Back to Journals » Journal of Pain Research » Volume 19
Multi-Institutional Pragmatic Randomized Controlled Trial to Evaluate the Effectiveness of Manual Maintenance Therapy for Chronic Bothersome Neck Pain
Authors Yun JM, Kim JY, Lee SH, Lee YJ ![]() , Heo I, Shin WC
, Heo I, Shin WC ![]() , Cho JH, Seo BK
, Cho JH, Seo BK ![]() , Ha IH
, Ha IH ![]()
Received 29 October 2025
Accepted for publication 10 March 2026
Published 18 March 2026 Volume 2026:19 577619
DOI https://doi.org/10.2147/JPR.S577619
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Jung Min Yun,1 Ju Yeon Kim,2 Sook-Hyun Lee,2 Yoon Jae Lee,2 In Heo,3 Woo-Chul Shin,4 Jae-Heung Cho,5 Byung-Kwan Seo,6 In-Hyuk Ha2
1Clinical Division, Jaseng Hospital of Korean Medicine, Seoul, Republic of Korea; 2Jaseng Spine and Joint Research Institute, Jaseng Medical Foundation, Seoul, Republic of Korea; 3Department of Korean Medicine Rehabilitation, Pusan National University Korean Medicine Hospital, Yangsan, Republic of Korea; 4Department of Korean Medicine Rehabilitation, Kyung Hee University Medical Center, Seoul, Republic of Korea; 5Department of Rehabilitation Medicine of Korean Medicine, Kyung Hee University, Seoul, Republic of Korea; 6Department of Acupuncture & Moxibustion, College of Korean Medicine, Kyung Hee University Hospital at Gangdong, Kyung Hee University, Seoul, Republic of Korea
Correspondence: In-Hyuk Ha, Jaseng Spine and Joint Research Institute, Jaseng Medical Foundation, Seoul, Republic of Korea, Tel +82-2-2222-2740, Fax +82-2-2222-2737, Email [email protected]
Purpose: Numerous studies have analyzed the effects of Chuna therapy, a manual therapy technique used in Korea, on musculoskeletal disorders. However, research on Chuna maintenance therapy (CMT), which aims to prevent the recurrence of disorders and improve health status through regular long-term application, is lacking. This protocol outlines a randomized clinical trial designed to evaluate the comparative effectiveness of CMT for chronic neck pain, particularly in cases where mild discomfort has become habitual.
Patients and Methods: This two-arm, multi-institutional, assessor-blinded, pragmatic randomized controlled trial will enroll 250 participants with chronic bothersome neck pain for more than 12 months and an average Numeric Rating Scale (NRS) score of 2– 4 over the past month, recruited from seven Korean medicine hospitals. Participants will be randomly assigned to one of two groups: the CMT group or the self-care and exercise (SE) group. Over a total period of 20 weeks, the CMT group will receive 10 treatment sessions, while the SE group will receive 5 education sessions. After treatment completion, a follow-up will be conducted twice over a 6-week period. The primary outcome are the average neck pain NRS score and the Neck Disability Index (NDI), both assessed over the preceding 2 weeks. Secondary outcomes include the Visual Analog Scale, number of days with bothersome neck pain, recurrence, the Patient Global Impression of Change, Credibility and Expectancy Questionnaire, quality of life, cost-effectiveness evaluation, and safety assessments. For the primary analysis, group-specific areas under the curve for NRS and NDI will be calculated using a linear mixed model. The primary endpoint is the first follow-up visit (Visit 11) after treatment completion.
Conclusion: The findings may inform clinical and policy decision-making by providing evidence on the effectiveness, safety, and cost-effectiveness of CMT.
Trial Registration Number: This study is registered at ClinicalTrials.gov (NCT06591221; September 7, 2024) and the Clinical Research Information Service (CRIS; KCT0009798).
Keywords: clinical trial protocol, Chuna therapy, manual maintenance therapy, neck pain, pragmatic clinical trial
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Srivastava has been published for this article.
Introduction
Neck pain refers to pain in and around the neck region, which may worsen with movement, potentially limiting neck mobility, and, in some cases, radiate to the upper extremities. Neck pain is a frequently occurring musculoskeletal disorder that has a highly variable prevalence. However, the lifetime prevalence in adults ranges from 14.2% to 71%.1 Within a year of onset, neck pain progresses to chronic neck pain in 25–60% of cases,2 and approximately 37% of cases experience persistent chronic bothersome neck pain for at least 12 months.3 Crucially, distinguishing between “persistent mild pain” and “full recovery” is vital for understanding chronicity patterns. As demonstrated by Irgens et al (2022), patients following a “persistent mild pain” trajectory (pain intensity 2–4) represent a distinct subgroup separate from those achieving full recovery (pain intensity <2). Unlike recovered cases where symptoms resolve, the persistent mild pain group continues to experience reduced physical health-related quality of life and functional limitations despite lower pain scores.4 This suggests that persistent mild pain is not merely a near-recovery phase but a stable chronic condition requiring distinct clinical attention. Specifically, patients with mild neck pain (pain intensity 2–4 on a 0–10 scale) who initially experienced pain relief during a 1-year clinical course continued to report persistent chronic bothersome neck pain.4 Patients with mild neck pain for 6 months exhibited worse outcomes in physical health-related quality of life than those without neck pain.5
Chuna therapy (CT) is a manual therapy used by Korean medicine doctors to treat structural or functional issues, in which they apply manual techniques to address structural or functional problems using their hands or auxiliary tools, such as a bed.6 Modern CT integrates not only Korea’s traditional CT but also Chinese Tuina, American chiropractic, osteopathic manual therapy, and Japanese manual therapy, which have all been developed on the theoretical foundations of Korean medicine.7,8 According to 2023 statistics from the Korean Health Insurance Review and Assessment, CT has been administered in over 4.79 million cases across more than 1.17 million patients.9 A Cochrane review of manual therapy for neck pain10 showed that manual therapy was more effective than medication in relieving pain and restoring function in acute and subacute neck pain. Manual therapy is also more effective for chronic neck pain than transcutaneous electrical nerve stimulation, oral medication, or physical therapy.10,11
In chiropractic care, maintenance care is a well-known therapeutic concept that constitutes ongoing management beyond symptom reduction to prevent new episodes of illness and continuously improve chronic pain symptoms.12 Based on several studies in Scandinavia that have investigated the indications, frequency, and content of chiropractic maintenance care, chiropractors share a common management strategy.13–16 However, despite the widespread use of maintenance care, there is limited evidence regarding its effectiveness.17,18 Furthermore, CT is based on the holistic perspectives of Korean medicine, and is used not only to treat symptoms but also address their underlying causes.19 Beyond these theoretical foundations, the plausibility of CT for maintenance care is supported by physiological mechanisms such as proprioceptive training and muscular adaptation.20,21 Manual interventions have been reported to improve cervical joint position sense and normalize paraspinal muscle activity, which may enhancing neuromuscular control.22 These biomechanical improvements could contribute to segmental stability and may help reduce symptom recurrence, supporting the plausibility of CT with long-term maintenance strategies. Chuna maintenance therapy (CMT) is intended as a long-term, low-frequency therapy to prevent recurrence and improve the quality of life in cases where disabling pain and functional disorders have improved, but habitual mild discomfort persists. However, a randomized controlled trial (RCT) on CMT has not yet been conducted.
