Back to Journals » Clinical Interventions in Aging » Volume 21
Muscle Ultrasound Parameters and Cognitive Function in H‑type Hypertension: A Cross-Sectional Study
Authors Weng XF, Li ST, Cui Y, Yang YL, Xie Z, Hu JY, Liu SW, Hu H, Wu YH, Mo LY
Received 9 April 2026
Accepted for publication 3 July 2026
Published 9 July 2026 Volume 2026:21 615425
DOI https://doi.org/10.2147/CIA.S615425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Xiao-Fen Weng,1,* Song-Tao Li,2,* Yan Cui,1 Yun-Long Yang,1 Zheng Xie,1 Jing-Yi Hu,3 Shan-Wen Liu,4 Hua Hu,4 Yong-Hua Wu,1 Li-Ya Mo1
1Department of Geriatric Medicine, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Suzhou, Jiangsu, People’s Republic of China; 2Department of General Practice, Pingjiang New Town Community Health Service Center, Suzhou, Jiangsu, People’s Republic of China; 3Ultrasound Center, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Suzhou, Jiangsu, People’s Republic of China; 4Department of Neurology, The Second Affiliated Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong-Hua Wu; Li-Ya Mo, Department of Geriatric Medicine, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Suzhou, Jiangsu, 215000, People’s Republic of China, Email [email protected]; [email protected]
Background: H-type hypertension is associated with an increased risk of cognitive impairment, but the relationship between muscle ultrasound parameters and cognitive function in this population remains unclear. This cross-sectional study investigated the association between muscle ultrasound parameters and cognitive function in patients with H-type hypertension and sought to identify ultrasound parameters associated with cognitive status.
Methods: This cross-sectional study included 125 patients with H-type hypertension. Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA). Participants were classified into non-cognitive impairment (n = 68) and cognitive impairment (n = 57) groups. Muscle thickness (MT), muscle cross-sectional area (MCSA), shear wave velocity (SWV), and pennation angle (PA) were measured at selected upper- and lower-limb muscles. Partial correlation analysis, multivariable linear regression, and binary logistic regression were performed to examine associations between ultrasound parameters and cognitive status.
Results: Compared with the non-cognitive impairment group, the cognitive impairment group had significantly lower MT and MCSA at multiple sites, including the biceps brachii, brachioradialis, rectus femoris, and lateral gastrocnemius (all P < 0.05), whereas SWV and PA did not differ significantly. After adjustment, rectus femoris MT showed the strongest correlation with total MoCA score (r = 0.470, P < 0.001). Rectus femoris MT remained independently associated with total MoCA score (B = 0.509, 95% CI: 0.330– 0.688, P < 0.001) and cognitive impairment (OR = 0.811, 95% CI: 0.706– 0.933, P = 0.003).
Conclusion: Reduced rectus femoris MT is independently associated with poorer cognitive function and the presence of cognitive impairment in patients with H-type hypertension. Rectus femoris MT may serve as a useful adjunctive ultrasound marker of concurrent cognitive status, but prospective studies are needed to determine its clinical utility.
Keywords: H-type hypertension, cognitive function, muscle ultrasound, rectus femoris, MoCA
Introduction
Population aging has emerged as a major global public health challenge, accompanied by an escalating burden of chronic diseases and functional decline. Hypertension is a well‑established risk factor for cognitive impairment (CI) and dementia.1 In China, approximately 75% of hypertensive patients exhibit the H‑type phenotype, defined as essential hypertension with concurrent hyperhomocysteinemia (homocysteine [Hcy] ≥ 10 μmol/L).2,3 Elevated plasma Hcy levels contribute to the pathophysiology of CI through several established mechanisms, including oxidative stress, neuroinflammation, endothelial dysfunction, and disruption of cerebral microcirculation.4,5 Owing to these neurotoxic and vasculotoxic properties, individuals with H-type hypertension are at increased risk for cognitive decline, necessitating objective and efficient strategies for early risk identification. Although cognitive screening tools such as the Montreal Cognitive Assessment (MoCA) are widely used in clinical practice, their performance may be influenced by education level, participant cooperation, fatigue, and testing environment, and they provide limited information on concurrent physical reserve or peripheral functional status. Therefore, complementary markers reflecting systemic or neuromuscular vulnerability may help characterize cognitive status more comprehensively in this population.
Recent investigations have identified an inter‑organ crosstalk between skeletal muscle and the central nervous system, often described as the brain–muscle axis.6,7 Skeletal muscle functions as an active endocrine organ, secreting various myokines that modulate neuroplasticity, neurogenesis, and cerebral energy metabolism.8,9 Sarcopenia, characterized by progressive loss of muscle mass and function, frequently co‑occurs with CI, suggesting shared biological determinants such as chronic low‑grade inflammation, insulin resistance, and endocrine dysregulation.10 In the context of H‑type hypertension, systemic metabolic disturbances may concurrently affect both skeletal muscle structure and cognitive integrity. This shared vascular-metabolic vulnerability provides a biological rationale for examining whether peripheral muscle characteristics are associated with cognitive status in this high-risk population.5,7
While conventional assessments of muscle status primarily emphasize mass or global function, they often exhibit limited sensitivity in detecting early morphological alterations. Musculoskeletal ultrasound has emerged as a reliable and non-invasive modality for the quantitative evaluation of diverse structural muscle attributes. Compared with routine anthropometric assessment or global functional evaluation, ultrasound can provide site-specific information on muscle morphology and mechanical properties. In addition, compared with magnetic resonance imaging (MRI) and computed tomography (CT), ultrasound is more accessible, radiation-free, less costly, and suitable for repeated bedside assessment; compared with DXA and bioimpedance analysis, it provides site-specific information on muscle morphology and architecture rather than only whole-body or segmental estimates of muscle mass. Muscle thickness and muscle cross-sectional area mainly reflect muscle quantity and structural reserve, whereas shear wave velocity and pennation angle provide complementary information on muscle stiffness and architecture.11 Preliminary evidence suggests that specific sonographic muscle parameters correlate with cognitive performance in certain geriatric populations.12,13 Therefore, ultrasound-derived muscle parameters may help characterize different dimensions of muscle status that are potentially related to cognitive function. Given the metabolic and vascular vulnerability inherent in H-type hypertension, these ultrasound-derived metrics may serve as adjunctive information related to cognitive status. However, the specific associations between multi-site muscle ultrasound parameters and cognitive status in this high-risk population remain to be fully elucidated.
The selected muscles were chosen to represent both upper- and lower-limb muscle groups with different functional roles. The biceps brachii and brachioradialis were included as representative upper-limb muscles, whereas the rectus femoris and gastrocnemius lateralis were selected as lower-limb muscles related to mobility, postural control, and functional reserve in older adults. Because muscle changes in older adults may vary across anatomical sites, a multi-site ultrasound assessment may provide a more comprehensive evaluation of muscle status than a single target muscle.14
The primary objective of this study was to evaluate the correlation between various skeletal muscle ultrasound parameters and cognitive function in patients with H‑type hypertension. We hypothesized that specific morphological metrics of skeletal muscle would demonstrate significant associations with cognitive scores and could potentially function as supplementary indicators of cognitive status in this population.
