")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Mother-to-Child Transmission of HIV and Associated Factors Among Exposed Infants in Pastoralist Health Facilities, South Omo Zone, Ethiopia, 2020 – A Retrospective Cross-Sectional Study
Authors Tadewos K, Adimasu M , Tachbele E
Received 25 August 2021
Accepted for publication 29 November 2021
Published 9 December 2021 Volume 2021:13 Pages 1015—1023
DOI https://doi.org/10.2147/HIV.S332904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
Kidist Tadewos,1 Mekonen Adimasu,2 Erdaw Tachbele2
1Department of Nursing, Wolaita Soddo University, Wolaita Soddo, Ethiopia; 2Department of Nursing, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Mekonen Adimasu Email [email protected]
Background: Although HIV/AIDS is affecting all age groups, it is a primary cause of illness and deaths among children globally. A significant bulk of HIV infections in children under the age of 15 were as a result of vertical transmission, where it accounts for 95% of childhood HIV infections in Ethiopia.
Objective: To assess the proportion of mother-to-child transmission (MTCT) of HIV and associated factors among exposed infants on follow-up in pastoralist health facilities, South Omo, Ethiopia.
Methodology: A retrospective, cross-sectional study was employed among 228 HIV-exposed infants. Medical records of HIV-exposed infant-mother pairs in the study institutions were extracted. The confirmatory HIV serostatus of every infant was taken at the end of 24 months. Data were entered in Epi Data 4.2 version and exported to SPSS version 25 for final analysis. Multivariable logistic regression analysis was used to identify significant predictor variables at P-value < 0.05.
Results: A total of 228 records were included in the analysis. The rate of HIV transmission was 5.3% (95% CI: 2.6– 8.3%). Not receiving antiretroviral prophylaxis at birth (AOR = 5.8, 95% CI: 1.02– 33.53), absence of maternal antiretroviral prior to current pregnancy (AOR = 5.6, 95% CI: 1.14– 28.1), and mother’s advanced World Health Organization clinical stage of HIV (AOR: 10.5, 95% CI: 1.4– 81) were associated with MTCT of HIV.
Conclusion: This study identified a high proportion of MTCT among exposed infants in the study area. Not receiving antiretrovirals prior to pregnancy and advanced WHO clinical stage of HIV, and not getting antiretroviral prophylaxis at birth resulted in higher risk of MTCT of HIV. Hence, health workers and policy-makers should offer antiretroviral prophylaxis, put mothers on antiretroviral therapy and limit the stage of HIV at lower WHO clinical stages.
Keywords: HIV exposed, infant, Ethiopia
Introduction
HIV/AIDS can affect all age groups, and it is the leading cause of pediatrics morbidity and mortality in the world.1 A vast majority of HIV infections in children under the age of 15 were through mother-to-child transmission (MTCT).2 MTCT of HIV is a core public health challenge for sub-Saharan African countries. In Ethiopia, MTCT accounts for 95% of childhood HIV infections, and the risk of transmission increases significantly if the mother is untreated.2
In 2009, prior to the launch of the Global Plan, the overall mother-to-child HIV transmission rate was 28% in 21 priority countries including Ethiopia and it has been halved to 14% in 2014.3 After implementation of Option B+, around 91% of the 1.1 million women receiving antiretroviral drugs as part of the prevention of mother-to-child transmission (PMTCT).4 Around 1.4 million HIV infections among children were prevented between 2010 and 2018 due to PMTCT programs.2
Based on a global summary of AIDS epidemics in 2018, approximately 100,000 AIDS-related deaths were reported among children <15 years.5 Children living with HIV were about half as likely as pregnant women to receive treatment.3 Such great disparities should be addressed urgently, because if they are not treated, 50% of children living with HIV will die before their second birthday.6 Africa is the most seriously affected continent where the spread of HIV has been enhanced by a variety of factors, including widespread poverty, gender inequality, and health systems weakness.2,7,8
MTCT plays a huge role in new infection of children. Early diagnosis and treatment of mothers is essential because the risk of MTCT of HIV is much higher among newly infected women who are not yet diagnosed and not on treatment. The risk of HIV transmission from an untreated mother living with HIV to her child is as high as 15–45%, depending upon the presence and duration of breastfeeding.4 However, appropriate implementation of PMTCT can reduce the high transmission rate and enable us to reduce the final HIV transmission rate to 5% or less among breastfeeding women and to 2% or less among non-breastfeeding women by 2020.2
Despite the increased coverage of PMTCT in Ethiopia, a huge problem has been observed in the continuation of PMTCT care due to fear of stigma and discrimination, lack of sufficient mother-baby pair tracking mechanisms after delivery and low male partners’ involvement. As a result, MTCT rate has been shown to increase from 6% at 6 months to 18.1% after breastfeeding ends, according to national Strategic Plan for the Elimination of Mother to Child Transmission of HIV and Syphilis report. These problems become worse among pastoralist communities.
