Back to Journals » Journal of Asthma and Allergy » Volume 19
Multiallergen Immunotherapy for Polysensitized Patients with Allergic Rhinitis: A Systematic Review and Meta-Analysis
Authors Shi Y ![]() , Pan Z
, Pan Z ![]() , Tian X, Li L
, Tian X, Li L ![]() , Guan K
, Guan K
Received 2 April 2026
Accepted for publication 16 June 2026
Published 30 June 2026 Volume 2026:19 610465
DOI https://doi.org/10.2147/JAA.S610465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Yu Shi *, Zhouxian Pan *, Xinyu Tian, Lisha Li , Kai Guan
Department of Allergy, Beijing Key Laboratory of Precision Medicine for Diagnosis and Treatment on Allergic Diseases, Chinese Academy of Medical Sciences & Peking Union Medical College Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kai Guan, Department of Allergy, Beijing Key Laboratory of Precision Medicine for Diagnosis and Treatment on Allergic Diseases, Chinese Academy of Medical Sciences & Peking Union Medical College Hospital, Beijing, 100730, People’s Republic of China, Email [email protected]
Background: Polysensitization occurs in 80% of allergic patients. Allergen immunotherapy (AIT) formulations with multiple allergens remain debated for polysensitized patients.
Objective: This study aims to evaluate the clinical effectiveness and safety profile of multiallergen AIT in polysensitized allergic rhinitis (AR) patients.
Methods: We searched for polysensitized AR patients treated with multiple allergens in immunotherapy in PubMed, Embase, Web of Science and Cochrane Library until June 5, 2025.
Results: Seven randomized clinical trials and 7 nonrandomized studies were included. Multiallergen immunotherapy significantly reduced combined symptom and medication scores versus placebo from baseline (SMD: − 3.75, 95% CI (− 5.85, − 1.65; p < 0.001)). Compared to single-allergen AIT, symptom score changes were no difference (SMD: − 0.34, 95% CI − 1.21, 0.52; p = 0.44), while medication scores showed slight superiority (SMD: − 1.36, 95% CI − 2.44, − 0.28; p = 0.01). But both scores at the last follow-up were significantly reduced compared with single-allergen treatment (SMD: − 1.75, p = 0.01; SMD: − 1.30, p = 0.007). Systematic review highlighted superior outcomes with dual-allergen AIT in some studies. The multiallergen group had a safer profile in randomized studies (OR 0.58, 95% CI 0.35, 0.96, p = 0.03). No significant differences were found in adverse events due to AIT treatment among non-randomized studies (OR 0.86, 95% CI 0.64, 1.15, p = 0.3). Multiallergen AIT demonstrated enhanced immune tolerance and modulation of the type 2 immune response similar to single-allergen treatment.
Conclusion: Based on current evidence, multiallergen AIT demonstrates no significant difference in efficacy, a comparable safety profile, and equivalent immunological modulation compared to single-allergen AIT for the treatment of polysensitized allergic rhinitis. Dual-allergen approaches may optimize benefits in clinically relevant cases, though study heterogeneity necessitates standardized trials.
Keywords: polysensitization, multiallergen immunotherapy, allergen immunotherapy, allergic rhinitis, systematic review and meta-analysis
Introduction
Allergen immunotherapy (AIT) is the only treatment targeting the underlying cause to modify the disease course in patients with IgE-mediated allergic diseases such as allergic rhinitis (AR) or rhinoconjunctivitis with or without allergic asthma. It has been studied for more than a century ever since Noon et al1 first demonstrated its potential as a promising therapeutic option and showed its effectiveness in the management of airway allergic diseases2,3 Although many innovations have been implemented to improve clinical efficacy and tolerability of AIT, there are still many unmet needs.
Polysensitization is more prevalent than monosensitization. Data from several large-scale epidemiological studies in the US and Europe have consistently shown a higher proportion of polysensitization in the general population and patients consulting allergists.4–6 However, published practice guidelines by the American Academy of Allergy, Asthma and Immunology7 and the European Academy of Allergy and Clinical Immunology8 regarding AIT formulations in polysensitized patients differ substantially. Most of the US formulations contain multiple allergens, while fewer than 10% of European formulations contain more than 1 non-cross-reacting allergen.9 Allergists in the US prefer to include all clinically relevant allergens due to concerns over the time investment required for AIT, particularly during the build-up phase. The prevailing view in Europe is to select a most troublesome allergen because polysensitization does not necessarily mean poly-allergy.
Multiallergen AIT (whether with mixed allergens or with the separate administration of multiple allergen extracts) has long been acknowledged as an effective therapy for allergic respiratory disease and has been implemented in double-blind, placebo-controlled trials since the mid-1960s.10 It was also conducted in several rigorously conducted clinical trials evaluating the effect on bronchial hyperreactivity and quality of life.11,12 The primary immunological mechanism of AIT involves a profound modulation of the adaptive immune system, characterized by shifting the immune response away from a T helper cell (Th) 2 phenotype toward a regulatory T and Th1 response.13 Given that a head-to-head comparison of single and multiallergen AIT would be expensive and time-consuming, the number of well-controlled trials focusing on this issue has been relatively scarce. However, recent clinical research conducted over the past few decades provides an opportunity to aggregate new evidence on the efficacy and safety profile of multiallergen AIT.
In this context, polysensitization indicates sensitization to two or more distinct allergens, demonstrated by a positive skin prick test (SPT) with a wheal diameter of ≥3 mm, and/or an allergen-specific IgE (sIgE) level of >0.35KUA/L. Single-allergen immunotherapy includes the use of extracts containing several closely related allergens, and that multiallergen immunotherapy refers to mixtures with little or no cross-reactivity such as grass pollen, tree pollen, weed pollen, house dust mite (HDM), etc.
The use of multiallergen AIT for polysensitized patients remains one of the biggest debates in clinical practice. This systematic review and meta-analysis aim to collect and analyze available data to provide more relatively high-quality evidence for the multiallergen debate. Additionally, a review of the relevant literature can help identify the research gaps within this field and highlight areas that require further investigation.