Methods
Study Participants
This cross-sectional study recruited a total of 125 patients with H-type hypertension attending the Department of Geriatric Medicine at Suzhou Municipal Hospital between April 2025 and November 2025.
Inclusion criteria were as follows: ① age ≥ 60 years; ② diagnosis of H-type hypertension, defined as essential hypertension with a plasma Hcy level ≥10 μmol/L, according to the China Guidelines for Prevention and Treatment of Hypertension (Revised Edition 2024).15 Hypertension was defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on repeated measurements, current use of antihypertensive medication, or a documented physician diagnosis in the medical record; ③ sufficient capacity to understand the study instructions and complete all clinical, cognitive, and ultrasound assessments.
Exclusion criteria were as follows: ① secondary hypertension; ② a confirmed diagnosis of dementia; ③ severe sensory impairments (eg, hearing or visual deficits) that precluded cognitive assessment; ④ active malignancy, autoimmune diseases, thyroid disorders, diabetes mellitus, or other significant metabolic conditions; ⑤ severe hepatic or renal dysfunction (defined as liver enzymes exceeding three times the upper limit of normal, or serum creatinine >256 μmol/L); ⑥ history of major surgery within the preceding six months; ⑦ use of medications known to affect plasma Hcy levels within the previous six months, including folic acid, vitamin B supplements, or methotrexate; ⑧ musculoskeletal or joint conditions that interfered with the accurate measurement of muscle ultrasound parameters.
Sample Size
No formal a priori sample size calculation was performed. The final sample included all eligible patients with H-type hypertension who completed the required clinical, cognitive, laboratory, and ultrasound assessments during the recruitment period; therefore, the sample size was determined by feasibility and available eligible participants.
Baseline Demographic and Clinical Data
Baseline demographic and clinical data were collected by trained researchers using standardized case report forms. Anthropometric measurements, including height and weight, were obtained for calculation of body mass index (BMI). Additional variables included age, sex, years of education, smoking status, alcohol consumption, medication history, and duration of hypertension.
Laboratory Measurements
Venous blood samples were collected in the morning after an overnight fast. All biochemical parameters were measured using an automated clinical chemistry analyzer according to standardized laboratory procedures. Assessed biomarkers included renal function markers [blood urea nitrogen (BUN), serum creatinine (SCr), uric acid (UA), and cystatin C (CysC)], lipid profile parameters [triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C)], nutritional and hematological markers [albumin (ALB) and hemoglobin (Hb)], and other metabolic markers [homocysteine and 25-hydroxyvitamin D, 25(OH)D].
Assessment of Cognitive Function
Cognitive function was assessed using the Beijing version of the MoCA.16 This screening instrument evaluates multiple cognitive domains, including attention and concentration, executive function, memory, language, visuoconstructional ability, conceptual reasoning, and orientation. Total scores range from 0 to 30, with higher scores indicating better cognitive performance. For participants with ≤12 years of formal education, 1 point was added to the total score, with the adjusted score capped at 30.17 Cognitive impairment (CI) was defined as an education-adjusted MoCA score <26. Participants with education-adjusted MoCA scores ≥26 were classified as the non-cognitive impairment (Non-CI) group.
Muscle Ultrasonographic Measurement
Muscle ultrasound was performed using a high-resolution color Doppler system (ACUSON Oxana 3, Siemens, Germany) equipped with a 9L4 linear-array transducer (4–9 MHz). All examinations were conducted by a single sonographer with five years of experience in musculoskeletal ultrasonography, who was blinded to the participants’ clinical characteristics, laboratory findings, and cognitive status. All examinations followed a standardized study-specific scanning protocol, including participant positioning, anatomical landmark identification, probe orientation, minimal-pressure technique, region-of-interest placement, and offline measurement procedures. A written operating protocol was used throughout the study to ensure consistency across all examinations. Each parameter was measured three times from separate image acquisitions, with the transducer lifted and repositioned between measurements, and the mean value was used for analysis. Intra-rater reliability was evaluated in 20 randomly selected participants, with repeat measurements obtained one week apart. Reliability was quantified using intraclass correlation coefficients (ICCs). The ICC for rectus femoris shear wave velocity was 0.884 (95% CI: 0.812–0.934). For all remaining parameters, intra-observer reliability was excellent, with all ICCs exceeding 0.90.
A standardized minimal-pressure (“floating”) technique was used to minimize compression artifacts. The transducer was applied with only sufficient pressure to maintain acoustic coupling, and a generous amount of acoustic gel was used. For the biceps brachii (BB), brachioradialis (BR), and rectus femoris (RF), participants were examined in the supine position with muscles fully relaxed. For the gastrocnemius lateralis (GL), participants were examined prone with the knee fully extended and the ankle maintained in a neutral position using a standardized foam support. Ultrasound settings, including gain, depth, and frequency, were kept constant for each muscle across all participants.
For each target muscle (BB, BR, RF, and GL), the transducer was first positioned perpendicular to the muscle fascicles at the point of maximal muscle belly to obtain a transverse image. Muscle cross-sectional area (MCSA) was measured by manually tracing the inner fascial border along the epimysium while excluding subcutaneous fat and intermuscular adipose tissue. The transducer was then rotated 90° at the same site to obtain a longitudinal image, and muscle thickness (MT) was defined as the perpendicular distance between the superficial and deep aponeuroses. Mean values from both limbs were used for analysis.
For shear wave velocity (SWV), the transducer was aligned parallel to the muscle fibers on a standard longitudinal view, and the system was switched to shear wave elastography mode. A region of interest was placed in the middle of the muscle belly while avoiding fascia, vessels, and tendons. After image stabilization, a 3-mm-diameter Q-box was positioned at the center of the region of interest, and the mean shear wave speed was recorded. Pennation angle (PA) of the GL was measured on the longitudinal view as the angle between the muscle fascicles and the deep aponeurosis. All images were anonymized and randomly reordered before offline analysis to reduce measurement bias.
Statistical Analysis
Data were analyzed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA) and GraphPad Prism version 10.0 (GraphPad Software, San Diego, CA, USA). Normality was assessed using the Shapiro–Wilk test. Continuous variables are presented as mean ± standard deviation (SD) or median (interquartile range [IQR]), as appropriate, and categorical variables as number (percentage). Between-group differences were assessed using the independent-samples t test, Mann–Whitney U-test, or chi-square test, as appropriate.
Partial correlation analyses adjusted for age, sex, and years of education were performed to examine associations between ultrasound parameters and MoCA scores. Multivariable linear regression and binary logistic regression were used to evaluate independent associations of ultrasound parameters with cognitive performance and cognitive impairment, respectively. Covariates were selected a priori based on clinical relevance, prior literature, and baseline between-group differences. Age, sex, and years of education were included as core covariates, and Hcy, TG, 25(OH)D, and ALB were further included in the fully adjusted models because they differed significantly between the cognitive impairment and non-cognitive impairment groups and may reflect metabolic or nutritional status. No stepwise variable selection was used in order to preserve model stability, and multicollinearity was assessed using the variance inflation factor (VIF), with VIF > 5 considered indicative of collinearity.
