Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Motor Functional Characteristics in Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorders: A Systematic Review
Authors Takagi S ![]() , Hori H, Yamaguchi T
, Hori H, Yamaguchi T ![]() , Ochi S
, Ochi S ![]() , Nishida M
, Nishida M ![]() , Maruo T, Takahashi H
, Maruo T, Takahashi H
Received 7 April 2022
Accepted for publication 26 July 2022
Published 9 August 2022 Volume 2022:18 Pages 1679—1695
DOI https://doi.org/10.2147/NDT.S369845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Shunsuke Takagi,1 Hikaru Hori,2 Tatsuya Yamaguchi,3,4 Shinichiro Ochi,5 Masaki Nishida,6 Takashi Maruo,1 Hidehiko Takahashi1
1Department of Psychiatry and Behavioral Neurosciences, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, 113-8510, Japan; 2Department of Psychiatry, School of Medicine, Fukuoka University, Fukuoka, 814-0180, Japan; 3Institute for Integrated Sports Medicine, School of Medicine, Keio University, Shinjuku-ku, Tokyo, 160-8582, Japan; 4Department of Neuropsychiatry, Keio University School of Medicine, Shinjuku-ku, Tokyo, 160-8582, Japan; 5Department of Neuropsychiatry, Molecules and Function, Ehime University Graduate School of Medicine, Shitsukawa, Ehime, 791-0295, Japan; 6Faculty of Sport Science, Waseda University Tokorozawa, Saitama, 359-1192, Japan
Correspondence: Shunsuke Takagi, Department of Psychiatry and Behavioral Sciences, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, 1-5-45 Yushima, Bunkyo-ku, Tokyo, 113-8510, Japan, Tel +81-3-5803-5238, Fax +81-3-5803-0135, Email [email protected]
Background: The development of attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorders (ASDs) has various influences on physical abilities. Identification of specific physical abilities of people with ADHD/ASDs as biomarkers for diagnosing these conditions is necessary. Therefore, in the present review, we aimed firstly to extract the difference in physical abilities of people with ADHD or ASDs compared to those of normal individuals. Secondly, we aimed to extract the specific physical ability characteristics for identifying potential diagnostic biomarkers in people with ADHD/ASDs.
Methods: A systematic literature review was performed. The databases were searched for relevant articles on motor function deficits and characteristics of ADHD or ASD.
Results: Forty-one cross-sectional studies and three randomized controlled trials were identified, comprising 33 studies of ADHD, 10 studies of ASDs, and 1 study of both ADHD and ASDs. The quality of studies varied. Three types of physical activities/exercises were identified, including coordinated movement, resistance-type sports, and aerobic-type sports. People with ADHD/ASDs generally exhibited poorer physical abilities for all types of activities, possibly because of low levels of physical activity. Specifically, we found temporal discoordination of movement in ADHD and integration or synchronization of separate movements in ASDs.
Conclusion: Specific deficits in physical ability may be attributed to ADHD/ASDs. However, there is not enough research on the physical abilities of people with ADHD and ASDs to clarify the specific deficits. Investigation of specific motor functions that characterize ADHD/ASDs should be facilitated.
Keywords: motor function, neurodevelopmental disorders, sports, coordination, neural deficits
Corrigendum for this paper has been published.
Introduction
Neurodevelopmental disorders, such as attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorders (ASDs), are characterized by deficits in social communication and behavior that become increasingly apparent from childhood.1 ADHD and ASDs are the most frequent neurodevelopmental disorders that adversely affect people’s lives.2–4 ADHD is defined by contextual difficulties related to inattention, hyperactivity, and impulsivity.5 ADHD is a risk factor for adverse outcomes in later life, including poor educational attainment, social difficulties, substance misuse, and criminality.6,7 ASDs are a group of developmental disorders characterized by contextual difficulties in social communication and restricted repetitive sensory behaviors or interests.2 ADHD and ASDs can be huge obstacles to overcome. Owing to these characteristics, problems in social life, such as being subjected to bullying, have been observed in people with ADHD and ASDs since childhood.8
Attention should be paid to the physical abilities of people with these conditions, since the development of ADHD and ASDs has various influences on physical abilities. People with ADHD and ASDs might have biases in physical abilities in addition to cognitive and behavioral biases. Since ADHD/ASDs often occur with physical performance disorders, developmental coordination disorder (DCD) was recognized. Notably, former studies reported that a certain percentage of ADHD and ASDs are comorbid with such disorders.9–11 Physical abilities are frequently affected in children and adolescents suffering from psychiatric conditions.12,13 Many clinicians have reported that co-occurring deficits in physical abilities are very common in individuals with ADHD14,15 and ASDs.15–17 Some studies which included people with ADHD and ASDs have shown that poor motor skills were more frequent in people with poor cognitive skills.18–20 Abnormalities in the nervous system that have been reported2,12,13 in individuals with ADHD/ASDs might also affect their physical abilities. Particularly, structural and functional alteration of the cerebellum have been reported in people with ADHD and ASDs.21–23 Although the cerebellar deficits could explain part of motor dysfunctions in ADHD and ASDs, many dysfunctions remain unexplained. Further, a child’s development depends upon the continuous interaction of different functional areas related to motor, psychological, cognitive, linguistic, and social aspects. Therefore, physical activity plays an essential role in the normal development of these functional areas in children. Moreover, the experience of varied motor activities in childhood is essential to strengthen the foundations for other developmental domains.24 Motor impairments may limit the social opportunities for children with ADHD/ASDs and result in academic difficulties.15,25,26 Poor motor ability adversely impacts psychosocial and emotional functioning.26–31 These deep bidirectional relationships suggest that specific physical ability characteristics are associated with these conditions.
The diagnosis of neurodevelopmental disorders is predominantly based on symptoms, and the neural mechanisms underlying these disorders remain unclear. To date, effective biomarkers and specific tests for diagnosing these disorders are lacking. Although current symptom-based diagnostic criteria are reliable, developing clear and specific diagnostic methods is critical to facilitate accurate diagnosis and elucidate disease mechanisms. ADHD and ASDs are underscored by specific cognitive symptoms; hence, they may also be associated with specific motor functional characteristics with specific deficits associated with disease development and may therefore function as useful biomarkers or facilitate the development of accurate diagnostic tests. However, studies examining the specific motor functional characteristics in developmental disorders are scarce.
To the best of our knowledge, there is no systematic review identifying the specific physical abilities of people with ADHD or ASD as biomarkers for diagnosing these conditions. Further, the possibility that this research could lead to specific biomarkers or tests compelled us to perform a systematic review of motor functions in ADHD and ASDs. First, we systematically reviewed the physical abilities of people with ADHD or ASD compared to those of normal individuals. Subsequently, we attempted to find articles that examined the specific physical abilities of people with ADHD or ASD as candidates for diagnostic biomarkers.
Methods
Selection Procedures
This systematic review was conducted according to the preferred reporting items for systematic review and meta-analysis (PRISMA) guidelines32,(Supplementary Table 1). To account for features specific to observational studies, we also followed the meta-analyses of observational studies in epidemiology (MOOSE) guidelines33 (see Supplementary Table 2). We conducted the quality in prognosis studies (QUIPS) analysis to evaluate the risk of bias in the included studies.34 For QUIPS, two authors (S.T. and S.O.) independently evaluated the studies. Discrepancies between the authors were resolved through discussion until a consensus was reached. This systematic review was conducted in accordance with the international prospective register of systematic reviews (PROSPERO) guidelines. A protocol was developed and registered at the PROSPERO (registration number: CRD42020172568; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=172568).
Search Strategies
Literature searches were conducted on 1 December 2020 using Medline and PubMed, covering the period from 1 January 1970 to 31 December 2019. The search strategy was based on a combination of keywords and medical subject headings (MeSH) terms and included the following: [(“attention deficit hyperactivity disorder”[TIAB] OR “ADHD”[TIAB] OR “attention deficit disorder”[TIAB] OR “ADD”[TIAB] OR “attention deficit disorder with hyperactivity”[Mesh]) AND (“sports”[TIAB] OR “physical performance”[TIAB] OR “regulation of movement”[TIAB] OR “motor function”[TIAB] OR “Musculoskeletal Physiological Phenomena”[Mesh] OR “Sports”[Mesh] OR “motor skills”[TIAB])] for ADHD and [(“autism spectrum disorder”[TIAB] OR “ASD”[TIAB] OR “Asperger Syndrome”[TIAB] OR “Autistic Disorder”[TIAB] OR “Child development disorder, Pervasive”[Mesh]) AND (“sports”[TIAB] OR “physical performance”[TIAB] OR “regulation of movement”[TIAB] OR “motor function”[TIAB] OR “Musculoskeletal Physiological Phenomena”[Mesh] OR “Sports”[Mesh] OR “motor skills”[TIAB])] for ASD (see Supplemental Methods). The search was restricted to English articles and human studies. Additional studies were identified by cross-referencing the included studies and previous reviews.
