Back to Journals » International Medical Case Reports Journal » Volume 19
Multi-Route Administration Therapy for Intracranial Acinetobacter baumannii Infection After Postoperative Cerebral Hemorrhage: A Case Report
Authors Wu H ![]() , Gao W, Cheng Y, Yuan Z, Zhang L, Zhao H
, Gao W, Cheng Y, Yuan Z, Zhang L, Zhao H
Received 19 March 2026
Accepted for publication 10 June 2026
Published 16 June 2026 Volume 2026:19 609143
DOI https://doi.org/10.2147/IMCRJ.S609143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Hao Wu,* Wenwen Gao,* Yingying Cheng, Zhihai Yuan, Liang Zhang, Haikang Zhao
Department of Neurosurgery, The Second Affiliated Hospital of Xi’an Medical University, Xi’an, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haikang Zhao, Email [email protected] Hao Wu, Email [email protected]
Objective: To explore the early diagnosis and treatment plan of intracranial infection with Acinetobacter baumannii.
Methods: The clinical data of a patient with intracranial infection caused by Acinetobacter baumannii after intracranial hemorrhage surgery were analyzed. Combined with literature review, analyze the treatment plan for intracranial infection of Acinetobacter baumannii.
Results: During the hospitalization of this patient, cerebrospinal fluid culture and routine biochemical monitoring were combined with procalcitonin and C-reactive protein for auxiliary diagnosis. The antibiotic treatment regimen was intravenous injection of meropenem and vancomycin, combined with artificial cerebrospinal fluid replacement and lumbar cisterior drainage. After one week of treatment, the patient’s condition improved and the bacterial culture of cerebrospinal fluid was negative.
Conclusion: For intracranial infection caused by Acinetobacter baumannii, in this case, the patient was treated with meropenem + vancomycin via intravenous administration, combined with artificial cerebrospinal fluid replacement surgery + lumbar cistern drainage surgery. Although this treatment approach achieved relatively satisfactory therapeutic results, it is still a single-case empirical treatment. Due to the high rate of drug resistance and poor prognosis of intracranial Acinetobacter baumannii infection, there is currently no standardized unified treatment plan. More clinical studies are needed to accumulate data and further explore effective and with fewer adverse reactions treatment strategies to improve the clinical prognosis of such patients.
Keywords: Acinetobacter baumannii, intracranial infection, meropenem, vancomycin, lumbar cistern drainage, artificial cerebrospinal fluid replacement surgery
Introduction
Intracranial infection following neurosurgical craniotomy is a serious surgical complication, with a difficult treatment due to the existence of the blood-brain barrier which restricts the effective penetration of drugs into the cerebrospinal fluid, making it difficult to achieve an effective therapeutic concentration.1,2 At the same time, the pathogenic bacteria causing intracranial infection often exhibit resistance to multiple antibiotics, which further increases the complexity of treatment and makes it significantly different from infections in other parts. Acinetobacter baumannii, as a non-fermenting Gram-negative coccus, is widely distributed in water, soil, hospital environments, and human skin surfaces. In recent years, it has become one of the important opportunistic pathogenic bacteria causing nosocomial infections, presenting significant challenges to clinical treatment.3 Acinetobacter baumannii is not neurotropic by nature. Its intracranial infection is secondary, iatrogenic, and invasive, and rarely occurs spontaneously through hematogenous dissemination. All confirmed cases of intracranial infection are closely related to direct channels that breach the human anatomical barriers. Based on clinical evidence and the biological characteristics of the pathogen, the routes of intracranial infection can be systematically classified into the following four types: The first is the direct implantation route through medical devices (the most important and common), such as infections related to external ventricular drainage tubes (EVD) or lumbar cistern drainage tubes, infections from ventriculoperitoneal shunt (VP shunt), intracranial pressure monitoring probes, deep brain stimulation electrodes and other neurosurgical implants; The second is the direct inoculation route through open head trauma or neurosurgical surgery (high-risk, acute onset), such as open head injuries (such as depressed fractures, firearm wounds, scalp avulsion with skull defect), contamination during craniotomy; The third is the secondary hematogenous dissemination route (rare but highly fatal), which is common in critically ill patients with sepsis, especially those with ventilator-associated pneumonia (VAP), central venous catheter-related bloodstream infection (CLABSI), or abdominal infections in ICU patients; Acinetobacter baumannii breaches the vascular endothelium, enters the brain parenchyma or meninges through choroid plexus capillaries or damaged blood-brain barrier (such as disruption of tight junctions due to inflammation or hypoxia). This route often leads to concurrent meningitis and brain abscesses, and multiple ring-enhanced lesions can be seen on imaging; The presence of a clear extracranial infection focus and systemic intoxication symptoms (persistent high fever, shock, DIC, etc.) is required, and blood cultures are often positive. The fourth is the direct spread from adjacent structures (relatively rare, with anatomical specificity), such as sinusitis/mastoiditis → epidural/subdural abscess → meningitis, which is common in patients who are bedridden for a long time, immunosuppressed, or diabetic.4,5 The department of neurosurgery of the second affiliated hospital of Xi’an Medical University recently admitted a patient with intracranial infection caused by Acinetobacter baumannii after craniotomy for hemorrhage in the thalamus that entered the ventricular system. Through a multi-pathway combined medication treatment plan, good clinical results were achieved. This study systematically summarized and analyzed the diagnosis and treatment process of this patient and conducted discussions based on relevant literature. The results are presented below.
Clinical Data
Statement
All the data involved in this case report have been obtained with the consent of the patient’s relatives (patient’s son) and have been approved for publication.(the patient has authorized her son to handle all matters on her behalf, we have a delegate authorization letter signed by the patient and her son). Institutional approval to publish the case details was also obtained from the Ethics Committee of the Second Affiliated Hospital of Xi ’an Medical University.
General Information
The patient in this case is a 51-year-old female. She was admitted to our neurosurgery department at 07:40 on April 21, 2024 due to “aphasia and hemiplegia on the right side of the body for 1 hour”.
Present Illness History
The patient suddenly lost the ability to speak and experienced limb movement disorders on the right side when getting up in the morning 1 hour ago. After the onset, there was no convulsive episode or incontinence of urine or stool. Later, the family members discovered this and rushed him to our emergency center for treatment. A cranial CT examination was performed and it showed: left thalamus hemorrhage that had broken into the ventricular system (Figure 1). Subsequently, he was admitted to our neurosurgery department for emergency treatment.
