Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Multidisciplinary Conservative Treatment Outcomes of in-Patient Physiotherapy Set-Up Among Patients with Lumbar Disc Herniation in Dhaka City, Bangladesh: A Retrospective, Cross-Sectional Study
Authors Hossain MS, Akter S, Siddique MAE, Siddique MKB, Reza GM, Alom FMM, Ali M ![]() , Noman ORM
, Noman ORM ![]() , Rahman MM, Islam MS
, Rahman MM, Islam MS ![]() , Hossain KMA
, Hossain KMA ![]()
Received 2 December 2022
Accepted for publication 26 January 2023
Published 1 March 2023 Volume 2023:16 Pages 587—601
DOI https://doi.org/10.2147/JMDH.S400021
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Md Shahadat Hossain,1,* Sapia Akter,1,* Mustafa Amimul Ehsan Siddique,2 Md Kaoser Bin Siddique,3 G M Reza,1 Foisal Mohammad Mosiul Alom,4 Mohammad Ali,5 Md. Obayadur Rahman Noman,6 M Mazibar Rahman,2 Md. Shofiqul Islam,6 K M Amran Hossain7,*
1Bangladesh Institute of Manual Therapy & Research, Dhaka, Bangladesh; 2Department of Statistics, Jahangirnagar University, Dhaka, Bangladesh; 3Department of Research, Planning & Development, Grand Health Sector, TMSS, Bogura, Bangladesh; 4Department of Physiotherapy, National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka, Bangladesh; 5Department of Physiotherapy and Rehabilitation, Uttara Adhunik Medical College and Hospital, Dhaka, Bangladesh; 6Department of Physiotherapy, Bangladesh Health Professions Institute (BHPI), Dhaka, Bangladesh; 7Department of Physiotherapy & Rehabilitation, Jashore University of Science & Technology (JUST), Jashore, Bangladesh
*These authors contributed equally to this work
Correspondence: K M Amran Hossain, Department of Physiotherapy & Rehabilitation, Jashore University of Science & Technology (JUST), Jashore, 7408, Bangladesh, Tel +8801735661492, Email [email protected]
Background: The study aimed to determine the outcome of Multidisciplinary physiotherapist-led conservative treatment of lumbar disc herniation at an in-patient set-up of a specialized spine center in Dhaka, Bangladesh.
Methods: This was a retrospective cross-sectional study of 228 cases completing treatment and follow-up sessions. The outcome was evaluated as pain at rest and five different functional positions, neurological recovery, and Magnetic resonance imaging (MRI) changes during discharge and follow-up.
Results: 80.3% had a complete recovery with a typical motor and sensory status, no limitations in straight leg raise (SLR), no cauda equina symptom (CES), and no or < 3 pain during more than 30 minutes of daily living activities. Statistically significant changes were noted at all outcome measures at the follow-up (day 90), compared to baseline (day 1) P< 0.01. In the posthoc tests, pain, SLR, and CES had the most significant improvement at discharge (day 12) compared to the baseline (P < 0.01) and at follow-up compared to discharge (P < 0.01). No major adverse events noted.
Conclusion: Physiotherapist-led in-patient treatment results in significant resting and functional pain outcomes in 12 days. Also, the improvements in neurological recovery and normalizing disc position are statistically significant in 90 days.
Keywords: lumbar disc herniation, multidisciplinary, conservative treatment, physiotherapy
Introduction
Lumbar disc herniation (LDH) is one of the most prevalent causes of low back pain,1,2 that frequently affects the L4-L5 and L5-S1 levels.1 The condition results from the abnormal biomechanical pressures imposed on the intervertebral disc and their inability to reconstruct due to their avascular nature.3 The predominant symptoms are radicular, perceptual abnormalities, and weakness in the distribution of one or more lumbosacral nerve roots.4,5 In the early days, the patient typically complains of discomfort in postures that increase disc pressure, such as sitting, standing, walking, or activities. The pain eases with rest or lying in bed.6 In recent studies, the average age of patients with a herniated disc was 41 years, and males were more likely to be diagnosed than females (57% versus 43%, respectively).7 There are many predisposing factors, but an increase in body mass index (BMI) is a risk factor for lumbar disc herniation, which is assumed to be owing to more significant axial stress on the lumbar spine.8 Also, a positive correlation exists between cumulative exposure to physical workload and lumbar disc herniation, indicating a higher risk of herniation in jobs with high physical demands.9
The clinical diagnosis of lumbar disc herniation is a comprehensive approach. The North American Spine Society’s (NASS) Evidence-Based Guideline Development Committee suggested manual muscle testing, sensory testing, and the supine SLR test (including its crossed leg variation) as the gold standard for the clinical diagnosis of LDH.10,11 Treatment of LDH has two approaches, conservative and operative treatment. Conservative treatment is the primary treatment option, but surgical treatment is required for cases with Cauda Equina Syndrome (CES).12 In a study in Dhaka, Bangladesh, Cauda equina syndrome (CES) was found in 4.7% of LDH cases.8,9 CES is a clinical consequence of LDH characterized by severe impairments in the lumbosacral motor or sensory distribution, bowel or bladder incontinence, and progressive deterioration of pain or function (especially walking).8,9,12 However, some studies suggest that surgery reduces disco-genic pressure that extends for a shorter duration of fewer than two years.13 After surgical treatment, almost 32% of recurrences are reported,14 and possible causes were a higher rate of disc height, a higher percentage of the occupied spinal canal by the herniation of disc materials, and the presence of degenerative facet joint changes. Conservative management of LDH includes medication, spinal epidural, decompression therapy, physiotherapy, manual and exercise therapy, electrotherapeutic modalities, and lifestyle modifications.15 The multidisciplinary team for conservative treatment includes a physician, surgeon, or interventional physician and a physical therapist. Additional team members may consist of nurses, radiologists, neurologists, anesthesiologists, spine fellows, psychologists, and case managers.1 Evidence suggests conservative management has a similar long-term effect to surgical management.15 Among conservative approaches, Physiotherapy management of LDH aims to improve myofascial and neural sensitivity, osteokinemetic or arthrokinematic mobility, and functional restoration, which reduces or abolishes pain and enhances intervertebral disc healing and decompresses the neural structures.16 The outcome of physiotherapy in LDH was found to be significantly positive on pain, spinal range of motion, bothersome in activities, fear avoidance in functional tasks, neurological recovery, and disability in experimental studies in Bangladeshi settings for short and longer duration in outpatient set-up.17 The stated study did not estimate any indicators of success rates. Still, a study from Australia18 has 59% of LDH cases with an improvement of disability by a mean duration of 8.7 months in an outpatient setting.
