the reported pain interfered with daily activities, required medical consultation, or resulted in taking medication. Additionally, it assessed the frequency of pain occurrences. Its reliability and applicability across occupational groups make it a robust instrument for identifying musculoskeletal risks and evaluating their functional impact.19 For analytical purposes, reported pain sites were further grouped into three main anatomical regions: (1) Spinal pain, which included pain in the neck, upper back, and lower back; (2) Upper limb pain, comprising the shoulder, elbow, and hand/wrist; and (3) Lower limb pain, encompassing the hip, knee, foot, and ankle.
Workplace Stress Scale (WSS)
Psychological stress was assessed using the Workplace Stress Scale (WSS), developed by Marlin and the American Institute of Stress.20 The WSS consists of eight items, each rated on a five-point Likert scale ranging from “never” (1) to “very often” (5). It is designed to measure the frequency of stress-related thoughts and feelings specific to the workplace context. The total score ranges from 8 to 40, with higher scores indicating greater perceived stress. Previous studies have established the WSS as a reliable and valid instrument for occupational stress evaluation across various professional populations.21,22
World Health Organization Health and Work Performance Questionnaire (WHO-HPQ)
Work functioning and productivity were assessed using the World Health Organization Health and Work Performance Questionnaire (WHO-HPQ): Clinical Trials Baseline Version, a validated instrument developed in accordance with the International Classification of Functioning, Disability, and Health (ICF). The WHO-HPQ is designed to quantify the impact of physical and mental health on job performance, absenteeism, and presenteeism in the workplace.23 It has demonstrated strong psychometric properties and has been validated across diverse populations, including those with and without chronic health conditions.24 The 7-day version, used in this study, is optimized for clinical trials and short-term recall, offering a reliable and standardized framework for evaluating work-related outcomes over the past week.
Health-related absenteeism was assessed based on the number of full workdays missed due to physical or mental health problems during the past seven days (Item A6a). Presenteeism was evaluated using three self-report items: perceived performance of coworkers (Item A10), self-rated actual performance during days worked (Item A11), and usual performance (Item A12). Two indices of presenteeism were derived: absolute presenteeism, calculated by multiplying the self-rated performance score (A11) by 10, yielding a value from 0 to 100, with higher scores indicating greater productivity; and relative presenteeism, computed as the ratio of usual performance (A12) to the perceived average performance of coworkers (A10). Work functioning was evaluated through seven items (A9a–A9g) reflecting difficulties in attention, physical and emotional stamina, clarity of thought, and task completion. Each item was rated on a 5-point Likert scale ranging from “all of the time” to “none of the time.” One item (A9a) was reverse-coded, and a total score was derived to reflect overall functional limitations, with lower scores indicating greater impairment.
Ethical Consideration
Participants received the English-language questionnaire electronically. Clear instructions were provided, and a contact number was made available for support. Informed consent was obtained prior to data collection by selecting “Agree” on the first page of the questionnaire. The study protocol was approved by the Institutional Review Board at Princess Nourah bint Abdulrahman University (IRB Number: 23–0572, dated August 06, 2023).
Statistical Analysis
All statistical analyses were conducted using IBM SPSS Statistics in version 31. Descriptive statistics were used to summarize participant characteristics, MSP status, workplace stress scores, and work performance outcomes. Categorical variables were reported as frequencies and percentages. Sample sizes varied slightly across items due to partial non-response; valid percentages are reported to ensure interpretive accuracy. Continuous variables were assessed for normality using the Shapiro–Wilk test, histograms, and Q–Q plots. As continuous variables were not normally distributed, they were summarized using medians and interquartile ranges (IQR), and non-parametric statistical tests were applied.
Associations were examined using Pearson’s chi-square test, with effect size evaluated through the Phi coefficient (φ). The strength of association was interpreted as follows: negligible (>0), weak (>.05), moderate (>.10), strong (>.15), and very strong (>.25).25 Given multiple bivariate comparisons, chi-square analyses were considered exploratory and interpreted cautiously. When significant associations were found, odds ratios (OR) and their 95% confidence intervals (CI) were reported. For relationships involving a categorical and a continuous variable, Eta was used as the measure of association, ranging from 0 to 1. Values between 0 and 0.1 indicated minimal association, 0.1 to 0.3 weak, 0.3 to 0.5 moderate, and above 0.5 indicated a strong association.25 Group comparisons for continuous outcomes across two or more categorical groups were performed using the Mann–Whitney U-test.
Binary logistic regression was employed to identify independent predictors of MSP presence. MSP was defined as a composite variable derived from nine body regions assessed using the standardized Nordic Musculoskeletal Questionnaire. These regions were grouped into three categories: (1) upper limbs (shoulder, elbow, wrist/hand), (2) lower limbs (hip, knee, ankle/foot), and (3) spinal region (neck, upper back, lower back). Pain in any site within a group, reported in the past 7 days, was coded as the presence of pain in that area. For continuous dependent variables, a general linear model was used to evaluate the effects of multiple predictors, based on the assumption that the standardized residuals were normally distributed. A p-value less than 0.05 was considered statistically significant.
Results
Participants Demographic and Occupational Characteristics
A total of 369 faculty members participated in the study, and their details are presented in Table 1. The participants had a median age of 40 years, with an interquartile range of 12.5 years (33.75–46.25). Over half of the participants were female (64.5%), while the remaining 35.5% were male. Based on BMI classification, 30.1% had a normal weight, 38.7% were overweight, and 28.4% were classified as obese. Regarding academic ranks, assistant professors represented the most prominent category, while the majority had teaching experience between 11–20 years, as shown in the table.
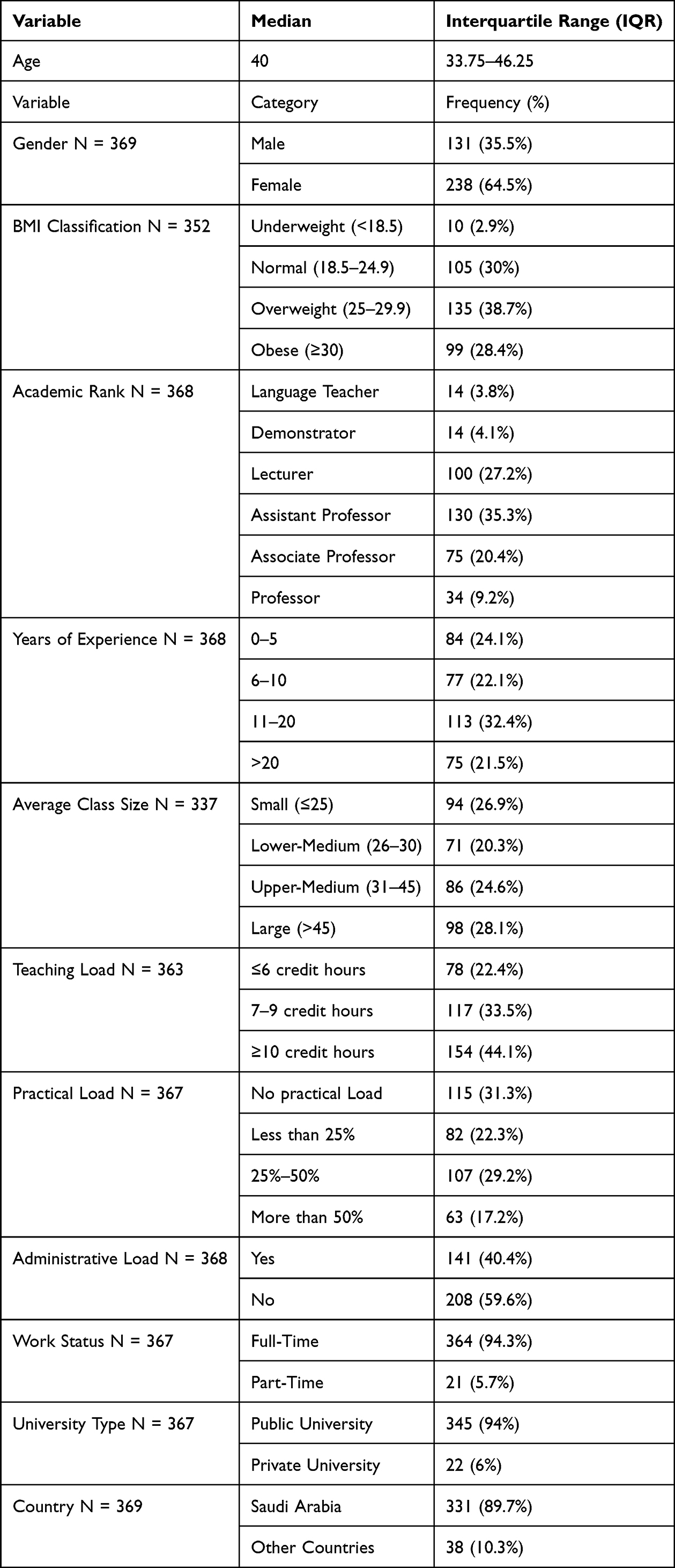 |
Table 1 Demographic and Occupational Characteristics of the Sample (N = 369) |
The highest proportion of participants had a teaching load of ≥10 credit hours, followed by those teaching 7–9 credit hours. With regard to class size, responses were fairly evenly distributed, with 28.1% reporting large class sizes (>45 students). Administrative responsibilities were reported by 40.4% of participants. Nearly all respondents were full-time faculty (94.3%), and most were employed at public universities (94%). A large majority (89.7%) were working in Saudi Arabia, with 10.3% from other countries.