Because multiple ultrasound parameters were examined, correlation analyses were considered exploratory. No formal adjustment for multiple comparisons was applied; instead, P < 0.01 and 0.01 ≤ P < 0.05 were interpreted as robust and nominal significance, respectively. Because of the cross-sectional design, all regression models were used to evaluate associations rather than causal or predictive relationships. All tests were two-sided, and P < 0.05 was considered statistically significant, except for the tiered interpretation applied to the exploratory correlation analyses.
Results
Baseline characteristics of the 125 participants are presented in Table 1. The Non-CI (n=68) and CI (n=57) groups were comparable in age, sex, years of education, BMI, and hypertension-related characteristics (all P > 0.05). Laboratory findings showed that the CI group had significantly higher Hcy levels [14.70 (12.40–18.50) vs. 13.35 (12.00–15.15) μmol/L], but significantly lower 25(OH)D, ALB, and TG levels than the Non-CI group (all P < 0.05). No other laboratory parameters differed significantly between the groups (all P > 0.05).
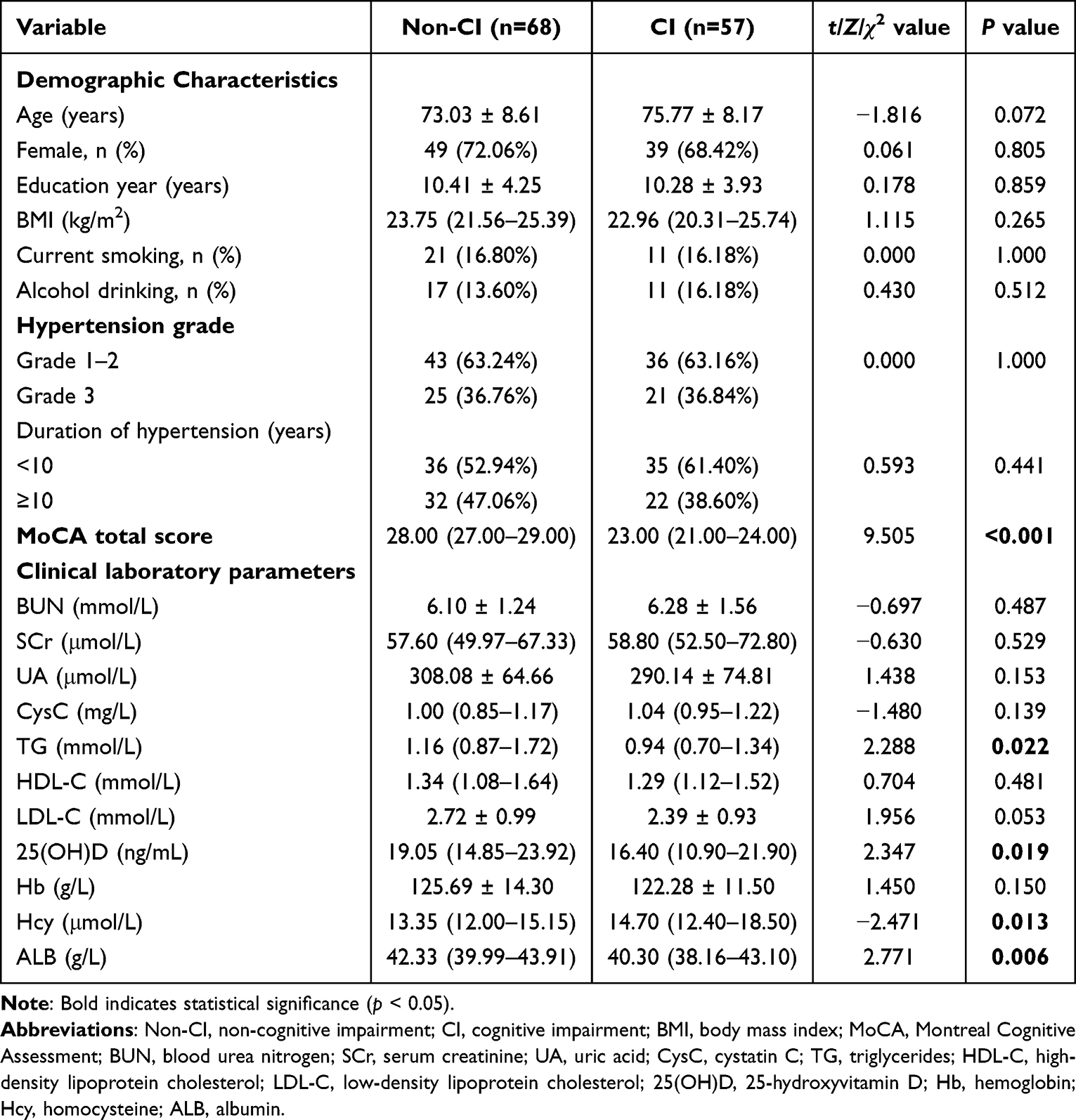 |
Table 1 Baseline Demographic and Clinical Characteristics of Participants According to Cognitive Status |
The comparison of musculoskeletal ultrasound metrics between groups is detailed in Table 2. All parameters for MT and MCSA were significantly lower in the CI group than in the Non-CI group (all P < 0.05). Specifically, MT was markedly reduced in the CI group across all anatomical sites, including the BB-MT (18.81 ± 4.05 vs. 21.69 ± 3.57 mm), BR-MT (11.08 ± 2.39 vs. 12.38 ± 2.55 mm), RF-MT (P < 0.001), and GL-MT (P < 0.001). Similarly, MCSA was significantly smaller in the CI group for the BB (P < 0.001), BR (P = 0.039), RF (P < 0.001), and GL (P = 0.023) compared to the Non-CI group. In contrast, no statistically significant differences were observed in SWV across any of the assessed muscles, nor in the PA of the gastrocnemius lateralis (all P > 0.05).