Although there is evidence of outpatient physiotherapy services, In-patient physiotherapy set-ups are designed to focus on physiotherapists-led rehabilitation in the musculoskeletal area.19 In in-patient physiotherapy services, patients have an extended scope to receive Advanced practice physiotherapy (APP)20 and extensive supervision from a physiotherapist and a multidisciplinary team. Evidence suggests that physiotherapists can provide equal care and efficiency in musculoskeletal health compared to physicians.21 To the best of our knowledge, there are no studies evaluating the multidisciplinary outcome of LDH in the in-patient physiotherapy set-up where physicians and physiotherapists worked as a team, performed a comprehensive assessment, and ensured the best possible care for the patients. The study aimed to find the multidisciplinary conservative treatment outcomes among patients with Lumbar Disc Herniation at an in-patient physiotherapy set-up in Dhaka City, Bangladesh. The objectives are to (1) present the demographic, social, and physical factors associated with LDH, (2) Characterize the clinical variables of LDH at Baseline before the intervention, (3) detect the overall outcome of a multidisciplinary approach to pain, function and neurological indicators for the cases with LDH, (4) detect the success rate of interventions and (5) elicit the outcome based on successful versus unsuccessful cases.
Methodology
Study Design
The study is a retrospective cross-sectional study of lumbar disc herniation (LDH) cases who completed in-patient physiotherapy services and post-discharge follow-up between January 2021 and July 2022.
Population and Sample
We have screened 338 files of LDH cases from the specialized Spine center of the Agrani Specialized Physiotherapy Centre (ASPC) in Dhaka, Bangladesh, served between January 2021 and July 2022 as population. Two hundred twenty-eight files were taken as a sample according to eligibility criteria. The inclusion criteria were (1) Diagnosis of Lumbar disc herniation through magnetic resonance imaging (MRI) with sensory, motor testing, and supine straight leg raise test (SLR) according to the Working Group of the North American Spine Society’s (NASS),10,11 (2) Completed at least 12 days’ in-patient physiotherapy treatment, and (3) have a follow-up evaluation for at least 90 days after discharge. The exclusion criteria were (1) patients diagnosed without an MRI, (2) completed in-patient rehabilitation with a break in the middle of stay, (3) patients with a previous history of LDH surgery, (4) patients having other issues along with LDH (eg, spondylolisthesis, spinal fracture, etc.).
Multidisciplinary Assessment
The physician’s assessment and diagnosis were the primary MRI and clinical examination screening. Physicians were of neuro-medicine, neurosurgery, orthopedic surgery, and Physiatry specialty. The physiotherapist’s assessment was supervised by two advanced physiotherapy practitioners with a Master of Physiotherapy degree and 20 years of experience in musculoskeletal services who were recruited separately out of the research team. The assessment protocol was pre-determined, structured, and stored in a repository.22 The physiotherapy assessment had five parts [Supplementary file 1]. The first part was a subjective assessment comprised identities, anthropometric measurement, referral diagnosis, chief complaints, and history of present complaints. The second part includes pain assessment at rest, sitting for more than 5 minutes, standing for more than 5 minutes, walking for more than 5 minutes, pain in maintaining functional movements, and pain in performing 30 minutes of daily activities. The third part was the selective lumbopelvic muscle stretch and strength test. The fourth part was the neurological assessment of sensory and motor examination of lumbosacral nerve roots, straight leg raise (SLR), Dural test or sign, and nerve sensitivity test. And the last part is the provisional diagnosis of affected structures. Physiotherapy assessment was performed during admission (Day 1), discharge, and follow-up sessions.
Multidisciplinary Treatment
The treatment approach is described in Table 1. Physicians prescribed a wide range of medications to control pain and associated impairments as a simple analgesic as paracetamol, tramadol/paracetamol, codeine-based analgesics, Non-steroidal anti-inflammatory drug, opioid analgesics, muscle relaxants, corticosteroids, neuropathic medications. The physiotherapy treatment process included stretching exercises, activation, isometric exercise, isotonic exercises, neural stretching, local release of neuro-sensitive structures, activation of nerve function, spinal mobilization and ROM exercises, postural advice or modifications, home exercise, and interventions to manage adverse events.
 |
Table 1 Interventions by the Multi-Disciplinary Team |
Study Variables
Outcome Variables
There were five main outcome variables for assessing the multidisciplinary conservative management of LDH.
Magnetic Resonance Imaging (MRI)
The changes in MRI imaging from initial diagnosis (Day 1) and follow-up sessions (after Day 90) were the first outcome variable; this variable was categorized by bulging, protrusion, extrusion, migration, and sequestration as per MRI reports.23
10-Centimeter Visual Analogue Scale
The second variable was pain assessment from the initial day of center-based rehabilitation, with a follow-up after discharge. Pain variables were documented three times, at rest, sitting for more than 5 minutes, standing for more than 5 minutes, walking for more than 5 minutes, maintaining regular transitional movements, and 30-minutes of daily activities. VAS is a validated tool for measuring the outcome of LDH;24 in a 10 cm scale pain is quantified by a 10 cm Visual Analogue Scale ranging between 0 and 10 cm, with higher scores indicating extreme pain.
Neurological Outcome Indicators
The third outcome variable was the sensory and motor status, directed to the lumbar 2 to sacral one dermatome and myotome. Sensory had three categories, intact, impaired, and diminished, and the motor score was determined by the universal system of Oxford muscle grading (0–5). The fourth was the straight leg raise (SLR) test, ranging from positive and negative. Any provocation of leg radicular symptoms within 75 degrees is considered positive.25 The fifth outcome variables were the equine cauda syndrome (CES) as the red flag signs of lumbar radiculopathy diagnosed according to NICE guideline.26 The presence of any one symptom of CES was considered positive. All outcomes were documented for baseline, discharge, and follow-up, and MRI changes were recorded at baseline and follow-up.
Successful Cases
In the follow-up data taken on Day 90, the cases with five positive indicators as (1) 0 pain sore in 30 minutes of daily activities, (2) intact sensory status, (3) grade 5 motor score in all dermatome and myotomes at L1-S1, (4) negative SLR, and (5) negative CES were considered successful cases of treatment.
Explanatory Variables
The explanatory variables were age, gender, BMI, occupation or work, co-morbidities, duration of symptom, duration of work, and symptom description (central, ipsilateral, contralateral, and bilateral symptoms).
Data Collection
From 228 files, the investigation, diagnosis, drug treatment, physiotherapy interventions, and periodic assessments were documented, preserved, and audited from structured printed medical documents in the means of the measurements taken on day 1, discharge after day 12, and follow-up after day 90. Seven physiotherapists converted the hard copies of medical data to a Microsoft Excel dataset, and two independent researchers completed data extraction; missing data were further queried and filled up. The incomplete dataset was removed and audited by a team member of the authors. After that, the data were prepared for analysis. The study process followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline [Supplementary file 2].
