Back to Journals » Infection and Drug Resistance » Volume 15
Lumbar Cistern Drainage and Gentamicin Intrathecal Injection in the Treatment of Carbapenem-Resistant Klebsiella Pneumoniae Intracranial Infection After Intracerebral Hemorrhage craniotomy: A Case Report
Authors Zhou M, Liang R, Liao Q, Deng P, Fan W, Li C ![]()
Received 19 July 2022
Accepted for publication 23 November 2022
Published 30 November 2022 Volume 2022:15 Pages 6975—6983
DOI https://doi.org/10.2147/IDR.S378753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Min Zhou, Richu Liang, Quan Liao, Pingfu Deng, Wentao Fan, Chenzhuo Li
The Second affiliated Hospital, Department of Neurosurgery, Hengyang Medical School, University of South China, Hengyang, 421001, People’s Republic of China
Correspondence: Richu Liang, The Second AFfiliated Hospital, Department of Neurosurgery, Hengyang Medical School, University of South China, Hengyang, 421001, People’s Republic of China, Email [email protected]
Background: Intracranial infection is a common complication caused by craniotomy. In particular, patients in Intensive Care Units (ICU) are prone to intracranial infection with multiple drug-resistant bacteria. Due to the lack of sensitive antibiotics for the treatment of multiple drug-resistant bacteria, there are few literatures focusing on the treatment of intracranial infection, and patients often fail to receive unified and standardized treatment. Consequently, patients with Carbapenem-resistant bacteria intracranial infection report poor prognosis and high mortality. It is very important to discuss how to treat patients with intracranial infection caused by multidrug resistant bacteria.
Case Presentation: We reported a case of intracranial infection of Carbapenem-resistant Klebsiella pneumoniae(CRKp) due to high flap tension, poor wound healing and CSF leakage caused by subcutaneous fluid accumulation after intracerebral hemorrhage craniotomy. Since the patient was exposed to intracranial infection resulted from subcutaneous fluid accumulation, we adopted the method of continuous drainage with subcutaneous tube. When subcutaneous effusion disappeared, the subcutaneous drainage tube was pull out, while patients exhibited high fever again, the waist big pool drainage catheter and continuous drainage were carried out. According to the result of Subcutaneous effusion and CSF culture indicated multiple drug resistant Klebsiella pneumoniae intracranial infection and drug susceptibility, The treatment of gentamicin intrathecal injection, intravenous use amikacin and oral Paediatric Compound Sulfamethoxazole Tablets was adopted, the condition of intracranial infection was eventually controlled, with the consciousness restored. This patient was characterized by intracranial infection with Carbapenem-resistant Klebsiella pneumoniae(CRKp).
Conclusions: Subcutaneous effusion is a high-risk factor for poor wound healing and interventions are required to be conducted to promote healing as early as possible to contribute to decreasing the menace of CSF leakage. In this case, Continuous drainage and intrathecal injection of sensitive antibiotics serve as critical process to determine the best strategy for clinical treatment of intracranial infection.
