Back to Journals » Journal of Asthma and Allergy » Volume 16
Multiple Biologics for Multiple T2 Diseases: A Pharmacoepidemiological Algorithm for Sorting Out Patients by Indication
Authors Charriot J ![]() , Descamps V, Jankowski R, Maravic M
, Descamps V, Jankowski R, Maravic M ![]() , Bourdin A
, Bourdin A
Received 17 June 2023
Accepted for publication 7 November 2023
Published 29 November 2023 Volume 2023:16 Pages 1287—1295
DOI https://doi.org/10.2147/JAA.S424152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Jeremy Charriot,1 Vincent Descamps,2 Roger Jankowski,3 Milka Maravic,4,5 Arnaud Bourdin1
1Department of Respiratory Diseases, University of Montpellier, PhyMedExp, INSERM, CNRS UMR, CHU Montpellier, Montpellier, France; 2Department of Dermatology, Hôpital Bichat AP-HP Nord - University of Paris Cité, Paris, France; 3Service d’ORL et de Chirurgie Cervico-Faciale, CHRU – Institut Louis Mathieu, Vandoeuvre, France; 4Department of Rheumatology, Lariboisière Hospital Lariboisière, APHP Nord, Paris, France; 5General Management, IQVIA, Paris, France
Correspondence: Jeremy Charriot, CHU Montpellier, 371 Avenue du Doyen Gaston Giraud, Montpellier, 34295, France, Email [email protected]
Background: Several biologics (Bx) and targeted synthetic drugs (TSD) exist to treat T2 diseases, including chronic spontaneous urticaria (CSU), severe asthma (SA), chronic rhinosinusitis with nasal polyposis (CRSwNP) or atopic dermatitis (AD).
Objective: To identify patients treated with Bx/TSD from a dynamic dispensing database using an algorithm-based methodology.
Methods: We used the LRx database (Lifelink Treatment dynamics, IQVIA) which covers nearly 45% of the French retail pharmacies. Patients who had at least one Bx/TSD dispensing from April 2021 to March 2022 were included. An algorithm was designed to determine the indication of the Bx/TSD prescription analyzing all previous drug dispensation since March 2012 following a 3-steps procedure.
Results: A total of 21,677 patients received at least one Bx/TSD between March 2021 and April 2022. The algorithm identified 91.7% (n = 19,884) patients with a T2 disease (AD = 18.4%, CRSwNP = 1.5%, SA = 59.5%, and CSU = 12.4%), the rest having either an association of diseases (1%) or an undetermined one (7.3%). SA was the main reason for Bx/TSD initiation (52%), followed by AD (29%), CSU (14%) and CRSwNP (5%). For SA patients already under biologic at entry, omalizumab was the most frequently prescribed (48%) followed by benralizumab, mepolizumab (22% each) and dupilumab (8%). Dupilumab was mostly prescribed for AD patients (89% for patient-initiated vs 96% for patient-renewed) followed by baricitinib.
Conclusion: The algorithm was able to identify patients with T2 diseases under Bx/TSD treatments. This tool may help to follow the evolution of prescription patterns in the future.
Plain Language Summary: Nowadays, physicians have a choice of multiple biologics. Although some prospective cohorts of patients receiving those therapeutics exist, there are very few large up-to-date databases. Our algorithm based on a nationwide dynamic dispensing database was able to identify the T2 diseases of patients under biologics or targeted synthetic drugs and to characterize this population. This is a step toward a better understanding and monitoring of prescription patterns in a nationwide setting.
Keywords: severe asthma, atopic dermatitis, nasal polyposis, urticaria, T2 diseases, biologics
Introduction
Chronic inflammatory diseases have seen their therapeutic sphere turned upside down by the revolution provided by the rise of monoclonal antibodies and other “small molecule” agents. Especially, new biologics targeting diseases gathered under the type 2 (for type 2 inflammation) umbrella such as severe asthma (SA), atopic dermatitis (AD), chronic spontaneous urticaria (CSU) and chronic rhinosinusitis with nasal polyps (CRSwNP)1 have transformed their burden: omalizumab (Anti-IgE), mepolizumab (Anti-IL5), reslizumab, benralizumab (Anti-IL5Rc) and dupilumab (Anti-IL4/13Rc). The multiple actions of these molecules stem from the pathophysiology of type 2 inflammation which is a fine balance between tolerance and intolerance to the external environment through the airways, the skin or the digestive tract. Indeed, it is driven by both the innate immune system triggered by pollutants, viral or fungal infections involving type 2 innate lymphoid cells (ILC2) and the adaptive immune system, triggered by contact with an allergen involving type 2 T-helper (Th2) cells. Both ILC2 and Th2 cells produce the type-2 cytokines (interleukin (IL)-4, IL-5 and IL-13), each with several roles in the inflammation cascade.2
One of the first monoclonals, omalizumab, was first approved for SA and then for CSU. More recently, it has been approved for CRSwNP. Then mepolizumab, reslizumab, benralizumab and finally dupilumab have proved efficacy in severe eosinophilic asthma in reducing exacerbations, oral steroids use and in improving symptoms.3 They have also shown great results in CRSwNP in improving nasal and endoscopic scores,4–7 though only dupilumab, mepolizumab and omalizumab are approved in this indication in France. Reslizumab was not approved in France because of the intravenous route. Among those drugs, dupilumab is the only one to be approved for atopic dermatitis thanks to a drastic mitigation of disease activity in Phase III studies.8 Baricitinib, initially approved for rheumatoid arthritis (RA)9 and further for moderate-to-severe AD,10 has a special place because it is not a biological treatment as such, rather a selective immunosuppressant which inhibits the enzymatic activity of Janus Kinases 1 and 2.