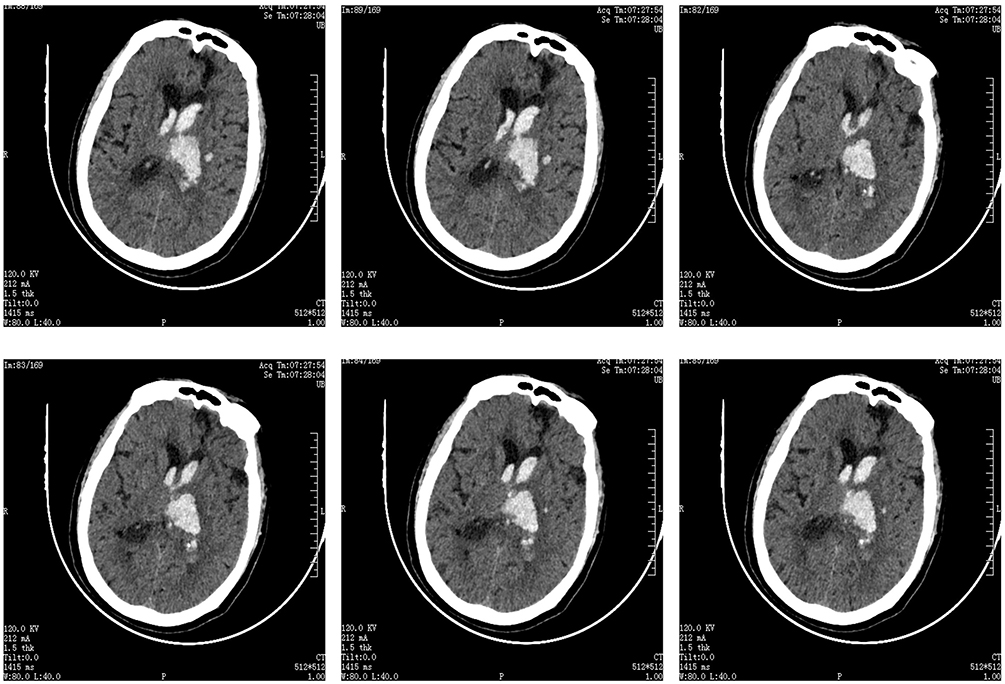 |
Figure 1 Preoperative Cranial CT Scan. |
Past Medical History
The patient was diagnosed with “hypertension” 10 years ago and has been regularly taking “Compound Reserpine” to control blood pressure; 2 years ago, the patient was diagnosed with “coronary heart disease” and was treated with oral medications, but the specific treatment details are unknown; 6 years ago, “Type 2 diabetes” was discovered, and the patient has been taking “Metformin Hydrochloride Extended-release Tablets” regularly to control blood sugar, but the specific efficacy is unknown.
Physical Examination
Temperature: 36.1°C, Pulse: 76 beats per minute, Respiration: 20 breaths per minute, Blood pressure: 174/103 mmHg.
Specialized Examination
Consciousness is in a drowsy state. When called, the eyes can be opened and simple questions can be answered. GCS score is 10 points, E3V3M4. Both pupils are equal in size and round, with a diameter of approximately 3.0 mm. The light reflex is sluggish. The muscle strength of the left limb is 3+ grade, with normal muscle tone. The muscle strength of the right limb is 1 grade, with relatively high muscle tone; Both Babinski signs are suspiciously positive.
Initial Diagnosis
1. Left thalamus hemorrhage; 2. Secondary ventricular hemorrhage; 3. Grade 3 hypertension (extremely high risk); 4. Type 2 diabetes; 5. Coronary heart disease.
Diagnosis and Treatment Process
After admission, comprehensive preoperative examinations and preparations were carried out actively. On the same day, under general anesthesia, a left lateral ventricle intracranial pressure probe implantation surgery + right lateral ventricle puncture and drainage surgery were performed. On the second day after the operation, a cranial CT scan was conducted (Figure 2), and after 7 days of drainage, the bilateral ventricular drainage tubes were removed on April 28, 2024 and a cranial CT scan was performed again (Figure 3); On April 29, 2024, a high fever occurred, and a high suspicion of intracranial infection was raised. On April 28, 2024, a lumbar puncture was performed and cerebrospinal fluid tests were conducted, indicating: color: red; coagulation: no; transparency: turbid; protein qualitative: (+); white blood cell count: 0.125×1012/L↑; glucose: 6.28mmol/L↑; protein: 98.71mmol/L↑; chloride: 117.21mmol/L↓; smear + drug sensitivity: (-). On April 29, 2024,a second lumbar puncture was performed and cerebrospinal fluid tests were conducted again, indicating: color: pale red; coagulation: no; transparency: slightly turbid; protein qualitative: (+); white blood cell count: 4.55×1012/L↑; glucose: 0.3mmol/L↓; protein: 543.54mmol/L↑; chloride: 101.50mmol/L↓; smear + drug sensitivity: (-). On May 1, 2024, a third lumbar puncture was performed and cerebrospinal fluid tests were conducted again, indicating: color: yellow; coagulation: no; transparency: turbid; protein qualitative: (+); white blood cell count: 21.3×1012/L↑; glucose: 0.3mmol/L↓; protein: 238.85mmol/L↑; chloride: 98.60mmol/L↓; smear + drug sensitivity: G+ cocci 2+: a small amount; white blood cells 3+: a moderate amount; drug sensitivity suggested: Acinetobacter baumanii. The patient presented with persistent high fever, and the treatment plan was adjusted to: meropenem + vancomycin + lumbar cistern drainage surgery. After the third lumbar puncture, the cerebrospinal fluid was milky in appearance and the drainage tube was blocked (Figure 4). Therefore, the drainage tube was removed and a new lumbar cistern drainage surgery was performed. At the same time, meropenem (2024 May 4th, 1g every 8 hours), vancomycin (2024 May 1st, 1000mg every 8 hours), lumbar cistern drainage surgery + cerebrospinal fluid replacement surgery (2024 May 1st–May 6th, continuous replacement for 6 days) were performed. From May 2nd to May 6th, 2024, the cerebrospinal fluid culture was positive for Acinetobacter baumanii. After active treatment, the patient’s body temperature gradually improved, and the cerebrospinal fluid culture was (-) on May 7th, 2024. The process of cerebrospinal fluid culture is shown in Figure 5.The cerebrospinal fluid color changes (Figure 6), laboratory test changes of cerebrospinal fluid glucose, protein, chloride, and white blood cells, as well as changes of calcium, calcitonin, and C-reactive protein (Figures 7–10); Changes in body temperature over time (Figure 11); Changes in white blood cell and neutrophil ratio in blood tests (Figures 12 and 13); Changes in calcitonin and C-reactive protein in blood tests (Figures 14 and 15). After active treatment, the patient’s consciousness response improved, vital signs were stable, body temperature was normal, and there were no obvious abnormalities in the test results. The intracranial condition was stable, and no obvious complications were observed.