Keywords: intracranial infection, carbapenem-resistant Klebsiella pneumoniae, lumbar cistern drainage, intrathecal injection, gentamicin
Graphical Abstract:

Background
Intracranial infection, as a common complication after craniotomy that we strive to avoid while still often occur, is one of the most serious postoperative complications in neurosurgery. According to a meta-analysis study, number of operations, cerebrospinal fluid (CSF) leakage, CSF drainage, duration of operation (>four hours) and venous sinus entry are the risk factors for neurosurgical site infection after craniotomy.1 They are also mentioned in a case-control study.2 Non-standard operation during surgery, CSF leakage and Poor tightness of drainage device can be risk factors for intracranial infection.2 Especially in Intensive Care Units (ICU), once CSF leakage occurs, the bacteria are generally composed of multiple drug resistant bacteria,3,4 involving Acinetobacter baumannii, Klebsiella pneumoniae, Escherichia coli, Pseudomonas aeruginosa, etc.5 A study have shown that gentamycin irrigation can significantly reduce 28-day surgical site infection after emergency neurosurgery.6 A number of antibiotics fail to effectively enter the intracranial because of the blood-brain barrier. Without forming sufficient intracranial blood drug concentration, there have no effective drugs for multiple drug-resistant bacteria, resulting in the high mortality rate of intracranial infection. Continuous and effective drainage, the application of sensitive antibiotic and elevation of the individual immunity are the essential aspects of the treatment of intracranial infection. Due to the patient’s own disease status, the body’s immune capacity is generally at a low level.7 Therefore, the control of intracranial infection depends on continuous and effective drainage as well as the application of sensitive antibiotics. Intrathecal injection has developed to be an effective measure to elevate the concentration of intracranial antibiotics. Carbapenem-resistant Klebsiella pneumoniae(CRKp) is a kind of multi-drug resistant bacteria prevalent in the world, which is characterized by strong virulence, high adaptability and high infectivity.8 Intracranial infection caused by carbapenem-resistant Klebsiella pneumoniae(CRKp) is uncommon, while has a strong drug resistance and rather high mortality, as was reported to be about 42.14% in a meta-analysis study about the combined mortality of pneumonia patients infected with carbapenem-resistant Klebsiella pneumoniae(CRKp).9 Currently, intracranial infection of carbapenem-resistant Klebsiella pneumoniae(CRKp) is rarely reported, which, however, results in higher mortality than pneumonia. At present, the treatment of carbapenem-resistant Klebsiella pneumoniae(CRKp) mainly adopts polymyxin B and tigecycline,10,11 but there still appears drug resistance transformation in the treatment process.12 In this report, a patient with carbapenem-resistant Klebsiella pneumoniae(CRKp) intracranial infection after intracerebral hemorrhage craniotomy was treated with continuous Lumbar cistern drainage, Polymyxin and tigecycline could not be purchased in time due to the cost pressure on the family of patient, the treatment options of amikacin intravenous injection, gentamicin intrathecal injection and the use of oral co-trimoxazole, and the intracerebral infection was rapidly controlled, reporting a better prognosis.
Case Presentation
The 40-year-old male patient was admitted to hospital on April 18, 2022 due to sudden hemiplegia of the right limb for 1 hour and subsequent coma for 2 hours. Physical examination on admission reported, coma, GCS score = E1V1M3 =5, muscle strength of the right limb level 0, with stabbing and flexion of the left limb, diagnosed with cerebral hemorrhage in the left basal ganglia region (Figure 1A); After admission, the left frontotemporal parietal craniotomy was performed for hematoma removal and decompression with bone flap removal. The head CT reexamination on April 19 (Figure 1B) suggested that the hematoma