")
Back to Journals » Clinical Epidemiology » Volume 14
Mortality Among Danish Patients with a Hospital Diagnosis of Overweight or Obesity Over a 40-Year Period
Authors Gribsholt SB, Farkas DK, Thomsen RW , Richelsen B, Sørensen HT
Received 1 December 2021
Accepted for publication 18 February 2022
Published 14 March 2022 Volume 2022:14 Pages 309—325
DOI https://doi.org/10.2147/CLEP.S350459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Eyal Cohen
Sigrid Bjerge Gribsholt,1,2 Dóra Körmendiné Farkas,3 Reimar Wernich Thomsen,3 Bjørn Richelsen,1,2 Henrik Toft Sørensen3
1Department of Endocrinology and Internal Medicine, Aarhus University Hospital, Aarhus, Denmark; 2Steno Diabetes Center, Aarhus University Hospital, Aarhus, Denmark; 3Department of Clinical Epidemiology, Aarhus University Hospital and Aarhus University, Aarhus, Denmark
Correspondence: Sigrid Bjerge Gribsholt, Tel +4561651148, Email [email protected]
Purpose: Data on long-term mortality among patients with hospital-diagnosed overweight/obesity are limited. Thus, we aim to examine 40-year mortality among patients with hospital-diagnosed overweight/obesity, including cause-specific deaths, secular time trends, and potential effect modification by age, comorbidity, and socioeconomic factors.
Patients and Methods: From national registries, we identified all Danes with a first hospital-based overweight/obesity diagnosis (N=331,185), 1979– 2018, and constructed an age- and gender-matched general population comparison cohort (N=1,655,925). We computed mortality rates (MRs) per 1000 person-years and adjusted mortality rate ratios (aMRRs) with 95% confidence intervals (CIs), using Cox regression with adjustment for comorbidities and educational level. We performed stratified analyses on age, comorbidities, and socioeconomic factors.
Results: The overall aMRR was 1.70 (95% CI: 1.68– 1.72) for patients with overweight/obesity, mainly due to diabetes and other endocrine diseases (aMRR=2.68 [95% CI: 2.57– 2.81]), cardiovascular (aMRR=1.95 [95% CI: 1.91– 1.98]), and respiratory diseases (aMRR=1.83 [95% CI: 1.77– 1.89]). The 1– 10-year aMRR decreased from 2.06 (95% CI: 2.01– 2.11) in 1979– 1989 to 1.29 (95% CI: 1.26– 1.32) in 2000– 2009. We found effect modification by age: age 18 to < 30 years: aMRR=2.44 (95% CI: 2.24– 2.66) vs age ≥ 70 years: 1.35 (95% CI: 1.33– 1.37); comorbidities: baseline comorbidities: aMRR=1.13 (95% CI: 1.10– 1.15) vs no comorbidities: aMRR=1.83 (95% CI: 1.80– 1.85); and educational level: high educational level: aMRR=1.81 (95% CI: 1.74– 1.88) vs low educational level: aMRR=1.70 (95% CI: 1.67– 1.72).
Conclusion: Patients with overweight/obesity had a substantially increased long-term mortality, mainly due to diabetes, cardiovascular, and respiratory diseases. The excess mortality decreased during recent decades. Age, comorbidities, and socioeconomic factors modified the association.