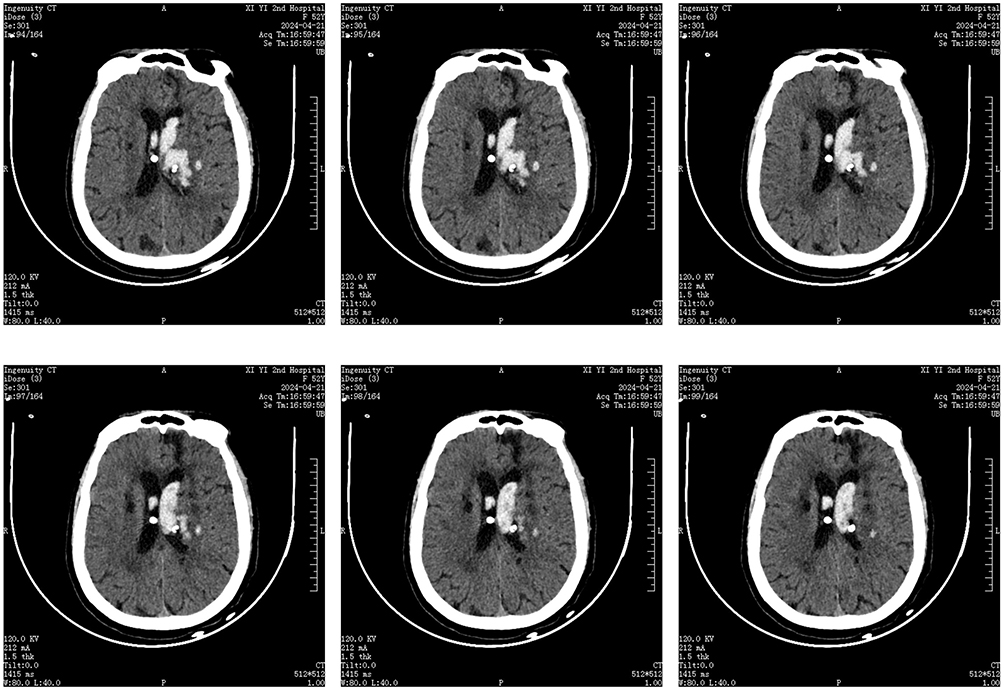 |
Figure 2 Postoperative review of cranial CT scan. |
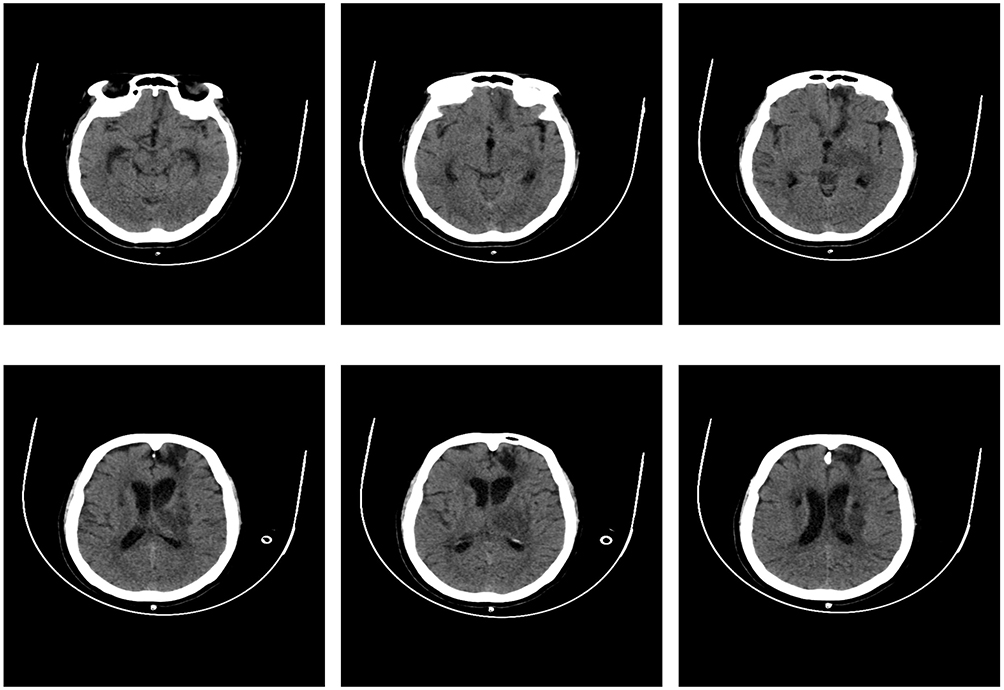 |
Figure 3 Re-examination of cranial CT after removal of the head drainage tube. |
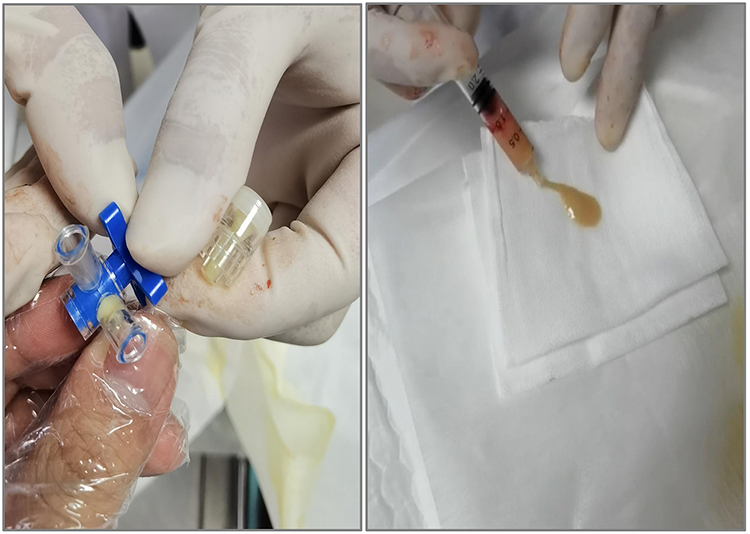 |
Figure 4 The cerebrospinal fluid appears like rice soup and has blocked the drainage tube. |
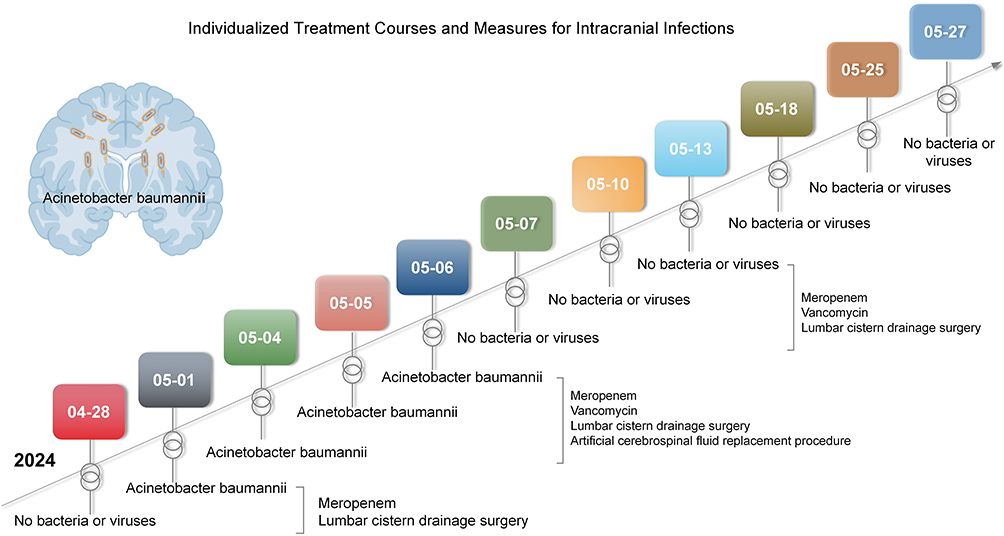 |
Figure 5 Cerebrospinal fluid culture and treatment measures. |
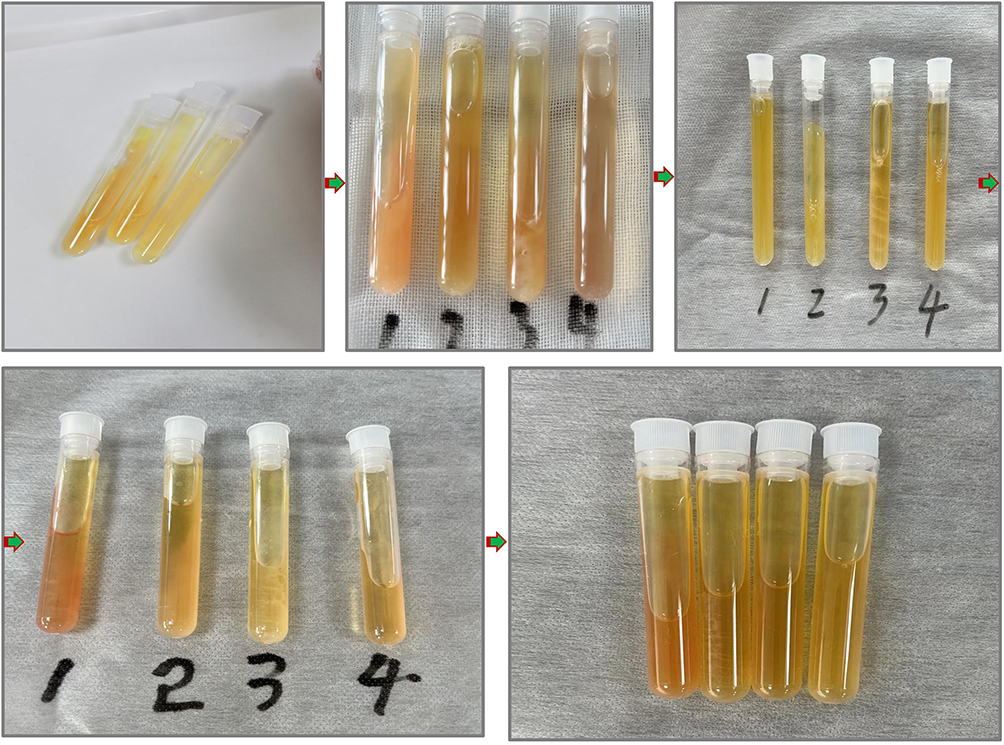 |
Figure 6 The process of cerebrospinal fluid morphological changes. |
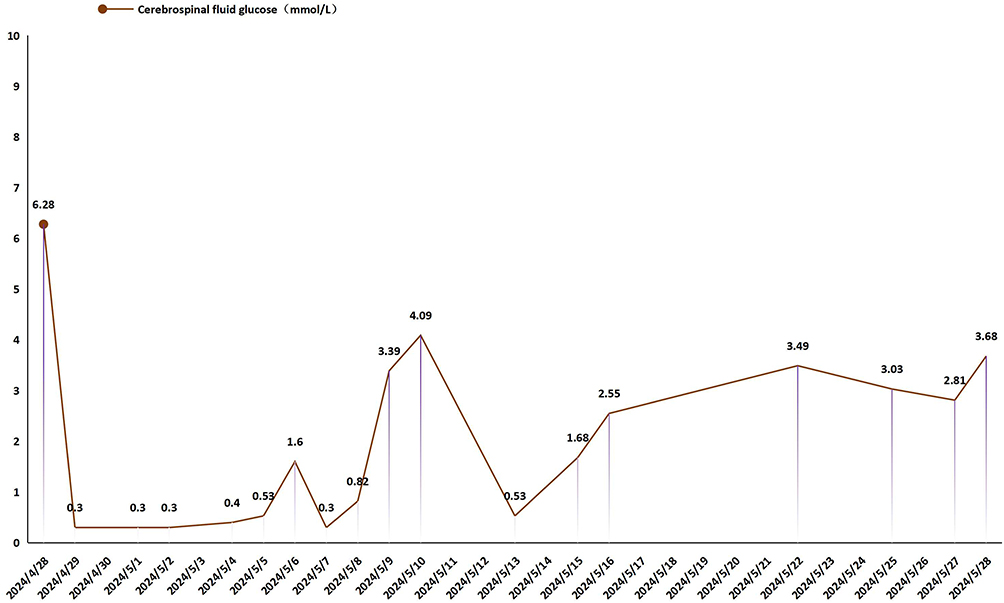 |
Figure 7 Curve of cerebrospinal fluid glucose variation. |
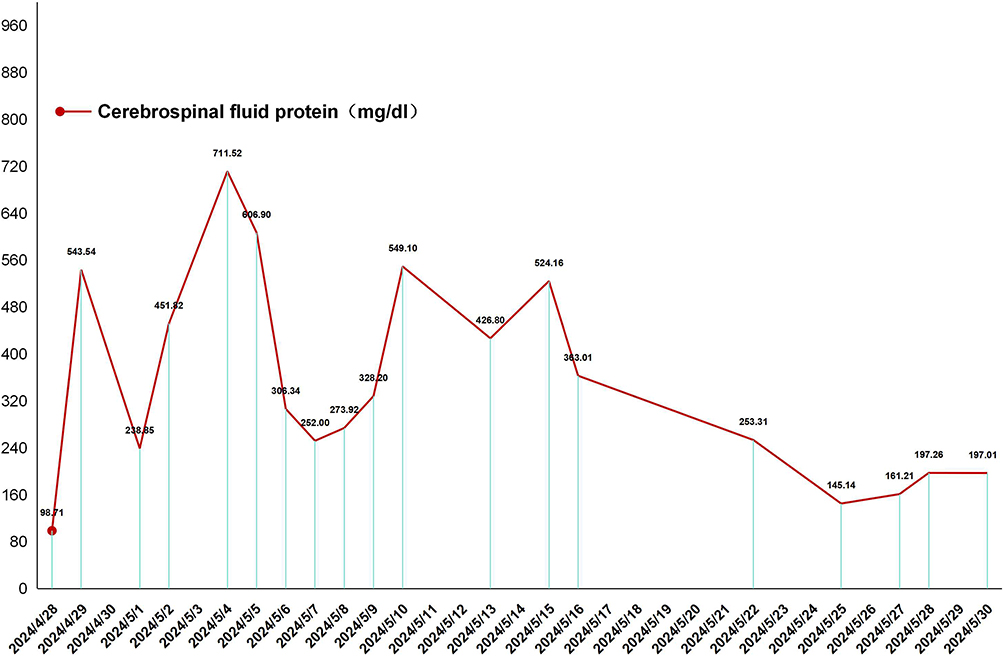 |
Figure 8 Curve of Cerebrospinal Fluid Protein Changes. |
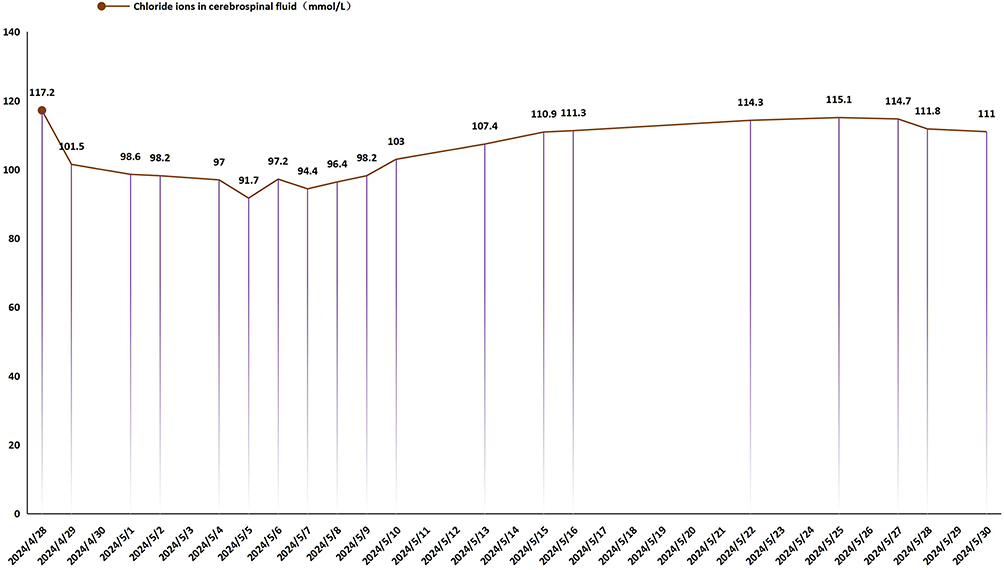 |
Figure 9 Curve of Chloride Ion Changes in Cerebrospinal Fluid. |
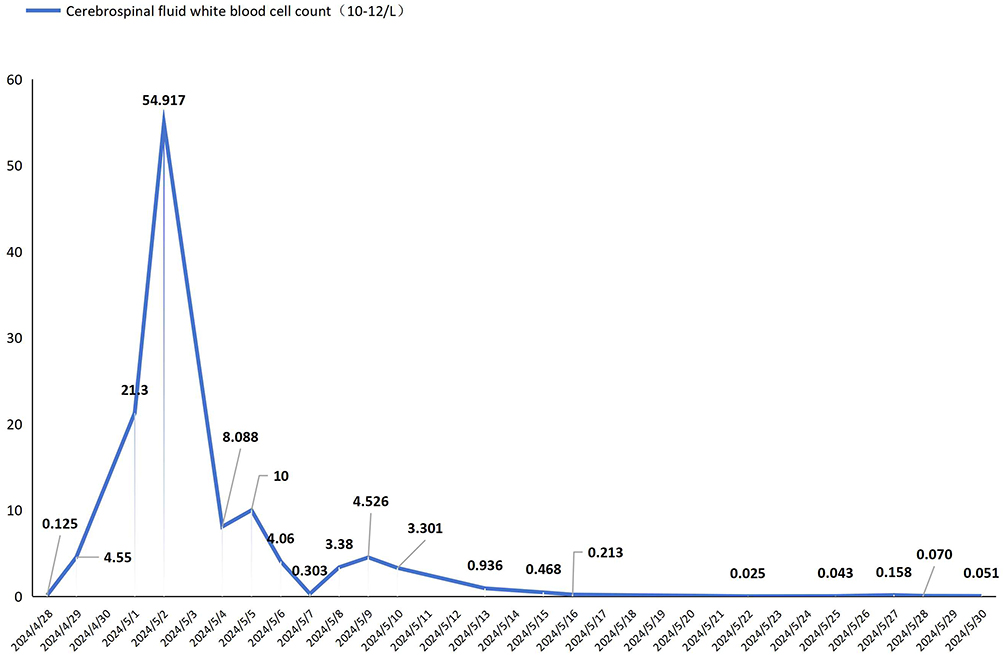 |
Figure 10 Curve of Changes in Cerebrospinal Fluid White Blood Cells. |
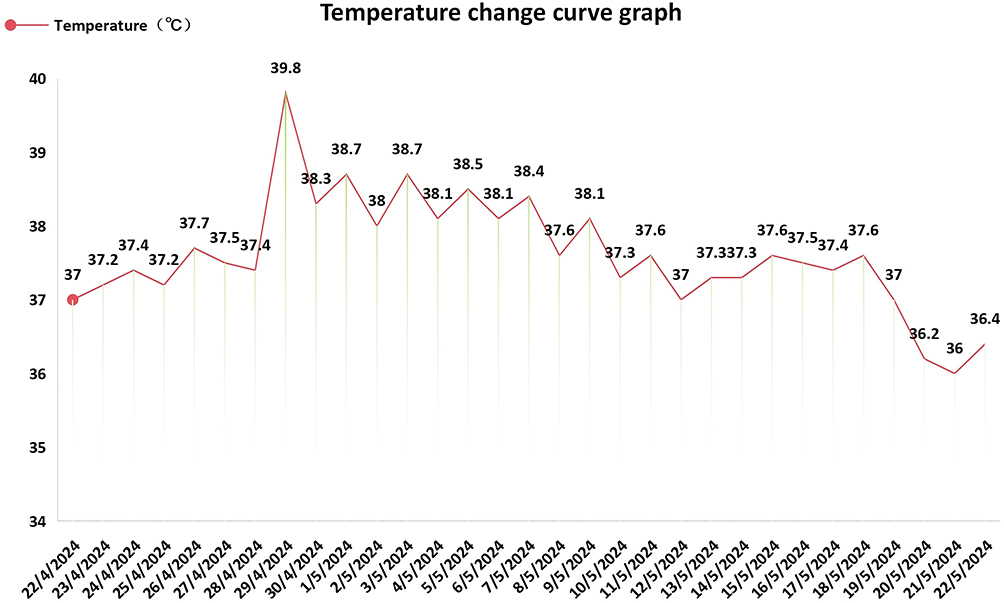 |
Figure 11 Curve of Body Temperature Changes. |
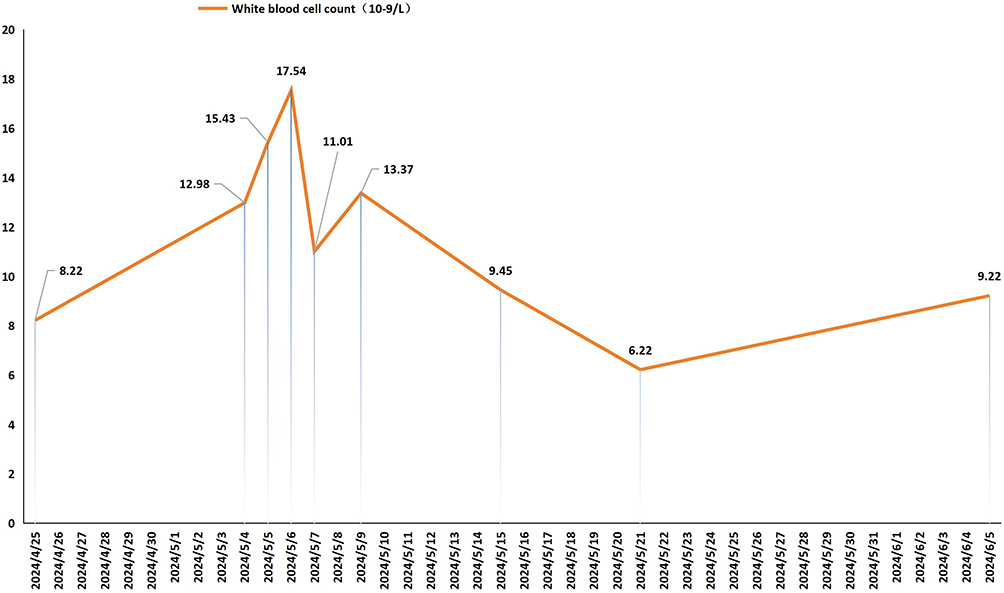 |
Figure 12 Curve of white blood cell changes in blood routine examination. |
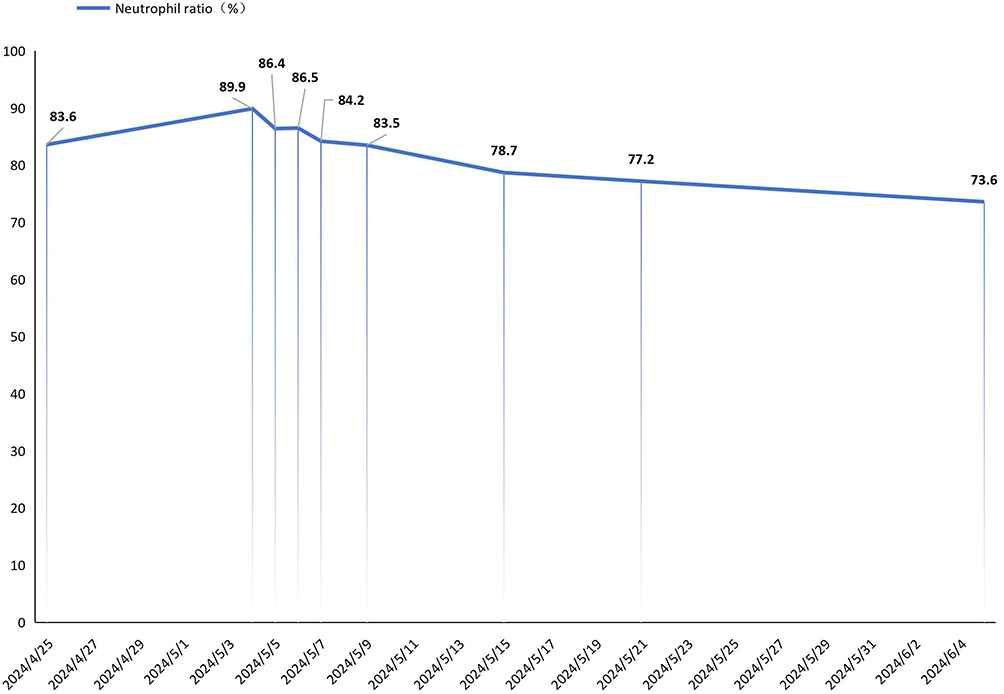 |
Figure 13 Curve of Neutrophil Ratio Change. |
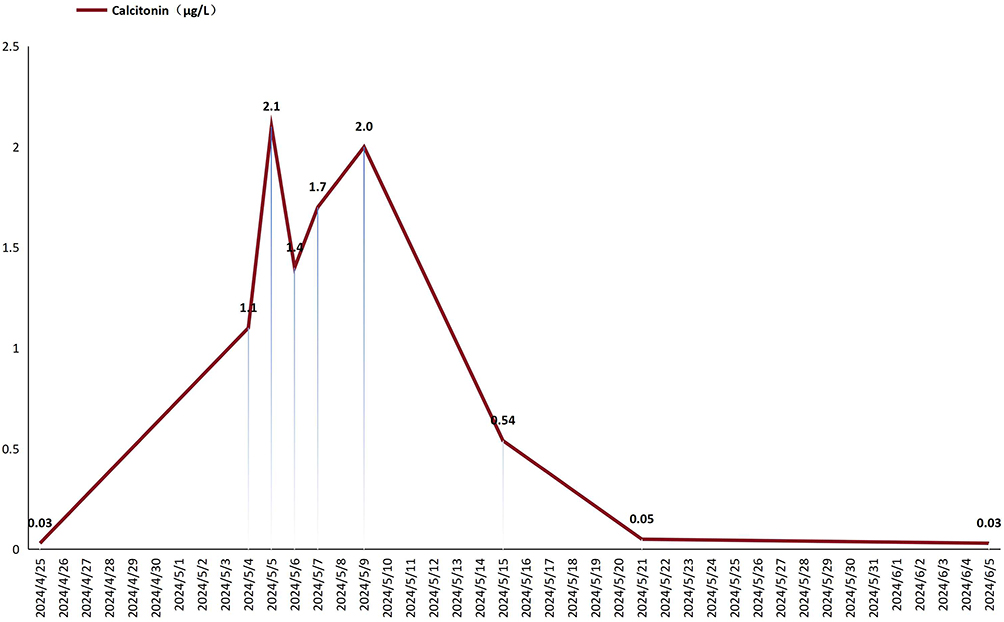 |
Figure 14 Curve of Calcitonin Changes. |
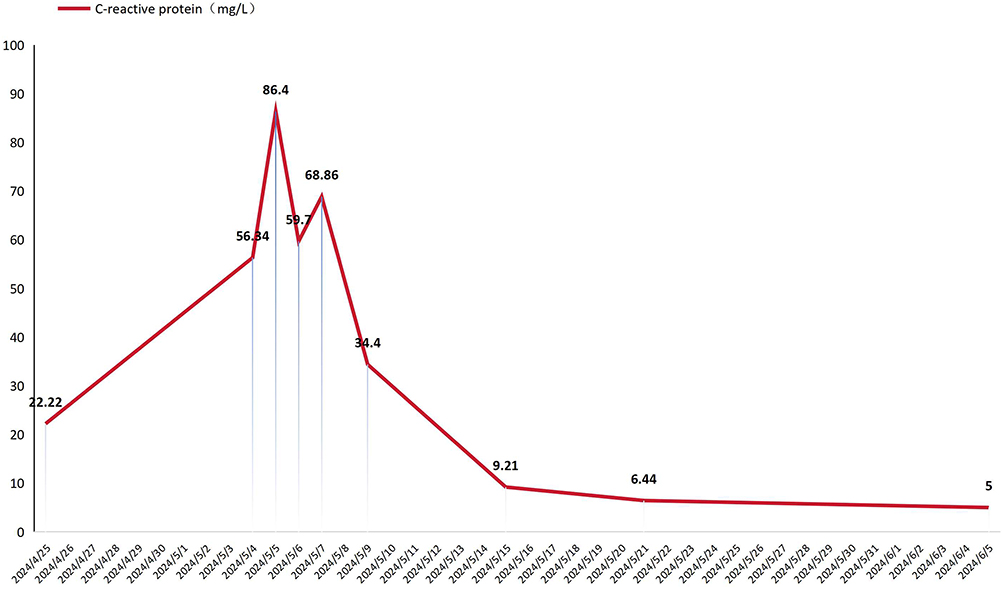 |
Figure 15 Curve of C-reactive protein variation. |
Discussion
The Acinetobacter baumannii strain is highly capable of acquiring resistance and spreading through cloning. Multiple-resistant, extensively-resistant, and fully-resistant Acinetobacter baumannii strains are globally prevalent and have become one of the most important pathogenic bacteria causing nosocomial infections in China.6 Antibiotic-resistant Acinetobacter baumannii is classified into three types: multidrug-resistant (MDR),7 extensively-resistant (XDR),8 and fully-resistant (PDR).9 Extensively-resistant Acinetobacter baumannii refers to the strain that is only sensitive to 1–2 types of potential antibiotic-resistant agents (mainly referring to tigecycline and/or polymyxin).10 In this