Selection Criteria
Studies that met all the following criteria were included: a) available in English; b) included inpatients or outpatients with a Diagnostic and Statistical Manual of Mental Disorders (DSM) or International Classification of Diseases (ICD) diagnosis of ADHD, ASD, or related developmental disorder. Any version of DSM and ICD was acceptable; c) an observational study (cohort studies, case-control studies, and cross-sectional studies) or a clinical trial reporting a baseline measurement; and d) reported ability to perform physical exercise or sports. Studies that met any of the following criteria were excluded: a) meta-analyses, reviews, case reports, and posters; b) reported populations with other diagnoses; and c) articles with overlapping datasets (only the more relevant article was retained). The reasons for exclusion were reported. Two groups of authors (group A: S.T., H.H., and T.Y. and group B: S.O., M.N., and A.M.) independently applied the inclusion criteria to the identified studies. Discrepancies between the groups were resolved through discussion until consensus was reached.
Data Extraction
To achieve a high standard of reporting and to assess study comparability, we performed a full-text review with a detailed analysis of each included study. Two groups independently performed data extraction. Discrepancies between the two groups were resolved using a joint full-text analysis conducted by another author (H.T.). For the outcomes, physical performance data were extracted.
Results
Literature Search
Following a careful assessment of the identified publications in accordance with our inclusion and exclusion criteria, 34 studies were included in the analyses for ADHD (Figure 1) and 11 studies were included in the analyses for ASDs (Figure 1). In total, 41 cross-sectional studies and 3 randomized controlled trials (RCTs) were included in the analyses—33 for ADHD, 10 for ASDs, and 1 for both ADHD and ASDs, since the study by Classen et al35 included both ADHD and ASD (Table 1).
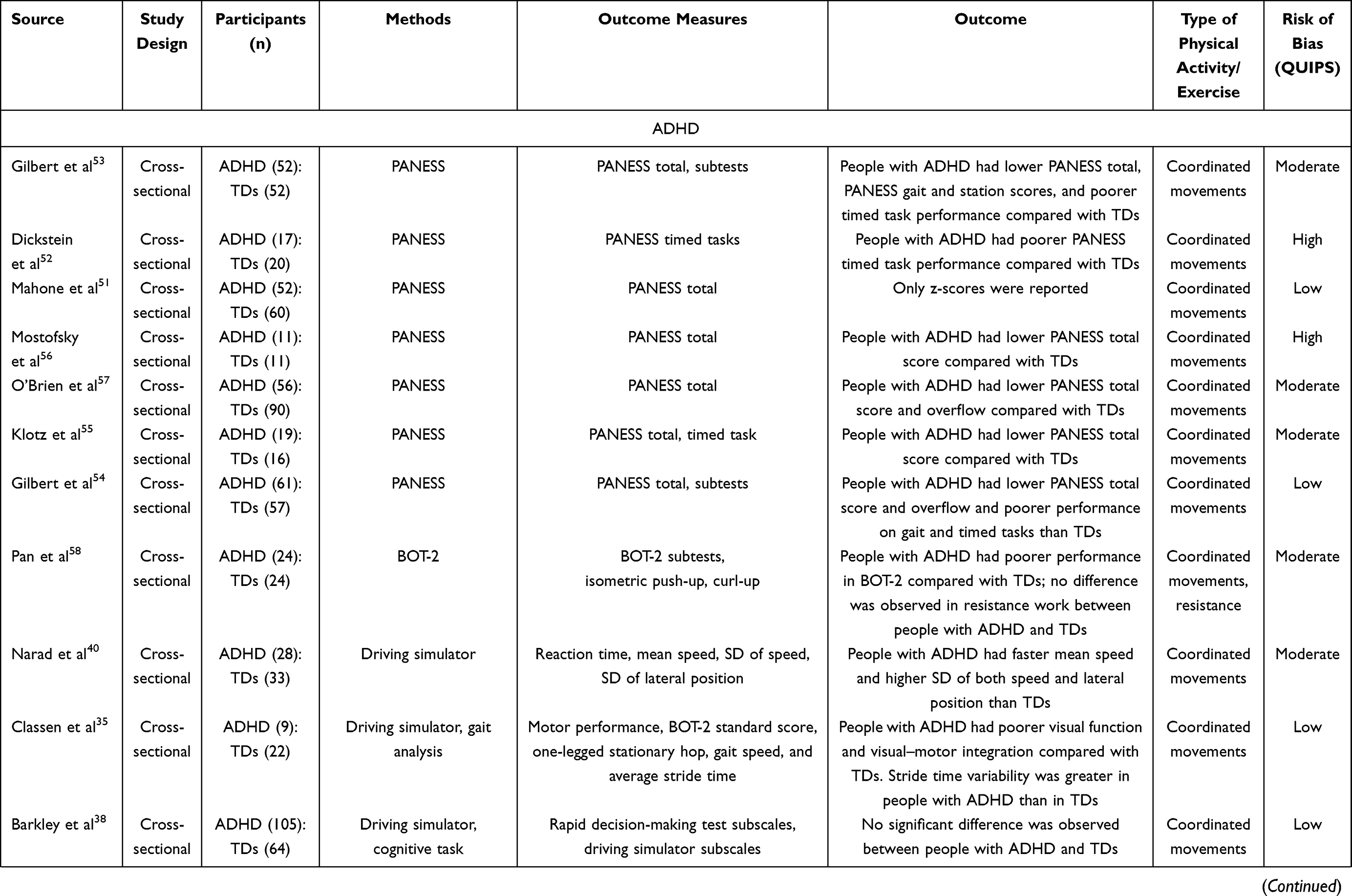 | 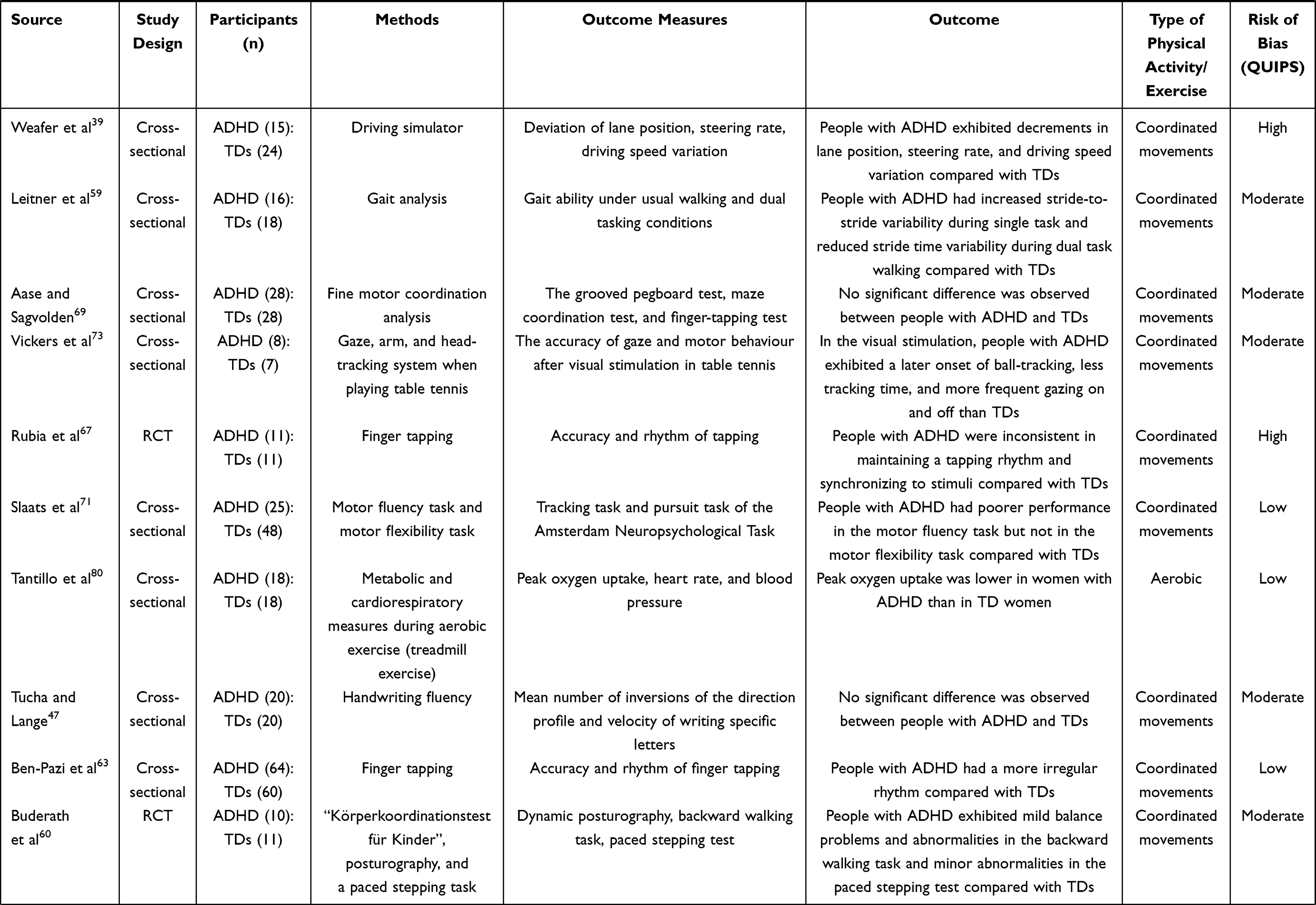 | 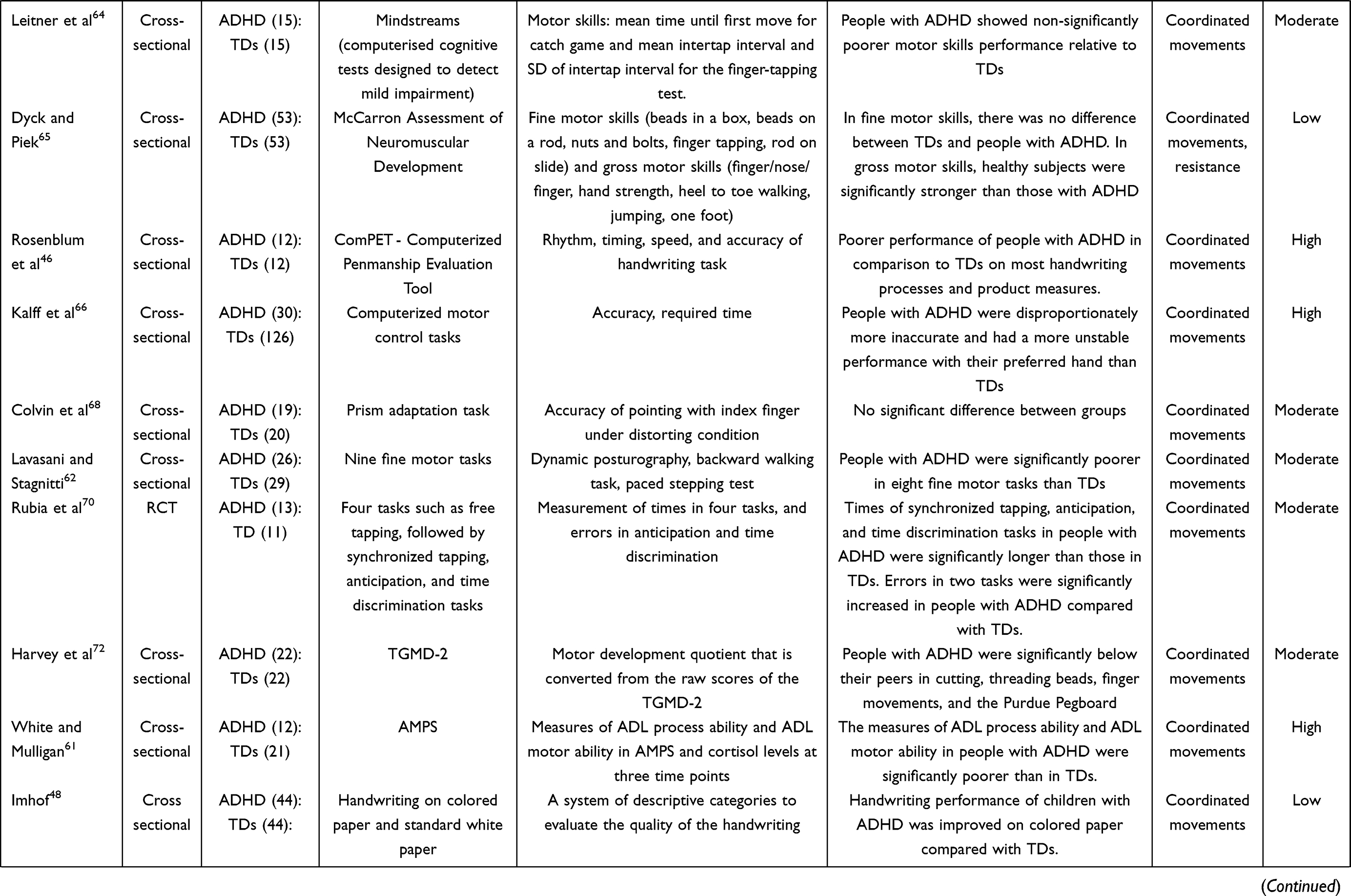 | 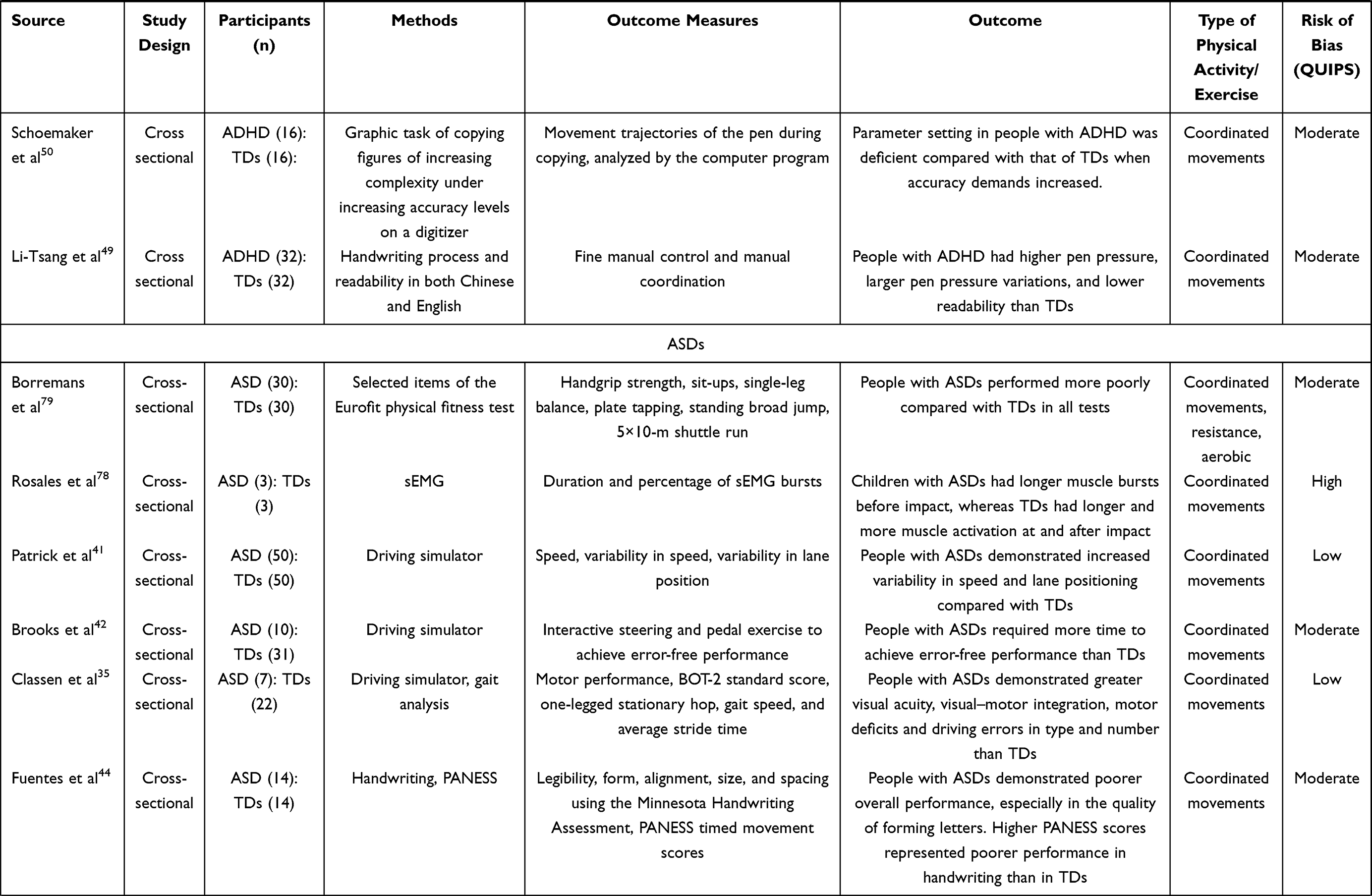 |
Table 1 Characteristics of Studies on the Physical Abilities of People with Attention-Deficit/Hyperactivity Disorder (ADHD)/Autism Spectrum Disorders (ASDs) That Met the Inclusion Criteria |
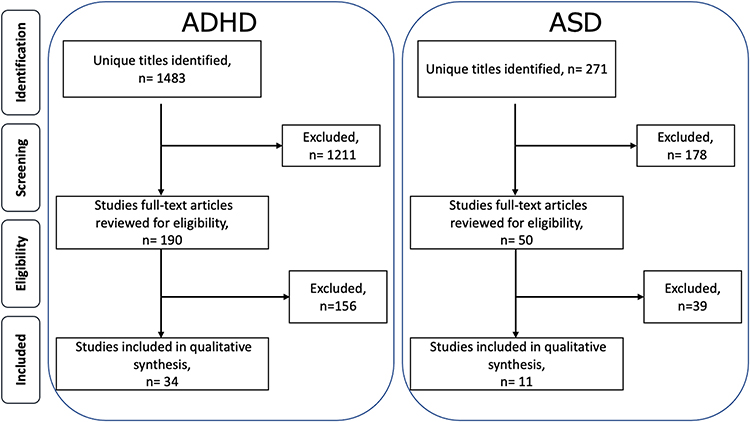 |
Figure 1 Preferred reporting items for systematic review and meta-analysis flow diagram for study inclusion and exclusion. Abbreviations: ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder. |
The quality of studies (assessed using the QUIPS tool) was considered to vary from a low to high risk of bias. The high risk of bias was predominantly due to the lack of consideration of confounding factors (Supplementary Table 3). Since a wide range of methodologies was adopted to assess physical abilities, we performed a qualitative evaluation without meta-analysis. Analysis of the types of physical activities/exercises revealed three different types: coordinated movements, resistance-type sports, and aerobic-type sports. We defined these three types according to previous reports.36,37 Resistance-type sports were defined as physical activities that required maximum muscle power. Aerobic-type sports were defined as physical activities that elevated the cardiorespiratory response without maximum muscle power. Coordinated movements were defined as movements that involved technique, skill, balance, or timing.