Prevalence and Distribution of Musculoskeletal Pain
Musculoskeletal pain was highly prevalent in the sample. A total of 92.6% (N = 323/349) of participants reported experiencing pain over the past 12 months, and 74% (N = 259/350) reported pain within the past 7 days. In contrast, only 7.4% of the sample were completely symptom-free during the past year. In the 7-day recall period, 40.3% of respondents reported pain in three or more sites, and 14.8% reported involvement in five or more regions. Only 26.0% of participants reported no pain during the previous week. A full summary of the number of pain sites across both time frames is provided in Table 2.
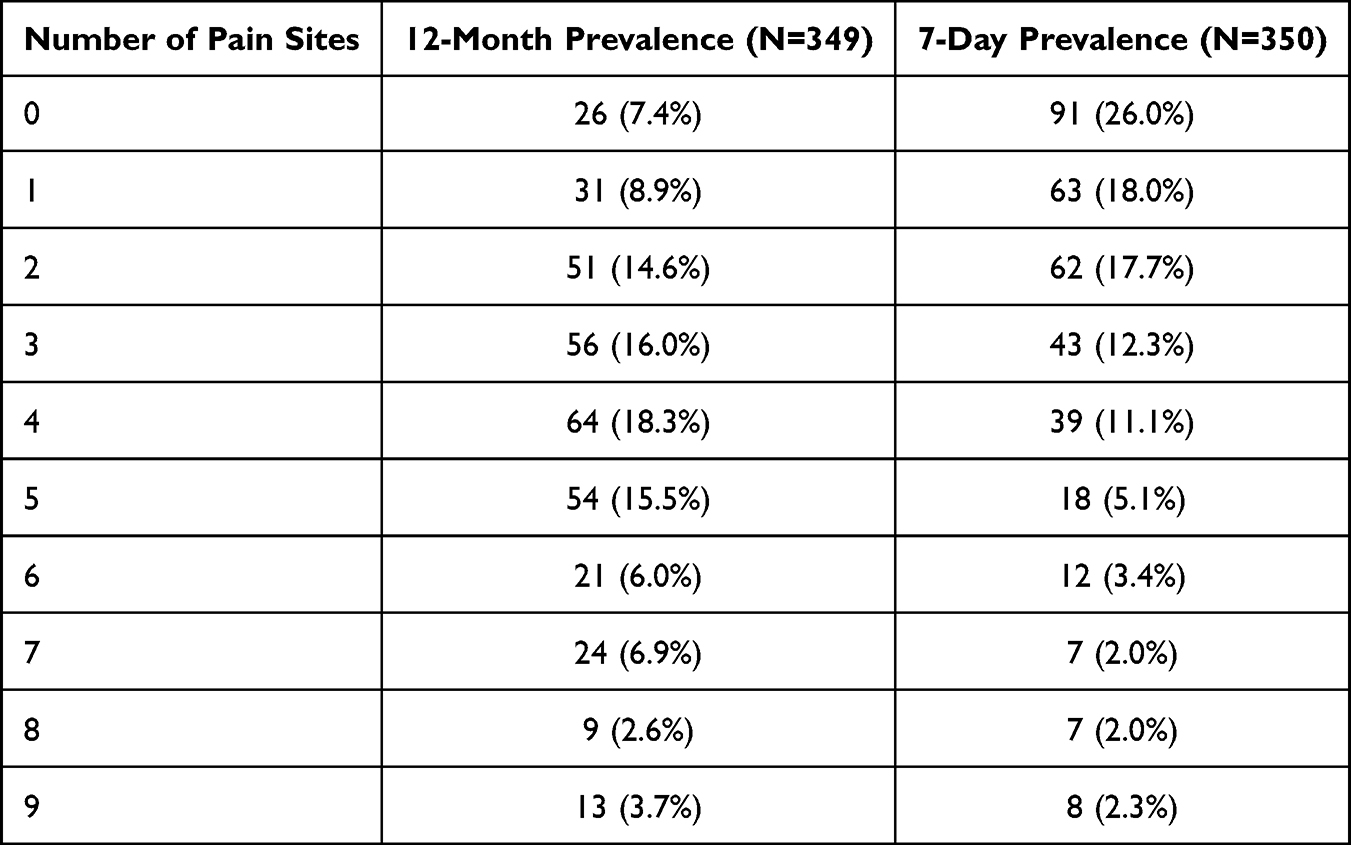 |
Table 2 Frequency Distribution of Pain Site Over Annual and Weekly Timeframes |
Anatomical Distribution of Musculoskeletal Pain
A comprehensive summary of prevalence, activity-related limitations, healthcare engagement, and recent symptom experiences across all nine anatomical regions in addition to main body areas is presented in Table 3. The shoulder and neck emerged as the most frequently affected anatomical regions, with reported 12-month prevalence rates of 69.1% and 66.9%, respectively. The neck and shoulder driving the highest rates of weekly pain, functional interference, and healthcare/medication use. Low-back pain followed at 59.3% (weekly 38.8%), with functional limits in 27.5%.
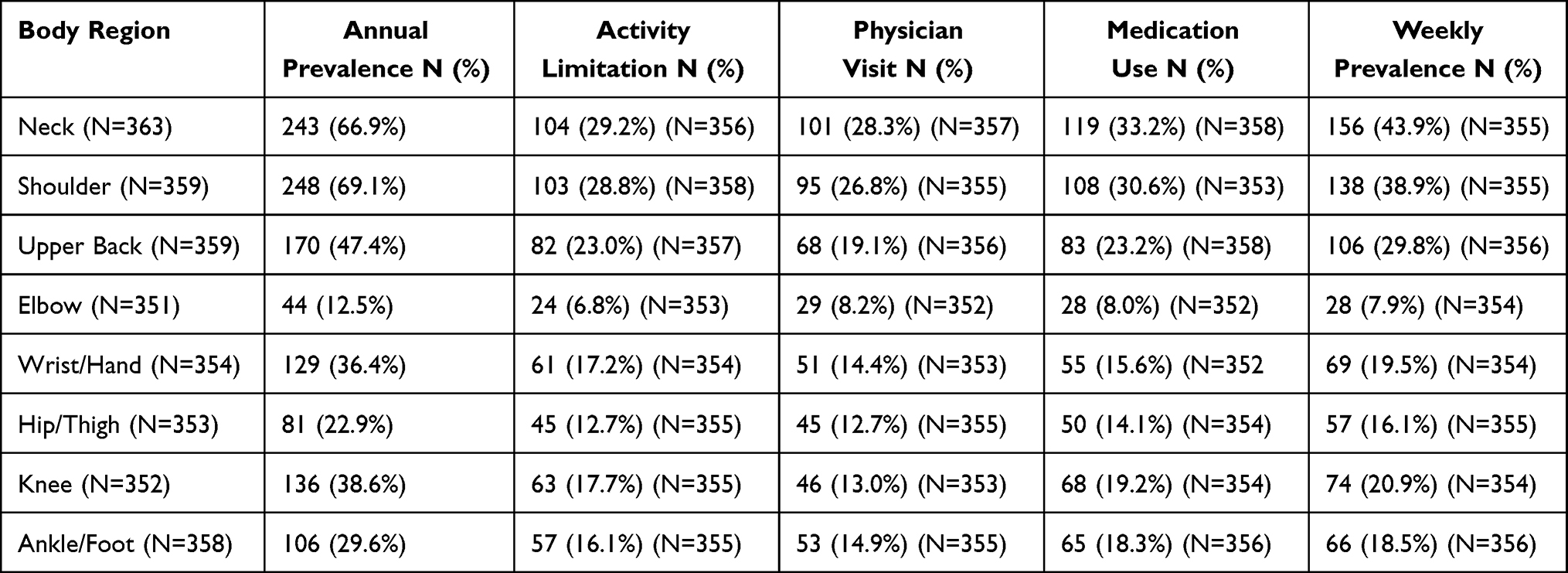 |
Table 3 Prevalence and Impact of Musculoskeletal Pain by Body Region and Time Frames |
Upper-back (47.4%) and knee (38.6%) complaints formed a middle tier, each producing weekly pain in roughly one quarter of cases. Wrist/hand (36.4%), ankle (29.6%), and hip (22.9%) symptoms were progressively rarer and less disabling.