in the left basal ganglia region had been cleared, the middle line was in the center, and the cistern was clearly displayed. After craniotomy on Apr 21, subdural effusion can be seen (Figure 1C). The head CT reexamination on April 24 (Figure 1D) indicated that residual hematoma and intraventricular hematoma in left basal ganglia region were basically absorbed, and effusion could be seen beside falx and subcutaneously. The head CT reexamination On May 10 (Figure 1E) showed that subcutaneous effusion significantly progressed. On May 11, due to the high tension of the flap, cerebrospinal fluid (CSF) leakage occurred in the wound, and the highest body temperature was 39.5°C. Lumbar puncture was performed, and the CSF was cloudy, with 1690×106/L white blood cells, 2034.6 mg/ L protein and 0.16 mmol/L glucose (Table 1). On May 12, the intracranial infection was considered to be caused by CSF leakage from the wound caused by subcutaneous effusion. In order to solve the flap tension and continuous drainage, the decompression window flap was subcutaneous drainage (Figure 2A) and drainage tube was fixed (Figure 2B). The test results of subcutaneous effusion were 4916×106/L white blood cell, 3.30 mmol/L glucose and 2565.8 mg/L protein (Table 1). Four groups of puncture fluid were taken for culture and drug sensitivity test. The head CT reexamination on May 14 (Figure 1F) showed a significant decrease in subcutaneous effusion. On May 16, the tension of the flap had decreased significantly and the body temperature was normal. The subcutaneous drainage tube was removed. On May 17, the head CT reexamination (Figure 1G) indicated that the subcutaneous effusion of left frontotemporal parietal had disappeared, and CT enhancement (Figure 1H) showed no obvious enhancement. However, after the removal of subcutaneous drainage tube, high fever occurred again, and the body temperature continued above 39.5°C. Lumbar puncture was performed, with 570×106/L white blood cells, 2.56 mmol/L glucose and 2506.8 mg/ L protein in CSF (Table 1), indicating that severe intracranial infection still existed, so lumbar cistern catheter drainage was performed. On May 18, all CSF culture and drug sensitivity results suggested multiple drug resistant Klebsiella pneumoniae, and the isolated strain was Enterobacteriaceae resistant to carbapenems antibiotics (Table 2). Due to the lack of polymyxin B and tigecycline of our hospital, patients’ families failed to buy polymyxin B and tigecycline, only can use amikacin. On May 19, the patient’s body temperature continued to be above 39.5°C, and the CSF was cloudy (Figure 3A). The white blood cells in the CSF rose again to 6168×106/L, glucose 1.83 mmol/L, and protein 1403.0mg/ L (Table 1). Due to the lack of polymyxin B and tigecycline, intrathecal injection of gentamicin and oral cotrimoxazole were used according to drug sensitivity results (Table 2). On May 20, the patient’s body temperature was controlled below 38°C, and the CSF white blood cells were 112×106/L, glucose 2.03 mmol/L, and protein 1643.0mg/L (Table 1). On May 21, the patient’s body temperature was controlled at about 38°C, and the CSF white blood cells were 366×106/L, glucose 2.95 mmol/L, and protein 1464.6 mg/ L (Table 1). On May 22, the patient’s body temperature was controlled at 37°C, and the CSF white blood cells were 84×106/L, glucose was 2.93 mmol/L, and protein was 1093.6 mg/ L (Table 1). On May 23, the patient’s body temperature was normal, with CSF white blood cells of 6×106/L, glucose of 2.20 mmol/L, and protein of 1683.6 mg/L (Table 1). The lumbar cistern is blocked, and the tube should be pulled out. On May 24, the head CT (Figure 1I) showed no obvious hydrocephalus, subcutaneous effusion disappeared, the middle line was centered, and the cistern was clear. On May 28, the patient’s body temperature was normal, and the CSF white blood cells were 8×106/L, glucose was 2.41 mmol/L, protein was 1279.3mg/ L (Table 1), the CSF was clear (Figure 3B). On May 30, slight hydrocephalus was observed (Figure 1J). At present, the infection has been controlled and the consciousness was regained. The patient has been transferred to a rehabilitation hospital for further treatment.