CSU, AD, SA and CRSwNP share some pathophysiological mechanisms gathered under the T2 acronym, and as a consequence Bx/TSD has progressively acquired overlapping indications. Moreover, initially restricted to tertiary care center specialists, their prescriptions are now authorized in secondary care centers. This situation likely modified the profile of patients initiated with these molecules, making the collection of real-life data paramount. Long-term data from open-label extension studies11 or from early access programs12 and “real-world data” are now available.13–15 The latest mostly derived from national healthcare databases, which implies a significant delay between the last available data and present time, imposing very frequent updates.16 Accordingly, a real-time updating tool describing Bx/TSD prescription pattern is needed, as no large cohort of patients exists in France (the prospective French cohort RAMSES (recherche sur les asthmes sévères, AP-HP, NCT04077528) involves currently less than two thousand patients).
Lifelink Treatment dynamics (LRx) is a dynamic dispensing database regrouping 45% of the French retail pharmacies (see Materials and Methods). Using that database, we aimed to develop an algorithm able to describe and sort the population treated or initiated by Bx/TSD drugs (disease identification, demographic data, co-treatments) at a large scale, starting from the dispensation of these drugs over a given period of time.
Materials and Methods
Design
We designed a retrospective observational study using non-medical sources. The study period of interest was April 2021 to March 2022.
Database
LRx (Lifelink Treatment dynamics), an IQVIA database, contains all anonymized ambulatory care drug dispensing data in a panel of 10,000 pharmacies.17–19 This panel covers nearly 45% of the French retail pharmacies and around 40 million of patients covered by the French Health Insurance Funds or by other insurance schemes. It is representative of the general population, in terms of geographical spread in metropolitan France and age of covered population (https://pharmastat.iqvia.com/protection-des-donnees-personnelles).
The available variables included patients’ characteristics (unique identification number, year of birth, gender), prescribers’ (age, gender, geographical area of exercise, private or hospital practice, specialty), treatments (prescription and dispensing dates, packaging, dosage, “code identifiant de presentation” [CIP, a unique code considering treatment packaging], dispense volume).
A longitudinal assessment of patients’ dispensations since March 2012 is possible due to its unique identifier regardless of the pharmacy where the dispense occurred. Data do not include treatments delivered during hospitalizations.
Drugs of Interest
The algorithm focused on the Bx/TSD prescribed in the management of AD, CRSwNP, SA, and CSU delivered in outpatient care setting by a private or hospital-based practice physician. Patients identified with rheumatoid arthritis (RA) were excluded (as RA is not considered as a T2 disease and is targeted only by Baricitinib in our study). The Bx/TSD of interest was benralizumab, dupilumab, mepolizumab, and omalizumab for Bx, and baricitinib for TSD. The first indication and the date of following indication were based on the date of their approval in France (ie, date of the transparency committee).
Sorting Rules Using TD
In order to discriminate the different diseases, the tracking drugs (TD) usually prescribed for each were assessed and set up to feed the algorithm described below. For AD, the TD included those delivered before Bx/TSD initiation (alitretinoin, fusidic acid for topical use, clobetasone), and those co-prescribed with Bx/TSD (ciclosporin or methotrexate in association with emollient or topical tacrolimus or topical corticosteroids and topical tacrolimus). For SA, dispense of inhaled corticosteroids (ICS) and long-acting beta-2 agonist (LABA) combination was recorded. More specifically, at least 1 delivery of ICS/LABA (irrespective of the dosing) co-prescribed with a Bx/TSD during the study period, and/or at least ≥2 deliveries of an (high/medium dose) ICS/LABA combination in a historical period of 12 months prior to biologic initiation were recorded. No relevant TD were found for CRSwNP and CSU (Figure 1).
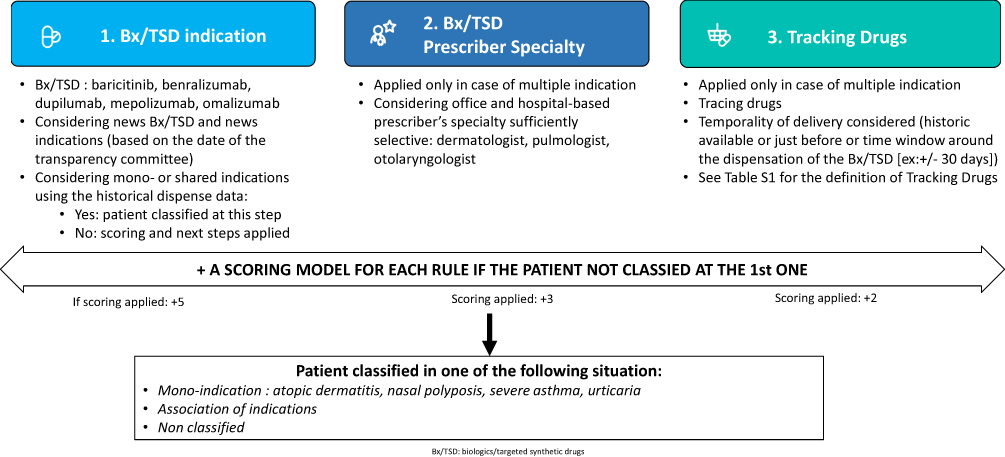 |
Figure 1 An algorithm constructed using consecutive steps including a scoring model and considering a maximum of 10-years historical dispense data. |
We also focused on prescribed drug(s) to evaluate either the burden of each disease or the adequacy with the guidelines (Table S1). For each drug, at least one prescription during the study period was considered.
3-Step Algorithm for Diagnosis Identification
Patients from the LRx database who had at least one Bx/TSD dispensing from April 2021 to March 2022 were included in the present study. Then, an algorithm was designed to determine the indication (ie, which disease of interest) for which a patient received a Bx/TSD. This algorithm analyzed all previous drug dispensing since March 2012 for each patient following a 3-steps procedure if needed (Figure 1):
Step1: Firstly, the indication for which each Bx/TSD dispense during a 10-year historical period was analyzed. At this stage, a patient could be sorted as having one disease in case of mono-indication of the Bx/TSD dispenses or common indication shared by at least two Bx/TSD dispensed for the same patient.
