")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Mothers’ Attitudes Towards Breastfeeding in Terms of Health Safety and Professional Lactation Education: A National Survey of Women
Authors Bednarek A, Bodys-Cupak I, Serwin A, Cipora E
Received 20 July 2023
Accepted for publication 28 September 2023
Published 3 November 2023 Volume 2023:16 Pages 3273—3286
DOI https://doi.org/10.2147/JMDH.S431576
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Anna Bednarek,1 Iwona Bodys-Cupak,2 Adrianna Serwin,1 Elżbieta Cipora3
1Department of Health Promotion, Faculty of Health Sciences, Medical University of Lublin, Lublin, Poland; 2Department of Nursing Fundamentals, Institute of Nursing and Midwifery, Faculty of Health Sciences, Jagiellonian University Medical College, Krakow, Poland; 3Medical Institute, Jan Grodek State University in Sanok, Sanok, Poland
Correspondence: Anna Bednarek, Department of Health Promotion Chair of Nursing Development, Faculty of Health Sciences, Medical University of Lublin, S. Staszica 4-6 Street, 20-081, Lublin, Poland, Tel +48 81 448 67 20 ; +48 607 607 115, Email [email protected]
Introduction and Objective: An important role in building opinions and attitudes regarding breastfeeding by mothers is played by the medical staff taking care of the mother woman expecting a baby. Breastfeeding is a standard in infant nutrition. The knowledge and support of the medical staff can help a woman make the decision to breastfeed. At the same time, it creates conditions for an optimal working environment for medical staff, affecting the quality of care. The aim of the study was identify mothers’ attitudes towards breastfeeding in the context of health safety and professional lactation education.
Materials and Methods: Data for the study were obtained on the basis of a proprietary questionnaire and a standardized research tool, which was the questionnaire for assessing knowledge and attitudes towards breastfeeding The Iowa Infant Feeding Attitude Scale designed by Arlene De la Mora (IIFAS). The study involved 439 women who gave birth to a child in the last 5 years.
Results: Extensive knowledge about the benefits of breastfeeding for the child’s body is declared by 67.9% of women. The vast majority of respondents (94.1%) pointed to supporting the development of the immune system. Most women (85%) obtained information on breastfeeding from the Internet, and 58.5% from medical personnel. Most respondents (88.8%) assessed their partner’s attitude towards breastfeeding as positive. The result, The Iowa Infant Feeding Attitude Scale was equal to 50.97, which proves the positive attitude of women to breastfeeding.
Conclusion: Promoting the best way to feed children, which is breastfeeding, plays an important role in building mothers’ opinions and attitudes about breastfeeding.
Keywords: mothers’ attitudes towards breastfeeding, lactation education, health safety, nurses, midwives
Introduction
Breastfeeding has long been considered the best way to feed infants and young children. Breastfeeding was originally chosen solely for the sake of being in harmony with the laws of nature. With the development of scientific research on the properties of human milk, the long-term health benefits of breastfeeding for the baby and mother have been proven.1
The World Health Organization (WHO) has been encouraging future moms to breastfeed since 1974 as the healthiest way to feed babies for the first 6 months of their lives. After the age of 6 months, the WHO recommends introducing other foods, while maintaining breastfeeding until the child reaches 2 years of age, and even for a longer time. The WHO also advises that newborns should be breastfed in the first hour after birth and then fed “on demand”, that is, when they show the need for food. The WHO strongly advises against feeding infants using a bottle and pacifier.2
The American Academy of Pediatrics (AAP) also recommends exclusive breastfeeding for the first 6 months of a baby’s life. The APP recommends introducing complementary foods after 6 months of age and continuing breastfeeding until the age of 1 or until the woman and the child show the need for breastfeeding. The AAP does not specify an upper limit for the duration of breastfeeding. In addition, the APP recommends avoiding additional drinks or food for infants without an undue reason and introducing a pacifier only after 3–4 weeks of age or after achieving regular and cyclical lactation.3
At the same time, global and Polish teams of experts in the field of medical science, guided by the recommendations of the WHO and AAP based on the results of scientific research, are unanimous in promoting the need and value of breastfeeding for the first 6 months of a child’s life. The European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) states that infants who are fully or partly breastfed should be introduced to complementary foods, other than formula milk, after 17 weeks of age, but no later than 26 weeks of age. ESPGHAN emphasizes that the decision to continue breastfeeding should be based on the unique factors of both the baby and the mother.2,4
The Polish Society of Gastroenterology, Hepatology, and Nutrition for Children (PTGHiŻDz) also assumes that the main goal to be pursued is exclusive breastfeeding for the first 6 months of a child’s life. Experts believe that breastfeeding is the best way to ensure optimal and proper development of the child and conclude that breastfeeding is the standard when it comes to infant feeding.5
Breast milk has an ideal quantitative and qualitative composition for the requirements of the developing infant’s organism. The content of various nutrients varies depending on the duration of lactation, the time of day, and the diet of the breastfeeding mother. Initial milk, ie, colostrum, is produced for about 4 days after birth, then transitional milk is produced, which becomes mature milk after 2–3 weeks.6
Breast milk contains anti-inflammatory and anti-infective substances such as IgA antibodies, B lymphocytes, prostaglandins, lysozyme, and interferon, which protect the infant’s digestive tract against infections and strengthen the infant’s immune system. Colostrum protects the baby from the first feeding against toxins, allergens, and pathogenic strains of Escherichia coli bacteria. Colostrum also provides stimulation of Lactobacillus bifidus bacteria beneficial for the digestive system, which constitute the normal bacterial flora (so-called microbiota). Breastmilk is a source of polyamines, necessary for the maturation of the newborn intestines.7,8 Polypeptide hormones (resistin, lectin, ghrelin, and adiponectin) in milk are responsible for regulating energy balance.9,10
Lactose, constituting 80% of all carbohydrates in breast milk, supports the growth of beneficial bacteria in the infant’s digestive tract, and facilitates the absorption of iron and the absorption of calcium, and magnesium. An equally important carbohydrate is galactose, which supports the development of the brain and nervous system.11
Fats are an essential component of breast milk. Cholesterol, the content of which in mature milk is 10–22mg/dL, is irreplaceable when it comes to the myelination of the central nervous system of a child and protects adults against its high concentration. The essential nutrients for the infant also include the fatty acids LC-PUFAs (arachidonic acid and docosahexaenoic acid). They are responsible for the proper development of the nervous system, lungs, and the structure of the eye.12,13
Breast milk contains trace elements and vitamins soluble in fats and water. They contribute to a very rapid weight gain. They play an important role in the maturation of the infant’s systems and organs. The proportion of calcium and phosphorus (1:4) promotes better calcium absorption and proper bone development. The exceptions are vitamins D and K, which should be supplemented when breastfeeding.7,14
The scientific literature clearly indicates many benefits of breastfeeding both for the health of the child and the health of the child’s mother. Breastfeeding supports the development of the immune system of newborns and infants, reducing the frequency and severity of respiratory infections in children, and reducing the risk of bacterial meningitis, otitis media, and necrotizing enterocolitis.10 The beneficial effect of breastfeeding in the prevention of sudden infant death syndrome (SIDS) has been confirmed. In addition, breastfeeding also has a positive effect on the cognitive and neurobehavioral development of infants. Breastfed babies score higher on intelligence tests.15–17 In people who were breastfed, a reduced risk of chronic diseases such as obesity, type I and type II diabetes, allergy, leukemia, hypercholesterolemia, and heart disease is observed in later years of life.8,11 The benefits of breastfeeding for mothers include reduced risk of postpartum hemorrhage, and lower risk of breast cancer, ovarian cancer, and osteoporosis. Breastfeeding women also tend to return to their pre-pregnancy weight more quickly than those who choose not to breastfeed.17
Mothers of newborn children often face various difficulties related to breastfeeding. They may be caused by anatomical and physiological conditions on the part of the mother’s breast or the child’s oral cavity, or have a psychological background. The main difficulties in breastfeeding include sore nipples and their abnormal structure, breast fullness, inflammation and swelling of the breast, postpartum depression, poor motivation to feed, and problems with starting and maintaining lactation.18