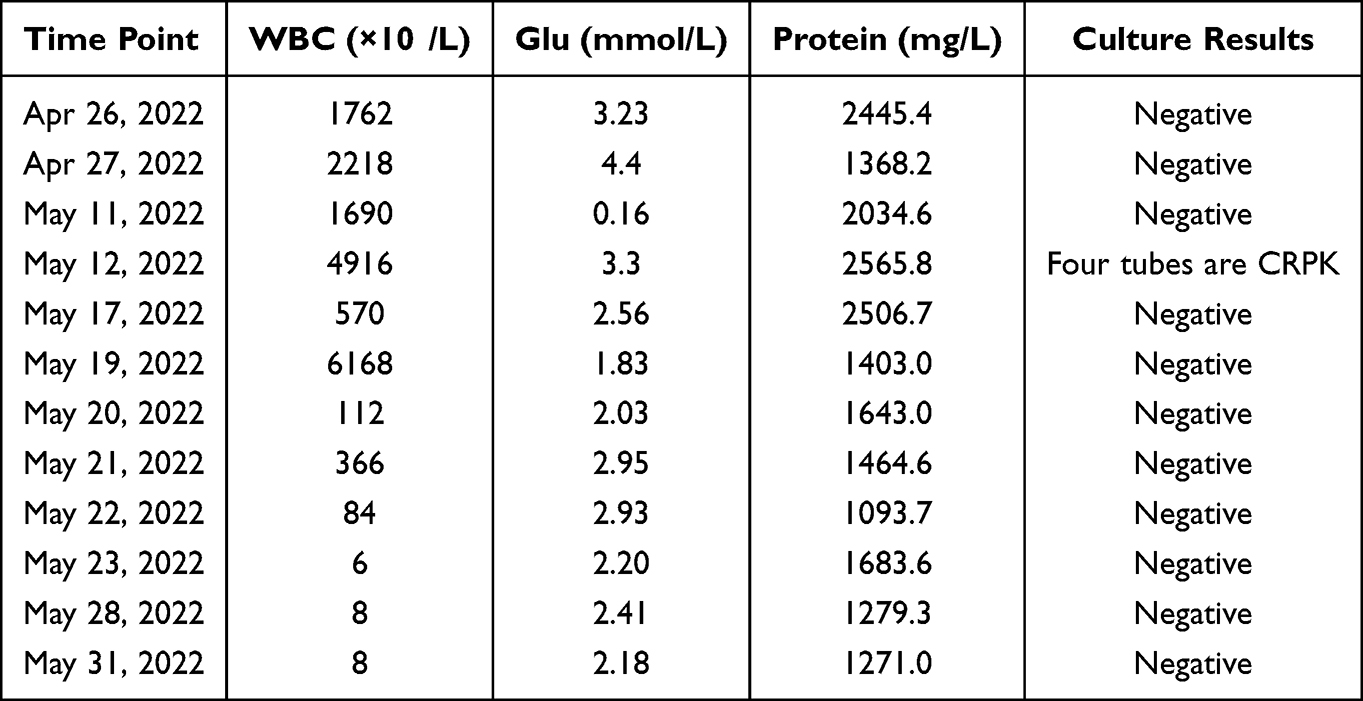 |
Table 1 Laboratory Examination of CSF in Patient with Intracranial CRPK Infection |
 |
Table 2 Bacterial Culture of CSF in Patient with Intracranial Infection |
 |
Figure 1 Brain CT after admission in patient with intracranial CRPK infection. (A) Before craniotomy on Apr 18. (B) After craniotomy on Apr 19. (C) After craniotomy on Apr 21, subdural effusion can be seen. (D) After craniotomy on Apr 24, a small amount of subdural effusion appeared. (E) After craniotomy on May 10, Subdural Effusion has developed significantly. (F) After cerebrospinal fluid leakage and intracranial infection on May 14, subcutaneous drainage tube was inserted, subdural Effusion decrease. (G) After cerebrospinal fluid leakage and intracranial infection on May 17, Subdural Effusion disappear. (H) enhanced CTbrain scanning showed no brain abscess on May 17. (I) After the treatment of anti-infective regimen on May 24. (J) After the treatment of anti-infective regimen on May 30, Ventricular Dilatation was observed. |
 |
Figure 2 Location of subcutaneous drainage tube and method of compression in skull defect area. (A) Location of subcutaneous drainage tube. (B) A sport headband is used to pressurize the skull defect area. |
 |
Figure 3 Changes in cerebrospinal fluid (CSF) in patient with intracranial A. baumannii infection before and after treatment. (A) CSF on May 19; (B) CSF on May 28. |
Discussion and Literature Review
Causes of Intracranial Infection
Here reported a case of hypertensive intracerebral hemorrhage, and the patient’s body temperature remained low in the early postoperative period. The subdural effusion progressed gradually after craniotomy, and broke through the incision,13 causing the CSF leakage on wound. The body temperature of patient obviously elevated the second day, lasting more than 39.5 °C, the physical measures such as ice blankets exhibited poor cooling effect. CSF examination revealed an obvious elevation of CSF protein and white cells level, the CSF glucose level decreased, which prompted severe intracranial infection. In this case, the intracranial infection sourced from a leak of CSF from the wound, which has always acted as the primary cause of intracranial infection, whether it is CSF leakage from incision, skull base fracture, or poor sealing of drainage device. Once intracranial infection occurs, the condition will be significantly aggravated, generally accompanied with difficult treatment.14 Therefore, close attention requires to be paid to the existence of CSF leakage in clinical course management, and maintain the characteristic of an airtight seal of cranial cavity by preventing the CSF leakage through early intervention.15
Selection of Anti-Infection Treatment Strategies for Carbapenem-Resistant Klebsiella Pneumoniae(CRKp)
The patient was clearly diagnosed in a rather short period from onset. Previous to the use of high-intensity antibiotics, we consciously obtained CSF samples, the obtained culture and drug sensitivity results indicated carbapenem-resistant Klebsiella pneumoniae(CRKp), of which the polymyxin B and tigecycline serve as the first choice for the treatment of infection according to the literature and guidelines.10,16 Vancomycin and meropenem were adopted before CSF culture and drug sensitivity results were obtained, but failed to achieve the expected effect. The patient’s family had not purchased polymyxins B or tigecycline, while the high fever continued to become worse. We had no choice but to select sensitive antibiotics from CSF cultures, taking the protocol of amikacin intravenous injection. After two days of amikacin intravenous injection, the body temperature exhibited a downward trend, but the white blood cells in CSF showed a significant upward trend, counted to be 6168×106/L. Therefore, continuous drainage plus intravenous amikacin failed to achieve significant results. So we added