When analyzed as a composite variable derived from the nine body regions, spine pain emerged as the most prevalent, with 80.3% of participants reporting symptoms in the past 12 months, followed by upper limb pain at 75.4% and lower limb pain at 53.3%. A similar trend was observed for 7-day prevalence, with 63.4% reporting spine pain, 47.2% reporting upper limb pain, and 33.0% reporting lower limb pain.
Occurrence of Musculoskeletal Symptoms
Figure 1 presents details percentage of distribution of symptom occurrence across the nine anatomical regions assessed. Musculoskeletal symptoms have varied notably across the region. Neck, shoulder, upper and lower-back pain dominate roughly one-third of faculty feel discomfort “sometimes. “Wrist/hand and knee symptoms fall further (≈27.3% and 23.7% “sometime”, <8% “all the time”), while hip and ankle complaints are rarer still. The elbow remains least affected, with only 4.5% reporting constant pain.
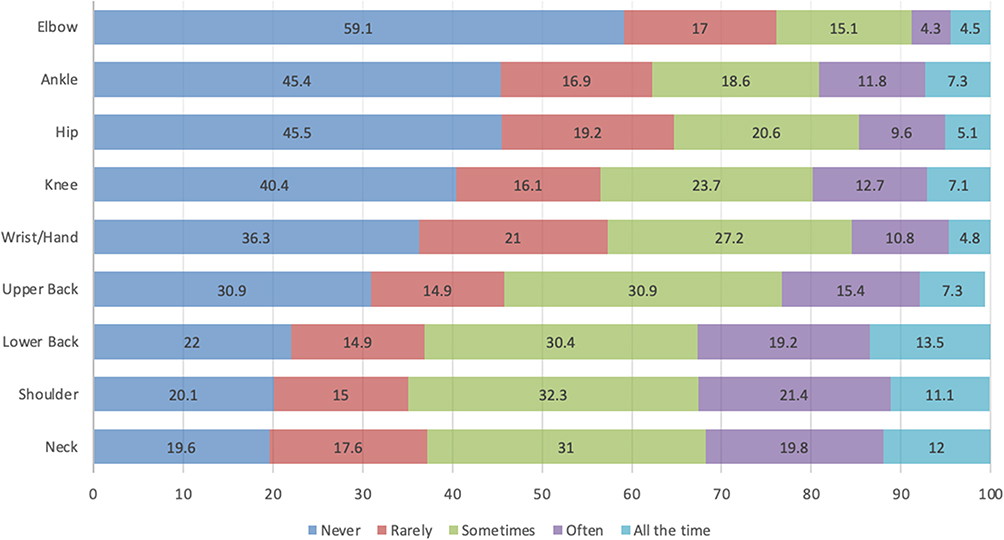 |
Figure 1 Reported Occurrence of Musculoskeletal Symptoms by Anatomical Region. |
Psychological Stress and Work Performance Across the Musculoskeletal Pain Areas
Table 4 presents the descriptive statistics of workplace stress, health-related absenteeism, absolute and relative presenteeism, and work functioning impairment across the three main pain areas. For presenteeism and work functioning measures, higher scores indicate better work performance and functioning, whereas higher absenteeism indicate greater work-related burden. Participants with lower limb pain reported the highest psychological stress levels, with a median score of 25, compared to those with upper limb or spinal pain, who had slightly lower median stress scores of 24. Notably, individuals reporting pain in all three regions demonstrated elevated stress levels relative to those without pain.
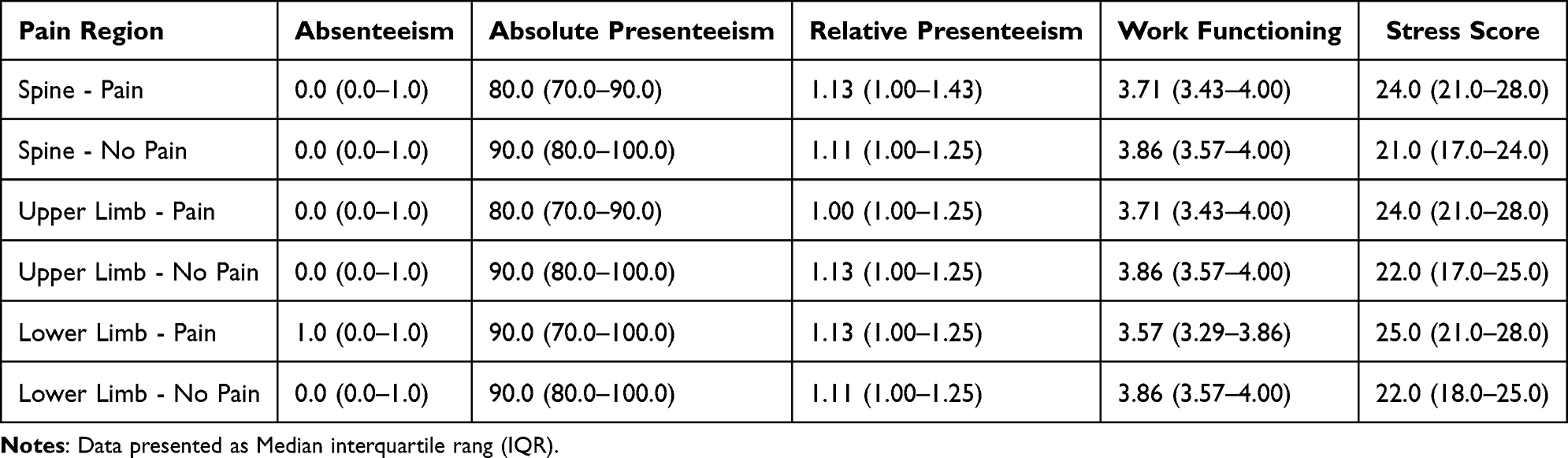 |
Table 4 Descriptive Statistics of Work Performance and Psychological Stress by Pain Region |
Participants with pain showed variable work performance patterns, particularly in absenteeism and presenteeism. Days missed remained negligible across most groups. Only lower-limb pain showed rising from a median of 0 to 1 day in the past month. In contrast, absolute presenteeism scores were consistently lower among participants with pain. Median scores were 80 for both spinal and upper limb pain (vs 90 in pain-free groups), indicating reduced productivity. For lower limb pain, medians were equal (90) for both groups. Higher variability in pain groups was also observed. Relative presenteeism scores, reflecting performance compared to peers, followed a similar pattern. Median scores were slightly lower in pain groups—1.13 vs 1.11 (spine), 1 vs 1.13 (upper limb), and 1.13 vs 1.11 (lower limb). Mean values were also reduced among those with pain. These trends suggest MSP is linked to reduced productivity, particularly for spinal and upper limb pain.
Additionally, work functional impairment scores were consistently lower among participants with musculoskeletal pain. Those with spinal pain reported a median score of 3.71 compared to 3.86 in the no-pain group, and similar trends were seen in upper limb pain (median = 3.71 vs 3.86) and lower limb pain (median = 3.57 vs 3.86). Median scores followed a similar trend, indicating a modest but consistent reduction in work functioning among participants reporting pain.
Factors Associated with Presence of Musculoskeletal Pain
The pain distribution was further categorized into three main anatomical areas: the spine, upper limbs, and lower limbs. Pain reports were based on a 7-day recall period. Several associations were observed between pain presence and demographic characteristics, work-related variables, psychological stress, and working postures.
Associations Between MSP, Demographics, Occupational Factors and Work Positions
Table 5 demonstrates the results of Chi-square analyses of demographics, occupational characteristics, and working positions. Females were more likely to report spine pain (χ2 = 9.296, p = 0.002, OR = 2.01, 95% CI [1.28, 3.15], φ = 0.16), upper limb pain (χ2 = 10.315, p = 0.001, OR = 2.07, 95% CI [1.33, 3.25], φ = 0.17), and lower limb pain (χ2 = 21.324, p < 0.001, OR = 3.37, 95% CI [1.98, 5.72], φ = 0.25), with the strongest association observed for lower limb pain). Eta was used to examine the association between pain presence and age in years. Similarly, age showed a moderate association with pain across all three body regions, with the strongest association observed for spinal pain (η = 0.400), followed by upper limb (η = 0.338) and lower limb pain (η = 0.298), suggesting that reported pain increased with age.