Mothers of children with Down syndrome and craniofacial developmental defects may also have difficulties with breastfeeding. They are caused by the symptoms that accompany them. Children with these disorders are recommended to be fed expressed breast milk using a bottle and bottle nipple.19
Most mothers can breastfeed their newborns from the first hours of their lives, but there are contraindications, both on the part of the mother and the child, which justify temporary or permanent discontinuation of breastfeeding. Classic galactosemia and congenital lactose intolerance are contraindications and reasons for the permanent discontinuation of breastfeeding. Treatment consists of the inclusion of an elimination diet and the exclusion of lactose. This means the need to replace breastfeeding with lactose-free formulas.7,20
Actions to promote breastfeeding are undertaken at the global, national, and individual levels. These actions consist of raising awareness about breastfeeding and motivating women to initiate it. An important aspect when it comes to maintaining lactation is the image of breastfeeding developed among women. Knowledge and support can help a woman decide to breastfeed. A successful lactation process gives a breastfeeding woman satisfaction, as well as a sense of fulfillment in the role of a mother. The positive aspect of breastfeeding is also convenience and economy.21
Early cessation of breastfeeding can cause anxiety for mothers and health problems for themselves and their babies. The variation in rates of initiation and continuation of breastfeeding around the world shows that key factors influencing infant feeding are likely to be sociocultural in nature and related to group social norms, as well as public health policies and the availability of professional care. Few health behaviors have as broad and long-lasting impact on population health as breastfeeding infants. Therefore, offering women professional support allows you to avoid or overcome breastfeeding problems, which extends its duration and exclusivity. These can be offered to women on a one-to-one basis, proactively by contacting women directly, or reactively by waiting for women to reach out and ask for breastfeeding support.22 Stopping breastfeeding early is not a decision that women can easily make. It is associated with frequent problems such as sore breasts and nipples, concerns about the sufficiency of the milk supply and the baby’s behavior, and in some cases, confusion about breastfeeding in public places. Many mothers report anxiety about the decision to stop breastfeeding, even in cultures where breastfeeding rates are high, which means women often do not receive the quality of health care they need. Therefore, a key factor is the training and education of medical workers in the prevention and treatment of problems related to breastfeeding.23,24
Most women decide on how to feed their baby immediately before giving birth. Breastfeeding is also often perceived as a woman’s personal choice. Despite initial declarations regarding breastfeeding, many mothers decide to use artificial formula after giving birth, which is related to various factors, most often health, socio-demographic, and psychological. Maternity and neonatal units in many countries, including Poland, are obliged to promote and support breastfeeding. Most countries also collect information on breastfeeding rates in various forms, such as surveys and epidemiological data. These methods vary from country to country, so comparative analyses are not always possible. In the literature on the subject, the authors emphasize the need for effective methods of promoting breastfeeding, which would help shape a positive attitude towards breastfeeding and improve its social perception. Education and support from medical staff are therefore important for women to regain confidence in breastfeeding.8,11–13,18
The promotion of breastfeeding, which has been going on for years in Poland, is on an increasingly higher level. Educational programs and documents resulting from the national health policy are created. Nurses, midwives, and doctors who have professional contact with a woman preparing for motherhood are obliged to promote breastfeeding by providing reliable information in this regard. It is also appropriate to tell women that breastfeeding is a part of life that also has a place in social and public life. Well-conducted lactation education affects the quality of care for mother and child and relieves communication stress.25–27 So far, only a few studies on women’s attitudes toward breastfeeding have been conducted in Poland using standardized research tools, which is why research on this subject is fully justified.
The aim of this study is to identify mothers’ attitudes toward breastfeeding in the context of health safety and professional lactation education. Establishing a positive interpersonal relationship between the mother of a newborn and the medical staff builds trust, opens up a motivating educational dialogue, and promotes the exchange of information. This guarantees the willingness of the mother to cooperate and relieves postpartum stress, at the same creating the conditions for an optimal working environment for medical staff which affects the quality of care. Taking and continuing breastfeeding contributes to the biological and psychosocial health of both the mother and the child. The quality of lactation education provided by medical staff supports this process. Friendly relationships with mothers through support and professional education result in a positive impact on the professional functioning of medical staff, which is very important for the well-being and diligent undertaking of various professional tasks in the care of mothers.
Materials and Method
The research for this study was carried out using the diagnostic survey method. The research technique was a questionnaire, and the collected data were obtained based on an own questionnaire and a standardized research tool, which was a questionnaire for assessing knowledge and attitudes towards breastfeeding, ie, The Iowa Infant Feeding Attitude Scale designed by Arlene De la Mora (IIFAS).28 The IIFAS has good predictive validity and excellent internal consistency in Cronbach’s alpha range of 0.79 to 0.86.
The questionnaire of the study’s authors consisted of two parts. The first part contained 13 single-choice or multiple-choice questions, which aimed to collect information on the duration of breastfeeding, the level of knowledge about the benefits of breastfeeding for the child and the mother, the reasons for discontinuation of breastfeeding, as well as support and education of the woman before and during the lactation. The second part contained 7 questions that concerned the socio-demographic data of the surveyed women, such as age, place of residence, education, type of delivery, number of already given births, profession, and marital status.
The IIFAS questionnaire contained 17 statements regarding natural and artificial methods of feeding infants and the benefits of breastfeeding for the child and mother. The statements in the questionnaire are presented in a way that about half of the questions show a view in favor of breastfeeding, and the remaining questions are in favor of formula feeding. The task of the surveyed women was to determine compliance with statements using a 5-point Likert scale, where 1 means “I strongly disagree” and 5 - “I strongly agree”. The remaining categories are 2 - “I rather disagree”, 3 – “I have no opinion”, and 4 – “I rather agree”. The IIFAS total score can range from 17 to 85. Scores are interpreted so that a high score reflects a preference for breastfeeding. IIFAS total scores can be divided into three groups, including positive for breastfeeding (IIFAS score 70–85), neutral (IIFAS score 49–69), and positive for formula feeding (IIFAS score 17–48).
From the collected information, a database was created in MS Excel 2007. Statistical calculations were made using Statistica 10. The values of qualitative variables were presented using absolute values and percentages. The significance of differences for particular groups of variables was checked with the chi-square test (Pearson’s χ2). The values of quantitative variables are represented by mean and standard deviation, median, and minimum and maximum values. To select the statistical methods, the distribution of the analyzed variables was compared with the normal distribution using the Kolmogorov–Smirnov test. The dependence of quantitative variables in individual groups for variables with a normal distribution was checked by parametric, one-way analysis of variance ANOVA for independent groups. The obtained results were considered statistically significant at the level of p<0.05.
The Course of the Study
The study covered women who gave birth to a child in the last 5 years. The results of the survey questionnaire were collected online from November 2020 to April 2021 using Google Forms (https://forms.gle/xW4ezNZWzP3Zx6KeA) among online groups integrating women with children. A total of 439 women participated in the study. Each respondent was informed via the questionnaire about the purpose and anonymity of the study and agreed to participate in the study. All questionnaires were fully completed.