two other sensitive antibiotics, intrathecal injection of gentamicin and oral co-trimoxazole, and the patient’s body temperature decreased significantly in two days. The body temperature and CSF indicators gradually returned to normal under this treatment, and the consciousness regained. In this case, co-trimoxazole was generally difficult to form effective intracranial concentrations across the BLOOD-brain barrier, and amikacin was initially ineffective. Therefore, continuous drainage of lumbar cisterns and intrathecal injection of gentamicin may be the crux to successful treatment of carbapenem-resistant Klebsiella pneumoniae(CRKp) intracranial infection.17
Characteristics of Carbapenem-Resistant Klebsiella Pneumoniae(CRKp)
Carbapenem-resistant Klebsiella pneumoniae(CRKp), as a well-known superbug, causes hospital infections and develops to a major threat to public health security. Carbapenem-resistant KLEbsiella pneumoniae(CRKp) is common in the ICU and exhibits colonizing, which has a significantly increased risk to be contracted by patients hospitalized in the ICU.18 Carbapenem-resistant Klebsiella pneumoniae(CRKp) infections account for 64% of carbapenem-resistant enterobacteria(CRE), aggravating hospital stay and medical costs to a large extent, and affecting prognosis.19 Resulted from the conjugate plasmids of carbapenem-resistant Klebsiella pneumoniae(CRKp) that encode drug resistance and high virulence, its capability to transmit infection is greatly enhanced. Typical of carbapenem-resistant Klebsiella pneumoniae(CRKp) ST11 and ST307, widespread in ICU environment, often cause hospital outbreaks and transmission.12,20–22 Polymyxin B and tigecycline have large molecular weight with weak BBB permeability. Therefore, intrathecal injection is recommended for the clinical use of these two drugs.17,23
Applicability and Application of Gentamicin in the Treatment of Carbapenem-Resistant Klebsiella Pneumoniae(CRKp)
Gentamicin is recommended for the treatment of severe infections caused by sensitive Gram-negative bacteria such as Escherichia coli, Klebsiella, Enterobacter, Proteus, Serratia, Pseudomonas aeruginosa and methicillin-sensitive strains of staphylococcus. At the same time, the instructions clearly stated that gentamicin can serve for the treatment of central nervous system (CNS) infection caused by sensitive bacteria, such as meningitis, ventriculitis, and can also be injected intrathecal as an auxiliary treatment. However, gentamicin is not the first choice for the treatment of CRKp intracranial infection. In this case, amikacin and gentamicin are commonly used injection preparations, but the drug instruction manual of amikacin does not specify that it can be used for intrathecal injection, which is a legal risk. And the MIC value of amikacin is four. According to the drug instruction manual, the antibacterial spectrum of amikacin and gentamycin are similar, gentamicin prospectus can specify intrathecal injection treatment of intracranial infection and ventricle inflammation, and the MIC value of gentamicin is one, it is lower than amikacin, and more sensitive than amikacin. In the routine operation process, We also often use gentamicin for irrigation,6 so we chose gentamicin for intrathecal injection. The dose of intrathecal and intraventricular injection was 4–8 mg for adults and 1–2 mg for children (over 3 months old) every 2–3 days. During injection, the drug solution was diluted to a concentration of no more than 0.2%, pumped into a sterile syringe of 5 mL or 10 mL. After lumbar puncture, a considerable amount of CSF was injected into the syringe, and all the drug solution was slowly injected within 3 ~ 5 minutes by pumping and pushing. In this case, intracranial infection of carbapenem-resistant Klebsiella pneumoniae(CRKp) was finally controlled by intrathecal injection of 8 mg/time/day as per the instruction for 4 days. Although aminoglycosides are historically susceptible antibiotics for CRE, they are not widely adopted as monotherapy for severe infections due to the lower clinical