")
Back to Journals » Infection and Drug Resistance » Volume 16
Multidrug-Resistant Organism Infections of Inpatients in a Hospital in Eastern China from 2015 to 2021
Authors Fan ZY, You SJ, Li LB, Bian J, Tan FL
Received 30 March 2023
Accepted for publication 23 June 2023
Published 5 July 2023 Volume 2023:16 Pages 4387—4395
DOI https://doi.org/10.2147/IDR.S412491
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Zhao-Ya Fan, Shou-Jiang You, Liu-Bing Li, Jing Bian, Feng-Ling Tan
Department of Infection Management, The Second Affiliated Hospital of Soochow University, Suzhou, Jiangsu, 215000, People’s Republic of China
Correspondence: Feng-Ling Tan, Department of Infection Management, The Second Affiliated Hospital of Soochow University, 1055 Sanxiang Road, Gusu District, Suzhou, 215004, People’s Republic of China, Tel +8613701544030, Email [email protected]
Background: The prevalence of multidrug-resistant organisms (MDRO) is gradually increasing in the global scope, causing serious burden to patients and society, which is an important public health problem.
Objective: To analyze the distribution and trend of MDROs and provide a reference for hospital infection control.
Methods: Collected data on MDROs infections among inpatients in a Grade III Level A hospital in Suzhou from 2015 to 2021, including drug-resistant bacteria strains and specimen sources, etc. Mantel-Haenszel χ2 test was used to evaluate the trend of infection rates over the years and SPSS version 26.0 was used for statistics analysis.
Results: The hospital infection rate showed an overall downward trend across the seven-year period, ranging from 1.53% to 2.10%. According to the analysis of change of drug-resistant bacteria strains, the highest infection rate was carbapenem-resistant Acinetobacter baumannii (CRABA) (63.74%), followed by methicillin-resistant Staphylococcus aureus (MRSA) (46.37%), carbapenem-resistant Pseudomonas aeruginosa (CRPAE) (24.87%), carbapenem-resistant Enterobacteriaceae (CRE) (13.14%) and vancomycin-resistant Enterococcus (VRE) (0.42%). The results of Mantel-Haenszel χ2 test showed that there was a linear relationship between the detection rate of CRE and CRPAE and the time (P< 0.001), but the correlation was not strong (R = 0.136; R = 0.139). The overall detection rate of the five pathogens also increased (P< 0.001). The majority of the specimens, mainly from sputum, airway secretions, and midstream urine, had a detection rate of over 70%.
Conclusion: Our data showed that the detection rate of MDROs generally increased from 2015 to 2021, although the hospital infection rate displayed a declining trend. Among the detection rate MDROs, the highest was CRABA, and the lowest was VRE. It is necessary to enhance the prevention, control, and management of MDROs infections in the clinical practice.
Keywords: MDRO, hospital infection, distribution characteristics
Introduction
Healthcare-associated Infection (HAI) is also known as hospital-acquired infection or nosocomial infection, refers to the infection acquired by patient in the hospital, including the infection occurring during hospitalization and the infection acquired in the hospital but occurring after discharge, excluding the infection that has started before admission or that were in the incubation period at the time of admission. Infections acquired by hospital staff in the hospital also belong to HAI. HAI prevention and control is an important part of medical work, which affects the safety and treatment effect of patients, is closely related to medical quality and safety, and is also an important indicator to evaluate the overall medical service level of the hospital.1 As a negative event, HAI will significantly increase the medical costs of patients, prolong the hospitalization time and increase the burden of disease. It is estimated that 100,000 cases of HAI occur in the UK every year, resulting in 5000 deaths and an additional expenditure of 1.6 billion euros.2 The annual economic burden caused by HAI in the United States is about 6.5 billion dollars every year.3 The direct economic loss caused by HAI in China has already exceeded 10 billion yuan every year, resulting in a 70% increase in total medical expenses.4 HAI is the key and difficult point of hospital management, and its high mortality and huge economic burden are gradually becoming the focus of clinical attention.
