Back to Journals » Infection and Drug Resistance » Volume 16
Multiplex Polymerase Chain Reaction/Pooled Antibiotic Susceptibility Testing Was Not Associated with Increased Antibiotic Resistance in Management of Complicated Urinary Tract Infections
Authors Korman HJ, Mathur M, Luke N ![]() , Wang D
, Wang D ![]() , Zhao X, Levin M, Wenzler DL, Baunoch D
, Zhao X, Levin M, Wenzler DL, Baunoch D
Received 14 February 2023
Accepted for publication 3 May 2023
Published 9 May 2023 Volume 2023:16 Pages 2841—2848
DOI https://doi.org/10.2147/IDR.S406745
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Howard J Korman,1 Mohit Mathur,2 Natalie Luke,2 Dakun Wang,3 Xihua Zhao,4 Michael Levin,1 David L Wenzler,1 David Baunoch5
1Comprehensive Urology Division, Michigan Healthcare Professionals, Royal Oak, MI, USA; 2Department of Medical Affairs, Pathnostics, Irvine, CA, USA; 3Department of Writing, Stat4Ward, Pittsburgh, PA, USA; 4Department of Statistical Analysis, Stat4Ward, Pittsburgh, PA, USA; 5Department of Research and Development, Pathnostics, Irvine, CA, USA
Correspondence: Mohit Mathur, Pathnostics, 15545 Sand Canyon Suite 100, Irvine, CA, 92618, USA, Email [email protected]
Objective: To compare antibiotic resistance results at different time points in patients with urinary tract infections (UTIs), who were either treated based upon a combined multiplex polymerase chain reaction (M-PCR) and pooled antibiotic susceptibility test (P-AST) or were not treated.
Methods: The M-PCR/P-AST test utilized here detects 30 UTI pathogens or group of pathogens, 32 antibiotic resistance (ABR) genes, and phenotypic susceptibility to 19 antibiotics. We compared the presence or absence of ABR genes and the number of resistant antibiotics, at baseline (Day 0) and 5– 28 days (Day 5– 28) after clinical management in the antibiotic-treated (n = 52) and untreated groups (n = 12).
Results: Our results demonstrated that higher percentage of patients had a reduction in ABR gene detection in the treated compared to the untreated group (38.5% reduction vs 0%, p = 0.01). Similarly, significantly more patients had reduced numbers of resistant antibiotics, as measured by the phenotypic P-AST component of the test, in the treated than in the untreated group (42.3% reduction vs 8.3%, p = 0.04).
Conclusion: Our results with both resistance gene and phenotypic antibiotic susceptibility results demonstrated that treatment based upon rapid and sensitive M-PCR/P-AST resulted in reduction rather than induction of antibiotic resistance in symptomatic patients with suspected complicated UTI (cUTI) in an urology setting, indicating this type of test is valuable in the management of these types of patients. Further studies of the causes of gene reduction, including elimination of ABR gene-carrying bacteria and loss of ABR gene(s), are warranted.
Keywords: urinary tract infection, complicated urinary tract infection, antibiotic resistance, antibiotic resistance genes, diagnostic testing, polymerase chain reaction
Introduction
PCR-based diagnostic tests can reduce the time to results and improve sensitivity, but there are concerns that the increased sensitivity may lead to overtreatment and increase in antibiotic resistance, potentially preventing its wide clinical use for the diagnosis of complicated UTIs (cUTIs).1–5
The rapid increase of resistant bacterial strains due to the overuse of antibiotics is one of the most serious health threats worldwide.6–8 The bacterial population can resist antibiotics through a variety of mechanisms, including acquiring antibiotic resistance (ABR) genes, mutations to chromosomal target genes, active removal of drugs by efflux pumps, inactivation, or degradation of antibiotics, modifying bacterial cell wall to prevent antibiotics from reaching their target sites, and building biofilms.9 To combat this health challenge, antimicrobial stewardship programs endorsed by the Centers for Disease Control and prevention (CDC) and World Health Organization (WHO), have been implemented to improve appropriate antibiotic utilization. Timely diagnosis and appropriate antibiotic selection are critical components of these antimicrobial stewardship programs.10,11
UTIs are a leading cause for antibiotic prescriptions and a significant healthcare problem in the US, accounting for 10.5 million office visits and over $3.5 billion in healthcare costs per year.12–16 While simple UTIs can be managed successfully with outpatient antibiotics, patients with complicated UTIs (cUTIs) have higher treatment failure rates and poor outcomes, including UTI recurrence.