Step2: If a patient was not classified in the first step (multiple indications for the prescribed biologic), after assigning a score of 5 for each indication in competition, the algorithm proceeded to the next step. In this step, only the specialty prescribing the Bx/TSD having an ability to differentiate the disease (dermatology, ENT, and pulmonology) were analyzed. A score of 3 was added to each indication related to the prescriber’s specialty. If multiple physicians from different specialties were associated to one patient’s prescriptions over the study period, this score was attributed to each indication related to different specialties, regardless of the number of prescriptions. For CRSwNP, only a biologic initiated and prescribed by an ENT allowed to classify the patient.
Step3: If the biologic prescribed for one patient had more than one indication (disease not identified in step 1) AND if the prescriber specialty was not able to differentiate the disease (disease not identified in step 2), the third step considered the previous dispensations, focusing on several TD (described above) dispensed before Bx/TSD initiation and/or ±30 days around the Bx/TSD dispensation. A score of 2 was attributed to these TD, regardless of the number of dispensations throughout the follow-up.
If a patient was not classified at the first step, a global score for each indication was computed from the subscores obtained at each step, and the patient was then classified as having the disease with the highest score. In case of equal scores for two indications, the patient was considered as having both diseases. If the algorithm could not determine the indication accurately, the patient was classified as having an “undetermined disease” (ie, ≥3 indication, if at least one Bx/TSD dispense with multiple indication without information regarding prescriber’s specialty and no TD, with Bx/TSD indication in one disease and another with other indication not shared with the previous Bx/TSD dispense) (Figure 1).
Statistical Analysis
The total raw number of patients receiving Bx/TSD from April 2021 to March 2022 was described from the LRx database. The following characteristics of patients classified as having a specific disease were described: demographic characteristics (age category, gender), Bx/TSD (initiated or not during the study period) and co-treatments dispensed at least once during the study period. An initiation was defined as no Bx/TSD delivered 12 months before the first Bx/TSD recorded during the study period from April 2021 to March 2022.
Only descriptive statistics were performed. Quantitative data were expressed by mean and standard deviation, and qualitative data as percentages.
Ethics
Access to and processing of data were done in compliance with applicable laws and regulations including GDPR. LRx database was authorized by the French Data Protection Authority (CNIL) on the 21st of October 2011 [reference: DE-2011-097] and updated on July 2018 for compliance with the GDPR (Délibération 2018-289 du 12 septembre 2018 - Légifrance (legifrance.gouv.fr)).
Results
Identification of Diseases by the Algorithm and Demographic Characteristics
In the LRx database, 21,677 patients received at least one Bx/TSD from March 2021 to April 2022. The algorithm identified 91.7% (n = 19,884) patients as having a unique disease. Among them, a majority had SA (59.5%), then AD (18.4%), CSU (12.4%) and CRSwNP (1.5%). One percent were sorted as suffering from an association of diseases, whereas the indication remained undetermined for 7.3% (Table 1).
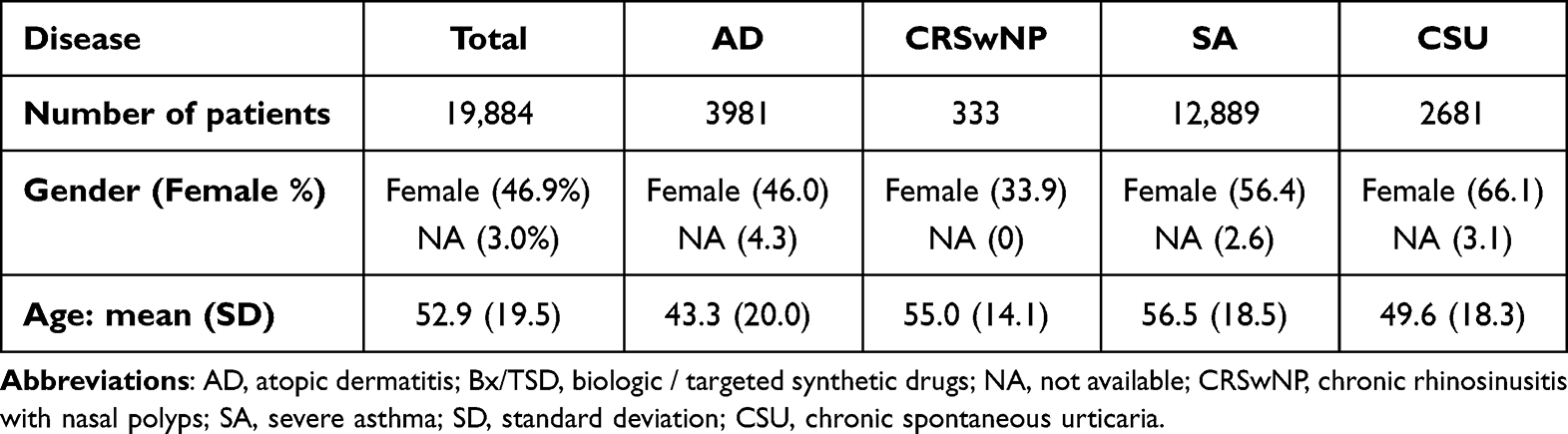 |
Table 1 Demographic Characteristics of Patients Treated by Bx/TSD Classified as Having One Unique sT2-Disease |
Patients with AD were on average younger (mean age = 43.3 years; SD = 20) versus other conditions: 56.5 (SD = 18.5) for SA, 55 (SD = 14.1) for CRSwNP and 49.6 (SD = 18.3) for CSU. Men were mostly represented in CRSwNP (66.1%) and women in CSU (66.1%) (Table 1 and Figure 2).