Coordinated Movements
Studies investigating coordinated movements in people with ADHD/ASDs comprised studies on driving skills, handwriting, physical and neurological examination for soft signs (PANESS), and other coordinated movements. The studied movements varied widely and were included in many studies.
Driving Skills
Four simulated driving studies comparing driving skills between people with ADHD and typically developed individuals (TDs) were identified,35,38–40 but their results varied. Classen et al, Weafer et al, and Narad et al reported that people with ADHD exhibited impaired driving performance compared with TDs in a driving simulator.35,39,40 However, a large cohort study by Barkley et al did not observe any significant difference between people with ADHD and TDs.38 These studies predominantly evaluated driving techniques and reported general driving skill deficits but did not identify any disease-specific features. Three simulated driving studies comparing driving skills between individuals with ASDs and TDs were identified.35,41,42 One study reported significantly unstable driving skills in people with ASDs, including steering misses and speed variability, which contributed to collisions.41
Handwriting
The literature search identified two studies that evaluated handwriting impairments in people with ADHD and two in people with ASDs.43–45 Rosenblum et al found that individuals with ADHD had poorer handwriting performance compared to TDs.46 However, Tucha and Lange investigated handwriting fluency associated with attentional control but did not identify any evidence of handwriting deficits in the ADHD group.47 Imhof showed that the handwriting performance of individuals with ADHD was better on improved on colored paper than TDs.48 Li-Tsang et al assessed the handwriting process and readability in both Chinese and English. They found that individuals with ADHD had higher pen pressure, larger pen pressure variations, and lower readability than TDs.49 Schoemaker et al assessed the graphic task of copying figures of increasing complexity with increasing accuracy on a digitizer. They found that individuals with ADHD performed worse than TDs when accuracy demands increased.50 One case-control study compared children with ASDs with TDs,44 and another compared adolescents with ASDs with TDs.45 In both studies, the total score and subcategory scores in the Minnesota Handwriting Assessment were significantly lower in the ASD group than in the control group.44,45
PANESS
The revised PANESS is a screening tool for fine and gross motor function in children. The PANESS assesses gait, balance, aim, and the presence of “soft neurological signs.” Overflow movements from one body part to another during timed, rapid, repetitive motor tasks, and lack of persistence during stressed gait and oral motor tasks are classified as “soft neurological signs.”51
The literature search identified seven studies that used the PANESS in people with ADHD and two in people with ASDs. Seven studies evaluated motor skills in people with ADHD and TDs using the PANESS.51–57 Pan et al used a similar assessment tool for psychomotor development (Bruininks-Oseretsky Test of Motor Proficiency Second Edition [BOT-2]).58 The majority of these studies reported that PANESS total scores were significantly lower in the ADHD group than in the TD group. Since the results of the subtests were generally poorer in the ADHD group, disease-specific features could not be identified.
Fuentes et al compared motor skills between TDs and children44 or adolescents with ASDs45 using the PANESS and reported that PANESS total scores were significantly lower in the ASD group than in the TD group. Additionally, PANESS subtest scores for overflow movements, gait/balance, and timed movements were significantly lower in the ASD group than in the TD group.44,45
Other Coordinated Movements
Several other assessments have been employed to investigate coordinated movements in people with ADHD. Several studies examined gait under variable conditions.59–62 The results were varied, ranging from no difference compared with TDs to mild deficits under task conditions. Tasks related to finger tapping were used in some studies to assess rhythmic movement, accuracy, and synchronization.63–71 The results of finger tapping studies were also varied, ranging from no difference to mild deficits when compared with TDs. Ben-Pazi et al and Kalff et al reported rhythmic motor abnormalities and inaccuracy in people with ADHD.63,66 Rubia et al reported abnormalities in synchronization, anticipation, and time discrimination in people with ADHD.67 In a study by Aase and Sagvolden, the grooved pegboard test was used in addition to finger tapping; however, no significant differences in test results were observed between children with ADHD and TDs.69 In contrast, Harvey et al found that people with ADHD were less skilled in all fine motor tests than TDs in the pegboard test.72 Slaats et al investigated tracking and pursuit tasks using the finger to assess motor fluency.71 The results indicated that people with ADHD had significantly poorer performance for motor fluency and a high level of movement flexibility than TDs.71
Vickers et al employed modified table tennis to examine the accuracy of gaze and motor behavior after visual stimulation in people with ADHD.73 Compared with the control group, the ADHD group demonstrated lower accuracy in the pre- and early-cues. In the pre-cue condition, the target to smash was indicated 2 s before the opponent’s starting serve. In the early-cue condition, the target was indicated 350 ms after the serve. The ADHD group exhibited a later onset of ball-tracking, lesser tracking time, and more frequent gazing toward and away from the ball and cue than the control group. When examining motor behavior, they found that the onset time and velocity of arm movements in the pre-cue condition were slower in the ADHD group than in the control group. These results suggest that the people with ADHD could process short duration information, but long duration information contributed to irregular movement control, which adversely impacted motor behavior.73 Pan et al conducted an RCT that included an ADHD training group, ADHD non-training groups, and TD group to evaluate the effects of an exercise intervention combined with a 12-week simulated developmental horse-riding program and fitness training in children with ADHD.58 The results of standardized tests of motor skill and physical fitness revealed significant improvements in motor proficiency, cardiovascular fitness, and flexibility in the ADHD training group after the 12-week intervention. These results suggest that evidence-based exercise interventions reduce the gap in motor skills and physical fitness levels between children with and without ADHD.58 Based on these findings, especially those of Vickers et al73 and Rubia et al,70 temporal–motor discoordination may be a specific deficit in physical abilities in people with ADHD.
Several other assessments have also been used to investigate coordinated movements in people with ASDs. Esposito and Venuti assessed independent walking gait in people with ASDs and TDs using the walking observation scale.74 Significant differences were observed in the results of the walking observation scale between children with ASDs and TDs.74 David et al compared the temporal coordination of precision grip between people with ASDs and TDs. They reported that grip-to-load force onset latencies and grip forces at the onset of load forces differed significantly between people with ASDs and TDs and that people with ASDs displayed temporal discoordination between grip and load forces.75 de Moraes et al compared the timing errors, ie, temporal interval between the visual stimulus and the end of participants’ motor response in people with ASDs and TDs in virtual and real situations. People with ASDs exhibited more errors in the virtual task and better performance in the real task than TDs.76
Glazebrook et al performed a comparative study of manual aiming movements in people with ASDs and TDs by investigating how people with ASDs used vision and proprioception to land successfully on one of two targets. People with ASDs took longer to plan and execute manual reaching movements and perform movements that required greater visual–proprioceptive integration.77 Rosales et al performed leg surface electromyography (sEMG) in individuals with ASDs and TDs.78 The study procedure was as follows: people with ASDs hung from a vertical bar, landed, and reacted to a light cue that signaled the child to run to the right or left or to stay in place. Notably, children with ASDs exhibited more frequent and longer bursts of muscle activation during pre-impact.78 Further, Borremans et al compared people with ASDs and TDs using the single-leg balance and plate-tapping tests and reported significantly poorer performance in people with ASDs than in TDs.79 Collectively, these results indicate that the integration or synchronization of separate movements may reflect deficits in physical abilities in people with ASDs.
Resistance-Type Sports
We found few studies regarding resistance-type sports in people with ADHD/ASDs, which reflected their sedentary lifestyle. In a study by Pan et al, children with ADHD and TDs were assessed using isometric push-up and curl-up tests. The performance of children in the ADHD group was significantly poorer than that of the TD group for both physical measurement items (isometric push-up test: 33.84 s vs 39.25 s; curl-up test: 4.51 vs 6.04).58 Dyck and Piek showed that gross motor skills including hand strength are weaker in individuals with ADHD than in TDs.65 Borremans et al investigated selected items of the European test of physical fitness in young adults with ASDs and TDs.79 For resistance-type physical performance, handgrip strength, sit-ups, and standing broad jumps were assessed. Performance on all items was significantly poorer in young adults with ASDs than in TDs.79 Overall, these results indicated that individuals with ASDs had poor strength and coordination and those with ADHD had poor strength in resistance-type sports.