A typical initial diagnostic for UTIs is dipstick urinalysis, which provides rapid results and in conjunction with clinical findings can inform management decisions. In many cases, empiric broad spectrum antimicrobial therapy is initiated.17 The selection of empiric antibiotics depends on susceptibility of prior urinary isolates, patient clinical circumstances (such as allergy, drug interaction, expected compliance, and tolerability), hospital and local community antibiotic resistance patterns, and other factors.18 For cUTIs in the outpatient setting, current guidelines (Infectious Diseases Society of America and European Society of Clinical Microbiology and Infectious Diseases) recommend the use of oral fluoroquinolones (such as ciprofloxacin), and oral amoxicillin-clavulanate potassium (AMC), cephalosporin, and trimethoprim-sulfamethoxazole (TMP-SMX) as alternatives.19 Nitrofurantoin, is restricted to cUTIs that only involve the lower genitourinary tract.20 Increased resistance to all of these antibiotics has been observed, raising the risk of choosing an empirical antibiotic to which an infecting pathogen is resistant.20,21
For many cUTI patients, physicians will also order a standard urine culture (SUC) with antibiotic susceptibility testing (AST). SUC is the accepted standard method to identify UTI pathogens, but it is time-consuming, with identification of pathogens taking 24 to 48 hours and AST needing an additional 18 to 24 hours. SUC also has significant limitations including poor growth of fastidious organisms and inability to grow out polymicrobial sets of organisms.22–24 This results in limited sensitivity and a high frequency of false negative and inconclusive results for patient management.24,25
A focus on improving how physicians diagnose UTIs is integral to improving UTI antibiotic stewardship. Recently more advanced tests have emerged with the potential to aid UTI diagnosis and make bacterial identification and antibiotic susceptibility evaluation faster and simpler. The M-PCR/P-AST test studied here is one such test, using both multiplexed PCR technology for detecting and quantifying 23 bacteria and 4 yeast organisms, 3 bacterial groups, and 32 resistance genes and Pooled Antibiotic Susceptibility Testing (P-AST), to provide phenotypic susceptibility results for organisms present in the urine sample. Results of the test are routinely available within 24 hours thus can decrease the need for empirical antibiotic treatment. Clinical studies have demonstrated its superiority in detecting specific bacteria, including E. coli and other Gram-negative bacteria, Gram-positive bacteria, and polymicrobial infections, capturing the impacts of bacterial interactions for more reliable susceptibility results and with a faster turnaround time,21,26,27 compared with SUC. In addition, Daly et al showed that the patients treated based on the M-PCR/P-AST test results were associated with a 13.7% decrease in emergency department (ED) visits and/or hospital admissions compared to the patients based on the SUC results.28
The inherent sensitivity of PCR for identification of organisms raises the potential for overtreatment leading to increased antibiotic resistance instead of reducing it. Some important factors to consider are the selection of organisms in the PCR panel corresponding to known UTI pathogens, and the use of the test in a specialist setting where management of cUTIs is standard. This study compares the detections of ABR genes and the number of resistant antibiotics for cUTI cases in an urology setting using the M-PCR/P-AST test, at baseline and after clinical management with or without antibiotics.
Materials and Methods
Study Design and Participants. This is an interim analysis of an ongoing observational, prospective study that aims to investigate the impact of an M-PCR/P-AST test (Guidance® UTI, performed by Pathnostics, Irvine) in the clinical management of cUTI by measuring ABR gene and phenotypic resistance changes with and without treatment. Study subject inclusion criteria included 18 years or older, male or female patients presenting to urology clinics with symptoms and clinical presentations highly suspicious of cUTI (see Supplemental Table 1 for full Inclusion and Exclusion Criteria). Exclusion criteria included lack of UTI symptoms, antibiotics use for any reason other than UTI at the time of enrollment, urinary diversion, presence of chronic (≥ 10 days) indwelling catheters, and self-catheterization at the time of consultation. This study was conducted in accordance with the Declaration of Helsinki. The study protocol was reviewed and approved by WCG IRB (20214705) Trial registration: NCT05091931. Registered 25 October 2021, https://clinicaltrials.gov/ct2/show/NCT05091931. All subjects gave verbal informed consent prior to enrollment because the WCG IRB determined the study protocol satisfied three requirements for partial waiver of authorization under 45 CFR 164.512 including the use of protected health information (PHI) involved no more than minimal risk to the study participants, the research could not be practicably conducted without access to PHI, and the research could not practicably be conducted without the waiver.