Methods
Search Strategy and Eligibility Criteria
A comprehensive search was conducted in PubMed, Embase, Web of Science, and Cochrane Library databases to identify relevant studies on polysensitized AR with or without mild/controlled comorbid asthma treated with multiallergen AIT until June 5, 2025 following the PRISMA guidelines.14 The eligibility criteria to include in our systematic review were as follows: (1) Randomized controlled trials (RCTs), cohort studies, and case-control studies; (2) polysensitized patients treated with multiallergen AIT; (3) Clinical outcomes including assessment of symptoms and medication use or safety profile. Search terms used were “immunotherapy” OR “subcutaneous immunotherapy” OR “sublingual immunotherapy” OR “SCIT” OR “SLIT” AND “multiallergen” OR “multi-allergen” OR “polysensitization” OR “polysensitized”. The search strings employed are detailed in the Supplementary Table S1. Relevant articles were manually identified and reviewed. We also searched for clinical trials on Clinicaltrials.gov to include any data that may have been missing from the previous search but found no relevant data. Only studies focusing AR were included in the systematic review. This systematic review was registered on PROSPERO (ID: CRD42024567545).
Inclusion Criteria for Meta-Analysis
To be included in this meta-analysis, study outcomes had to entail data on one or more of the following parameters: (1) combined or separated symptom score and medication score. (2) adverse events after administering AIT, and number of patients discontinued AIT treatment due to adverse effect. The detailed inclusion criteria were presented in the Supplementary Table S2.
Data Extraction
Two authors independently extracted data and used a standardized data extraction form including first and corresponding author, year of publication, study type, disease type, age, gender, disease duration, type of allergens, number of patients and controls, administration, follow-up duration, assessment of outcome and adverse events. Discrepancies identified during data extraction were resolved by consensus meetings of the authors.
Bias Assessment
Quality and risk of bias of included RCTs were assessed by the Cochrane Risk-of-Bias version 2 (RoB 2). The tool consists of five domains, each containing a list of questions linked to specific aspects of the RCT. An algorithm marks the risk of bias in each domain as “low”, “some concerns”, or “high” depending on the answers to the questions. Non-randomized studies were assessed by Newcastle-Ottawa Scale (NOS).
Data Synthesis and Statistical Analysis
The mean and standard deviation (SD) of symptom score and medication score at baseline and post-treatment were extracted from each study in all groups. Some studies reported post-treatment scores at several time points, the last time point (maximum 2 years) was extracted for further analysis. Obtaining SDs for group of means were calculated from 95% confidence intervals (CIs) by using equations from the Cochrane Handbook15 chapter 6.5.2.2 when the group SDs were not provided directly [SD =  ]. When scores were provided in medians and 25th–75th percentile, we converted these into means by Luo et al,16 and SDs by using the equation by Wan et al (Cochrane Handbook chapter 6525).15 Furthermore, when not reported, change-from-baseline SDs were estimated using the equation by Follmann et al assuming a correlation coefficient of 0.50 between baseline and post-intervention values [Cochrane Handbook chapter 6.5.2.8, 2:
]. When scores were provided in medians and 25th–75th percentile, we converted these into means by Luo et al,16 and SDs by using the equation by Wan et al (Cochrane Handbook chapter 6525).15 Furthermore, when not reported, change-from-baseline SDs were estimated using the equation by Follmann et al assuming a correlation coefficient of 0.50 between baseline and post-intervention values [Cochrane Handbook chapter 6.5.2.8, 2:  ].15,17 To verify the robustness of our findings, sensitivity analyses were performed by re-running the models using alternative correlation coefficients (
].15,17 To verify the robustness of our findings, sensitivity analyses were performed by re-running the models using alternative correlation coefficients ( and
and  ). Statistical analyses were performed using Review Manager (RevMan) v5.4 (the Cochrane Collaboration, Copenhagen, Denmark) and R statistical software, version 4.3.1 (http://www.R-project.org/). Pooled results were estimated using 9a random-effects model due to the heterogeneity of included studies. The risk of publication bias was assessed visually by funnel plots symmetry and quantitatively by Egger’s test, with a p value <0.05 indicating statistically significant publication bias. Heterogeneity was tested using I2, with values >50% indicating heterogeneity among studies. A p-value of <0.05 was considered statistically significant. Sensitivity analysis was performed by removing one single study at a time to evaluate its impact on the overall results.
). Statistical analyses were performed using Review Manager (RevMan) v5.4 (the Cochrane Collaboration, Copenhagen, Denmark) and R statistical software, version 4.3.1 (http://www.R-project.org/). Pooled results were estimated using 9a random-effects model due to the heterogeneity of included studies. The risk of publication bias was assessed visually by funnel plots symmetry and quantitatively by Egger’s test, with a p value <0.05 indicating statistically significant publication bias. Heterogeneity was tested using I2, with values >50% indicating heterogeneity among studies. A p-value of <0.05 was considered statistically significant. Sensitivity analysis was performed by removing one single study at a time to evaluate its impact on the overall results.
Results
Literature Search and Characteristics of Included Studies
A flow chart presenting the search and selection process is shown in Figure 1. A total of 14 studies met the eligibility criteria and were included in this systematic review, of which 7 were RCTs, 1 pilot study, and 6 non-randomized studies. Figure 2 presents the risk-of-bias assessment of the included RCTs, while Table 1 summarizes the quality assessment of cohort and case-control studies using the Newcastle-Ottawa Scale (NOS). Random-effect models were used. Bar graphs illustrating the relative contributions of RCTs with each risk-of-bias judgement are shown in Supplementary Figure S1.