Aerobic-Type Sports
We found few studies where aerobic-type sports were assessed in people with ADHD/ASDs and those reflected their sedentary lifestyle. A study on aerobic-type sports by Tantillo et al examined people with ADHD and TDs using metabolic and cardiorespiratory measures during aerobic exercise (treadmill exercise).80 Peak oxygen uptake was measured using an automated open-circuit spirometry system in addition to post-exercise measurements of heart rate and blood pressure. Peak oxygen uptake was lower in girls with ADHD than in TDs, but no other major differences were noted between the groups.80 Borremans et al investigated selected items of the European test of physical fitness in young adults with ASDs and TDs.79 For aerobic-type physical performance, a 5×10-m shuttle run, 2-km walking test, and heart rate at the end of the walking test were assessed. Performance on all items was significantly poorer in young adults with ASDs than in TDs.79 Overall, these results indicated that people with ADHD/ASDs performed poorly in aerobic-type sports.
Discussion
This systematic review analyzed motor function in people with ADHD and ASDs. The available evidence in the literature was summarized to establish the strength of the analysis of motor function in people with ADHD and ASDs. We found that physical ability studied in literature can be divided into three types, viz., coordinated movements, resistance-type exercises, and aerobic-type exercises. The majority of studies reported that the motor performance of people with ADHD/ASDs was poorer than that of TDs. Studies of resistance-type and aerobic-type sports were few and appeared to reflect the sedentary lifestyle of people with ADHD/ASDs. Most studies of coordinated movements showed general deficits in movement in people with ADHD/ASDs. In some studies of coordinated movements, we identified potential features of motor function that were specific to ADHD/ASDs.
Our review identified studies about coordinated movement motor functional characteristics in people with ADHD/ASDs among many kinds of studies on motor function. Studies using screening tools for motor symptoms, such as the PANESS, account for some part of our study. In many of these studies, motor functional characteristics were found to be significantly different between people with ADHD/ASDs and TDs. Therefore, only global deficits were found, and specific characteristics of people with ADHD/ASDs could not be delineated by these studies. Other studies employed simple movement tests such as driving performance, gait, and finger tapping. With these simple movement tests, studies could depict the accuracy or timing errors among people with ADHD/ASDs. However, detailed specific neurological deficits were not well studied. Several studies attempted to clarify characteristics in people with ADHD/ASDs using motion capture such as eye-tracking devices.43,53 Nevertheless, there is a paucity of studies using such approaches, and the sample sizes were small. Accordingly, future research employing these methods is warranted to clarify the specific motor functional characteristics of people with ADHD/ASDs.
In this review, apparent deficits in specific physical abilities, which were consistently reported across many studies, were not conclusively identified. Based on a few reports using random assessments, the current findings suggested the integration or synchronization of separate movements in people with ASDs and temporal discoordination of movements in people with ADHD. These deficits were associated with the core symptoms of ADHD/ASDs and may therefore reflect specific deficits in physical abilities in people with ADHD/ASDs. People with ADHD/ASDs exhibited poorer performance in resistance- and aerobic-type sports than TDs. However, these results may have reflected inactivity or a lack of exercise in daily life and may not represent the characteristics of neurodevelopmental disorders. We did not include these deficits as specific characteristics of ADHD/ASDs. Indeed, previous studies that assessed and examined activities of daily living reported that people with ADHD/ASDs had significantly lower levels of physical activity and motor functioning than TDs,81–85 which is further supported by the findings of the current systematic review. Only part of the study by de Moraes et al76 showed better results by people with ASDs than TDs. The found that people with ASDs had more errors in the virtual task. However, they had better performance in the subsequent real task. Thus, people with ASDs might be better at transferring practice from a virtual to a real environment than TDs. At the very least, this result does not support baseline motor deficits of people with ASDs.
In this systematic review, we divided physical activity into three types: resistance-type, aerobic-type, and coordinative. Resistance-type categorizes the physical ability which is measured by maximum strength. Aerobic-type categorizes the physical ability which is measured by endurance capacity. And coordinative categorizes the other physical ability which is skillful, accurate or complex type. Specific physical abilities of people with ADHD/ASDs were included under coordinative-type sports for the following reasons: The items for evaluating the motor component of voluntary movements are classified into externally triggered and self-paced movements. The components of motion include reaction time to stimulus input, temporal accuracy such as spatial accuracy and timing of movement output, and complex movements including executive function.86–89 The latency from the presentation of an external stimulus to movement is measured by the reaction time. In a study that assessed the correlation between reaction time and regional cerebral blood flow during a simple response task in normal human participants, a significant increase in blood flow was observed in the anterior cingulate gyrus as the reaction speed increased in auditory, somatosensory, and visual sensory modalities.90 The anterior cingulate cortex communicates bidirectionally with the primary motor cortex, premotor cortex, and supplementary motor cortex. Further, blood flow in the anterior cingulate cortex is strongly correlated with that in the thalamus, a region associated with attention, arousal, and motivation.91
ADHD symptoms are underpinned by cognitive deficits in attention and executive functioning, which manifest due to prefrontal cortex dysfunction. A meta-analysis of imaging studies of executive functioning and timing tasks reported frontal–striatal, frontal–parietal, and frontal–cerebellar dysfunction in people with ADHD. The ventral striatum in people with ADHD is reportedly inactive during low reward in a monetary reward task.92 Moreover, resting-state functional magnetic resonance imaging (fMRI) revealed reduced functional connectivity in the default mode network, abnormal interactions between the frontoparietal and attention networks, and abnormalities in networks related to the reward system.93 Based on the studies included in this review, especially those of Vickers et al73 and Rubia et al,70 temporal–motor discoordination may be a specific deficit in physical abilities in people with ADHD. Temporal–motor coordination is related to prefrontal cortex function.94 These findings indicate that ADHD is characterized by impaired prefrontal cortex functioning, which may lead to increased impulsive behavior and inability to control emotions and attention; impaired delayed gratification, which leads to impulsive behavior and prioritization of immediate rewards over future rewards; and impaired cerebellar functioning, which leads to symptoms such as impaired time intervals and timing.
In people with ASDs, visuospatial cognition is superior to verbal processing,95 and executive performance is lower than that in controls because of retention responses and adherence to regularity.91 In particular, the performance of people with Asperger’s syndrome is poorer in terms of non-verbal learning skills, such as fine and gross motor skills, compared to people with autism.96 Consistent with these findings, an fMRI study in people with ASDs revealed a right hemisphere-dominant decrease in superior temporal gyrus and inferior frontal gyrus activity and reduced bilateral middle temporal gyrus activity during language comprehension and speech compared with TDs.97 Another fMRI study reported that individuals with ASDs demonstrated stronger effects in the inferior parietal lobule and altered effects in the occipital lobe, dorsolateral prefrontal cortex, cingulate cortex, and insula when watching or imitating the actions of others.98 These alterations in brain activity may reflect specific characteristics of motor function in people with ASDs.
In summary, characteristics of ADHD and ASDs, such as attentional and executive dysfunction and visual cognitive impairments, are likely to affect fine motor movements. In this review, 20 studies on ADHD and 11 studies on ASDs included fine motor movements, cognitive function, and motor components as outcomes. Furthermore, functional imaging studies have demonstrated that cerebral blood flow increases in the contralateral dorsal premotor cortex and superior parietal lobule during fine motor movements, which include elements such as selection, compared with that during gross motor movements.99 In light of these findings, future research should focus on fine motor and cognitive aspects, including attention, visuoperceptual function, and executive function tests, as assessment items for motor performance.
This systematic review has several limitations. First, this review focused only on literature in English. Given the lack of evidence, additional literature searches in other languages are warranted. Second, the measured outcomes and assessment tools used in the studies included herein were diverse, which precluded direct comparisons among studies using meta-analytical techniques. The assessment methods we reviewed have further problems. Driving and writing skills are assessments that require some cognitive functions (eg, attention, working memory) and so may not directly evaluate motor function. Third, many of the studies included in this review had small sample sizes, which were subject to bias. Since no sample size or power calculations were performed in any of the studies, several studies may have been underpowered, thereby obscuring the detection of relevant differences. Moreover, the sample sizes of the studies varied considerably. Additionally, the relationship between this review’s main questions and historically recognized disorders related to ADHD/ASDs is difficult to determine. Historically recognized disorders like DCD or deficits in attention, motor control and perception (DAMP) were disorders containing movement deficits related to ADHD/ASDs. We investigated the specific physical ability characteristics of people with ADHD/ASDs which can eventually become a biomarker. DCD and DAMP were disorders which were thought to exist be prevalent in people with ADHD/ASDs. But these are not the concepts of the tendency which affects the total ADHD/ASDs entity that interest us. However, they could have affected our results because of their high occurrence in ADHD/ASDs. Finally, significant heterogeneity in the study populations and inclusion and exclusion criteria was observed among studies, which prevented direct comparisons.
In conclusion, we systematically reviewed motor performance and functioning in people with ADHD/ASDs. We did not identify specific motor functional characteristics of people with ADHD/ASDs based on the available literature. The motor performance of people with ADHD/ASDs was generally poorer than that of TDs across multiple domains. While movement disorders such as DCD or DAMP do somewhat relationship in terms of concept with ADHD/ASDs, how to differentiate these conditions is still under debate since the diagnostic classification has not been fully established. Our findings suggest that the integration or synchronization of separate movements in people with ASDs and temporal discoordination of movements in people with ADHD may reflect specific deficits in physical abilities. These deficits in people with ASDs may reflect specific characteristics of motor function in this population. Regarding ADHD, because temporal-motor coordination is related to prefrontal cortex function, which is charactery impaired in ADHD, this finding is interesting in understanding physical ability of people with ADHD and might have a relationship with ADHD’s core symptoms like impulsiveness. Future studies should further characterize motor functioning and performance in people with ADHD/ASDs to address these issues. Using objective assessments and apparatus, such as accelerometers, should facilitate more precise diagnosis and elucidate the pathophysiology of ADHD/ASDs.