Some scholars have tried to investigate the MTCT of HIV and associated factors among HIV-exposed children. A study done in Zimbabwe found that time to initiate maternal ART was related to MTCT. It shows that starting ART preconception and during pregnancy significantly reduced the risk of MTCT throughout 18 months post-delivery by 88% and 58% respectively, compared with mothers without ARTs.9 Mothers starting ART post-delivery had a 33% reduced MTCT risk compared with mothers without ARTs.9 A finding of a Systematic Review and Meta-Analysis in Ethiopia showed that HIV-positive women with no PMTCT intervention were seven-fold more likely to have an HIV-positive child.10 From the study done at Dil Chora Referral Hospital, in Dire Dawa City Administration, infants born at home had a three times higher risk for HIV infection compared with those delivered at health institutions.11
Some studies have been conducted in relation to MTCT in Ethiopia, however almost all studies were done around urban areas with high access to education and health information, and scientific studies that can clearly show the MTCT of HIV and its associated factors among exposed children in the pastoralist region of Ethiopia are limited. This area is unique because it is one of the least developed areas of the country with poor infrastructure and mainly inhabited by pastoralist and agro-pastoralist populations, including more than 16 ethnic groups with lifestyles and cultures different from those of the rest of the country and with poor access to health information.
Therefore, the main aim of this study was to assess MTCT of HIV and associated risk factors among exposed infants in pastoralist health facilities, South Omo Zone, Ethiopia, 2020.
Methods
Study Design, Area and Period
This study was conducted in South Omo, one of the 14 zones in South Nation Nationality and Peoples’ Region (SNNPR), Ethiopia. The zone is one of the areas with lowest economic growth and dominated by pastoralist livelihood. It is 750 km south of Addis Ababa and 550 km away from the regional capital, Hawassa. The zone is located in 4.430–6.460 North latitude and 35.790–36.060 South longitude. It is a home for 16 tribes, with magnificent cultural diversity and afro-traditionalism.
Institutional-based retrospective cross-sectional study was conducted among records of exposed infant-mother pairs who were on follow-up at PMTCT clinics in two selected public health facilities in South Omo from September 2014 to August 2018. The confirmatory HIV serostatus of every infant was determined at the end of 24 months follow-up.
Eligibility Criteria
All records of exposed infant-mother pairs who were on follow-up care at PMTCT clinics in selected health facilities in South Omo and registered from September 2014 to September 2019. HIV-exposed infants without confirmatory tests and infant-mother pairs who had no complete data were excluded.
Sample Size Determination, Sampling Technique and Study Variables
The sample size was calculated using a single population proportion formula assuming P as 15.7% from a study conducted in Dire Dawa, Ethiopia,11 and 5% margin of error with 95% confidence interval, and 10% of non-response rate was added. Finally, a total of 228 medical records of infant-mother pairs were selected using simple random sampling.
HIV sero-status of the baby at the end of the follow-up period, 24 months, was the main outcome variable, while socio-demographic characteristics, mother’s antenatal care (ANC) follow-up, illness during pregnancy, ARV prophylaxis, ART, CD4 count, pregnancy plan, place of delivery and mode of delivery, infant feeding practice, infant’s ARV prophylaxis, infant’s age at which DBS was done were considered as the main predictor variables.