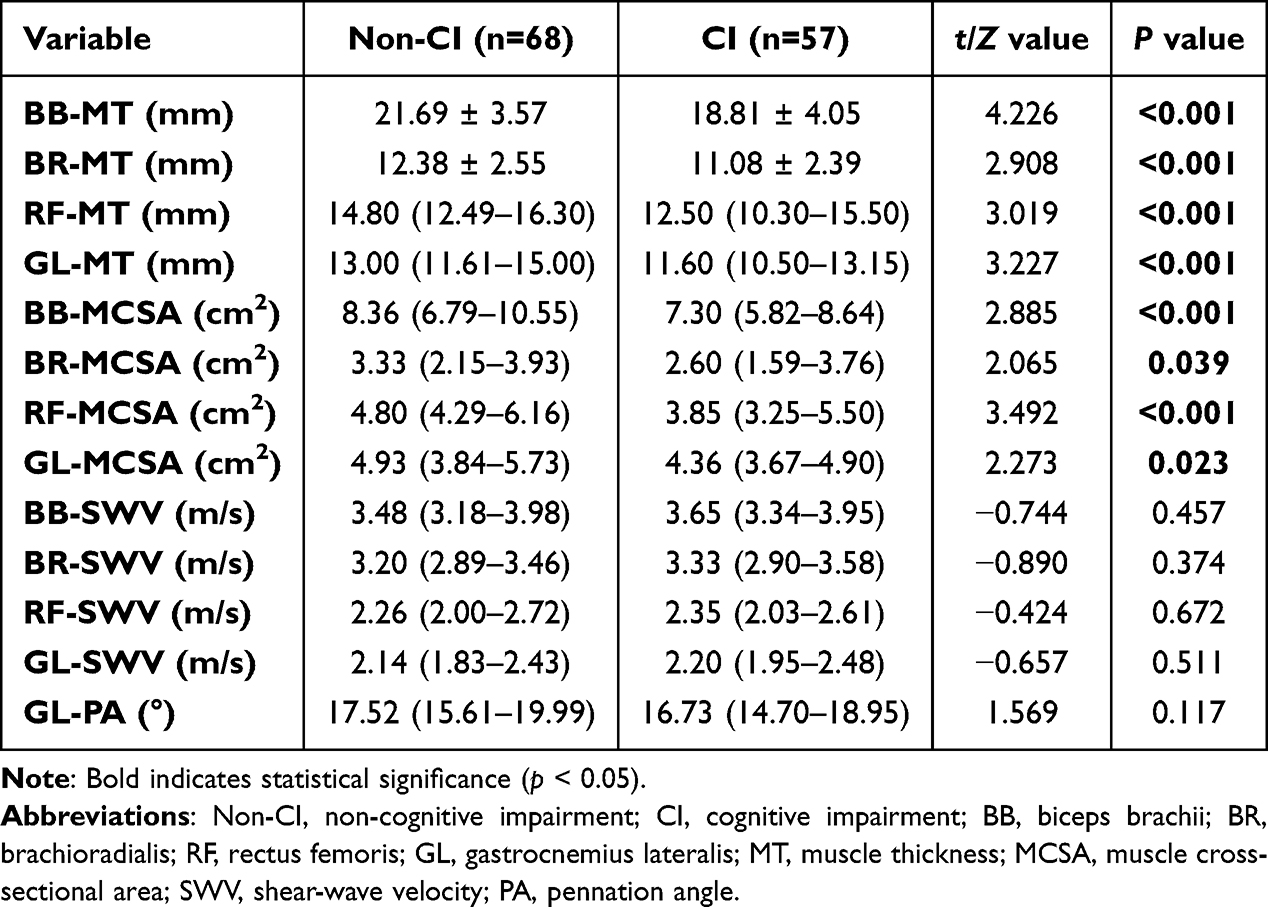 |
Table 2 Comparison of Muscle Ultrasound Parameters Between the Non-CI and CI Groups |
Partial correlation analysis, adjusted for age, sex, and education years, was performed to evaluate the relationship between MoCA total scores and muscle ultrasound metrics (Table 3).
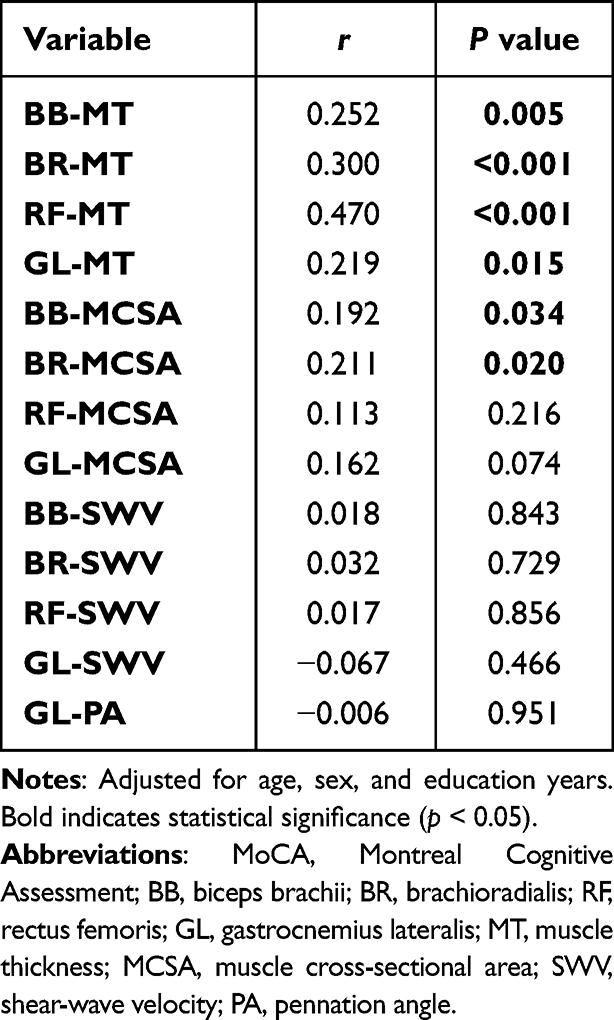 |
Table 3 Partial Correlations Between MoCA Total Score and Muscle Ultrasound Parameters in All Participants |
The results showed that MT at all assessed anatomical sites was significantly and positively correlated with MoCA total scores (all P < 0.05). Notably, RF-MT exhibited the strongest association with cognitive function (r = 0.470, P < 0.001). This positive correlation is illustrated in Figure 1.
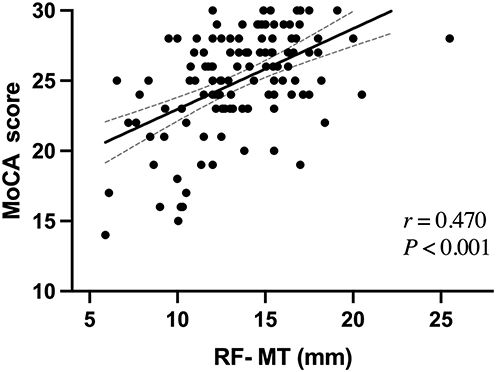 |
Figure 1 Scatter plot of Rectus femoris MT versus MoCA total score. Scatter plot of RF-MT versus total MoCA score in patients with H-type hypertension (n = 125). Each black dot represents an individual participant. The solid line shows the fitted linear regression line, and the dashed lines indicate the 95% confidence interval. After adjustment for age, sex, and years of education, partial correlation analysis demonstrated a significant positive correlation between RF-MT and total MoCA score (r = 0.470, P < 0.001). |
Regarding MCSA, significant positive correlations were observed for the BB-MCSA (r = 0.192, P = 0.034) and BR-MCSA (r = 0.211, P = 0.02), both of which were nominally significant (as 0.01 < P < 0.05). No significant associations were found for the RF-MCSA or GL-MCSA (P > 0.05). Furthermore, no statistically significant correlations were identified between MoCA scores and any SWV parameters or GL-PA (all P > 0.05).
Domain‑specific analyses further indicated that these correlations were primarily concentrated in the visuospatial and attention domains (Supplementary Table 1). Stratified analysis confirmed that RF‑MT was the only parameter that remained significantly correlated with MoCA scores in both the Non‑CI and CI subgroups (Supplementary Table 2); all other muscle parameters lost statistical significance in the stratified cohorts (all P > 0.05).
Multivariable linear regression was performed to further examine the independent associations between significant ultrasound parameters and MoCA score (Supplementary Table 3). When entered separately, several MT metrics, particularly BB-MT, BR-MT, and RF-MT, remained associated with MoCA scores after adjustment for demographic and metabolic covariates, whereas the associations for MCSA metrics were attenuated in the fully adjusted model (Models 1 and 2, Supplementary Table 3). In the mutually adjusted model including the MT parameters that remained significant after full adjustment (Model 3, Supplementary Table 3), only RF-MT maintained an independent association with cognitive function (B = 0.471, 95% CI: 0.279–0.663, P < 0.001), whereas the other MT metrics lost statistical significance.