The study questionnaire was available on the website from November 3, 2020, from 12:00 p.m. to April 30, 2021, at midnight. Completing the questionnaire took about 30 minutes. Each mother who wanted to take part in the study had the opportunity to access the survey questionnaire at any place and time, after logging in to the indicated website and completing the research consent form as an attachment to the research questionnaire. Then, all completed survey questionnaires were carefully checked by the authors to minimize bias and increase the quality of online survey research. Information about the availability of the online survey for this study was also provided by phone to the maternity and neonatal departments of clinical and provincial hospitals in Lublin, Krakow, and Podkarpackie counties. The snowball sampling method was also used, which involved recruiting friends of women with small children through other women of the same status.
The research was conducted after approval of the Council of the Faculty of Health Sciences of the Medical University of Lublin (Appendix No. 2 to Resolution No. 63/2018-2019 of the Council of the Faculty of Health Sciences of the Medical University of Lublin of October 22, 2020) and in accordance with the assumptions of the Declaration of Helsinki.
The criterion for inclusion in the research:
- Study group: women
- Having a child under the age of 5
The criterion for exclusion from the research:
- Study group: men
- Having a child over the age of 5
Results
The characteristics of the study group are presented in Table 1, which shows that the people participating in the study are mostly young women, in the procreative period, living in the city, with higher education, and professionally active. The vast majority of the study participants are married women with one child delivered naturally.
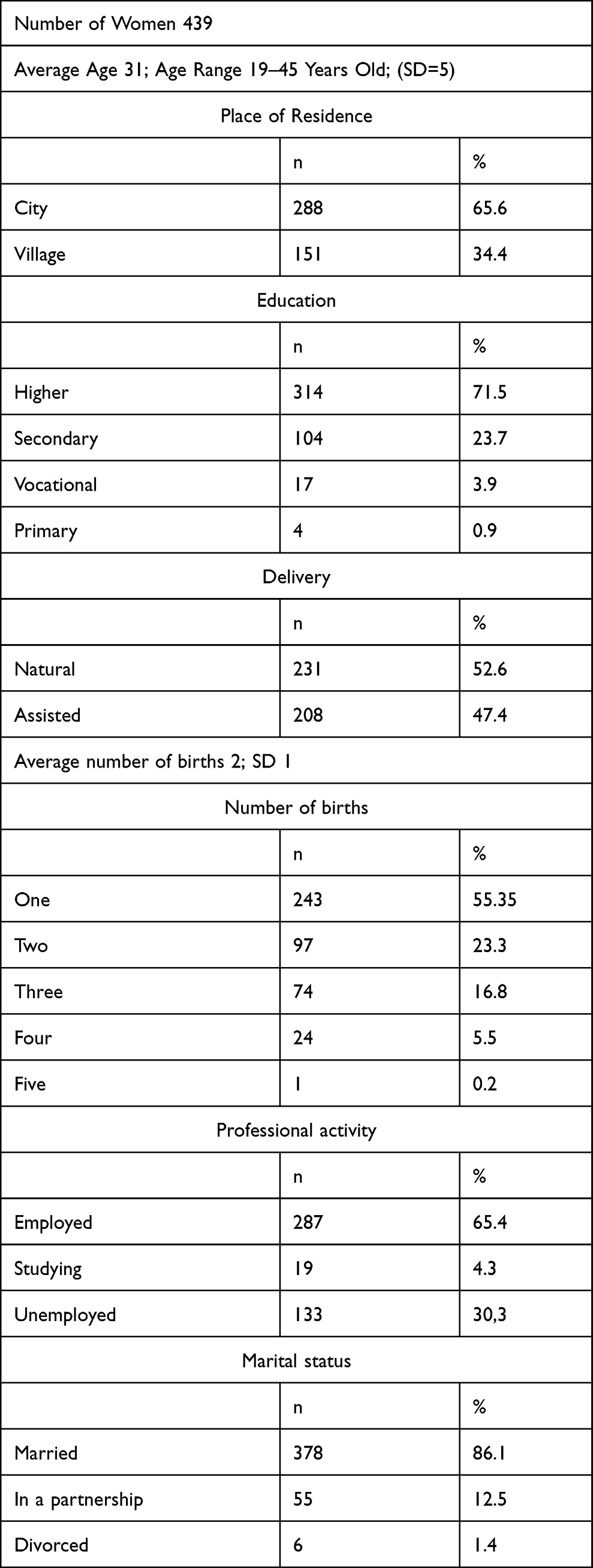 |
Table 1 Characteristics of the Surveyed Women |
Data Analysis Based on an Own Survey Questionnaire
Information collected from the surveyed women on breastfeeding, including the reasons for not breastfeeding or early cessation of breastfeeding, was analyzed and presented in the form of a description.
Analyzing attitude of the husband/partner towards breastfeeding in the opinion of the surveyed women (n=439) it turned out that, the vast majority of the surveyed women (n=390; 88.8%) claimed that the attitude of their husband or partner towards their willingness to breastfeed was positive, 45 women (10.3%) claimed it was neutral, and 4 respondents (0.9%) considered that the attitude of their husband or partner was negative.
Subjective assessment of knowledge about breastfeeding (n=439) showed that 279 women (63.6%) described their knowledge of breastfeeding as extensive, 45 respondents (34.6%) stated that they had basic knowledge about breastfeeding, and 4 respondents (1.8%) stated that they did not know a lot about breastfeeding.
As a source of seeking knowledge about breastfeeding, the majority of respondents (n=373; 85%) indicated the Internet, 257 women (58.5%) medical staff, 215 women (49%) scientific and popular science literature, 179 respondents (40.8%) friends. For 171 respondents (39%), the source of knowledge was the birthing school, for 117 women (26.7%) mother or mother-in-law, and for 56 respondents (12.8%) the media. Significantly, more respondents obtained knowledge about breastfeeding from the Internet and medical staff, as well as from scientific and popular science literature (n=439; Ch2=318.089; p<0.001).
In a subjective assessment, extensive knowledge about the positive impact of breastfeeding on the child was reported by 395 respondents (90%), while 44 women (10%) considered that their knowledge in this area is not extensive. Among the surveyed women, 413 of them (94.1%) stated that breastfeeding supports the development of the child’s immune system. According to 394 mothers (89.7%), breastfeeding gives a child a sense of security. For 219 respondents (49.9%) breastfed children suffer from bacterial infections less severely and less frequently. 218 respondents (49.7%) believed that thanks to breastfeeding later in life children are protected against overweight, obesity, and diabetes, and according to 212 women (48.3%), breastfeeding stimulates the development of beneficial microbiota of the child’s digestive tract. Significantly, more children receive support in the development of the immune system through breastfeeding and have a sense of security (Ch2 = 314.379; p<0.001).
According to 298 respondents (67.9%), their knowledge of the positive impact of breastfeeding on the mother’s body is extensive. 131 respondents (29.8%) considered that their knowledge is not extensive and 10 women (2.3%) considered that they had no knowledge of the subject.
For 397 women (90.4%), breastfeeding creates a strong bond between the child and the mother, and 277 respondents (63.1%) stated that breastfeeding helps the mother’s weight return to its pre-pregnancy state. 258 respondents (58.8%) stated that breastfeeding reduces the risk of breast and ovarian cancer. 228 mothers (51.9%) believe that breastfeeding has a positive effect on reducing postpartum depression. For 104 respondents (23.7%), breastfeeding delays the first ovulation and menstruation after childbirth, and 76 women (17.3%) indicated that breastfeeding reduces the risk of type II diabetes. Significantly more respondents pointed to the benefits of breastfeeding as the creation of a strong bond between the child and the mother, faster return of the mother’s body weight to the pre-pregnancy state, and lowering the risk of breast and ovarian cancer (Ch2 = 314.379; p<0.001).
Analyzing the method of feeding a newborn (n=439) it turned out that, exactly 280 surveyed mothers (63.8%) exclusively breastfed their child, 17 respondents (3.9%) fed their child with infant formula, and 142 respondents (32.3%) fed their child with both breast and infant formula.