Chronic neck pain imposes a substantial economic burden on the healthcare system, consistently ranking among the top causes of disability and healthcare spending globally.23,24 This burden is driven not only by severe acute episodes but significantly by the cumulative costs of managing persistent mild symptoms and frequent recurrences over the long term. Given this high resource utilization, identifying efficient management strategies is critical from a health economics perspective.
Therefore, this study aims to evaluate the effectiveness and cost-effectiveness of CMT in patients with chronic neck pain. We will conduct a pragmatic RCT to consider the applicability of CMT in real-world clinical settings to provide evidence base for CT use not only in cases of pain worsening but also to prevent symptom recurrence and continuously improve chronic pain symptoms, thereby addressing both clinical needs and the growing healthcare burden.
Materials and Methods
This study protocol follows the 2013 SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) guidelines.25 The completed SPIRIT checklist that has been included as Supplementary Material 1 as well as Table 1 outline the recommended schedule for enrollment, interventions, and assessments.
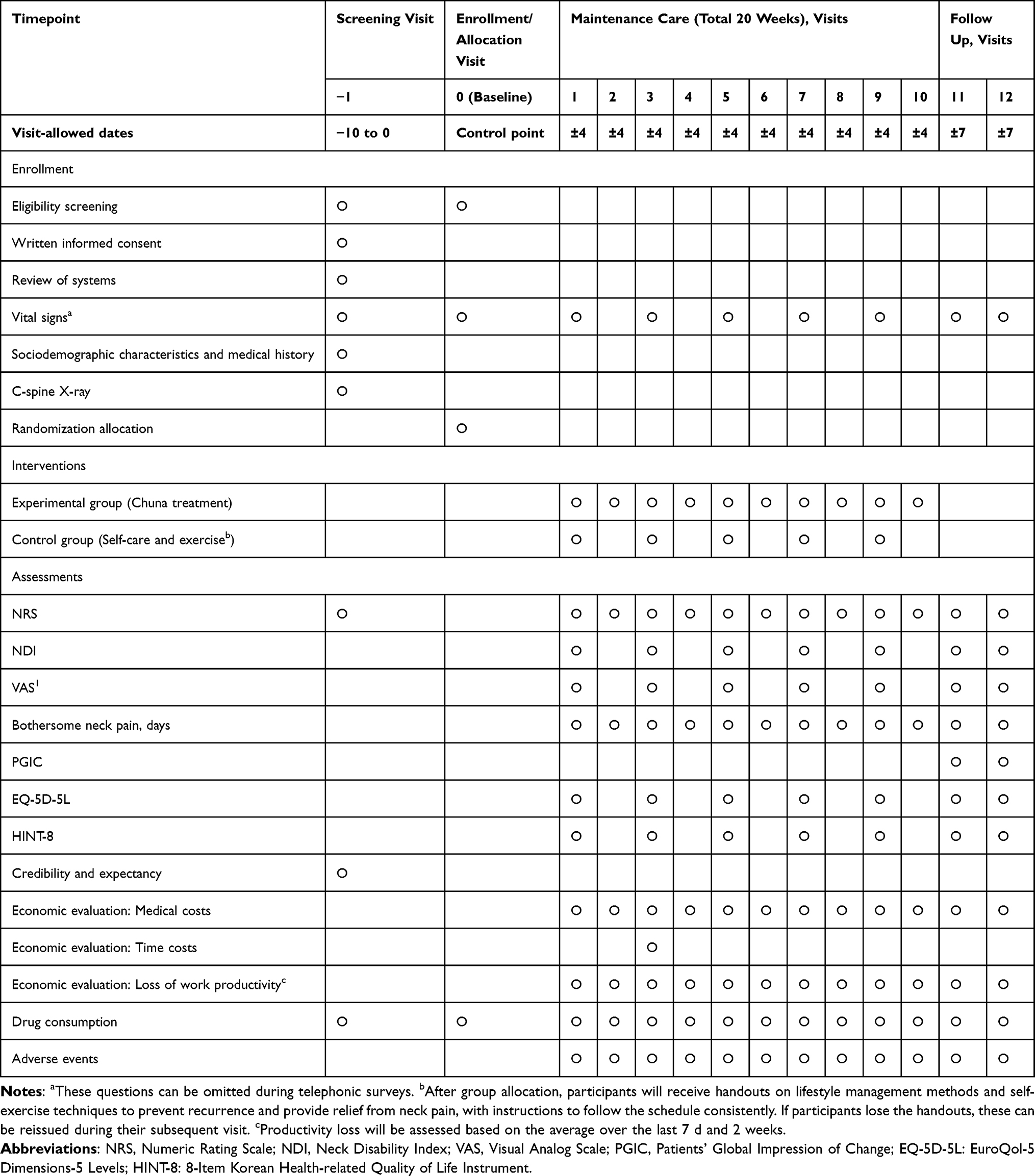 |
Table 1 Schedule of Enrollment, Intervention, and Assessment |
Study Design and Setting
A two-armed, multi-institution, pragmatic randomized controlled study with 250 participants will be conducted at a total of seven institutions: Jaseng Hospital of Korean Medicine (Seoul, Republic of Korea), Daejeon Jaseng Hospital of Korean Medicine (Daejeon, Republic of Korea), Bucheon Jaseng Hospital of Korean Medicine (Bucheon, Republic of Korea), Haeundae Jaseng Hospital of Korean Medicine (Haeundae, Republic of Korea), Kyung Hee University Korean Medicine Hospital (Seoul, Republic of Korea), Kyung Hee University Hospital at Gangdong (Seoul, Republic of Korea), and Pusan National University Korean Medicine Hospital (Yangsan, Republic of Korea). Participants will be recruited through competitive enrollment. The study protocol was approved by the institutional review board (IRB) of each institution prior to participant recruitment (approval nos. JASENG 2024–02-006, JASENG 2024–02-007, JASENG 2024–02-008, JASENG 2024–02-009, KOMCIRB 2024–03-004, KHNMCOH 2024–03-002-004, and PNUKHIRB 2024–03-007). Furthermore, this protocol has been registered at ClinicalTrials.gov (NCT06591221) on September 7, 2024, and with the Clinical Research Information Service (KCT0009798) and will be continuously updated as the study progresses. Prior to the commencement of the study, the principal investigator will lead training on standard operating procedures (SOPs) to ensure standardization of clinical trial procedures.
Participant Timeline
At the first visit, participants will receive detailed information about the study and will provide written informed consent. Next, an X-ray examination (C-Spine anteroposterior/lateral) will be conducted to confirm the safety of the cervical spine prior to the procedure, and the investigator will screen participants for eligibility according to the prespecified inclusion/exclusion criteria. During the second visit, participants will be randomly assigned (1:1) to either the CMT or self-care and exercise (SE) groups. During the 20-week study period, participants in the CMT and SE groups will visit the institution 10 and 5 times (one session every 2 and 4 weeks), respectively, for the interventions. For both groups, face-to-face assessments will be conducted during the 1st, 3rd, 5th, 7th, and 9th visits, whereas telephonic assessments will be performed for the 2nd, 4th, 6th, 8th, and 10th visits. During the posttreatment follow-up phase, face-to-face assessments will be conducted during the 11th and 12th visits. The schedules for participant enrollment, interventions, and assessments are shown in Table 1.