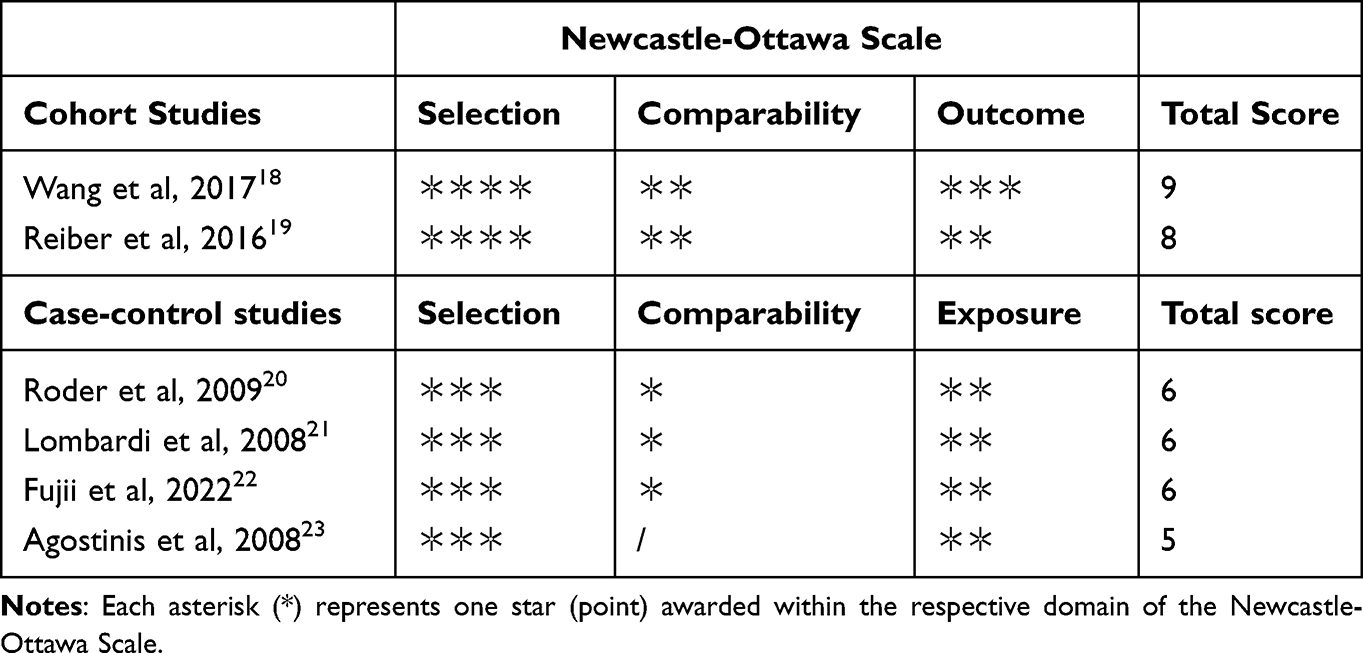 |
Table 1 Assessment of Risk of Bias in Non-Randomized Studies Using Newcastle-Ottawa Scale |
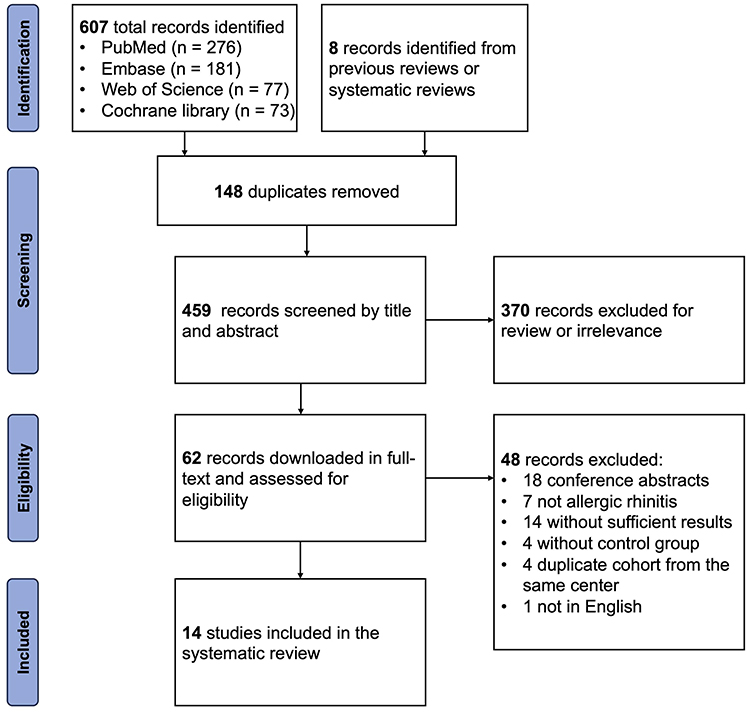 |
Figure 1 Flow diagram of the search and selection process. |
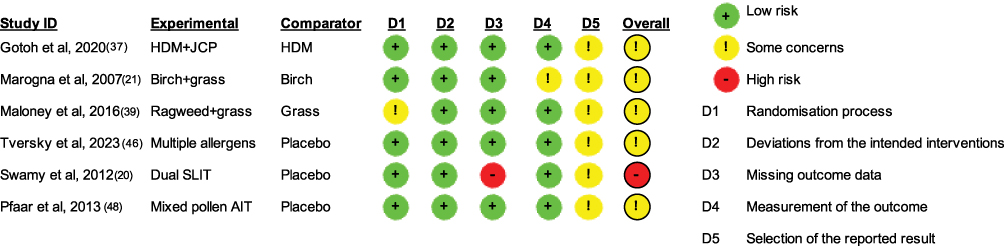 |
Figure 2 Assessment of risk of bias using Cochrane Risk-of-Bias tool 2 for randomized trials. |
The 14 studies analyzed 1692 polysensitized patients with AR in 5 countries Dust mites, tree pollen, and grass pollen were the most common allergens in these polysensitized patients Seven, and 10 of the included treatment protocols were meta-analyzed for treatment effects, safety of multiallergen AIT. The characteristics of the included studies are summarized in Table 2. Among the 7 RCTs, 5 were conducted with a placebo group or drug therapy only group, while 2 of them, and other than those, a pilot study compared AIT of multiple allergens and single allergen. All nonrandomized studies compared multiallergen AIT and AIT using single allergen. In only 5 studies were patients administered AIT treatment via subcutaneous injection, the other via sublingual tablets. One of the included RCT was deemed to have a relatively high risk of bias due to a notable proportion of missing outcomes, which could potentially affect the accuracy of the study results. According to the funnel plot, there appeared to be a publication bias in favor of single-allergen AIT (Supplementary Figure S2A), which was further confirmed by Egger’s linear regression test (p = 0.0014). Visual asymmetry was also examined in the funnel plots for the symptom scores (Supplementary Figure S2B), medication scores (Supplementary Figure S2C), adverse events of randomized studies (Supplementary Figure S2D), and adverse events of non-randomized studies (Supplementary Figure S2E).