Abbreviations
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; BOT-2, Bruininks-Oseretsky Test of Motor Proficiency Second Edition; DAMP, Deficits in Attention, Motor control and Perception; DCD, Developmental coordination disorder; DSM, Diagnostic and Statistical Manual of Mental Disorders; fMRI, functional magnetic resonance imaging; ICD, International Classification of Diseases; MeSH, medical subject headings; MOOSE, Meta-analyses of observational studies in epidemiology; PANESS, physical and neurological examination for soft signs; PRISMA, Preferred reporting items for systematic review and meta-analysis; QUIPS, quality in prognosis studies; RCT, randomized controlled trial; sEMG, surface electromyography; TDs, typically developed individuals.
Acknowledgments
We thank Ryuhei So for providing valuable advice. We thank for the support by the Japanese Association of Sports Psychiatry (JASP), JSPS KAKENHI Grant Number 20K16643, and AMED under Grant Number 20dm0307105h0002.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Japanese Association of Sports Psychiatry (JASP), JSPS KAKENHI Grant Number 20K16643, and AMED under Grant Number 20dm0307105h0002. The funding sources did not have any involvement to study contents.
Disclosure
S.T. received funding from the Japanese Association of Sports Psychiatry (JASP) for availing English editing service. Dr Shinichiro Ochi reports personal fees from Dainippon Sumitomo Pharma Co. Ltd., personal fees from Meiji Seika Pharma Co. Ltd., personal fees from Otsuka Pharmaceutical Co. Ltd., personal fees from Kowa Company, Ltd., outside the submitted work. The authors have no other competing interests to declare.
References
1. Thapar A, Cooper M, Rutter M. Neurodevelopmental disorders. Lancet Psychiatry. 2017;4(4):339–346. doi:10.1016/S2215-0366(16)30376-5
2. Lord C, Elsabbagh M, Baird G, Veenstra-Vanderweele J. Autism spectrum disorder. Lancet. 2018;392(10146):508–520. doi:10.1016/S0140-6736(18)31129-2
3. Baxter AJ, Brugha TS, Erskine HE, Scheurer RW, Vos T, Scott JG. The epidemiology and global burden of autism spectrum disorders. Psychol Med. 2015;45(3):601–613. doi:10.1017/S003329171400172X
4. Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: a meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry. 2015;56(3):345–365. doi:10.1111/jcpp.12381
5. Thapar A, Cooper M. Attention deficit hyperactivity disorder. Lancet. 2016;387(10024):1240–1250. doi:10.1016/S0140-6736(15)00238-X
6. Faraone SV, Asherson P, Banaschewski T, et al. Attention-deficit/hyperactivity disorder. Nat Rev Dis Primers. 2015;1:15020.
7. Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med. 2006;36(2):159–165. doi:10.1017/S003329170500471X
8. Ochi M, Kawabe K, Ochi S, Miyama T, Horiuchi F, Ueno SI. School refusal and bullying in children with autism spectrum disorder. Child Adolesc Psychiatry Ment Health. 2020;14:17. doi:10.1186/s13034-020-00325-7
9. Gillberg C. Deficits in attention, motor control, and perception: a brief review. Arch Dis Child. 2003;88(10):904–910. doi:10.1136/adc.88.10.904
10. Gillberg C, Kadesjo B. Why bother about clumsiness? The implications of having developmental coordination disorder (DCD). Neural Plast. 2003;10(1–2):59–68. doi:10.1155/NP.2003.59
11. Landgren M, Kjellman B, Gillberg C. Deficits in attention, motor control and perception (DAMP): a simplified school entry examination. Acta Paediatr. 2000;89(3):302–309. doi:10.1111/j.1651-2227.2000.tb01332.x
12. Emck C, Bosscher R, Beek P, Doreleijers T. Gross motor performance and self-perceived motor competence in children with emotional, behavioural, and pervasive developmental disorders: a review. Dev Med Child Neurol. 2009;51(7):501–517. doi:10.1111/j.1469-8749.2009.03337.x
13. Emck C, Bosscher RJ, Van Wieringen PC, Doreleijers T, Beek PJ. Gross motor performance and physical fitness in children with psychiatric disorders. Dev Med Child Neurol. 2011;53(2):150–155. doi:10.1111/j.1469-8749.2010.03806.x
14. Mavrides N. Attention-deficit hyperactivity disorder: a handbook for diagnosis and treatment, 4th edition. J Nerv Ment Dis. 2016;204(1):66. doi:10.1097/NMD.0000000000000412
15. Dewey D, Kaplan BJ, Crawford SG, Wilson BN. Developmental coordination disorder: associated problems in attention, learning, and psychosocial adjustment. Hum Mov Sci. 2002;21(5–6):905–918. doi:10.1016/S0167-9457(02)00163-X
16. Hilton CL, Zhang Y, Whilte MR, Klohr CL, Constantino J. Motor impairment in sibling pairs concordant and discordant for autism spectrum disorders. Autism. 2012;16(4):430–441. doi:10.1177/1362361311423018
17. Lane A, Harpster K, Heathcock J. Motor characteristics of young children referred for possible autism spectrum disorder. Pediatr Phys Ther. 2012;24(1):21–29. doi:10.1097/PEP.0b013e31823e071a
18. Mandelbaum DE, Stevens M, Rosenberg E, et al. Sensorimotor performance in school-age children with autism, developmental language disorder, or low IQ. Dev Med Child Neurol. 2006;48(1):33–39. doi:10.1017/S0012162206000089
19. Green D, Charman T, Pickles A, et al. Impairment in movement skills of children with autistic spectrum disorders. Dev Med Child Neurol. 2009;51(4):311–316. doi:10.1111/j.1469-8749.2008.03242.x
20. Staples KL, Reid G. Fundamental movement skills and autism spectrum disorders. J Autism Dev Disord. 2010;40(2):209–217. doi:10.1007/s10803-009-0854-9
21. Allen G, Muller RA, Courchesne E. Cerebellar function in autism: functional magnetic resonance image activation during a simple motor task. Biol Psychiatry. 2004;56(4):269–278. doi:10.1016/j.biopsych.2004.06.005
22. Wegiel J, Flory M, Kuchna I, et al. Stereological study of the neuronal number and volume of 38 brain subdivisions of subjects diagnosed with autism reveals significant alterations restricted to the striatum, amygdala and cerebellum. Acta Neuropathol Commun. 2014;2:141. doi:10.1186/s40478-014-0141-7
23. Stoodley CJ. The Cerebellum and Neurodevelopmental Disorders. Cerebellum. 2016;15(1):34–37. doi:10.1007/s12311-015-0715-3
24. Damme TV, Simons J, Sabbe B, van West D. Motor abilities of children and adolescents with a psychiatric condition: a systematic literature review. World J Psychiatry. 2015;5(3):315–329. doi:10.5498/wjp.v5.i3.315
25. Losse A, Henderson SE, Elliman D, Hall D, Knight E, Jongmans M. Clumsiness in children–do they grow out of it? A 10-year follow-up study. Dev Med Child Neurol. 1991;33(1):55–68. doi:10.1111/j.1469-8749.1991.tb14785.x
26. Tseng MH, Howe TH, Chuang IC, Hsieh CL. Cooccurrence of problems in activity level, attention, psychosocial adjustment, reading and writing in children with developmental coordination disorder. Int J Rehabil Res. 2007;30(4):327–332. doi:10.1097/MRR.0b013e3282f144c7
27. Piek JP, Rigoli D, Pearsall-Jones JG, et al. Depressive symptomatology in child and adolescent twins with attention-deficit hyperactivity disorder and/or developmental coordination disorder. Twin Res Hum Genet. 2007;10(4):587–596. doi:10.1375/twin.10.4.587
28. Sigurdsson E, Van Os J, Fombonne E. Are impaired childhood motor skills a risk factor for adolescent anxiety? Results from the 1958 U.K. birth cohort and the National Child Development Study. Am J Psychiatry. 2002;159(6):1044–1046. doi:10.1176/appi.ajp.159.6.1044
29. Lingam R, Jongmans MJ, Ellis M, Hunt LP, Golding J, Emond A. Mental health difficulties in children with developmental coordination disorder. Pediatrics. 2012;129(4):e882–891. doi:10.1542/peds.2011-1556
30. Pearsall-Jones JG, Piek JP, Rigoli D, Martin NC, Levy F. Motor disorder and anxious and depressive symptomatology: a monozygotic co-twin control approach. Res Dev Disabil. 2011;32(4):1245–1252. doi:10.1016/j.ridd.2011.01.042
31. Skinner RA, Piek JP. Psychosocial implications of poor motor coordination in children and adolescents. Hum Mov Sci. 2001;20(1–2):73–94. doi:10.1016/S0167-9457(01)00029-X
32. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336–341. doi:10.1016/j.ijsu.2010.02.007
33. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283(15):2008–2012. doi:10.1001/jama.283.15.2008
34. Hayden JA, van der Windt DA, Cartwright JL, Cote P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013;158(4):280–286. doi:10.7326/0003-4819-158-4-201302190-00009
35. Classen S, Monahan M, Brown KE, Hernandez S. Driving indicators in teens with attention deficit hyperactivity and/or autism spectrum disorder. Can J Occup Ther. 2013;80(5):274–283. doi:10.1177/0008417413501072
36. Villareal DT, Aguirre L, Gurney AB, et al. Aerobic or resistance exercise, or both, in dieting obese older adults. N Engl J Med. 2017;376(20):1943–1955. doi:10.1056/NEJMoa1616338
37. Dunsky A, Abu-Rukun M, Tsuk S, Dwolatzky T, Carasso R, Netz Y. The effects of a resistance vs. an aerobic single session on attention and executive functioning in adults. PLoS One. 2017;12(4):e0176092. doi:10.1371/journal.pone.0176092
38. Barkley RA, Murphy KR, Dupaul GI, Bush T. Driving in young adults with attention deficit hyperactivity disorder: knowledge, performance, adverse outcomes, and the role of executive functioning. J Int Neuropsychol Soc. 2002;8(5):655–672.