Subject urine samples were collected via midstream clean catch or in-and-out catheterization for the M-PCR/P-AST testing on the day of enrollment. (Day 0) The clinical treatment plan for each subject was determined by the clinicians with the knowledge of the M-PCR/P-AST testing results and was recorded as part of the study. A second urine sample was collected between Days 5 and 28 (Day 5–28) and tested again with M-PCR/P-AST. In this interim analysis, only subjects with M-PCR/P-AST test results on both Day 0 and Day 5–28 AND positive uropathogen detection on Day 0 were included (N = 64). Patient’s treatment was at the discretion of the clinician. Treatment status was determined based on the clinical evaluation form completed by physicians, patients’ daily surveys, and medical records. The terms “treated” and “untreated” indicate whether or not the patient was treated with antibiotics between Day 0 and Day 2. M-PCR/P-AST test results were compared between Day 0 and Day 5–28 in these patients in treated (with antibiotics) (n = 52), and untreated (without antibiotics) (n = 12) groups, respectively.
M-PCR/P-AST. The uropathogen detection by M-PCR was performed as previously described, with the exceptions of the use of Bacillus atrophaeus as an inhibition control and inclusion of probes and primers to detect Gardnerella vaginalis.20,28,29
Bacterial positive samples were analyzed for their presence of ABR genes by M-PCR, including 32 ABR genes in 6 classes: ampicillin resistance genes (AmpC, FOX, ACC, DHA, MOX/CMY, and BIL/LAT/CMY), 2) extended-spectrum beta-lactamases (ESBL) resistance genes (CTX-M group 1, CTX-M group 2, CTX-M group 8/25, CTX-M group 9, OXA-1, SHV, TEM, VEB, GES, PER-1 and PER-2), 3) Methicillin resistance genes (mecA), 4) quinolone and fluoroquinolone resistance genes (QnrA and QnrS), 5) vancomycin resistance genes (vanA1, vanA2, and vanB), and 6) carbapenems resistance genes (IMP-1 group, KPC, OXA-23, OXA-40, blaOXA-48, VIM, IMP-7, IMP-16, and OXA-72).
The P-AST component was performed, as described previously.20 Briefly, the cell pellet from a 1 mL aliquot of patient urine sample was suspended in 1 mL of Mueller Hinton Growth Media and incubated at 35°C in a non-CO2 incubator for 6 h. Samples reaching a minimum threshold of 10,000 cells/mL were diluted 1:100 with growth media and used to inoculate 96-well plates preloaded with antibiotics then incubated for 12–16 hours at 35°C in a single layer. The optical density of samples was read on a DensiCHEK plate reader™ (BioMerieux, Marcy-l’Étoile, France).
Statistical Analysis. Subject demographics, including age and sex, and clinical information, including urine collection method, days between baseline (Day 0) and second collection (Day 5–28), and treatment status, were summarized using mean (SD) for continuous variables and frequency (proportion) for dichotomized variables. Changes in ABR gene presence were classified as reduced (number of ABR gene detected on Day 5–28 < number of ABR gene detected on Day 0), no change (number of ABR gene detected on Day 5–28 = number of ABR gene detected on Day 0), or gained (number of ABR gene detected on Day 5–28 > number of ABR gene detected on Day 0) between the treated and untreated groups. The above analyses were replicated for numbers of antibiotics reported as resistant on Day 0 and Day 5–28 by P-AST and compared between the treated and untreated groups. Changes were classified as reduced (number of resistant antibiotics detected on Day 5–28 < number of resistant antibiotics detected on Day 0), no change (number of resistant antibiotics detected on Day 5–28 = number of resistant antibiotics detected on Day 0) or gained (number of resistant antibiotics detected on Day 5–28 > number of resistant antibiotics detected on Day 0). The Fisher’s Exact test was used to determine if the presence of ABR genes and the number of resistant antibiotics, respectively, differed statistically (p < 0.05) between the treated and untreated groups. The population size was not large enough to perform a multivariate analysis. However, we have compared the age, sex, and days between baseline and second collection, and found that the treated and untreated groups are similar.