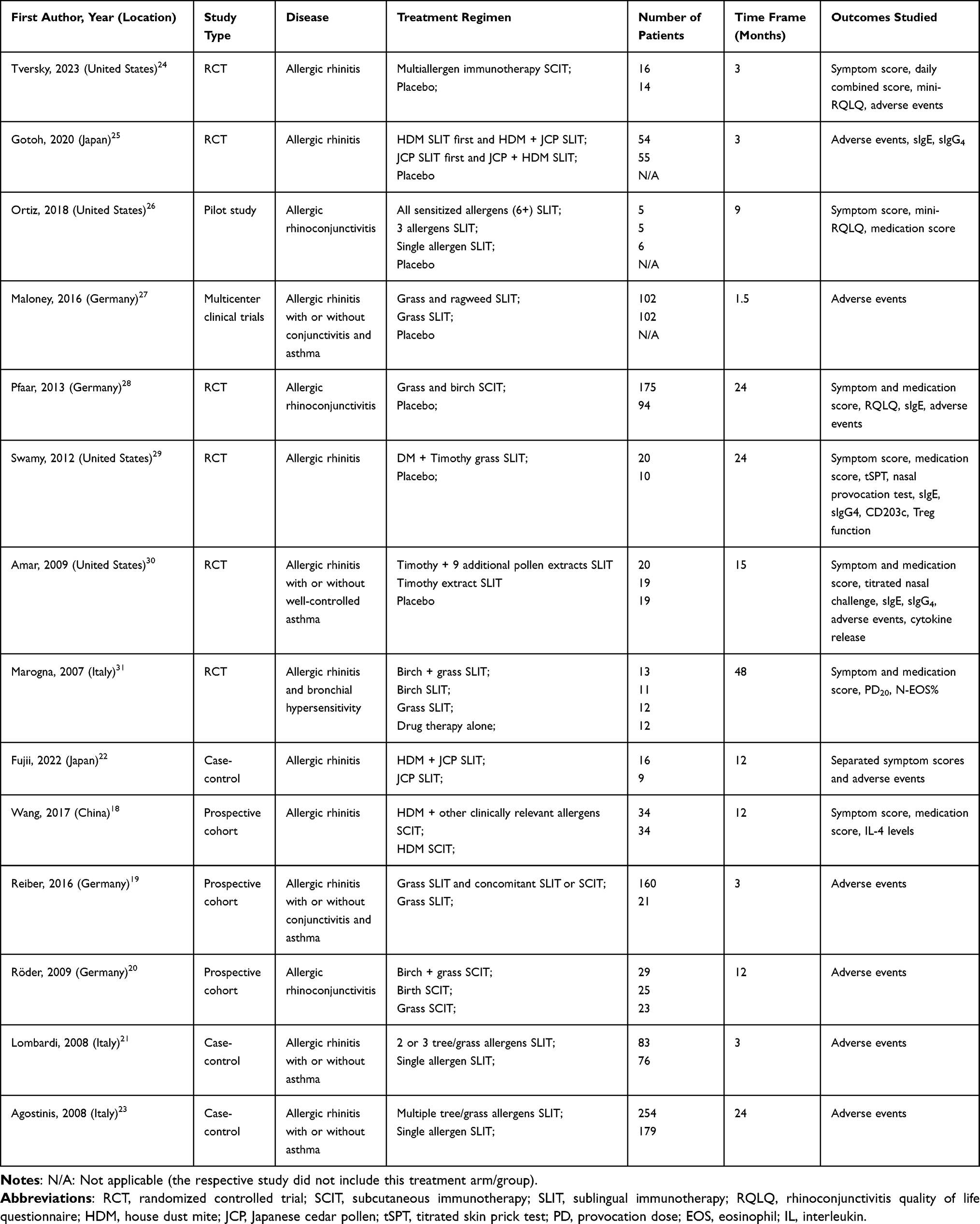 |
Table 2 Characteristics of the Included Studies |
Efficacy of Multiallergen AIT on Polysensitized Patients
First, the efficacy of multiallergen AIT was established by comparing combined symptom and medication score at the last follow-up with placebo or drug therapy only in 5 RCTs, which yielded a standardized mean difference (SMD) of −2.85 (95% CI −4.24, −1.46; p < 0.001, Supplementary Figure S3A). Due to a lack of baseline information, the mean change of combined scores of multiallergen group from baseline was analyzed in 4 RCTs. Results also showed a significantly lower SMD than the control group (SMD −3.75, 95% CI −5.85, −1.65; p < 0.001, Figure 3A). Sensitivity analyses using correlation coefficients of  and
and  yielded consistent results, indicating the robustness of the pooled SMDs. Although calculated I2 indicated high heterogeneity between studies. Then, we performed separate analysis on mean change of symptom score and medication score in randomized trials for multiallergen AIT compared with AIT of single allergen. The SMD of individual studies for symptom scores mostly lie on the side that favors multiallergen AIT, but total SMD and 95% CI was −0.34 (−1.21, 0.52) with a p value of 0.44 (Figure 3B). Multiallergen AIT showed a slightly bigger reduction in medication score with a total SMD of −1.36 (95% CI −2.44, −0.28, p = 0.01; Figure 3C). Symptom score and medication score at the last follow-up showed a significant reduction in multiallergen AIT (SMD −1.75, 95% CI −3.16, −0.34; p = 0.01, Supplementary Figure S3B; SMD −1.30, 95% CI −2.18, −0.43; p = 0.007, Supplementary Figure S3C). Sensitivity analyses showed robustness of the synthesized result. Several studies included titrated nasal challenge and SPT after AIT treatment, but the results differed greatly in their presented form to perform a meta-analysis.29–31
yielded consistent results, indicating the robustness of the pooled SMDs. Although calculated I2 indicated high heterogeneity between studies. Then, we performed separate analysis on mean change of symptom score and medication score in randomized trials for multiallergen AIT compared with AIT of single allergen. The SMD of individual studies for symptom scores mostly lie on the side that favors multiallergen AIT, but total SMD and 95% CI was −0.34 (−1.21, 0.52) with a p value of 0.44 (Figure 3B). Multiallergen AIT showed a slightly bigger reduction in medication score with a total SMD of −1.36 (95% CI −2.44, −0.28, p = 0.01; Figure 3C). Symptom score and medication score at the last follow-up showed a significant reduction in multiallergen AIT (SMD −1.75, 95% CI −3.16, −0.34; p = 0.01, Supplementary Figure S3B; SMD −1.30, 95% CI −2.18, −0.43; p = 0.007, Supplementary Figure S3C). Sensitivity analyses showed robustness of the synthesized result. Several studies included titrated nasal challenge and SPT after AIT treatment, but the results differed greatly in their presented form to perform a meta-analysis.29–31
 |
Figure 3 Meta-analysis of (A) mean change of combined symptom and medication score; (B) mean change of symptom score; (C) mean change of medication score; (D) adverse events of randomized studies; (E) adverse events of non-randomized studies between multiallergen immunotherapy and placebo or single allergen. Abbreviations: CI, confidence interval; HDM, house dust mite; IV, inverse variance; JCP, Japanese cedar pollen; M-H, Mantel-Haenszel; OR, odds ratio; SD, standard deviation; SMD, standardized mean difference. |
The included studies employed a heterogeneous array of allergen types, with combinations such as perennial allergens with tree pollen, perennial allergens with grass pollen, and tree pollen with grass pollen, etc. As a result, it was not feasible to conduct separate discussions based on distinct allergen categories. Nevertheless, studies utilizing dual-allergen approaches in multiallergen immunotherapy yielded noteworthy findings. Specifically, two studies investigated dual-allergen AIT: one RCT compared birch and grass pollen combination therapy against single-allergen SLIT,31 while another case-control study contrasted HDM and Japanese cedar pollen dual therapy with single Japanese cedar pollen therapy.22 Both studies demonstrated that dual-allergen AIT resulted in significantly greater reductions in symptom scores among patients with AR. Other studies comparing dual-allergen AIT with single-allergen AIT consistently reported similar outcomes.