Multidrug-resistant organism (MDRO) refers to bacteria that are resistant to three or more types of antimicrobial drugs at the same time. It is the main pathogenic bacteria of HAI, which significantly increases the difficulty of clinical treatment and brings great challenges to the prevention and control of HAI. The Scientific Advisory Committee of the Academia Europaea estimates that more than half of the deaths caused by HAI in the European Union every year are due to MDRO infections. Compared with non-MDRO infection, the mortality of MDRO infection is 1.3–2 times higher.5 How to control and reduce MDRO infection has become the top priority in the management of medical institutions. In 2015, the National Health Commission of the People’s Republic of China issued 13 indicators for the quality control of HAI, of which MDRO monitoring is the most important work in HAI management. MDRO is prone to hospital transmission and cluster events, so it is necessary to timely and accurately monitor relevant information, through which the type and severity of HAI in medical institutions can be monitored, and problems in infection prevention and control can be found in time. Long-term and systematic collection and analysis of MDRO infection data is of great significance for establishing preventive measures.6 This study aims to provide reference for the implementation of infection control plans by analyzing MDRO surveillance data from a Grade III Level A hospital in eastern China from 2015 to 2021.
Methods
Study Design and Data Collection
A retrospective study was conducted to select MDRO monitoring data of all inpatients in a hospital from January 1, 2015 to December 31, 2021. This hospital was established in December, 1988. It is a comprehensive “Grade III Level A” hospital which integrates medical treatment, teaching, scientific research, disease prevention and nuclear emergency treatment. It has first national nuclear emergency medical rescue technical support center, rescue unit and training base.
Surveillance of HAIs was performed with a real-time nosocomial infection surveillance system (RT-NISS). The algorithm of system screening considers the data of positive microbiological examinations, antibiotic administration, serological and molecular testing, imaging reports, temperature, invasive device usage, and inpatient transfer.7 Clinicians and infection control practitioners then confirmed the suspected HAI cases pushed by the system. The determination of HAI cases was based on the Diagnostic Criteria for Healthcare-associated Infection (Trial) issued by the National Health Commission of the PRC in 2001.8 For the same strains cultured from the same site in the same patient, only the first results were recorded, excluding repeated isolates.
Enter the time and bacterial species in the system for retrieval, and collect the number and type of target bacteria, the distribution of specimens submitted, and the proportion of MDRO in hospital infection of all hospitalized patients. For the confidentiality of patient information, all data collected in our study were de-identified, that is, they do not have individual identification and cannot be traced.
Target Detection of Bacterial Species
According to the Healthcare-associated Infection Quality Control Index (2015 edition), the type of MDRO monitored includes Carbapenem-resistant Enterobacteriaceae (CRE), Vancomycin-resistant Enterococcus (VRE), Methicillin-resistant Staphylococcus aureus (MRSA), Carbapenem-resistant Pseudomonas aeruginosa (CRPAE) and Carbapenem-resistant Acinetobacter baumannii (CRABA). CRE includes Carbapenem-resistant Klebsiella pneumoniae (CRKPN) and Carbapenem-resistant Escherichia coli (CRECO). VRE includes Vancomycin-resistant Enterococcus faecium (VREfm) and Vancomycin resistant Enterococcus faecalis (VREfa).
Materials
BD Phoenix™ M50 automated microbiology system was used, and the results were determined according to the Clinical and Laboratory Standards Institute (CLSI) standards. The quality control strains were Escherichia coli (ATCC25922), Klebsiella pneumoniae (ATCC700603), Staphylococcus aureus (ATCC25923), Acinetobacter baumannii (ATCC19606), Pseudomonas aeruginosa (ATCC27853), Enterococcus faecium (ATCC35667) and Enterococcus faecalis (ATCC29212).
Statistical Analysis
SPSS 26.0 was used for data analysis, and Mantel-Haenszel χ2 test was used to evaluate whether there was a linear trend of infection rate over the years. The significance was set at P < 0.05 and all statistical tests were two-tailed.
Results
HAI Situation Over the Years
From 2015 to 2021, a total of 542,754 inpatients were included, and the number of inpatients gradually increased. During this period, 9912 patients were infected in hospital, and the infection rate over the years was 2.10%, 1.62%, 1.58%, 2.09%, 2.07%, 1.85%, and 1.53%, respectively, which were basically maintained at a relatively stable level. The total incidence of HAI in the seven years was 1.83%. The detailed distribution is shown in Figure 1.
 |
Figure 1 Healthcare-associated infection of inpatients in 2015–2021. |
Detection of MDRO
From 2015 to 2021, a total of 7841 strains of five categories of pathogens were detected, of which 2127 strains were detected as MDRO, with a total detection rate of 27.13%. The detection rate of CRABA was the highest (958 strains, 63.74%), followed by MRSA 460 strains (46.37%), CRPAE 334 strains (24.87%), CRE 370 strains (13.14%) and VRE 5 strains (0.42%). Among the five pathogens, the detection rates of CRPAE and CRE showed an annual increase (P < 0.001), while the detection rates of the other three pathogens fluctuated slightly. In general, the total detection rate of five pathogens also showed an increasing trend (P < 0.001). The detection of each pathogen over the years is shown in Table 1, and the change in detection rate is shown in Figure 2.