Among the respondents, 115 women (26.2%) felt social pressure to breastfeed, and 324 respondents (73.8%) did not experience it. Exactly 42 respondents (9.6%) breastfed their child only for the first month of life, 60 respondents (13.7%) over 1 month of age, and 58 (13.2%) breastfed up to 6 months of age. 71 women (16.1%) breastfed the child after the child was 6 months old, and 208 respondents (47.4%) continued breastfeeding after the child was 12 months old. Significantly more respondents breastfed their children over 12 months of age compared to the rest (Ch2 = 210.579; p<0.001).
Exactly 132 women (30.1%) indicated the right time to stop breastfeeding as the reason for discontinuation of breastfeeding. In 102 respondents (23.2%), there was a drop in milk supply, and 92 respondents (21%) stated that the child did not want to be breastfed any longer. Among the respondents, 84 women (19.1%) were still breastfeeding, 67 respondents (15.3%) stopped breastfeeding due to medical contraindications, and for 45 women (10.3%) the reason was the need to return to work. 14 respondents (3.2%) stopped breastfeeding due to the time-consuming nature of breastfeeding. According to 13 respondents (3%), formula feeding was more convenient than breastfeeding, and 11 women (2.5%) stopped breastfeeding due to another pregnancy. Statistical tests (p value <0.05) showed statistically significant differences Ch2 = 249.164; p<0.001. The most common significant reasons turned out to be the right time to stop breastfeeding, the drop in milk supply, and the child who no longer wanted to be breastfed.
Exactly 319 women (72.7%) received help from medical staff during breastfeeding, and 120 respondents (27.3%) did not receive such support.
Among the surveyed women, 303 of them (69%) received support in the form of learning how to latch the baby to the breast, information brochures were provided to 190 respondents (43.3%), 196 respondents (44.6%) had an educational conversation about breastfeeding, and 39 respondents (8.9%) did not receive postpartum support from medical staff on breastfeeding. Statistical tests showed significant differences in the types of education of women by medical staff. Significantly more women received support in learning how to breastfeed a child (Ch2 = 194.231; p<0.001).
Analysis of the Significance of the Impact and Differences in Breastfeeding in the Authors’ Survey Questionnaire
In order to determine the normality of the distribution, the results of the questionnaire questions regarding the age and duration of breastfeeding were used. Initially, it was checked whether the age distribution did not differ significantly from the normal distribution. Statistical tests (Kolmogorov–Smirnov test) confirmed that age distributions with different duration of breastfeeding did not differ significantly from the normal distribution, therefore parametric tests were used, specifically the one-way analysis of variance ANOVA for independent groups.
Then, the significance of the influence of age on the duration of breastfeeding was checked. Statistical tests (test F=7.377; p<0.001) showed that age significantly affected the duration of breastfeeding.
In order to determine the dependence, the results of the questionnaire questions concerning the subjective assessment of women’s knowledge about the benefits of breastfeeding for both the child and the mother and the duration of breastfeeding were used. In order to determine the dependence between these variables, the value of the chi-square test statistic was calculated and its significance level was determined. The results are presented in Table 2 and Table 3.
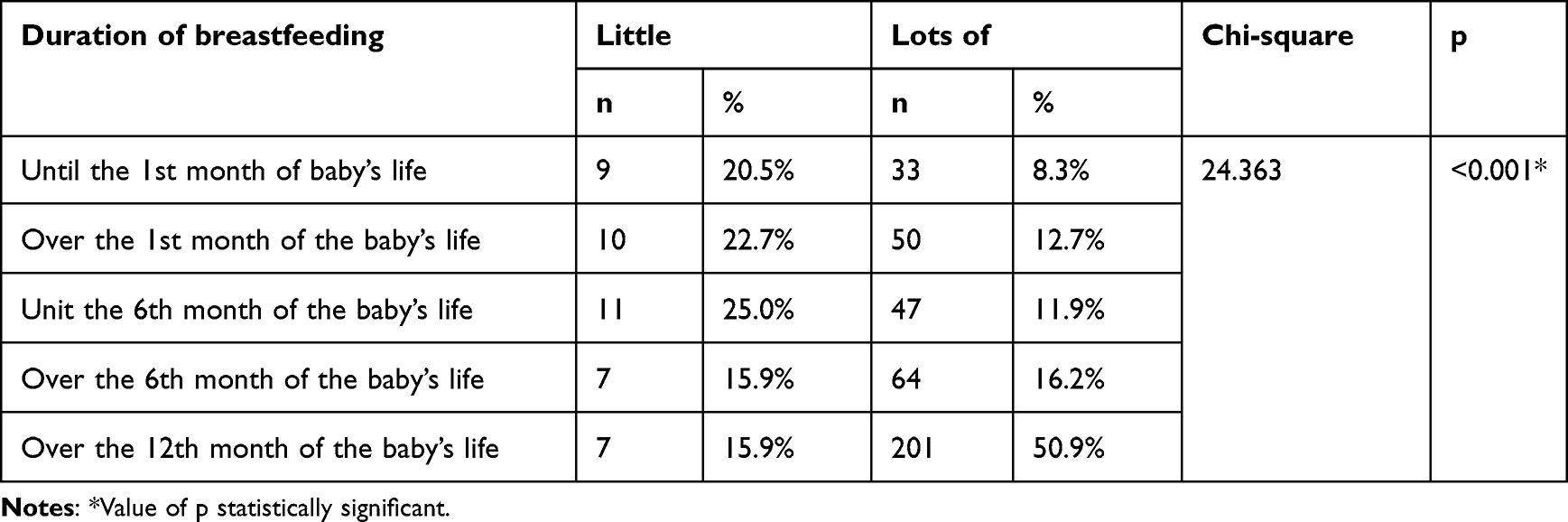 |
Table 2 Analysis of the Dependence Between the Subjective Assessment of Women’s Knowledge About the Benefits of Breastfeeding for the Child and the Duration of Breastfeeding (n=439) |
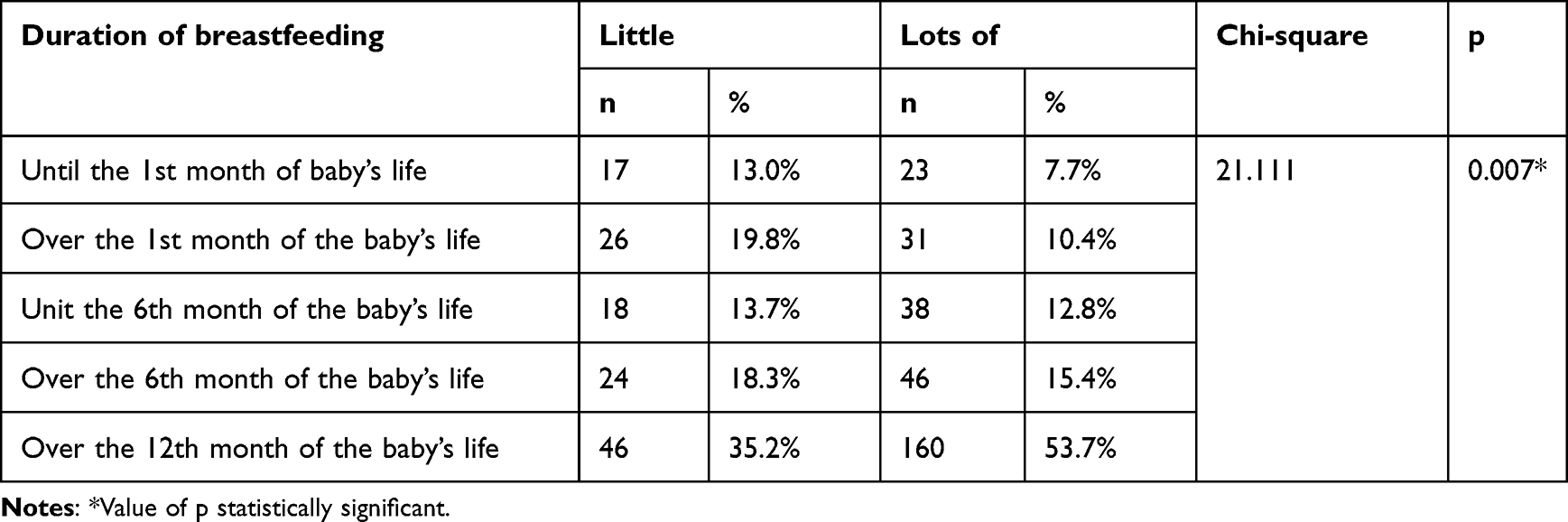 |
Table 3 Analysis of the Dependence Between the Subjective Assessment of Women’s Knowledge About the Benefits of Breastfeeding for the Mother and the Duration of Breastfeeding (n=439) |
Statistical tests (p value <0.05) showed that the subjective assessment of women’s knowledge about the benefits of breastfeeding for the child significantly affected the duration of breastfeeding (Table 2).