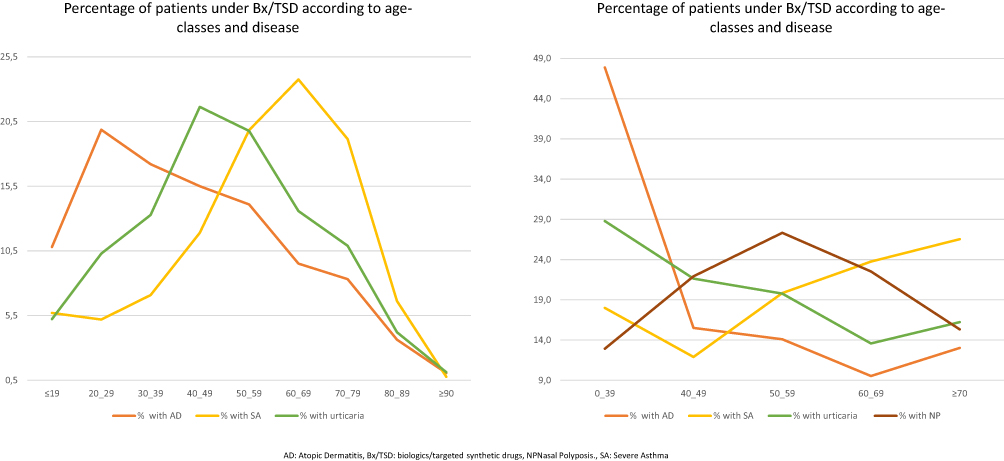 |
Figure 2 Age-classes distribution of patients under Bx/TSD. |
Repartition of Bx/TSD Prescriptions
Among the 19,884 patients classified in one specific disease, 34.5% (n = 6.925) were initiated with a Bx/TSD mainly for SA (52%) followed by AD (29%), CSU (14%), and CRSwNP (5%). In SA, omalizumab was the first biologic initiated (32%) followed by equivalent respective parts of prescription for the anti-IL5/IL5Rc and IL4/13 monoclonal antibodies (mepolizumab, benralizumab, dupilumab), respectively, 23%, 22% and 22%. Dupilumab and omalizumab represented the only initiated or renewed biologic for CRSwNP and CSU, respectively. Dupilumab was mostly prescribed for AD patients (89% for patient-initiated vs 96% for patient-renewed) followed by baricitinib. For SA patients already under biologic before the study period, omalizumab was the most frequent biologic (48%) followed by benralizumab and mepolizumab (22% for each) and dupilumab (8%) (Table 2).
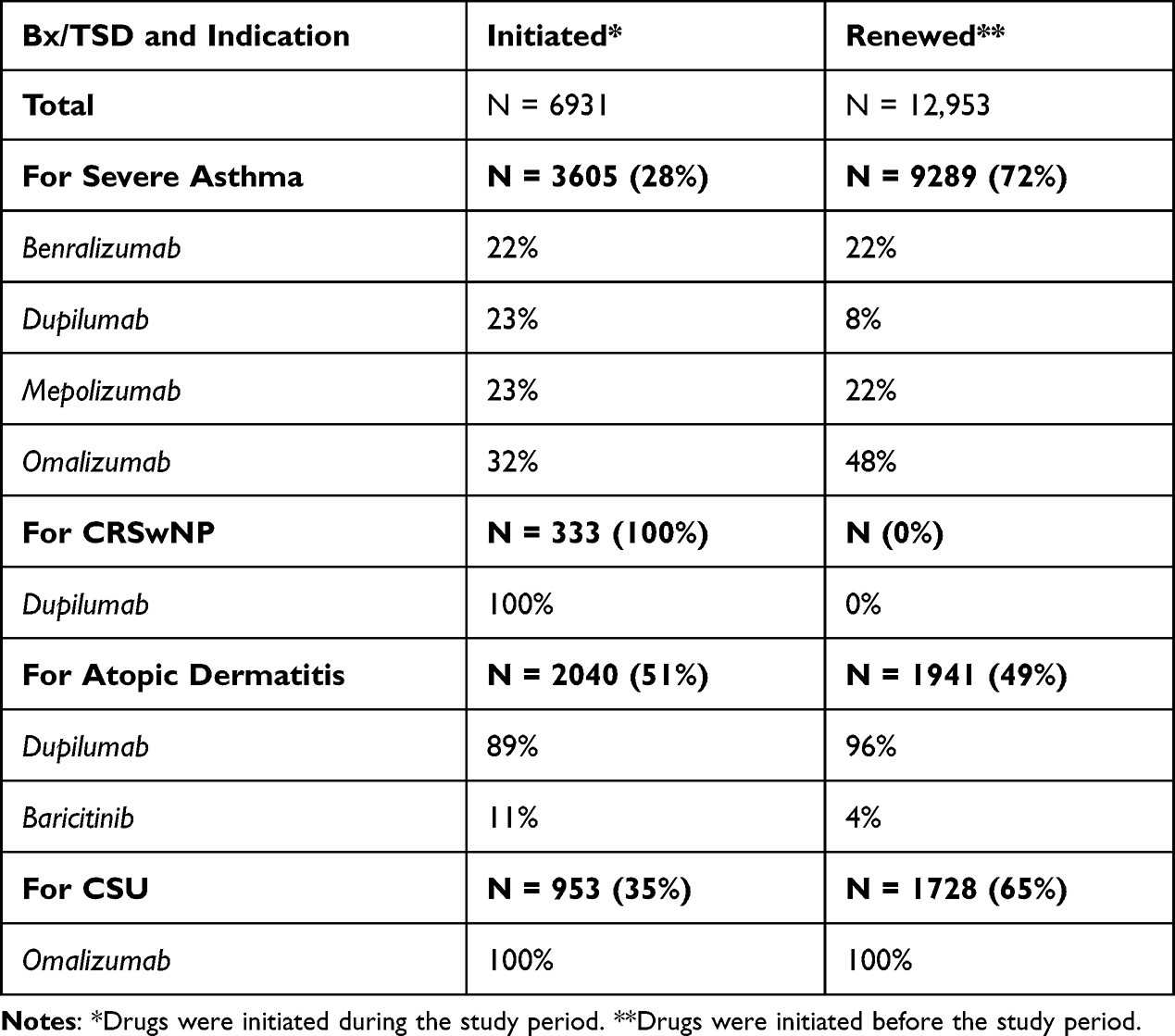 |
Table 2 Proportion of Bx/TSD Initiated or Renewed During the Study Period, by Algorithm-Identified Indication |
Co-Treatments of Interest
Figure 3 described the frequency of oral corticosteroid (OCS) dispenses among patients under Bx/TSD during the study period: SA and CRSwNP represented the main diseases for which patients had at least 2 OCS delivery during the study period (41.5% and 40.5% respectively). Hypnotics and sedatives are frequently co-prescribed in T2 diseases and AD, with the highest proportion for CSU (28.5%). Antibiotics and especially penicillin were mostly co-prescribed in CRSwNP (34.8%) and SA (35.6%). Influenza vaccine prescriptions were detected in almost half of patients identified with SA (47.8%) (Table 3).