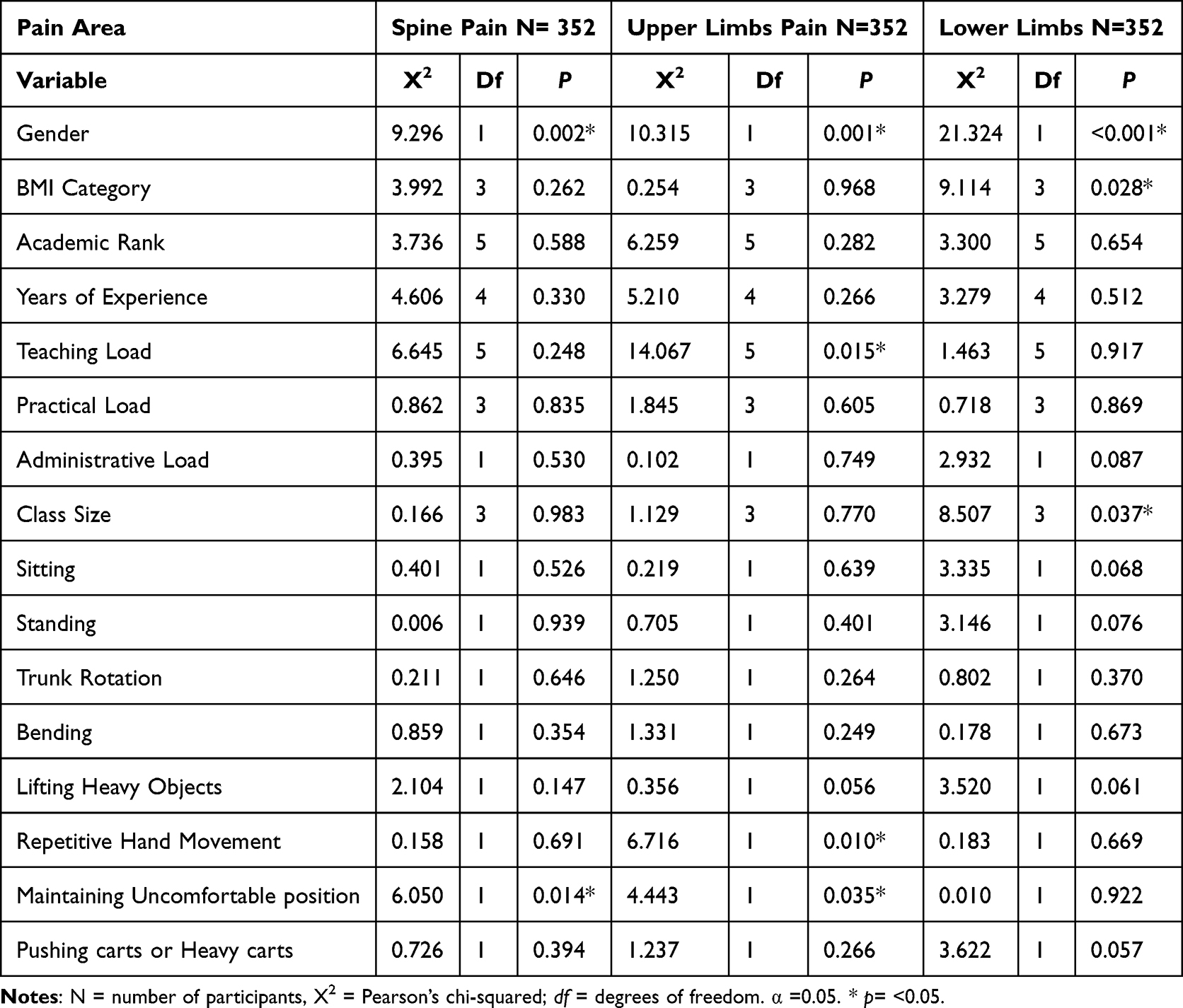 |
Table 5 Chi-Square Associations Between Acute Musculoskeletal Pain and Demographic and Occupational Variables |
Regarding BMI, no significant associations were observed between BMI categories and pain presence in the spine (χ2 = 3.992, p = 0.262, φ = 0.109) or upper limbs (χ2 = 0.254, p = 0.968, φ = 0.027). However, lower limb pain was significantly associated with BMI (χ2 = 9.114, p = 0.028, φ = 0.165). Participants classified as obese, and overweight were more likely to report lower limb pain than those with normal or underweight status.
For the occupation characteristics, a significant association was observed between upper limb pain and academic load a weak to moderate effect size (χ2 = 14.07, p = 0.015, φ = 0.202). Increased academic load was associated with a higher prevalence of upper limb pain. Similarly, lower limb pain showed a significant relationship with class size (χ2 = 8.507, p = 0.037, (φ = 0.162), with pain more prevalent among faculty members teaching larger classes. No significant associations were found between other work-related variables and pain in the spine, upper limbs, or lower limbs.
For working position, sustaining uncomfortable body postures during work was significantly associated with the presence of pain in the spine with a weak effect size (χ2 = 6.050, p = 0.014, φ = 0.131). Individuals who sustained such postures had twice the odds of reporting spine pain compared to those who did not (OR = 2.006, 95% CI [1.145, 3.516]). Similarly, upper limb pain was significantly associated with prolonged uncomfortable postures (χ2 = 4.443, p = 0.035, φ = 0.112) and participants reporting such postures had 1.71 times higher odds of upper limb pain (OR = 1.714, 95% CI [1.036, 2.836]). Additionally, repetitive hand and wrist movement was significantly associated with upper limb pain with a weak effect size (χ2 = 6.716, p = 0.010, φ = 0.138), and those engaging in repetitive movements had 1.78 times higher odds of upper limb pain (OR = 1.775, 95% CI [1.148, 2.745]). No statistically significant associations were found between lower limb pain and any of the examined work-related postures.
Association Between MSP, Psychological Stress and Work Performance
Eta coefficients indicated a moderate association between psychological stress levels and the presence of MSP across all body regions: spinal pain (η = 0.399), upper limb pain (η = 0.353), and lower limb pain (η = 0.338). Participants with spinal pain reported significantly higher WSS-8 scores (median = 24.0, IQR = 21.0–28.0) compared to those without spinal pain (median = 21.0, IQR = 17.0–24.0), U = 18,969, z = 5.232, p < 0.001. A similar pattern was observed for lower limb pain (median = 25.0 vs 22.0, IQR = 21.0–28.0 vs 18.0–25.0, U = 17,465.5, z = 4.297, p < 0.001) and upper limb pain (median = 24.0 vs 22.0, IQR = 21.0–28.0 vs 17.0–25.0, U = 18,666, z = 4.708, p < 0.001). These findings indicate that individuals with MSP consistently experience higher psychological stress across all assessed body regions.
For absolute presenteeism, weak associations were observed with spine pain (η = 0.189), upper limb pain (η = 0.144), and lower limb pain (η = 0.133). Relative presenteeism showed minimal associations with spine (η = 0.078), upper limb (η = 0.017), and lower limb pain (η = 0.025). Work functioning impairment demonstrated weak associations with spine pain (η = 0.121), upper limb pain (η = 0.178), and lower limb pain (η = 0.212), while absenteeism also yielded weak associations: spine (η = 0.115), upper limb (η = 0.117), and lower limb pain (η = 0.178).
Psychological stress, when examined independently, showed weak associations with all four work performance indicators: absenteeism (η = 0.110), absolute presenteeism (η = 0.217), relative presenteeism (η = 0.120), and work functioning impairment (η = 0.238). Among these, the strongest associations were observed with absolute presenteeism and work functioning, suggesting that stress may more directly impact aspects of productivity and functional efficiency than time missed from work.
Multivariate Predictors of Musculoskeletal Pain: Binary Logistic Regression Analysis
Binary logistic regression analyses were conducted to identify predictors of MSP across spinal, upper limb, and lower limb regions. Variables that showed significant or marginal associations in bivariate analyses were included in each respective model. Full model results for the three pain areas are presented in Table 6.