Statistical tests (p value <0.05) showed that the subjective assessment of women’s knowledge about the benefits of breastfeeding for the mother significantly affected the duration of breastfeeding (Table 3).
Data Analysis Based on the Iowa Infant Feeding Attitude Scale (IIFAS) Questionnaire
By analyzing the statements of the subjects of The Iowa Infant Feeding Attitude Scale, women’s attitudes toward breastfeeding were examined. The data obtained are summarized in Table 4. Women were strongly convinced that: “breastfeeding strengthens the mother-child bond” (n=348; 79.2%), “breast milk is the ideal food for infants” (n=315; 71, 8%), “breast milk is more easily digestible than formula” (n=241; 54.9%), “breastfeeding is more comfortable for the mother than formula” (n=218; 49.7%), “breastfeeding is cheaper than formula” (n=346; 78.7%), “breastfed babies are healthier than formula-fed babies” (n=111; 25.3%).
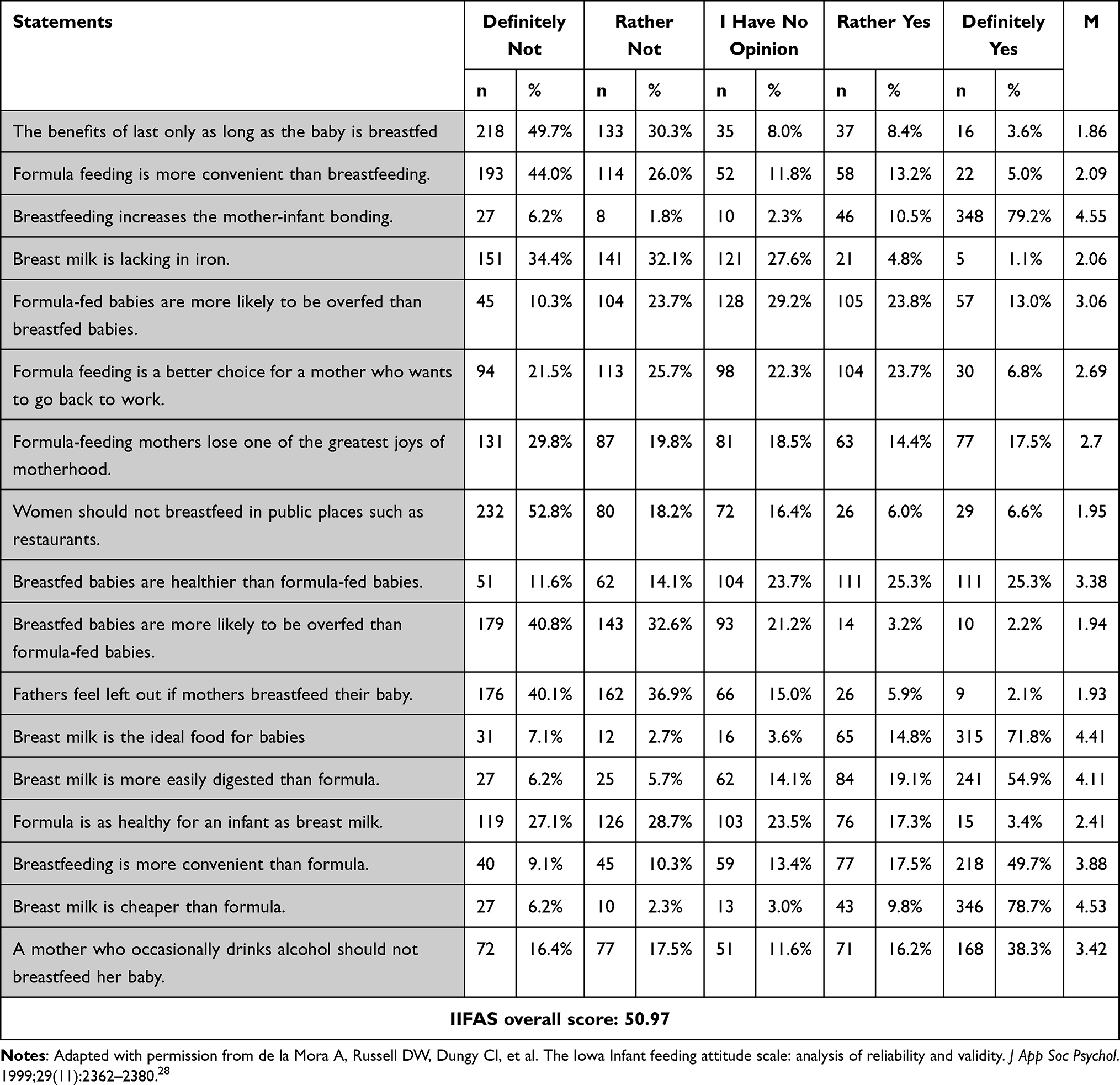 |
Table 4 Opinions of the Surveyed Women on the Given Statements Contained in the IIFAS Questionnaire (n=439) |
Based on The Iowa Infant Feeding Attitude Scale, the intensity of women’s attitudes towards breastfeeding was analysed. A positive attitude towards breastfeeding was characteristic of 315 respondents (71.8%), 95 respondents (21.6%) had a neutral attitude and 29 respondents (6.6%) had a negative attitude.
Discussion
The research conducted in this paper was aimed at understanding mothers’ attitudes towards breastfeeding when it comes to health safety resulting from professional lactation education.
According to the recommendations, lactation education for a woman and her relatives should start in the middle of pregnancy, along with information about childbirth, the postpartum period, and being a parent. Women’s attitude toward breastfeeding is formed long before pregnancy. The closest environment, childhood observations, and memories, as well as the attitude of a life partner and previous knowledge about the benefits of breastfeeding, play an important role.11,12,26,29
The lactation period is challenging for a woman. When adapting to a new situation, the social support system created by family, friends, and medical staff is extremely important. The priority of the health policy is to shape women’s attitudes that support breastfeeding and to learn how to latch the baby to the breast effectively. An extremely important element is the implementation of procedures supporting breastfeeding by the staff working in hospitals and primary health care. The components of support for lactating women include informational, practical, and emotional support.23,27,30,31
According to the recommendations of the WHO and the AAP, breastfeeding is an appropriate way to nourish the newborn and infant. A child should be exclusively breastfed for at least the first 6 months of the child’s life.3,4 In the study by Gawęda and Fica,32 which included 200 mothers, the largest group of women breastfed their child for a year or more, ie, 38% of respondents living in the city and 27% of women living in rural areas. 18% of women from rural areas and 17% from urban areas breastfed until the 6th month of a child’s life. In a report published by Szyber and Nehring-Gugulska,33 it was found that 98% of newborns are breastfed in the first month of life, while the percentage of women who breastfeed for the first six months of a child’s life is 50%, and 20% breastfed a child for a year. According to the research results obtained by Królak-Olejnik and Hordowicz,34 4% of mothers exclusively breastfed their children until the 6th month of life. On the other hand, Osuch et al35 showed in their studies that 51.2% of newborns were supplemented with modified cow’s milk mixtures. Mathew36 showed a significantly shorter duration of breastfeeding in mothers aged 15–24, which indicates that this group of women requires more attention and support in breastfeeding education. In turn, Sarki13 analyzed the relationship between mothers’ education and breastfeeding duration and found that those who completed higher education breastfed more often and longer than mothers with lower education. The results of own research in this area show that more than half of the respondents (63.8%) exclusively breastfed their newborn child, and 13.2% did so until the 6th month of the child’s life. 47.4% of the respondents continued breastfeeding beyond the age of twelve months.