Inclusion Criteria
The inclusion criteria are as follows:
- Age between 19 and 70 years
- Neck pain, with persistent symptoms for >12 months
- Average Numeric Rating Scale (NRS) score between 2 and 4 for neck pain in the past month
- Willingness to participate in the clinical study and provide written informed consent.
Exclusion Criteria
The exclusion criteria are as follows:
- Diagnosed with severe specific diseases that may cause neck pain (eg, spinal metastasis of tumors, acute fractures, and spinal dislocation).
- Progressive neurological deficit or severe neurological symptoms.
- Non-spinal soft-tissue diseases as the source of pain (eg, tumors, fibromyalgia, rheumatoid arthritis, and gout).
- Chronic diseases that could interfere with treatment effects or the interpretation of results (eg, stroke, myocardial infarction, kidney disease, diabetic neuropathy, dementia, and epilepsy).
- Current use of steroids/immunosuppressants/psychiatric medications or other drugs that could significantly affect overall health.
- Pregnant, planning to conceive, or currently breastfeeding.
- Less than 3 months since cervical surgery.
- Participation in another clinical study within the preceding month or plans to participate in another clinical study or follow-up assessment within 6 months from the date of selection.
- Inability to provide informed consent.
- Patients for whom the investigator deemed that participation in the clinical study would prove difficult.
Criteria for Discontinuation and Withdrawal
The study may be discontinued for participants under the following conditions:
- Subsequent discovery of a violation of the inclusion/exclusion criteria during the study.
- Diagnosis of a disease that could affect the evaluation of the study results that was undetected during the initial screening.
- If the participant or their legal representative requests to withdraw from the study, or if the participant withdraws consent to participate.
- If pregnancy is confirmed during the study.
- If there are issues with performing medical or Korean medicine procedures related to neck pain for the participant.
- If, in the judgment of the research investigator, continued participation is deemed inappropriate for any other reason.
Recruitment, Randomization, Allocation, and Blinding
Participants will be recruited through online media releases and promotional posters that are posted both inside and outside the study sites. Participants who voluntarily sign the informed consent form and are deemed eligible for the study after review of the inclusion and exclusion criteria will be randomly assigned to one of the two groups (125 participants in each group), based on a randomization table generated by a statistician using R Studio 1.1.463 (© 2009–2018 R Studio, Inc). The random sequence will be generated using permuted block randomization, with block sizes randomly set to 2, 4, or 6, and stratified by the study site. Sealed, opaque randomization envelopes will be assigned through competitive enrollment and stored in a double-locked cabinet. The researchers at each site will open the randomization envelope for each participant to assign them to a group. As blinding is not feasible for this study, this trial will be conducted as an open-label study with assessor blinding. The assessors, who are either study nurses or specialist trainees blinded to group allocation and not involved in the interventions, will perform assessments in a separate area prior to the study-related procedures. Details of outcome measures that could compromise the blinding (eg, Credibility and Expectancy Scale, cost data collection, drug consumption, adverse events) will be excluded to ensure effective assessor blinding.