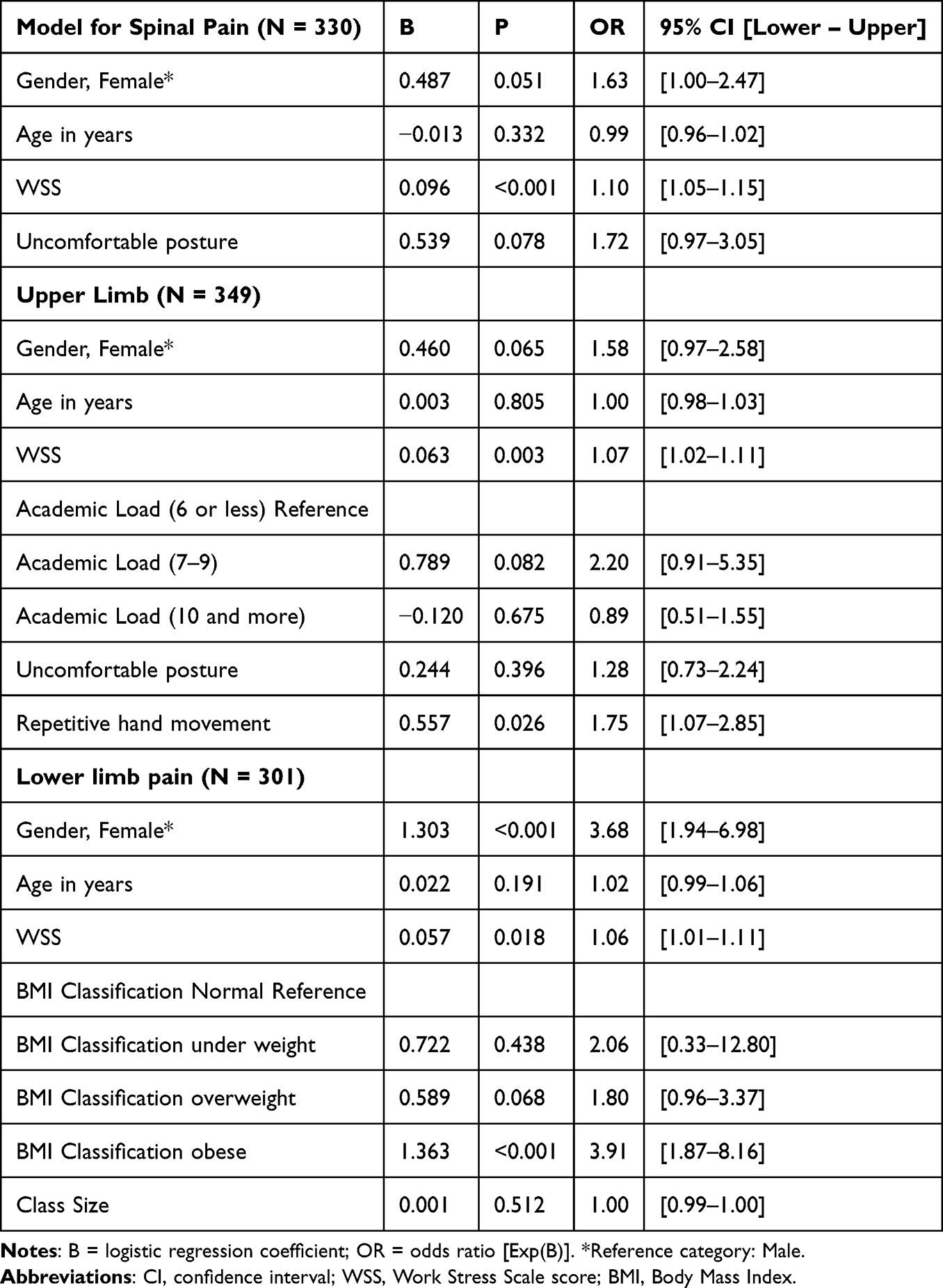 |
Table 6 Binary Logistic Regression Results for MSP by Body Areas |
For spinal pain, the regression model was statistically significant (χ2 = 36.39, p < 0.001, R2 = 0.143), correctly classifying 68.2% of cases. Higher psychological stress scores (WSS) were a significant predictor (p < 0.001, OR = 1.10), with each unit increase associated with a 10% increase in the odds of spinal pain. Gender showed a marginal association, with females having 63% higher odds compared to males (p = 0.051). Additionally, for upper limb pain, the model was statistically significant, (χ2) = 30.68, p < 0.001, R2 = 0.120), with a classification accuracy of 63.4%. Significant predictors included higher psychological stress (p = 0.003) and frequent repetitive hand and wrist movements (p = 0.0265). Other predictors—including academic load, gender, age, and postural discomfort—were not statistically significant.
The regression model for lower limb pain demonstrated the strongest performance (χ2(= 41.93, p < 0.001, R2 = 0.183), correctly classifying 71.8% of cases. Psychological stress remained a significant predictor (p = 0.018). Gender was also significant, with females showing 3.68 times the odds of reporting lower limb pain compared to males (p < 0.001). Obesity was associated with significantly higher odds (p < 0.001) compared to normal BMI. Being overweight showed a marginal association (p = 0.068). Other predictors, including posture, age, and class size, were not statistically significant.
Bivariate Analysis and Multivariate Predictors of Work Performance, Musculoskeletal Pain and Psychological Stress
Since the dependent variables were not normally distributed, Spearman’s rank-order correlation was used to assess associations between the proposed predictors (age, gender, stress levels, and presence of musculoskeletal pain in the spine, upper limb, and lower limb) and work performance outcomes (absolute presenteeism, absenteeism, and work functioning). Significant negative correlations were found between stress levels and both work functioning (ρ = –0.361, p < 0.001) and absolute presenteeism (ρ = –0.233, p < 0.001), indicating that higher stress is associated with poorer performance. Similarly, MSP in all three regions (spine, upper limb, and lower limb) was negatively associated with work functioning (ρ range = –0.122 to –0.202, all p < 0.01), and with absolute presenteeism (ρ range = –0.103 to –0.225, all p < 0.01). In contrast, these pain variables were positively correlated with absenteeism (ρ range = 0.155 to 0.255, all p < 0.01), suggesting that pain contributes to greater work absences. Age demonstrated weak but significant positive correlations with both work functioning (ρ = 0.235, p < 0.001) and absolute presenteeism (ρ = 0.227, p < 0.001). Based on these findings, Generalized Linear Models were constructed separately for each outcome. Age and gender were entered as covariates, and stress along with binary MSP variables (spine, upper limbs, lower limbs) were included as key predictors due to their demonstrated bivariate associations.
Multiple linear regression analyses were conducted to examine the effects of psychological stress, and MSP in the spine, upper limbs, and lower limbs on three work-related outcomes: absenteeism, absolute presenteeism, and work functioning (Table 7) controlling for age and gender. The model predicting absenteeism was statistically significant, F(6, 262) = 2.478, p = 0.024, but explained only a small proportion of variance (R2 = 0.054, Adjusted R2 = 0.032). None of the individual predictors, including stress or regional pain, reached statistical significance (p > 0.05), indicating that while the overall model was significant, no single factor had a strong or reliable effect on absenteeism. In the model predicting absolute presenteeism, results were also statistically significant, F(6, 321) = 8.531, p < 0.001, explaining 13.8% of the variance (R2 = 0.138, Adjusted R2 = 0.121). Higher psychological stress (B= −0.558, p <0.001) was a significant negative predictor of absolute presenteeism, whereas MSP variables did not contribute significantly (p > 0.05). Older age (B = 0.438, p < 0.001) and male gender (B = 4.596, p = 0.023) were also associated with higher productivity scores.
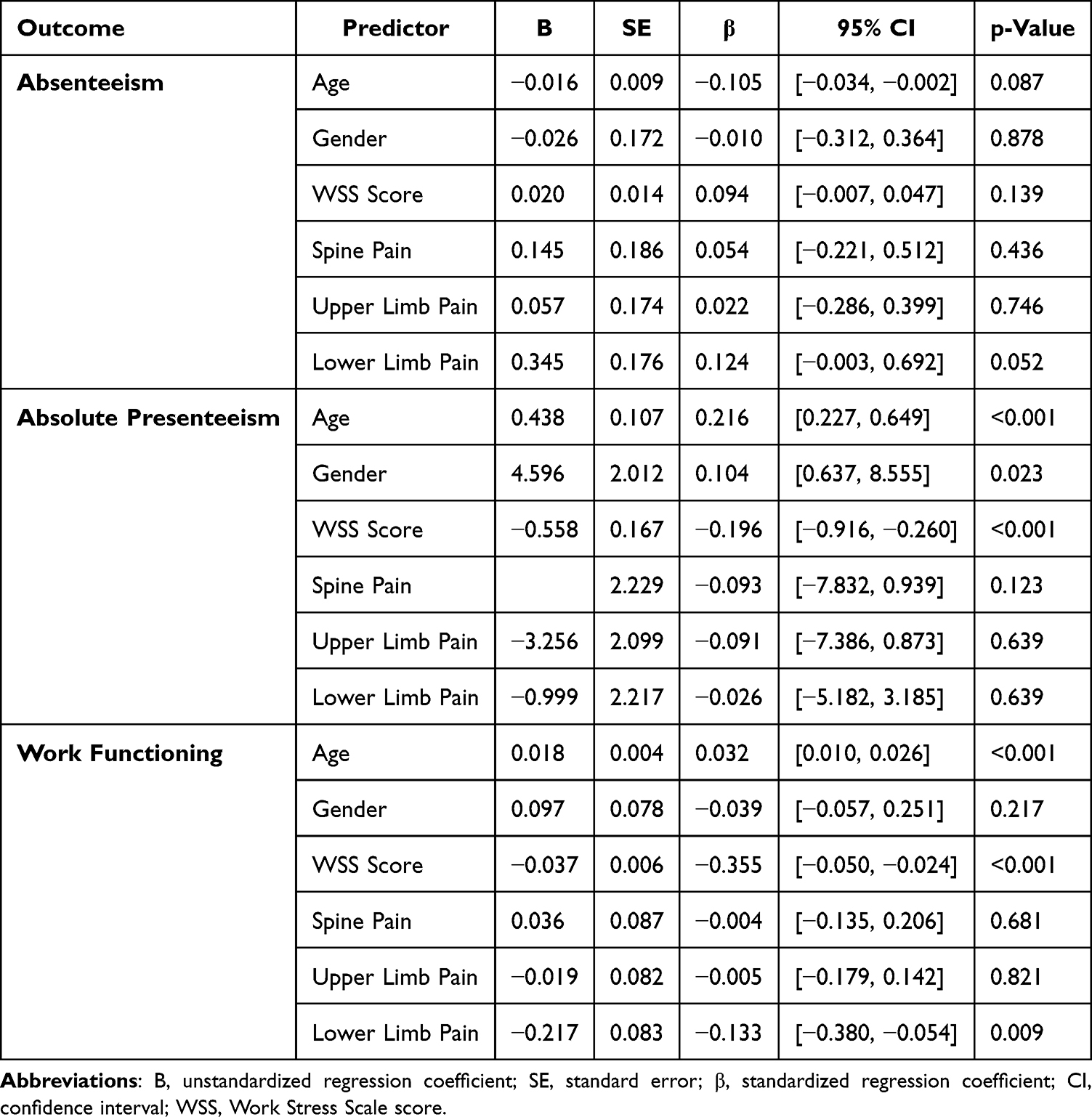 |
Table 7 Multiple Linear Regression Predicting Absenteeism, Absolute Presenteeism and Work Functional Impairments |
Lastly, the model predicting work functioning yielded the strongest explanatory power among the three, F (6, 322) = 11.775, p < 0.001, accounting for 18.0% of the variance (R2 = 0.180, Adjusted R2 = 0.165). Both higher psychological stress (B = −0.037, p < 0.001) and the presence of lower limb pain (B = −0.217, p = 0.009) were significant negative predictors of work functioning, suggesting that individuals experiencing more stress or lower limb MSP tend to report greater impairment in their ability to perform work tasks effectively.