Safety and Immunological Profile of Multiallergen AIT on Polysensitized Patients
The majority of reported adverse events were mild or localized events associated with routes of administration including injection site wheal, oral irritation, mouth swelling, throat irritation, etc. Randomized studies and non-randomized studies were analyzed separately. In both analyses, the multiallergen AIT group and the single allergen group had a similar incidence of adverse events. Among randomized studies, the meta-analysis revealed an odds ratio (OR) of 0.58 (95% CI 0.35, 0.96, p = 0.03; Figure 3D). The multiallergen group had a slightly safer profile because of the Maloney study. Regarding non-randomized studies, the OR was 0.86 (95% CI 0.64, 1.15, p = 0.3; Figure 3E). The incidence of discontinuation due to adverse events was also similar between the two groups in both randomized and non-randomized studies (data not shown). The calculated I2 values were below 50%, indicating a high level of homogeneity. Adverse events leading to discontinuation recorded in the studies include persistent oral itching, lip and mouth swelling.
Multiallergen AIT induced notable immunological changes in polysensitized patients with AR. Studies by Amar and Gotoh both reported elevated levels of sIgE, whereas Gotoh’s study also demonstrated this elevation in allergen-specific IgG4 (sIgG4). Additionally, Wang and Amar observed reductions in interleukin-4 (IL-4) and interferon-γ (IFN-γ) levels, suggesting enhanced immune tolerance and modulation of the type 2 immune response. Compared with single-allergen AIT, multiallergen approaches demonstrated comparable effects on IL-4 suppression and sIgE/sIgG4 elevations. However, certain indicators like IFN-γ showed attenuated responses in multiallergen groups, potentially due to antigen competition.
Discussion
To our knowledge, this is the first and most comprehensive systematic review and meta-analysis summarizing the efficacy and safety of multiallergen AIT compared to single-allergen AIT. The results suggest that multiallergen AIT is effective in the treatment of polysensitized AR patients. There was no clear or definitive indication that the clinical efficacy of multiallergen AIT was superior to that of single-allergen AIT, although formulations of multiple allergens do not seem to cause more adverse events. This study covers different categories of allergen and routes of administration including subcutaneous immunotherapy (SCIT) and sublingual immunotherapy (SLIT), though they were not analyzed separately due to the limited number of studies.
Numerous studies have examined the efficacy of single-allergen AIT in both mono- and polysensitized patients. Several cohort studies investigating the clinical effectiveness of short-term dust mite AIT found no significant difference between polysensitized and monosensitized patients.32,33 A post-hoc analysis of a clinical trial with grass pollen SLIT34 separately analyzed monosensitized patients and pollen polysensitized patients. The results showed significant reductions in symptom and medication use, regardless of their sensitization profile. Similar results were reported by another post-hoc analysis by Malling et al35 of a sublingual tablet containing 5 related grass pollens. An Italian team published consecutive trials with possibly overlapping patients that confirmed primarily single-allergen SLIT improved symptom and quality of life in polysensitized patients.36–39 However, the course of treatment was relatively short and the time of symptom evaluation was not clear enough to draw a conclusion whether AIT of a certain seasonal allergen could improve symptoms caused by allergens in different season or perennial allergens. A review on multiallergen AIT for patients with AR and asthma published by Nelson40 identified 13 studies between 1961 and 2007 in which 2 or more unrelated allergens were simultaneously administered. Although results were not reported separately for single or multiple allergens in several studies, and the population was not clarified to be polysensitized patients, the findings of this review strongly suggest that the simultaneous delivery of multiple unrelated allergens can be clinically effective.