Method of Data Collection, Processing, and Analysis
The data collection was conducted by health professionals using structured data extraction sheets. The data were collected by reviewing mothers’ PMTCT and exposed infants’ care and follow-up records at PMTCT clinics. The collected data were checked for completeness then coded and entered in Epi Data 4.2 version and final analysis was done using SPSS version 25. Descriptive statistics (frequency, mean and percentage) were used to describe each individual variable. Binary logistic regression was employed to determine predictor variables. A p value of less than 0.05 was considered as significant to determine association of variables. Normality of data was checked using graphical methods, such as histogram, and Q-Q scatter plot. Multi-collinearity of independent variables was checked using Variance Inflation Factor (VIF).
Ethics Approval
This study was conducted in accordance with the Declaration of Helsinki. Ethical clearance was obtained from the School of Nursing and Midwifery Research Ethics Committee (REC), Addis Ababa University with a protocol number-063/20/SNM. Permission was obtained from each health institution. Informed consent was waived due to the retrospective nature of the review. However, privacy and confidentiality of study participants were maintained by ensuring that the data abstraction form was anonymous and by protecting our personal computers with strong passwords.
Results
Socio-Demographic Characteristics of the Mothers and HEIs
This study included 228 exposed infants and their mothers who enrolled to PMTCT clinics in five consecutive years (September 2014 to August 2018) in South Omo public health facilities. The age of the participant mothers ranged from 17 to 37 with the mean ±SD being 26.13±5.304 years. The majority of them (59.6%) were aged between 25 and 37 years old. Concerning the level of education, nearly half (47.4%) were illiterate. More than 60% of infants were female. Of the total, 94.7% of HIV-exposed infants (HEIs) had delivered at gestational age ≥ 37 weeks and 95.2% of HEIs had ≥ 2500 g birth weight (Table 1). Socio-demographic characteristics of HEIs and their mothers, in South Omo health facilities, Ethiopia, 2020 (N = 228).
 |
Table 1 Shows Socio-Demographic Characteristics of HEIs and Their Mothers, in South Omo Health Facilities, Ethiopia, 2020 (n = 228) |
PMTCT Intervention Given for the Mother
From the total 228, 144 (63.2%) of mothers attended antenatal care during current pregnancy, of which 98 (68%) had three or more visits. Eighty-four (36.8%) had no ANC follow-up. From the total mothers who participated in the study, 170 (74.6%) were already on ART follow-up at enrollment. The remaining 25.4% were newly diagnosed during their current pregnancy with gestational age at the time of diagnosis ranging from 6–39 weeks and the mean gestational age at the time of diagnosis was 23.60 weeks. For 217 (90.8%) of the mothers a syphilis test was done during the prenatal, intrapartum or postnatal period, out of which 18 (8.3%) reported as positive and 199 (91.7%) were negative; the remaining 21 were not tested for syphilis at all (Table 2).
 |
Table 2 Shows PMTCT Interventions Given for the Mother in South Omo Health Facilities, South Ethiopia, 2020 (n = 228) |
Two hundred and eleven (92.5%) of the mothers had given birth at a health institution and 7.5% at home, 75.9% had a spontaneous vaginal delivery (SVD). Of the total mothers who participated in the study, 70.2% of them were on ARV prior to their current pregnancy. For 82.5% of the mothers, ART was initiated during this pregnancy, more than three-quarters of them had good adherence to ART. Out of these, 161 (70.6%) were taking highly active ART treatment. Twenty percent of the couples (n = 33/162) were sero-discordant. The majority, i.e. 148/170 (87.1%) of mothers, had a CD4 count ≥351/mm3. Except one participant mother, the others had no recorded comorbidity during pregnancy. Regarding WHO stage, more than half (61.4%) of the mother were stage I. Only 30 (13.2%) of the mothers were prescribed cotrimoxazole prophylactic therapy (CPT), of which 26 had good adherence to CPT. The proportion of mothers who tested positive for tuberculosis (TB) was 5.3% (n=12). Almost all (99.6%) of breast-feeding mothers had normal breasts (Table 2). PMTCT interventions were given for the mothers in South Omo health facilities, South Ethiopia, 2020 (n = 228).
PMTCT Intervention Given for the Infant
Concerning infant feeding practice in the first 6 months, 227 (99.6%) of HEIs were on exclusive breast feeding, while only 0.4% received mixed feeding. HEIs were given NVP syrup after birth (96.5%), the remainder were not given NVP or CPT. DNA/PCR test was done for 76.8% of the HEIs by 6 weeks of age, 94.6% of HEIs were discharged as negative after 18 months or cessation of breast feeding (Table 3). PMTCT interventions were given for the infants in Jinka town health facilities, south Ethiopia, 2020 (n = 228).
