Back to Journals » Infection and Drug Resistance » Volume 16
Multiple Lung Cavity Lesions, Thoracic Wall Abscess and Vertebral Destruction Caused by Streptococcus constellatus Infection: A Case Report
Authors Su ZQ, Rao WY, Pan XY ![]() , Tang JX, Fan MY, Chen XB, Li SY
, Tang JX, Fan MY, Chen XB, Li SY
Received 1 May 2023
Accepted for publication 26 July 2023
Published 15 August 2023 Volume 2023:16 Pages 5329—5333
DOI https://doi.org/10.2147/IDR.S416483
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Zhu-Quan Su,* Wan-Yuan Rao,* Xiao-Yi Pan, Jia-Xin Tang, Ming-Yue Fan, Xiao-Bo Chen, Shi-Yue Li
State Key Laboratory of Respiratory Disease, National Clinical Research Center for Respiratory Disease, Guangzhou Institute of Respiratory Health, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shi-Yue Li; Xiao-Bo Chen, State Key Laboratory of Respiratory Disease, National Clinical Research Center for Respiratory Disease, Guangzhou Institute of Respiratory Health, The First Affiliated Hospital of Guangzhou Medical University, 151 Yanjiang Road, Guangzhou, 510120, People’s Republic of China, Tel +86 20 8306 2896, Email [email protected]; [email protected]
Abstract: Disseminated infection caused by Streptococcus constellatus was seldom occurred. We reported a case of Streptococcus constellatus infection, presenting as multiple pulmonary cavities, thoracic wall abscess and vertebral destruction. The 37-year-old male had recurrent fever, chest wall swelling and pain, and lower limb numbness, he had weak physical condition and previously suffered from poorly controlled diabetes and severe periodontal disease for 3 years. Definite diagnosis of Streptococcus constellatus infection was made by metagenomic next‑generation sequencing (mNGS) in abscess drainage fluid. Systemic antibiotics and thoracic wall drainage were given, and the pulmonary cavity and the thoracic intermuscular abscess were significantly decreased. Few to no study reported the disseminated infection (pulmonary cavities, thoracic wall abscess and vertebral destruction) caused by Streptococcus constellatus. This case report highlighted the importance of mNGS for accurate diagnosis, as well as the timely drainage and antibiotics for effective treatment of Streptococcus constellatus infection.
Keywords: Streptococcus constellatus, pulmonary cavity, thoracic wall abscess, vertebral destruction, metagenomic next‑generation sequencing
Introduction
Disseminated infection, commonly considered as an intractable case, is giving rise to a potential challenge in the clinical practice. Streptococcus constellatus is a gram-positive and catalase test-negative coccus, it was reported to cause liver abscess, cerebellar abscess and empyema in patients with immunosuppression.1,2 Risk factors for Streptococcus constellatus infection include history of smoking, alcohol abuse, chronic pulmonary disease, periodontal disease and diabetes mellitus.3,4 The special culture of Streptococcus constellatus should be accessed to oxygen and higher concentration of carbon dioxide,5 making it difficult to be detected. We reported a case with initial clinical manifestations of recurrent fever and multiple pulmonary cavity lesions in a middle-aged diabetic patient. The mNGS detection in thoracic wall abscess obtained from percutaneous puncture indicated Streptococcus constellatus infection.
Case Presentation
A 37-year-old male, office worker, began to suffer from cough, breathing difficulty and upper back pain six months ago; afterwards, he experienced worsening shortness of breath, as well as chest wall and upper back swelling and pain. He denied expectoration, fever, or hemoptysis prior to admission. He denied any birds and poultry contact, aspiration, or recent travel. Noteworthily, he suffered from poorly controlled diabetes and severe periodontal disease for 3 years, which induced more than 12 teeth loss.
After hospitalization, he developed fever with a maximum body temperature of 39°C. He felt the left upper back haphalgesia, while the anterior and lateral chest wall swelling and pain without skin temperature arisen. Pressure sore (1 × 1 cm) on the buttock was noted by physical examination. The laboratory tests demonstrated increased blood glucose (32 mmol/L), procalcitonin (1.41 ng/mL), and white blood cell counts (18.28×109/L) with 92.0% neutrophils, but without acute hypoxemic respiratory failure on room air (arterial blood gas: PH 7.49; PCO2 43.2 mmHg; PAO2 68.7 mmHg; HCO3 26.6 mEq/L). Liver and renal function, autoimmune antibody tests, ANCA detection, as well as molecular assay for tuberculosis were otherwise unremarkable. Transthoracic echocardiography and blood culture found no evidence of infective endocarditis or bacteraemia.
