Back to Journals » Patient Preference and Adherence » Volume 20
Metamemory and Emotional Contributions to the Relationship Between Cognitive Function and Medication Adherence in H-Type Hypertension: A Cross-Sectional Mediation Analysis
Authors Wu G, Li S, Jin Q, Nan J, Liu X, Zhu Q, Guo L
Received 13 March 2026
Accepted for publication 24 June 2026
Published 30 June 2026 Volume 2026:20 609015
DOI https://doi.org/10.2147/PPA.S609015
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Gang Wu1,*, Sixuan Li2,*, Qiansheng Jin3, Jiang Nan4, Xuehua Liu1, Qingjie Zhu3, Lingxiang Guo1
1Department of Cardiac Intensive Care Unit, Northern Jiangsu People’s Hospital, Yangzhou, Jiangsu, People’s Republic of China; 2Department of Thoracic Surgery, Northern Jiangsu People’s Hospital, Yangzhou, Jiangsu, People’s Republic of China; 3Department of Intensive Care Unit, Northern Jiangsu People’s Hospital, Yangzhou, Jiangsu, People’s Republic of China; 4Wuxi School of Medicine, Jiangnan University, Wuxi, Jiangsu, People’s Republic of China
*These authors have contributed equally to this work
Correspondence: Lingxiang Guo, Department of Cardiac Intensive Care Unit, Northern Jiangsu People’s Hospital, Yangzhou, Jiangsu Province, People’s Republic of China, Tel +86 180 5106 0157, Email [email protected]; Qingjie Zhu, Department of Intensive Care Unit, Northern Jiangsu People’s Hospital, Yangzhou, Jiangsu, People’s Republic of China, Email [email protected]
Purpose: H-type hypertension substantially increases cardiovascular and cerebrovascular risk. In older adults, medication adherence is often challenged by cognitive decline, symptom burden, and emotional distress. This study examined the relationship between cognitive function and medication adherence in older adults with H-type hypertension and tested whether metamemory and emotional states mediate this relationship.
Patients and Methods: This cross-sectional study recruited 380 older adults with H-type hypertension. Cognitive function, metamemory, anxiety, depression, and medication adherence were assessed using validated instruments. Pearson correlations and a parallel mediation model were performed. Indirect effects were tested using bias-corrected bootstrapping (5,000 resamples), reporting standardized coefficients (β) and 95% confidence intervals (CIs).
Results: Cognitive function was positively associated with medication adherence (r = 0.196, p < 0.01). The total indirect effect was significant (β = 0.151, 95% CI 0.087– 0.227), whereas the direct effect of cognitive function on adherence was not significant after including mediators (β = 0.028, p = 0.636). Metamemory showed a significant mediating effect (β = 0.164, 95% CI 0.109– 0.225), and depressive symptoms demonstrated a smaller but significant mediating role (β = − 0.031, 95% CI − 0.078 to − 0.002); anxiety was not a significant mediator. Higher serum homocysteine level and greater daily medication frequency were also associated with poorer adherence.
Conclusion: In older adults with H-type hypertension, the link between cognitive function and medication adherence appears to operate mainly through modifiable psychological mechanisms, particularly metamemory and depressive symptoms, rather than cognitive function alone. Routine chronic care may benefit from brief screening for metamemory difficulties and depressive symptoms, followed by patient centered adherence support and appropriate referral for mood management. Prospective studies are needed to confirm directionality and inform targeted interventions.
Keywords: H-type hypertension, medication adherence, metamemory, cognitive function, emotional state
Introduction
H-type hypertension refers to hypertension concomitant with elevated plasma homocysteine levels (≥10 µmol/L).1 In China, 68.3% to 80% of hypertensive patients are classified as having H-type hypertension.2 Compared to patients with uncomplicated hypertension, individuals with H-type hypertension have approximately five times higher risk of cardiovascular events, and 25 to 30 times higher than non-hypertensive individuals.3 With the accelerating population aging in China, the number of H-type hypertension cases has been increasing steadily each year, posing a significant public health challenge.4 Medication adherence plays a crucial role in achieving effective blood pressure control and minimizing the risk of associated complications. Studies have demonstrated that patients with H-type hypertension typically require long-term combination therapy involving antihypertensive agents and folic acid; however, adherence to this regimen remains suboptimal.5 Improving adherence has therefore emerged as a critical challenge in the management of chronic diseases. However, existing research has mainly focused on demographic factors such as age, education level, and disease duration,6 with limited attention to the psychological and cognitive mechanisms underlying medication behavior.
In recent years, increasing research has demonstrated that medication behavior among patients with chronic diseases is not simply a passive medical to medical instructions. Rather, it is a complex decision-making process involving subjective cognition, self-monitoring, and psychological regulation.7,8 Building on this perspective, the present study identifies two key psychological mechanisms: metamemory and emotional state. Metamemory refers to an individual’s awareness of their memory abilities, use of memory strategies, and confidence in memory performance.9 As part of cognitive control, it may be associated with a patient’s ability to manage medication effectively.10 Emotional states, commonly observed alongside chronic conditions, may reduce adherence by lowering motivation and increasing cognitive burden.
Our previous studies suggests that cognitive decline may be associated with medication adherence through metamemory and emotional states,11 However, the potential contribution of emotional factors, including anxiety and depressive symptoms, has not been examined within the same analytical framework. Current research on medication adherence in hypertensive patients largely focuses on external objective factors, such as demographic characteristics (eg, age, education level), disease-related variables (eg, disease duration, complications), and treatment burden (eg, daily medication frequency, number of medications).12,13 Limited attention has been given to psychological factors such as cognitive function, metamemory, and emotional state in explaining medication adherence behaviors.
Although elevated homocysteine (HCY) levels serve as a biological marker of H-type hypertension,14 HCY is also closely associated with cerebrovascular dysfunction and cognitive decline.15 However, the potential impact of HCY on medication adherence behavior has been largely overlooked in existing research. In other words, HCY has not yet been integrated into theoretical models of behavioral decision-making and continues to be regarded primarily as a biological marker of stroke risk. Moreover, existing studies often lack an integrated “cognition–emotion–behavior” framework in their model construction, thereby overlooking the complex psychological mechanisms underlying adherence behavior. Specifically, it remains unclear whether cognitive function influences adherence indirectly through metamemory and emotional responses such as anxiety and depression. Therefore, this study proposes two complementary models. Model A examines metamemory, anxiety, and depressive symptoms as parallel mediators linking cognitive function and medication adherence. Model B, the Extended Control Variable Model, extends the analysis by incorporating a multiple linear regression approach to assess the robustness of the psychological pathways. This model simultaneously includes cognitive function, metamemory, emotional variables, and key non-psychological factors, the model tested whether the effects of the mediators remained stable after accounting for disease burden and treatment-related characteristics.