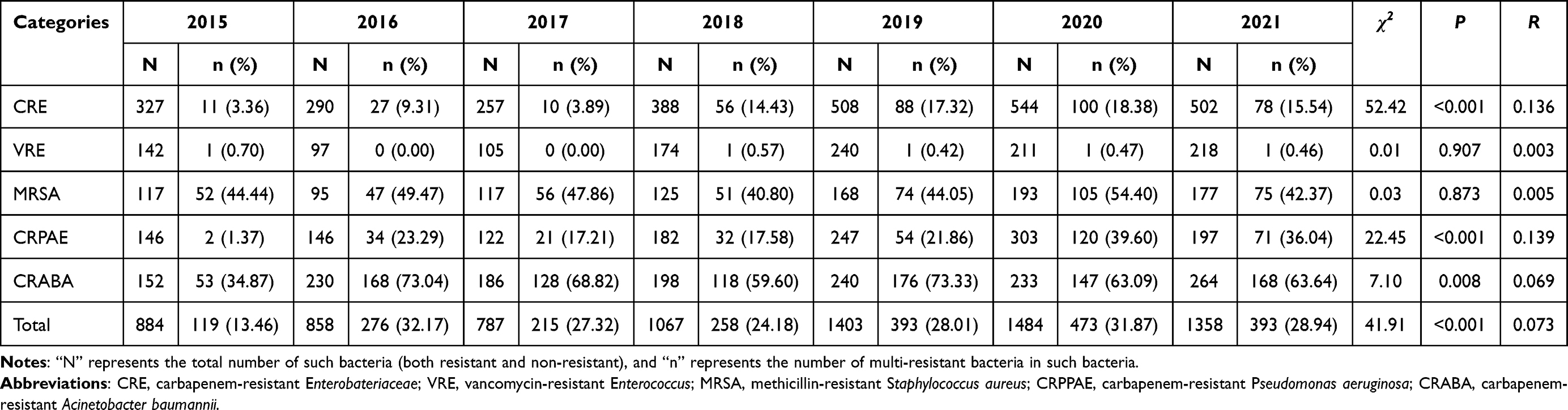 |
Table 1 Detection of Multidrug-Resistant Organisms from 2015 to 2021 |
 |
Figure 2 Distribution of the multidrug-resistant organisms detection rate. |
Distribution of MDRO Specimens
The top five sources of MDRO specimens were sputum (1032, 96.63%), airway secretions (424, 95.71%), midstream urine (103, 45.78%), wound secretions (142, 88.20%) and drainage fluid (118, 83.69%).
Although the number of specimens was not large, the detection rate of lavage fluid, fiberscope brush specimens, ascites, nasal swabs, vaginal secretions, puncture fluid and peritoneal dialysis solution was 100%. The detection rate was above 70% in all specimens except midstream urine and faeces. All specimens were collected at the patient’s visit for screening purposes. The distribution of specimens classified by pathogen type is shown in Table 2, and the distribution of specimens classified by year is shown in Table 3.