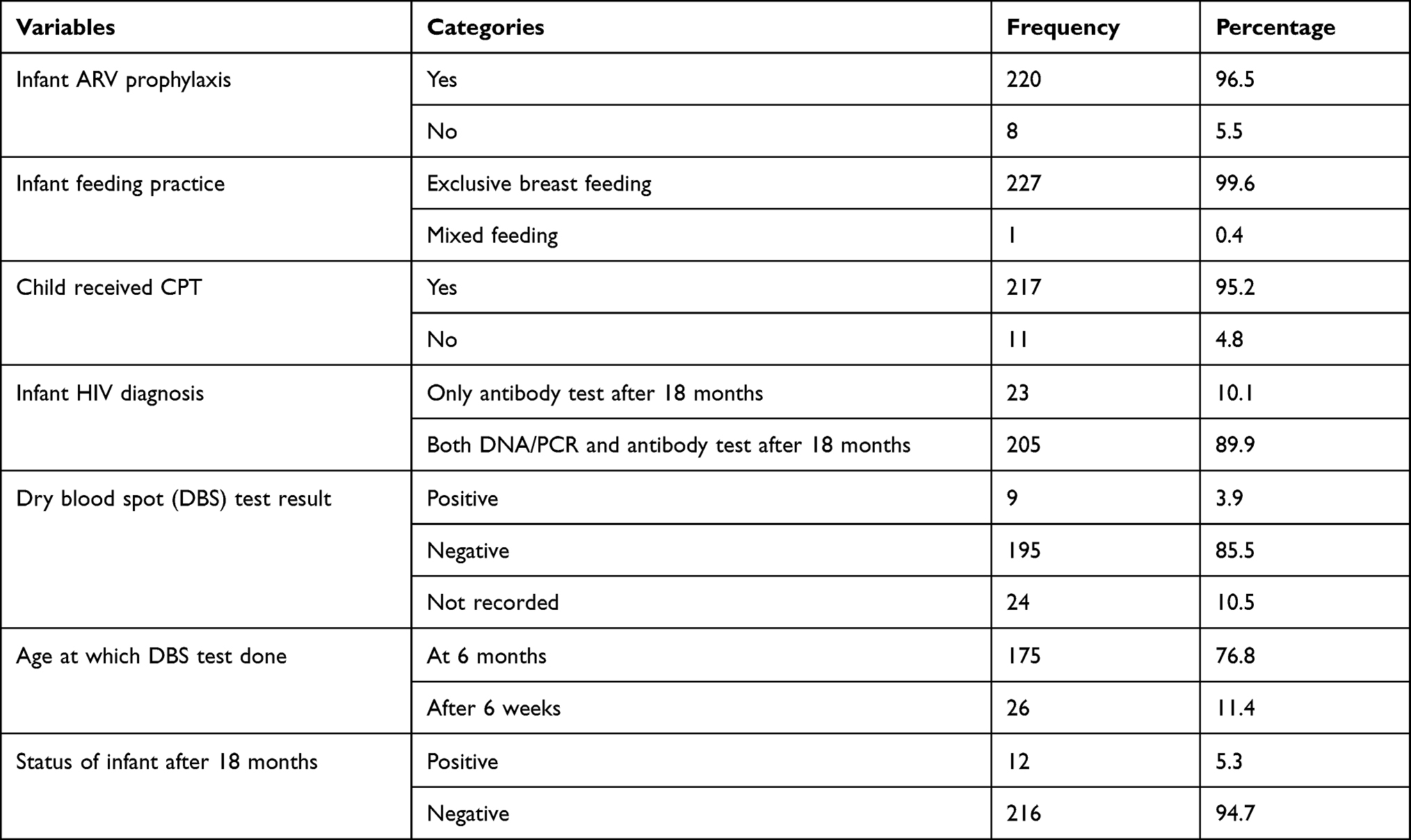 |
Table 3 Shows PMTCT Intervention Given for the Infants in Jinka Town Health Facilities, South Ethiopia, 2020 (n = 228) |
Rate of Mother-to-Child Transition of HIV and Associated Factors
The overall rate of MTCT was about 5.3%. In the bivariate analysis, factors associated with MTCT of HIV (p-value <0.2) were mothers on ARV prior to current pregnancy, maternal ART adherence, gestational age at the time of delivery, marital status, child CPT at birth, infant ARV prophylaxis at birth, ANC follow-up, time in which the mother knew her sero-status, WHO stage of the mother when enrolled to PMTCT and initial CD4 count of the mother when enrolled to PMTCT.