case, the patient developed high fever 7 days after ventricular puncture for cerebral hemorrhage. The initial consideration was intracranial infection, and antibiotics meropenem were promptly administered. After abnormal cerebrospinal fluid tests and the appearance of cerebrospinal fluid resembling rice soup, combined treatment with vancomycin was given, and lumbar cistern drainage and cerebrospinal fluid replacement were performed. According to the 2012 “Expert Consensus on Diagnosis, Treatment and Prevention of Acinetobacter baumannii Infection in China”, for central nervous system infections caused by multi-drug-resistant Acinetobacter baumannii, combined medication is recommended; thus, the antibiotic regimen was adjusted to meropenem + vancomycin and combined with lumbar cistern drainage + cerebrospinal fluid replacement. The continuous lumbar cistern drainage mainly involves opening the lumbar cistern drainage tube to establish a flushing and drainage channel, promptly removing inflammatory substances and pathogens in the ventricles and subarachnoid space to avoid secondary damage caused by their retention; this method is also conducive to dynamic observation of cerebrospinal fluid, allowing for routine, biochemical tests and bacterial cultures to be performed at any time to understand the infection control situation and guide treatment.11 Due to the appearance of rice soup-like cerebrospinal fluid, drainage was prone to cause poor drainage or blockage during the procedure. In this case, the patient experienced a blocked drainage tube during the drainage period, so the lumbar cistern drainage tube was replaced promptly and cerebrospinal fluid replacement was further adopted. This not only allowed for the placement of a new blocked drainage tube but also facilitated the replacement of the rice soup-like cerebrospinal fluid, accelerating the circulation of cerebrospinal fluid and achieving better therapeutic effects with lumbar cistern drainage combined with cerebrospinal fluid replacement for Acinetobacter baumannii intracranial infections. Studies have shown that for 30 patients with Acinetobacter baumannii intracranial infections after