Results
Patient Demographics. A total of 64 subjects (65.6% female and 34.4% male) enrolled between 06/13/2022 and 8/16/2022 were included in this interim analysis. The average age of these patients was 70.1 years. The urine samples were collected via midstream clean catch. The length between the initial and the second urine collection ranged between 5 and 28 days, with an average length of 15.1 days and the majority (64.1%) between 7 and 15 days. Most patients (52, 81.3%) were treated, while 12 (18.8%) were not treated with antibiotics as part of the clinical management plan (Table 1).
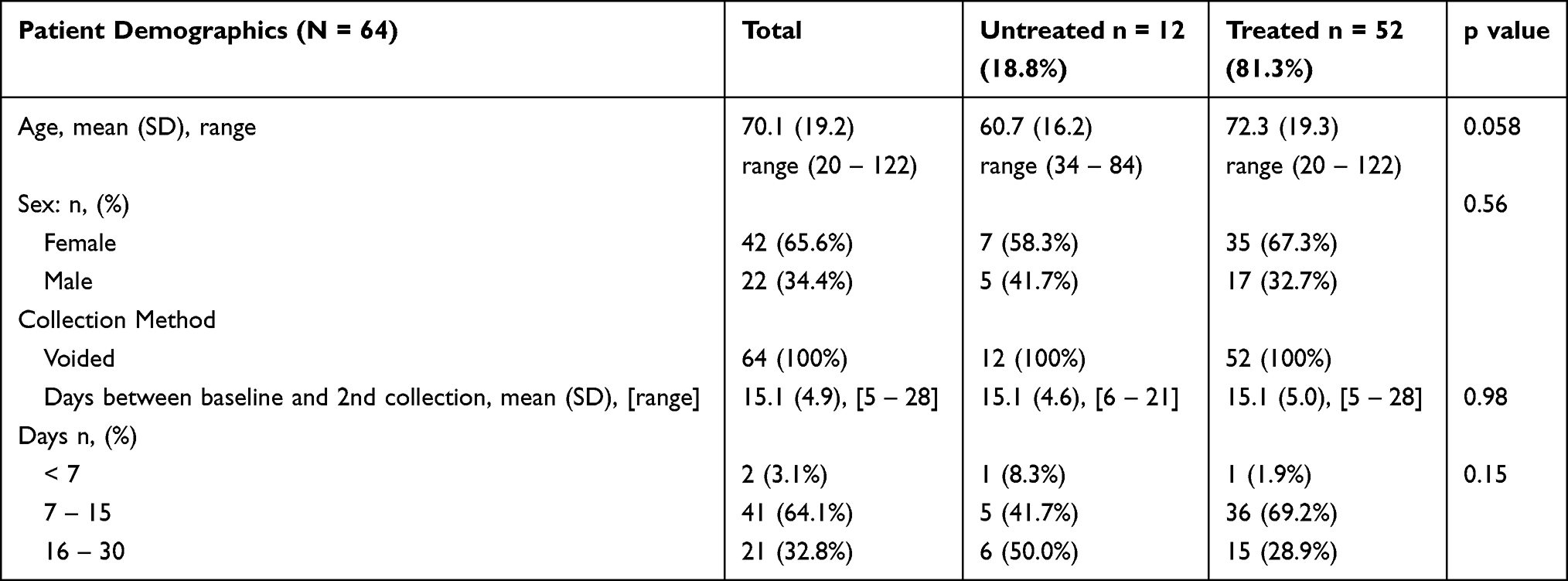 |
Table 1 Patient Demographic and Clinical Information |
Overall changes of ABR gene detection from Day 0 to Day 5–28 in treated and untreated patients. We evaluated the overall presentation of any of the 32 ABR genes and the presentation of each of the six classes of ABR genes. Among the 64 symptomatic patients highly suspicious of cUTI, we detected no carbapenem or vancomycin resistance genes and only two patients with quinolone/fluoroquinolone resistance genes. For each patient, we compared the ABR genes detection status (unchanged, reduced, or gained) between the initial and second collections for the treated (n = 52) and untreated (n = 12) group, respectively (Table 2). In the untreated group the number of ABR genes was unchanged in 9 (75.0%), reduced in 0 (0%), and gained in 3 (25.0%) cases. In the treated group, the number of resistance genes were unchanged in 21 (40.4%), reduced in 20 (38.5%), and gained in 11 (21.2%) cases. The status of the ABR genes in the treated and the untreated group differ significantly in the overall distribution of the three categories (p = 0.01), with higher percent of patients with ABR genes reduced in the treated than untreated group (38.5% vs 0%, p = 0.01) and similar distribution in the unchanged (p = 0.05) and the gained category (p = 0.72) (Table 2).