Interventions
Experimental Group: CMT
CMT will be administered to participants with chronic neck pain, where mild discomfort has become habitual, once every 2 weeks for a total of 20 weeks. CT will be based on the Chuna Manual Medicine (2.5nd edition),26,27 published by the Korean Society of Chuna Manual Medicine for Spine and Nerves, which is used as a textbook in Korean medical schools. The type of CT will be selectively determined according to the clinician’s judgment and diagnosis, and the specific type of CT will be recorded in each session. Details of the CT scanners used in this study are listed in Supplementary Material 2. To minimize inter-practitioner differences in the application of therapy, standardized CT training sessions will be provided. CT will be performed by a specialist in Korean rehabilitation medicine/acupuncture and moxibustion medicine, a licensed Korean medicine doctor with more than 1 year of clinical experience in CT under the supervision of a specialist, or a Korean medicine doctor who has completed more than 1 year of workshop-based training organized by the Korean Society of Chuna Manual Medicine for Spine and Nerves.
Control Group: SE
Participants will be provided with handouts on lifestyle management and self-exercise methods for the prevention of recurrence and relief from neck pain and, at each visit, will be educated to practice these methods consistently. The handouts will include information on the definition and causes of neck pain as well as illustrations, explanations, and effects of various stretching methods that can be practiced in different situations. Participants will be instructed to select and perform at least one stretching method once a day, and their adherence to this requirement will be checked and recorded at each visit. Education on lifestyle management and self-exercise methods will be provided once every 4 weeks for a total of 20 weeks.
Cointerventions
Participants of this clinical study are not restricted from choosing any additional treatments (cointerventions). As in actual clinical settings, participants may select any cointervention to alleviate discomfort during the study-related treatment and observation periods. In the case report form (CRF), the researcher will record the type, frequency, and purpose of any cointervention that the participant receives.
Outcomes
Primary Outcome Measurements
NRS
At 2-week intervals for a total of 20 weeks, the NRS will be used to assess the average neck pain score over the past 2 weeks. Participants will choose the number that best represents their current level of discomfort on a scale from 0 (no pain) to 10 (worst imaginable discomfort).28 Furthermore, the NRS score of the most severe pain experienced in the past 2 weeks will be assessed. During the 6-week posttreatment follow-up period, the average NRS scores for neck pain and the most severe pain in the preceding 2 weeks will be assessed twice (at visits 11 and 12).
Neck Disability Index (NDI)
The NDI is used to assess the level of disability caused by neck pain in daily life. The NDI consists of 10 items, with each scored from 0 to 5. The final NDI score is the average of the total scores divided by the number of items answered.29 NDI will be evaluated at 4-week intervals during the treatment period (visits 1, 3, 5, 7, and 9) and twice during the 6-week posttreatment follow-up period (visits 11 and 12).
Secondary Outcome Measurements
Visual Analog Scale (VAS)
The VAS will be used to assess neck pain over the preceding 2 weeks. Participants will record the intensity of pain that they feel on a horizontal 100-mm line, where one end represents “no pain” and the other end represents the “worst imaginable pain”.30 The average VAS scores for neck pain and the most severe pain experienced in the past 2 weeks will be assessed at 2-week intervals for a total of 20 weeks. Two additional assessments will be conducted during the 6-week posttreatment follow-up period (visits 11 and 12).
Number of Days of Bothersome Neck Pain
Participants will be asked to report the number of days (between 0 and 14 d) that they experienced bothersome neck pain in the past 2 weeks during all 12 visits.
Recurrence
In this study, “recurrence” is defined as the occurrence of moderate-level pain,31 operationalized as an average pain NRS score ≥6 over the past 2 weeks and will be assessed every 2 weeks during the treatment and posttreatment follow-up periods.
Patient Global Impression of Change (PGIC)
The PGIC is a subjective assessment tool for participants to self-assess their level of improvement on a 7-point scale: 1 = very much improved; 2 = much improved; 3 = minimally improved; 4 = no change; 5 = minimally worse; 6 = much worse; and 7 = very much worse.32
Credibility and Expectancy
The participants’ expectations of the treatment will be assessed using a 9-point Likert scale.33
Quality of Life Assessments
The quality of life will be assessed as follows:
EuroQol-5 Dimension-5Level ((EQ-5D-5L)
EQ-5D-5L assesses health status from multiple perspectives using predefined preference weights to indirectly calculate quality-of-life scores. The five items assess mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.34,35
Korean 8-Item Health-Related Quality of Life Instrument (HINT-8)
HINT-8 was developed to assess the health-related quality of life in Koreans and consists of eight items that cover four health domains (physical, social, mental, and positive health dimensions).36
Cost Data Investigation
The questionnaire for cost assessment will include items that measure costs related to medical, non-medical, time, and loss of productivity aspects.37–39 Medical costs include formal medical expenses (costs incurred for medical services at healthcare institutions) and informal medical expenses (eg, costs for health supplements or medical devices). Nonmedical costs include transportation, patient time, and caregiving costs. Loss of productivity will be assessed using the Work Productivity and Activity Impairment questionnaire,40 and the results will be converted into costs for the cost-effectiveness analysis. The loss of productivity loss will be assessed based on the average loss over the previous 7 days and 2 weeks.
Drug Consumption
The type and dosage of any medication taken by the participants during the study (including prescription and rescue medications) will be recorded through surveys conducted during participant visits. Furthermore, other treatments, such as physical or injection therapy, will be recorded by counting the number of sessions.