The present analysis is based on an expanded dataset collected within the same research program, with partial participant overlap with our earlier report. Importantly, the current study addresses a broader research question by incorporating emotional variables, including anxiety and depressive symptoms, and by applying an expanded analytical framework. Specifically, we used a parallel mediation model to estimate the unique indirect associations of metamemory and emotional states with adherence while accounting for their shared variance, and we further evaluated the robustness of these psychological pathways using an extended regression model that included clinical and treatment burden indicators (eg, serum HCY level and medication regimen characteristics) This expanded approach allows us to quantify the incremental explanatory value of emotional factors beyond metamemory and to situate psychological mechanisms within a more comprehensive clinical context. Building on previous findings, the present study aimed to examine the mediating roles of metamemory and emotional states in the relationship between cognitive function and medication adherence in older adults with H-type hypertension. Guided by Bandura’s Social Cognitive Theory,16 which emphasises that health behaviours are shaped by cognitive processes, self-regulation, and affective states, we developed our conceptual model. Because these psychological factors may co-occur and our cross-sectional data cannot establish their temporal order, we applied a parallel mediation model. Based on this framework, we selected a parallel mediation framework because metamemory, anxiety, and depressive symptoms are distinct psychological factors that may co-occur in older adults with chronic conditions. In addition, the cross-sectional design does not allow temporal ordering among these mediators. Therefore, we modelled them in parallel to estimate their unique indirect associations with medication adherence while accounting for shared variance.
Methods
Study Design and Participants
This study employed a cross-sectional observational design and included a total of 380 valid samples. Participants were recruited from the cardiology and neurology departments (both outpatient and inpatient) of a tertiary general hospital in Wuxi, China. All patients were clinically diagnosed with H-type hypertension by specialist physicians according to the 2010 Chinese Guidelines for the Management of Hypertension. Data were collected from December 2022 to December 2023.
Participants were eligible if they were aged 60 or older, diagnosed with H-type hypertension (blood pressure≥140/90 mmHg and homocysteine≥10 μmol/L), had been on medication for at least six months, had no severe visual, auditory, speech, or psychiatric impairments that would prevent them from completing questionnaires (visual, hearing, speech, and relevant psychiatric conditions were screened through review of medical records and a brief face-to-face assessment by trained clinicians to confirm the participant’s ability to complete the questionnaires) and had voluntarily provided written informed consent. Patients were excluded if they had severe cognitive or psychiatric disorders that precluded reliable questionnaire completion, severe hearing or speech disorders, or other serious medical conditions that could substantially affect psychological status (including severe heart disease or chronic renal failure requiring hemodialysis).
Ethical Considerations
This study was approved by the Ethics Committee of Jiangnan University (approval number: JNU20221201IRB04, approved on 8 December 2022) and was registered with the Chinese Clinical Trial Registry (ChiCTR2300068337). All procedures were conducted in accordance with the ethical standards of the institutional research committee and the Declaration of Helsinki. Written informed consent was obtained from all participants prior to participation. Participants were informed of the study purpose, the voluntary nature of participation, and their right to withdraw at any time without penalty. Participant confidentiality and data privacy were strictly maintained throughout the study.
Measurement Tools and Variable Definitions
The study variables were categorized into three types: psychological mechanism variables (primary variables in the theoretical model); non-psychological control variables (control items in the extended model); demographic variables. Total scores were used for each scale according to published scoring guidelines, and continuous variables were standardised prior to modelling to facilitate interpretation of effect sizes.
Chinese Mini Mental Status (CMMS)
Cognitive function was assessed using the Chinese Mini Mental Status (CMMS), a Chinese adaptation of the Mini Mental State Examination originally developed by Folstein et al, which consists of 30 items evaluating orientation, memory, attention and calculation, recall, and language abilities.17 Each correct response scores one point, with a total score ranging from 0 to 30; higher scores indicate better cognitive performance. As the study was conducted in China, the Chinese version translated by Mingyuan Zhang et al was used.18 This version has demonstrated high reliability (Cronbach’s α = 0.91) and good construct validity when compared with other cognitive assessment tools.19 Educational level influences cutoff scores for cognitive impairment: ≤17 for illiterate individuals, ≤20 for primary education, and ≤24 for secondary education or above.
Multifactorial Memory Questionnaire (MMQ)
Metamemory was assessed using the Multifactorial Memory Questionnaire (MMQ), originally developed by Troyer et al in 200220 and later translated into Chinese by Jiang Yunyun et al in 2018 for use in evaluating metamemory characteristics.21 The MMQ comprises three dimensions: memory satisfaction, memory ability, and memory strategy. It includes 51 items rated on a 5-point Likert scale, with a total possible score of 204; higher scores indicate better metamemory performance. The original version demonstrated good internal consistency, with Cronbach’s α coefficients ranging from 0.772 to 0.929 across subscales, and a content validity index of 0.90.
8-Item Morisky Medication Adherence Scale (MMAS-8)
Medication adherence was assessed using the 8-item Morisky Medication Adherence Scale (MMAS-8).22 As this study was conducted in China, the Chinese version of the MMAS-8, authorized and validated by the original authors, was used.23 The scale has demonstrated good reliability and validity, with a Cronbach’s α coefficient of 0.723 and a content validity index of 0.89.24 The MMAS-8 yields a maximum score of 8, with higher scores indicating better adherence. A score of 8 denotes high adherence, 6–8 indicates moderate adherence, and scores below 6 reflect poor medication-taking behaviour. MMAS-8 was used under license from the copyright holder.
Self-Rating Depression Scale (SDS)
The Self-Rating Depression Scale (SDS), developed in 1965 by Dr. William Zung at Duke University Medical Center, is used to assess the severity of depressive symptoms and subjective feelings of depression experienced over the past week.25 Each item is rated on a 4-point scale (1 to 4), and the raw score is obtained by summing all item scores. The standard score is calculated by multiplying the raw score by 1.25 and rounding down to the nearest whole number. A standard score below 53 indicates no depression; scores between 53–62 suggest mild depression; 63–72 indicate moderate depression; and scores above 72 reflect severe depression. Higher SDS scores represent more pronounced depressive tendencies. The scale is widely used and has demonstrated good psychometric properties, with a Cronbach’s α above 0.75 and a validity index of 0.84.26
Self-Rating Anxiety Scale (SAS)
Anxiety was assessed using the Self-Rating Anxiety Scale (SAS), developed by Zung in 1971.27 This instrument is widely used in both clinical and research settings due to its strong practicality and diagnostic accuracy in identifying anxiety symptoms over the past week.28 The SAS consists of 20 items, with a Cronbach’s α coefficient of 0.824. Each item is rated on a 4-point Likert scale (1 to 4), corresponding to “occasionally or not at all,” “sometimes,” “often,” and “most or all of the time.” Items 5, 9, 13, 17, and 19 are reverse scored. The raw score is calculated by summing all item responses, and the standard score is obtained by multiplying the raw score by 1.25 and rounding down to the nearest integer. A standard score below 50 indicates no anxiety; scores between 50–59 indicate mild anxiety; 60–69 indicate moderate anxiety; and scores of 70 or above indicate severe anxiety.
Study Hypotheses
H1: Better cognitive function is associated with higher medication adherence in older adults with H-type hypertension. H2: Metamemory, anxiety, and depressive symptoms mediate the association between cognitive function and medication adherence when modelled in a parallel mediation framework. H3: Metamemory and emotional factors provide unique and complementary indirect pathways linking cognitive function with medication adherence. H4: The associations between cognitive function, the proposed psychological mediators, and medication adherence remain when relevant clinical and behavioural covariates are considered.
Non-Psychological Control Variables (Included in Model B)
- Disease-related variables: These include homocysteine (HCY) levels (μmol/L), daily medication frequency, smoking and drinking status, all measured as continuous variables to reflect disease severity and cumulative treatment burden.