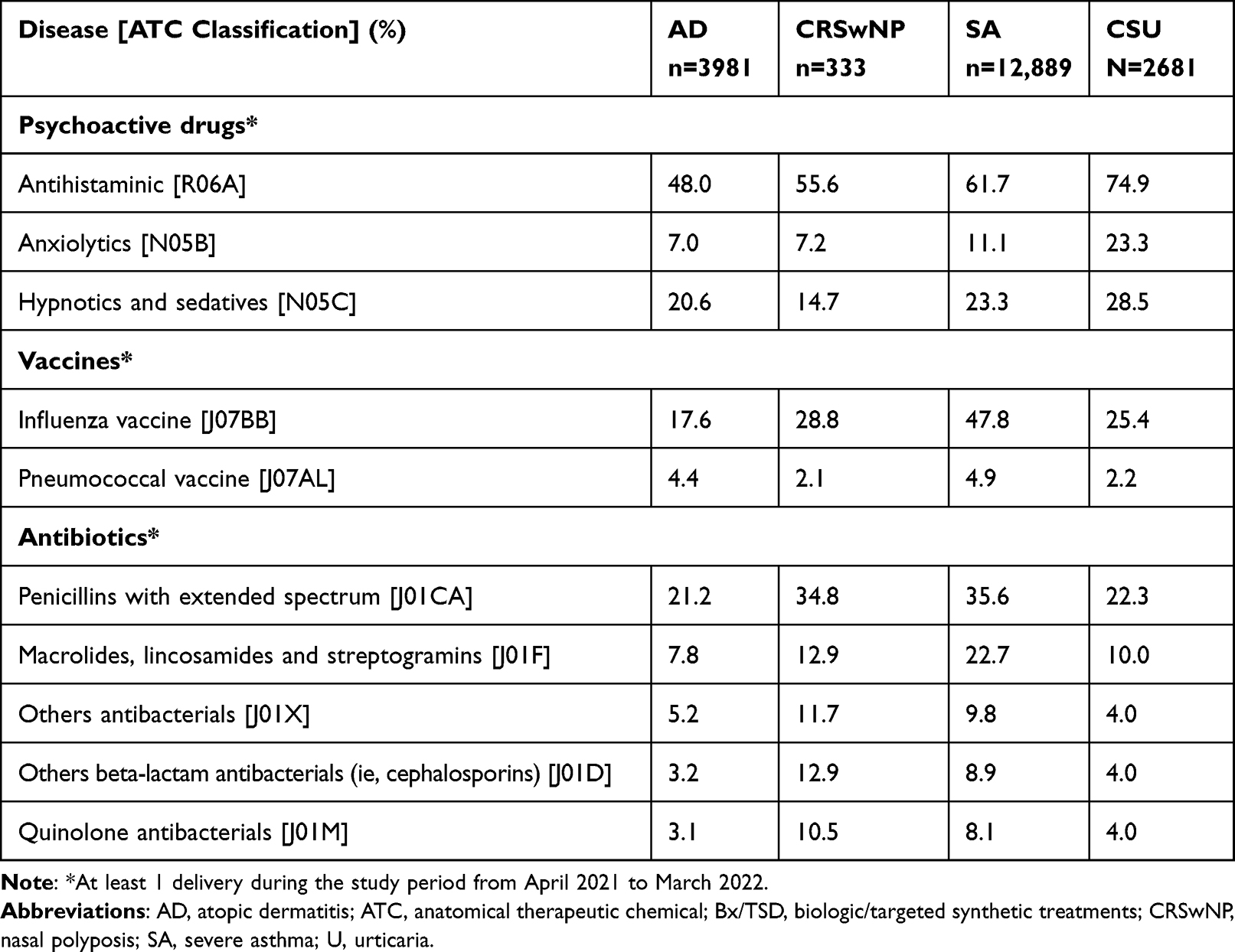 |
Table 3 Other Treatments of Interest Dispensed at Least Once in Patients Treated by Bx/TSD for a T2 Disease |
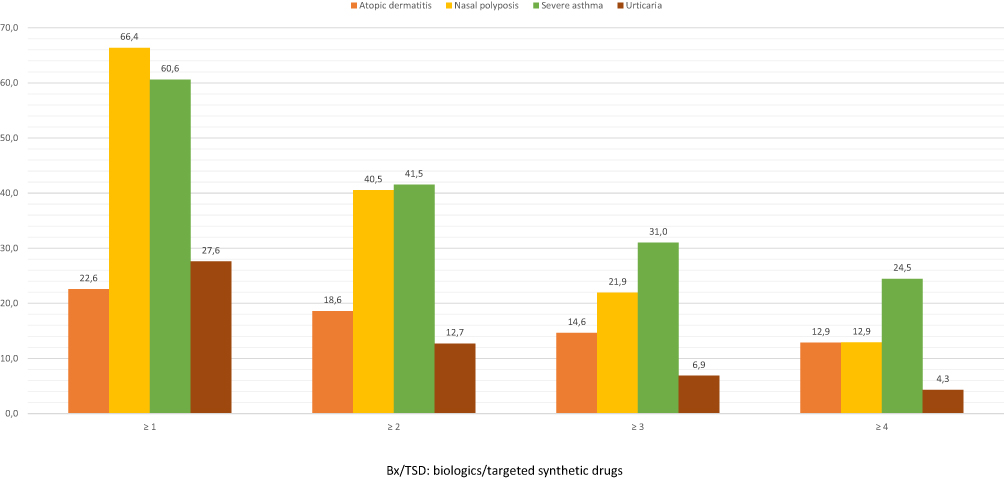 |
Figure 3 Focus on the frequency of oral corticosteroids in patient classified in one disease under Bx/TSD during the period of interest. |
Discussion
Our 3-step algorithm identified almost 20,000 patients under Bx/TSD for a T2 disease, in a real-life setting, and provided interesting data about their demographic characteristics and their co-treatments. The accuracy of the data we obtained becomes more meaningful when compared to “real-life” studies. Indeed, in accordance with the results of the CHRONICLE cohort which concerns 2793 patients in the United States, we here found approximately the same proportion of biologic prescriptions for severe asthma: 48% for omalizumab, an equal proportion for mepolizumab and benralizumab and the rest for dupilumab. The age-class distribution was similar,20 as was the proportion of adult women within the SA group.21 The well-known burden of oral corticosteroids (OCS) in SA or CRSwNP was also highlighted in our research, with a similar number of OCS bursts over a one-year period,22,23 The psychological comorbidities and the prescriptions related to them were also in line with published data; indeed, we found a high prescription of anxiolytics or hypnotics among patients with SA or severe CRSwNP.24,25 Based on the classification of patients we obtained, we were then able to depict accurately the repartition of the prescription of each Bx/TSD according to the identified underlying diseases, and their trends in terms of prescription shares over the study period; indeed, in addition to the Bx/TSD dispenses observed at the beginning of the period of interest (renewed), we were able to capture all new drug dispensing from March 2021 to April 2022 (initiated). Thus, we observed a decreasing number of prescription of omalizumab, as opposed to the increased prescription of dupilumab, in SA, that fits with the reality of the successive marketing-authorizations in this indication. We were also able to detect the co-treatments: this way, we and highlighted the burden of such severe diseases from an iatrogenic perspective with a significant proportion of antibiotics or oral corticosteroid bursts, which are far from being harmless.26,27
The reliability of our algorithm comes from the fact that it has also proved efficient in previous studies in different settings. For instance, it was able to identify patients with type 1 and type 2 diabetes, which could be helpful to monitor changes in strategies to control blood glucose.17 In a completely different field, that of epidemiological monitoring of acute gastroenteritis, the data obtained with our algorithm had a strong agreement with validated primary care French surveillance network data collected during winter months in the overall population.19