Statistical Analysis
Data were coded and analyzed using the Statistical Package of Social Sciences (SPSS) software V.20 (IBM Corporation). Normality distribution of the data was performed using the Kolmogorov–Smirnov and Shapiro–Wilk tests. The descriptive statistics [Table 2] were performed by frequency and percentage for categorical and non-parametric data, and mean and standard deviation for continuous and parametric data. In addition, baseline compatibility is accomplished by successful versus unsuccessful cases by pretest indicators through the Independent t-test or Mann–Whitney U-test. The overall outcome [Table 3] from Day 1 to day 90 was determined through one-way ANOVA or Friedman test for three measurements, for two measures, or as a Post-hoc test, paired t-test or Wilcoxon test was used. A further determination of Clinical outcomes between successful and unsuccessful cases [Table 4] from day 1 to day 90, the Kruskal–Wallis test and Repeated measure ANOVA between subjects’ estimates were employed, with a posthoc test by Independent t-test or Mann–Whitney U-test. Levels of significance were at <0.05, <0.01, <0.001, and for the posthoc test, Bonferroni correction has been made and p values estimated as a minimum of P<0.01.
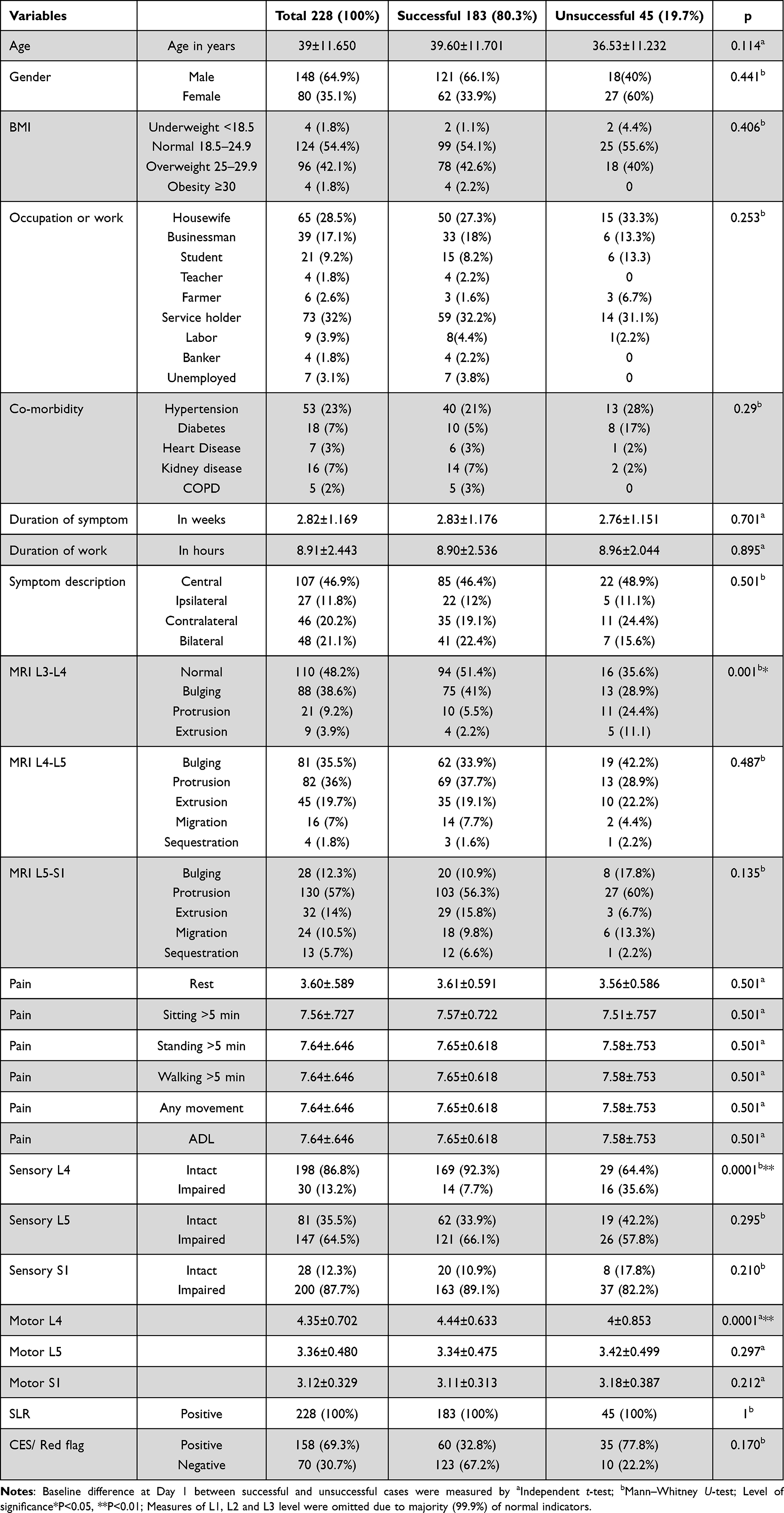 |
Table 2 Descriptive of Socio-Demographic and Baseline Clinical Values (Day 1) |
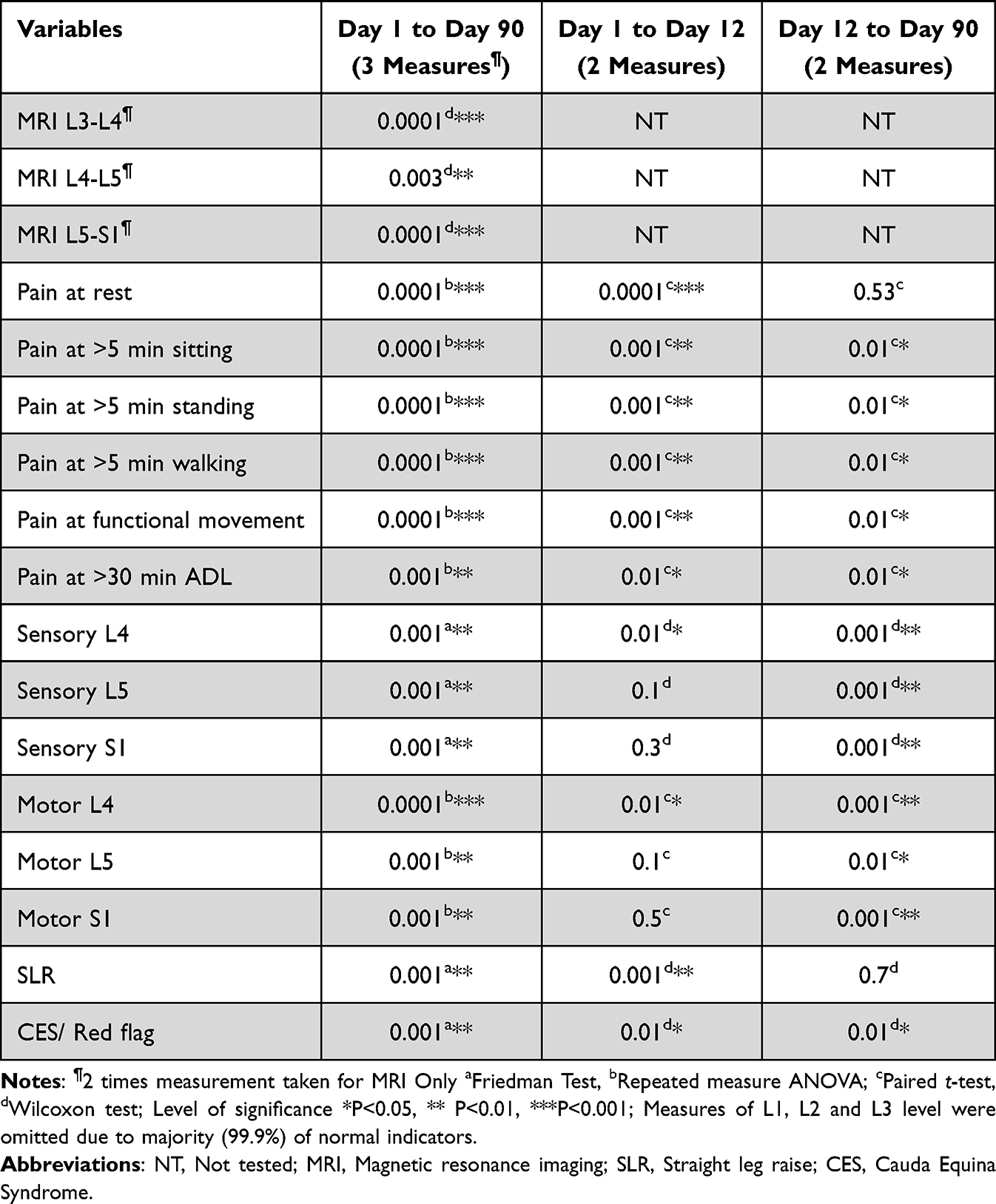 |
Table 3 Overall Clinical Outcome in Different Time Frame |
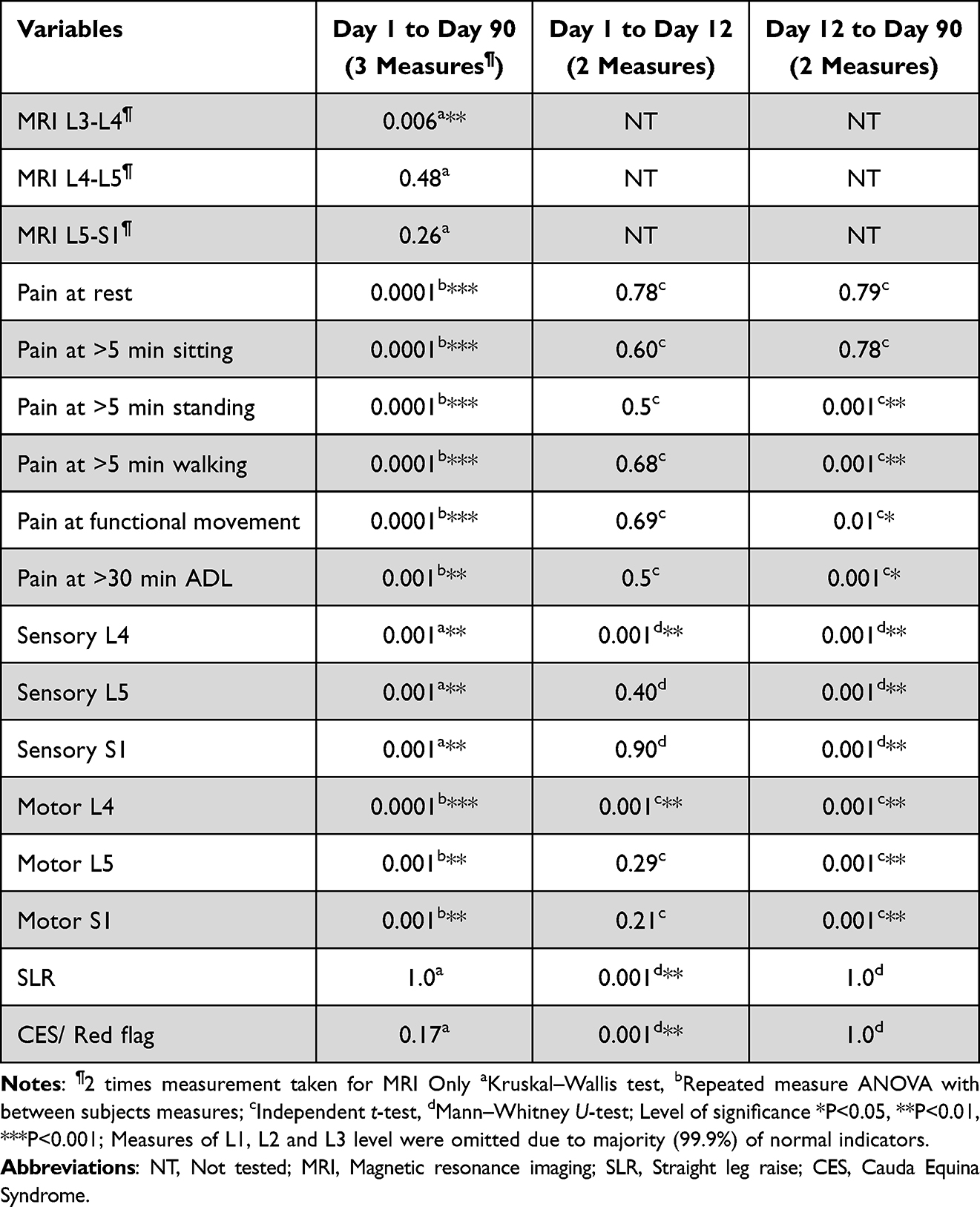 |
Table 4 Clinical Outcome in Between Group Comparison (Successful versus Unsuccessful Cases) |
Results
Two hundred twenty-eight cases with a lumbar disc herniation (LDH) received multidisciplinary conservative management, and we retrieved their clinical information on Day 1, Day 12, and Day 90. Overall, 183 (80.3%) cases were successfully treated, and 45 (19.7%) did not have clinical success, according to our indicators. The