craniocerebral trauma surgery, the treatment group receiving lumbar cistern drainage plus gentamicin irrigation had significantly better efficacy than the control group, with total effective rates of 86.7% and 66.7%, respectively.12 Additionally, it has been reported that tigecycline is the first member of the glycosylated cycline class of antibacterial drugs and has good antibacterial activity against extensively-resistant Acinetobacter baumannii, but due to its extensive tissue distribution, low blood concentration, and poor ability to penetrate the blood-brain barrier, it is difficult to reach an effective inhibitory concentration in cerebrospinal fluid and often requires combination with other antibacterial drugs; its pharmacokinetics does not fully support the treatment of Acinetobacter baumannii intracranial infections.13 Therefore, although this patient was treated with intravenous medication without combined intrathecal injection of tigecycline, but a physiological saline artificial cerebrospinal fluid replacement was adopted, which also achieved good therapeutic effects. Some scholars have reported successful treatment of extensively-resistant Acinetobacter baumannii intracranial infections with meropenem combined with cefoperazone sodium sulbactam; some have reported the use of meropenem and amikacin for treatment of neurosurgical postoperative infections caused by Acinetobacter baumannii.14,15 This patient also achieved good therapeutic effects by using meropenem combined with vancomycin.
Acinetobacter baumannii rarely causes community-acquired meningitis, but its association with intracranial infections after neurosurgery is becoming increasingly close, and it has become the main pathogen causing central nervous system infections in hospitals. The mortality rate of intracranial infections caused by it is 15%–71%.16 Preoperative GCS score < 5 points, cerebrospinal fluid leakage, placement of ventricular drainage, contamination of surgical incision, long surgical duration (> 4 hours), more than one surgery, and concurrent infections in other parts are independent risk factors for intracranial infections after neurosurgery.17,18 This