In multivariable logistic regression, infants who did not receive ARV prophylaxis at birth (AOR = 5.8, 95% CI: 1.02–33.53), mothers who were not on ARV prior to current pregnancy (AOR = 5.6, 95% CI: 1.14–28.1), and mother’s advanced WHO clinical stage of HIV at enrollment to PMTCT (AOR: 10.5; 95% CI: 1.4–81) were found to be the most important significant determinants of mother-to-child HIV transmission (Table 4).
 |
Table 4 Shows Factors Associated with MTCT of HIV in South Omo Health Facilities, South Ethiopia, 2020 (n = 228) |
Discussion
According to this study, the overall rate of MTCT was 5.3%. This indicates that MTCT still affects a huge number of children even though the WHO and the Ethiopian federal ministry of health planned and designed to eliminate MTCT.
The rate of MTCT in this study was high compared with studies conducted in Rwanda, Malawi, Adama, Ethiopia and Dessie, Ethiopia (1.58%, 3.7%, 0.4% and 3.8%, respectively).12–15
The possible discrepancy might be poor socio-economic status, poor access to health information and the pastoral nature of living in the study area. However, MTCT was low compared with studies conducted in India (7.8%),16 Brazil (6.6%),17 Eastern Cameroon (11.6%),18 and other parts of Ethiopia.11,19–21 The possible reason for discrepancies from studies done in India and Brazil might be the sample size (478 and 1200 respectively) and this might increase the proportion of children affected by MTCT of HIV. Additionally, studies in Brazil and Cameron were done starting from 1999 to 2011. At this time since PMTCT (especially option B+) was not applied fully, MTCT might be higher.
In this study, not receiving antiretroviral prophylaxis at birth, absence of maternal antiretrovirals prior to current pregnancy, and mother’s advanced WHO clinical stage of HIV at enrollment to PMTCT were significantly associated factors at a p-value of <0.05.
In this study, HEIs who did not receive antiretroviral prophylaxis at birth were 5.9 times more likely to be positive than infants who received antiretroviral prophylaxis after birth (AOR: 5.9; 95% CI: 1.04–33.5). The scientific explanation is that it is an established and accepted fact by the WHO and other health organizations that antiretroviral prophylaxis has a high viral suppression effect. Similar studies in Ethiopia have also supported infant antiretroviral prophylaxis as an independent predictor of MTCT of HIV, however, studies in India and Brazil do not show a significant association between nevirapine prophylaxis at birth and infant HIV status.11,12,16,17,19 The discrepancy of the result might be the study period, studies in Brazil and India were done before 15 years and the impact of nevirapine prophylaxis might not be implemented effectively by that time.
Mother’s advanced WHO clinical stage of HIV at enrollment to PMTCT was significantly associated with MTCT of HIV. Mothers who were at WHO clinical stage III at enrollment were over 10 times more likely to transmit HIV to their infants than mothers who enrolled to PMTCT care at stage I (AOR: 10.5; 95% CI: 1.4–81). The possible scientific explanation for this might be that mothers in advanced clinical stage might develop different opportunistic infections, and they may become immunodeficient as well having a high viral load and the transmission rate may increase. This study is in line with studies done in Jimma and Addis Ababa, Ethiopia.22,23 The possible justification for similarity might be that advanced WHO stage of HIV (higher viral load) in the mother will increase the risk of MTCT whether the mothers reside in urban or pastoralist region. According to the findings of this study, mothers who were diagnosed positive but not on antiretrovirals prior to their current pregnancy had more than five-fold risk to have an HIV-positive child than mothers who were on antiretrovirals prior to current pregnancy (AOR: 5.68; 95% CI: 1.15–28.1). The scientific explanation for this association might be that taking antiretrovirals prior to pregnancy may suppress the viral load and prevent transmission of HIV to the fetus. In addition to this, mothers who took antiretrovirals priory to pregnancy may have good awareness about how to take them and may have good adherence to the protocol. This study is consistent with those conducted in Dessie and Gonder, Ethiopia;12,21 some studies do not include taking antiretroviral prior to pregnancy as co-factor.22,23
Limitation
Since the data were collected from routine medical records, some variables were missed in records which might be associated with MTCT.