Breastfeeding has benefits for both the baby and the mother. The obtained results of own research show that 67.9% of women admitted that they had a lot of knowledge on this subject. Among the most important benefits of breastfeeding, 90.4% of respondents indicated the creation of a strong bond between the child and the mother. These results are consistent with studies conducted by Cierpka et al37 in which 96.08% of the respondents considered breastfeeding to be an important element of the emotional bond with a newborn child. Similarly, in the study by Jarosz et al,38 100% of respondents consider breastfeeding to be a natural need and an essential element in building a strong bond between mother and child. It is highly probable, that this attitude of women toward breastfeeding is due to the fact that this way of feeding a child is the basis of motherhood and is a physiological process that ensures the healthy development of offspring. However, research conducted by Hairston et al39 does not confirm this thesis. Their observations showed that breastfeeding, so beneficial for the health of mother and child, has no significant impact on the parental bond. In addition, the authors are of the opinion that caution should be exercised in stating that it promotes a maternal bond. According to them, this can lead to stigma and guilt in relation to the bonding process among mothers who for various reasons do not breastfeed. At the same time, they point out that there is not enough research on this issue and suggest further research.
In own research, it was found that an equally important benefit of breastfeeding, according to 63.1% of respondents, is a faster return to pre-pregnancy weight, and for 58.8% of women, also the fact that breastfeeding reduces the risk of breast and ovarian cancer. Similar research results were obtained by Dzbuk et al40 in which 87.67% of the respondents stated that during breastfeeding, the return to pre-pregnancy body weight is faster, and 57.0% of women stated that breastfeeding reduces the risk of breast cancer.
In own research, among the benefits of breastfeeding for the child, the vast majority of respondents, ie, 94.1%, indicated support for the development of the immune system, 49.9% of respondents indicated a reduction in the frequency of bacterial infections, and 49.7% of respondents indicated a protective effect against overweight, obesity, and diabetes later in life. This is also confirmed by studies by Gebuza et al26 in which 93% of respondents indicate the positive impact of breastfeeding on the child’s immunity. On the other hand, studies by Dzbuk et al36 show that 91.67% of respondents consider breastfeeding to be important when it comes to reducing the risk of diabetes and obesity in adulthood. An attempt to obtain information on the benefits of breastfeeding for the child’s future life was also made by Klejewski et al41 who showed that, according to 77% of the respondents, breastfeeding positively affects health functioning in the later period of the child’s life.
The obtained data from own research showed that the most common reasons for discontinuation of breastfeeding were the woman’s belief that it was the right time to stop breastfeeding (30.1%), a drop in milk supply (23.2%) and the child’s unwillingness to be breastfed (21%). On the other hand, in the report by Iwanowicz-Palus and Bogusz,42 the reasons for discontinuation of breastfeeding include lack of food (36.76%), insufficient knowledge about the benefits of breastfeeding (25.9%), and illness or hospitalization of the child (13.88%). Moreover, 23.06% of women stated that breastfeeding is time-consuming. In own research, only 3.2% of respondents considered breastfeeding to be an activity that takes a lot of time.
The conducted own research showed that the vast majority of women (85%) obtained information on breastfeeding from the Internet, 58.5% from medical staff, and 49.0% from scientific and popular science literature. Similarly, in the study by Dzbuk et al40 most respondents chose the Internet (89.0%). On the other hand, research published by Cierpka et al37 shows that only 29% of respondents searched for information on breastfeeding on the Internet and other media. The key role for the respondents was played by the medical staff in the ward (80.0% of the respondents) and information contained in the scientific literature (73.0% of the respondents).
Based on the obtained results of own research, it was found that the respondents’ decision to breastfeed is influenced by public opinion. Of 439 women, 115 respondents (26.2%) felt social pressure regarding the obligation to breastfeed. Similarly, in the research conducted by Broers and Królak-Olejnik,43 almost half of the postpartum women (48.2%) felt as if they were being forced when making decisions about breastfeeding. In our own research, the surveyed women were also asked about their partner’s attitude toward breastfeeding. Most of the respondents (88.8%) assessed it as positive.
Based on the analysis of own research, it was found that 72.7% of women received support from medical staff in the field of breastfeeding. On the other hand, in the study conducted by Ulman-Włodarz et al,44 86.25% of women could count on the support of medical staff in this regard. In own research, the most common type of support provided by medical personnel (for 69.0% of respondents) turned out to be teaching how to put the baby to the breast. 44.6% of women had an educational conversation and 43.3% received information/instruction booklets. In the research presented by Broers and Królak-Olejnik,43 significantly more women (89.3%) underwent an educational conversation on lactation and 58.9% of respondents received help in latching the baby to the breast.
Women’s attitude toward breastfeeding is extremely important when deciding how to feed their own child. The Iowa Infant Feeding Attitude Scale questionnaire is a tool for assessing attitudes towards infant feeding methods, the high index of which indicates a positive attitude of women toward breastfeeding. The score obtained in own research was equal to 50.97. In a study by Inoue et al45 among Japanese mothers, the score was 54.2. On the other hand, Chen et al46 showed that Chinese women living in Australia obtained a score of 60.0, while women living in China obtained a score of 57.7. The average IIFAS score obtained in the study by Shosh et al47 for Jordanian mothers was 63.5. In Spanish mothers, the average score was 69.76 (±7.75),48 and in Hungarian mothers – 66.76 (±9.0).49 These results show that women have a neutral attitude towards breastfeeding. However, Greek women obtained higher results, indicating a positive attitude towards breastfeeding: 70.0 (±7.6).50
Professional lactation support and counseling can be crucial for initiating and continuing breastfeeding and developing positive attitudes towards breastfeeding, as Pérez-Escamilla19 highlights in her review of research from 19 countries on the impact of following the “10 Steps to Successful Breastfeeding”. Breastfeeding interventions are most effective when individual and group support are combined. Mothers appreciated face-to-face interventions, which allowed both time to discuss breastfeeding and talk about other topics outside the area of breastfeeding. Mothers spoke positively about practical and personalized breastfeeding support, especially from professionals who had previous experience in this area. They appreciated the social aspects of contact with a competent medical professional who provided them with support when they felt the need, without excessive pressure from the organizers of the intervention.31
The presented research analysis shows that the attitudes of Polish mothers obtained in our own research are not as positive as the attitudes of women in other countries. The observations of many authors in the world literature prove that mothers with a positive attitude towards breastfeeding have greater knowledge on this subject, identify this type of child feeding with health, initiate breastfeeding right after delivery, and continue to breastfeed longer than women with negative attitudes.21,25,51–54 The results of our own research showed that most of the respondents presented extensive knowledge and positive attitudes toward breastfeeding.
