Back to Journals » International Journal of Women's Health » Volume 12
Multi-stakeholder Perspectives on the Maternal, Provider, Institutional, Community, and Policy Drivers of Disrespectful Maternity Care in South-East Nigeria
Authors Okedo-Alex IN, Akamike IC, Nwafor JI ![]() , Abateneh DD
, Abateneh DD ![]() , Uneke CJ
, Uneke CJ ![]()
Received 19 August 2020
Accepted for publication 25 November 2020
Published 7 December 2020 Volume 2020:12 Pages 1145—1159
DOI https://doi.org/10.2147/IJWH.S277827
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Ijeoma Nkem Okedo-Alex,1,2 Ifeyinwa Chizoba Akamike,1,2 Johnbosco Ifunanya Nwafor,3 Dejene Derseh Abateneh,4 Chigozie Jesse Uneke2
1Department of Community Medicine, Alex Ekwueme Federal University Teaching Hospital, Abakaliki, Ebonyi State, Nigeria; 2African Institute for Health Policy and Health Systems, Ebonyi State University (EBSU), Abakaliki, Nigeria; 3Department of Obstetrics and Gynaecology, Alex Ekwueme Federal University Teaching Hospital, Abakaliki, Ebonyi State, Nigeria; 4Department of Medical Laboratory Sciences, Menelik II College of Medicine and Health Sciences, Kotebe Metropolitan University, Addis Ababa, Ethiopia
Correspondence: Ijeoma Nkem Okedo-Alex
African Institute for Health Policy and Health Systems, Ebonyi State University (EBSU), Abakaliki, Nigeria
Email [email protected]
Dejene Derseh Abateneh
Department of Medical Laboratory Sciences, Menelik II College of Medicine and Health Sciences, Kotebe Metropolitan University, Addis Ababa, Ethiopia
Tel +251920514158
Email [email protected]
Purpose: Understanding the contextualized perspectives of stakeholders involved in maternal health care is critical to promoting respectful maternity care. This study explored maternal, provider, institutional, community, and policy level drivers of disrespectful maternity care in Southeast Nigeria. This study also identified multi-stakeholder perspectives on solutions to implementing respectful maternity care in health facilities.
Materials and Methods: This was a mixed-methods cross-sectional study conducted in two urban cities of Ebonyi State, South-eastern Nigeria. Data were collected using semi-structured questionnaires, focus group discussions, and key informant interviews with mothers, providers, senior facility obstetric decision-makers, ministry of health policymaker, and community members. Quantitative data and qualitative data were analysed using SPSS version 20 and manual thematic analysis, respectively.
Results: Maternal level drivers were poor antenatal clinic attendance, uncooperative clients, non-provision of birthing materials, and low awareness of rights. Provider factors included work overload/stress, training gaps, desire for good obstetric outcome, under-remuneration and under-appreciation. Institutional drivers were poor work environments including poorly designed wards for privacy, stressful hospital protocols, and non-provision of work equipment. Community-level drivers were poor female autonomy, empowerment, and normalization of disrespect and abuse during childbirth. The absence of targeted policies and the high cost of maternal health services were identified as policy-related drivers.
Conclusion: A variety of multi-level drivers of disrespectful maternity care were identified. A diverse and inclusive multi-stakeholder approach should underline efforts to mitigate disrespectful maternity care and promote respectful, equitable, and quality maternal health care.
Keywords: respectful maternity care, disrespect and abuse during childbirth, facility-based childbirth, drivers, Nigeria
Introduction
Women of childbearing deserve respectful care and protection of their autonomy and rights especially in times of heightened vulnerability such as pregnancy and childbirth.1 Despite the availability of maternal health services, disrespectful and abusive care oftentimes compromises the quality and perceived quality of care. Disrespect and abuse (D&A) during childbirth in health facilities and poor quality of care have been shown to significantly contribute to preventable maternal mortality.2,3 It can result in a preference for non-skilled obstetric care such as traditional birth attendants or no care at all as in the case of women who deliver at home.4–8 This is particularly worrisome given that D&A during childbirth could negatively impact facility-based childbirth (and skilled birth attendance by extension) with a possible increase in maternal and child mortality due to non/poor or delayed access to life-saving interventions, and management.9–12
The need to prevent and eliminate disrespect and abuse in maternal care has led to an increased global focus on respectful maternity care with a collaborative approach. This has been exemplified in the charter on the universal rights of childbearing women, mother-baby friendly birthing facility initiative, the World Health Organization’s statement on prevention, and elimination of disrespect and abuse during facility-based childbirth and standards for improving the quality of maternal and newborn care in health facilities.1,13–15
The burden of disrespect and abuse during childbirth in Nigeria has been estimated and described from the perspectives of both mothers and providers. A systematic review on D&A during childbirth also conducted in Nigeria reported a prevalence of 11–98% from the studies included in the review. The highest prevalence of 98% was reported in Enugu, a State in Southeast Nigeria.16 In Ebonyi State, 39.1% and 73.1% of maternal health providers reported perpetrating and witnessing D&A during childbirth, respectively.17 Various categories of D&A during childbirth have also been documented in Nigeria mostly using qualitative study designs.18–20 Studies have shown that both mothers and service providers have deemed mistreatment during childbirth necessary when women were disobedient, uncooperative, or in a bid to save the life of the baby. The mistreatment of women during childbirth has also been considered appropriate and acceptable in order to gain compliance from the woman and ensure a good outcome for the baby.19,21 This is referred to as normalization, a phenomenon in which disrespect and abuse during childbirth are considered the norm among providers, or has become the expected standard of care by clients such that it is not recognized as wrong in the health system.22 This can bias both maternal and provider estimates of D&A during childbirth thus making abusive care less visible. It also emphasizes the need for objective assessments using standardized and structured checklists.23
Since D&A during childbirth can impact women’s decision about utilising health facilities for the present or subsequent births and even for non-maternal health concerns, it is important to identify barriers that discourage positive birthing experiences and address them at all levels and components of the health system.24 A variety of factors have been found to facilitate mistreatment during childbirth spanning individual, provider, facility, and policy factors. These include maternal socioeconomic status, parity, health provider type, heavy workload, and lack of professional development/training opportunities, inadequate infrastructure, and supplies. Other drivers were insufficient funds, poor planning, accepted norms and gender inequalities, normalization of D&A during childbirth, weak implementation of existing policies, lack of accountability, and inadequate legal redress mechanisms.16,25–32 As part of situational analysis, a desk review of major policies on health and reproductive health in Nigeria for content on respectful maternity care and quality of care in maternal health preceded this study. The policies reviewed were the National Health policy 2016, National reproductive health policy 2017, and National Reproductive Health Strategic framework 2002–2006.33–35 None of the policies specifically mentioned respectful care or Respectful Maternity Care (RMC) however all the policies had statements on improving patient care experiences. Although these policies did not explicitly mention respectful care or RMC, their proper implementation, monitoring, and review are expected to contribute towards promoting RMC. The aim of this study was to explore maternal, provider, institutional, community, and policy level drivers of disrespectful maternity care in Southeast Nigeria. This study also identified multi-stakeholder perspectives on solutions to implementing respectful maternity care in health facilities.