mean age of the cases was 39 years (SD 11.650); male cases were 148 (64.9%) compared to female 80 (35.1%). Body mass index (BMI) of the cases was normal for 124 (54.4%) cases, whereas 96 (42.1%) had overweight and 4(1.8%) had obese. Among female 65 (28.5%) were homemaker, and among male 39 (17.1%) was businessman. Another major portion 73 (32%) service holders from both gender working in the offices of Dhaka city. Hypertension was the major co-morbidity 53 (23%), 18 (7%) had diabetes, and 16 (7%) had kidney diseases. There was no statistically significant baseline compatibility (P < 0.05) between the socio-demographic variables of the successful and unsuccessful cases, except for the baseline compatibility of L3-L4 MRI, motor and sensory status (P < 0.05). Before taking the multidisciplinary treatment, LDH cases had a mean duration of their symptoms as 2.82 weeks (SD 1.169). For the cases with LDH, the usual duration of office work was 8.91 hours in a day (SD 2.4). The majority had central low back pain 107 (46.9%), 27 (11.8%) had ipsilateral referred pain (problem and symptom on the same side), 46 (20.2%) had contralateral referred pain (problems and symptoms are on the opposite side) and 48 (21.1%) had symptoms in both legs. MRI of the lumbosacral spine finds discs of L1-2 and L2-3 level was normal for all the cases, but there was a diverse report in the rest of the levels [Table 2]. The disc in between lumbar 3 and 4, 110 (48.2%) were normal, 88 (38.6%) were bulged, 21 (9.2%) was protruded and 9(3.9%) had extrusion. There was no normal status of the disc position in between L4 and L5; 81 (35.5%) had bulging, 82 (36%) had a protrusion, 45 (19.7%) were extruded, 16 (7%) were migrated, 4(1.8%) were sequestrated. In the disc situated between L5 and S1 level, 28 (12.3%) were bulged, 130 (57%) were protruded, 32 (14%) were extruded, 24 (10.5%) was migrated in the space of spinal cord and 13 (5.7%) were sequestrated.