In Poland, the official Standard of Perinatal Care55 imposes an obligation to provide lactation counseling in the hospital and during the first weeks after delivery to all mothers by medical workers. In the hospital, newborns can be fed with formula only at the express request of the mother or on the order of a doctor for health reasons. Under health insurance, mothers have access to support from community midwives for the first 2 months after giving birth, whose task is to promote breastfeeding and provide education and support in the field of lactation. The original IIFAS questionnaire used in our study may be useful in identifying beliefs about breastfeeding that are widespread among women. Both knowledge and attitude are variables that can be modified to improve breastfeeding practices. Understanding mothers’ attitudes toward infant feeding may be useful in targeting and evaluating breastfeeding promotion efforts.
To sum up, it should be stated that promoting the most beneficial way of feeding children, ie, breastfeeding, plays an important role in building mothers’ opinions and attitudes about breastfeeding. Many of the factors that affect the duration of breastfeeding are often due to a lack of information about the benefits of breastfeeding and how to deal with breastfeeding difficulties. The decision to breastfeed is mainly made by the woman. In order for her choice to be conscious, reliable lactation knowledge obtained from medical staff is necessary, which, as shown by our own research and the research of other authors, is still in demand.56
Limitations
Own research was conducted online only. It was addressed only to a specific group of recipients, ie, women with young children. Hence, the results obtained by us allow only general conclusions regarding some aspects of the factors studied, but do not allow us to determine the cause-and-effect relationships between them. The conducted research does not fully cover the complex issue of attitudes toward breastfeeding when it comes to health safety, which may determine the effective and long-term need for breastfeeding. It would also be worth examining the attitude of the husband or partner and the immediate family toward breastfeeding. It would also be important to examine the attitudes of the medical staff regarding breastfeeding and preparation for lactation education. Hence, there is a need for further multifaceted research in this area.
Conclusions
The most common attitude towards breastfeeding expressed by women is a positive attitude. Making decisions about breastfeeding and its duration is related to women’s knowledge about breastfeeding, including professional lactation education by medical staff. Women’s declared knowledge about the advantages of breastfeeding and the support they receive from medical staff influence the development of favorable attitudes toward breastfeeding.
Institutional Review Board Statement
The study was conducted after approval of the Council of the Faculty of Health Sciences of the Medical University of Lublin (Annex No. 2 to Resolution No. 63/2018-2019 of the Council of the Faculty of Health Sciences of the Medical University of Lublin of October 22, 2020).
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on request.
Informed Consent Statement
Informed consent was obtained from all participants of the study.
Acknowledgments
The authors would like to thank Ms. Magda Jarocka, BSN, for her help in organizing the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gutierrez Dos Santos B, Perrin MT. What is known about human milk bank donors around the world: a systematic scoping review. Public Health Nutr. 2022;25(2):312–322. doi:10.1017/S1368980021003979
2. Bosi ATB, Eriksen KG, Sobko T, et al. Breastfeeding practices and policies in WHO European Region Member States. Public Health Nutr. 2016;19(4):753–764. doi:10.1017/S1368980015001767
3. Guideline: protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services. World Health Organization; 2017. Available from: https://apps.who.int/iris/handle/10665/259386.
4. World Health Organization. UNICEF Increasing Commitment to Breastfeeding Through Funding and Improved Policies and Programmes: Global Breastfeeding Scorecard 2019. New York, NY, USA; Geneva, Switzerland: World Health Organization; 2019.
5. Fewtrell M, Bronsky J, Campoy C, et al. Complementary feeding: a position paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J Pediatr Gastroenterol Nutr. 2017;64(64):119–132. doi:10.1097/MPG.0000000000001454
6. Szajewska H, Socha P, Horvath A, et al. Principles of feeding healthy infants. Position of the Polish Society of Pediatric Gastroenterology, Hepatology and Nutrition. Nutrition of healthy term infants. Recommendations of the Polish Society for Paediatrics Gastroenterology, Hepatology and Nutrition. Medical Standards/Pediatrics. 2021;18:808–822.
7. Senghore T, Omotosho TA, Ceesay O, et al. Predictors of exclusive breastfeeding knowledge and intention to or practice of exclusive breastfeeding among antenatal and postnatal women receiving routine care: a cross-sectional study. Int Breastfeed J. 2018;13(13):9. doi:10.1186/s13006-018-0154-0
8. Lis-Kuberka J, Orczyk-Pawiłowicz M. Polish women have moderate knowledge of gestational diabetes mellitus and breastfeeding benefits. Int J Environ Res Public Health. 2021;18(19):10409. doi:10.3390/ijerph181910409
9. Donda K, Maheshwari A. Human milk lipids induce important metabolic and epigenetic changes in Neonates. Clin Perinatol. 2022;49(2):331–353. doi:10.1016/j.clp.2022.02.006
10. Koletzko B, Bergmann K, Brenna JT, et al. Should formula for infants provide arachidonic acid along with DHA? A position paper of the European Academy of paediatrics and the child health foundation. Am J Clin Nutr. 2020;111(111):10–16. doi:10.1093/ajcn/nqz252
11. Baranowska B, Malinowska M, Stanaszek E, et al. Extended breastfeeding in Poland: knowledge of health care providers and attitudes on breastfeeding beyond infancy. J Hum Lact. 2018;35(2):371–380. doi:10.1177/0890334418819448
12. Gertosio C, Meazza C, Pagani S, et al. Breastfeeding and its gamut of benefits. Minerva Pediatr. 2016;68(3):201–212.
13. Sarki M, Parlesak A, Robertson A. Comparison of national cross-sectional breast-feeding surveys by maternal education in Europe (2006–2016). Public Health Nutr. 2018;22(5):848–861. doi:10.1017/S1368980018002999
14. Brahm P, Valdés V. Benefits of breastfeeding and risks associated with not breastfeeding. Rev Chil Pediatr. 2017;88(1):15–21.
15. Binns C, Lee M, Low W, et al. Guidelines for complementary feeding of infants in the Asia pacific region: APACPH public health nutrition group. Asia Pac J Public Health. 2020;32(4):179–187. doi:10.1177/1010539520931328
16. Lyons K, Ryan C, Dempsey E, et al. Brest milk, a source of beneficial microbes and associated benefits for infant health. Nutriens. 2020;12(4):1039. doi:10.3390/nu12041039
17. Cato K, Sylvén SM, Henriksson HW, et al. Breastfeeding as a balancing act - Pregnant Swedish women’s voices on breastfeeding. Int Breastfeed J. 2020;15(15):16–19. doi:10.1186/s13006-020-00257-0
18. Bartick M, Schwarz EB, Green BD, et al. Suboptimal breastfeeding in the United States: maternal and pediatric health outcomes and costs. Matern Child Nutr. 2017;13(1):e12366. doi:10.1111/mcn.12366
19. Pérez-Escamilla R, Martinez JL, Segura-Pérez S. Impact of the Baby-friendly Hospital Initiative on breastfeeding and child health outcomes: a systematic review. Matern Child Nutr. 2016;12(3):402–417. doi:10.1111/mcn.12294
20. Foudil-Bey I, Murphy MS, Keely EJ, et al. Maternal and newborn outcomes of antenatal breastmilk expression: a scoping review protocol. BMJ Open. 2020;10(5):e033101. doi:10.1136/bmjopen-2019-033101
21. Onyango S, Kimani-Murage E, Kitsao-Wekulo P, et al. Associations between exclusive breastfeeding duration and children’s developmental outcomes: evidence from Siaya county, Kenya. PLoS One. 2022;3117(3):e0265366. doi:10.1371/journal.pone.0265366
22. Kim SK, Park S, Oh J, et al. Interventions promoting exclusive breastfeeding up to six months after birth: a systematic review and meta‐analysis of randomized controlled trials. Int J Nurs Stud. 2018;80(80):94–105. doi:10.1016/j.ijnurstu.2018.01.004
23. McFadden A, Siebelt L, Marshall JL, et al. Counselling interventions to enable women to initiate and continue breastfeeding: a systematic review and meta‐analysis. Int Breastfeed J. 2019;14(14):42. doi:10.1186/s13006-019-0235-8
24. Edwards R. An exploration of maternal satisfaction with breastfeeding as a clinically relevant measure of breastfeeding success. J Hum Lact. 2018;34(1):93–96. doi:10.1177/0890334417722509
25. Russell K, Ali A. Public attitudes toward breastfeeding in public places in Ottawa, Canada. J Hum Lact. 2017;33(2):401–408. doi:10.1177/0890334417695203