Materials and Methods
Study Area
This study was conducted in Abakaliki and Afikpo, the two major cities in Ebonyi State, Southeast Nigeria. There are three senatorial zones and thirteen Local Government Areas (LGAs) in the State. Infants (under one year) constitute 4%, the under-five children 20%, and women of childbearing make up 22% of the population.36 About 75% of the population is involved in subsistence agriculture as their major economic activity. The health facilities in Ebonyi State are as follows: 2 tertiary hospitals, 13 general hospitals, 534 primary health centers, and 6 faith-based (mission) hospitals.36 Ebonyi State has the lowest rates of facility-based births (41%) and skilled birth attendance (46%) in South-Eastern Nigeria.37
The study was conducted in the teaching hospital and a mission hospital in the State. The two hospitals were purposively selected because they are referral facilities for obstetric services with high obstetric client load and patronage in the State. Furthermore, the choice of a public (teaching hospital) and private (mission hospital) provided insights on experiences in facilities with different ownership/funding arrangements. The Obstetrics and Gynecology department in the teaching hospital comprising consultants, resident doctors, house officers, and midwives provide obstetric care services in outpatient clinics and wards. During the study, there were about 40 consultants, 80 resident doctors, 38 house officers, and 69 midwives in the department. On a monthly basis, about 150 childbirths occur in the facility. Similarly, maternal services in the mission hospital are provided by 6 doctors and 27 midwives in the department of Obstetrics and Gynecology. An average of 85 births occurs in the mission hospital monthly. Both hospitals run weekly immunization clinics with about 100–150 mother-baby pairs in attendance per week.
Study Design and Participants
This was a cross-sectional survey using a mixed-methods approach. A mixed-method approach was used because mixed methodologies are recommended for research on the complex and dynamic issue of mistreatment during childbirth. They have been found to provide more comprehensive information than single methods.38 The participants in the quantitative survey were maternal health care providers (doctors and nurses) while the qualitative aspect involved facility-level obstetrics, decision-makers, mothers, and community stakeholders. Resident doctors and house officers who were undergoing or had recently completed obstetrics and gynecology posting were targeted for the study because, in the hierarchy of care, they are usually the first contact with the patient and tend to spend more time with the patient than the consultants. All employed midwives in the department were eligible to participate in the study.
Data Collection Activities
This study involved both quantitative and qualitative data collection using self-administered questionnaires, focus group discussions (FGDs), and key informant interviews (KIIs). Data were collected from September 2018 to February 2019 as part of a larger study.
Qualitative Data Collection
The study population was doctors, midwives, mothers, facility-level obstetric decision-makers, policymakers, and community members. Resident doctors and midwives in the departments of obstetrics and gynecology and mothers (0–14weeks post-childbirth) recruited through the immunization clinics in both hospitals participated in the FGDs. The key informants included: the chief resident obstetrics and gynecology department of the teaching hospital, chief nursing officer/matron in charge of Labor ward in the 2 facilities, and the head of the reproductive health unit at the State ministry of health. To get a community perspective of D&A during childbirth and its drivers, two husbands whose wives birthed in the health facilities, and a market leader were also interviewed as key informants.
Participants for the qualitative aspect of the study were purposively selected. Health providers who were outspoken and willing to participate were selected with the aid of the departmental and unit heads. The key informants were selected based on individuals/providers who played key roles in maternal health at the family, facility, and ministry of health or community levels. Previous personal use or witness of use of the hospital by someone close such as family member/neighbor for childbirth and willingness to participate/share experiences informed the selection of the husbands and community leader.
Information was collected using discussion and key informant interview guides adapted previous studies and they explored the multi-level drivers of disrespect and abuse during childbirth in health facilities based on classifications by Bowser, Bohren, and Freedman.22,31,32,39–42 The FGD and KII guides also sought recommendations for mitigating D&A during childbirth from the participants.
The FGDs and interviews were conducted in the English language. The principal investigator moderated the FGDs assisted by 2 research assistants: an electronic recorder handler and a note-taker who recorded key issues raised (including non-verbal responses). The researcher was the moderator and an electronic audio recorder was used to record the FGDs. The FGDs had 8–9 participants each and lasted an average of 45 minutes and were terminated following data saturation. The FGDs were held in a serene environment within the health facilities that afforded privacy and was consensually agreed on by the discussants and the researcher. The key informant interviews were also conducted in the English language. Each interview was held in a designated quiet location as preferred by the key informant, lasted approximately an hour, and ended after data saturation was reached. Recording of the interviews was done using an electronic audio recorder. Two FGDs were held with the midwives while one was held with doctors. Four FGDs were held with mothers (two per facility). Seven KIIs were also held.
The study participants were approached face-to-face and gave written informed consent and approval to record the FGDs and KIIs before commencing the discussions and interviews. Participation was voluntary and confidentiality of responses was ensured. All the participants were aware that they were at liberty to withdraw from the study at any point without feeling obligated or being afraid of repercussions however none opted out. The anonymity of the participants was also ensured. After proof-reading and correcting the anonymised transcripts, the transcripts for both the FGDs and KIIs were saved on a password-protected computer.
Quantitative Data Collection
Data were collected from 156 health providers and the minimum sample size was calculated using the formula for a single proportion.43,44 Given the sensitive nature of the subject matter, all the participants who were willing to participate were included in the study. A detailed explanation of the sample size determination and sampling has been presented in another paper.17
The questionnaire collected information on the socio-demographics of the respondents and drivers of D&A during childbirth classified as maternal, provider, community, facility, and policy factors. Furthermore, respondents were asked to propose the three most important solutions for addressing the identified drivers. Doctors and midwives working in the teaching hospital participated in the questionnaire-based survey. The study participants were approached face-to-face, and the self-administered paper-based questionnaires were distributed by the researcher and five trained research assistants who were resident doctors in Community medicine. The researcher and research assistants were totally uninvolved in the care of the women during pregnancy and childbirth in the health facility.
Data Analysis
Quantitative Data Analysis
The quantitative data entry and was analyzed using Statistical Package for Social Sciences (IBM-SPSS) for Microsoft Windows version 20 software. Descriptive statistics of the variables: relevant means, standard deviations, and proportions were calculated, and the results presented using frequency tables.
Qualitative Data Analysis
Manual thematic analysis was employed in qualitative data analysis using a deductive approach based on existing categories of drivers of D&A during childbirth. At first, the recordings from focus group discussions and key informant interviews were transcribed verbatim and the transcripts compared with the hand-written notes. This was done to confirm that the data were properly captured including non-verbal responses. Some responses were quoted verbatim to capture the original ideas of the participants and informants. Themes envisaged from the discussion and interview guides were then used to develop an initial coding framework. Following this, the transcripts were compared with the coding framework to detect other themes not present in the coding framework. The revised coding framework was then applied to all the transcripts. Two data coders were involved in data coding. In the final coding framework, the overarching themes fit into the categories of drivers of D&A during childbirth initially proposed, namely, maternal, provider, facility, community, and policy drivers. The themes, sub-themes, and sub-categories were summarized in a table.