One strength of our study is that it relies on a large dispensing database which represent 45% of the French retail pharmacies. As a consequence, we obtained a representative sample of the French population. Another strength of our study is that the LRx database may be queried anytime starting from past month, allowing real-time updates and evolving Bx/TSD prescription patterns. This might be particularly relevant to monitor adherence to guidelines according to the evolution of marketing-authorizations of each molecule. Although this kind of pharmacoepidemiological tool appears obviously useful for companies, many interests can be identified also for clinicians, regulators, payers and policy makers, varying with the level of granularity (level of zoom) chosen: trends in incidence, regional specificities and heterogeneities, impact of new safety warnings when applicable, trends in costs, trends in OCS sparing, adherence to comedications, and needs for targeted continuous medical education. In addition, the 3rd step of our algorithm, based on Tracking Drugs to classify patients not previously categorized, is particularly original as it provides insights into the “polymedication” burden of patients with T2 diseases. These data plaid for a therapeutic de-escalation that Bx/TSD might bring some day: after oral corticosteroids, this could concern inhaled treatment tapering or discontinuation in patients with severe asthma controlled with Bx.
Besides, our study has limitations. First, as for any algorithm, some patients could not be classified in one disease. However, this represents a minor fraction of the general population of the study (7.3%). Secondly, the fact that no relevant Tracking Drugs were identified as relevant for CSU and AD could be perceived as a pitfall, despite the test of multiple combinations. For instance, high-dose anti-histaminics were tested for AD but did not change the performance of our algorithm in terms of disease classification. Moreover, during our period of interest, dupilumab was the only marketed monoclonal available for CSU and AD; as a consequence, the step 2 (based on the prescriber specialty) was reliable enough to classify the patients. At last, one limitation is the absence of a validation cohort with clinically established firmed diagnosis. Thus, we are not able to fairly extrapolate our results to the national population, though our database represents 45% of the retail pharmacies.
Conclusion
The algorithm was able to identify and describe the current landscape of T2 diseases treated by Bx/TSD. This tool could be helpful to monitor the general adherence to guidelines and the temporal evolution of the dispensed drugs according to their market authorizations in a real-life setting.
Abbreviations
AD, atopic dermatitis; CRSwNP, chronic rhinosinusitis with nasal polyps; CSU, chronic spontaneous urticaria; OCS, oral corticosteroids; LRx, Lifelink Treatment dynamics; RA, rheumatoid arthritis; SA, severe asthma.