 |
Table 2 Specimen Sources of Multidrug-Resistant Organisms from 2015 to 2021 |
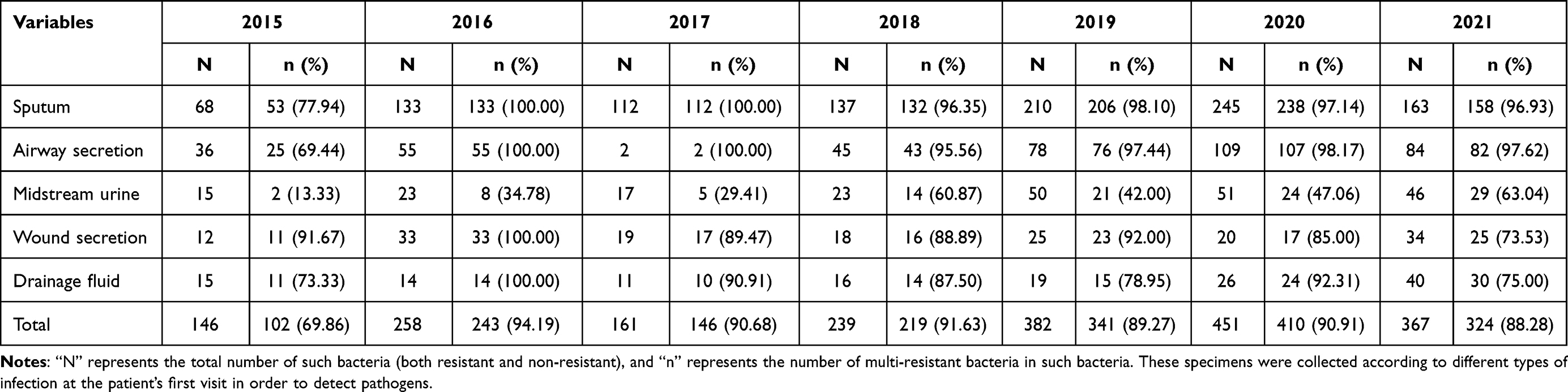 |
Table 3 Distribution of Major Specimen Sources of Multidrug-Resistant Organisms from 2015–2021 |
Discussion
HAI surveillance is important for the implementation and follow-up evaluation of infection prevention and control measures. From 2014, the prevalence of HAI in China is 2.3–2.7%, which is lower than that of the United States (3.2–4%) and Europe (5.9%) during this period.9 The present study showed that the seven-year average infection rate of the hospital was 1.83%, which met the relevant requirements of the National Health Commission (the prevalence rate of HAI in Grade III Level A hospitals ≤10%). The overall infection rate showed a downward trend, from 2.10% to 1.53%. Our data are similar to the infection rate of other tertiary hospitals in the region.10 Compared with the results reported by comprehensive tertiary hospitals in other regions of the country, the data were slightly different, with higher or lower infection rates.11–14 It may be related to the different disease types and severity of patients admitted by hospitals in different regions, as well as the different scale of hospitals, diagnosis and treatment conditions and the rate of examination. Compared with general hospitals in other countries, the infection rate in this study was significantly lower,15–17 which is closely related to our country’s efforts in HAI prevention and control. In recent years, the relevant laws and regulations on the management of HAI have been gradually improved, the allocation of HAI teams has been continuously optimized, the awareness of prevention and control of medical staff has been continuously strengthened, and the management of HAI has been carried out steadily, with certain achievements made. At the end of 2019, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection spread rapidly around the world and became a public health emergency of global concern.18 The COVID-19 pandemic has improved people’s awareness of infection prevention and control strategies, changed people’s lifestyles and medical treatment behavior, and hospitals at all levels have strengthened infection control. The literature suggests that as the risk of COVID-19 has increased, health care professionals have comprehensively improved infection prevention and control behaviors.19,20 The decrease in infection rates in 2020 and 2021 may be related to this reason. In 2018, due to the needs of business work, the study hospital added comprehensive intensive care unit and neurosurgery ward II, which are also prone to multidrug-resistant organism infection. The increase in infection rate in 2018 may be related to this reason.
It is important to understand the composition, distribution and infection characteristics of clinical MDRO in order to control and reduce HAI. In our study, the total detection rate of MDRO was 27.13%, and the detection rate of CRABA ranked first for six consecutive years since 2016. In terms of specimen types, the isolates were mainly derived from lower respiratory tract, and sputum specimens were the main source (1032, 48.52%), which was consistent with other reports in China and other countries.20,21 It is worth noting that the collection of respiratory specimens is susceptible to contamination, and it is recommended to collect as far as possible not easily contaminated, meaningful specimens. The qualified rate of respiratory tract specimens was as follows: bronchoalveolar lavage fluid > aspiration secretion > induced sputum > deep sputum. Although sputum specimens have limited clinical significance, they are the specimens with the highest rate of examination. The key to their reliability lies in the standard collection and examination of specimens in clinical work, which is also the focus of infection managers. CRABA is an important opportunistic pathogen of HAI in critically ill and immunocompromised patients, mainly causing respiratory infections. In recent two years, there have been increasing reports of CRABA associated with hospital-acquired pneumonia, especially ventilator-associated pneumonia.22–26 The infection is difficult to treat may be related to the following reasons: First, once A. baumannii exhibits carbapenem resistance, resistance to most other antibiotics expected to be active against wild-type A. baumannii usually develops, leaving few therapeutic options. Second, there is no clear “gold standard” for evaluating the effectiveness of various treatment regimens for CRABA infection, and studies on the effectiveness of commonly used drug treatments are limited. Third, the data on whether specific drugs have an advantage in CRABA treatment or whether combination regimens have additive benefit in treating CRABA infection are still incomplete.27
Limitations
There are also limitations in our study. First, the data collected were all from one hospital, and sample representation may be insufficient. So, we tried to extend the research time to overcome this limitation. Second, the identification and classification of our cases are based on clinical microbiology results and the judgment of professional staff. Despite the existence of official guidelines, variations may exist among individuals in identifying the occurrence of HAI. Third, the sensitivity of colistin is an important part of MDRO. Due to the limitations of conditions, we did not conduct colistin sensitivity tests, but it may be involved in our following research.