Discussion
The causal inferences cannot be made due to the cross-sectional design of the study. In this cross-sectional survey of university faculty, MSP was highly prevalent and often multisite. The shoulders, neck, and lower back were the most frequently affected regions, showing an association with computer-intensive work and prolonged static postures. Repetitive hand and wrist activity was strongly associated with upper limb pain, while female sex and obesity emerged as important correlates of lower limb pain. Psychological stress was also consistently associated with MSP across many regions and was significantly associated with reduced work productivity. These findings are consistent with prior evidence showing that academia is an emerging high-risk sector, where faculty face intensive workloads, minimal ergonomic support, and high rates of musculoskeletal complaints.26,27
Building on this, the distribution of pain in our study further highlights the vulnerability of specific anatomical regions. The shoulders, neck, and lower back were most frequently affected, a pattern that aligns with evidence demonstrating the susceptibility of these areas to sedentary work and static postures.25–27 Previous studies have similarly reported that prolonged sitting or standing, static posture, and inadequate back support contributed to high rates of neck, shoulder, and back pain among faculty and office workers.27–30 Pain in other regions such as the wrist/hand, knees, and upper back showed moderate prevalence, while hip, ankle, and elbow pain were less common but still contributed to functional impairment. These patterns suggest that MSP among faculty is rarely confined to one region, but rather reflect the cumulative impact of their occupational demands. These findings are consistent with prior evidence indicating high MSP prevalence in occupations characterized by prolonged sitting, computer use, and cognitive demands.31,32
The predictors identified in this study provide further insight into these trends. Repetitive hand and wrist movement were significantly associated with upper limb pain, with participants engaged in frequent computer use showing higher odds of symptoms. Gender was a significant factor, with women more likely than men to report MSP across various body regions, particularly in the neck and lower limbs.33 Women in academia often balance multiple responsibilities, resulting in longer sedentary periods and increased stress both linked to higher MSP reports. Societal norms may also lead women to prioritize caregiving over their health, even as they are generally more inclined to report and seek help for pain than men. These factors underscore the need for targeted interventions to address the unique challenges faced by women in academic settings.This aligns with multiple studies that indicated that females were more likely to report MSP across all body regions and age groups. For example, women were disproportionately affected by chronic MSP and are more likely to experience persistent neck and wrist pain compared to their male counterparts.33,34 This disparity may reflect combined physical and psychosocial exposures as well as dual roles at work and home.35 Obesity also was associated with MSP, particularly in weight-bearing joints, echoing global findings that overweight individuals face a significantly higher risk of musculoskeletal disorders.36 Together, these factors demonstrate that MSP in faculty usually associated with interplay of ergonomic, biological, and social determinants.
A primary finding of this study was the strong association between lower extremity pain and decreased work productivity among participants. While this finding may be unexpected, it invites speculation regarding the underlying factors that co-occur with both lower extremity pain and functional decline. For instance, prolonged standing time, limited mobility within the office environment, and obesity may be contributing factors that lead to this observed relationship. As participants classified as obese, and overweight were more likely to report lower limb pain than those with normal or underweight status. However, as this study is cross-sectional, further longitudinal research is required to determine if these variables are precursors to the pain or consequences of it.
Alongside these physical and demographic predictors, psychological stress played a central role. Stress was strongly associated with MSP, especially in participants reporting lower limb pain, reinforcing the bidirectional relationship between pain and psychological distress.37,38 Academic staff are often exposed to overlapping stressors including high workloads, prolonged static postures, insufficient recovery, and poor ergonomic environments. Prior studies highlighted that faculty frequently reported work overload, lack of recognition, and insufficient colleague support as drivers of WRS, which in turn contribute to burnout and dissatisfaction.39–42 Findings underline the complex interaction between physical strain and psychosocial pressures in shaping the experience of MSP.
The consequences of this interaction are most evident in work performance outcomes.43,44 WRS emerged as a significant negative predictor of absolute presenteeism, with no significant associations found for absenteeism or relative presenteeism. Faculty with spinal or upper limb pain were more likely to continue working despite reduced productivity, reflecting a pattern of presenteeism rather than absenteeism. This finding is consistent with prior research indicating that WRS and MSP are linked more strongly to presenteeism than absenteeism, and that presenteeism contributes more substantially to productivity loss and impaired work performance.45–47 Reduced relative presenteeism and impaired work functioning have also been reported in pain groups, indicating diminished effectiveness and elevated risk of long-term disability.47,48 Interestingly, older participants in our study reported somewhat better productivity despite MSP, which may reflect compensatory adaptations developed over time. Older faculty members might have gained experience in balancing their workload and implementing self-care practices that mitigate the impact of pain on their performance. Moreover, they may possess a greater understanding of their limitations, allowing them to prioritize tasks more effectively and thus sustain productivity levels. This could also indicate that older participants are more adept at leveraging their accumulated knowledge and skills, enabling them to navigate challenges inherent to their roles while experiencing MSP.
Ergonomic risk factors also played a significant role in shaping outcomes. Uncomfortable and sustained postures were associated with higher odds of spine and upper limb pain, nearly doubling the risk of reporting symptoms.49 This supports ergonomic principles and previous evidence showing that awkward postures and biomechanical loading contribute to musculoskeletal discomfort, particularly in the back, shoulders, and upper limbs.30 These findings emphasize the importance of ergonomic interventions such as proper equipment, education on posture, and task redesign to reduce static loading.26 Addressing these issues is crucial, as faculty often spend prolonged periods in fixed positions that intensify biomechanical strain.26 Implementing these ergonomic strategies not only helps mitigate the risk of musculoskeletal disorders but also promotes a healthier and more efficient work environment. By addressing these ergonomic challenges, universities can support faculty wellness, enhance job satisfaction, and ultimately improve performance outcomes in academic settings.
The broader context of these findings situates MSP in academia within a global public health framework. The widespread nature of MSP among faculty mirrors the global burden of musculoskeletal disorders, which remain leading contributors to years lived with disability.50 Consistent with the Global Burden of Disease Study, low back and neck pain rank among the top causes of disability worldwide.51–53 MSP is therefore not a transient occupational issue but a chronic condition with significant economic and social costs, particularly as MSP account for over one-third of occupational injuries globally.54 By recognizing MSP as both an occupational and public health issue, institutions can better appreciate the scale of the problem.
These findings highlight the urgent need for institutional interventions to reduce MSP risks among academic staff. Ergonomic training, adjustable workstations, workload redistribution, wellness programs, stress management, and access to physiotherapy are all critical strategies.26,55 Such measures not only reduce physical strain but also mitigate psychosocial stressors, offering dual benefits for faculty well-being and productivity.56 Several factors may explain the elevated prevalence of MSP in this study relative to previous research. First, cultural nuances and a higher awareness of MSP might have facilitated more acceptability of reporting physical and mental stressors. Additionally, the sampling strategy specifically targeted university faculty whom constantly exposed to persistent physical and psychological triggers compared to the general population. Furthermore, the data collection method via self-administered questionnaires potentially introduced self-selection bias, where symptomatic members were more motivated to respond than those without pain.