- Medication burden variables: These consist of daily medication frequency and number of medication types taken daily (both categorical variables), which indicate the complexity of daily medication routines, as well as the mode of medical expense payment (an ordinal variable) to represent economic burden and level of insurance coverage.
- Chronic comorbidity variable: These variable captures whether the patient has additional chronic conditions, to control for potential effects of comorbidities on adherence.
- Health behavior variables: Smoking and alcohol consumption are included as binary variables (0 = no, 1 = Yes/Formerly), to account for the influence of lifestyle behaviors on medication adherence.
These control variables are included in the path model as exogenous factors to eliminate potential confounding effects of disease burden, medication complexity, and lifestyle differences on the core psychological pathways.
Demographic Variables
Demographic information was collected via questionnaire and included age, gender, educational level and monthly household income.
Data Collection and Quality Control
Data were collected through face-to-face interviews and scale administration conducted by physicians and nursing staff who received standardized training. All instruments, including the CMMS, SDS, SAS, and MMAS-8, were administered in validated Chinese versions with established reliability and validity. Laboratory data (HCY levels) were tested uniformly by the hospital’s clinical laboratory. Questionnaire data were entered and verified through double-entry procedures to ensure accuracy.
Data Analysis
Model A: Psychological Mechanism Pathway Model (Primary Model)
Model A was designed to examine whether the association between cognitive function and medication adherence is mediated by metamemory, anxiety, and depressive symptoms. Mediation analyses were performed using the bias-corrected bootstrapping method based on partial regression, implemented with the PROCESS macro (Model 4, version 3.4.1) in SPSS 26.0. Statistical significance of indirect effects was evaluated using 5000 bootstrap resamples and bias-corrected 95% confidence intervals. In this model, drinking status and daily medication frequency were included as covariates to control for behavioral and regimen-related influences on adherence. To facilitate comparison of effect sizes across variables, all continuous variables were standardized prior to analysis, and standardized regression coefficients (β) were reported. A path diagram was generated to illustrate the direct and indirect pathways linking cognitive function, metamemory, emotional states, and medication adherence. A parallel mediation framework was selected to estimate the unique indirect associations of metamemory, anxiety, and depressive symptoms while accounting for their shared variance. Because the design is cross-sectional, alternative pathway structures such as sequential mediation were not tested.
Model B: Extended Control Variable Model (Objective Factor Modeling)
Model B was constructed to evaluate the robustness of the psychological pathways by incorporating additional clinical and behavioral variables associated with medication adherence. A multiple linear regression analysis was conducted with medication adherence as the dependent variable. Independent variables included cognitive function, metamemory, anxiety, and depressive symptoms. Serum homocysteine (HCY), drinking status, and daily medication frequency were added as covariates to account for physiological burden and medication regimen complexity. Before modelling, all continuous variables were standardized to allow comparison of standardized regression coefficients (β). Categorical variables were dummy coded. Model assumptions were checked through residual distribution, multicollinearity indicators (variance inflation factors), and Durbin–Watson values. The adjusted R2, F-statistics, and 95% confidence intervals were reported to describe overall model fit and estimation precision. This model was used to determine whether metamemory and emotional factors remained independent predictors of medication adherence after accounting for non-psychological influences, and to assess whether the direct effect of cognitive function persisted under extended adjustment. Covariates were selected based on clinical relevance and prior literature, and the modelling strategy for covariates in Model A and Model B is described to improve transparency.
Results
Sample Characteristics
A total of 412 older adults with H-type hypertension were approached, and 380 participants consented and completed all questionnaires, yielding a valid response rate of 92.2%. Among the 380 participants, 220 (57.9%) were male and 160 (42.1%) were female, with a mean age of 72.39 years (SD = 6.95). Most participants had completed junior high school education or above (76.8%). The mean duration of hypertension was 12.55 years, and more than half of the participants (55.3%) had two or more chronic comorbid conditions. Regarding medication-related characteristics, 85.0% of participants took antihypertensive medications once daily, and 32.1% reported current or former drinking. The daily number of medicines taken was median 2 (range 1–4). Detailed sociodemographic and clinical characteristics are presented in Table 1.
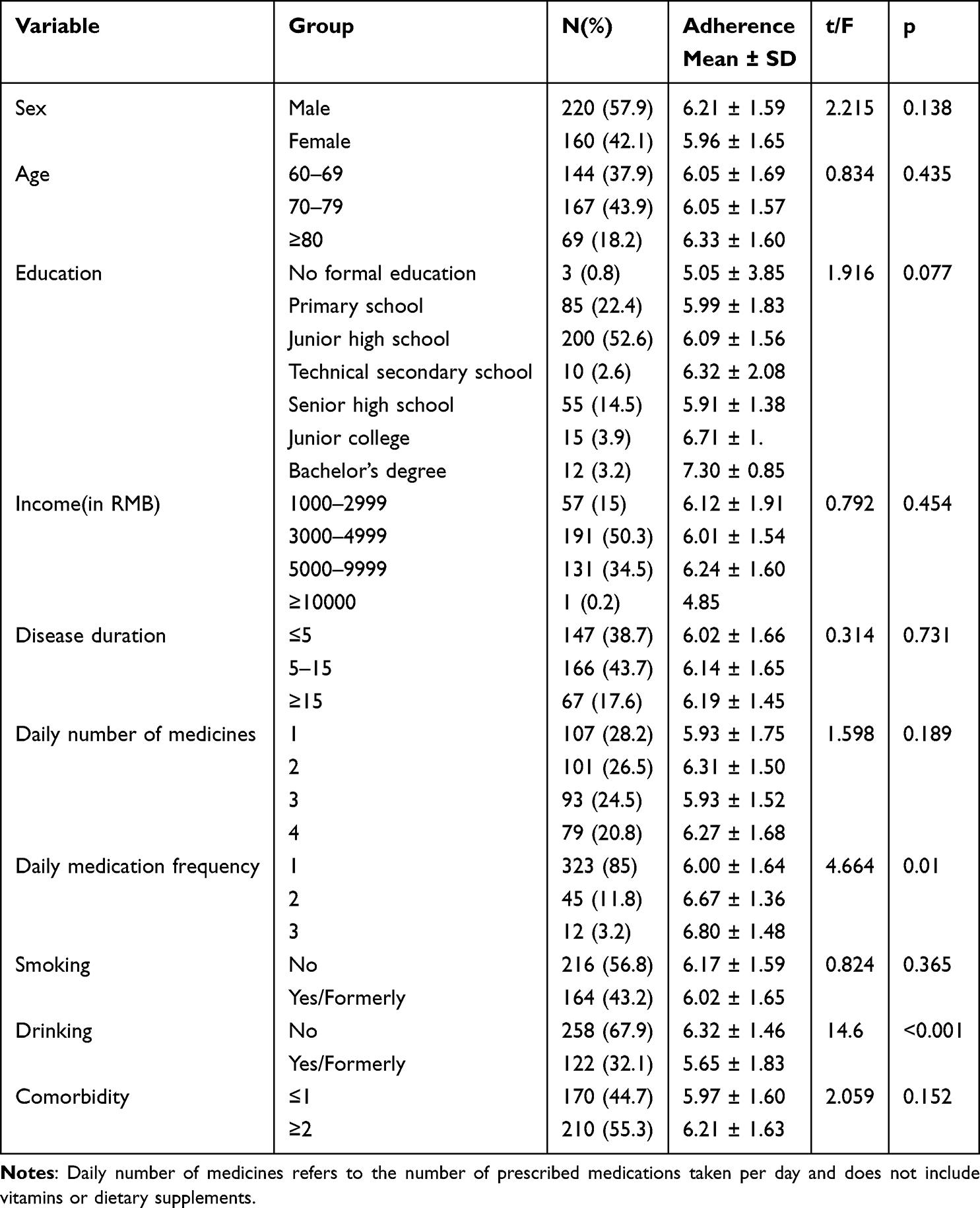 |
Table 1 Comparison of Medication Adherence Levels Across Different Sociodemographic Characteristics (N = 380) |
Correlation Analysis of Variables
We first examined bivariate associations among the study variables (Table 2). Medication adherence showed positive correlations with cognitive function (r = 0.196, p < 0.01) and metamemory (MMQ total score, r = 0.235, p < 0.01), and negative correlations with anxiety, depression and serum HCY levels (all p < 0.01). Cognitive function and metamemory were positively associated with each other (r = 0.402, p < 0.01). Correlations among the three psychological variables (metamemory, anxiety and depression) were modest. Overall, correlations with medication adherence were small in magnitude (absolute r values below 0.30), indicating statistically significant but weak associations. To determine appropriate covariates for the path model, associations between medication adherence and demographic or behavioral characteristics in Table 1 were examined. Drinking status and daily medication frequency were significantly related to adherence (p < 0.05) and were therefore included as covariates in subsequent analyses.