Results
Study Participants Characteristics
The mean age of the respondents was 31.97 ±6.82. The majority of the respondents were males (64.1%), unmarried (53.2%), and doctors (74.4%). Over half of the respondents (59.6%) had ever had a child. About half of the respondents (52.6%) earned $278.00-$556 monthly (Table 1)
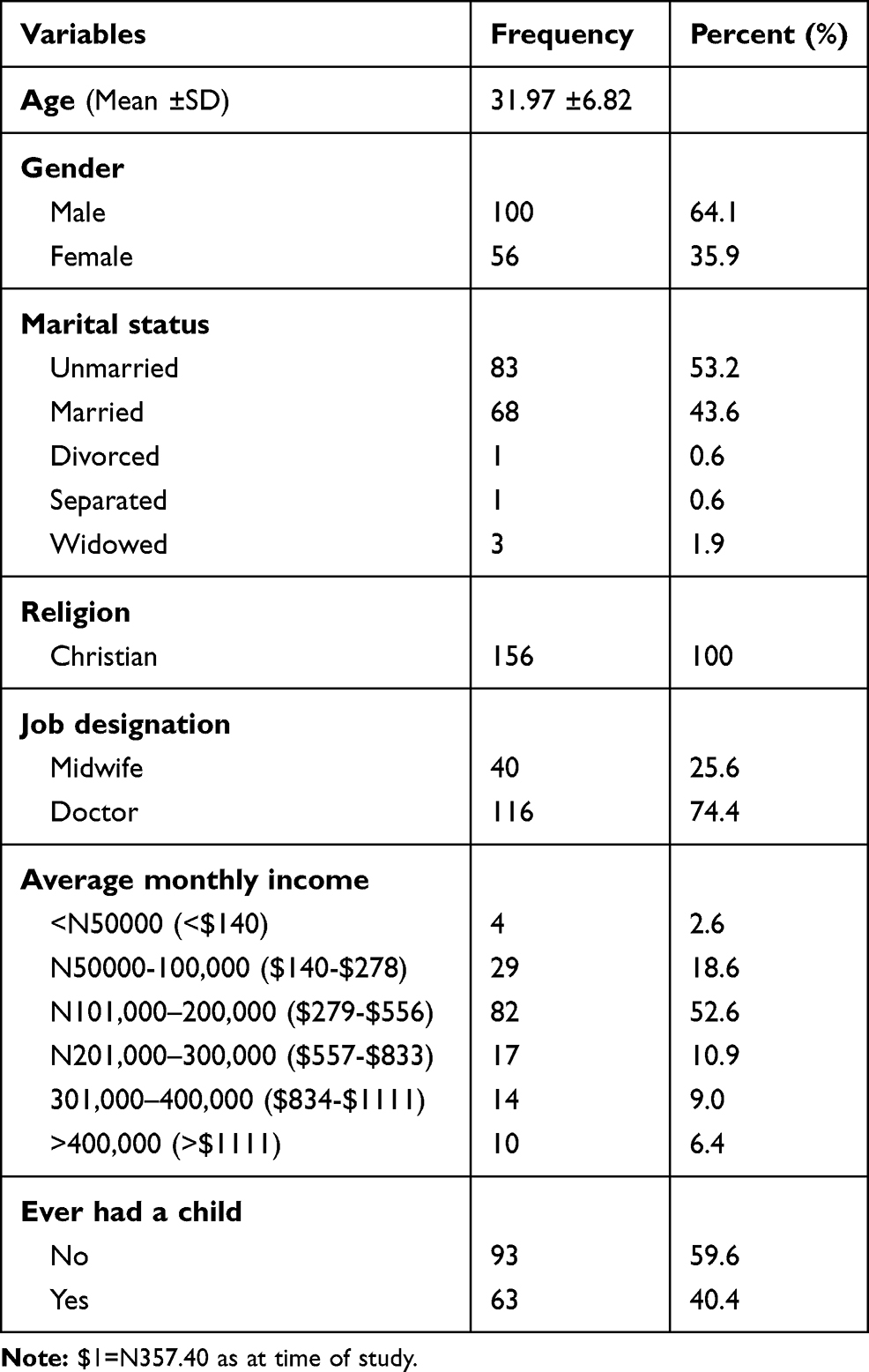 |
Table 1 Socio-Demographic Characteristics of the Respondents in the Quantitative Survey (n=156) |
The mothers involved in the FGD were aged 20–39 years and were all married. For the FGDs, all the midwives and 4 doctors were females while the rest of the doctors were males. The midwives were aged 30–52 years while the doctors were aged 31–46 years old. The key informants were 2 females (aged 43–54 years) and 3 males aged 35–40 years old.
Quantitative Results
At the maternal level, non-cooperation during childbirth (80.1%), not coming with birthing items (41.7%) and poor ANC attendance (41.0%) were the most cited drivers of D&A during childbirth. Major provider-associated drivers of D&A during childbirth were work overload (51.3%), personality type (44.2%) and, poor RMC training (42.9%). Poor design of Labor wards for privacy (54.5%), inadequate work equipment (46.8%) and facility type (39.1%) were the major facility drivers (Table 2).
 |
Table 2 Drivers of Disrespectful Maternity Care at Patient, Provider, Facility, Health Systems and Community Levels |
At the health system level, lack of focused training for health workers (55.1%) and lack of policies/enforcement (50.0%) were identified as drivers of disrespectful maternity care. The community-level drivers were poor awareness of fundamental rights and redress mechanisms (45.5%), lack of autonomy and empowerment of women (42.3%), and normalization of D&A during childbirth (40.4%) (Table 2). Generally, poor provider training, normalization, absence of policies and enforcement, lack of redress mechanisms, and low awareness of rights recurred across patient, provider, facility, policy, and community levels (Table 2).
Training/Retraining for providers (75.6%), provision of good work equipment/environment (51.9%) and policies and policy enforcement (51.9%) were the major recommendations to curb D&A during childbirth offered by the respondents (Table 3).
 |
Table 3 Recommendations for Mitigating Disrespectful Maternity Care by the Respondents |
Qualitative Results
Drivers of Disrespectful Maternity Care at the Maternal Level
At the level of the pregnant mother, the factors identified were grouped as obstetric-related factors, behavioural factors, and socio-economic factors. These factors included: poor ANC attendance, uncooperativeness/lack of self-control, poverty, dishonesty with clinical history, poor personal hygiene, illiteracy, low pain threshold, non-provision of birthing materials, and lack of birth experience (Table 4).