Adverse Events
Adverse events are defined as undesirable and unintended symptoms, signs, or diseases that occur after an intervention, regardless of their causal relationship with the intervention. All adverse event data will be collected and summarized, and serious adverse events will be described. The intergroup difference in the frequency of adverse events will be ascertained. For any delayed adverse events, the participants will be encouraged to seek medical attention as directed by the investigator.
The causal relationship between the intervention and the adverse events will be evaluated according to the World Health Organization Uppsala Monitoring Center causality assessment system. Using the Spilker Classification, the severity of adverse events will be classified into three levels (Mild, Moderate, or Severe). The rate of occurrence of adverse events will be calculated, and the proportion of participants with adverse events in each group will be compared using the chi-square or Fisher’s exact test.
Stopping Rules
The clinical trial may be stopped at any time if an unexpected, clinically significant, or unacceptable new risk related to CMT or SE is discovered in the study participants.
Sample Size
This study will compare the effects of CMT, lifestyle management, and self-exercise in patients with chronic neck pain that causes discomfort in daily life. Although no prior study has evaluated CMT, Cohen’s d was calculated using the outcome data from a previous study18 that compared three groups: a spinal manual therapy and self-exercise group, a self-exercise-only group, and a no-treatment group. In a two-group comparison between the spinal manual therapy and self-exercise groups and the no-treatment group, the pooled standard deviation (SD) was estimated as 2.59, with an assumed mean difference of 1.30, based on pain scores (VAS) from the reference study. The SD of 2.59 was estimated by considering the sample sizes and SDs of the test group (SD 2.3) and the control group (SD 2.9). The mean difference (1.30) was similarly estimated from the sample sizes and SDs, with a test group mean of 1.6 and a control group mean of 2.9.
Cohen’s d = (mean difference) / (pooled SD).
Cohen’s d was calculated as 0.50. Similarly, for NDI, using the same method, Cohen’s d was calculated as 0.79.
Given that this is a pragmatic study wherein cointerventions for the treatment of neck pain are allowed in both the test and control groups, and medical usage patterns are determined, the effect size may be small. Therefore, the sample size was calculated based on a Cohen’s d of 0.50. Using a Student’s t-test with Cohen’s d effect size and by applying the Bonferroni method, the significance level was set at α = 0.025 and power at 90%. This resulted in an estimation of 100 participants per group. To account for potential dropouts, which are difficult to predict, a dropout rate of 20% was assumed, which resulted in a requirement of 125 participants per group, or a total of 250 participants. Participants will be recruited from seven institutions, and the 250 participants required for the study will be enrolled through competitive enrollment until the target number is met.
Statistical Analysis
All statistical analyses will be performed using SAS 9.4 (© SAS Institute, Inc., Cary, NC, USA) or R Studio 1.1.463 (© 2009–2018 RStudio, Inc)., with the level of significance set at p<0.05.
Main Analysis
In this study, both ITT (intention-to-treat) and per-protocol analyses will be performed, with ITT serving as the primary analysis. Additional analyses will include sensitivity analyses based on the handling of missing data to assess the robustness of the results and will involve the multiple imputation and last observation carried forward (LOCF) methods. The sociodemographic characteristics and treatment expectations of the participants will be evaluated for each group. Continuous variables will be expressed as mean (standard deviation) or median (interquartile range), and the intergroup differences will be evaluated using the Student’s t-test. Categorical variables will be expressed as frequencies (%) and assessed using the chi-square or Fisher’s exact test.
In the primary analysis, the main outcomes, NRS and NDI, will be compared between the two groups over the observation period. Group-specific areas under the curve (AUC) for NRS and NDI will be calculated using a linear mixed model (LMM). The primary endpoint is the first follow-up visit (Visit 11) after treatment completion.
Secondary analyses will assess the intergroup differences in changes from baseline to each timepoint for continuous outcomes (NRS, NDI, VAS, days with bothersome neck pain, EQ-5D-5L, and HINT-8). An LMM will be used to analyze trends in each outcome over time. Missing data will be handled using a Mixed Model for Repeated Measures, and sensitivity analyses will be performed using multiple imputation and LOCF.
For the categorical outcome of recurrence, defined as an average pain NRS score ≥6 over the past 2 weeks, the number and proportion of participants experiencing recurrence at each timepoint will be presented. To statistically compare the recurrence rates between the two groups, a survival analysis will be conducted by comparing the time-to-event until recurrence. A Cox Proportional Hazard Ratio Model will be used to compare hazard ratios, and Kaplan–Meier survival analysis will be employed, with significance tested using the Log rank test and the confidence interval set at 95%. Participants who drop out will be treated with right censoring, and intermittent censoring will assume that no events have occurred during the censored period. Missing data will be handled using multiple imputation.
For the primary analysis, the comparison of AUCs calculated using the LMM and the analysis of changes from baseline in outcome measures will focus on the NRS and NDI. The Bonferroni correction will be applied to adjust for multiple comparisons, with the significance level for the primary outcome set at 0.025.
Subgroup Analysis
Exploratory subgroup analyses will be conducted to compare the degree of improvement in pain in the CMT and SE groups.
Data Collection, Management, and Monitoring
To ensure retention and completion of follow-up, the recruited participants will be contacted continuously from recruitment until the two posttreatment visits (visits 11 and 12). Participants can reach out to the researchers at any time to obtain the necessary information. This study utilizes the electronic CRF managed by the Korea Centers for Disease Control and Prevention. The SOP will be distributed for reference, covering CRF completion, data entry, and training of evaluators and investigators at each site. Data queries will be conducted to verify the range of data values. The data entered into the CRF will be isolated, locked, and concealed from all investigators except those responsible for data management. Data will be monitored to ensure the safety of the participants and the integrity of the study data. The safety of the participants will be reviewed, and the completeness of the data will be verified by comparing the CRFs with supporting documentation. Monitoring will be conducted three times: during the initial participant selection, once during the course of the study (after treatment completion), and once at the completion of the clinical study.