Conclusion
The study reports a higher rate of MTCT of HIV infection among exposed infants in the study area relative to the goal set by the WHO and the Ethiopian federal ministry of health. Children born from mothers who did not take maternal antiretrovirals prior to current pregnancy, and with advanced WHO clinical stage of HIV at enrollment to PMTCT, had higher risk of mother-to-child transmission of HIV infection. Additionally, children who did not receive antiretroviral prophylaxis at birth had a higher risk of MTCT of HIV. Hence, health workers and policymakers should stress in offering antiretroviral prophylaxis for neonates at birth; put mothers on antiretroviral therapy before delivery; and limit the stage of HIV at lower WHO stages of HIV to prevent MTCT of HIV infection.
Abbreviations
AIDS, Acquired Immunodeficiency Syndrome; ANC, Antenatal care; AOR, Adjusted Odds Ratio; ART, Anti-Retroviral Therapy; ARV, Antiretroviral; CPT, Co-trimoxazole preventive therapy; DBS, Dry blood spot; HEIs, HIV exposed infants; HAART, Highly Active Anti-Retroviral Therapy; HIV, Human Immunodeficiency Virus; MTCT, Mother to child transmission; PMTCT, Prevention of mother-to-child transmission; WLHIV, women living with HIV.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Informed Consent
This study was conducted in accordance with the Declaration of Helsinki. Ethical clearance was obtained from the Institutional Review Board (IRB) of Addis Ababa University, College of health sciences, school of nursing and midwifery with a protocol number-063/20/SNM. Permission was obtained from each health institution to review records of HIV-positive mothers and their infants. Informed consent was waived due to the retrospective nature of the review. However, privacy and confidentiality of study participants were maintained by making the data abstraction form anonymous and protecting our personal computers by strong password.
Acknowledgments
We are indebted to Addis Ababa University, College of Health Sciences for its financial support for data collection. We are thankful to the staff of South Omo health office, Jinka General Hospital, Millennium Health Center for their cooperation. The authors are also thankful to the supervisors and data collectors. Finally, we would like to acknowledge Addis Ababa University institutional repository that stores the thesis and allows as retrieving this article from the thesis. The source of this article is a thesis found in Addis Ababa University Institutional repository at: http://etd.aau.edu.et/handle/123456789/23993?show=full.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by Addis Ababa University, Ethiopia. The funder had no role in the study design, data collection, and analysis, interpretation of data, the decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. World Health Organization. Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV; 2015. Available from: www.who.int.
2. Avert. Prevention of mother-to-child transmission (PMTCT) of HIV; 2018.
3. UNAIDS. 2015 PROGRESS REPORT ON THE GLOBAL PLAN. Towards the elimination of new HIV infections among children and keeping their mothers alive; 2015. Available from: https://www.unaids.org/sites/default/files/media_asset/JC2774_2015ProgressReport_GlobalPlan_en.pdf.
4. UNAIDS. Prevention gap report; 2016. Available from: https://www.unaids.org/sites/default/files/media_asset/2016-prevention-gap-report_en.pdf.
5. UNAIDS. Global HIV & AIDS statistics — fact sheet; 2021. Available from: https://www.unaids.org/en/resources/fact-sheet.
6. UNAIDS. Start Free Stay Free AIDS Free. 2017 progress report; 2017. Available from: https://www.unaids.org/sites/default/files/media_asset/JC2923_SFSFAF_2017progressreport_en.pdf.
7. Ethiopian Federal Ministry of Health. National guidelines for comprehensive HIV prevention, care and treatment; 2017.
8. UNAIDS. UNAIDS DATA 2017. State of the AIDS epidemic; 2017. Available from: https://www.unaids.org/sites/default/files/media_asset/20170720_Data_book_2017_en.pdf.