Outcome of Pain
On day 1, the average pain at rest was 3.6 centimeters on the 10-centimeter scale (SD 0.5) [Table 2]. The pain had a statistically significant decline of scores noted on Day 90 compared to the scores of Day 1(P < 0.001) [Table 3] and at posthoc analysis on day 12 compared to day 1 (P < 0.001). The overall changes in resting pain from Day 12 to Day 90 were not statistically significant. Compared to the successful versus unsuccessful cases, there was a substantial change in resting pain in successful cases on the 90th day compared to the first day (P < 0.01) [Table 4]. Moreover, no statistical changes were noted in between-group posthoc tests of between-group analysis. The changes of pain in sitting for more than 5 minutes, standing for more than 5 minutes, walking for more than 5 minutes, functional movements, and daily living activities for more than 30 minutes have a statistically significant change on day 90 compared to day 1 (P < 0.01), and in all comparison of all time frames (Table 3). In the group comparison, significant changes were noted in successful cases on day 90 compared to day 1 (P < 0.01). In the between-group posthoc test majority, had no differences separately between day 1 and day 12 and day 12 to day 90 (Table 4). Figure 1 shows the changes in pain in their mean scores with 95% confidence interval error bars.
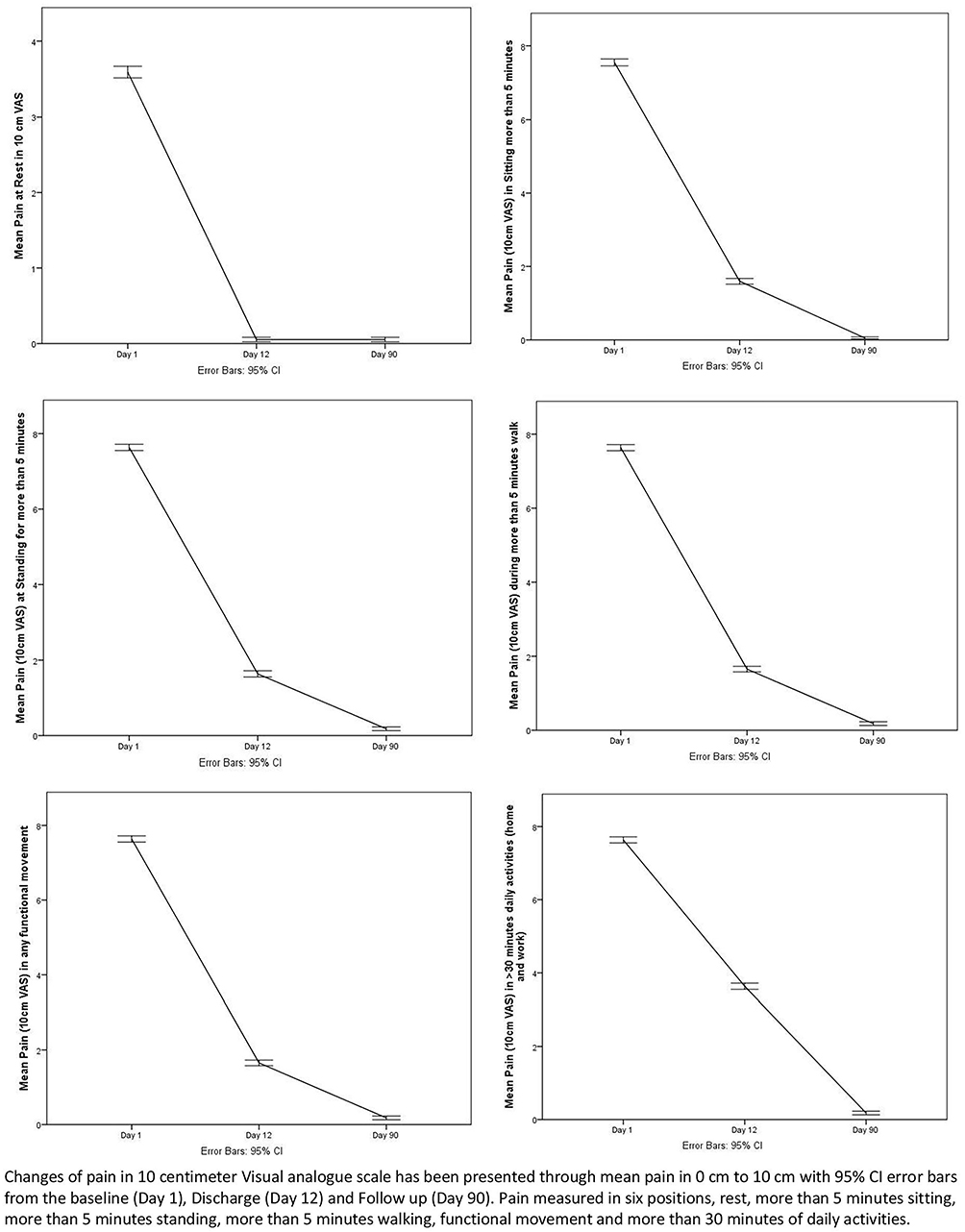 |
Figure 1 Changes of pain from baseline to follow up. |
Changes in Neurological Indicators
On day 1 (Table 2), in the L4 dermatome 30 (13.2%) had impaired sensation, and similar impairment in sensation was noted as 147 (64.5%) in L5 and 200 (87.7%) in the S1 dermatome. The sensory status of L1 to L3 was normal. The overall improvement of sensory status was statistically significant on day 90 compared to day 1 (P < 0.001), day 12 compared to day 1, and day 90 compared to day 12 (P < 0.05). The improvements in sensory status were significantly higher for the successful cases in the same time frames (P < 0.01) compared to the unsuccessful group. Before treatment, motor score measured in the oxford muscle grading system was found at muscles of the L5 nerve root as an average of 3.36 on a 0–5 scale (SD 0.4), and at muscles of the S1 nerve root, 3.12 (SD 0.3). Motor status of the muscles of L1 to L3 were grade 5. Overall improvements in the motor score of the muscles of L4, L5, and S1 nerve roots were significant in the outcome measures taken between day 90 compared to day 1 (P < 0.001). The result was consistent for post-hoc analysis of motor score from day 1 to day 12, and day 12 to day 90 (P < 0.01). The improvements were also noted in the successful group at day 90 compared to day 1 (P < 0.001) and at post-hoc between day 12 and day 90 (P < 0.01). The between-group changes of mean motor scores in three measurements are shown in Figure 2. All the cases had a positive straight leg raise (SLR) before the intervention, and 158 (69.3%) had any one of the symptoms of Cauda equina syndrome (CES) (Table 2). SLR and CES had significant improvement on day 90 (P < 0.001) and Day 12 (P < 0.001) compared to day 1 (Table 3). The changes in SLR and CES are also visualized in Figure 3.