Finally, several limitations must be acknowledged. The cross-sectional design and reliance on self-reported data may introduce recall bias, while the use of convenience sampling increases the potential for selection bias and limits the generalizability of the findings beyond the study population. In addition, body mass index was calculated using self-reported height and weight. This approach is widely used in occupational and population-based studies and is considered appropriate for categorical classification, although small variations in reporting cannot be entirely excluded. Key psychological determinants such as anxiety, depression, and fear-avoidance were not measured, leaving residual confounding. Furthermore, the high proportion of overweight or obese participants may independently influence both stress and MSP. Future studies should include objective measures, recruit balanced samples, and adjust for psychological and anthropometric variables to enhance generalizability. By investing in a holistic approach to faculty health, universities not only protect their workforce but also foster an environment conducive to academic excellence. This study underscores the critical importance of addressing both the physical and psychological dimensions of faculty well-being, advocating for lasting institutional change to enhance the working conditions for academic staff and improve their quality of life. Such changes could lead to a healthier, more engaged faculty, ultimately benefiting students and the broader academic community.
Conclusion
MSP was highly prevalent among faculty, commonly affecting multiple sites, including the spine, upper limbs, and lower limbs. The most consistent correlates of MSP were psychological stress and repetitive occupational demands, alongside contributions from demographic and lifestyle factors. Notably, gender disparities were evident, with women more likely to report lower-limb pain, while repetitive hand and wrist activity uniquely predicted upper-limb pain, underscoring the ergonomic burdens associated with academic work. Furthermore, obesity was found to increase vulnerability, particularly concerning weight-bearing joints.
Despite the substantial burden of MSP, its effects on productivity showed selective patterns; while absenteeism was minimally affected, presenteeism emerged as the primary occupational consequence. Stress and lower-limb pain independently impaired work functioning, whereas older age and being male modestly mitigated productivity loss. These findings highlight how MSP can subtly undermine on-the-job effectiveness, particularly when compounded by psychosocial strain.
In light of these results, it is imperative for universities to implement proactive measures to address the dual burden of physical and psychological factors affecting faculty well-being and performance. Specifically, institutions should consider the following recommendations: first, mandatory ergonomics training for academic staff to increase awareness of proper ergonomic practices; second, investment in adjustable office equipment to accommodate individual ergonomic needs and reduce strain; and third, the development of corporate stress management programs to support mental well-being and help faculty navigate psychological demands within the academic environment.
Integrating these strategies particularly for women, individuals engaged in high-repetitive hand tasks, and those with elevated body mass indices has significant potential to reduce MSP and its adverse effects on productivity. Additionally, future longitudinal studies are essential to clarify causal pathways and evaluate the effectiveness of combined ergonomic and psychosocial interventions in academic settings, thus ensuring a healthier and more productive workforce.
MSP was highly prevalent among faculty and commonly multisited, affecting the spine, upper, and lower limbs. The most consistent correlates were psychological stress and repetitive occupational demands, with demographic and lifestyle factors also contributing. Gender disparities were evident, as women were more likely to report lower-limb pain, while repetitive hand and wrist activity uniquely predicted upper-limb pain, underscoring the ergonomic burden of academic work. Obesity further increased vulnerability, particularly for weight-bearing joints. Despite the high burden of MSP, effects on productivity were selective. Absenteeism was minimally affected, but presenteeism emerged as the dominant occupational consequence. Stress and lower-limb pain independently impaired work functioning, whereas older age and being male modestly buffered productivity loss. This highlights how MSP subtly undermines on-the-job effectiveness, especially when compounded by psychosocial strain.
Taken together, these findings emphasize the dual burden of physical and psychological factors on faculty well-being and performance. Integrating stress management with targeted ergonomic interventions—particularly for women, those with high repetitive hand use, and individuals with elevated BMI—offers the greatest potential for reducing MSP and its impact on productivity. Future longitudinal studies are needed to clarify causal pathways and evaluate the effectiveness of combined ergonomic and psychosocial programs in academic settings.
Abbreviations
WRS, work-related stress; MSP, musculoskeletal pain; NMQ, Nordic Musculoskeletal Questionnaire; WSS, psychological stress with the Workplace Stress Scale; WHO-HPQ, WHO Health and Work Performance Questionnaire; BMI, Body Mass Index; IQR, interquartile ranges; φ, Phi coefficient; OR, odds ratios; CI, confidence intervals.
Data Sharing Statement
The datasets generated and/or analyzed during the current research are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board at Princess Nourah bint Abdulrahman University (IRB Number: 23-0572, dated August 06, 2023). Informed consent was obtained from all subjects involved in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research project was funded by the Deanship of Scientific Research and Libraries, Princess Nourah bint Abdulrahman University, through the Pioneer Researcher Funding Initiative, Grant No (PRFI- 2026).
Disclosure
The authors declare that they have no competing interests or conflicts to disclose for this work.
References
1. McDougall J, Wright V, Rosenbaum P. The ICF model of functioning and disability: incorporating quality of life and human development. Dev Neurorehabil. 2010;13(3):204–18. doi:10.3109/17518421003620525
2. Meaza H, Temesgen MH, Redae G, et al. Prevalence of Musculoskeletal Pain Among Academic Staff of Mekelle University, Ethiopia. Clin Med Insights Arthritis Musculoskelet Disord. 2020;13:117954412097467. doi:10.1177/1179544120974671
3. Aldhafian OR, Alsamari FA, Alshahrani NA, et al. Musculoskeletal pain among male faculty members of the College of Medicine and College of Dentistry. Medicine. 2021;100(21):e26176. doi:10.1097/MD.0000000000026176
4. Zenbaba D, Sahiledengle B, Dibaba D, et al. Work-Related Musculoskeletal Symptoms and Associated Factors Among Academic Staff in Ethiopian Universities. Environ Health Insights. 2022;16:11786302221131690. doi:10.1177/11786302221131690
5. Sun W, Yin L, Zhang T, et al. Prevalence of work-related musculoskeletal disorders among nurses: a meta-analysis. Iran J Public Health. 2023;52(3):463–475. doi:10.18502/ijph.v52i3.12130
6. Bonzini M, Bertu’ L, Veronesi G, et al. Is musculoskeletal pain a consequence or a cause of occupational stress? A longitudinal study. Int Arch Occup Environ Health. 2015;88(5):607–612. doi:10.1007/s00420-014-0982-1
7. Andersen LL, Vinstrup J, Sundstrup E, et al. Combined ergonomic exposures and development of musculoskeletal pain in the general working population: a prospective cohort study. Scand J Work Environ Health. 2021;47(4):287–295. doi:10.5271/sjweh.3954
8. Yongu WT, Iorvaa T, Burbwa SN, et al. Correlation between Job Satisfaction and Musculoskeletal Disorders among Academic Staff of Universities in Benue State: a Theoretical Narrative. Educ Res Rev. 2024;19:135–142.
9. Volcheck MM, Graham SM, Fleming KC, Mohabbat AB, Luedtke CA. Central sensitization, chronic pain, and other symptoms: better understanding, better management [Review of Central sensitization, chronic pain, and other symptoms: better understanding, better management]. Cleveland Clinic J Med. 2023;90(4):245. doi:10.3949/ccjm.90a.22019
10. Ibrahim M, El-Zoghby SM, Zaghloul N, Shehata SA, Farghaly RM. Musculoskeletal pain among medical residents: role of workplace safety climate and sexual harassment. BMC Musculoskeletal Disorders. 2024;25(1). doi:10.1186/s12891-024-07272-w
11. Søgaard K, Sjøgaard G. Physical Activity as Cause and Cure of Muscular Pain: evidence of Underlying Mechanisms [Review of Physical Activity as Cause and Cure of Muscular Pain: evidence of Underlying Mechanisms. Exer Sport Sci Rev. 2017;45(3):136. doi:10.1249/jes.0000000000000112
12. Meaza H, Temesgen MH, Redae G, et al. Prevalence of Musculoskeletal Pain Among Academic Staff of Mekelle University, Ethiopia. Clin Med Insights Arthritis Musculoskelet Disord. 2020;13:1179544120974671. doi:10.1177/1179544120974671
13. Diaz MP, Velásquez SG, López CRG, Ávila SO. Musculoskeletal discomfort associated with remote work conditions of professors during the COVID-19 confinement in Colombia. Christian J Glob Health. 2023;10. doi:10.15566/cjgh.v10i1.747.
14. González-de-la-Flor A, Bravo-Aguilar M, Almazán-Polo J, et al. Exploring the Multifactorial Predictors of Pain in Chronic Musculoskeletal Pain: a Regression-Based Study. J Pain Res. 2025;18:2081–2091. doi:10.2147/JPR.S500636
15. Brattig B, Schablon A, Nienhaus A, Peters C. Occupational accident and disease claims, work-related stress and job satisfaction of physiotherapists. J Occup Med Toxicol. 2014;9:36. doi:10.1186/s12995-014-0036-3
16. Ahmad M, Maon SN, Aziz NISA. The Relationship Between Job Stress and Quality of Life Among Working Adults. In: Noordin F, Othman AK, Kassim ES, eds.