The selection of multiple allergens for AIT should be approached with caution. First of all, the clinically relevant allergens must be properly identified, defined as those with demonstrable sIgE positivity and clinical relevance. According to the US practice update,7 “inclusion of allergens to which IgE antibodies are present but that are not clinically relevant might dilute the essential allergen components of the allergen immunotherapy extract so that immunotherapy might be less effective”. The premise of mixing multiple allergens is to ensure the effective concentration of each allergen. Also, certain allergens containing cockroach or mold extracts have a risk of proteolytic degradation of other allergen extracts.41,42 Formulations containing cockroach or mold extracts should be administered separately. Appropriately chosen allergens, correct dosage, and pharmaceutical stability could be hard to achieve, potentially affecting the efficacy of multiallergen AIT.
Safety issues were raised by some case reports that prescribed AIT of multiple allergen extracts and led to severe adverse effects.43,44 Some of the included studies sought to determine whether multiallergen AIT increases the risk of adverse events.19–23,25,27 It turned out the majority of the studies observed no significant differences in safety profile between the groups, and our meta-analysis had the same conclusion with low heterogeneity. Available evidence suggests that appropriately administered AIT utilizing standardized extracts, when prescribed at clinically validated dosages and limited to an appropriate number of allergens, does not appear to elevate the incidence of adverse events in polysensitized patients compared to single-allergen protocols.
Whether the change of sIgE or sIgG4 could be used as a biomarker of AIT has been controversial. Yang et al45 conducted a case-control study and found the changes of sIgE, sIgG4, sIgE/sIgG4 ratio had no correlations with the improvement of combined symptom and medication score after AIT. While a subgroup of RCT showed evidence for coordinated sIgE and sIgG4 responses in subjects benefiting the most from AIT.46 However, there is evidence that polysensitized patients present distinct immune responses. Prigione et al47 found that peripheral blood mononuclear cells from patients who remained mono-sensitized produced higher levels of IFN-γ than cells from patients who had become polysensitized. The different immune reactivity made it complicated to determine interpretation of the changed immunological parameters.
Integrating the findings from our meta-analysis and narrative synthesis, multiple studies comparing dual-allergen AIT with single-allergen AIT have demonstrated superior outcomes for the dual approach, potentially offering enhanced efficacy in polysensitized patients with AR while maintaining comparable safety profiles. Balancing the economic implications of incorporating additional allergens into AIT regimens, the current evidence leans toward recommending dual-allergen AIT using clinically relevant allergens for polysensitized individuals, as this strategy may optimize therapeutic benefits without substantial increases in risk or cost.
Given the limited number and variability of studies, the results of this meta-analysis should be interpreted with caution. The lack of standardization of study protocols concerning AIT poses a difficulty in forming high quality clinical trials and meta-analysis. Another limitation involves the potential dilution and degradation within mixed formulations. As studies rarely assessed the precise final active concentrations, the therapeutic efficacy of multiallergen formulations might have been underestimated. Additionally, publication bias may have been an issue, as negative results may not have been reported. The included studies exhibited a wide range of follow-up duration, introducing inherent clinical heterogeneity. This should be considered when interpreting our findings. Also, our findings regarding safety outcomes warrant careful consideration, as the inclusion of non-randomized cohort and case-control studies introduces inherent confounding bias.
Conclusion
In conclusion, findings from our systematic review demonstrate that multiallergen AIT exhibits no significant difference in therapeutic efficacy compared to single-allergen therapy in polysensitized patients with AR. Moreover, multiallergen AIT does not appear to increase the incidence of overall adverse events or treatment discontinuation due to side effects. However, significant heterogeneity across studies, particularly in administer routes, treatment protocols, and the format in which results are presented, calls for more robust clinical trials to further clarify the optimal approach for treating polysensitized patients with AIT.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval
Ethical approval was not required for this systematic review and meta-analysis as it involved the synthesis of previously published data and did not include new data collection from human participants. This systematic review was registered on PROSPERO (ID: CRD42024567545).
Acknowledgments
The authors would like to thank professor Stephan R. Durham and Dr. Martin Penagos for their thorough review and insightful comments, which substantially enhanced the quality of this manuscript. Also, the authors thank the participants of the included studies for their contributions. The abstract of this paper was presented at the 2026 AAAAI Annual Meeting as a poster presentation with interim findings. The poster’s abstract was published in ‘Poster Abstracts’ in The Journal of Allergy and Clinical Immunology: 10.1016/j.jaci.2025.12.952.