The PET/CT and thoracic MRI revealed multiple cavity lesions in the middle and upper lungs, intermuscular abscess on the lateral chest and abdominal wall, as well as T3-T4 thoracic vertebral destruction (Figures 1 and 2). Transbronchial lung biopsy revealed hyperplastic epithelioid foci with numerous neutrophil infiltration, indicating pyogenic granulomatous inflammation. The mNGS in bronchoalveolar lavage fluid (BALF) and lung tissue samples detected EB virus and staphylococcus epidermidis, but no tuberculosis or aspergillosis, whereas the thoracic abscess continued to deteriorate, which had no response to empirical antifungal agents. Furthermore, the bacterial culture onsite and mNGS in thoracic wall intermuscular abscess, obtained from percutaneous puncture under ultrasound guidance, indicated Streptococcus constellatus, which was susceptible to vancomycin, penicillin G, linezolid, cefotaxime and levofloxacin by drug sensitivity test. Afterwards, his fever allayed, the thoracic swelling and pain alleviated, and the lung cavity lesions were shrunk following the treatment with piperacillin-tazobactam (4.5g q8h) and levofloxacin (0.5g qd), as well as drainage of thoracic wall intermuscular abscess (Figure 3B and E), compared with those of pre-therapy (Figure 3A and D). The duration of antibiotic use was eight weeks. Three months post-discharge, this patient was clinically stable, the chest CT showed the lung cavity lesions were mostly resolution, as well as the thoracic wall intermuscular abscess was significantly decreased (Figure 3C and F), whereas this patient refused thoracic spinal surgery for his own concern of surgical risk and financial reason.
 |
Figure 1 PET/CT imaging on pulmonary cavity lesions and thoracic wall abscess. (A and B) CT imaging on multiple lung cavity lesions in the upper lobes. (C and D) PET scan revealed that the lung lesions, chest wall and thoracic vertebrae had higher levels of glucose metabolism (Green arrows). |
 |
Figure 2 Thoracic vertebrae MRI, (A) sagittal plane and (B) coronal plane, indicate hyperintense signals in T3-T4 vertebral bodies and paravertebral tissue (Yellow arrows). |
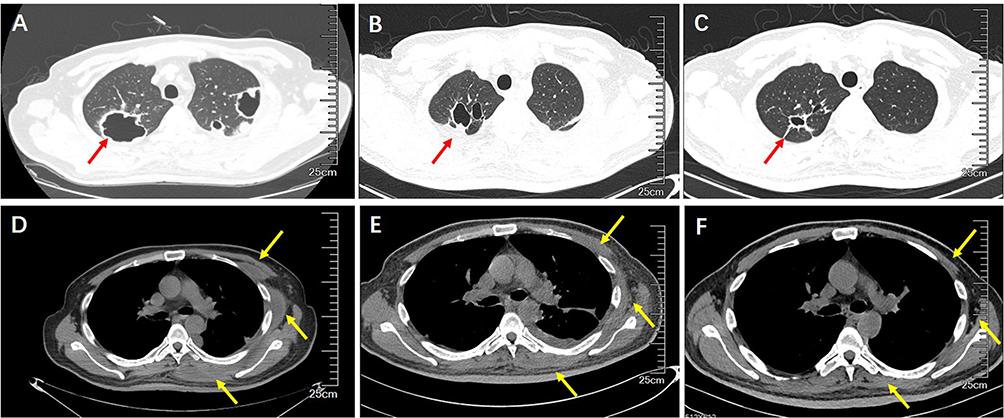 |
Figure 3 Chest CT on pulmonary lesions and thoracic wall abscess before and after treatment. (A and D) Chest CT scan prior to admission. (B and E) Chest CT scan on discharge. (C and F) Chest CT scan at 3-month follow up. The red arrow indicated the change of the pulmonary cavities. The yellow arrow indicated the change of the thoracic wall abscess. |
Discussion
Streptococcus constellatus, accounting for 17.1–36.7% of Streptococcus milleri group (SMG),6,7 is a commensal on the human body surface, oropharynx and gastrointestinal tract,8 it is commonly regarded as a conditional pathogen, which could cause purulent infection in immuno-compromised host. Streptococcus constellatus infection was commonly occurred in male middle-aged and elderly patients (41.43%),3,9 it was reported more likely to be polymicrobial in suppurative infections and associated with pneumonia and pulmonary abscess formation (15.6–40%).6,7,10,11 Streptococcus constellatus infection might develop respiratory failure, severe pneumonia or even ARDS, and patients with comorbidity of disseminated infection and infective endocarditis were reportedly predicted prolonged hospital stay and increase in mortality.7 The potential high-risk factors for Streptococcus constellatus empyema include alcohol abuse, diabetes mellitus and oral infection.3,4 In this case, the middle-aged patient had uncontrolled diabetes mellitus that considered immunocompromised, and severe parodontopathy for more than 3 years, which might be responsible for pulmonary and thoracic soft tissue and vertebral purulent infection. Streptococcus constellatus was reportedly a pathogen in purulent infections including intracranial empyema, liver abscess, pleural effusion, head and neck infections.12–16 Whereas, few to no studies have reported Streptococcus constellatus leading to multiple pulmonary cavity lesions and vertebral purulent infection. Streptococcus constellatus was considered causing pulmonary infections via aspiration, direct implantation, and hematogenous dissemination.4,17,18