Acknowledgments
The authors would like to thank the IQVIA Team and particularly Deborah Desprez, Eric Martinho and Daniel Poitevin.
Disclosure
A.B. received payment or honoraria for lectures, presentations, speakers, bureaus, manuscript writing or educational events from AstraZeneca, GSK, Sanofi, Chiesi, Regeneron, ABScience, Novartis, and was principal investigator in clinical trials for AstraZenaca, GSK and Boehringer Ingelheim. J.C. received payment or honoraria for lectures, presentations, speakers, bureaus, manuscript writing or educational events from AstraZeneca, GSK, Sanofi, Chiesi. V.D. received payment or honoraria for lectures, presentations, speakers, bureaus, manuscript writing or educational events from ABBVIE, Janssen, Lilly, Novartis and Sanofi. R.J. reports personal fees from IQVIA, during the conduct of the study; personal fees from Sanofi, outside the submitted work. M.M is affiliated with IQVIA. The authors report no other conflicts of interest in this work.
References
1. Scadding GK, Scadding GW. Innate and adaptive immunity: ILC2 and Th2 cells in upper and lower airway allergic diseases. J Allergy Clin Immunol Pract. 2021;9:1851–1857.
2. Maspero J, Adir Y, Al-Ahmad M, et al. Type 2 inflammation in asthma and other airway diseases. ERJ Open Res. 2022;8(3):00576–02021. doi:10.1183/23120541.00576-2021
3. Brusselle GG, Koppelman GH, Taichman DB. Biologic therapies for severe asthma. Taichman DB, editor. N Engl J Med. 2022;386(2):157–171. doi:10.1056/NEJMra2032506
4. Bachert C, Han JK, Desrosiers MY, et al. Efficacy and safety of benralizumab in chronic rhinosinusitis with nasal polyps: a randomized, placebo-controlled trial. J Allergy Clin Immunol. 2022;149:1309–1317.e12.
5. Bachert C, Han JK, Desrosiers M, et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group Phase 3 trials. Lancet. 2019;394(10209):1638–1650. doi:10.1016/S0140-6736(19)31881-1
6. Gevaert P, Omachi TA, Corren J, et al. Efficacy and safety of omalizumab in nasal polyposis: 2 randomized phase 3 trials. J Allergy Clin Immunol. 2020;146(3):595–605. doi:10.1016/j.jaci.2020.05.032
7. Han JK, Bachert C, Fokkens W, et al. Mepolizumab for chronic rhinosinusitis with nasal polyps (SYNAPSE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med. 2021;9:1141–1153.
8. Beck LA, Thaçi D, Hamilton JD, et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis. N Engl J Med. 2014;371(2):130–139. doi:10.1056/NEJMoa1314768
9. Genovese MC, Kremer J, Zamani O, et al. Baricitinib in patients with refractory rheumatoid arthritis. N Engl J Med. 2016;374(13):1243–1252. doi:10.1056/NEJMoa1507247
10. Simpson EL, Lacour J-P, Spelman L, et al. Baricitinib in patients with moderate-to-severe atopic dermatitis and inadequate response to topical corticosteroids: results from two randomized monotherapy phase III trials. Br J Dermatol. 2020;183:242–255. doi:10.1111/bjd.18898
11. Wechsler ME, Ford LB, Maspero JF, et al. Long-term safety and efficacy of dupilumab in patients with moderate-to-severe asthma (TRAVERSE): an open-label extension study. Lancet Respir Med. 2022;10:11–25. doi:10.1016/S2213-2600(21)00322-2
12. Taillé C, Chanez P, Devouassoux G, et al. Mepolizumab in a population with severe eosinophilic asthma and corticosteroid dependence: results from a French early access programme. Eur Respir J. 2020;55:1.
13. Pilette C, Canonica GW, Chaudhuri R, et al. REALITI-A Study: real-world oral corticosteroid-sparing effect of mepolizumab in severe asthma. J Allergy Clin Immunol Pract. 2022;10:2646–2656. doi:10.1016/j.jaip.2022.05.042
14. Dupin C, Belhadi D, Guilleminault L, et al. Effectiveness and safety of dupilumab for the treatment of severe asthma in a real-life French multi-centre adult cohort. Clin Exp Allergy. 2020;50(7):789–798. doi:10.1111/cea.13614
15. Humbert M, Bourdin A, Taillé C, et al. Real-life omalizumab exposure and discontinuation in a large nationwide population-based study of paediatric and adult asthma patients. Eur Respir J. 2022;60:2103130.
16. Prada-Ramallal G, Takkouche B, Figueiras A. Bias in pharmacoepidemiologic studies using secondary health care databases: a scoping review. BMC Med Res Methodol. 2019;19:53.
17. Larger E, Alexandre-Heymann L, Pilet S, Raoul T, Perray L, Maravic M. Polypharmacy in diabetes: a nation-wide, pharmacy-based, observational study. Diabetes Epidemiol Manag. 2022;8:100088. doi:10.1016/j.deman.2022.100088
18. Joumaa H, Sigogne R, Maravic M, Perray L, Bourdin A, Roche N. Artificial intelligence to differentiate asthma from COPD in medico-administrative databases. BMC Pulm Med. 2022;22(1):357. doi:10.1186/s12890-022-02144-2
19. Vilcu A-M, Blanchon T, Sabatte L, et al. Cross-validation of an algorithm detecting acute gastroenteritis episodes from prescribed drug dispensing data in France: comparison with clinical data reported in a primary care surveillance system, winter seasons 2014/15 to 2016/17. BMC Med Res Methodol. 2019;19(1):110. doi:10.1186/s12874-019-0745-5
20. Panettieri RA, Ledford DK, Chipps BE, et al. Biologic use and outcomes among adults with severe asthma treated by US subspecialists. Ann Allergy Asthma Immunol. 2022;129:467–474.e3.