Based on this screening, RF‑MT was selected for focused multivariable analysis (Table 4). In the final fully adjusted model (Model 2, Table 4), RF-MT remained independently associated with cognitive performance (B = 0.509, 95% CI: 0.330–0.688, P < 0.001), even after rigorous adjustment for Hcy, TG, 25(OH)D, and ALB. Education years remained a significant covariate (P = 0.008), whereas no circulating biochemical markers reached independent significance in the final model (all P > 0.05).
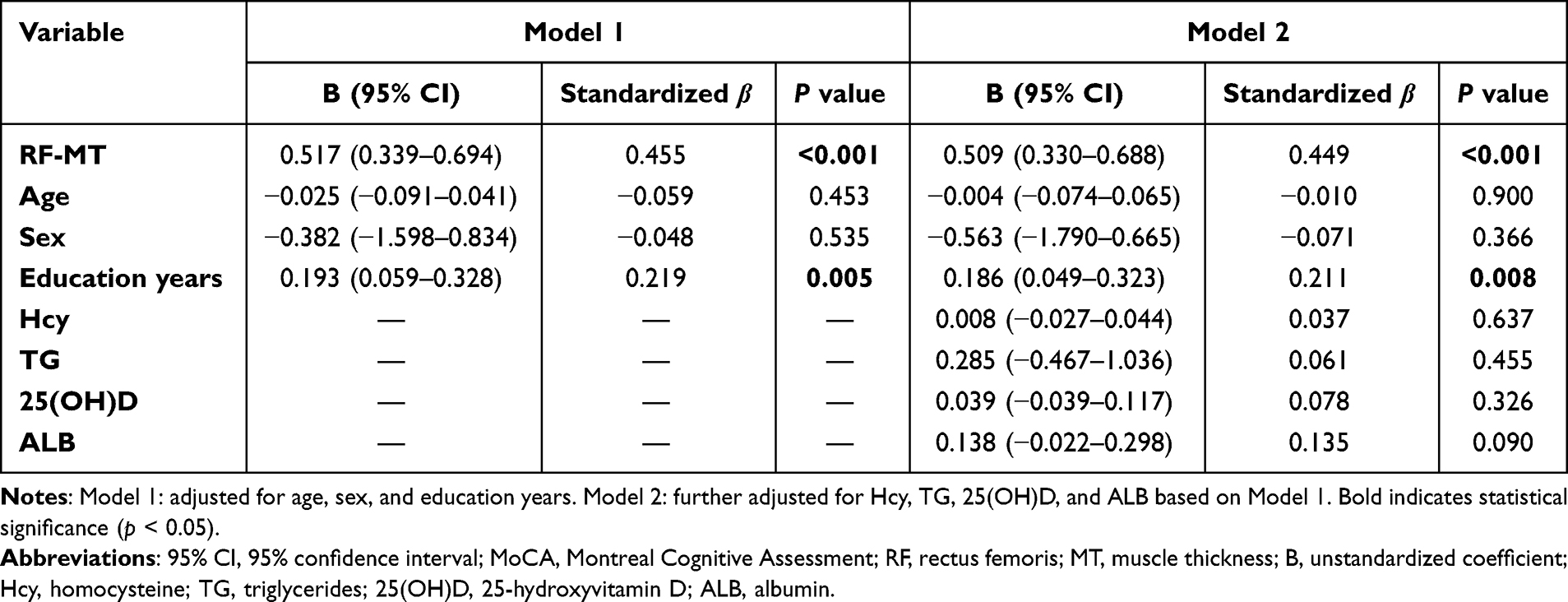 |
Table 4 Multivariable Linear Regression Analysis of Rectus Femoris Muscle Thickness Associated with MoCA Total Score |
Binary logistic regression was performed to evaluate the association between RF-MT and the presence of cognitive impairment (Table 5). In Model 1, after adjusting for age, sex, and education years, RF-MT was inversely associated with cognitive impairment (OR = 0.817, 95% CI: 0.716–0.932, P = 0.003). In the fully adjusted Model 2, which further accounted for Hcy, TG, 25(OH)D, and ALB, RF-MT remained independently associated with cognitive status (OR = 0.811, 95% CI: 0.706–0.933, P = 0.003). Specifically, each 1-mm increase in RF-MT was associated with approximately 18.9% lower odds of cognitive impairment.
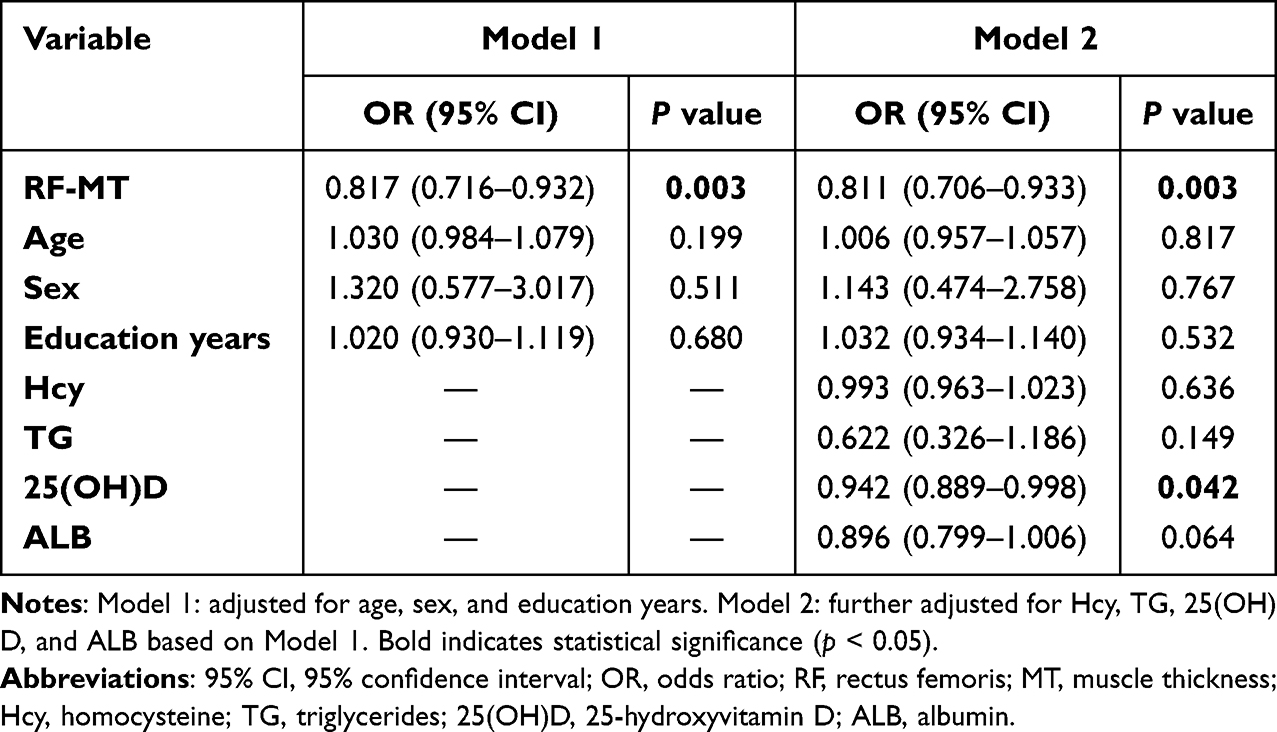 |
Table 5 Binary Logistic Regression Analysis of Rectus Femoris MT Associated with Cognitive Impairment |
Additionally, 25(OH)D was also independently associated with cognitive impairment in the final model (OR = 0.942, 95% CI: 0.889–0.998, P = 0.042), whereas no significant independent associations were observed for age, sex, Hcy, TG, or ALB (all P > 0.05).