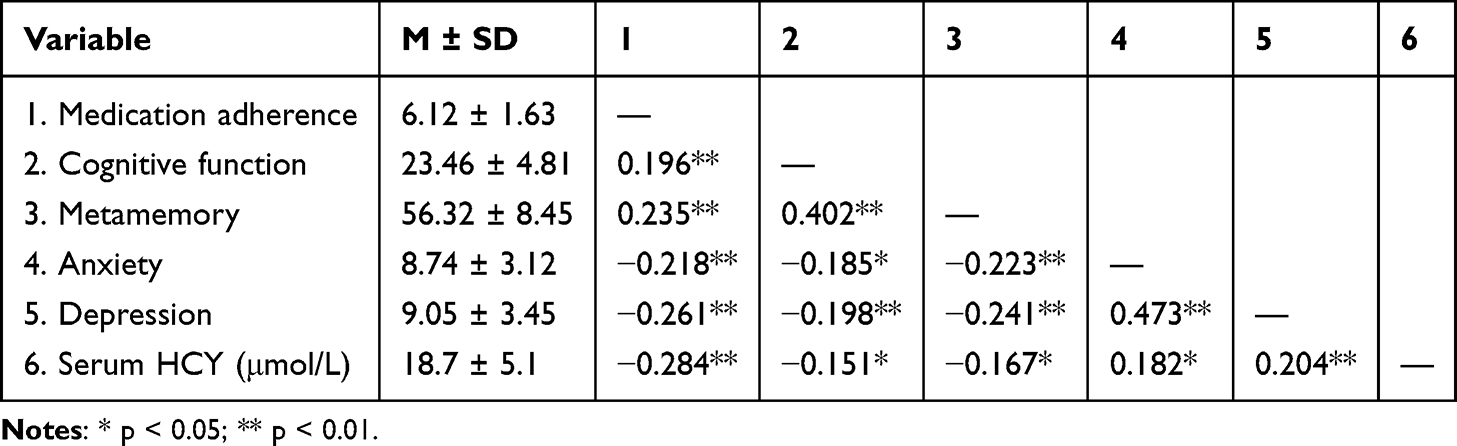 |
Table 2 Means, Standard Deviations, and Pearson Correlations Among Key Continuous Variables (N = 380) |
Mediation Analysis
We then tested the parallel mediation model with drinking status and daily medication frequency as covariates (Table 3 and Figure 1). Cognitive function was significantly associated with all three mediators. It was positively related to metamemory (β = 0.655, p < 0.001) and negatively related to anxiety (β = −0.210, p = 0.015) and depression (β = −0.228, p = 0.006). Among the mediators, metamemory showed a significant positive association with medication adherence (β = 0.251, p < 0.001). Depression showed a significant negative association (β = −0.136, p = 0.004). Anxiety was not significant (p = 0.062). Indirect effect analysis showed a significant mediation pathway through metamemory (β = 0.164, 95% CI 0.109 to 0.225). The indirect effect through depression was also significant (β = −0.031, 95% CI −0.078 to −0.002). The pathway through anxiety was not significant. The total indirect effect was significant (β = 0.151, 95% CI 0.087 to 0.227). The direct effect of cognitive function on medication adherence was not significant (β = 0.028, p = 0.636). The total effect was significant (β = 0.179, p = 0.001). The base mediation model explained 33.7% of the variance in adherence (R2 = 0.337). When HCY was included as an additional predictor, the model explained 46.4% of the variance (R2 = 0.464).
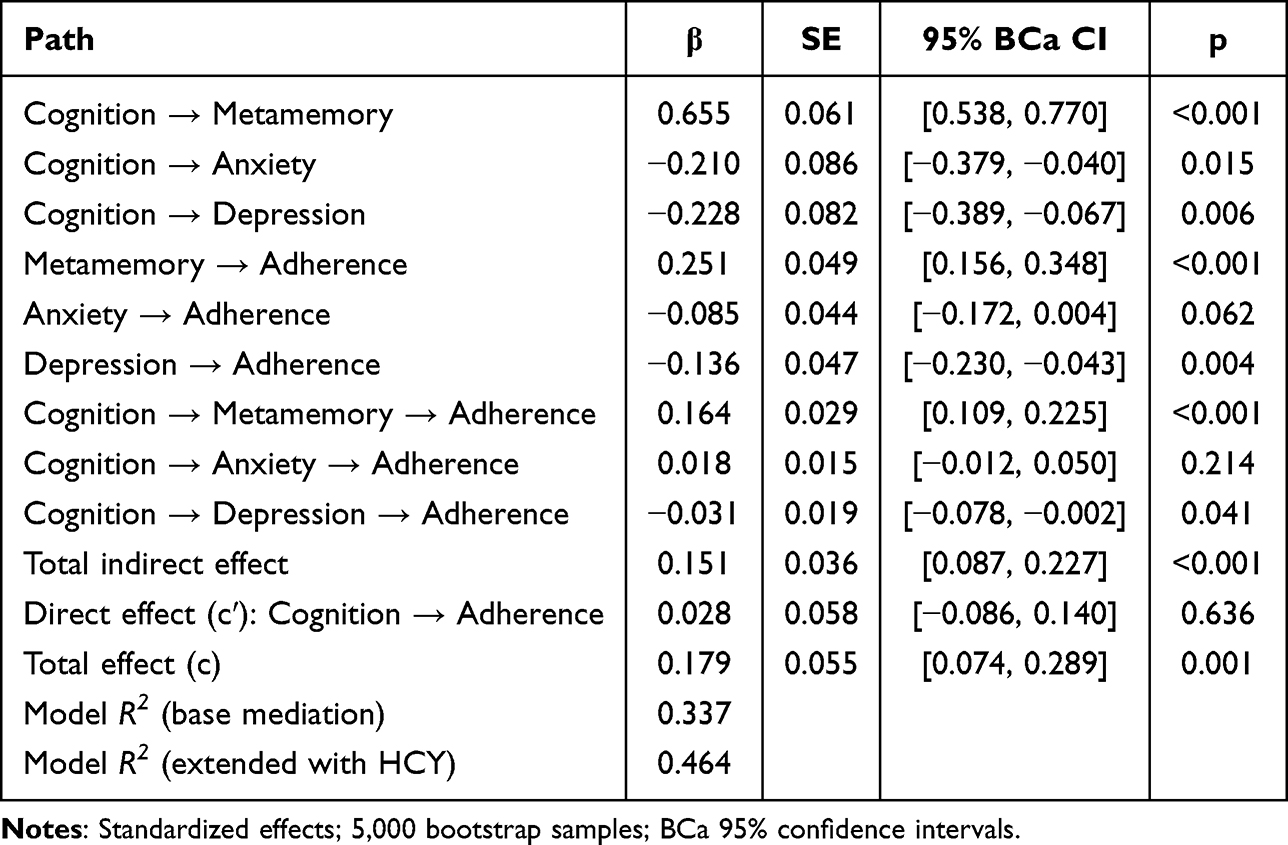 |
Table 3 Parallel Mediation of the Association Between Cognitive Function and Medication Adherence via Metamemory, Anxiety, and Depression |
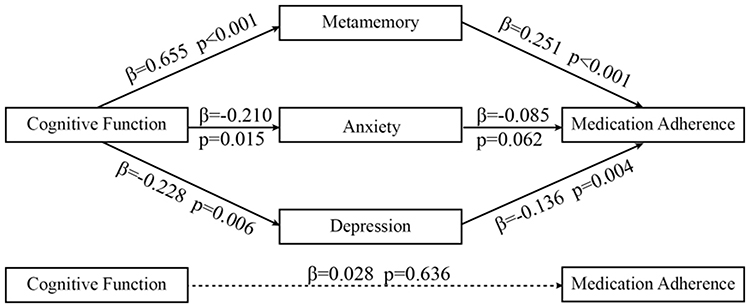 |
Figure 1 Parallel mediation model linking cognitive function to medication adherence. |
Extended Regression Analysis
Finally, we evaluated the robustness of the psychological variables in an extended regression model including clinical and treatment burden indicators (Table 4). Metamemory was a significant positive predictor of medication adherence (β = 0.251, p < 0.001). Serum HCY showed a significant negative association (β = −0.346, p < 0.001). Depression was also negatively associated with adherence (β = −0.089, p = 0.031). Daily medication frequency (β = −0.131, p = 0.027) and drinking status (β = −0.142, p = 0.022) were significant predictors as well. Cognitive function was not a significant predictor when all variables were included (β = 0.028, p = 0.636). Anxiety and medical insurance type were not significant. Sex showed a trend but was not statistically significant (p = 0.085). Disease duration showed a small but significant negative association with adherence (β = −0.097, p = 0.033). The extended model accounted for 46.4% of the variance in medication adherence (adjusted R2 = 0.464). All variance inflation factors were below 2.5, indicating no multicollinearity.
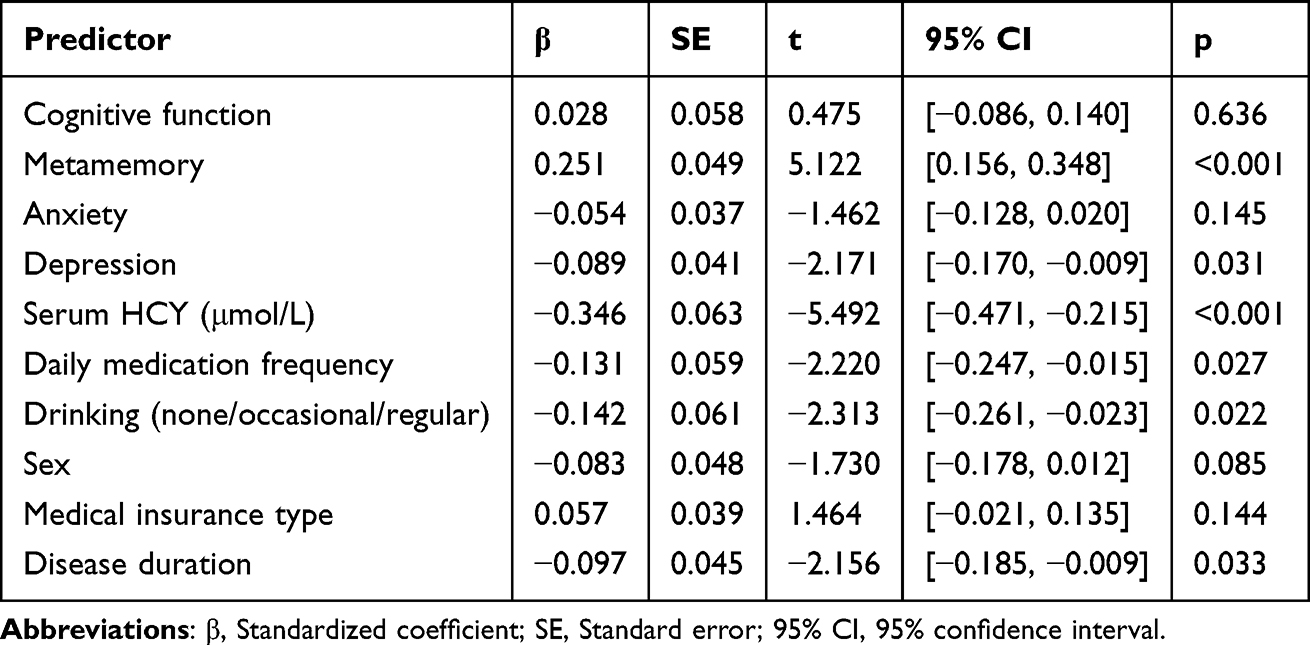 |
Table 4 Multiple Linear Regression Analysis of Factors Associated with Medication Adherence (Extended Model Including HCY) |
Discussion
This study investigated the relationships between cognitive function, metamemory, and emotional states in relation to medication adherence among older adults with H-type hypertension. Among 380 patients, the mean medication adherence score was 6.12 (SD = 1.63). Cognitive function and metamemory were modestly but significantly positively correlated with medication adherence (r = 0.196, p < 0.01; r = 0.235, p < 0.01). In the mediation model, the total effect of cognitive function on medication adherence was significant (β = 0.179, p = 0.001), but the direct effect became non-significant after adding mediators. Metamemory showed the strongest indirect effect (β = 0.164, 95% CI 0.109 to 0.225), while depressive symptoms exhibited a smaller but significant indirect pathway, and anxiety did not mediate the relationship. Although several associations were statistically significant, effect sizes were generally small, and practical implications should be interpreted cautiously. In the extended model including homocysteine level and daily medication frequency, metamemory, depressive symptoms and homocysteine remained significant predictors, whereas the direct path from cognition to medication adherence remained non-significant. Overall, these findings suggest that medication adherence in older adults with H-type hypertension is mainly mediated through metamemory and emotional factors and can be further modulated by biochemical and treatment-related burden factors.