efficacy, potential toxicity, and extensive drug resistance.24 Chen Xiuli et al studied Synergistic Effect and Mechanism of Plumbagin with Gentamicin Against Carbapenem-Resistant Klebsiella pneumoniae(CRKp), so as to reduce the dosage of gentamicin in the treatment.25 Intrathecal injection of gentamicin may cause convulsions and other symptoms. During the use of gentamicin, attention should be paid to preventing seizures and strictly control the concentration of intrathecal injection during the use of gentamicin at the same time, In fact, the incidence of seizures is very low when gentamicin is widely used in China. In this case, gentamicin appeared no toxic or side effects. Marcelino Gonzalez-Padilla et al reported a research about gentamicin therapy for sepsis due to carbapenem-resistant and colistin-resistant Klebsiella pneumoniae.26 Shmuel Benenson et al reported a case of Carbapenem-Resistant Klebsiella pneumoniae(CRKp) endocarditis successful treated by gentamicin and colistin.27 Therefore, If the susceptibility test is positive, gentamicin is also effective in treating carbapenem-resistant Klebsiella pneumoniae(CRKp).
Summary
The good effect in this case may benefit from the following aspects. Firstly, the diagnosis in a timely manner. In the CSF leak on the first day, the patient showed a fever, the line of lumbar puncture was carried out in time, the CSF examination has cleared the diagnosis of intracranial infection, and the bacteriology examination has cleared the resistance to carbon penicillium alkene with Klebsiella pneumoniae intracranial infection. Secondly, decisive treatment. Continuous subcutaneous drainage was conducted punctually, with a daily drainage flow of about 200 mL, subcutaneous effusion disappeared, and the infected dead cavity was eliminated. Thirdly, lumbar cistern drainage. The lumbar cistern drainage was immediate, and the intracerebral inflammation was relieved. The last, treatment of sensitive antibiotics. The key is the high sensitivity of gentamicin to carbapenem-resistant Klebsiella pneumoniae(CRKp). After intrathecal injection of gentamicin only once, white blood cells significantly decreased, indicating that gentamicin has rather robust bactericidal capacity to this bacterium.
Conclusion
Firstly, subcutaneous effusion is a high-risk factor resulting in poor wound healing, which should be treated punctually to reduce flap tension and inhibit the chance of CSF leakage. The second, lumbar cisternal drainage with intrathecal injection of sensitive antibiotics is an effective way to treat intracranial infection. At present, the successful case of gentamicin in the treatment of carbapenem-resistant Klebsiella pneumoniae intracranial infection has not been reported, and lacks large sample randomized controlled studies, its effectiveness remains to be further studied.
Abbreviations
BBB, blood-brain barrier; CNS, Central nervous system; CSF, Cerebrospinal fluid; CT, Computed tomography; GCS, Glasgow Coma Scale; MIC, Minimum inhibitory concentration; MDR, multiple drug-resistant; CRKp, Carbapenem-resistant Klebsiella pneumoniae.
Author Details
The Second Affiliated Hospital, Department of Neurosurgery, Hengyang Medical School, University of South China, Hengyang, Hunan, 421001, China.
Data Sharing Statement
The data and information are true and reliable. If you need this data, you can get it from Min Zhou or the corresponding author.
Ethics Approval and Informed Consent
The treatment of this case was conducted in accordance with the Declaration of Helsinki. All procedures were performed in accordance with the ethical standards of the Clinical Research ethical committee of The Second Affiliated Hospital, University of South China(2022k061701). Informed consent was obtained by the patient and his family in the case.
Acknowledgments
We would like to thank to all the medical staff in ICU of the Second Affiliated Hospital of University of South China.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Key Project of Hunan Provincial Health Commission of China (20201912).