Discussion
The present study investigated the association between CI and skeletal muscle ultrasound parameters in patients with H‑type hypertension. Our analysis yielded several key findings. First, patients with H-type hypertension and CI showed lower ultrasound-derived muscle size indices, reflected by reduced MT and MCSA at multiple anatomical sites. In contrast, stiffness- and architecture-related parameters, including SWV and PA, did not differ significantly between groups. This pattern suggests that differences associated with cognitive status were more evident in ultrasound-derived muscle size indices than in stiffness- or architecture-related parameters. Second, among the evaluated metrics, RF-MT showed the strongest correlation with MoCA scores and remained independently associated with cognitive function after adjustment for metabolic and demographic confounders. Therefore, RF-MT was selected as the representative ultrasound metric for further interpretation, although this association should not be interpreted as evidence of a predictive relationship. The relatively consistent association observed for RF-MT may be partly related to the functional importance of the rectus femoris as a major lower-limb muscle involved in mobility and physical reserve. In addition, its larger muscle size and clearer anatomical landmarks may facilitate more reproducible ultrasound measurement compared with smaller upper-limb muscles. However, this interpretation remains speculative and requires confirmation in future studies.
A notable pattern in our findings is that significant results were predominantly clustered in MT and MCSA rather than in SWV and PA. This observation is consistent with methodological expectations. From a phenotypic perspective, MT and MCSA generally reflect muscle quantity and structural reserve, whereas SWV and PA—indices of muscle stiffness and architectural configuration—are more susceptible to confounding factors such as scanning posture, passive tension, equipment presets, and operator‑dependent protocols.11,18 Existing systematic reviews have confirmed that ultrasound has good reliability and validity for quantifying muscle size in older adults, with muscle thickness and cross-sectional area being among the most consistently supported parameters.11 Therefore, the concentration of significant results on these metrics is consistent with the current evidence base in musculoskeletal ultrasonography.
Contextualizing these findings within the clinical background of H-type hypertension underscores their potential relevance, although the present study was not designed to test mechanistic pathways. Our results suggest that the association between muscle and cognitive function in this population may not be solely age-related and could be influenced by multiple vascular and metabolic factors. Previous studies have reported that the coexistence of hypertension and hyperhomocysteinemia is associated with cognitive decline and brain structural changes.19–21 In this high-risk cohort, both the brain and skeletal muscle may be affected by systemic vascular and metabolic stress, including endothelial dysfunction and oxidative stress.22,23 Therefore, the observed association between RF-MT and cognitive function should be interpreted as a cross-sectional correlation, and further longitudinal studies are needed to clarify its underlying mechanisms.
Exploratory domain‑specific analyses further showed that the correlations between muscle parameters and cognitive function were primarily concentrated in the visuospatial/executive and attention domains. This pattern is consistent with prior evidence suggesting that vascular‑related cognitive impairment often affects executive control and attentional efficiency in its early stages.24 However, these findings must be interpreted with caution: although recent studies indicate that MoCA domain scores correspond to some extent with standardized neuropsychological tests, they are not a substitute for a comprehensive neuropsychological battery.17 Therefore, these domain‑specific results should be viewed as hypothesis‑generating rather than definitive.
Comparison with previous studies. Several previous studies have reported associations between muscle ultrasound parameters and cognitive function in older adults, although findings have varied across populations and methodologies. In a cross‑sectional study of 20 institutionalized older adults (mean age 85 years), Mateos‑Angulo et al found that rectus femoris echo intensity, rather than muscle thickness, was the strongest correlate of cognitive function, explaining a substantial proportion of variance in Pfeiffer Short Portable Mental Status Questionnaire scores (adjusted R2 = 0.605).13 In contrast, our study—conducted in a larger sample of older outpatients with H‑type hypertension from a geriatric medicine clinic—identified muscle thickness, not echo intensity, as the dominant correlate. This discrepancy may be explained by several factors. First, the very high mean age (85 years) and institutionalized setting of the Mateos‑Angulo cohort may have resulted in more advanced muscle quality deterioration (eg, fatty infiltration), rendering echo intensity a more sensitive marker, whereas our outpatient population (mean age approximately 74 years) had relatively preserved muscle quality. Second, we measured SWV as a proxy for muscle stiffness, whereas echo intensity reflects tissue composition (eg, fat and fibrous tissue infiltration). Alternatively, in this cohort of patients with H-type hypertension, muscle size indices may have been more closely related to cognitive status than stiffness- or architecture-related parameters, although this interpretation requires confirmation in studies that directly examine metabolic markers and muscle ultrasound features.
Ulger et al (2022) examined 221 older adults and reported that gastrocnemius muscle thickness measured by ultrasound was significantly lower in patients with dementia compared to those without dementia, and the presence of dementia independently increased the risk of sarcopenia diagnosed by ultrasound (OR = 5.109, 95% CI: 2.002–13.033).12 Our findings extend these observations by demonstrating that the association between muscle thickness and cognitive function persists in H‑type hypertensive patients without a formal dementia diagnosis, and that rectus femoris thickness remains independently associated with MoCA scores after rigorous adjustment for homocysteine, vitamin D, and nutritional markers.
Beyond ultrasound‑specific studies, large‑scale meta‑analyses support the muscle‑cognition link. Huang et al reported that sarcopenia was associated with cognitive impairment (OR = 1.83) across 32 studies,25 and Amini et al found similar associations with mild cognitive impairment (OR = 1.58), Alzheimer’s disease (OR = 2.97), and other dementias (OR = 1.68) across 77 studies.26 However, none of these analyses specifically focused on the H‑type hypertensive population or used ultrasound‑derived muscle parameters.
Prior evidence suggests a possible shared vascular-metabolic background in H-type hypertension. Elevated homocysteine has been associated with lower skeletal muscle mass in large cohorts. Kositsawat et al found that each 1‑μmol/L increase in homocysteine was linked to a 0.09‑kg decrease in appendicular lean mass (NHANES, n = 1480),22 and a meta‑analysis of 114,583 adults reported that hyperhomocysteinemia was associated with low muscle mass (OR = 1.958).27 However, because the present study did not directly examine the pathway linking Hcy, muscle ultrasound parameters, and cognitive outcomes, these findings should be interpreted as a biologically plausible background rather than direct mechanistic evidence.