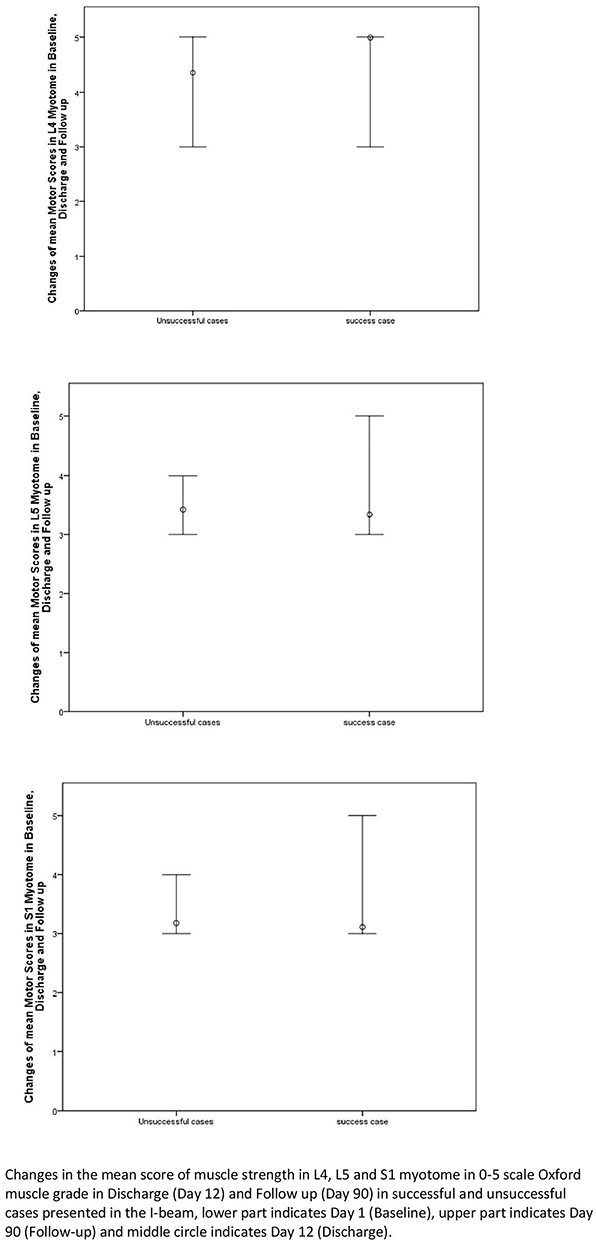 |
Figure 2 Changes of motor status of lower limb motor nerves. |
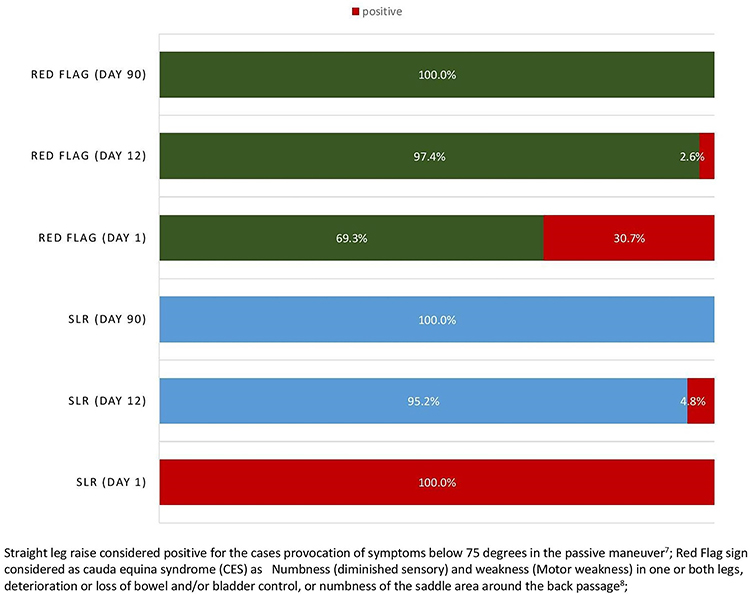 |
Figure 3 Changes of red flag sign and straight leg raise. |
Changes in MRI
There were statistically significant changes in the disc position at the level between L3 and L4, L4 and L5, and L5 and S1 in the MRI images noted at day 90 compared to day 1 (P < 0.01) (Table 3). In group comparison, the Successful group had a significant change of disc position at the L3 and L4 level only (P < 0.01) compared to the unsuccessful cases. The changes in MRI are presented in Figure 4.