Confidentiality
The principal investigator will assign a unique identification number to each participant and the information of all participants registered in the study will be encrypted. The medical information obtained in this clinical study will remain confidential and will only be disclosed to third parties within the limits permitted by the consent form (or separate authorization for the use and disclosure of personal health information) that is signed by the participants. Medical information may be provided to appropriate healthcare professionals responsible for the well-being of the participants for treatment purposes. If necessary, the data from this study may be used for investigations by monitoring personnel, contractors, or the IRB of the research institution upon request.
Ethics and Dissemination
Before the commencement of the study, the study protocol, CRF, informed consent form (ICF), and recruitment notices were submitted to the IRB of each institution for approval (JASENG March 20; KOMCIRB May 13; KHNMCOH May 07; PNUKHIRB April 02). Amendments to the study protocol, CRF, ICF, or recruitment notices will only be made with IRB approval, and all changes will be updated in the trial registries. All clinical researchers involved in this study will be trained on the Declaration of Helsinki, Korean Good Clinical Practice Guidelines, study protocol, and SOPs to ensure the protection of the study participants. Furthermore, this protocol has been registered at ClinicalTrials.gov (NCT06591221) and with the Clinical Research Information Service (KCT0009798).
Before starting the clinical trial, participants will be fully informed about the study details (including effects, adverse events, and safety) and will provide voluntary consent by signing an informed consent form to ensure that they are eligible to participate in the study; a copy of the consent form will be provided to each participant.
The results of this study will be disseminated internationally through manuscript publication in peer-reviewed journals.
Discussion
CT has been utilized for neck pain at various stages from acute to chronic presentations, and numerous studies have reported its clinical effectiveness.11,41–43 Previous studies have reported significant pain relief when CT was administered for 3–5 weeks during the pain-onset period, with short-term effects. However, this study is distinct in that it is designed to evaluate the use of CT as a long-term, maintenance-oriented intervention for patients with chronic neck pain, where persistent mild discomfort has become habitual. The study will target patients who have had neck pain for more than 12 months, with an average NRS of 2 to 4, and whose chronic neck pain causes discomfort in daily life. Thus, this study aims to address a patient population characterized by chronic, bothersome symptoms that may not consistently prompt active treatment, yet can lead to intermittent care-seeking when symptoms worsen.
Generally, maintenance care is interpreted as “a therapy designed to provide ongoing well-being to the patient or to minimize the recurrence of clinical conditions while maintaining optimal health”.44 In musculoskeletal disorders, 98% of chiropractors affiliated with the Swedish Chiropractors’ Association asserted the necessity of chiropractic maintenance care to prevent the recurrence of back pain and suggested that it should be considered as tertiary preventive care when the patient’s symptoms have improved by more than 75%.45 In chiropractic clinical practice, a long history of neck pain serves as a major clinical index in patients who receive chiropractic maintenance care after initial treatment for at least 4 weeks.46
Mechanistically, CT may influence longer-term symptom control through improvements in proprioception and neuromuscular control, as suggested in prior studies.20,21 However, these proposed mechanisms have not been established specifically for maintenance care and warrant further investigation. Thus, this study is designed to evaluate CMT as a maintenance-oriented approach in a pragmatic trial setting.
Unlike previous explanatory trials, which were optimized for evaluating the validity of physiological or clinical hypotheses under controlled conditions, pragmatic trials contribute to clinical or policy decisions by providing evidence for the implementation of interventions in real-world clinical practice.47 Pragmatic trials are designed to determine the real-world outcomes of treatments, and in many cases, focus on verifying the effectiveness of popular clinical treatments or observing comparative effectiveness, rather than on the development or approval of new medical technologies. Therefore, in this study, we deemed that the pragmatic clinical trial model was appropriate.
In previous pragmatic RCTs, patients with chronic bothersome lower back pain were evaluated over 52 weeks while receiving maintenance care. The intervention group, which received regular maintenance care, showed a more stable pain trajectory than the control group, which only received intermittent care when the pain became severe, and reported fewer days with pain per week.48 These findings informed the design rationale for evaluating maintenance-oriented care within a pragmatic framework. Unlike this pragmatic RCT study, the control group in our study will receive education on lifestyle management and self-exercise, reflecting the general course of chronic bothersome neck pain, and serving as a comparator. Furthermore, this study will explore the continuous and preventive significance of CMT by comprehensively evaluating not only pain severity and the number of days with bothersome neck pain, but also function, recurrence rates, quality of life, and healthcare costs, to characterize outcomes relevant to long-term management in a pragmatic setting.
This study has a few limitations. First, as the study targets patients with chronic neck pain that causes mild discomfort, the degree of pain reduction may be smaller than that reported in studies that targeted patients with moderate neck pain. Furthermore, because the academic definition of the recurrence rate of chronic neck pain remains unclear, we operationally defined recurrence in the participants as an average pain NRS score of ≥6 over the past 2 weeks. In addition, while the follow-up duration is 26 weeks, longer-term follow-up (eg, 6 to 12 months) would better evaluate the durability of effects and potential maintenance benefits. Other design-related limitations of the study can be indirectly confirmed in the scores assigned to each area of the PRagmatic-Explanatory Continuum Indicator Summary 2 evaluation tool (Supplementary Material 3).
Conclusion
This study describes a pragmatic clinical trial protocol evaluating the effectiveness, safety, and cost-effectiveness of CMT in patients with chronic bothersome neck pain that disrupts daily life. The trial includes repeated assessments and objective clinical indicators during treatment and follow-up, and will also examine the healthcare utilization patterns over a chronic course (≥26 weeks). The findings are expected to inform clinical practice and future research on long-term, periodic, rehabilitative, and preventive use of CT.
Trial Status
Participant recruitment commenced in June 2024 and is expected to be completed by December 2025.