Disclosure
The authors declare that they have no competing interests.
References
1. Fang C, Zhu T, Zhang P, et al. Risk factors of neurosurgical site infection after craniotomy, A systematic review and meta-analysis. Am J Infect Control. 2017;45(11):e123–e134. doi:10.1016/j.ajic.2017.06.009
2. Wang LY, Cao XH, Shi LK, et al. Risk factors for intracranial infection after craniotomy, A case-control study. Brain Behav. 2020;10(7):e01658. doi:10.1002/brb3.1658
3. Ramos LL, García C, Iribarren J, et al. Colonization and infection by potential Gram-negative multiresistant microorganism in a medical–surgical ICU. Crit Care. 2008;12(Suppl 2):P36. doi:10.1186/cc6257
4. Wang L, Huang X, Zhou J, et al. Predicting the occurrence of multidrug-resistant organism colonization or infection in ICU patients, development and validation of a novel multivariate prediction model. Antimicrob Resist Infect Control. 2020;9(1):66. doi:10.1186/s13756-020-00726-5
5. Lee B, Yan J, Ulhaq A, et al. Vitro activity of rifabutin and rifampin against antibiotic-resistant Acinetobacter baumannii, Escherichia coli, staphylococcus aureus, pseudomonas aeruginosa, and Klebsiella pneumoniae. mSphere. 2021;6(6):e0092021. doi:10.1128/msphere.00920-21
6. Wang J, Yang Y, Lv W, et al. Gentamycin irrigation significantly reduces 28-day surgical site infection after emergency neurosurgery. Br J Neurosurg. 2021;1–5. doi:10.1080/02688697.2021.1902472
7. Castro I, Ruiz J, Tasias M, et al. Central nervous system infections in immunocompromised patients. Rev Esp Quimioter. 2018;31(Suppl1):56–61. doi:10.1007/s11910-021-01119-w
8. Ernst CM, Braxton JR, Rodriguez-Osorio CA, et al. Adaptive evolution of virulence and persistence in carbapenem-resistant Klebsiella pneumoniae. Nat Med. 2020;26(5):705–711. doi:10.1038/s41591-020-0825-4
9. Xu L, Sun X, Ma X. Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae. Ann Clin Microbiol Antimicrob. 2017;16(1):18. doi:10.1186/s12941-017-0191-3
10. Tian Y, Zhang Q, Wen L, Chen J. Combined effect of polymyxin B and tigecycline to overcome heteroresistance in carbapenem-resistant Klebsiella pneumoniae. Microbiol Spectr. 2021;9(2):e0015221. doi:10.1128/Spectrum.00152-21
11. Liang Q, Huang M, Xu Z. Early use of polymyxin B reduces the mortality of carbapenem-resistant Klebsiella pneumoniae bloodstream infection. Braz J Infect Dis. 2019;23(1):60–65. doi:10.1016/j.bjid.2018.12.004
12. Jin X, Chen Q, Hen F, et al. Resistance evolution of hypervirulent carbapenem-resistant Klebsiella pneumoniae ST11 during treatment with tigecycline and polymyxin. Emerg Microbes Infect. 2021;10(1):1129–1136. doi:10.1080/22221751.2021.1937327
13. Kinaci A, Algra A, Heuts S, et al. Effectiveness of dural sealants in prevention of cerebrospinal fluid leakage after craniotomy, a systematic review. World Neurosurg. 2018;118:368–376.e1. doi:10.1016/j.wneu.2018.06.196
14. Ter Horst L, Brouwer MC, van der Ende A, van de Beek D. Community-acquired bacterial meningitis in adults with cerebrospinal fluid leakage. Clin Infect Dis. 2020;70(11):2256–2261. doi:10.1093/cid/ciz649
15. Kinaci A, Van Doormaal TPC. Dural sealants for the management of cerebrospinal fluid leakage after intradural surgery, current status and future perspectives. Expert Rev Med Devices. 2019;16(7):549–553. doi:10.1080/17434440.2019.1626232
16. Hou SY, Wu D, Feng XH. Polymyxin monotherapy versus polymyxin-based combination therapy against carbapenem-resistant Klebsiella pneumoniae, A systematic review and meta-analysis. J Glob Antimicrob Resist. 2020;23:197–202. doi:10.1016/j.jgar.2020.08.024
17. Wang J, Liu H, Zheng K, et al. Clinical effect of intrathecal injection of medicine combined with continuous lumbar cistern drainage on intracranial infection after intracranial tumor surgery. Pak J Pharm Sci. 2021;34(1):65–67.