 |
Table 2 ABR Gene Detection Status, Unchanged, Reduced, or Gained After Clinical Management in Treated and Untreated Groups, Compared to the Baseline |
Overall changes of the numbers of antibiotics reported by Guidance® UTI as resistant on Day 0 and Day 5–28 in treated and untreated patients. In addition to detecting microbes and ABR gene by M-PCR, the test evaluated phenotypic antibiotic susceptibilities using P-AST (reported as resistant or sensitive) to 19 common UTI antibiotics. We compared the numbers of antibiotics reported as resistant by P-AST on Day 0 and Day 5–28 (unchanged, reduced, or gained) for patients in the treated (n = 52) and untreated (n = 12) groups (Table 3). In the treated group, most patients (22, 42.3%) illustrated a reduction in the number of resistant antibiotics, with 9 (17.3%) and 21 (40.4%) patients showing an unchanged and increased number of resistant antibiotics, respectively. In the untreated group, most patients (8, 66.7%) increased numbers of resistant antibiotics, with 1 (8.3%) and 3 (25.0%) patients showing a reduced and unchanged number of resistant antibiotics, respectively. The number of resistant antibiotics in the treated and untreated cohorts was similar in the overall distribution of the three categories (p = 0.07); however, significantly more patients had reduced numbers of resistant antibiotics in the treated than in the untreated group (42.3% vs 8.3%, p = 0.04), with no significant difference detected between the unchanged and gained groups (Table 3).
 |
Table 3 The Numbers of Antibiotics Reported as Resistant by P-AST per Patient (Unchanged, Reduced or Gained) After Clinical Management in Treated and Untreated Groups, Compared to the Baseline |
Discussion
Culture-independent molecular diagnostics tests are revolutionizing the clinical practice of infectious disease, especially in specialty outpatient settings, where timely and accurate diagnostic tools are critical for patient therapeutic decisions and outcomes.1 Compared with SUC, PCR-based testing is better able to detect polymicrobial UTI infections and non-E. coli Gram-negative and Gram-positive bacteria, which have been shown to cause UTIs.25 In addition to providing organism identification and genetic resistance gene information, by M-PCR/P-AST, evaluates phenotypic antibiotic susceptibility of the detected uropathogens. Both genotypic results with PCR (ID and resistance genes) plus phenotypic P-AST results are important to guide management decisions for patients. Clinicians need to both know which organisms are present, with cell density, and which antibiotics the pool of organisms in the urine sample are sensitive to. Identification of the organism by M-PCR is essential to the success of P-AST because the organism identity determines the concentration of antibiotic used in susceptibility testing. Additionally, organism identity informs the clinical application of susceptibility results. Since there is a 40% discordance between resistance gene and phenotypic information, P-AST is a critical component of the test.26
This comprehensive information, provided by M-PCR/P-AST testing, usually available within 24 hours, allows for the timely selection of directed antibiotic treatment, reducing the need for empiric treatment with broad-spectrum antibiotics, which may be ineffective and increases antibiotic resistance over time. Indeed, Daly et alshowed that patients treated based on M-PCR/P-AST were associated with better outcomes, including fewer ED visits and/or hospital admissions compared to patients treated based on SUC.20 The aim of this analysis was to address the concern that the sensitivity of M-PCR/P-AST could result in increased antibiotic resistance. The power level was sufficient for composite analysis, but not for individual gene analysis.