Streptococcus constellatus needs to be cultured in 5% CO2 or anaerobic environment, which would be relatively insensitive and time consuming, making it limited to the identification of anaerobes in the clinical practice.5 Bronchoscopy, CT or ultrasound-guided percutaneous biopsy are the most common techniques to obtain lung biopsy for identifying the causative pathogens and to confirm pulmonary infectious diseases. Streptococcus constellatus mainly induced pneumonia and lung abscess followed by spreading to cause empyema. The early diagnosis and timely treatment (sometimes empirical antibiotics) are crucial to improve the prognosis and outcome of Streptococcus constellatus infection, whereas, in this case, the routine bacterial culture and mNGS were negative in BALF specimens, which brought a great challenge in aetiological diagnosis. The previous study indicated that Streptococcus constellatus was detected in only 13.6% by culture methods of the BALF specimens,19 similar observation was reported by Claridge et al that Streptococcus constellatus detection rate was low in pulmonary infection without pleural effusion.10 In the current case, pyogenic infections involved intramuscular soft tissue, pulmonary parenchyma, as well as thoracic vertebrae, diagnostic performance of the mNGS in biopsy tissues and abscess should be given priority to identify the suspected etiology of purulent infections, achieving a diagnostic rate of 86.30% compared to 45.21% detected by the routine culture tests.20,21
Streptococcus constellatus is commonly sensitive to penicillin G, linezolid, levofloxacin, ceftriaxone and chloramphenicol. In the treatment of lung abscess and empyema caused by Streptococcus constellatus, penicillins and their derivatives could be preferred, with regular doses until the full course of treatment is 6 to 8 weeks, or until the pulmonary abscess cavity and inflammation disappear and there is only a small amount of residual fibrosis. In this case, patient obtained a favorable outcome by receiving intravenous antibiotics (piperacillin-tazobactam and levofloxacin) for eight weeks, as well as timely thoracic intermuscular abscess drainage and nutrition support therapy. We learned from this case that mNGS in abscess or pyogenic fluid serves as the essential detection for complicated infections, furthermore, systemic antibiotics and abscess drainage are of equal importance to effective treatment for Streptococcus constellatus purulent infection.
Conclusion
In this report, we presented a case of Streptococcus constellatus infection, causing multiple pulmonary cavities, thoracic wall abscess and vertebral destruction, which was associated with poorly controlled diabetes and severe periodontal disease. The mNGS detection is conducive to identify the suspected etiology of disseminated purulent infections. The accurate antibiotics and early abscess drainage could improve the prognosis of the Streptococcus constellatus disseminated infection.
Patient Consent and Ethics Statement
The study was approved by the First Affiliated Hospital of Guangzhou Medical University Medical Ethics Committee [Medical Ethics [Year 2022] No. 138]. The patient gave written informed consent for publication of the case and the relevant images. No institutional approval was required for the publishing of this case report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Dr. Su declared that he had received the Youth Fund of State Key Laboratory of Respiratory Disease (SKLRD-Z-202314).
Disclosure
Drs. Zhu-Quan Su and Wan-Yuan Rao are co-first authors for this study. All authors declare no potential conflicts of interest in this work.
References
1. Garcia Carretero R. Cerebellar abscesses, infective endocarditis and bacteraemia due to a rare pathogen: streptococcus constellatus. BMJ Case Rep. 2017;2017:bcr–2017.