patient developed high fever 7 days after surgery, with a cerebrospinal fluid white blood cell count of 54.917×1012 /L, increased protein content and decreased sugar content, but the cerebrospinal fluid bacterial culture was still negative at this time; To confirm the diagnosis, procalcitonin and C-reactive protein tests were performed, with results of 2.1 μg/L and 56.34 mg/L respectively; At the same time, cerebrospinal fluid culture was continued, and Acinetobacter baumannii was detected, thus highly suspecting Acinetobacter baumannii infection. Studies have shown that compared with patients with viral meningitis or no meningitis, the procalcitonin content in the cerebrospinal fluid of patients with bacterial meningitis is significantly increased. Procalcitonin in the cerebrospinal fluid may be a valuable marker for diagnosing bacterial meningitis, especially for patients after neurosurgery.19 Some studies have also shown that procalcitonin content can be used to assist in the differential diagnosis of patients with postoperative intracranial bacterial infections, with a diagnostic threshold of 0.803 ng/mL; and procalcitonin has the same change trend as other cerebrospinal fluid routine indicators (white blood cells, sugar, protein, etc.) and C-reactive protein in bacterial meningitis.20 Therefore, procalcitonin testing can indicate suspected intracranial bacterial infection in advance and guide medication. Currently, high-throughput pathogen gene testing (NGS technology) is also a good choice for diagnosing intracranial infections and is worthy of clinical adoption.21
At present, Acinetobacter baumannii can also be detected in blood samples, and there are several clinically validated nucleic acid testing methods available for its rapid, specific and sensitive identification and characterization. The current mainstream nucleic acid testing methods include conventional polymerase chain reaction (PCR) and its derivative technologies, such as targeted single-gene PCR, multiplex PCR and real-time fluorescent quantitative PCR (qPCR). Additionally, isothermal amplification techniques and high-throughput and cutting-edge molecular technologies are also gradually being applied.22–24