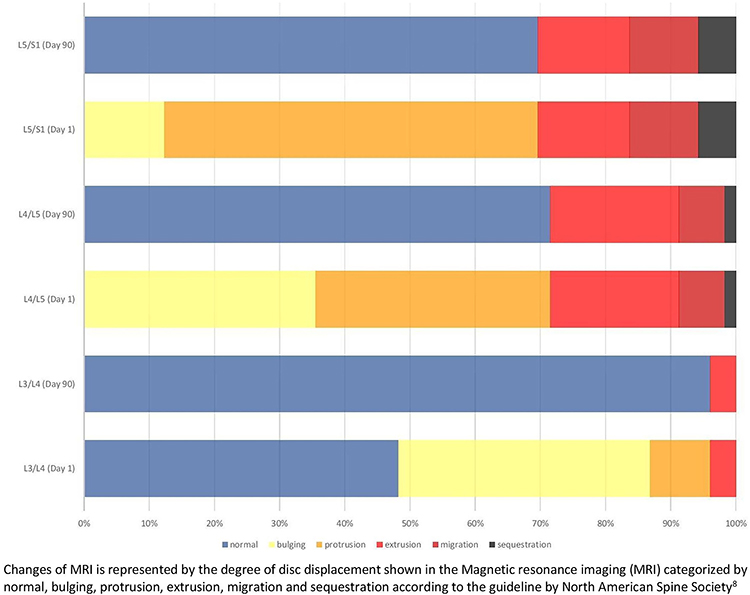 |
Figure 4 Changes of magnetic resonance imaging of lumbar discs. |
Discussion
The study was intended to find the outcome of a multidisciplinary approach of conservative management for LDH cases in a physiotherapist-led in-patient set-up in Dhaka city. From the database of a specialized spine center, 18 months of clinical data were extracted to generate the result. Two hundred twenty-eight cases of LDH completing 12-days comprehensive in-patient care by taking medications prescribed by a physician and physiotherapy prescribed by an advanced practice physiotherapy practitioner had statistically significant (P<0.05) outcomes in pain at rest and five different functional positions, neurological changes measured by physical tests (SLR, sensory, motor, CES), and normalization of disc position measured by MRI in the short term for 12 days and in the long term for 90 days. 80.3% were successful cases as they have complete recovery in physical and functional status. Full recovery is indicated by performing daily or livelihood activities for more than 30 minutes without painful symptoms, intact neurological functions in sensory and motor tests, a negative result in provocation tests as straight leg raise, and no cauda equina signs. On Day 1, the MRI study shows all the participants have either one or multiple compression in unilateral and bilateral nerve roots of L4, L5, and S1 levels according to Van Rijn classification systems.27 Only 48% of cases had a normal disc position at L3/L4 level on day one, and at day 90, it improved to 96%, so 48% of herniated discs recovered up to day 90. The rate of improvement by changing the abnormal disc position to normal was 71% for L4/L5 and 69% for L5/S1 (Figure 4). A recent systematic review and meta-analysis on the physiotherapy interventions for lumbar disc herniation elicits manual and manipulative interventions that can correct the position of the intervertebral disc by restoring spine biomechanics and restoring the neurological functions by reducing the pressure on nerves and synovial fold.28 The restoration of spinal biomechanics is enhanced by ensuring flexibility and strength of the intra-spinal muscles, improving the mobility of the motion segments of the spine that reduces the intradiscal pressure facilitating the nucleus pulposus to migrate towards the center of the intervertebral disc.29 The biomechanical correction minimizes the sensitivity of the nerves, creating decompression to the spinal nerves, and straight leg raise (SLR) improves. The meta-analysis28 shows any advanced practice physiotherapy (such as specialized manual therapy) can significantly reduce lower limb radicular pain, improve neural mobility examined by (SLR) and improves function-related disability status. Our study measured painful impairments at rest and 5 functional positions that relate to the patient’s impairment in function (more than 5 minutes sitting, standing, walking. Functional movements), livelihood, and participation (more than 30 minutes daily living activities) and found a significant change between day one and day 90, day 1 and day 12, and day 12 and day 90 (P<0.01). Our study had 54% patients with lower limb radiculopathy and 69% with any one of the symptoms of red flag sign or cauda equina syndrome (CES). Their improvements were clinically and statistically significant in improving SLR and CES syndromes with a conservative physiotherapist-led in-patient management approach. A randomized clinical crossover trial on 120 patients29 elicits that physiotherapists’ manipulative therapy has an equal outcome for patients with lumbar disc herniation compared to microdiscectomy (surgery) in the short and long term. This crossover trial reports three failed patients with manipulative therapy underwent surgery. They resulted in no change of their state, whereas five failed surgery patients who underwent manipulative therapy had a favored outcome. After one year of intervention, surgery and manipulative therapy cases had equal results.29 None of our patients were reported to have surgery after the follow-up screening.
Our study cases had an acute or sub-acute stage of LDH as they attended within 1 to 4 weeks of their symptoms. Patients with early intervention have a good outcome in pain, fear avoidance in work, function, and disability induced by LDH.17 However, chronic cases with LDH also have a sustainable and favorable outcome in pain, function, and disability.18 Still, early physiotherapy intervention is a cost-saving, efficient and effective intervention for LDH.30 Our study result adheres to the hypothesis of “Virginia Mason example for a pathway for LBP management”30 in the context of an efficient, quicker, and sustainable outcome of a physiotherapist-led multidisciplinary intervention for LDH. We did not perform a cost analysis as it was not documented along with the clinical data stored in the study setting; the maximum cost of treatment of the in-patient physiotherapy set-up was 3000 per day in Bangladeshi currency (USD 30) except the cost of medicine, MRI and physician’s visit. A usual MRI cost for the Lumbosacral spine costs between 5000 and 7000, and physician’s visits reneged from 500 to 1200 in Bangladeshi currency. The study had some limitations as this was a retrospective cross-sectional survey of the clinical records of LDH, no randomization process or control, and the possibility of documentation bias. Also, the study was conducted in a single set-up. There are a few physiotherapist-led in-patient set-ups for mechanical spinal disorders, and designing a prospective clinical trial needs well-structured on-field data. To our best knowledge, this is the first study in this region to evaluate a short and long-term outcome of advanced physiotherapy practice with a multidisciplinary team within an in-patient set-up. The future direction of the study will be a randomized clinical or crossover trial to examine the outcome unbiased, rigorous, and conclusive.
Conclusion
Physiotherapist-led multidisciplinary conservative treatment in an in-patient physiotherapy set-up results in a significant outcome in resting and functional pain, neurological recovery, and disc position for patients with Lumbar Disc Herniation. The pain outcome is rapid and more influential in 12 days’ admission, but neurological recovery and normalizing disc position are more significant in 90 days. The treatment has an 80% of success rate concerning complete neurological recovery and restoration of daily living activities for more than 30 minutes, with no relapsing of symptoms.
Data Sharing Statement
Data is available as LDH dataset.xls in Mendeley Data, V1, www.doi.org/10.17632/ym5h3prdmp.1.
Institutional Review Board
Ethical approval was obtained before data collection from the Institutional review board of the Institute of Physiotherapy, Rehabilitation and Research (BPA-IPRR/IRB/06/16/20394) on June 16, 2022.
Informed Consent Statement
The study was a retrospective study on treated patients. During the intervention, participants provided consent in written form through informed consent of assessment, treatment, and using unanimous data for conducting research later.
Acknowledgment
The authors acknowledge Md. Arif Hossain for coordinating the data collection process and the volunteers of “Amran’s School of Thoughts” for their contribution to data auditing and analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was a self-funded study by the authors.