Data Sharing Statement
Data presented are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study protocol, CRF, ICF, and recruitment notices were submitted to the institutional review board (IRB) of each institution for approval (JASENG March 20; KOMCIRB May 13; KHNMCOH May 07; PNUKHIRB April 02, and has been approved by the IRBS of the respective participating institutions (approval nos. JASENG 2024-02-006, JASENG 2024-02-007, JASENG 2024-02-008, JASENG 2024-02-009, KOMCIRB 2024-03-004, KHNMCOH 2024-03-002-004, and PNUKHIRB 2024-03-007). Amendments to the study protocol, CRF, ICF, or recruitment notices will only be made with IRB approval, and all changes will be updated in the trial registries. All clinical researchers involved in this study will be trained on the Declaration of Helsinki, Korean Good Clinical Practice Guidelines, study protocol, and SOPs to ensure the protection of the study participants. Additionally, this protocol has been registered at ClinicalTrials.gov (NCT06591221) in the Clinical Research Information Service (KCT0009798).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: RS-2023-KH139336).
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the world population: a systematic critical review of the literature. Eur Spine J. 2006;15(6):834–12. doi:10.1007/s00586-004-0864-4
2. Manchikanti L, Singh V, Datta S, Cohen SP, Hirsch JA. Comprehensive review of epidemiology, scope, and impact of spinal pain. Pain Physician. 2009;12(4):E35–70. doi:10.36076/ppj.2009/12/E35
3. Childs JD, Cleland JA, Elliott JM, et al. Neck pain: clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopedic section of the American physical therapy association. J Orthop Sports Phys Ther. 2008;38(9):A1–a34. doi:10.2519/jospt.2008.0303
4. Irgens P, Myhrvold BL, Kongsted A, Natvig B, Vøllestad NK, Robinson HS. Exploring visual pain trajectories in neck pain patients, using clinical course, SMS-based patterns, and patient characteristics: a cohort study. Chiropractic Man Ther. 2022;30(1):37. doi:10.1186/s12998-022-00443-3
5. Nolet PS, Côté P, Kristman VL, Rezai M, Carroll LJ, Cassidy JD. Is neck pain associated with worse health-related quality of life 6 months later? A population-based cohort study. Spine J. 2015;15(4):675–684. doi:10.1016/j.spinee.2014.12.009
6. Shin B, Shin J, Lee J, Lim H. Chuna coordinative and orthopedic manual medicine. In: Seoul. Korea: Korean Society of Chuna Manual Medicine for Spine and Nerves; 2006:5–6.
7. Park J-M, Shin S-W, Park J-H. A comparative study on the concepts of the Chuna (推拿). J Korean Med Classics. 2008;21(2):173–191.
8. Moon TW, Choi TY, Park TY, Lee MS. Chuna therapy for musculoskeletal pain: a systematic review of randomized clinical trials in Korean literature. Chin J Integr Med. 2013;19(3):228–232. doi:10.1007/s11655-012-1238-0
9. Jung-Sik Park -H-HL, Lim -H-H. Analysis of Chuna manual therapy usage status after the application of Chuna manual therapy health insurance (2019-2021). J Korean Med Rehab. 2022;32(4):61–72. doi:10.18325/jkmr.2022.32.4.61
10. Gross A, Langevin P, Burnie SJ, et al. Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment. Cochrane Database Syst Rev. 2015;2015(9):Cd004249. doi:10.1002/14651858.CD004249.pub4
11. Lee J, Cho J-H, Kim K-W, et al. Chuna manual therapy vs usual care for patients with nonspecific chronic neck pain: a randomized clinical trial. JAMA Network Open. 2021;4(7):e2113757–e2113757. doi:10.1001/jamanetworkopen.2021.13757
12. Iben A, Lise H, Charlotte LY. Chiropractic maintenance care - what’s new? A systematic review of the literature. Chiropr Man Therap. 2019;27(1):63. doi:10.1186/s12998-019-0283-6
13. Axén I, Bodin L. The Nordic maintenance care program: the clinical use of identified indications for preventive care. Chiropr Man Therap. 2013;21(1):10. doi:10.1186/2045-709x-21-10
14. Bringsli M, Berntzen A, Olsen DB, Hestbæk L, Leboeuf-Yde C. The nordic maintenance care program: maintenance care - what happens during the consultation? Observations and patient questionnaires. Chiropr Man Therap. 2012;20(1):25. doi:10.1186/2045-709x-20-25
15. Eklund A, Jensen I, Lohela-Karlsson M, et al. The nordic maintenance care program: effectiveness of chiropractic maintenance care versus symptom-guided treatment for recurrent and persistent low back pain-A pragmatic randomized controlled trial. PLoS One. 2018;13(9):e0203029. doi:10.1371/journal.pone.0203029
16. Møller LT, Hansen M, Leboeuf-Yde C. The nordic maintenance care program--an interview study on the use of maintenance care in a selected group of Danish chiropractors. Chiropr Osteopat. 2009;17(1):5. doi:10.1186/1746-1340-17-5
17. Descarreaux M, Blouin JS, Drolet M, Papadimitriou S, Teasdale N. Efficacy of preventive spinal manipulation for chronic low-back pain and related disabilities: a preliminary study. J Manipulative Physiol Ther. 2004;27(8):509–514. doi:10.1016/j.jmpt.2004.08.003
18. Martel J, Dugas C, Dubois JD, Descarreaux M. A randomised controlled trial of preventive spinal manipulation with and without a home exercise program for patients with chronic neck pain. BMC Musculoskelet Disord. 2011;12(1):41. doi:10.1186/1471-2474-12-41
19. Kwon CY, Lee B, Lee BJ, Kim KI, Jung HJ. Comparative effectiveness of western and eastern manual therapies for chronic obstructive pulmonary disease: a systematic review and network meta-analysis. Healthcare. 2021;9(9). doi:10.3390/healthcare9091127
20. Gong W. Effects of cervical joint manipulation on joint position sense of normal adults. J Phys Ther Sci. 2013;25(6):721–723. doi:10.1589/jpts.25.721
21. Pickar JG. Neurophysiological effects of spinal manipulation. Spine J. 2002;2(5):357–371. doi:10.1016/S1529-9430(02)00400-X
22. Haavik H, Murphy B. The role of spinal manipulation in addressing disordered sensorimotor integration and altered motor control. J Electromyography Kinesiol. 2012;22(5):768–776. doi:10.1016/j.jelekin.2012.02.012
23. Dieleman JL, Cao J, Chapin A, et al. US health care spending by payer and health condition, 1996-2016. JAMA. 2020;323(9):863–884. doi:10.1001/jama.2020.0734
24. Safiri S, Kolahi -A-A, Hoy D, et al. Global, regional, and national burden of neck pain in the general population, 1990-2017: systematic analysis of the global burden of disease study 2017. BMJ. 2020;368. doi:10.1136/bmj.m791
25. Chan AW, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346(jan08 15):e7586. doi:10.1136/bmj.e7586
26. Jang G, Cho TY, Cha YY, et al. Techniques section. In: Cheon YH, editor. Chuna manual medicine. Korean Society of Chuna Manual Medicine for Spine and Nerves; 2022. 94–312.