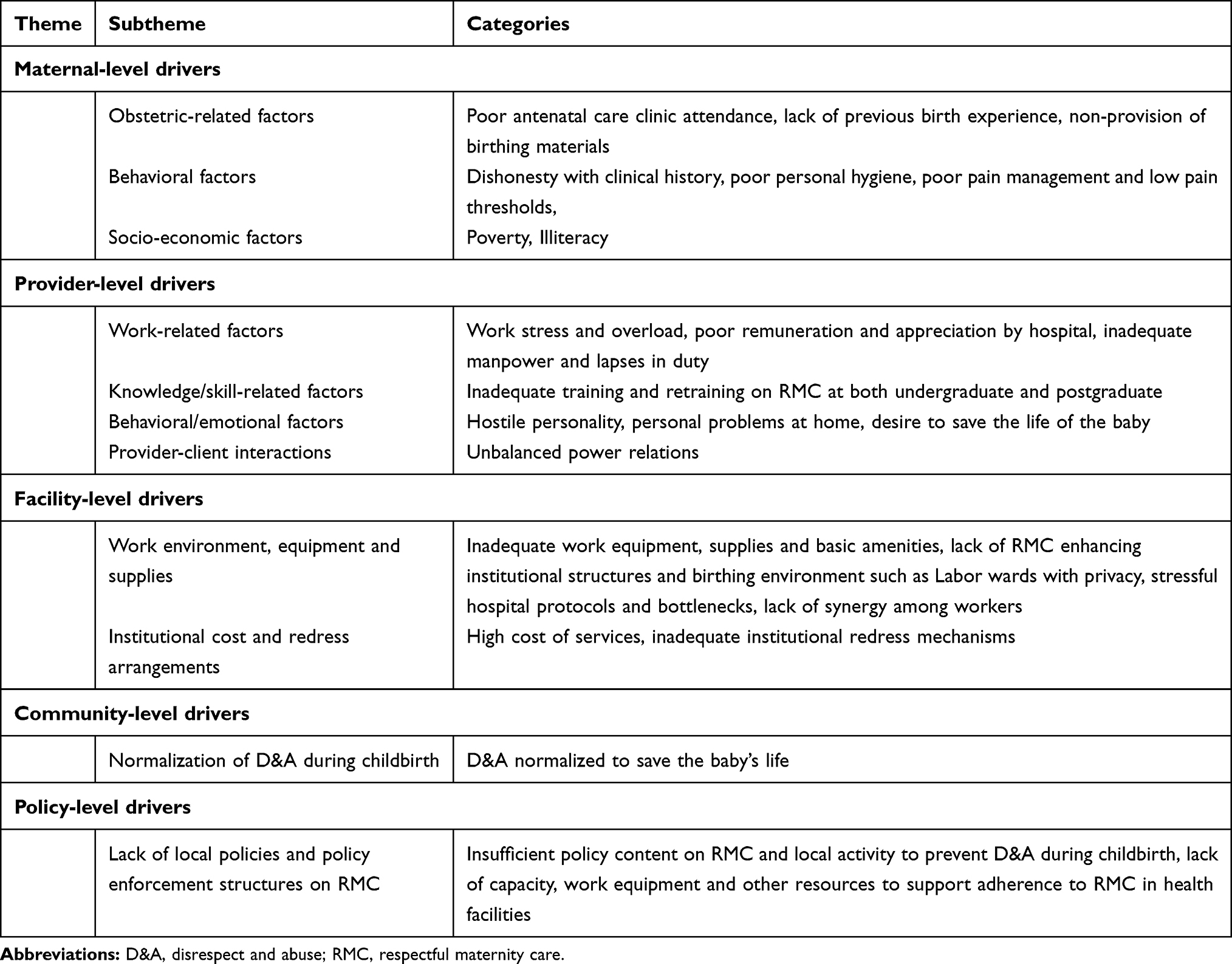 |
Table 4 Summary of Qualitative Findings on Drivers of Mistreatment During Childbirth |
Poor antenatal attendance was most cited because participants believed that it was an important preparatory to provide women with information that will enhance their cooperation and readiness during childbirth.
What causes disrespect against women during childbirth is when a woman does not go for antenatal until her delivery day. This is because I know that when a woman keeps the instructions of the doctors and nurses, she will not have problems with them. (Key Informant 1)
Most of the women don’t come for the antenatal clinic. In the antenatal clinic you will be taught something about child delivery and when they don’t know what was taught, the health worker can get angry. (Woman, FGD)
Midwives, doctors, and mothers identified non-provision of birthing materials as another driver of D&A during childbirth (especially verbal abuse) because it often frustrated the efforts of the providers in caring for the woman and her baby. This was deemed more infuriating for women who had attended ANC and received the list of birthing materials to be obtained ahead of time.
You give a woman a list of what she should procure before delivery, she comes with nothing. When I mean nothing, I mean without diapers and being a mother, you will have emotions that how will you expose this newborn? And you might tend to talk to the woman ‘’what’s wrong with you? You have been coming for antenatal care, what is the problem?. (Doctor, FGD)
“Most of them don’t come with delivery items or materials. This alone has given the nurses the opportunity to talk to them anyhow” (Woman, FGD).
Shyness and inexperience with childbirth were cited as a factor that encourages disrespectful maternity care.
“Most women don’t like opening their legs because they are shy especially the first-timers and this makes the health worker angry” (Woman, FGD).
Low pain thresholds and poor pain management especially due to non-acceptability and inability to afford epidural anesthesia were also identified because they increased the uncooperativeness of the patient and frustration of the maternal health provider thus leading to verbal, physical abuse, and even neglect during childbirth.
Some patients have a low pain threshold, no matter what you do, they will still be aggressive and feeling that you did not do much because of their low pain threshold. They will be shouting and remain irritable even you will give them the normal drug for pain. And when you come to reassure her, she will say the nurse is neglecting them. Also, maybe you might have other patients that are in Labor that you want to take care of but because of the low pain threshold, she needs your attention more. (Midwife, FGD)
“The traditional anesthesia cannot handle the pain the women face and we do not often use epidural anesthesia for every woman in Labor because some refuse it and cost concerns. This pain makes the women uncooperative and so annoys the health care worker making them beat and shout at the woman„. (Key Informant 2).
Drivers of Disrespectful Maternity Care at the Provider Level
At the level of the providers/health workers; lapses in duty, personal issues, work stress, and overload, lack of manpower, training gaps, desire to save baby’s life, power imbalances, poor remuneration, lack of resources and encouragement were highlighted. These were grouped as work-related factors, knowledge/skill-related factors, behavioural/emotional factors, and provider–client interactions (Table 4).
Inadequate training and retraining on RMC at both undergraduate and postgraduate levels were highlighted as a major driver of D&A during childbirth because of the lack of focus on respectful care in the traditional content of medical training. Additionally, providers lacked practical guidelines for implementing/contextualizing some RMC concepts.
I think we have training gaps for both nurses and doctors. For instance, the only thing we were taught in the management of a patient is that you should welcome a patient and provide psychological support in counseling the patient, after that’s all. Health workers need more updates and reorientation on these modern concepts. This RMC, if not for residency, many doctors won’t have heard about it and I am sure many nurses are not even aware. (Key Informant 3)
We need special training; for instance, the ideal RMC teaches that a woman has the right to adopt any position she wants and most of us don’t do it here. I think we need training on that. (Doctor FGD)
Both midwives and doctors affirmed that they were less motivated to treat clients respectfully because of insufficient salary payments. Additionally, they opined that their work efforts were often unappreciated by the hospital management thus further acting as de-motivation.
When you are not paid your salary for some time, you will not be happy working without a salary, and you can transfer your annoyance to the women in Labor. The hospital management never appreciates our efforts but is quick to punish us when anything goes wrong or patients complain. We are doing extra work; our patients are peculiar. We offer primary, secondary, and tertiary care and generate revenue for the hospital, yet we get no encouragement. This can make you unconsciously treat a patient poorly. (Doctor, FGD)
The hostile personality of some health providers and personal emotional issues were found to influence the occurrence of D&A often leading to transferred aggression during childbirth.
Some health workers are naturally easily provoked and hard to please. Sometimes, they carry their personal life problems to the workplace and maltreat the patients. (Midwife, FGD)
“Allowing your home emotional or psychological problems affect your work can make a health worker transfer all the aggression to the patient” (Key Informant 4).
Work overload and stress from work were highlighted as a prominent driver of disrespectful maternity care. Both midwives and users (Husbands) agreed that stress from long work hours without rest and an inadequate number of staff could result in aggression and inadvertent maltreatment of women during childbirth.
“Work overload can make somebody become aggressive because sometimes when you are doing night duty you stand up throughout the night” (Midwife, FGD).
“Stress is one thing that makes health workers disrespect women in Labor. They should have two doctors on the ground, not just one as I encountered.” (Key Informant-Husband).