17. Fouad DM, Mahmoud M, Mohamed MM, TAE-H A-A. Prevalence of Work-Related Musculoskeletal Disorders Among Academic Staff in Medical Faculties: a Narrative Review. Deraya Int J Med Sci Rehabil. 2025. doi:10.21608/dijms.2025.373417.1019
18. Crawford JO. The Nordic musculoskeletal questionnaire. Occup Med. 2007;57(4):300–301. doi:10.1093/occmed/kqm036
19. Chairani A. Validity and reliability test of the Nordic Musculoskeletal questionnaire with formal and informal sector workers. In:
20. Paschoal T, Tamayo Á. Validation of the work stress scale. Estud Psicol. 2004;9:45–52.
21. Saini R, Kaur S, Das K. Assessment of stress and burnout among intensive care nurses at a tertiary care hospital. J Ment Health Hum Behav. 2011;16:43–48.
22. Soltan MR, Al-Hassanin SA, Soliman SS, Gohar SF. Workplace-related stress among oncologists: egyptian single-centered observational study. Middle East Curr Psychiatry. 2020;27:19. doi:10.1186/s43045-020-00026-z
23. Kessler RC, Barber C, Beck A, et al. The world health organization health and work performance questionnaire (HPQ). J Occup Environ Med. 2003;45(2):156–174.
24. AlHeresh R, LaValley MP, Coster W, Keysor JJ. Construct validity and scoring methods of the World Health Organization: health and work performance questionnaire among workers with arthritis and rheumatological conditions. J Occup Environ Med. 2017;59:e112–e118.
25. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Academic press; 2013.
26. Almeida TEN, Ferreira REA, Bezerra LÂ, Pereira TMM. Analysis of the prevalence of musculoskeletal disorders and occupational stress in professors of a higher education institution in the state of Pernambuco. Rev Bras Med Trab. 2020;18:274–279. doi:10.47626/1679-4435-2020-542
27. Besharati A, Daneshmandi H, Zareh K, et al. Work-related musculoskeletal problems and associated factors among office workers. Int J Occup Saf Ergon. 2018;26:632–638. doi:10.1080/10803548.2018.1501238
28. Cagnie B, Danneels L, Van Tiggelen D, De Loose V, Cambier D. Individual and work related risk factors for neck pain among office workers: a cross sectional study. Eur Spine J. 2007;16:679–686. doi:10.1007/s00586-006-0266-9
29. Gerr F, Marcus M, Monteilh C. Epidemiology of musculoskeletal disorders among computer users: lesson learned from the role of posture and keyboard use. J Electromyogr Kinesiol. 2014;14(1):25–31. doi:10.1016/j.jelekin.2003.09.014
30. Hanna F, Daas RN, El-Shareif TJ, et al. The relationship between sedentary behavior, back pain, and psychosocial correlates among university employees. Front Public Health. 2019;7:80. doi:10.3389/fpubh.2019.00080
31. Oakman J, Kinsman N, Stuckey R, et al. A rapid review of mental and physical health effects of working at home: how do we optimise health? BMC Public Health. 2020;20. doi:10.1186/s12889-020-09875-z
32. Krishnan KS, Raju G, Shawkataly O. Prevalence of work-related musculoskeletal disorders: psychological and physical risk factors. Int J Environ Res Public Health. 2021;18(17):9361. doi:10.3390/ijerph18179361
33. Overstreet DS, Strath LJ, Jordan M, et al. A brief overview: sex differences in prevalent chronic musculoskeletal conditions. Int J Environ Res Public Health. 2023;20(5):4521. doi:10.3390/ijerph20054521
34. Sirajudeen MS, Alaidarous M, Waly M, Alqahtani M. Work-related musculoskeletal disorders among faculty members of college of Applied Medical Sciences, Majmaah University, Saudi Arabia: a cross-sectional study. Int J Health Sci. 2018;12:18–25.
35. Demissie B, Bayih ET, Demmelash AA. A systematic review of work-related musculoskeletal disorders and risk factors among computer users. Heliyon. 2024;10(3):e25075. doi:10.1016/J.HELIYON.2024.E25075
36. Etana G, Ayele M, Abdissa D, Gerbi A. Prevalence of work related musculoskeletal disorders and associated factors among bank staff in jimma city, southwest Ethiopia, 2019: an institution-based cross-sectional study. J Pain Res. 2021;14:2071–2082. doi:10.2147/JPR.S299680
37. Linton SJ. A review of psychological risk factors in back and neck pain. Spine. 2000;25(9):1148–1156. doi:10.1097/00007632-200005010-00015
38. Turk DC, Monarch ES. Biopsychosocial perspective on chronic pain. In: Gatchel RJ, Turk DC, editors. Psychological Approaches to Pain Management: A Practitioner’s Handbook. New York, NY: Guilford Press; 2002:3–32.
39. Tan JST. Factors affecting stress among faculty members of public universities in the Philippines: a multiple regression analysis. Int J Psychol Stud. 2017;9(3):64. doi:10.5539/IJPS.V9N3P64
40. Mohamed AG, Mohamed LK. Occupational Stress and Coping Strategies Among Academicians At Hafr al-Batin University, Saudi Arabia. J Nurs Health Sci. 2016;5:23–30. doi:10.9790/1959-0505072330
41. Iqbal A, Kokash H. Faculty Perception of Stress and Coping Strategies in a Saudi Private University: an Exploratory Study. Int Educ Stud. 2011;4:137. doi:10.5539/IES.V4N3P137
42. Al-Ghamdi NG. Role Overload and Job Stress among the Female University Teachers-Saudi Context. Eur Online J Nat Soc Sci. 2017;6:288–295.
43. Boles M, Pelletier B, Lynch W. The relationship between health risks and work productivity. J Occup Environ Med. 2004;46(7):737–745. doi:10.1097/01.JOM.0000131830.45744.97
44. Schultz AB, Chen CY, Edington DW. The cost and impact of health conditions on presenteeism to employers. J Occup Environ Med. 2009;51(1):1–10. doi:10.1097/JOM.0b013e31818d3c9a
45. Dietz C, Scheel T. Leadership and presenteeism among scientific staff: the role of accumulation of work and time pressure. Front Psychol. 2017;8:252646. doi:10.3389/FPSYG.2017.01885
46. Jia H, Shang P, Gao S, et al. Work Stress, Health Status and Presenteeism in Relation to Task Performance Among Chinese Medical Staff During COVID-19 Pandemic. Front Public Health. 2022;10:836113. doi:10.3389/fpubh.2022.836113
47. Goetzel RZ, Long SR, Ozminkowski RJ, et al. Health, Absence, Disability, and Presenteeism Cost Estimates of Certain Physical and Mental Health Conditions Affecting U.S. Employers. J Occup Environ Med. 2004;46(4):398–412. doi:10.1097/01.JOM.0000121151.40413.BD
48. Collins JJ, Baase CM, Sharda CE, et al. The assessment of chronic health conditions on work performance, absence, and total economic impact for employers. J Occup Environ Med. 2005;47(6):547–557. doi:10.1097/01.jom.0000166869.30353.4d
49. Wahlström J. Ergonomics, musculoskeletal disorders and computer work. Occup Med (Lond). 2005;55(3):168–176. doi:10.1093/occmed/kqi083
50. Júnior JPL, Silva TFA. Analysis of musculoskeletal disorders symptoms in professors of the University of Pernambuco – petrolina Campus. Rev Dor. 2014;15(4). doi:10.5935/1806-0013.20140060
51. Safiri S, Kolahi AA, Ferreira ML, Mansournia MA, Collins G, Buchbinder R. Global, regional, and national burden of low back pain, 1990–2017: a systematic analysis of the Global Burden of Disease Study 2017. Lancet Rheumatol. 2020;2(12):e775–e781.
52. Hoy D, March L, Brooks P, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):968–974. doi:10.1136/annrheumdis-2013-204428
53. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
54. Solidaki E, Chatzi L, Bitsios P, et al. Risk factors for musculoskeletal disorders among university staff: a multicenter cohort study. J Occup Health. 2021;63(1):e12241. doi:10.1002/1348-9585.12241
55. Tan SL. Factors contributing to work-related stress among university faculty members. Int J Psychol Stud. 2017;9(3):1–10. doi:10.5539/ijps.v9n3p1
56. Mohamed MA, Mohamed SA. Burnout and its relationship to psychological distress and job satisfaction among non-tenure lecturers in a Malaysian public university. Int J Acad Res Bus Soc Sci. 2016;6(11):1–10. doi:10.6007/IJARBSS/v6-i11/2412
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.