Conclusion
This study analyzed the HAI situation, especially the MDROs, in a Grade III Level A hospital. Our data indicated a general increase in the detection rate of MDROs, despite the declining trend observed in the hospital infection rate. The CRABA ranked first in detection rate for six years in a row. Lower respiratory tract infection was the main infection site, and sputum was the main specimen source. The increasing detection rate of MDRO hinders the clinical anti-infection treatment. Starting from the changeable influencing factors such as improving the hand hygiene compliance of medical staff, strict environmental disinfection, implementation of contact isolation, standardized use of antibiotics and appropriate administrative support, and take timely and effective control measures is imperative.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available from the corresponding author by request.
Ethics Approval
Ethical approval was not necessary for this study because our study has not affected participants directly. This study was retrospective and did not involve any prospective observation or intervention. The data were derived from biological samples from previous medical records, which had been collected before this study. All the data used in this study have been de-identified, that is, they do not have individual identification and cannot be traced. The information obtained is only used for this study to effectively protect the privacy of participants. The research project does not involve commercial interests, and the privacy and identity information of participants are protected.
Funding
This research was supported by the Advanced Research Fund of the Second Affiliated Hospital of Soochow University (SDFEYGL2246 and SDFEYGR2263).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Al-Tawfiq JA, Tambyah PA. Healthcare associated infections (HAI) perspectives. J Infect Public Health. 2014;7(4):339–344. doi:10.1016/j.jiph.2014.04.003
2. Klevens RM, Edwards JR, Richards CJ, et al. Estimating health care-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007;122(2):160–166. doi:10.1177/003335490712200205
3. Tchouaket NE, Beogo I, Sia D, et al. Economic analysis of healthcare-associated infection prevention and control interventions in medical and surgical units: systematic review using a discounting approach. J Hosp Infect. 2020;106(1):134–154. doi:10.1016/j.jhin.2020.07.004
4. Song TT, Li YT, Du JG, Meng W, Wang SH. Assessment of economic burden of stroke surgery patients due to nosocomial infection based on marginal analysis. Chin J Nosocomiol. 2020;30(06):888–892. doi:10.11816/cn.ni.2020-193169
5. Friedman ND, Temkin E, Carmeli Y. The negative impact of antibiotic resistance. Clin Microbiol Infect. 2016;22(5):416–422. doi:10.1016/j.cmi.2015.12.002
6. Wen R, Li X, Liu T, Lin G. Effect of a real-time automatic nosocomial infection surveillance system on hospital-acquired infection prevention and control. BMC Infect Dis. 2022;22(1):857. doi:10.1186/s12879-022-07873-7
7. Du M, Xing Y, Suo J, et al. Real-time automatic hospital-wide surveillance of nosocomial infections and outbreaks in a large Chinese tertiary hospital. BMC Med Inform Decis. 2014;14(1):9. doi:10.1186/1472-6947-14-9
8. National Health Commission of the People‘s Republic of China. Diagnostic criteria for healthcare-associated infection (trial). Natl Med J Chin. 2001;05:61–67.
9. Raoofi S, Pashazadeh KF, Rafiei S, et al. Global prevalence of nosocomial infection: a systematic review and meta-analysis. PLoS One. 2023;18(1):e274248. doi:10.1371/journal.pone.0274248
10. Xu J, Zhang YH, Hu YH, Zhang YQ. Characteristics and risk factors of hospital infection in a tertiary hospital in Suzhou, Jiangsu, from 2018 to 2020. Henan J Prev Med. 2022;33(05):355–358. doi:10.13515/j.cnki.hnjpm.1006-8414.2022.05.009
11. Wu PY, Yang CX, Du YY, Wang Q. A study on the prevalence rate and influencing factors of nosocomial infection in a tertiary hospital from 2015–2021. J Prev Med Inf. 2022;38(03):400–405.