At times we don’t have enough hands because there are so many women to attend to and as human beings, it will get to a stage where while you attend to different people, they call you to the next one and you will then react as a human being by mistreating the patient. (Midwife, FGD)
Health providers cited the desire to ensure a good obstetric outcome as a reason for maltreating women during childbirth opining that the women’s rights can be infringed when the baby’s life is at risk.
At times the right of the patient might be so harmful to the fetus so necessitating an in quote ‘disrespectful care’ in order to save the baby. In one of my experiences while in clinical practice, a woman in Labor gave me the permission to tie her up …. (Key Informant 3)
One of the key informants revealed that the traditional power imbalance in the client–provider relationship could also contribute to disrespectful maternity care.
“Some health care workers see themselves as God and treat patients anyhow. Because we are above the patients, we treat them as nothing” (Key Informant 2).
Drivers of Disrespectful Maternity Care at the Facility Level
The drivers of disrespectful maternity care at the facility level had the following subthemes: work environment, equipment and supplies, institutional cost, and redress arrangements. These included stressful hospital protocols, lack of synergy among workers, poor power supply, unfriendly birthing environments, and lack of equipment (Table 4).
This was the most reported driver of D&A during childbirth among both discussants and interviewees. Issues such as non-availability of medical supplies such as blood and poor lighting were severally mentioned.
Due to the frustration of the job, maybe the woman is bleeding and your junior colleague will now come and tell you that the lab people said there is no blood or something. So, you will now be angry or try to vent your frustration unfortunately on the woman. (Doctor, FGD)
Let me say that light issue is a very dangerous thing that is happening to us in this institution. Suturing an episiotomy with a rechargeable lantern or even with phone torch is very bad and frustrating
„Sometimes the women are uncomfortable when you use your phone torch thinking you are taking pictures of their private parts” (Doctor, FGD).
It is terrible when it comes to light at night; at a point when we got to the Labor ward, the light was off for a long time and the workers have to use phone torches. (Key Informant-Husband)
Unavailability of enabling structures for practicing RMC such as Labor wards that promote privacy and companionship and tranquility was highlighted. This made implementation difficult even after being trained.
There are setbacks because the hospital should provide these amenities. like there should be a water bed in the Labor so that when the woman comes, you will still be saying respective maternity care (general laughter) because sometimes we go for training but it isn’t possible to put it into practice. (Doctor, FGD)
“In the general ward, women who have delivered battle with rats and mosquitoes and this is a disrespect to them” (Key Informant-Husband).
We need more space because when space is there then privacy can be maintained and even companionship will be enforceable as the ideal. This is because with what we have here we cannot really practice. RMC well. (Key Informant 5)
Hospital bureaucracy, stressful hospital protocols, and lack of synergy among health workers were another factor challenging respectful and non-abusive care of women during childbirth. This often resulted in angry/irritated client relatives and easily provoked health providers thereby perpetrating D&A during childbirth.
Bottleneck bureaucracy and lack of synergy among health workers can also contribute. As a doctor, you may need something to handle an emergency urgently such as theatre clothes but the porters will be forming a big man saying he wants to maybe go and eat first. Sometimes they delay when their change of shift time is near. This way the patient is not treated respectfully. (Doctor, FGD)
Most times when a woman comes in Labor, we health workers will say, go and do PCV, go, and do analysis. Sometimes the patient and patient’s relative feel frustrated and when they come and you say ‘Oga you don’t have this or that thing’, they will start to react. At that particular time, they are going through stress, anything you say they will see it as disrespect. (Midwife, FGD)
The costliness of childbirth services was adduced to increase the likelihood of detention in the health facility following childbirth due to the inability to pay.
With the level of poverty in our environment, there is no reason why maternity care should not be free. The cost of delivery here is about N30, 000-40,000 for vaginal delivery and N80, 000-120,000 for CS. Non-implementation of free maternal care leads to detention due to the inability to pay bills. (Key Informant 2)
One of the key informants indicated that the lack of facility-level redress mechanisms designed to discourage the perpetration of D&A during childbirth contributed to its occurrence.
Except at the department level, there is no mechanism in place for redress. Although there is the service commission, when you go there, they don’t do anything. Like my own sister, when she had her baby here, the lady at the lab insulted her and she was crying. We went to the service commission and they told us to write and we wrote. Till today, nothing!. (Doctor, FGD)
Drivers of Disrespectful Maternity Care at the Community Level
Being mistreated during childbirth typically physical abuse was considered normal if it enables the health worker to facilitate childbirth since the woman is in so much pain (Table 4).
“Labor is not the same for everybody: Some endure their pain while some shout too much so it’s normal for nurses to tie the woman so as to help her give birth” (Key Informant 1).
Drivers of Disrespectful Maternity Care at the Policy Level
The major policy level drivers of DACF were lack of local policies and policy enforcement structures on RMC. The categories include lack of policies highlighting RMC and, poor ownership of local actors with respect to preventing D&A during childbirth (Table 4).
“I have not really seen national or sub-national policies highlighting RMC beyond some programs supported by development partners in the State” (Key Informant 3).
At the ministry level, our challenges include inadequate health manpower, lack of equipment to work or supplies i.e. drugs, lack of capacity training, and lack of good vehicles so that we can move around for supportive supervision towards RMC. (Key Informant 3)
Recommendations to Promote the Implementation of RMC
Recommendations were given by the respondents focusing on the client/community, provider, facility, and policy levels.
Creation of awareness on expected behaviors, possible experiences, and their rights during childbirth using antenatal clinics and social groups such as churches were recommended by the respondents. The statements below highlight some of these:
We have to tell the women the hospital policy, what is expected of them (such as hospital admission deposit), what they will see in the hospital during ANC and childbirth so that if they come to the hospital, they will not be embarrassed. (Midwife, FGD)
“The populace also needs to be enlightened on what their rights are.” (Key Informant 2)
The mothers should be taught how to deliver their baby, how to complain when they have challenges. Churches can be used as a platform to encourage women that health facilities to disabuse their minds that health care workers will inflict disrespect and abuse and tell them to report such incidences. (Key Informant 5)
Additionally, the care by clinically experienced health workers, regular RMC training and supervision, and proper remuneration were advocated. Some verbatim responses are stated thus:
“There is a need for regular training of health providers (on RMC) so that we de-emphasize our paternalistic way of treating our patients” (Key Informant 2).
Participants also suggested the use of personnel with adequate clinical skills to attend to patients rather than those with limited experience such as medical students.
“They should try and put experienced doctors in the Labor room and not student doctors” (Woman, FGD)
Proper remuneration was highlighted as a possible solution to mitigating D&A because of its motivational effect on their attitude to work.
“Health workers need to be appreciated, paid well and not owed so they can do their work with joy” (Key Informant 1).
Some other recommendations proffered were the provision of equipment/human resources, conducive working and birthing environment such as privacy in Labor rooms, customer care services, and redress mechanisms in health facilities.
Those equipment and materials we work with, the health workers salary and incentives should be provided so that they will be happy and motivated to work. More workers should be employed to avoid stress from overwork. (Midwife, FGD)
Participants equally recommended the improvement of the labor rooms and wards to promote privacy and engender relaxation by the women and their birth companions.