9. Dinh TH, Mushavi A, Shiraishi RW, et al. Impact of timing of antiretroviral treatment and birth weight on mother-to-child human immunodeficiency virus transmission: findings from an 18-month prospective cohort of a nationally representative sample of mother-infant pairs during the transition from Option A to Option B+ in Zimbabwe. Clin Infect Dis. 2018;66(4):576–585. doi:10.1093/cid/cix820
10. Kassa GM. Mother-to-child transmission of HIV infection and its associated factors in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2018;18(1):216. doi:10.1186/s12879-018-3126-5
11. Wudineh F, Damtew B. Mother-to-child transmission of HIV infection and its determinants among exposed infants on care and follow-up in Dire Dawa City, Eastern Ethiopia. AIDS Res Treat. 2016;2016:3262746. doi:10.1155/2016/3262746
12. Yitayew YA, Bekele DM, Demissie BW, Menji ZA. Mother to child transmission of HIV and associated factors among HIV exposed infants at public health facilities, Dessie Town, Ethiopia. HIV AIDS. 2019;11:343–350. doi:10.2147/HIV.S221409
13. Mugwaneza P, Lyambabaje A, Umubyeyi A, et al. Impact of maternal ART on mother-to-child transmission (MTCT) of HIV at six weeks postpartum in Rwanda. BMC Public Health. 2018;18:1248. doi:10.1186/s12889-018-6154-6
14. Barr BA, van Lettow M, Van Oosterhout JJ, et al. National estimates and risk factors associated with early mother-to-child transmission of HIV after implementation of option B +: a cross-sectional analysis. Lancet HIV. 2018;3018(18):1–8.
15. Chaka TE, Abebe TW, Kassa RT. Option B+ prevention of mother-to-child transmission of HIV/AIDS service intervention outcomes in selected health facilities, Adama town, Ethiopia. HIV AIDS. 2019;11:77–82. doi:10.2147/HIV.S192556
16. Potty RS, Sethumadhavan R, Isac S, Washington R, Washington R. Incidence, prevalence and associated factors of mother-to-child transmission of HIV, among children exposed to maternal HIV, in Belgaum district, Karnataka, India. BMC Public Health. 2019;19(1):386. doi:10.1186/s12889-019-6707-3
17. De Andrade SD, Sabidó M, Marcelo Monteiro W, Canellas L, Prazeres V, Schwartz Benzaken A. Mother-to-child Transmission of HIV From 1999 to 2011 in the Amazonas, Brazil. Pediatr Infect Dis J. 2016;35(2):189–195. doi:10.1097/INF.0000000000000966
18. Noubiap J, Bongoe A, Demanou S. Mother-to-child transmission of HIV: findings from an early infant diagnosis program in Bertoua, Eastern Cameroon. Pan Afr Med J. 2013;15:65.
19. Obsa S, Dabsu R, Ejeta E. Rate of mother to child transmission of HIV and factors associated among HIV exposed infants in Oromia Regional State, Ethiopia: retrospective study. Egypt Pediatr Assoc Gaz. 2018;66(3):61–65. doi:10.1016/j.epag.2018.07.002
20. Koye DN, Zeleke BM. Mother-to-child transmission of HIV and its predictors among HIV-exposed infants at a PMTCT clinic in northwest Ethiopia. BMC Public Health. 2013;13:398. doi:10.1186/1471-2458-13-398
21. Berhan Z, Abebe F, Gedefaw M, Tesfa M, Assefa M, Tafere Y. Risk of HIV and associated factors among infants born to HIV positive women in Amhara region, Ethiopia: a facility based retrospective study. BMC Res Notes. 2014;7:876. doi:10.1186/1756-0500-7-876
22. Beyene GA, Dadi LS, Mogas SB. Determinants of HIV infection among children born to mothers on prevention of mother to child transmission program of HIV in Addis Ababa, Ethiopia: a case control study. BMC Infect Dis. 2018;18(1):327. doi:10.1186/s12879-018-3217-3
23. Birlie B, Diriba T, Sisay K, Gurmessa A, Seyoum D, Tadesse M. Mother to child HIV transmission and its predictors among HIV-exposed infants: a retrospective follow-up study in Southwest Ethiopia. J AIDS Clin Res. 2016;7(9). doi:10.4172/2155-6113.1000605
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.