Post-neurosurgery intracranial infection is one of the serious and common complications. Due to the existence of the blood-brain barrier, it is difficult for antibacterial drugs to pass through it, and the drug concentration in the intracranial area is relatively low. Therefore, when there are widespread drug-resistant bacteria in intracranial infection, its treatment becomes a major clinical problem. In this case, the patient developed intracranial infection after ventricular puncture, with a critical condition and persistent high fever. Through the use of cerebrospinal fluid culture and routine biochemical monitoring combined with procalcitonin and C-reactive protein for auxiliary diagnosis to achieve early diagnosis of intracranial infection, effective guarantees were provided for timely treatment. After continuous intravenous administration of meropenem + vancomycin for 2 weeks, combined with lumbar cistern drainage + artificial cerebrospinal fluid replacement, the patient’s intracranial infection was controlled and improved. Thus, it can be seen that the above treatment plan has certain efficacy in treating Acinetobacter baumannii infection in the intracranial area. However, given that this study is merely an aggregated analysis of the diagnostic and treatment process for individual patients, and that advanced next-generation sequencing (NGS) technology was not employed for monitoring during the diagnosis stage, there is a certain lag in the treatment aspect. Therefore, regarding the treatment plan for Acinetobacter baumannii intracranial infection and its efficacy and safety, large-sample clinical studies are still needed to confirm these aspects.
Acknowledgments
The authors give thanks to all those who have helped with this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
1. Shaanxi Province Innovation Talent Promotion Program - Scientific and Technological Innovation Team (Number: 2024-RS-CXTD-83); 2. Doctoral Fund Project of the Second Affiliated Hospital of Xi’an Medical University (Number: X2Y-R11); 3. General Medical Research Project of Xi’an Science and Technology Bureau (Number: 24YXYJ0212).