18. Qin X, Wu S, Hao M, et al. The colonization of carbapenem-resistant Klebsiella pneumoniae, epidemiology, resistance mechanisms, and risk factors in patients admitted to intensive care units in China. J Infect Dis. 2020;221(Suppl 2):S206–S214. doi:10.1093/infdis/jiz622
19. Zhang H, Wang J, Zhou W, et al. Risk factors and prognosis of carbapenem-resistant Klebsiella pneumoniae infections in respiratory intensive care unit, A retrospective study. Infect Drug Resist. 2021;14:3297–3305. doi:10.2147/IDR.S317233
20. Liao W, Liu Y, Zhang W. Virulence evolution, molecular mechanisms of resistance and prevalence of ST11 carbapenem-resistant Klebsiella pneumoniae in China, A review over the last 10 years. J Glob Antimicrob Resist. 2020;23:174–180. doi:10.1016/j.jgar.2020.09.004
21. Yang Y, Yang Y, Chen G, et al. Molecular characterization of carbapenem-resistant and virulent plasmids in Klebsiella pneumoniae from patients with bloodstream infections in China. Emerg Microbes Infect. 2021;10(1):700–709. doi:10.1080/22221751.2021.1906163
22. Magi G, Tontarelli F, Caucci S, et al. High prevalence of carbapenem-resistant Klebsiella pneumoniae ST307 recovered from fecal samples in an Italian hospital. Future Microbiol. 2021;16:703–711. doi:10.2217/fmb-2020-0246
23. Li Z, An Y, Li L, Yi H. Intrathecal injection of tigecycline and polymyxin B in the treatment of extensively drug-resistant intracranial Acinetobacter baumannii infection, A case report and review of the literature. Infect Drug Resist. 2022;15:1411–1423. doi:10.2147/IDR.S354460
24. Zavascki AP, Klee BO, Bulitta JB. Aminoglycosides against carbapenem-resistant Enterobacteriaceae in the critically ill, the pitfalls of aminoglycoside susceptibility. Expert Rev Anti Infect Ther. 2017;15(6):519–526. doi:10.1080/14787210.2017.1316193
25. Chen X, Yin L, Peng L, et al. Synergistic effect and mechanism of plumbagin with gentamicin against carbapenem-resistant Klebsiella pneumoniae. Infect Drug Resist. 2020;13:2751–2759. doi:10.2147/IDR.S265753
26. Gonzalez-Padilla M, Torre-Cisneros J, Rivera-Espinar F, et al. Gentamicin therapy for sepsis due to carbapenem-resistant and colistin-resistant Klebsiella pneumoniae. J Antimicrob Chemother. 2015;70(3):905–913. doi:10.1093/jac/dku432
27. Benenson S, Navon-Venezia S, Carmeli Y, et al. Carbapenem-resistant Klebsiella pneumoniae endocarditis in a young adult. Successful treatment with gentamicin and colistin. Int J Infect Dis. 2009;13(5):e295–8. doi:10.1016/j.ijid.2009.01.006
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cerebrospinal Fluid Exchange Combined with Intrathecal Antibiotic Injection for the Management of Severe Intracranial Infection Caused by Hypervirulent Klebsiella pneumoniae: A Case Report
Wei H, Xu L, Li L, Shen Y, Yu S, Huang H, Huang X
Infection and Drug Resistance 2025, 18:4723-4730
Published Date: 4 September 2025
Multi-Route Administration Therapy for Intracranial Acinetobacter baumannii Infection After Postoperative Cerebral Hemorrhage: A Case Report
Wu H, Gao W, Cheng Y, Yuan Z, Zhang L, Zhao H
International Medical Case Reports Journal 2026, 19:609143
Published Date: 16 June 2026