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Buser Z, Tekmyster G, Licari H, Lantz JM, Wang JC. Team approach: management of an acute L4-L5 disc herniation. JBJS Rev. 2021;9(10). doi:10.2106/jbjs.Rvw.21.00003
2. Martin BI, Deyo RA, Mirza SK, et al. Expenditures and health status among adults with back and neck problems. JAMA. 2008;299(6):656–664. doi:10.1001/jama.299.6.656
3. Schroeder GD, Guyre CA, Vaccaro AR. The epidemiology and pathophysiology of lumbar disc herniations. Semin Spine Surg. 2016;28(1):2–7. doi:10.1053/j.semss.2015.08.003
4. Vroomen PC, de Krom MC, Wilmink JT, Kester AD, Knottnerus JA. Diagnostic value of history and physical examination in patients suspected of lumbosacral nerve root compression. J Neurol Neurosurg Psychiatry. 2002;72(5):630–634. doi:10.1136/jnnp.72.5.630
5. Vucetic N, Svensson O. Physical signs in lumbar disc hernia. Clin Orthop Relat Res. 1996;333:192–201. PMID: 8981896.
6. Nachemson AL. Disc pressure measurements. Spine. 1981;6(1):93–97. doi:10.1097/00007632-198101000-00020
7. Cummins J, Lurie JD, Tosteson TD, et al. Descriptive epidemiology and prior healthcare utilization of patients in the Spine Patient Outcomes Research Trial’s (SPORT) three observational cohorts: disc herniation, spinal stenosis, and degenerative spondylolisthesis. Spine. 2006;31(7):806–814. doi:10.1097/01.brs.0000207473.09030.0d
8. Weiler C, Lopez-Ramos M, Mayer HM, et al. Histological analysis of surgical lumbar intervertebral disc tissue provides evidence for an association between disc degeneration and increased body mass index. BMC Res Notes. 2011;4:497. doi:10.1186/1756-0500-4-497
9. Ahsan MK, Matin T, Ali MI, Ali MY, Awwal MA, Sakeb N. Relationship between physical work load and lumbar disc herniation. Mymensingh Med J. 2013;22(3):533–540. PMID: 23982545.
10. Kreiner DS, Hwang SW, Easa JE, et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J. 2014;14(1):180–191. doi:10.1016/j.spinee.2013.08.003
11. Petersen T, Laslett M, Juhl C. Clinical classification in low back pain: best-evidence diagnostic rules based on systematic reviews. BMC Musculoskelet Disord. 2017;18(1):188. doi:10.1186/s12891-017-1549-6
12. Benzakour T, Igoumenou V, Mavrogenis AF, Benzakour A. Current concepts for lumbar disc herniation. Int Orthop. 2019;43(4):841–851. doi:10.1007/s00264-018-4247-6
13. Delgado-Lo Pez PD, Rodri Guez-Salazar A, Castilla-Di EJ, et al. [Role of surgery in spinal degenerative disease. Analysis of systematic reviews on surgical and conservative treatments from an evidence-based approach]. Neurocirugia. 2005;16(2):142–157. Spanish. doi:10.1016/s1130-1473(05)70420-6
14. Camino Willhuber G, Kido G, Mereles M, et al. Factors associated with lumbar disc hernia recurrence after microdiscectomy. Rev Esp Cir Ortop Traumatol. 2017;61(6):397–403. doi:10.1016/j.recot.2017.07.002
15. Schoenfeld AJ, Weiner BK. Treatment of lumbar disc herniation: evidence-based practice. Int J Gener Med. 2010;3:209. doi:10.2147/ijgm.s12270
16. Choi J, Hwangbo G, Park J, Lee S. The effects of manual therapy using joint mobilization and flexion-distraction techniques on chronic low back pain and disc heights. J Phys Ther Sci. 2014;26(8):1259–1262. doi:10.1589/jpts.26.1259
17. Hossain MA, Jahid IK, Hossain MF, et al. Effectiveness of McKenzie manipulative therapy on pain, functional activity and disability for lumbar disc herniation. Rehabilit Med Phys Ther. 2020. doi:10.2174/1875399X02114010014
18. Hahne AJ, Ford JJ, Hinman RS, et al. Outcomes and adverse events from physiotherapy functional restoration for lumbar disc herniation with associated radiculopathy. Disabil Rehabil. 2011;33(17–18):1537–1547. doi:10.3109/09638288.2010.533814
19. Trulsson Schouenborg A, Rivano Fischer M, Bondesson E, Jöud A. Physiotherapist-led rehabilitation for patients with chronic musculoskeletal pain: interventions and promising long-term outcomes. BMC Musculoskelet Disord. 2021;22(1):1–4. doi:10.1186/s12891-021-04780-x
20. Desmeules F, Roy JS, MacDermid JC, Champagne F, Hinse O, Woodhouse LJ. Advanced practice physiotherapy in patients with musculoskeletal disorders: a systematic review. BMC Musculoskelet Disord. 2012;13(1):1–21. doi:10.1186/1471-2474-13-107
21. Marks D, Comans T, Bisset L, Scuffham PA. Substitution of doctors with physiotherapists in the management of common musculoskeletal disorders: a systematic review. Physiotherapy. 2017;103(4):341–351. doi:10.1016/j.physio.2016.11.006
22. Neuro-muscular impairments in Prolapsed Lumbar Intervertebral Disc (PLID) according to Structural Diagnosis and Management (SDM). Available from: https://www.protocols.io/view/neuro-muscular-impairments-in-prolapsed-lumbar-int-ewov14zr2vr2/v1.
23. Fardon DF, Milette PC. Nomenclature and classification of lumbar disc pathology: recommendations of the combined task forces of the North American Spine Society, American Society of Spine Radiology, and American society of neuroradiology. Spine. 2001;26(5):E93–113. doi:10.1016/j.spinee.2014.04.022
24. Takahashi H, Aoki Y, Inoue M, et al. Characteristics of relief and residual low back pain after discectomy in patients with lumbar disc herniation: analysis using a detailed visual analog scale. BMC Musculoskelet Disord. 2021;22(1):1–9. doi:10.1186/s12891-021-04015-z
25. Majlesi J, Togay H, Ünalan H, Toprak S. The sensitivity and specificity of the slump and the straight leg raising tests in patients with lumbar disc herniation. J Clin Rheumatol. 2008;14(2):87–91. doi:10.1097/RHU.0b013e31816b2f99
26. de Campos TF. Low back pain and sciatica in over 16s: assessment and management NICE guideline [NG59]. J Physiother. 2017;63(2):120. doi:10.1016/j.jphys.2017.02.012
27. Li Y, Fredrickson V, Resnick DK. How should we grade lumbar disc herniation and nerve root compression? A systematic review. Clin Orthop Relat Res. 2015;473(6):1896–1902. doi:10.1007/s11999-014-3674-y
28. Singh V, Malik M, Kaur J, Kulandaivelan S, Punia S. A systematic review and meta-analysis on the efficacy of physiotherapy intervention in management of lumbar prolapsed intervertebral disc. Int J Health Sci. 2021;15(2):49.
29. McMorland G, Suter E, Casha S, Du Plessis SJ, Hurlbert RJ. Manipulation or microdiskectomy for sciatica? A prospective randomized clinical study. J Manipulative Physiol Ther. 2010;33(8):576–584. doi:10.1016/j.jmpt.2010.08.013
30. Flynn TW, Smith B, Chou R. Appropriate use of diagnostic imaging in low back pain: a reminder that unnecessary imaging may do as much harm as good. J Orthop Sports Phys Ther. 2011;41(11):838–846. doi:10.2519/jospt.2011.3618
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.