One possible explanation is that lower RF-MT may reflect reduced lower-limb muscle reserve under cumulative vascular-metabolic stress in older patients with H-type hypertension. Previous studies have suggested that hyperhomocysteinemia may contribute to endothelial dysfunction, oxidative stress, impaired vasodilation, autonomic dysregulation, and skeletal muscle abnormalities.28–31 However, the present study did not directly test the pathway linking Hcy, muscle ultrasound parameters, and cognitive outcomes. Therefore, RF-MT should be interpreted as a peripheral correlate of muscle reserve associated with cognitive status, rather than as direct evidence of Hcy-mediated muscle injury or microvascular damage.
From a clinical perspective, musculoskeletal ultrasound is non-invasive, convenient, and reproducible. In the present cross-sectional setting, RF-MT should be interpreted as a concurrent marker associated with cognitive status rather than as a predictive biomarker. Its potential value may lie in providing adjunctive information on physical and muscular reserve in older patients with H-type hypertension, particularly when cognitive complaints coexist with functional decline or reduced mobility.32,33 However, whether RF-MT provides additional value beyond direct cognitive assessment or improves longitudinal cognitive risk stratification requires validation in future prospective studies incorporating physical activity, frailty assessment, functional measures, and mechanistic biomarkers.
In the fully adjusted logistic regression model, 25(OH)D was independently associated with cognitive impairment (OR = 0.942, 95% CI: 0.889–0.998, P = 0.042), whereas albumin showed only borderline significance. These findings should be interpreted with caution, as they were secondary observations. The association is biologically plausible given previous evidence linking vitamin D with neuroprotective mechanisms and cognitive function in older adults.34,35 Recent evidence also suggests that the co-occurrence of vitamin D deficiency and hyperhomocysteinemia may be associated with executive dysfunction in older adults with hypertension.36 This observation may be considered alongside our exploratory domain-specific findings, which showed that correlations between muscle parameters and MoCA scores were mainly localized to visuospatial/executive domains. However, given the modest effect size and the exploratory nature of this finding, it should be considered hypothesis-generating rather than definitive.
Several limitations should be acknowledged. First, the cross‑sectional design precludes causal inference regarding the directionality of the observed associations and does not allow us to determine whether reduced RF-MT precedes or follows cognitive impairment. Therefore, RF-MT should be interpreted as a concurrent marker associated with cognitive status rather than as a predictor of future cognitive decline. Second, the exclusion of patients with diabetes, thyroid disorders, and other common comorbidities limits the generalizability of our findings to the broader H‑type hypertensive population. Third, cognitive assessment relied solely on the MoCA, a screening tool; therefore, our domain‑specific findings are exploratory. Fourth, although we adjusted for several demographic, metabolic, and nutritional covariates, residual confounding cannot be excluded. In particular, physical activity, frailty status, dietary intake, and detailed functional measures were not systematically assessed which may have introduced residual confounding. Fifth, no formal a priori sample size calculation was performed, and the modest sample size limited subgroup and sensitivity analyses. Future prospective, multicenter studies with larger samples, comprehensive neuropsychological assessments, and longitudinal follow‑up are needed to validate our findings and elucidate underlying mechanisms.
Conclusion
In conclusion, this cross-sectional study found that reduced rectus femoris muscle thickness was independently associated with poorer cognitive performance and the presence of cognitive impairment in patients with H-type hypertension. RF-MT was emphasized because it showed the most consistent association with cognitive status among the evaluated ultrasound parameters. These findings should be interpreted as preliminary associations rather than evidence of causality or prediction. Future prospective studies with larger samples are needed to confirm whether RF-MT provides additional information on cognitive status in this population.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
The study protocol was approved by the Ethics Committee of Suzhou Municipal Hospital (approval No. K-2024-206-K02) and was conducted in accordance with the principles of the Declaration of Helsinki. All participants provided written informed consent before enrollment.
Acknowledgments
We would like to thank all the participants in the study and the staff involved.
Author Contributions
Li-ya Mo and Yong-hua Wu contributed to the conception and design of the study. Zheng Xie and Yun-long Yang supervised the study design and implementation. Xiao-fen Weng, Song-tao Li, Yan Cui, and Jing-yi Hu contributed to clinical data collection and ultrasound data acquisition. Jing-yi Hu and Shan-wen Liu contributed to data analysis and interpretation. Song-tao Li and Shan-wen Liu performed statistical analysis and data organization. Hua Hu critically reviewed the manuscript. Xiao-fen Weng drafted the manuscript. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Commissioned Project of the 2023 Annual Special Fund for Elderly Affairs Technology (No. JGS2023WTSY03 to Xiao‑fen Weng) and the 2025 Jiangsu Provincial Geriatric Health Research Project (No. LKM2025024 to Xiao‑fen Weng).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Yao J, Wang S, Li M, et al. Correlation between blood pressure control status and cognitive impairment in older adults: a national cross-sectional study. PLoS One. 2025;20(2):e0317861. doi:10.1371/journal.pone.0317861
2. Li N, Yang X, Zou Y, et al. Analysis of the relative risk factors for H-type hypertension and its correlation with the MTHFR C677T genotype in a health checkup population in Urumqi, China-a cross-sectional study. BMC Cardiovasc Disord. 2025;25(1):455. doi:10.1186/s12872-025-04926-y
3. Xiao K, Xv Z, Xv Y, et al. H-type hypertension is a risk factor for chronic total coronary artery occlusion: a cross-sectional study from southwest China. BMC Cardiovasc Disord. 2023;23(1):301. doi:10.1186/s12872-023-03345-1
4. Lauriola M, D’Onofrio G, Ciccone F, et al. Relationship of homocysteine plasma levels with mild cognitive impairment, Alzheimer’s disease, vascular dementia, psychobehavioral, and functional complications. J Alzheimers Dis. 2021;82(1):235–12. doi:10.3233/JAD-210166
5. Faraci FM, Lentz SR. Hyperhomocysteinemia, oxidative stress, and cerebral vascular dysfunction. Stroke. 2004;35(2):345–347. doi:10.1161/01.STR.0000115161.10646.67
6. Yu S, Fan Y, You B, et al. The muscle-brain axis in aging: mechanistic and clinical perspectives on resistance training and cognitive function. Biology. 2026;15(2):154. doi:10.3390/biology15020154