For the Labor room, I think that it should be properly upgraded (like fans, air conditioners, nets, etc.) because it is where women’s bodies is exposed to the environment. As I was taking care of my wife, I was killing mosquitoes and the place was cold at night. (Key informant-husband)
“We need to improve the privacy of our Labor wards so that we can allow women to stay with their birth companions during Labor” (Midwife, FGD).
One of the key informants recommended that hospitals should have customer service points as seen in other corporate organizations so that they can play a role in improving the cordiality accorded to clients who visit the hospital.
Hospital should employ people that will be working to organize things and make people feel at home when they come to the hospital. They should be teaching people that are sick some medical tips. (Key informant-husband)
Institutionalized mechanisms for incentivization for providers and redress for women who experienced disrespect and abuse during childbirth were also recommended.
“There should be an appropriate mechanism for complaints, investigation and punitive measures in place” (Key Informant 2).
Additionally, subsidized or free access to maternal health services was suggested because it could encourage utilization of antenatal care services, better pain management, and discourage detention in the facility following childbirth.
The government should provide free access to maternal health services as it will enable women to attend ANC where they will receive counseling, reduce pain in Labor by covering the cost of epidural analgesia and even eliminate detention in the facility because of inability to pay hospital bills. (Key Informant 2)
Discussion
This study has explored contextual drivers of disrespect and abuse during childbirth in health facilities in Southeast Nigeria. Additionally, recommendations proffered by the study participants were also highlighted in this paper. One major takeaway from this study is that various factors interact and inter-loop at different health system actor levels to cause mistreatment during childbirth thus a holistic concerted whole-of-system approach is important in tackling this scourge.3
At the maternal level, both qualitative and quantitative evidence highlighted maternal, socioeconomic characteristics, behavioral patterns, and practices that predisposed mothers to be disrespected during childbirth. Pregnant mothers who had suboptimal ANC attendance were uncooperative, or failed to provide the requisite materials for childbirth were considered most vulnerable to being abused during childbirth among other maternal factors. Antenatal care plays a vital role in preventing disrespect and abuse during labor and childbirth because it serves as an avenue for early diagnosis and education/preparation of the pregnant woman in order to enhance maximal cooperation during labor and childbirth.45,46 In both the FGDs and KIIs, the importance of ANC for birth preparedness and prevention of provider “vexation” through education of the pregnant mother was also highlighted. In agreement with the findings from this study, women who have never accessed ANC services have been found to avoid facility-based birth due to fear of being mistreated during childbirth.6 Failure to cooperate with or adhere to instructions given during childbirth or antenatal care (such as the provision of required items) could lead to frustration and provocation of the health provider unto deviation from the ideal compassionate and polite treatment of parturients to maltreatments such as verbal, physical abuse, neglect or any other form of D&A during childbirth.21,32,47–51
Community-level drivers of D&A during childbirth in this study were the normalization of disrespectful care, poor awareness of fundamental rights and redress mechanisms, lack of autonomy and empowerment of women.40 Normalization of mistreatment during childbirth in a bid to assist childbirth was the most-mentioned driver from the qualitative arm of the study and also recurred in the questionnaire-based survey. It contributes significantly to poor recognition, reporting, and demand for the right to be respected by women. Similarly, these factors have been found to perpetuate D&A during childbirth in other studies.16,18,52,53 These findings highlight the importance of addressing the wider socio-cultural and socio-economic influences on the status of women such as awareness of rights, education, financial independence, autonomy and decision-making power as these also affect their birthing and motherhood experiences.
The main provider-related drivers of disrespectful maternity care were work overload/fatigue due to unavailability of needed resources including financial motivation, inadequate conceptual and implementation training on RMC, normalization of D&A to ensure a healthy baby, and aggressive personality types. While personality type was the most cited driver from the questionnaire survey, work fatigue received more emphasis from the FGDs and KIIs. This is because caring for women in labor is characteristically stressful with the health provider under pressure to avoid being blamed for poor obstetric outcomes.54
Gaps in the medical training curricula at both undergraduate and postgraduate levels have been identified to encompass the absence of focused training on interpersonal communication and respectful care of clients (including RMC), and the inculcation of wrong mindsets. These mindsets are characterized by superiority, social distancing, class prejudice, over-medicalization and normalization of disrespectful care.31,39,42,55 Thus this finding represents an urgent call to begin to get things right in maternal health provider training by re-evaluating and revising the training curricula at all levels in line with best practices for promoting quality, person-centered rights-based care.21,54–57 Other possible underlying mechanisms of these provider-level factors leading to mistreatment during childbirth include lack of job satisfaction (de-motivation), perceived under-appreciation, and frustration all of which end up in transferred aggression.32,47,49,58
Health facility drivers of D&A during childbirth include inadequate work equipment, structures, and amenities, high cost of birthing services, and poor institutionalized redress mechanisms. These facility conditions did not foster an enabling environment for practicing RMC by health providers while the high cost of services deterred access to antenatal care and effective pain management (thus increasing the non-cooperation of parturient) and increased the likelihood of detention after childbirth due to inability to settle hospital bills. These represent the structural dimensions of disrespect and abuse in which health facilities offer unacceptable standards of care reflected in infrastructure, staff, equipment, and supplies needed for health service delivery.41 The lack of facility-level institutionalized mechanisms and processes that promote accountability has been found to significantly contribute to the normalization of D&A in such settings.42,59 It is important to note from the FGDs that the providers expressed that poor work environment and equipment strongly impeded respectful maternity care regardless of adequate provider knowledge and willingness to practice RMC. The policy drivers discovered in this study were the high cost of maternal health care, lack of local RMC policies, and policy enforcement challenges such as inadequate resources and capacities for supportive supervision. Globally, these policy factors have also been found to hamper progress in eliminating disrespectful maternity care.31,39–41
Although the study participants proffered some recommendations to promote respectful maternity care spanning the different levels of health system actors involved, we propose a more robust and systematic approach in addressing identified challenges. The community and woman-centered recommendations were awareness creation and patient education on rights and requirements for a successful birthing experience. Regular training and supervision of health providers on RMC were the most outstanding provider-level recommendation while the provision of good work supplies, enabling work environment for RMC, proper remuneration, and accountability mechanisms were the recommendations at the facility level. Policy recommendations were focused on the provision of free/subsidized maternal health care and enforcement of enacted policies. These recommendations are in consonance with that made in other studies.54,55,60–63
This study has some limitations. It was confined to two facilities in Ebonyi State therefore the findings cannot be generalized to all the facilities in the State or nation. The relatively small sample size is also another limitation of this study. The use of a mixed-methods approach involving different stakeholders to provide contextual evidence on drivers of disrespectful maternity care is a strength of this study.
Conclusions
A variety of multi-level drivers of disrespectful maternity care were identified. A diverse and inclusive multi-stakeholder approach should underline efforts to mitigate disrespectful maternity care and promote respectful, equitable, and quality maternal health care. We recommend the provision of free/subsidized maternal health services, rights-based community education, continuous health systems strengthening, regular training and supervision for health providers on interpersonal and client-friendly care, the institutionalization of accountability mechanisms and intersectoral collaboration (health, education, finance, gender, labor, and employment) to improve the status of women.
Abbreviations
D&A, Disrespect and Abuse; DACF, Disrespect and Abuse during Childbirth in Health Facilities; FGD, Focus Group Discussion; KII, Key Informant Interview; RMC, Respectful Maternity Care; SPSS, Statistical Package for Social Sciences.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the primary author on reasonable request ([email protected]).