12. Qu XJ, Chen YL, Liu Y, Fang XM. Current situation of nosocomial infection in a tertiary level-A hospital from 2015 to 2019. Chin J Disinfect. 2022;39(12):921–924. doi:10.11726/j.issn.1001-7658.2022.12.013
13. Jiang XJ, Lv M, Sun JH. Analysis of nosocomial infection in a general hospital from 2016–2021. Chin J Hosp Stat. 2022;29(04):253–256. doi:10.3969/j.issn.1006-5253.2022.04.003
14. Li SW, Jin YY, Liu YS, Cheng LL, Zhang XY. Survey of prevalence rates of nosocomial infections in a tertiary three-A hospital from 2021 to 2020. Chin J Nosocomiol. 2021;31(22):3474–3478. doi:10.11816/cn.ni.2021-211018
15. Ketata N, Ben AH, Ben HM, et al. Point prevalence survey of health-care associated infections and their risk factors in the tertiary-care referral hospitals of Southern Tunisia. Infect Dis Health. 2021;26(4):284–291. doi:10.1016/j.idh.2021.06.004
16. Nair A, Steinberg WJ, Habib T, Saeed H, Raubenheimer JE. Prevalence of healthcare-associated infection at a tertiary hospital in the Northern Cape Province, South Africa. S Afr Fam Pract. 2018;60(5):162–167. doi:10.1080/20786190.2018.1487211
17. Mpinda-Joseph P, Anand Paramadhas BD, Reyes G, et al. Healthcare-associated infections including neonatal bloodstream infections in a leading tertiary hospital in Botswana. Hosp Pract. 2019;47(4):203–210. doi:10.1080/21548331.2019.1650608
18. Sadeghi DA, Taati MM, Satarzadeh N. COVID-19 (Coronavirus Disease 2019): a new coronavirus disease. Infect Drug Resist. 2020;13:2819–2828. doi:10.2147/IDR.S259279
19. Lai X, Wang X, Yang Q, et al. Will healthcare workers improve infection prevention and control behaviors as COVID-19 risk emerges and increases, in China? Antimicrob Resist Infect Control. 2020;9(1):83. doi:10.1186/s13756-020-00746-1
20. Wu W, Wang W, Yuan Y, et al. Knowledge, attitude and practice concerning healthcare-associated infections among healthcare workers in Wuhan, China: cross-sectional study. BMJ Open. 2021;11(1):e42333. doi:10.1136/bmjopen-2020-042333
21. Shu MH, Huang WZ. Trend of prevalence rate of nosocomial infection in West China Hospital of Sichuan University from 2012–2018. Chin J Evid Based Med. 2020;20(07):759–763. doi:10.7507/1672-2531.201902066
22. Casarotta E, Bottari E, Vannicola S, et al. Antibiotic treatment of Acinetobacter baumannii superinfection in patients with SARS-CoV-2 infection admitted to intensive care unit: an observational retrospective study. Front Med. 2022;9:910031. doi:10.3389/fmed.2022.910031
23. De Benedetto I, Lupia T, Shbaklo N, et al. Prognostic evaluation of Acinetobacter baumannii ventilator-associated pneumonia in COVID-19. Infez Med. 2022;30(4):570–576. doi:10.53854/liim-3004-12
24. Montrucchio G, Corcione S, Lupia T, et al. The burden of carbapenem-resistant Acinetobacter baumannii in ICU COVID-19 patients: a regional experience. J Clin Med. 2022;11(17):5208. doi:10.3390/jcm11175208
25. Canturan SY, Yilmazer N, Sarikaya R, Avsar Z, Ertek M, Uyaner I. Retrospective assessment of ventilator-associated Pneumonias due to Acinetobacter baumannii in an oncology hospital. Sisli Etfal Hastan Tip Bul. 2021;55(2):193–196. doi:10.14744/SEMB.2021.01700
26. Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ Infectious diseases society of America guidance on the treatment of AmpC β-lactamase–producing enterobacterales, carbapenem-resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia Infections. Clin Infect Dis. 2021;74(12):2089–2114. doi:10.1093/cid/ciab101
27. Sumardika W, Cokro F, Suranadi W, Pinatih KJP. Multidrug-resistant organism infections correlate with increased mortality in COVID-19 patients: a retrospective, observational cohort study. Bali J Anesthesiol. 2022;6(4):231. doi:10.4103/bjoa.bjoa_181_22
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.