In the current study, the majority (62.9%) of older adults with H-type hypertension had a low to moderate level of medication adherence, which is similar to the results of surveys conducted in China.29,30 Earlier research has consistently shown that older adults often face difficulties in maintaining regular medication-taking.31,32 These difficulties are frequently linked to age-related cognitive decline.33 They are also influenced by complex medication regimens and long disease duration. Together, these factors create persistent barriers to stable adherence. In our sample, metamemory scores were moderately low.34 Compared with community-dwelling older adults, the metamemory scores in our sample were noticeably lower.35 This pattern is biologically plausible, as both hypertension and elevated homocysteine levels are known to impair cognitive function,36 particularly in domains related to memory processing and executive control. Older adults with H-type hypertension may therefore have reduced awareness of their memory performance and lower confidence in their ability to manage memory-dependent tasks such as daily medication routines.37 Such characteristics may further weaken their ability to manage long-term medication routines. Emotional symptoms were also associated with medication adherence. Both depression and anxiety showed negative correlations with medication-taking. This result is consistent with previous reports from chronic disease populations.38,39 Prior studies have demonstrated that depressive symptoms can weaken motivation and reduce engagement in self-management.40 They can also interfere with the execution of health-related behaviours, including medication adherence.41 Within this context, the significant mediating role of metamemory in our study becomes meaningful. The smaller, but still significant, indirect effect of depressive symptoms further supports the idea that cognitive function and emotional status jointly influence adherence. These findings underline that both cognition-related factors and affective factors contribute to medication-taking behaviour in older adults with hypertension and comorbid conditions.
In this study, cognitive function showed a clear and consistent association with metamemory. The path coefficient from cognition to metamemory was strong, indicating that individuals with better cognitive abilities were more capable of monitoring and managing their memory processes. This finding is in line with theoretical assumptions that metamemory processes depend on basic cognitive resources, particularly attention and executive functioning.42 When these abilities are intact, individuals are more likely to notice potential memory failures and to adopt compensatory strategies.43 Metamemory also showed a robust association with medication adherence. Participants who reported higher awareness of their memory processes were more likely to follow their medication plans.44 This pattern supports the idea that metamemory acts as a behavioural “bridge” between cognition and daily health behaviours. Older adults who recognise their memory limitations may rely on external aids, structured routines or reminders to avoid forgetting medications.45 This pattern may help interpret why metamemory showed the strongest indirect association in our model among all psychological variables, metamemory could also plausibly moderate the association between cognitive function and adherence by buffering the impact of lower cognitive function, but moderation was not examined in the present study. Depressive symptoms also played a mediating role, although the effect size was smaller. The negative indirect association suggests that lower cognitive function was related to higher depressive symptoms, which were in turn related to poorer adherence. Depression has long been associated with low motivation, reduced initiation of health behaviours and difficulty sustaining long-term routines.46 These characteristics may explain why depressive symptoms weakened adherence in our sample. The effect was modest but statistically meaningful, suggesting that emotional processes should not be overlooked when designing adherence interventions. In contrast, anxiety did not significantly mediate the association between cognition and adherence. This may be related to the emotional expression style of older adults. Anxiety symptoms in the elderly often present as somatic complaints, which overlap with chronic disease manifestations.47 Such overlap may reduce the sensitivity of self-report anxiety scales and may contribute to underestimation of anxiety-related pathways. It is also possible that anxiety influences adherence through routes not captured in our model, such as risk perception or worry about treatment side effects.48 These possibilities should be explored in future research. Overall, the pattern observed in this study suggests that psychological mechanisms linking cognition and medication adherence are multifaceted. Metamemory plays a primary role, while depressive symptoms contribute additional explanatory power. Anxiety appears less influential in this context. Together, these findings highlight the importance of integrating both cognitive and emotional assessments when evaluating adherence in older adults with H-type hypertension.
In the extended model, several non-psychological variables remained significant predictors of medication adherence. Serum homocysteine (HCY) demonstrated a strong negative association with adherence. Higher HCY levels often reflect poorer vascular health and a greater disease burden, which may impose additional therapeutic requirements or physical discomfort. Patients with elevated HCY frequently face more complex treatment plans or more intensive medication regimens.49 These conditions increase the behavioural load associated with daily medication management, making it more difficult to sustain consistent adherence. The pronounced effect of HCY in our model suggests that physiological burden may be associated with weaker links between cognitive or psychological resources and adherence.50 Daily medication frequency also emerged as an independent predictor of adherence. Interestingly, higher dosing frequency was associated with better adherence, despite previous studies commonly reporting the opposite trend.51 In our sample, patients who required multiple daily doses were more often under structured management plans, such as combination therapy for H-type hypertension. These patients tended to receive regular follow-up and additional support from healthcare providers or family members. For them, higher dosing frequency may indicate more intensive disease management rather than greater behavioural burden. This finding illustrates that the behavioural meaning of dosing frequency can differ across clinical contexts. Alcohol consumption was another significant predictor. Participants who reported current or past drinking showed lower adherence levels, which is consistent with previous hypertension research.52 Alcohol use may disrupt daily routines, reduce self-regulatory capacity and weaken medication-taking behaviour. Our results support the view that lifestyle-related factors may interact with psychological processes and be associated with adherence. Although several demographic and clinical characteristics did not show significant group differences in the univariate analysis, they were still included in the extended regression model. Some factors, such as disease duration or insurance type, may not show direct associations individually but can act as structural confounders that influence the pathways linking cognition, psychological processes and adherence. Including these variables therefore helps ensure a more rigorous control of potential confounding and provides a clearer estimation of the psychological pathways. Taken together, the extended model demonstrates that cognitive and psychological pathways do not operate in isolation. They are shaped by disease burden, treatment complexity and lifestyle patterns. When overall burden is high, the direct association between cognition and adherence becomes weaker, and behavioural execution relies more on compensatory mechanisms such as metamemory and emotional regulation. These findings highlight the value of tailoring adherence interventions to both psychological characteristics and clinical demands. Integrating medical management with cognitive–behavioural support may help older adults maintain stable medication-taking routines.
From a practice perspective, these findings support the value of brief screening for metamemory difficulties and depressive symptoms when evaluating adherence risk in older adults with H type hypertension. In routine care, this may inform more targeted support strategies, such as medication counselling tailored to memory related challenges, use of reminder tools and structured routines, and coordination to simplify regimens where feasible. Community pharmacists may play an important role by identifying nonadherence risk during dispensing and follow-up, reinforcing medication instructions, and collaborating with physicians and nurses to address psychological and treatment burden factors that may hinder adherence. However, external validity should be considered. Because participants were recruited from a single tertiary hospital and represented a specific clinical population, the findings may not fully generalise to community dwelling older adults or primary care settings, where care pathways and adherence support resources differ. In addition, contextual factors not measured in this study, such as caregiver support, family involvement, health literacy, and social support, may influence medication adherence and should be incorporated in future research.
This study has several limitations. First, its cross-sectional design prevents causal inference, and all variables were assessed using self-report questionnaires, which may introduce recall and reporting bias. Second, the sample was drawn from a single tertiary hospital, limiting generalisability to other regions or primary-care populations. Third, although key clinical and behavioural covariates were included, other potentially influential factors such as caregiver support and treatment complexity were not measured. In addition, because key constructs were assessed using self-report measures at a single time point, common method variance may have inflated the observed associations. We attempted to minimise this risk through standardized administration by trained staff and by assuring participants of confidentiality, although no specific statistical test of common method variance was performed and residual bias cannot be excluded. Future studies should adopt multi-centre, longitudinal designs to validate these pathways and strengthen causal interpretation.