2. Rodrigues AL, Soares MC, Ramos FL, Crociati Meguins L. Multiple pyogenic liver abscesses caused by Streptococcus constellatus in the Amazon region. Case report. Ann Hepatol. 2009;8(3):255–257. doi:10.1016/S1665-2681(19)31776-4
3. Lin J, Zhang Y, Bao C, et al. The clinical features and management of empyema caused by Streptococcus constellatus. Infect Drug Resist. 2022;15:6267–6277. doi:10.2147/IDR.S382484
4. Porta G, Rodriguez-Carballeira M, Gomez L, et al. Thoracic infection caused by Streptococcus milleri. Eur Respir J. 1998;12(2):357–362. doi:10.1183/09031936.98.12020357
5. Whiley RA, Hall LM, Hardie JM, Beighton D. A study of small-colony, beta-haemolytic, Lancefield group C streptococci within the anginosus group: description of Streptococcus constellatus subsp. pharyngis subsp. nov., associated with the human throat and pharyngitis. Int J Syst Bacteriol. 1999;49(Pt 4):1443–1449. doi:10.1099/00207713-49-4-1443
6. Kobo O, Nikola S, Geffen Y, Paul M. The pyogenic potential of the different Streptococcus anginosus group bacterial species: retrospective cohort study. Epidemiol Infect. 2017;145(14):3065–3069. doi:10.1017/S0950268817001807
7. Noguchi S, Yatera K, Kawanami T, et al. The clinical features of respiratory infections caused by the Streptococcus anginosus group. BMC Pulm Med. 2015;15:133. doi:10.1186/s12890-015-0128-6
8. Gossling J. Occurrence and pathogenicity of the Streptococcus milleri group. Rev Infect Dis. 1988;10(2):257–285. doi:10.1093/clinids/10.2.257
9. Jiang S, Li M, Fu T, Shan F, Jiang L, Shao Z. Clinical characteristics of infections caused by Streptococcus Anginosus Group. Sci Rep. 2020;10(1):9032. doi:10.1038/s41598-020-65977-z
10. Claridge JE, Attorri S, Musher DM, Hebert J, Dunbar S. Streptococcus intermedius, Streptococcus constellatus, and Streptococcus anginosus (“Streptococcus milleri group”) are of different clinical importance and are not equally associated with abscess. Clin Infect Dis. 2001;32(10):1511–1515. doi:10.1086/320163
11. Gogineni VK, Modrykamien A. Lung abscesses in 2 patients with Lancefield group F streptococci (Streptococcus milleri group). Respir Care. 2011;56(12):1966–1969. doi:10.4187/respcare.01316
12. Atemnkeng F, Al-Ttkrit A, David S, et al. An unusual case of intraabdominal abscess after a colonoscopy with polypectomy. J Med Cases. 2021;12(8):301–305. doi:10.14740/jmc3730
13. Carrera W, Lewis WB, Silkiss RZ. Frontal sinus abscess with cutaneous fistula secondary to Streptococcus constellatus. Orbit. 2021;40(2):171. doi:10.1080/01676830.2020.1760314
14. Hirai T, Kimura S, Mori N. Head and neck infections caused by Streptococcus milleri group: an analysis of 17 cases. Auris Nasus Larynx. 2005;32(1):55–58. doi:10.1016/j.anl.2004.09.003
15. Okada F, Ono A, Ando Y, et al. High-resolution CT findings in Streptococcus milleri pulmonary infection. Clin Radiol. 2013;68(6):e331–e337. doi:10.1016/j.crad.2013.01.019
16. Sahin S, Yazar U, Cansu A, Kul S, Kaya S, Ozdogan EB. Is sinusitis innocent? Unilateral subdural empyema in an immunocompetent child. Indian J Pediatr. 2015;82(11):1061–1064. doi:10.1007/s12098-015-1771-x
17. Jerng JS, Hsueh PR, Teng LJ, Lee LN, Yang PC, Luh KT. Empyema thoracis and lung abscess caused by viridans streptococci. Am J Respir Crit Care Med. 1997;156(5):1508–1514. doi:10.1164/ajrccm.156.5.97-03006
18. Kobashi Y, Mouri K, Yagi S, Obase Y, Oka M. Clinical analysis of cases of empyema due to Streptococcus milleri group. Jpn J Infect Dis. 2008;61(6):484–486. doi:10.7883/yoken.JJID.2008.484
19. Mukae H, Noguchi S, Naito K, et al. The importance of obligate anaerobes and the Streptococcus anginosus group in pulmonary abscess: a clone library analysis using bronchoalveolar lavage fluid. Respiration. 2016;92(2):80–89. doi:10.1159/000447976
20. Belko J, Goldmann DA, Macone A, Zaidi AK. Clinically significant infections with organisms of the Streptococcus milleri group. Pediatr Infect Dis J. 2002;21(8):715–723. doi:10.1097/00006454-200208000-00002
21. Zhang HC, Ai JW, Cui P, et al. Incremental value of metagenomic next generation sequencing for the diagnosis of suspected focal infection in adults. J Infect. 2019;79(5):419–425. doi:10.1016/j.jinf.2019.08.012
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acute Spinal Epidural Abscess of the Cervical Spine Caused by Streptococcus constellatus Leads to Paraplegia in an Adult: A Case Report

Zhang W, Lai Y, Li T, Wang X, Mu W, Jiang Z
Infection and Drug Resistance 2023, 16:1591-1598
Published Date: 18 March 2023