Funding
This study was supported by the National Natural Science Foundation of China (No. 82370041), Peking Union Medical College Hospital Talent Cultivation Program (Category B) (No. UGG06079), Noncommunicable Chronic Diseases-National Science and Technology Major Project (No. 2025ZD0548700), the Fundamental Research Funds for the Central Universities, Peking Union Medical College (No. 3332025091), and Peking Union Medical College Hospital Talent Cultivation Program Category D (UHB12266).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Noon L. Prophylactic inoculation against hay fever. Lancet. 1911;177(4580):1572–12. doi:10.1016/S0140-6736(00)78276-6
2. Zenner HP, Baumgarten C, Rasp G, et al. Short-term immunotherapy: a prospective, randomized, double-blind, placebo-controlled multicenter study of molecular standardized grass and rye allergens in patients with grass pollen-induced allergic rhinitis. J Allergy Clin Immunol. 1997;100(1):23–29. doi:10.1016/S0091-6749(97)70190-8
3. Roberts G, Hurley C, Turcanu V, Lack G. Grass pollen immunotherapy as an effective therapy for childhood seasonal allergic asthma. J Allergy Clin Immunol. 2006;117(2):263–268. doi:10.1016/j.jaci.2005.09.054
4. Bousquet PJ, Castelli C, Daures JP, et al. Assessment of allergen sensitization in a general population-based survey (European community respiratory health survey I). Ann Epidemiol. 2010;20(11):797–803. doi:10.1016/j.annepidem.2010.05.012
5. Arbes SJ Jr, Gergen PJ, Elliott L, Zeldin DC. Prevalences of positive skin test responses to 10 common allergens in the US population: results from the third National Health and Nutrition Examination Survey. J Allergy Clin Immunol. 2005;116(2):377–383. doi:10.1016/j.jaci.2005.05.017
6. Craig TJ, King TS, Lemanske RF Jr, et al. Aeroallergen sensitization correlates with PC(20) and exhaled nitric oxide in subjects with mild-to-moderate asthma. J Allergy Clin Immunol. 2008;121(3):671–677. doi:10.1016/j.jaci.2007.12.1153
7. Cox L, Nelson H, Lockey R, et al. Allergen immunotherapy: a practice parameter third update. J Allergy Clin Immunol. 2011;127(1 Suppl):S1–55. doi:10.1016/j.jaci.2010.09.034
8. Roberts G, Pfaar O, Akdis CA, et al. EAACI Guidelines on allergen immunotherapy: allergic rhinoconjunctivitis. Allergy. 2018;73(4):765–798. doi:10.1111/all.13317
9. Cox L, Jacobsen L. Comparison of allergen immunotherapy practice patterns in the United States and Europe. Ann Allergy Asthma Immunol. 2009;103(6):451–459. (). doi:10.1016/S1081-1206(10)60259-1
10. Lowell FC, Franklin W. A double-blind study of the effectiveness and specificity of injection therapy in ragweed hay fever. N Engl J Med. 1965;273(13):675–679. doi:10.1056/NEJM196509232731302
11. Hedlin G, Wille S, Browaldh L, et al. Immunotherapy in children with allergic asthma: effect on bronchial hyperreactivity and pharmacotherapy. J Allergy Clin Immunol. 1999;103(4):609–614. doi:10.1016/S0091-6749(99)70232-0
12. Alvarez-Cuesta E, Aragoneses-Gilsanz E, Martín-Garcia C, Berges-Gimeno P, Gonzalez-Mancebo E, Cuesta-Herranz J. Immunotherapy with depigmented glutaraldehyde-polymerized extracts: changes in quality of life. Clin Exp Allergy. 2005;35(5):572–578. doi:10.1111/j.1365-2222.2005.02245.x
13. Gueguen C, Bouley J, Moussu H, et al. Changes in markers associated with dendritic cells driving the differentiation of either TH2 cells or regulatory T cells correlate with clinical benefit during allergen immunotherapy. J Allergy Clin Immunol. 2016;137(2):545–558. doi:10.1016/j.jaci.2015.09.015
14. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700.
15. Higgins JPTTJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane Handbook for Systematic Reviews of Interventions.
16. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
17. Follmann D, Elliott P, Suh I, Cutler J. Variance imputation for overviews of clinical trials with continuous response. J Clin Epidemiol. 1992;45(7):769–773. doi:10.1016/0895-4356(92)90054-Q
18. Wang ZX, Shi H. Single-allergen sublingual immunotherapy versus multi-allergen subcutaneous immunotherapy for children with allergic rhinitis. Hua zhong ke ji da xue xue bao Yi xue Ying De wen ban. J Huazhong Univ Sci Technol Med Sci. 2017;37(3):
19. Reiber R, Keller M, Keller W, Wolf H, Schnitker J, Wüstenberg E. Tolerability of the SQ-standardised grass sublingual immunotherapy tablet in patients treated with concomitant allergy immunotherapy: a non-interventional observational study. Clin Transl Allergy. 2015;6:9. doi:10.1186/s13601-016-0097-8
20. Röder A, Darrelmann N, Klingenberg W, Krüll M, Suttorp N, Noga O. Simultaneous SCIT with 2 separate allergen extracts demonstrates comparable safety compared to SCIT with a single allergen extract. J Investig Allergol Clin Immunol. 2009;19(6):512–513.