Conclusion
This study clarifies the associations between cognitive function and medication adherence in older adults with H-type hypertension, and the indirect associations via metamemory and depressive symptoms. The observed correlations were small in magnitude, and the models explained a moderate proportion of variance in adherence (R2=0.337 in the base mediation model and R2=0.464 after adding serum HCY), suggesting that additional contextual factors are likely to contribute. These findings should be interpreted in light of the modest effect sizes and the moderate explained variance. Metamemory showed the largest indirect association in the parallel mediation model, suggesting that self-monitoring and memory-related confidence may represent important correlates in the association between cognition and adherence. Depressive symptoms also played a significant negative mediating role, while anxiety showed no significant effect in this sample. The extended model further demonstrated that clinical burden factors, particularly serum HCY levels and daily medication frequency, contribute independently to adherence and may weaken the direct influence of cognition. These findings highlight the necessity of integrating cognitive support, emotional management and disease-related burden reduction into adherence-enhancing strategies for older adults with H-type hypertension.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Jiangnan University (approval number JNU20221201IRB04). Written informed consent was obtained from all participants prior to enrollment.
Data Sharing Statement
Deidentified individual participant data will be shared upon reasonable request from qualified researchers. The data to be shared include the variables used in the analyses reported in this article, including questionnaire scores and relevant demographic and clinical variables. A data dictionary describing variable definitions, coding, units, and handling of missing values will be provided. Additional documents, such as the study protocol and statistical analysis plan, may be made available where appropriate. Requests should be directed to the corresponding author (Lingxiang Guo; email: [email protected]). Data will be available after publication and will remain available for 12 months.
Acknowledgments
The authors would like to thank the nursing students who participated in this study for their time and valuable contributions.
Author Contributions
Gang Wu and Sixuan Li share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Institutional Research Grant Program for Young Scholars and Nursing Studies of Northern Jiangsu People’s Hospital (SBHL24007, SBHL24012, and SBHL24013).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Qin X, Huo Y. H‐Type hypertension, stroke and diabetes in China: opportunities for primary prevention. J Diabetes. 2016;8(1):38–14. doi:10.1111/1753-0407.12333
2. Qian X-L, Cao H, Zhang J, et al. The prevalence, relative risk factors and MTHFR C677T genotype of H type hypertension of the elderly hypertensives in Shanghai, China: a cross-section study: prevalence of H type hypertension. BMC Cardiovasc Disorders. 2021;21:1–10. doi:10.1186/s12872-021-02151-x
3. Zaric BL, Obradovic M, Bajic V, Haidara MA, Jovanovic M, Isenovic ER. Homocysteine and hyperhomocysteinaemia. Curr Med Chem. 2019;26(16):2948–2961. doi:10.2174/0929867325666180313105949
4. Liang Z, Fan FF, Zhang Y, Qin XH, Li JP, Huo Y. Rate and characteristics of H-type hypertension in Chinese hypertensive population and comparison with American population. Beijing da Xue Xue Bao Yi Xue Ban. 2022;54(5):1028–1037. doi:10.19723/j.issn.1671-167X.2022.05.033
5. Zhang X, Guo B, Zhu H, et al. H-type hypertension status and influencing factors of the elderly people over 80 years old based on random forest model. Int Heart Jl. 2024;65(2):263–270. doi:10.1536/ihj.23-488
6. Simon ST, Kini V, Levy AE, Ho PM. Medication adherence in cardiovascular medicine. BMJ. 2021;374. doi:10.1136/bmj.n1493
7. Lauffenburger JC, Isaac T, Bhattacharya R, Sequist TD, Gopalakrishnan C, Choudhry NK. Prevalence and impact of having multiple barriers to medication adherence in nonadherent patients with poorly controlled cardiometabolic disease. Am J Cardiol. 2020;125(3):376–382. doi:10.1016/j.amjcard.2019.10.043
8. Gow K, Rashidi A, Whithead L. Factors influencing medication adherence among adults living with diabetes and comorbidities: a qualitative systematic review. Curr Diabetes Rep. 2024;24(2):19–25. doi:10.1007/s11892-023-01532-0
9. Xiaolan F. Meta-memory. In: The ECPH Encyclopedia of Psychology. Springer; 2024:908.
10. Jacobs Ú, De Castro MS, Fuchs FD, Ferreira MB. The influence of cognition, anxiety and psychiatric disorders over treatment adherence in uncontrolled hypertensive patients. PLoS One. 2011;6(8):e22925. doi:10.1371/journal.pone.0022925
11. Wu G, Liu P, Zhang J, et al. Cognitive function and medication adherence in older adults with H-Type hypertension: the mediating effect of metamemory. J Gerontol Nurs. 2024;50(6):44–52. doi:10.3928/00989134-20240503-03
12. Asgedom SW, Atey TM, Desse TA. Antihypertensive medication adherence and associated factors among adult hypertensive patients at Jimma University Specialized Hospital, southwest Ethiopia. BMC Res Notes. 2018;11(1):27. doi:10.1186/s13104-018-3139-6
13. Bourque G, Ilin JV, Ruzicka M, Davis AS, Hiremath S. The prevalence of nonadherence in patients with resistant hypertension: a systematic review protocol. Can J Kidney Health Dis. 2019;6:2054358119897196. doi:10.1177/2054358119897196
14. Wu DF, Yin RX, Deng JL. Homocysteine, hyperhomocysteinemia, and H-type hypertension. Eur J Prev Cardiol. 2024;31(9):1092–1103. doi:10.1093/eurjpc/zwae022
15. Price BR, Wilcock DM, Weekman EM. Hyperhomocysteinemia as a risk factor for vascular contributions to cognitive impairment and dementia. Front Aging Neurosci. 2018;10:350. doi:10.3389/fnagi.2018.00350
16. Bandura A. Social cognitive theory: an agentic perspective. Annual Review of Psychology. 2001;52(1):1–26. doi:10.1146/annurev.psych.52.1.1
17. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
18. Katzman R, Zhang MY, Ouang Ya Q, et al. A Chinese version of the mini-mental state examination; impact of illiteracy in a Shanghai dementia survey. J Clin Epidemiol. 1988;41(10):971–978. doi:10.1016/0895-4356(88)90034-0
19. Wang Z, Zhang M. The application of the Chinese version of the Mini-Mental State Examination (MMSE). Shanghai Arch Psychiatry. 1989;7(3):108–111.
20. Troyer AK, Rich JB. Psychometric properties of a new metamemory questionnaire for older adults. J Gerontol B Psychol Sci Soc Sci. 2002;57(1):P19–27. doi:10.1093/geronb/57.1.p19
21. Jiang Y, Yang Y, Huang L, Li S, Liu B, Cao J. Reliability and vadility of Chinese version of the multifactorial MemoryQuestionnaire in middle and old aged community residents. J Nurs Sci. 2018;33(08):89–92.
22. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
23. Ding P, Shi H, Li B. Reliability and validity of the Chinese version of the MMAS-8 scale in patients with hypertension. Electronic J Clin Med Literature. 2017;4(39):7566–7567.