21. Chowdhury NU, Guntur VP, Newcomb DC, Wechsler ME. Sex and gender in asthma. Eur Respir Rev. 2021;30(162):210067. doi:10.1183/16000617.0067-2021
22. Isaman D, Khan A, Lee S, et al. Oral corticosteroid burden and Healthcare Resource Utilization (HCRU) in patients with Chronic Rhinosinusitis with Nasal Polyps (CRSwNP) undergoing Functional Endoscopic Sinonasal Surgery (FESS): a Real-World Retrospective Cohort Study. J Allergy Clin Immunol. 2023;151:AB201.
23. Heatley H, Tran TN, Bourdin A, et al. Observational UK cohort study to describe intermittent oral corticosteroid prescribing patterns and their association with adverse outcomes in asthma. Thorax. 2023;78(9):860–867. doi:10.1136/thorax-2022-219642
24. Darmon D, Laforest L, Van Ganse E, Petrazzuoli F, Van Weel C, Letrilliart L. Prescription of antibiotics and anxiolytics/hypnotics to asthmatic patients in general practice: a cross-sectional study based on French and Italian prescribing data. BMC Fam Pract. 2015;16(1):14. doi:10.1186/s12875-015-0222-0
25. Workman AD, Dattilo LW, Mitchell MB, Rathi VK, Bhattacharyya N. Rates of antidepressant, anxiolytic, and ADHD medication use among patients undergoing ESS. Ann Otol Rhinol Laryngol. 2023;000348942311790. doi:10.1177/00034894231179016
26. Bourdin A, Adcock I, Berger P, et al. How can we minimise the use of regular oral corticosteroids in asthma? Eur Respir Rev. 2020;29(155):190085. doi:10.1183/16000617.0085-2019
27. Vanderweil SG, Tsai C, Pelletier AJ, et al. Inappropriate use of antibiotics for acute asthma in United States emergency departments. Acad Emerg Med. 2008;15(8):736–743. doi:10.1111/j.1553-2712.2008.00167.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Characterization of Patients in the International Severe Asthma Registry with High Steroid Exposure Who Did or Did Not Initiate Biologic Therapy
Chen W, Sadatsafavi M, Tran TN, Murray RB, Wong CBN, Ali N, Ariti C, Garcia Gil E, Newell A, Alacqua M, Al-Ahmad M, Altraja A, Al-Lehebi R, Bhutani M, Bjermer L, Bjerrum AS, Bourdin A, Bulathsinhala L, von Bülow A, Busby J, Canonica GW, Carter V, Christoff GC, Cosio BG, Costello RW, FitzGerald JM, Fonseca JA, Yoo KH, Heaney LG, Heffler E, Hew M, Hilberg O, Hoyte F, Iwanaga T, Jackson DJ, Jones RC, Koh MS, Kuna P, Larenas-Linnemann D, Lehmann S, Lehtimäki LA, Lyu J, Mahboub B, Maspero J, Menzies-Gow AN, Sirena C, Papadopoulos N, Papaioannou AI, Pérez de Llano L, Perng DW, Peters M, Pfeffer PE, Porsbjerg CM, Popov TA, Rhee CK, Salvi S, Taillé C, Taube C, Torres-Duque CA, Ulrik CS, Ra SW, Wang E, Wechsler ME, Price DB
Journal of Asthma and Allergy 2022, 15:1491-1510
Published Date: 21 October 2022
Allergen Sensitization in Patients with Skin Diseases in Shanghai, China
Zheng C, Zou Y
Journal of Asthma and Allergy 2023, 16:305-313
Published Date: 20 March 2023
Barrier Factors of Adherence to Dupilumab Self-Injection for Severe Allergic Disease: A Non-Interventional Open-Label Study
Hosoya K, Komachi T, Masaki K, Suzaki I, Saeki H, Kanda N, Nozaki M, Kamide Y, Matsuwaki Y, Kobayashi Y, Ogino E, Osada SI, Usukura N, Kurumagawa T, Ninomia J, Asako M, Nakamoto K, Yokoi H, Ohyama M, Tanese K, Kanzaki S, Fukunaga K, Ebisawa M, Okubo K
Patient Preference and Adherence 2023, 17:861-872
Published Date: 27 March 2023
Adult Severe Asthma Registries: A Global and Growing Inventory
Cushen B, Koh MS, Tran TN, Martin N, Murray R, Uthaman T, Goh CYY, Vella R, Eleangovan N, Bulathsinhala L, Maspero JF, Peters MJ, Schleich F, Pitrez P, Christoff G, Sadatsafavi M, Torres-Duque CA, Porsbjerg C, Altraja A, Lehtimäki L, Bourdin A, Taube C, Papadopoulos NG, Zsuzsanna C, Björnsdóttir U, Salvi S, Heffler E, Iwanaga T, al-Ahmad M, Larenas-Linnemann D, van Boven JF, Aarli BB, Kuna P, Loureiro CC, Al-lehebi R, Lee JH, Marina N, Bjermer L, Sheu CC, Mahboub B, Busby J, Menzies-Gow A, Wang E, Price DB
Pragmatic and Observational Research 2023, 14:127-147
Published Date: 20 October 2023
Real-World Biologic Use Patterns in Severe Asthma, 2015–2021: The CLEAR Study
Tran TN, Chen S, Emmanuel B, Altraja A, Bourdin A, Sheu CC, Tsai MJ, Hoyte FC, Quinton A, Cook B, Bulathsinhala L, Henley W, Goh CYY, Liu Y, Ariti C, Carter V, Price DB
Pragmatic and Observational Research 2025, 16:51-66
Published Date: 18 March 2025