7. Scisciola L, Fontanella RA, Surina N, Cataldo V, Paolisso G, Barbieri M. Sarcopenia and cognitive function: role of myokines in muscle brain cross-talk. Life. 2021;11(2):173. doi:10.3390/life11020173
8. Weng X, Liu S, Li M, et al. White matter hyperintensities: a possible link between sarcopenia and cognitive impairment in patients with mild to moderate Alzheimer’s disease. Eur Geriatr Med. 2023;14(5):1037–1047. doi:10.1007/s41999-023-00818-6
9. Xing Y, Li X, Ma L. Exploring the intricate nexus of sarcopenia and cognitive impairment. Aging Dis. 2023;15(6):2334–2344. doi:10.14336/AD.2023.1013
10. Weng XF, Liu SW, Li M, et al. Relationship between sarcopenic obesity and cognitive function in patients with mild to moderate Alzheimer’s disease. Psychogeriatrics. 2023;23(6):944–953. doi:10.1111/psyg.13015
11. Nijholt W, Scafoglieri A, Jager-Wittenaar H, Hobbelen JSM, van der Schans CP. The reliability and validity of ultrasound to quantify muscles in older adults: a systematic review. J Cachexia Sarcopenia Muscle. 2017;8(5):702–712. doi:10.1002/jcsm.12210
12. Ulger Z, Aycicek GS, Kara O, Kara M. Ultrasonographic/regional muscle measurements for diagnosing sarcopenia in older adults with and without dementia. Turk J Med Sci. 2022;52(6):1926–1932. doi:10.55730/1300-0144.5540
13. Mateos-Angulo A, Galan-Mercant A, Cuesta-Vargas AI. Muscle thickness and echo intensity by ultrasonography and cognitive and physical dimensions in older adults. Diagnostics. 2021;11(8):1471. doi:10.3390/diagnostics11081471
14. Prell T, Grimm A, Axer H. Uncovering sarcopenia and frailty in older adults by using muscle ultrasound-A narrative review. Front Med. 2024;11:1333205. doi:10.3389/fmed.2024.1333205
15. Chinese Hypertension Prevention and Treatment Guidelines Revision Committee HAC, Hypertension Branch of the China Association for the Promotion of International Exchange in Healthcare, Hypertension Branch of the Chinese Geriatrics Society. The Chinese guidelines for prevention and treatment of hypertension(Revised Edition 2024). Chin J Hyperten. 2024;32(7):603–700. doi:10.16439/j.issn.1673-7245.2024.07.002
16. Yu J, Li J, Huang X. The Beijing version of the montreal cognitive assessment as a brief screening tool for mild cognitive impairment: a community-based study. BMC Psychiatry. 2012;12:156. doi:10.1186/1471-244X-12-156
17. Nasreddine ZS, Phillips NA, Bedirian V, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
18. Zimmer M, Bunz EK, Ehring T, et al. In vivo assessment of shear wave propagation in pennate muscles using an automatic ultrasound probe alignment system. IEEE Open J Eng Med Biol. 2023;4:259–267. doi:10.1109/OJEMB.2023.3338090
19. Zhang L, Xu R, Ma X, Zhang X, Gong J, Li Z. Mechanism of arterial injury exacerbated by hyperhomocysteinemia in spontaneously hypertensive rats. Sci Rep. 2023;13(1):2482. doi:10.1038/s41598-023-28731-9
20. Wan C, Zong RY, Chen XS. The new mechanism of cognitive decline induced by hypertension: high homocysteine-mediated aberrant DNA methylation. Front Cardiovasc Med. 2022;9:928701. doi:10.3389/fcvm.2022.928701
21. Kong Y, Li X, Chang L, et al. Hypertension with high homocysteine is associated with default network gray matter loss. Front Neurol. 2021;12:740819. doi:10.3389/fneur.2021.740819
22. Kositsawat J, Vogrin S, French C, et al. Relationship between plasma homocysteine and bone density, lean mass, muscle strength and physical function in 1480 middle-aged and older adults: data from NHANES. Calcif Tissue Int. 2023;112(1):45–54. doi:10.1007/s00223-022-01037-0
23. Hainsworth AH, Yeo NE, Weekman EM, Wilcock DM. Homocysteine, hyperhomocysteinemia and vascular contributions to cognitive impairment and dementia (VCID). Biochim Biophys Acta. 2016;1862(5):1008–1017. doi:10.1016/j.bbadis.2015.11.015
24. Petersen M, Frey BM, Schlemm E, et al. Network localisation of white matter damage in cerebral small vessel disease. Sci Rep. 2020;10(1):9210. doi:10.1038/s41598-020-66013-w
25. Huang J, Li M, Luo Q, Li J. The association of sarcopenia, possible sarcopenia and cognitive impairment: a systematic review and meta-analysis. PLoS One. 2025;20(5):e0324258. doi:10.1371/journal.pone.0324258
26. Amini N, Ibn Hach M, Lapauw L, et al. Meta-analysis on the interrelationship between sarcopenia and mild cognitive impairment, Alzheimer’s disease and other forms of dementia. J Cachexia Sarcopenia Muscle. 2024;15(4):1240–1253. doi:10.1002/jcsm.13485
27. Choi JH, Seo JW, Lee MY, Lee YT, Yoon KJ, Park CH. Association between elevated plasma homocysteine and low skeletal muscle mass in asymptomatic adults. Endocrinol Metab. 2022;37(2):333–343. doi:10.3803/EnM.2021.1202
28. Givvimani S, Narayanan N, Armaghan F, Pushpakumar S, Tyagi SC. Attenuation of conducted vasodilation in skeletal muscle arterioles during hyperhomocysteinemia. Pharmacology. 2013;91(5–6):287–296. doi:10.1159/000350394
29. Veeranki S, Tyagi SC. Defective homocysteine metabolism: potential implications for skeletal muscle malfunction. Int J Mol Sci. 2013;14(7):15074–15091. doi:10.3390/ijms140715074
30. Majumder A, Singh M, Behera J, et al. Hydrogen sulfide alleviates hyperhomocysteinemia-mediated skeletal muscle atrophy via mitigation of oxidative and endoplasmic reticulum stress injury. Am J Physiol Cell Physiol. 2018;315(5):C609–C622. doi:10.1152/ajpcell.00147.2018
31. Majumder A, Singh M, George AK, Tyagi SC. Restoration of skeletal muscle homeostasis by hydrogen sulfide during hyperhomocysteinemia-mediated oxidative/ER stress condition (1). Can J Physiol Pharmacol. 2019;97(6):441–456. doi:10.1139/cjpp-2018-0501
32. Ticinesi A, Meschi T, Narici MV, Lauretani F, Maggio M. Muscle ultrasound and sarcopenia in older individuals: a clinical perspective. J Am Med Dir Assoc. 2017;18(4):290–300. doi:10.1016/j.jamda.2016.11.013
33. Fuentes-Abolafio IJ, Ricci M, Bernal-Lopez MR, Gomez-Huelgas R, Cuesta-Vargas AI, Perez-Belmonte LM. Biomarkers and the quadriceps femoris muscle architecture assessed by ultrasound in older adults with heart failure with preserved ejection fraction: a cross-sectional study. Aging Clin Exp Res. 2022;34(10):2493–2504. doi:10.1007/s40520-022-02189-7
34. Liu Y, Zhong Z, Xie J, Ni B, Wu Y. Neuroprotective roles of vitamin D: bridging the gap between mechanisms and clinical applications in cognitive decline. Int J Mol Sci. 2025;26(15). doi:10.3390/ijms26157146
35. Nakhaee S, Azadi R, Salehinia H, et al. The role of nitric oxide, insulin resistance, and vitamin D in cognitive function of older adults. Sci Rep. 2024;14(1):30020. doi:10.1038/s41598-024-81551-3
36. Tan L, Zhao L, Li H, Zhao Y, Chen Y. Association of serum 25-hydroxyvitamin D and homocysteine “double-risk” status with executive dysfunction in older adults with hypertension. Front Nutr. 2025;12:1718923. doi:10.3389/fnut.2025.1718923
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Metamemory and Emotional Contributions to the Relationship Between Cognitive Function and Medication Adherence in H-Type Hypertension: A Cross-Sectional Mediation Analysis
Wu G, Li S, Jin Q, Nan J, Liu X, Zhu Q, Guo L
Patient Preference and Adherence 2026, 20:609015
Published Date: 30 June 2026