Disclosure
Hao Wu and Wenwen Gao are co-first authors for this study. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Xiong X, Xie Y, Li B, Yin C, Hu K. Treatment of intracranial infection by extensively drug-resistant Acinetobacter baumannii after craniocerebral surgery. J Craniofacial Surg. 2024;35(7):e673–14. doi:10.1097/SCS.0000000000010542
2. Splavski B, Sisljagić V, Perić L, Vranković D, Ebling Z. Intracranial infection as a common complication following war missile skull base injury. Injury. 2000;31(4):233–237. doi:10.1016/s0020-1383(99)00273-9
3. Harding CM, Hennon SW, Feldman MF. Uncovering the mechanisms of Acinetobacter baumannii virulence. Nat Rev Microbiol. 2018;16(2):91–102. doi:10.1038/nrmicro.2017.148
4. Naseef Pathoor N, Valsa V, Ganesh PS, Gopal RK. From resistance to treatment: the ongoing struggle with Acinetobacter baumannii. Crit Rev Microbiol. 2025;51(6):1270–1291. doi:10.1080/1040841X.2025.2497791
5. Mahamad Maifiah MH, Velkov T, Creek DJ, Li J. Global metabolic analyses of Acinetobacter baumannii. Methods Mol Biol. 2019;321–328. doi:10.1007/978-1-4939-9118-1_28
6. Yue Z, Zhi X, Bi L, Zhao L, Ji J. Treatment and prognostic risk factors for intracranial infection after craniocerebral surgery. Neurosurg Rev. 2023;46(1):199. doi:10.1007/s10143-023-02106-0
7. Ibrahim S, Al-Saryi N, Al-Kadmy IMS, Aziz SN. Multidrug-resistant Acinetobacter baumannii as an emerging concern in hospitals. Mol Biol Rep. 2021;48(10):6987–6998. doi:10.1007/s11033-021-06690-6
8. Rezk S, Elwakeel NY, Ghazal A, Elsheredy A, Baecker D, Amer AN. In vitro evaluation of Colistin-Meropenem activity against XDR and PDR Carbapenemase-Producing Klebsiella pneumoniae and Acinetobacter baumannii. Pathogens. 2026;15(2):214. doi:10.3390/pathogens15020214
9. Falagas ME, Koletsi PK, Bliziotis IA. The diversity of definitions of multidrug-resistant (MDR) and pandrug-resistant (PDR) Acinetobacter baumannii and Pseudomonas aeruginosa. J Med Microbiol. 2006;55(Pt 12):1619–1629. doi:10.1099/jmm.0.46747-0
10. Hu Y, Li D, Zhang G, et al. Intraventricular or intrathecal polymyxin B for treatment of post-neurosurgical intracranial infection caused by carbapenem-resistant gram-negative bacteria: a 8-year retrospective study. Eur J Clin Microbiol Infect Dis. 2024;43(5):875–884. doi:10.1007/s10096-024-04794-y
11. Zhou H, Zhang X. Intracranial malignant lesions correlate with the requirement for a long treatment course in postoperative central nervous system infection. Neuropsychiatr Dis Treat. 2014;10:2071–2077. doi:10.2147/NDT.S71836
12. Paramythiotou E, Karakitsos D, Aggelopoulou H, Sioutos P, Samonis G, Karabinis A. Post-surgical meningitis due to multiresistant Acinetobacter baumannii. Effective treatment with intravenous and/or intraventricular colistin and therapeutic dilemmas. Med Mal Infectieuses. 2007;37(2):124–125. doi:10.1016/j.medmal.2006.11.011
13. Ma W, Zhang C, He B, Lv X, Luo P. Successful treatment of extensively drug-resistant Acinetobacter baumannii intracranial infection with meropenem and cefoperazone sodium sulbactam: a case report. Infect Drug Resist. 2025;18:1721–1727. doi:10.2147/IDR.S495491
14. Huang Q, Zhou Q, Ju T, Xu H, Wang W. Meropenem and amikacin for management of post-neurosurgical infections from Acinetobacter baumannii. Surg Infect. 2019;20(4):292–297. doi:10.1089/sur.2018.242
15. Li X, Sun S, Wang Q, Zhao Z. Population pharmacokinetics of combined intravenous and local intrathecal administration of meropenem in aneurysm patients with suspected intracranial infections after craniotomy. Eur J Drug Metabol Pharmacokinetics. 2018;43(1):45–53. doi:10.1007/s13318-017-0422-18
16. Datta D, Sekar A, Pasha A, Patnaik A, Sahu RN, Bansal S. Clinical, microbiological profile, and treatment response to intraventricular antibiotics in the management of post neurosurgical meningitis: a single-center experience. J Neurol Surg Part A. 2025;86(3):272–277. doi:10.1055/a-2312-92769
17. Alons IM, Verheul RJ, Kuipers I, et al. Procalcitonin in cerebrospinal fluid in meningitis: a prospective diagnostic study. Brain Behav. 2016;6(11):e00545. doi:10.1002/brb3.545
18. Yu Y, Li HJ. Diagnostic and prognostic value of procalcitonin for early intracranial infection after craniotomy. Braz J Med Biol Res. 2017;50(5):e6021. doi:10.1590/1414-431X20176021
19. Chen W, Liu G, Cui L, et al. Evaluation of metagenomic and pathogen-targeted next-generation sequencing for diagnosis of meningitis and encephalitis in adults: a multicenter prospective observational cohort study in China. J Infect. 2024;88(5):106143. doi:10.1016/j.jinf.2024.106143
20. Huang C, Gao Y, Lin H, Fan Q, Chen L, Feng Y. Prognostic factors that affect mortality patients with Acinetobacter baumannii bloodstream infection. Infect Drug Resist. 2024;17:3825–3837. doi:10.2147/IDR.S475073
21. Alshahni MM, Asahara M, Kawakami S, et al. Genotyping of Acinetobacter baumannii strains isolated at a Japanese hospital over five years using targeted next-generation sequencing. J Infect Chemother. 2015;21(7):512–515. doi:10.1016/j.jiac.2015.03.009
22. Tavares LCB, de Vasconcellos FM, Sant’Ana DA, Tiba-Casas MR, Camargo CH. Acinetobacter baumannii ST317 can be identified with Martins’ trilocus sequence-based multiplex-PCR. Infect Genet Evol. 2018;58:251–252. doi:10.1016/j.meegid.2018.01.008
23. Giselle Moreira M, Guimarães Oliveira AG, Ul Haq I, et al. Droplet digital PCR for Acinetobacter baumannii diagnosis in bronchoalveolar lavage samples from patients with ventilator-associated pneumonia. Antibiotics. 2024;13(9):878. doi:10.3390/antibiotics13090878
24. Gu Z, Liu T, Li J, et al. Enhancing upper respiratory tract infection detection: exploring qPCR negative respiratory samples using targeted next-generation sequencing. Infection. 2025;53(6):2433–2442. doi:10.1007/s15010-025-02578-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Lumbar Cistern Drainage and Gentamicin Intrathecal Injection in the Treatment of Carbapenem-Resistant Klebsiella Pneumoniae Intracranial Infection After Intracerebral Hemorrhage craniotomy: A Case Report

Zhou M, Liang R, Liao Q, Deng P, Fan W, Li C
Infection and Drug Resistance 2022, 15:6975-6983
Published Date: 30 November 2022
Successful Treatment of Extensively Drug-Resistant Acinetobacter baumannii Intracranial Infection with Meropenem and Cefoperazone Sodium Sulbactam: A Case Report
Ma W, Zhang C, He B, Lv X, Luo P
Infection and Drug Resistance 2025, 18:1721-1727
Published Date: 4 April 2025