27. Do HJ, Shin JS, Lee J, et al. Comparative effectiveness and economic evaluation of Chuna manual therapy for chronic neck pain: protocol for a multicenter randomized controlled trial. Trials. 2018;19(1):663. doi:10.1186/s13063-018-3016-6
28. Farrar JT, Young JP, LaMoreaux L, Werth JL, Poole MR. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/s0304-3959(01)00349-9
29. Vernon H, Mior S. The neck disability index: a study of reliability and validity. J Manipulative Physiol Ther. 1991;14(7):409–415.
30. Huskisson EC. Measurement of pain. Lancet. 1974;2(7889):1127–1131. doi:10.1016/s0140-6736(74)90884-8
31. Boonstra AM, Stewart RE, Köke AJ, et al. Cut-off points for mild, moderate, and severe pain on the numeric rating scale for pain in patients with chronic musculoskeletal pain: variability and influence of sex and catastrophizing. Frontiers in Psychology. 2016;7:1466. doi:10.3389/fpsyg.2016.01466
32. Scott W, McCracken LM. Patients’ impression of change following treatment for chronic pain: global, specific, a single dimension, or many? J Pain. 2015;16(6):518–526. doi:10.1016/j.jpain.2015.02.007
33. Devilly GJ, Borkovec TD. Psychometric properties of the credibility/expectancy questionnaire. J Behav Ther Exp Psychiatry. 2000;31(2):73–86. doi:10.1016/s0005-7916(00)00012-4
34. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727–1736. doi:10.1007/s11136-011-9903-x
35. Kim SH, Jo MW, Ahn J, et al. The valuation of EQ-5D-5L health states in Korea. Value Health. 2014;17(7):A753. doi:10.1016/j.jval.2014.08.211
36. Lee HJ, Jo MW, Choi SH, Kim YJ, Oh KW. Development and psychometric evaluation of measurement instrument for korean health-related quality of life. Public Health Weekly Report. 2014;9(24):447–454.
37. Gold MR. Cost-Effectiveness in Health and Medicine. Oxford university press; 1996.
38. Berger ML, Bingefors K, Hedblom EC, Pashos C, Torrance GW. Health Care Cost, Quality, and Outcomes: ISPOR Book of Terms. Lawrenceville NJ; 2003.
39. Rascati K. Essentials of pharmacoeconomics. Lippincott Williams & Wilkins; 2020.
40. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353–365. doi:10.2165/00019053-199304050-00006
41. Ha IH, Kim ES, Lee SH, et al. Cost-utility analysis of chuna manual therapy and usual care for chronic neck pain: a multicenter pragmatic randomized controlled trial. Front Med. 2022;9:896422. doi:10.3389/fmed.2022.896422
42. Kim BJ, Park AL, Hwang MS, et al. Comparative effectiveness and safety of concomitant treatment with Chuna manual therapy and usual care for whiplash injuries: a multicenter randomized controlled trial. Int J Environ Res Public Health. 2022;19(17). doi:10.3390/ijerph191710678
43. Kim D, Baek GG, Shin B-C. An umbrella review of systematic reviews for Chuna (or Tuina) manual therapy on musculoskeletal disorders. Perspect Integr Med. 2023;2(3):142–154. doi:10.56986/pim.2023.10.002
44. Mitchell M. Maintenance care: some considerations. Am Chiropr Assoc J Chiropractic. 1980;17:53–55.
45. Axén I, Jensen IB, Eklund A, et al. The nordic maintenance care program: when do chiropractors recommend secondary and tertiary preventive care for low back pain? Chiropr Osteopat. 2009;17(1):1. doi:10.1186/1746-1340-17-1
46. Myhrvold BL, Vøllestad NK, Irgens P, Robinson HS, Axén I. Clinical indicators for recommending continued care to patients with neck pain in chiropractic practice: a cohort study. Chiropr Man Therap. 2023;31(1):33. doi:10.1186/s12998-023-00507-y
47. Schwartz D, Lellouch J. Explanatory and pragmatic attitudes in therapeutical trials. J Clin Epidemiol. 2009;62(5):499–505. doi:10.1016/j.jclinepi.2009.01.012
48. Eklund A, Hagberg J, Jensen I, et al. The Nordic maintenance care program: maintenance care reduces the number of days with pain in acute episodes and increases the length of pain free periods for dysfunctional patients with recurrent and persistent low back pain - a secondary analysis of a pragmatic randomized controlled trial. Chiropr Man Therap. 2020;28(1):19. doi:10.1186/s12998-020-00309-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.