26. Gebuza G, Gierszewska M, Kaźmierczak M, et al. Preparing women for breastfeeding. Problem Piel. 2010;18(4):406–412.
27. Vanderlinden K, Buffel V, Van de Putte B, et al. Motherhood in Europe: an examination of parental leave regulations and breastfeeding policy influences on breastfeeding initiation and duration. Soc Sci. 2020;9(12):222. doi:10.3390/socsci9120222
28. de la Mora A, Russell DW, Dungy CI, et al. The Iowa Infant feeding attitude scale: analysis of reliability and validity. J App Soc Psychol. 1999;29(11):2362–2380. doi:10.1111/j.1559-1816.1999.tb00115.x
29. Habte MH, Seid SJ, Alemu A, et al. The effect of unemployment and post-natal care on the exclusive breast-feeding practice of women in Ethiopia: a systematic review and meta-analysis. Reprod Health. 2022;19(1):94. doi:10.1186/s12978-022-01404-y
30. Rinaldi AEM, Azeredo CM, Pereira LA, et al. Agreement between current status and retrospective data for prevalence and duration of exclusive breast feeding from low-and middle-income countries surveys. Paediatr Perinat Epidemiol. 2019;33(6):459–466. doi:10.1111/ppe.12581
31. Victora CG, Bahl R, Barros AJ, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475–490. doi:10.1016/S0140-6736(15)01024-7
32. Gawęda A, Fica S. Natural feeding of infants and post-infant-age children from urban and rural areas on the example of the city of Rybnik and the villages of Turze and Rudy. New Pediatrics. 2012;4:71–74.
33. Szyber B, Nehring-Gugulska M. Breastfeeding in Poland - report 2015. Available from: http://femaltiker.pl/wpcontent/uploads/2015/05/Raport_Karmienie_Piersia_w_Polsce_20151.pdf.
34. Królak-Olejnik B, Hordowicz M. Assessment of the feeding of newborns and infants up to 12 months of age - a multicenter survey. Stand Med Pediatrician. 2016;13:1057–1063.
35. Osuch K, Nehring I, Nehring-Gugulska M. Breastfeeding differently - experiences of Polish mothers. Midwife. Science and Practice. 2018;4(44):10–18.
36. Mathew AC, Benny JK, Philip DM, et al. Socio-demographic and clinical correlates of exclusive breastfeeding practices up to six months of age. Nepal J Epidemiol. 2019;9(3):772–780. doi:10.3126/nje.v9i3.21179
37. Cierpka A, Żuralska R, Olszewski J, et al. Obstetricians' knowledge about breastfeeding. Care Problem. 2007;2–3(15):172–178.
38. Jarosz K, Krawczyk A, Wielgoś M, et al. Assessment of knowledge of issues related to breastfeeding among obstetricians. Gynekol Pol. 2004;75(1):27–34.
39. Hairston IS, Handelzalts JE, Lehman-Inbar T, et al. Mother-infant bonding is not associated with feeding type: a community study. BMC Pregnancy Childbirth. 2019;19(1):125. doi:10.1186/s12884-019-2264-0
40. Dzbuk E, Bakalczuk G, Padała O, et al. Breastfeeding knowledge among postpartum women. Med Og Nauk Zdr. 2016;22(4):260–263. doi:10.5604/20834543.1227606
41. Klejewski A, Urbaniak T, Bączyk G, et al. Knowledge about the advantages of natural feeding among women giving birth to their first child. Overview M.D. 2012;69:1021–1025.
42. Iwanowicz-Palus G, Bogusz R. Research report. Opinions of young mothers about lactation and the role of the midwife in promoting breastfeeding. Study 2018. Supreme Council of Nurses and Midwives Warsaw. 2018;2018:1.
43. Broers B, Królak-Olejnik B. Is breastfeeding an obligation? The role of community midwives in choosing how to feed a newborn. Położna Nauka i Practice. 2018;1:8–12.
44. Ulman-Włodarz I, Mucha A, Kwiatkowska E. Natural feeding after family childbirth. Perin Ginek wedge. 2004;1:74–78.
45. Inoue M, Binns CW, Katsuki Y, et al. Japanese mothers’ breastfeeding knowledge and attitudes assessed by the Iowa infant feeding attitudes scale. Asia Pac J Clin Nutr. 2013;22(2):261–265. doi:10.6133/apjcn.2013.22.2.08
46. Chen S, Binns CW, Liu Y, et al. Attitudes towards breastfeeding – the Iowa infant feeding attitude scale in Chinese mothers living in China and Australia. Asia Pac J Clin Nutr. 2013;22(2):266–269. doi:10.6133/apjcn.2013.22.2.09
47. Shosha GMA. The influence of infants’ characteristics on breastfeeding attitudes among Jordanian mothers. Open J Nurs. 2015;5(04):295–302. doi:10.4236/ojn.2015.54032
48. Cotelo MDCS, Movilla-Fernández M, Pita-García P, et al. Infant feeding attitudes and practices of Spanish low-risk expectant women using the IIFAS (Iowa infant feeding attitude scale. Nutrients. 2018;10(4):520. doi:10.3390/nu10040520
49. Ungváry R, Ittzés A, Bóné V, et al. Psychometric properties of the original and short Hungarian version of the Iowa infant feeding attitude scale. Int Breastfeed J. 2021;16(1):54. doi:10.1186/s13006-021-00403-2
50. Iliadou M, Lykeridou K, Prezerakos P, et al. Reliability and validity of the Greek version of the Iowa infant feeding attitude scale among pregnant women. Mater Socio-Med. 2019;31:160–165.
51. Zahra Karimi F, Sadeghi R, Maleki-Saghooni N, Khadivzadeh T. Nahid maleki-saghooni talat khadivzadeh the effect of mother-infant skin to skin contact on success and duration of first breastfeeding: a systematic review and meta-analysis. Taiwan J Obstet Gynecol. 2019;58(1):1–9. doi:10.1016/j.tjog.2018.11.002
52. Tang X, Patterson P, MacKenzie-Shalders K, et al. Workplace programmes for supporting breast-feeding: a systematic review and meta-analysis. Public Health Nutr. 2021;24(6):1501–1513. doi:10.1017/S1368980020004012
53. Kaźmierczak M, Skoczylas E, Gebuza G, et al. Assessment of women's level of knowledge about natural feeding. Care Pol. 2016;3(61):308–316.
54. Costanian C, Macpherson AK, Tamim H. Inadequate prenatal care use and breastfeeding practices in Canada: a national survey of women. BMC Pregnancy Childbirth. 2016;16(1):100. doi:10.1186/s12884-016-0889-9
55. Regulation of the Minister of Health of September 11, 2018 on the Organizational Standard of Perinatal Care. OJ 2018.1756. 2018. Available from: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20180001756/O/D20181756.pdf.
56. Cox KN, Giglia RC, Binns CW. The influence of infant feeding attitudes on breastfeeding duration: evidence from a cohort study in rural Western Australia. Int Breastfeed J. 2015;10(10):25. doi:10.1186/s13006-015-0048-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.