Ethical Statement
This study was conducted in accordance with the Declaration of Helsinki and after ethical clearance for this study was obtained from Research and Ethics Committee of Alex-Ekwueme Federal University Teaching Hospital Abakaliki, Ebonyi State, Nigeria (approval number 06/10/2017-23/20/2017). The participants gave written informed consent before the study commenced. Voluntary participation, confidentiality and anonymity of responses were ensured. To protect the anonymity of the key informants, quotes attributed to the key informants in designated positions (except the husbands) were denoted by self-assigned identification numbers (Key informant 1–5) and not by official designation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest for this work.
References
1. White Ribbon Alliance. Respectful maternity care: the universal rights of childbearing women [Internet]; 2010 [
2. Reis V, Deller B, Carr C, Smith J. Respectful Maternity Care Country Experiences. New York; 2012.
3. Miller S, Lalonde A. The global epidemic of abuse and disrespect during childbirth: history, evidence, interventions, and FIGO ’ s mother − baby friendly birthing facilities initiative. Int J Gynecol Obstet. 2015;131:S49–52. doi:10.1016/j.ijgo.2015.02.005
4. Mselle LT, Moland KM, Mvungi A, Evjen-olsen B, Kohi TW. Why give birth in health facility? Users’ and providers’ accounts of poor quality of birth care in Tanzania. BMC Health Serv Res. 2013;13(1):174. doi:10.1186/1472-6963-13-174
5. Roro MA, Hassen EM, Lemma AM, Gebreyesus SH, Afework MF. Why do women not deliver in health facilities: a qualitative study of the community perspectives in south central Ethiopia? BMC Res Notes. 2014;7(556):1–7. doi:10.1186/1756-0500-7-556
6. Bohren MA, Hunter EC, Munthe-kaas HM, Souza JP, Vogel JP, Gülmezoglu AM. Facilitators and barriers to facility-based delivery in low- and middle-income countries: a qualitative evidence synthesis. Reprod Health. 2014;11(71):1–17. doi:10.1186/1742-4755-11-71
7. Sychareun V, Hansana V, Somphet V, Xayavong S, Phengsavanh A, Popenoe R. Reasons rural laotians choose home deliveries over delivery at health facilities: a qualitative study. BMC Pregnancy Childbirth. 2012;12(1):1.
8. Wilunda C, Scanagatta C, Putoto G, et al. Barriers to institutional childbirth in rumbek north county, South Sudan: a qualitative study. PLoS One. 2016;11(12):e0168083. doi:10.1371/journal.pone.0168083
9. Moyer CA, Mustafa A. Drivers and deterrents of facility delivery in sub-Saharan Africa: a systematic review. Reprod Health. 2013;10(1):40. doi:10.1186/1742-4755-10-40
10. Moyer CA, Dako-Gyeke P, Adanu RM. Facility-based delivery and maternal and early neonatal mortality in sub-Saharan Africa: a regional review of the literature. Afr J Reprod Health. 2013;17(3):30–43.
11. World Health Organization. Maternal mortality [Internet]. Factsheets; 2018 [
12. Girum T, Wasie A. Correlates of maternal mortality in developing countries: an ecological study in 82 countries. Matern Health Neonatol Perinatol. 2017;3(1):19. doi:10.1186/s40748-017-0059-8
13. Federation of Gynecol I, International Federation of Gynecology and Obstetrics International Confederation of Midwives, White Ribbon Alliance, International Pediatric Association, World Health Organization. Mother-baby friendly birthing facilities initiative. Int J Gynecol Obstet. 2015;128(2):95–99. doi:10.1016/j.ijgo.2014.10.013
14. Tunçalp Ӧ, Were W, MacLennan C, et al. Quality of care for pregnant women and newborns-the WHO vision. BJOG. 2015;122(8):1045–1049. doi:10.1111/1471-0528.13451
15. World Health Organization. The prevention and elimination of disrespect and abuse during facility-based childbirth: WHOstatement [Internet]. Geneva, Switzerland; 2014 [
16. Ishola F, Owolabi O, Filippi V. Disrespect and abuse of women during childbirth in Nigeria: a systematic review. PLoS One. 2017;12(3):e0174084. doi:10.1371/journal.pone.0174084
17. Okedo-Alex IN, Akamike IC, Okafor LC. Does it happen and why? Lived and shared experiences of mistreatment and respectful care during childbirth among maternal health providers in a tertiary hospital in Nigeria. Women Birth. 2020;in press.
18. Orpin J, Puthussery S, Davidson R, Burden B. Women’s experiences of disrespect and abuse in maternity care facilities in Benue State, Nigeria. BMC Pregnancy Childbirth. 2018;18(1):1–9.
19. Bohren MA, Vogel JP, Tunçalp Ö, et al. By slapping their laps, the patient will know that you truly care for her: a qualitative study on social norms and acceptability of the mistreatment of women during childbirth in Abuja, Nigeria. SSM Popul Health. 2016;2:640–655. doi:10.1016/j.ssmph.2016.07.003
20. Bohren MA, Vogel JP, Tunçalp Ö, et al. Mistreatment of women during childbirth in Abuja, Nigeria: a qualitative study on perceptions and experiences of women and healthcare providers. Reprod Health. 2017;14(9):1–13. doi:10.1186/s12978-016-0265-2
21. Balde MD, Bangoura A, Diallo BA, et al. A qualitative study of women ’ s and health providers ’ attitudes and acceptability of mistreatment during childbirth in health facilities in Guinea. Reprod Health. 2017;14(4):1–13.
22. Freedman LP, Ramsey K, Abuya T, et al. Defining disrespect and abuse of women in childbirth: a research, policy and rights agenda. Bull World Health Organ. 2014;92(12):915–917. doi:10.2471/BLT.14.137869
23. Sando D, Abuya T, Asefa A, et al. Methods used in prevalence studies of disrespect and abuse during facility based childbirth: lessons learned. Reprod Health. 2017;14(1):127. doi:10.1186/s12978-017-0389-z
24. World Health Organization. Maternal mortality fact sheet [Internet]. Geneva; 2015 [
25. Abuya T, Ndwiga C, Ritter J, et al. The effect of a multi-component intervention on disrespect and abuse during childbirth in Kenya. BMC Pregnancy Childbirth. 2015;15(1):224. doi:10.1186/s12884-015-0645-6
26. Azhar Z, Oyebode O, Masud H. Disrespect and abuse during childbirth in district Gujrat, Pakistan: a quest for respectful maternity care. Ann Glob Health. 2017;83(1):108. doi:10.1016/j.aogh.2017.03.240
27. Abuya T, Warren CE, Miller N, et al. Exploring the prevalence of disrespect and abuse during childbirth in Kenya. PLoS One. 2015;10(4):1–13. doi:10.1371/journal.pone.0123606
28. Raj A, Dey A, Boyce S, et al. Associations between mistreatment by a provider during childbirth and maternal health complications in Uttar Pradesh, India. Matern Child Health J. 2017;21(9):1821–1833. doi:10.1007/s10995-017-2298-8
29. Sudhinaraset M, Treleaven E, Melo J, Singh K, Diamond-smith N. Women's status and experiences of mistreatment during childbirth in Uttar Pradesh: a mixed methods study using cultural health capital theory. BMC Pregnancy Childbirth. 2016;26(1):332. doi:10.1186/s12884-016-1124-4
30. Sethi R, Gupta S, Oseni L, Mtimuni A, Rashidi T, Kachale F. The prevalence of disrespect and abuse during facility-based maternity care in Malawi: evidence from direct observations of labor and delivery. Reprod Health. 2017;14(1):111. doi:10.1186/s12978-017-0370-x
31. Bohren MA, Vogel JP, Hunter EC, et al. The mistreatment of women during childbirth in health facilities globally: a mixed-methods systematic review. PLoS Med. 2015;12(6):1–32. doi:10.1371/journal.pmed.1001847
32. Warren CE, Njue R, Ndwiga C, Abuya T. Manifestations and drivers of mistreatment of women during childbirth in Kenya: implications for measurement and developing interventions. BMC Pregnancy Childbirth. 2017;17(102):1–14.