The status of the ABR genes in the treated and the untreated group differed significantly in the overall distribution between reduced, unchanged, and gained. The treated patients had more cases end up with reduced ABR genes after treatment at Day 5–28 than the untreated patients at Day 5–28. This reduction may result from of the elimination of ABR gene-carrying bacteria and/or loss of the gene(s).
The presence or absence of genes does not always indicate sensitivity or resistance. Several other mechanisms are involved in manifesting resistance in a pooled population of bacteria. One of our previous studies demonstrated 40% discordance between ABR gene detection and antibiotic susceptibility.29 The test used in this study detects phenotypic antibiotic susceptibility component with P-AST, which allowed comparison of the numbers of resistant antibiotics in the treated and the untreated group. Similarly to the ABR findings, the number of resistant antibiotics in the treated group was also reduced compared to the untreated group. Overall, both ABR gene detection and antibiotic susceptibility level demonstrated that treating patients based on M-PCR/P-AST results was not associated with an increase of resistance, and indeed demonstrated a reduction in antibiotic resistance in treated patients as compared to untreated patients. These results indicate that utilization of this type of advanced UTI test, which incorporates both genotypic and pooled susceptibility results, can be beneficial when used by specialists for complicated UTI infections, instead of being harmful.
Study limitations include a small sample size, resulting in an inability to study the relationship between classes of antibiotics or comparing the effects of empirical treatment vs directed treatment on ABR gene detection. In addition, even though the 32 ABR genes included in the evaluation in our study are among the most well studied ABR genes associated with resistance to common antibiotics used to treat UTI, other potentially important ABR genes exist. A more extensive study with an increased number of patients is underway to better decipher the changes in the detection of specific ABR genes and susceptibility to individual antibiotics and their relationships with treatment responses.
Conclusion
In summary, utilizing an advanced diagnostic, which includes M-PCR and P-AST components for management of cUTIs was not associated with increased antibiotic resistance after treatment compared to patients who were not treated. In fact, these results also show an increased fraction of cases that had decreased resistance after treatment compared to the untreated patients. Utilization of the M-PCR/P-AST test was beneficial in these cases, by reducing instead of increasing resistance, indicating its use should be considered for complicated UTIs.
Data Sharing Statement
All relevant data are present within the manuscript text and tables.
Ethics Approval and Consent to Participate
All patients provided verbal informed consent (Western IRB 20214705) prior to enrollment.
Funding
Pathnostics and Thermo Fisher funded the study.
Disclosure
D.B., N.L., and M.M. are employees of Pathnostics, and HJK, D. Wa. and X.Z. are paid consultants for Pathnostics. Dr Natalie Luke reports grants from Thermofisher, during the conduct of the study. In addition, Dr Natalie Luke has a patent US 10,160,991 issued to Pathnostics, a patent US 11,053,532 issued to Pathnostics, a patent US 17/178,091 pending to Pathnostics, a patent US 17/335,767 pending to Pathnostics, a patent US 17/830,227 pending to Pathnostics, a patent PCT/US22/16816 pending to Pathnostics, a patent PCT/US22/77477 pending to Pathnostics, a patent AU 2018254514 B2 issued to Pathnostics, a patent BR112019021943-9 B1 issued to Pathnostics, a patent NZ 759292 issued to Pathnostics, a patent EP 3612638 pending to Pathnostics, a patent JP 2020-507493 pending to Pathnostics, a patent JP 2022-042545 pending to Pathnostics, a patent CA 3,175,879 pending to Pathnostics, a patent CA 3,176,586 pending to Pathnostics, a patent CA 3,061,015 pending to Pathnostics, a patent HK 62020014337.3 pending to Pathnostics, a patent CN 201880039956.9 pending to Pathnostics, a patent IL 294577 pending to Pathnostics. Dr David L Wenzler reports grants, personal fees from Pathnostics, during the conduct of the study. Dr David Baunoch reports a patent US 10,160,991 issued to PATHNOSTICS, a patent US 11,053,532 issued to PATHNOSTICS, a patent US 17/178,091 pending to PATHNOSTICS, a patent US 17/830,227 pending to PATHNOSTICS, a patent US 17/335/767 pending to PATHNOSTICS, a patent PCT/US22/16816 pending to PATHNOSTICS, a patent PCT/US22/77477 pending to PATHNOSTICS, a patent AU 2018254514 B2 issued to PATHNOSTICS, a patent BR112019021943-9 B1 issued to PATHNOSTICS. The authors report no other conflicts of interest in this work.