21. Lombardi C, Gargioni S, Cottini M, Canonica GW, Passalacqua G. The safety of sublingual immunotherapy with one or more allergens in adults. Allergy. 2008;63(3):375–376. doi:10.1111/j.1398-9995.2007.01608.x
22. Fujii T, Kitamura Y, Kamimura S, Ishitani K, Takeda N. Efficacy of dual sublingual immunotherapy with Japanese cedar pollen and house dust mite allergens in patients with allergic rhinitis sensitized to multiple allergens. Laryngoscope Investig Otolaryngol. 2022;7(1):36–42. doi:10.1002/lio2.740
23. Agostinis F, Foglia C, Landi M, et al. The safety of sublingual immunotherapy with one or multiple pollen allergens in children. Allergy. 2008;63(12):1637–1639. doi:10.1111/j.1398-9995.2008.01742.x
24. Tversky J, Patel P, Sowho M, et al. Randomized double-blind pilot study of universal, species abundant, multiallergen subcutaneous immunotherapy for moderate-severe allergic rhinitis. Ann Allergy Asthma Immunol. 2023;131(1):
25. Gotoh M, Okubo K, Yuta A, et al. Safety profile and immunological response of dual sublingual immunotherapy with house dust mite tablet and Japanese cedar pollen tablet. Allergol Int. 2020;69(1):104–110. doi:10.1016/j.alit.2019.07.007
26. Ortiz AS, McMains KC, Laury AM. Single vs multiallergen sublingual immunotherapy in the polysensitized patient: a pilot study. Int Forum Allergy Rhinol. 2018;8(4):
27. Maloney J, Berman G, Gagnon R, et al. Sequential treatment initiation with timothy grass and ragweed sublingual immunotherapy tablets followed by simultaneous treatment is well tolerated. J Allergy Clin Immunol Pract. 2016;4(2):301–9.e2. doi:10.1016/j.jaip.2015.11.004
28. Pfaar O, Biedermann T, Klimek L, Sager A, Robinson DS. Depigmented-polymerized mixed grass/birch pollen extract immunotherapy is effective in polysensitized patients. Allergy. 2013;68(10):
29. Swamy RS, Reshamwala N, Hunter T, et al. Epigenetic modifications and improved regulatory T-cell function in subjects undergoing dual sublingual immunotherapy. J Allergy Clin Immunol. 2012;130(1):
30. Amar SM, Harbeck RJ, Sills M, Silveira LJ, O’Brien H, Nelson HS. Response to sublingual immunotherapy with grass pollen extract: monotherapy versus combination in a multiallergen extract. J Allergy Clin Immunol. 2009;124(1):
31. Marogna M, Spadolini I, Massolo A, et al. Effects of sublingual immunotherapy for multiple or single allergens in polysensitized patients. Ann Allergy Asthma Immunol. 2007;98(3):274–280. doi:10.1016/S1081-1206(10)60718-1
32. Li P, Li Q, Huang Z, Chen W, Lu Y, Tian M. Efficacy and safety of house dust mite sublingual immunotherapy in monosensitized and polysensitized children with respiratory allergic diseases. Int Forum Allergy Rhinol. 2014;4(10):796–801. doi:10.1002/alr.21397
33. Soyyigit S, Guloglu D, Ikinciogullari A, et al. Immunologic alterations and efficacy of subcutaneous immunotherapy with Dermatophagoides pteronyssinus in monosensitized and polysensitized patients. Ann Allergy Asthma Immunol. 2016;116(3):244–51.e2. doi:10.1016/j.anai.2016.01.002
34. Emminger W, Durham SR, Riis B, Maloney J, Nolte H. The efficacy of single-grass-allergen-immunotherapy-tablet treatment in mono- and multi-sensitized allergic rhinitis patients: findings from a post hoc analysis. J Allergy Clin Immunol. 2009;123(2):S75. doi:10.1016/j.jaci.2008.12.257
35. Malling HJ, Montagut A, Melac M, et al. Efficacy and safety of 5-grass pollen sublingual immunotherapy tablets in patients with different clinical profiles of allergic rhinoconjunctivitis. Clin Exp Allergy. 2009;39(3):387–393. doi:10.1111/j.1365-2222.2008.03152.x
36. Ciprandi G, Cadario G, Valle C, et al. Sublingual immunotherapy in polysensitized patients: effect on quality of life. J Investig Allergol Clin Immunol. 2010;20(4):274–279.
37. Ciprandi G, Incorvaia C, Puccinelli P, Scurati S, Masieri S, Frati F. The POLISMAIL lesson: sublingual immunotherapy may be prescribed also in polysensitized patients. Inter J Immuno Pharmacol. 2010;23(2):637–640. doi:10.1177/039463201002300227
38. Ciprandi G, Cadario G, Di Gioacchino M, et al. Sublingual immunotherapy in polysensitized allergic patients with rhinitis and/or asthma: allergist choices and treatment efficacy. J Biol Regul Homeost Agents. 2009;23(3):165–171.
39. Ciprandi G, Cadario G, Di Gioacchino GM, et al. Sublingual immunotherapy in children with allergic polysensitization. Allergy Asthma Proc. 2010;31(3):227–231. doi:10.2500/aap.2010.31.3337
40. Nelson HS. Multiallergen immunotherapy for allergic rhinitis and asthma. J Allergy Clin Immunol. 2009;123(4):763–769. doi:10.1016/j.jaci.2008.12.013
41. Grier TJ, LeFevre DM, Duncan EA, Esch RE. Stability of standardized grass, dust mite, cat, and short ragweed allergens after mixing with mold or cockroach extracts. Ann Allergy Asthma Immunol. 2007;99(2):151–160. doi:10.1016/S1081-1206(10)60639-4
42. Grier TJ, LeFevre DM, Duncan EA, Esch RE, Coyne TC. Allergen stabilities and compatibilities in mixtures of high-protease fungal and insect extracts. Ann Allergy Asthma Immunol. 2012;108(6):439–447. doi:10.1016/j.anai.2012.04.012
43. Eifan AO, Keles S, Bahceciler NN, Barlan IB. Anaphylaxis to multiple pollen allergen sublingual immunotherapy. Allergy. 2007;62(5):567–568. doi:10.1111/j.1398-9995.2006.01301.x
44. Dunsky EH, Goldstein MF, Dvorin DJ, Belecanech GA. Anaphylaxis to sublingual immunotherapy. Allergy. 2006;61(10):1235. doi:10.1111/j.1398-9995.2006.01137.x
45. Yang L, Yang Y, Xu Q, et al. Specific IgE and IgG4 profiles of house dust mite components in allergen-specific immunotherapy. Front Immunol. 2021;12:786738. doi:10.3389/fimmu.2021.786738
46. Bordas-Le Floch V, Berjont N, Batard T, et al. Coordinated IgG2 and IgE responses as a marker of allergen immunotherapy efficacy. Allergy. 2022;77(4):1263–1273. doi:10.1111/all.15107
47. Prigione I, Morandi F, Tosca MA, et al. Interferon-gamma and IL-10 may protect from allergic polysensitization in children: preliminary evidence. Allergy. 2010;65(6):740–742. doi:10.1111/j.1398-9995.2009.02285.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Systemic Immune Dysregulation in Allergic Rhinitis: Mechanisms, Comorbidities, and Implications for Targeted Therapy
Hui D, Shi C, Fan Y, Han M, Wang Y, Sun J, Xue Y, Li E
Journal of Asthma and Allergy 2026, 19:589195
Published Date: 9 March 2026
Advances in Nanotechnology-Based Immunomodulatory Strategies for the Treatment of Allergic Rhinitis
Liu X, Zhao W
International Journal of Nanomedicine 2026, 21:620098
Published Date: 22 June 2026