24. Ding P, Shi H, Li B. Evaluation of reliability and validity of the Chinese Version of the MMAS-8 scale in patients with hypertension. Electronic J Clin Med Literature. 2017;4(39):7566–7567. doi:10.16281/j.cnki.jocml.2017.39.028
25. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12(1):63–70. doi:10.1001/archpsyc.1965.01720310065008
26. Wang F, Yuan L, Li R, Xiong Z. Analysis of anxiety and depression status and influencing factors among hospitalized patients with type 2 diabetes. J Nurs Sci. 2015;22(14):28–31.
27. Dunstan DA, Scott N. Norms for Zung’s self-rating anxiety scale. BMC Psychiatry. 2020;20(1):1–8. doi:10.1186/s12888-019-2427-6
28. Wang XD, Wang XL, Ma H. Manual of mental health rating scales. Chin Mental Health J. 1999;13(1):31–35.
29. Hou Y, Zhang D, Gu J, et al. The association between self-perceptions of aging and antihypertensive medication adherence in older Chinese adults. Aging Clin Exp Res. 2016;28(6):1113–1120. doi:10.1007/s40520-015-0516-z
30. Ma C. A cross-sectional survey of medication adherence and associated factors for rural patients with hypertension. Appl Nurs Res. 2016;31:94–99. doi:10.1016/j.apnr.2016.01.004
31. Valenzuela-Beltrán M, Andrade ÁG, Stawarz K, Rodríguez MD. A participatory sensing study to understand the problems older adults faced in developing medication-taking habits. MDPI. 2022;1238.
32. Zhai S, Zhang Z, Zhang R, et al. Community-dwelling older adults’ perspectives on health risks: a qualitative study exploring anxieties, priorities, and expectations in ageing. BMC Public Health. 2024;24(1):1657. doi:10.1186/s12889-024-18878-z
33. Caruso MG, Nicolas S, Lucassen PJ, Mul JD, O’Leary OF, Nolan YM. Ageing, cognitive decline, and effects of physical exercise: complexities, and considerations from animal models. Brain Plast. 2024;9(1–2):43–73. doi:10.3233/BPL-230157
34. Gualtieri L, Rigby M, Wang D, Mann E. Medication management strategies to support medication adherence: interview study with older adults. Interactive J Med Res. 2024;13(1):e53513. doi:10.2196/53513
35. Jiang YY, Yang YN, Huang L, et al. Correlation between metamemory characteristics and depressive symptoms among community-dwelling middle-aged and older adults. Nurs Res. 2019;33:1–5.
36. Wan C, Zong R-Y, Chen X-S. The new mechanism of cognitive decline induced by hypertension: high homocysteine-mediated aberrant DNA methylation. Front Cardiovasc Med. 2022;9:928701. doi:10.3389/fcvm.2022.928701
37. de Menezes ST, Giatti L, Brant LCC, et al. Hypertension, prehypertension, and hypertension control: association with decline in cognitive performance in the ELSA-Brasil cohort. Hypertension. 2021;77(2):672–681. doi:10.1161/HYPERTENSIONAHA.120.16080
38. Khatooni M, Rahimi S, Bahrami M. The relationship between stress, anxiety, depression and medication adherence behavior in patients with epilepsy: a cross-sectional study. Epilepsy Behav. 2024;151:109616. doi:10.1016/j.yebeh.2023.109616
39. Wang T, Li Z, Wei Y, et al. Association between anxiety disorders and medication adherence in patients with cardiovascular disease: a systematic review and meta-analysis of observational studies. BMC Psychiatry. 2025;25(1):1–14. doi:10.1186/s12888-024-06458-9
40. Ould Brahim L, Lambert SD, Feeley N, et al. The effects of self-management interventions on depressive symptoms in adults with chronic physical disease (s) experiencing depressive symptomatology: a systematic review and meta-analysis. BMC Psychiatry. 2021;21(1):584. doi:10.1186/s12888-021-03504-8
41. Salvador Á, Mansuklal SA, Moura M, Crespo C, Barros L. Facilitators and barriers to adherence to medical recommendations among adolescents with cancer: a systematic review. J Child Health Care. 2025;29(2):501–522. doi:10.1177/13674935231208502
42. Yeung MK. Metamemory and executive function mediate the age-related decline in memory. J Int Neuropsychol Soc. 2024;30(5):479–488. doi:10.1017/S1355617723011451
43. Lencsés A, Mikula B, Mioni G, Rendell PG, Dénes Z, Demeter G. Prospective memory functions in traumatic brain injury: the role of neuropsychological deficits, metamemory and impaired self‐awareness. J Neuropsychol. 2025;19(1):51–66. doi:10.1111/jnp.12388
44. Chin J, Wang H, Awwad AW, Graumlich JF, Wolf MS, Morrow DG. Health literacy, processing capacity, illness knowledge, and actionable memory for medication taking in type 2 diabetes: cross-sectional analysis. J Gen Intern Med. 2021;36(7):1921–1927. doi:10.1007/s11606-020-06472-z
45. Ross SD, Hofbauer LM, Rodriguez FS. Coping strategies for memory problems in everyday life of people with cognitive impairment and older adults: a systematic review. Int J Geriatric Psychiatry. 2022;37(5). doi:10.1002/gps.5701
46. Lu Z, Yu L, Fan K, et al. Associations between social support and proactive health behaviours among Chinese adolescents: the mediating role of self-efficacy and peer relationships. BMC Public Health. 2024;24(1):2548. doi:10.1186/s12889-024-20070-2
47. Howell C, Segal DL, Segal S. Diagnosis and assessment of somatic symptom and related disorders among older adults: issues and strategies. J Clin Basic Psychosomatics. 2025;025080013.
48. Fan Y, Shen BJ, Tay HY. Depression, anxiety, perceived stress, and their changes predicted medical adherence over 9 months among patients with coronary heart disease. British J Health Psychol. 2021;26(3):748–766. doi:10.1111/bjhp.12496
49. González-Lamuño D, Arrieta-Blanco FJ, Fuentes ED, et al. Hyperhomocysteinemia in adult patients: a treatable metabolic condition. Nutrients. 2023;16(1):135. doi:10.3390/nu16010135
50. Clemente-Suárez VJ, Martín-Rodríguez A, Curiel-Regueros A, Rubio-Zarapuz A, Tornero-Aguilera JF. Neuro-nutrition and exercise synergy: exploring the bioengineering of cognitive enhancement and mental health optimization. Bioengineering. 2025;12(2):208. doi:10.3390/bioengineering12020208
51. Baryakova TH, Pogostin BH, Langer R, McHugh KJ. Overcoming barriers to patient adherence: the case for developing innovative drug delivery systems. Nat Rev Drug Discov. 2023;22(5):387–409. doi:10.1038/s41573-023-00670-0
52. Choudhry NK, Kronish IM, Vongpatanasin W, et al. Medication adherence and blood pressure control: a scientific statement from the American Heart Association. Hypertension. 2022;79(1):e1–e14. doi:10.1161/HYP.0000000000000203
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Muscle Ultrasound Parameters and Cognitive Function in H‑type Hypertension: A Cross-Sectional Study
Weng XF, Li ST, Cui Y, Yang YL, Xie Z, Hu JY, Liu SW, Hu H, Wu YH, Mo LY
Clinical Interventions in Aging 2026, 21:615425
Published Date: 9 July 2026