39. Weafer J, Camarillo D, Fillmore MT, Milich R, Marczinski CA. Simulated driving performance of adults with ADHD: comparisons with alcohol intoxication. Exp Clin Psychopharmacol. 2008;16(3):251–263. doi:10.1037/1064-1297.16.3.251
40. Narad M, Garner AA, Brassell AA, et al. Impact of distraction on the driving performance of adolescents with and without attention-deficit/hyperactivity disorder. JAMA Pediatr. 2013;167(10):933–938. doi:10.1001/jamapediatrics.2013.322
41. Patrick KE, Hurewitz F, McCurdy MD, et al. Driving comparisons between young adults with autism spectrum disorder and typical development. J Dev Behav Pediatr. 2018;39(6):451–460. doi:10.1097/DBP.0000000000000581
42. Brooks J, Kellett J, Seeanner J, et al. Training the motor aspects of pre-driving skills of young adults with and without autism spectrum disorder. J Autism Dev Disord. 2016;46(7):2408–2426. doi:10.1007/s10803-016-2775-8
43. Finke EH, Wilkinson KM, Hickerson BD. Social referencing gaze behavior during a videogame task: eye tracking evidence from children with and without ASD. J Autism Dev Disord. 2017;47(2):415–423. doi:10.1007/s10803-016-2968-1
44. Fuentes CT, Mostofsky SH, Bastian AJ. Children with autism show specific handwriting impairments. Neurology. 2009;73(19):1532–1537. doi:10.1212/WNL.0b013e3181c0d48c
45. Fuentes CT, Mostofsky SH, Bastian AJ. Perceptual reasoning predicts handwriting impairments in adolescents with autism. Neurology. 2010;75(20):1825–1829. doi:10.1212/WNL.0b013e3181fd633d
46. Rosenblum S, Epsztein L, Josman N. Handwriting performance of children with attention deficit hyperactive disorders: a pilot study. Phys Occup Ther Pediatr. 2008;28(3):219–234. doi:10.1080/01942630802224934
47. Tucha O, Lange KW. Handwriting and attention in children and adults with attention deficit hyperactivity disorder. Motor Control. 2004;8(4):461–471. doi:10.1123/mcj.8.4.461
48. Imhof M. Effects of color stimulation on handwriting performance of children with ADHD without and with additional learning disabilities. Eur Child Adolesc Psychiatry. 2004;13(3):191–198. doi:10.1007/s00787-004-0371-5
49. Li-Tsang CWP, Li TMH, Lau MSW, Ho CHY, Leung HWH. Handwriting assessment to distinguish comorbid learning difficulties from attention deficit hyperactivity disorder in Chinese adolescents: a case-control study. Int J Methods Psychiatr Res. 2018;27(4):e1718. doi:10.1002/mpr.1718
50. Schoemaker MM, Ketelaars CE, van Zonneveld M, Minderaa RB, Mulder T. Deficits in motor control processes involved in production of graphic movements of children with attention-deficit-hyperactivity disorder. Dev Med Child Neurol. 2005;47(6):390–395. doi:10.1017/S0012162205000769
51. Mahone EM, Powell SK, Loftis CW, Goldberg MC, Denckla MB, Mostofsky SH. Motor persistence and inhibition in autism and ADHD. J Int Neuropsychol Soc. 2006;12(5):622–631. doi:10.1017/S1355617706060814
52. Dickstein DP, Garvey M, Pradella AG, et al. Neurologic examination abnormalities in children with bipolar disorder or attention-deficit/hyperactivity disorder. Biol Psychiatry. 2005;58(7):517–524. doi:10.1016/j.biopsych.2004.12.010
53. Gilbert DL, Huddleston DA, Wu SW, et al. Motor cortex inhibition and modulation in children with ADHD. Neurology. 2019;93(6):e599–e610. doi:10.1212/WNL.0000000000007899
54. Gilbert DL, Isaacs KM, Augusta M, Macneil LK, Mostofsky SH. Motor cortex inhibition: a marker of ADHD behavior and motor development in children. Neurology. 2011;76(7):615–621. doi:10.1212/WNL.0b013e31820c2ebd
55. Klotz JM, Johnson MD, Wu SW, Isaacs KM, Gilbert DL. Relationship between reaction time variability and motor skill development in ADHD. Child Neuropsychol. 2012;18(6):576–585. doi:10.1080/09297049.2011.625356
56. Mostofsky SH, Rimrodt SL, Schafer JG, et al. Atypical motor and sensory cortex activation in attention-deficit/hyperactivity disorder: a functional magnetic resonance imaging study of simple sequential finger tapping. Biol Psychiatry. 2006;59(1):48–56. doi:10.1016/j.biopsych.2005.06.011
57. O’Brien JW, Dowell LR, Mostofsky SH, Denckla MB, Mahone EM. Neuropsychological profile of executive function in girls with attention-deficit/hyperactivity disorder. Arch Clin Neuropsychol. 2010;25(7):656–670. doi:10.1093/arclin/acq050
58. Pan CY, Chang YK, Tsai CL, Chu CH, Cheng YW, Sung MC. Effects of physical activity intervention on motor proficiency and physical fitness in children with ADHD: an Exploratory Study. J Atten Disord. 2017;21(9):783–795. doi:10.1177/1087054714533192
59. Leitner Y, Barak R, Giladi N, et al. Gait in attention deficit hyperactivity disorder: effects of methylphenidate and dual tasking. J Neurol. 2007;254(10):1330–1338. doi:10.1007/s00415-006-0522-3
60. Buderath P, Gartner K, Frings M, et al. Postural and gait performance in children with attention deficit/hyperactivity disorder. Gait Posture. 2009;29(2):249–254. doi:10.1016/j.gaitpost.2008.08.016
61. White BP, Mulligan SE. Behavioral and physiologic response measures of occupational task performance: a preliminary comparison between typical children and children with attention disorder. Am J Occup Ther. 2005;59(4):426–436. doi:10.5014/ajot.59.4.426
62. Lavasani NM, Stagnitti K. A study on fine motor skills of Iranian children with attention deficit/hyper activity disorder aged from 6 to 11 years. Occup Ther Int. 2011;18(2):106–114. doi:10.1002/oti.306
63. Ben-Pazi H, Shalev RS, Gross-Tsur V, Bergman H. Age and medication effects on rhythmic responses in ADHD: possible oscillatory mechanisms? Neuropsychologia. 2006;44(3):412–416. doi:10.1016/j.neuropsychologia.2005.05.022
64. Leitner Y, Doniger GM, Barak R, Simon ES, Hausdorff JM. A novel multidomain computerized cognitive assessment for attention-deficit hyperactivity disorder: evidence for widespread and circumscribed cognitive deficits. J Child Neurol. 2007;22(3):264–276. doi:10.1177/0883073807299859
65. Dyck MJ, Piek JP. Developmental delays in children with ADHD. J Atten Disord. 2014;18(5):466–478. doi:10.1177/1087054712441832
66. Kalff AC, de Sonneville LM, Hurks PP, et al. Low- and high-level controlled processing in executive motor control tasks in 5–6-year-old children at risk of ADHD. J Child Psychol Psychiatry. 2003;44(7):1049–1057. doi:10.1111/1469-7610.00189
67. Rubia K, Noorloos J, Smith A, Gunning B, Sergeant J. Motor timing deficits in community and clinical boys with hyperactive behavior: the effect of methylphenidate on motor timing. J Abnorm Child Psychol. 2003;31(3):301–313. doi:10.1023/A:1023233630774
68. Colvin AN, Yeates KO, Enrile BG, Coury DL. Motor adaptation in children with myelomeningocele: comparison to children with ADHD and healthy siblings. J Int Neuropsychol Soc. 2003;9(4):642–652. doi:10.1017/S1355617703940045
69. Aase H, Sagvolden T. Infrequent, but not frequent, reinforcers produce more variable responding and deficient sustained attention in young children with attention-deficit/hyperactivity disorder (ADHD). J Child Psychol Psychiatry. 2006;47(5):457–471. doi:10.1111/j.1469-7610.2005.01468.x
70. Rubia K, Taylor A, Taylor E, Sergeant JA. Synchronization, anticipation, and consistency in motor timing of children with dimensionally defined attention deficit hyperactivity behaviour. Percept Mot Skills. 1999;89(3 Pt 2):1237–1258. doi:10.2466/pms.1999.89.3f.1237
71. Slaats-Willemse D, de Sonneville L, Swaab-Barneveld H, Buitelaar J. Motor flexibility problems as a marker for genetic susceptibility to attention-deficit/hyperactivity disorder. Biol Psychiatry. 2005;58(3):233–238. doi:10.1016/j.biopsych.2005.03.046