References
1. Chang SS, Hsieh WH, Liu TS, et al. Multiplex PCR system for rapid detection of pathogens in patients with presumed sepsis – a systemic review and meta-analysis. PLoS One. 2013;8(5):e62323. doi:10.1371/journal.pone.0062323
2. Florio W, Morici P, Ghelardi E, Barnini S, Lupetti A. Recent advances in the microbiological diagnosis of bloodstream infections. Crit Rev Microbiol. 2017;44(3):1–20. doi:10.1080/1040841x.2017.1407745
3. Scerbo MH, Kaplan HB, Dua A, et al. Beyond blood culture and gram stain analysis: a review of molecular techniques for the early detection of bacteremia in surgical patients. Surg Infect. 2016;17(3):294–302. doi:10.1089/sur.2015.099
4. Gayet-Ageron A, Combescure C, Lautenschlager S, Ninet B, Perneger TV. Comparison of Diagnostic Accuracy of PCR Targeting the 47-kilodalton protein membrane gene of Treponema pallidum and PCR Targeting the DNA polymerase I gene: systematic review and meta-analysis. J Clin Microbiol. 2015;53(11):3522–3529. doi:10.1128/jcm.01619-15
5. Zboromyrska Y, Diagnostics VJ. Review of molecular. Advanced PCR-based molecular diagnosis of gastrointestinal infections: challenges and opportunities. Expert Rev Mol Diagn. 2016;16(6):631–640. doi:10.1586/14737159.2016.1167599
6. Prestinaci F, Pezzotti P, Pantosti A. Antimicrobial resistance: a global multifaceted phenomenon. Pathog Glob Health. 2015;109(7):309–318. doi:10.1179/2047773215y.0000000030
7. Gould IM. A review of the role of antibiotic policies in the control of antibiotic resistance. J Antimicrob Chemoth. 1999;43(4):459–465. doi:10.1093/jac/43.4.459
8. Harbarth S, Samore MH. Antimicrobial resistance determinants and future control. Emerg Infect Dis. 2005;11(6):794–801. doi:10.3201/eid1106.050167
9. Peri L. Fighting urinary tract infections with antibiotic and non-antibiotic therapies. Urologia J. 2016;83(1_suppl):5–10. doi:10.5301/uro.5000186
10. Abbott IJ, Peel TN, Cairns KA, Stewardson AJ. Antibiotic management of UTI in the post-antibiotic era: a narrative review highlighting diagnostic and antimicrobial stewardship. Clin Microbiol Infec. 2022. doi:10.1016/j.cmi.2022.05.016
11. Goebel MC, Trautner BW, Grigoryan L. The five ds of outpatient antibiotic stewardship for urinary tract infections. Clin Microbiol Rev. 2021;34(4):e00003–20. doi:10.1128/cmr.00003-20
12. Aabenhus R, Hansen MP, Siersma V, Bjerrum L. Clinical indications for antibiotic use in Danish general practice: results from a nationwide electronic prescription database. Scand J Prim Health. 2017;35(2):162–169. doi:10.1080/02813432.2017.1333321
13. Mireles F. Nature reviews microbiology - supplement.pdf; 2015.
14. Siff LN. Recurrent urinary tract infections. Deckermed Obstetrics Gynecol. 2021. doi:10.2310/obg.19160
15. Wagenlehner FM, Lichtenstern C, Rolfes C, et al. Diagnosis and management for urosepsis. Int J Urol. 2013;20(10):963–970. doi:10.1111/iju.12200
16. NCBI Bookshelf. Complicated urinary tract infections. StatPearls - NCBI Bookshelf. Available from: https://www.ncbi.nlm.nih.gov/books/NBK436013/.