33. Federal Ministry of Health. National Health Policy 2016. Abuja; 2016.
34. Federal ministry of health. National Reproductive Health Policy. Abuja Nigeria; 2001.
35. Federal Ministry of Health. National Reproductive Health Strategic Framework 2002–2006. Abuja; 2002.
36. Ebonyi State Ministry of health. Ebonyi State Government Strategic Health Development Plan. Abakaliki; 2010.
37. National Population Commission (NPC) [Nigeria] and ICF Macro. Nigeria Demographic and Health Survey 2013. Abuja; 2013.
38. Savage V, Castro A. Measuring mistreatment of women during childbirth: a review of terminology and methodological approaches. Reprod Health. 2017;14(1):138. doi:10.1186/s12978-017-0403-5
39. Bowser D, Hill K. Exploring Evidence for Disrespect and Abuse in Facility-Based Childbirth: Report of a Landscape Analysis. New York; 2010.
40. Ratcliffe HL. Creating an Evidence Base for the Promotion of Respectful Maternity Care. Harvard School of Public Health; 2013.
41. Freedman L, Kruk M. Disrespect and abuse of women in childbirth: challenging the global quality and accountability agendas. Lancet. 2014;384(9948):e42–4. doi:10.1016/S0140-6736(14)60859-X
42. Bradley S, McCourt C, Rayment J, Parmar D. Disrespectful intrapartum care during facility-based delivery in sub-Saharan Africa: a qualitative systematic review and thematic synthesis of women’s perceptions and experiences. Soc Sci Med. 2016;169:157–170. doi:10.1016/j.socscimed.2016.09.039
43. Araoye MO. Research Methodology with Statistics for Health and Social Sciences.
44. Lwanga S, Lemeshow S. Sample Size Determination in Health Studies: A Practical Manual. Geneva; 1991.
45. Okedo-Alex IN, Akamike IC, Ezeanosike OB, Uneke CJ. Determinants of antenatal care utilisation in sub-Saharan Africa: a systematic review. BMJ Open. 2019;9(10):e031890. doi:10.1136/bmjopen-2019-031890
46. World Health Organization. WHO recommendations on antenatal care for a positive pregnancy experience [Internet]. Geneva; 2016 [
47. Balde MD, Diallo BA, Bangoura A, et al. Perceptions and experiences of the mistreatment of women during childbirth in health facilities in Guinea: a qualitative study with women and service providers. Reprod Health. 2017;14(3):1–13.
48. Rominski SD, Lori J, Nakua E, Dzomeku V, Moyer CA. When the baby remains there for a long time, it is going to die so you have to hit her small for the baby to come out: justification of disrespectful and abusive care during childbirth among midwifery students in Ghana. Health Policy Plan. 2017;32(2):215–224.
49. Burrowes S, Holcombe SJ, Jara D, Carter D, Smith K. Midwives’ and patients’ perspectives on disrespect and abuse during labor and delivery care in Ethiopia: a qualitative study. BMC Pregnancy Childbirth. 2017;17(1):263. doi:10.1186/s12884-017-1442-1
50. Rominski S. Ghanaian midwifery students’ perceptions and experiences of disrespect and abuse during childbirth. Lancet Glob Health. 2015;3:S13. doi:10.1016/S2214-109X(15)70132-4
51. Afulani PA, Kelly AM, Buback L, Asunka J, Kirumbi L, Lyndon A. Providers’ perceptions of disrespect and abuse during childbirth: a mixed-methods study in Kenya. Health Policy Plan. 2020;35(5):577–586. doi:10.1093/heapol/czaa009
52. Graner S, Mogren I, Duong LQ, Krantz G, Klingberg-allvin M. Maternal Health Care Professionals ’ perspectives on the provision and use of antenatal and delivery care: A qualitative descriptive study in rural Vietnam. 2010.
53. Kim J, Motsei M. Women enjoy punishment: attitudes and experiences of gender-based violence among PHC nurses in rural south Africa. Soc Sci Med. 2002;54(8):1243–1254. doi:10.1016/S0277-9536(01)00093-4
54. Holmes W, Goldstein M. Being treated like a human being: Attitudes and behaviours of reproductive and maternal health care providers Mother and baby in the marketplace in Lagos. 2012:1–87.
55. Moyer CA, Rominski S, Nakua EK, Dzomeku VM, Agyei-Baffour P, Lori JR. Exposure to disrespectful patient care during training: data from midwifery students at 15 midwifery schools in Ghana. Midwifery. 2016;41:39–44. doi:10.1016/j.midw.2016.07.009
56. Mannava P, Durrant K, Fisher J, Chersich M, Luchters S. Attitudes and behaviours of maternal health care providers in interactions with clients: a systematic review. Global Health. 2015;11(1):36. doi:10.1186/s12992-015-0117-9
57. Bohren MA, Mehrtash H, Fawole B, et al. How women are treated during facility-based childbirth in four countries: a cross-sectional study with labour observations and community-based surveys. Lancet. 2019;394(10210):1750–1763. doi:10.1016/S0140-6736(19)31992-0
58. Banchani E, Tenkorang EY. Implementation challenges of maternal health care in Ghana: the case of health care providers in the Tamale Metropolis. BMC Health Serv Res. 2014;14(1):7. doi:10.1186/1472-6963-14-7.
59. Warren CE, Ndwiga C, Sripad P, et al. Sowing the seeds of transformative practice to actualize women’s rights to respectful maternity care: reflections from Kenya using the consolidated framework for implementation research. BMC Women's Health. 2017;17(1):69. doi:10.1186/s12905-017-0425-8
60. Sadler M, Santos MJ, Ruiz-Berdún D, et al. Moving beyond disrespect and abuse: addressing the structural dimensions of obstetric violence. Reprod Health Matters. 2016;24(47):47–55. doi:10.1016/j.rhm.2016.04.002
61. Mesenburg MA, Victora CG, Serruya SJ, et al. Disrespect and abuse of women during the process of childbirth in the 2015 pelotas birth cohort. Reprod Health. 2018;15(1):54. doi:10.1186/s12978-018-0495-6
62. Mcmahon SA, George AS, Chebet JJ, Mosha IH, Mpembeni RNM, Winch PJ. Experiences of and responses to disrespectful maternity care and abuse during childbirth; a qualitative study with women and men in Morogoro Region, Tanzania. BMC Pregnancy Childbirth. 2014;14(268):1–13.
63. Downe S, Lawrie TA, Finlayson K, Oladapo OT. Effectiveness of respectful care policies for women using routine intrapartum services: a systematic review. Reprod Health. 2018;15(1):23. doi:10.1186/s12978-018-0466-y
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.