72. Harvey WJ, Reid G, Grizenko N, Mbekou V, Ter-stepanian M, Joober R. Fundamental movement skills and children with attention-deficit hyperactivity disorder: peer comparisons and stimulant effects. J Abnorm Child Psychol. 2007;35(5):871–882. doi:10.1007/s10802-007-9140-5
73. Vickers JN, Rodrigues ST, Brown LN. Gaze pursuit and arm control of adolescent males diagnosed with attention deficit hyperactivity disorder (ADHD) and normal controls: evidence of a dissociation in processing visual information of short and long duration. J Sports Sci. 2002;20(3):201–216. doi:10.1080/026404102317284763
74. Esposito G, Venuti P. Analysis of toddlers’ gait after six months of independent walking to identify autism: a preliminary study. Percept Mot Skills. 2008;106(1):259–269. doi:10.2466/pms.106.1.259-269
75. David FJ, Baranek GT, Giuliani CA, Mercer VS, Poe MD, Thorpe DE. A pilot study: coordination of precision grip in children and adolescents with high functioning autism. Pediatr Phys Ther. 2009;21(2):205–211. doi:10.1097/PEP.0b013e3181a3afc2
76. de Moraes IAP, Monteiro CBM, Silva TDD, et al. Motor learning and transfer between real and virtual environments in young people with autism spectrum disorder: a prospective randomized cross over controlled trial. Autism Res. 2020;13(2):307–319. doi:10.1002/aur.2208
77. Glazebrook C, Gonzalez D, Hansen S, Elliott D. The role of vision for online control of manual aiming movements in persons with autism spectrum disorders. Autism. 2009;13(4):411–433. doi:10.1177/1362361309105659
78. Rosales MR, Romack J, Angulo-Barroso R. sEMG analysis during landing in children with autism spectrum disorder: a pilot study. Pediatr Phys Ther. 2018;30(3):192–194. doi:10.1097/PEP.0000000000000514
79. Borremans E, Rintala P, McCubbin JA. Physical fitness and physical activity in adolescents with Asperger's syndrome: a comparative study. Adapt Phys Activ Q. 2010;27(4):308–320. doi:10.1123/apaq.27.4.308
80. Tantillo M, Kesick CM, Hynd GW, Dishman RK. The effects of exercise on children with attention-deficit hyperactivity disorder. Med Sci Sports Exerc. 2002;34(2):203–212. doi:10.1097/00005768-200202000-00004
81. Muntaner-Mas A, Ortega FB, Femia P, et al. Low cardiorespiratory fitness and obesity for ADHD in childhood and adolescence: a 6-year cohort study. Scand J Med Sci Sports. 2021;31(4):903–913. doi:10.1111/sms.13905
82. Tyler K, MacDonald M, Menear K. Physical activity and physical fitness of school-aged children and youth with autism spectrum disorders. Autism Res Treat. 2014;2014:312163. doi:10.1155/2014/312163
83. Irwin LN, Soto EF, Chan ESM, et al. Activities of daily living and working memory in pediatric attention-deficit/hyperactivity disorder (ADHD). Child Neuropsychol. 2021;27(4):468–490. doi:10.1080/09297049.2020.1866521
84. Weaver LL. Effectiveness of work, activities of daily living, education, and sleep interventions for people with autism spectrum disorder: a systematic review. Am J Occup Ther. 2015;69(5):6905180020p6905180021–6905180011. doi:10.5014/ajot.2015.017962
85. Yela-Gonzalez N, Santamaria-Vazquez M, Ortiz-Huerta JH. Activities of daily living, playfulness and sensory processing in children with autism spectrum disorder: a Spanish study. Children. 2021;8(2). doi:10.3390/children8020061
86. Naito E, Kinomura S, Geyer S, Kawashima R, Roland PE, Zilles K. Fast reaction to different sensory modalities activates common fields in the motor areas, but the anterior cingulate cortex is involved in the speed of reaction. J Neurophysiol. 2000;83(3):1701–1709. doi:10.1152/jn.2000.83.3.1701
87. Kudo K, Miyazaki M, Kimura T, et al. Selective activation and deactivation of the human brain structures between speeded and precisely timed tapping responses to identical visual stimulus: an fMRI study. Neuroimage. 2004;22(3):1291–1301. doi:10.1016/j.neuroimage.2004.03.043
88. Harris CM, Wolpert DM. Signal-dependent noise determines motor planning. Nature. 1998;394(6695):780–784. doi:10.1038/29528
89. Honda M, Deiber MP, Ibanez V, Pascual-Leone A, Zhuang P, Hallett M. Dynamic cortical involvement in implicit and explicit motor sequence learning. A PET study. Brain. 1998;121(Pt 11):2159–2173. doi:10.1093/brain/121.11.2159
90. Paus T, Zatorre RJ, Hofle N, et al. Time-related changes in neural systems underlying attention and arousal during the performance of an auditory vigilance task. J Cogn Neurosci. 1997;9(3):392–408. doi:10.1162/jocn.1997.9.3.392
91. Ozonoff S, Rogers SJ, Pennington BF. Asperger’s syndrome: evidence of an empirical distinction from high-functioning autism. J Child Psychol Psychiatry. 1991;32(7):1107–1122. doi:10.1111/j.1469-7610.1991.tb00352.x
92. Mizuno K, Yoneda T, Komi M, Hirai T, Watanabe Y, Tomoda A. Osmotic release oral system-methylphenidate improves neural activity during low reward processing in children and adolescents with attention-deficit/hyperactivity disorder. Neuroimage Clin. 2013;2:366–376. doi:10.1016/j.nicl.2013.03.004
93. Castellanos FX, Aoki Y. Intrinsic functional connectivity in attention-deficit/hyperactivity disorder: a science in development. Biol Psychiatry Cogn Neurosci Neuroimaging. 2016;1(3):253–261. doi:10.1016/j.bpsc.2016.03.004
94. Rubia K, Overmeyer S, Taylor E, et al. Prefrontal involvement in “temporal bridging” and timing movement. Neuropsychologia. 1998;36(12):1283–1293. doi:10.1016/S0028-3932(98)00038-4
95. Jolliffe T, Baron-Cohen S. Are people with autism and Asperger syndrome faster than normal on the embedded figures test? J Child Psychol Psychiatry. 1997;38(5):527–534. doi:10.1111/j.1469-7610.1997.tb01539.x
96. Klin A, Volkmar FR, Sparrow SS, Cicchetti DV, Rourke BP. Validity and neuropsychological characterization of Asperger syndrome: convergence with nonverbal learning disabilities syndrome. J Child Psychol Psychiatry. 1995;36(7):1127–1140. doi:10.1111/j.1469-7610.1995.tb01361.x
97. Herringshaw AJ, Ammons CJ, DeRamus TP, Kana RK. Hemispheric differences in language processing in autism spectrum disorders: a meta-analysis of neuroimaging studies. Autism Res. 2016;9(10):1046–1057. doi:10.1002/aur.1599
98. Yang J, Hofmann J. Action observation and imitation in autism spectrum disorders: an ALE meta-analysis of fMRI studies. Brain Imaging Behav. 2016;10(4):960–969. doi:10.1007/s11682-015-9456-7
99. Grafton ST, Fagg AH, Arbib MA. Dorsal premotor cortex and conditional movement selection: a PET functional mapping study. J Neurophysiol. 1998;79(2):1092–1097. doi:10.1152/jn.1998.79.2.1092
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Cost of Neurodevelopmental Disability: Scoping Review of Economic Evaluation Methods
Kularatna S, Jadambaa A, Senanayake S, Brain D, Hawker N, Kasparian NA, Abell B, Auld B, Eagleson K, Justo R, McPhail SM
ClinicoEconomics and Outcomes Research 2022, 14:665-682
Published Date: 18 October 2022
The Role of Mitochondrial DNA Copy Number in Neurodevelopmental Disorders: A Bidirectional Two-Sample Mendelian Randomization Study
Qiu X, Song H, Wu C, Chen C, Zhi H, Zhang C, Zhu X
Psychology Research and Behavior Management 2025, 18:2323-2332
Published Date: 24 November 2025
High Fever Manifestation During Acute Infections Coincides with Improvement in Autism Spectrum Disorder (ASD) While Under Classical Homeopathy, A Case Report
Jaggi A, Jaggi L, Batra M, Mahesh S, Vithoulkas G
Pediatric Health, Medicine and Therapeutics 2026, 17:583452
Published Date: 27 March 2026