17. Waller TA, Pantin SAL, Yenior AL, Pujalte G. Urinary tract infection antibiotic resistance in the United States. Prim Care Clin Office Pract. 2018;45(3):455–466. doi:10.1016/j.pop.2018.05.005
18. Acute complicated urinary tract infection (including pyelonephritis) in adults - UpToDate. Available from: https://www.uptodate.com/contents/acute-complicated-urinary-tract-infection-including-pyelonephritis-in-adults?search=complicated-urinary%20tract%20infection%20including%20pyelonephritis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
19. Ong LT. Antibiotics for complicated urinary tract infection and acute pyelonephritis: a systematic review. World J Clin Infect Dis. 2020;10(3):33–41. doi:10.5495/wjcid.v10.i3.33
20. Wojno KJ, Baunoch D, Luke N, et al. Multiplex PCR Based Urinary Tract Infection (UTI) analysis compared to traditional urine culture in identifying significant pathogens in symptomatic patients. Urology. 2019;136:119–126. doi:10.1016/j.urology.2019.10.018
21. Vollstedt A, Baunoch D, Wolfe A, et al. Bacterial interactions as detected by pooled antibiotic susceptibility testing (P-AST) in polymicrobial urine specimens. J Sur Urology. 2020;203(101). doi:10.29011/jsu-101.100001
22. Khasriya R, Sathiananthamoorthy S, Ismail S, et al. Spectrum of bacterial colonization associated with urothelial cells from patients with chronic lower urinary tract symptoms. J Clin Microbiol. 2013;51(7):2054–2062. PMID: 23596238; PMCID: PMC3697662. doi:10.1128/JCM.03314-12
23. Folaranmi T, Harley C, Jolly J, Kirby A. Clinical and microbiological investigation into mixed growth urine cultures. J Med Microbiol. 2022;71. doi:10.1099/jmm.0.001544
24. Price TK, Dune T, Hilt EE, et al. The clinical urine culture: enhanced techniques improve detection of clinically relevant microorganisms. J Clin Microbiol. 2016;54:1216–1222. doi:10.1128/JCM.00044-16
25. Price TK, Hilt EE, Dune TJ, et al. Urine trouble: should we think differently about UTI? Int Urogynecol J. 2018;29(2):205–210. doi:10.1007/s00192-017-3528-8
26. Vollstedt A, Baunoch D, Wojno KJ, et al. Multisite prospective comparison of multiplex polymerase chain reaction testing with urine culture for diagnosis of urinary tract infections in symptomatic patients. J Sur Urology. 2020;102. doi:10.29011/jsu-102.100002
27. Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the infectious diseases society of America and the European Society for microbiology and infectious diseases. Clin Infect Dis. 2011;52(5):e103–e120. doi:10.1093/cid/ciq257
28. Daly A, Baunoch D, Rehling K, et al. Utilization of M-PCR and P-AST for diagnosis and management of urinary tract infections in home-based primary care. JOJ Uro Nephron. 2020;7(2):555707. doi:10.19080/jojun.2020.07.555707
29. Baunoch D, Luke N, Wang D, et al. concordance between antibiotic resistance genes and susceptibility in symptomatic urinary tract infections. Infect Drug Resist. 2021;14:3275–3286. doi:10.2147/idr.s323095
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Diagnostic Test Combining Molecular Testing with Phenotypic Pooled Antibiotic Susceptibility Improved the Clinical Outcomes of Patients with Non-E. coli or Polymicrobial Complicated Urinary Tract Infections
Korman HJ, Baunoch D, Luke N, Wang D, Zhao X, Levin M, Wenzler DL, Mathur M
Research and Reports in Urology 2023, 15:141-147
Published Date: 1 May 2023
Sociodemographic and Clinical Correlates of Multidrug-Resistant Uropathogens in Hospitalized Children
Muhsen K, Haleem S, Mansour B, Shapira M, Pitashny M, Masarwa M, Omar M, Na’aminh W, Kassem E
Infection and Drug Resistance 2026, 19:588989
Published Date: 8 April 2026
Bacteriological Profile and Antibiotic Resistance Patterns of Uropathogenic Bacteria at HPGRB
Cito B, Corneille KA, Gates IM, Bruno KK, Ruhimbasa KC, Gloire MH, Bahaya J, Kawala ZL, Makeshe OM, Lupande Mwenebitu D
Infection and Drug Resistance 2026, 19:603097
Published Date: 20 April 2026