Keywords: cohort study, epidemiology, mortality, multi-morbidity, obesity, overweight, socio-economy
Introduction
Obesity prevalence has increased dramatically during recent decades and is a global pandemic.1,2 Obesity is associated with multi-morbidity, diminished quality of life, and increased global health costs.3 General population studies have reported increased mortality among persons with obesity vs persons with normal weight.4–8
The aetiology of obesity and its clinical consequences is complex and multifactorial. Physiological consequences of obesity such as systemic low-grade inflammation, oxidative stress, and endothelial dysfunction9 may contribute to the important associations between obesity and risk of diabetes,10 cardiovascular disease,11–13 several cancers,14–16 infections,17 and neuropsychiatric diseases.18,19 People in lower socioeconomic positions live shorter lives, and they spend more years with disability.20 Socioeconomic factors may most likely modulate the mortality risk in patients with overweight/obesity.21
Short-term studies have indicated a protective effect of obesity on in-hospital mortality in relation to severe illness; the so-called “obesity paradox”,22–25 but a few studies with a median follow-up time of 1.5 to 4 years have shown that the apparent protective effect of obesity may decrease over time.25–27 The clinical implications of these long-term changes in risk remain poorly understood. Attempts to clarify these issues have been hampered by small cohorts, lack of co-morbidity data, and lack of information on causes of death. Such data are needed to understand and potentially improve the clinical course after a hospital diagnosis of obesity. A hospital contact which result in registration of an overweight/obesity discharge diagnosis code by a caregiver indicates that the overweight/obesity status may be of significant importance for the patient’s future health. A hospital contact is thus a window of risk assessment and an opportunity to initiate preventive interventions that may improve patients’ long-term health and reduce their mortality.
We conducted a nationwide hospital-based study to examine overall and cause-specific mortality in a large cohort of patients with an inpatient or outpatient hospital contact leading to registration of an overweight/obesity diagnosis code, compared with a general population age-and gender-matched cohort. We also examined secular time trends and potential effect modification by comorbidities and socioeconomic factors.
Materials and Methods
Study Design, Data Sources, and Setting
This cohort study drew on the entire Danish population, with 8.8 million residents between January 1, 1979 and December 31, 2018. In Denmark, health care services are free and tax supported28 and all health care contacts are registered in the Danish health care registries. Civil registration numbers (unique identifiers encoding sex and birth date) are used to track all medical records for individual patients.29 We included data from The Danish Civil Registration System (CRS),29 The Danish National Patient Registry (DNPR),30 The Danish Register of Causes of Death (DRCD),31 and The Integrated Database for Labour Market Research (IDLMR).32 Further details on data sources are provided in Supplementary Materials.
Patients with Overweight or Obesity
From the CRS and the DNPR, we identified patients with a first inpatient or outpatient diagnosis code for overweight/obesity recorded at any Danish hospital during 1979–2018 (Supplementary Data 1 and 2). We did not include patients with a diagnosis code of overweight/obesity recorded during 1977–1978, to ensure at least a 2-year comorbidity history before the diagnosis. We obtained complete hospital histories for all persons beginning in 1977 and linked the resulting dataset to records in the CRS. For patients with secondary diagnosis codes of overweight/obesity, we tabulated the 25 most common primary diagnosis codes (Supplementary Data 3).
Population Comparison Cohort
We used the CRS and the DNPR to generate a population-based comparison cohort. For each patient with a first overweight/obesity record in the DNPR, we randomly frequency matched five comparison persons from the general population of Denmark, using the CRS linked to the DNPR, which together combine sex, birth date, and a complete hospital discharge history for the entire Danish population. The five comparisons were frequency matched on the date of the corresponding index patient’s first overweight/obesity record, among all general population members with the same sex and year of birth as the index patient. We performed the matching with replacement.33 We defined the hospital contact/matching date for patients with overweight/obesity and persons in the comparison cohort as the index date. People in the comparison cohort were not registered with a hospital diagnosis of overweight/obesity before or at the index date, but they may have had other hospital contacts, and they may be diagnosed with overweight/obesity later in the study period. If a person in the comparison cohort subsequently was diagnosed with overweight/obesity, he or she joined the overweight/obesity cohort.34
Effect Modification
Age, comorbidities, and socio-economic factors may impact mortality risk and modify the association between obesity and mortality.3 We obtained information on age from the CRS. We used the DNPR data to summarize each participant’s (patient with overweight/obesity or comparison) available lifetime comorbidity history, based on the Charlson Comorbidity Index (CCI).35 We grouped participants according to their overall level of comorbidity, defined as a CCI score of 0 (none), 1–2 (moderate), and 3+ (high) (Supplementary Data 4).
We obtained information on the following diseases separately, due to their potential impact on mortality risk: cancer, diabetes, stroke, acute myocardial infarction, and heart failure (Supplementary Data 1). From the IDLMR we obtained information on yearly personal gross income and highest level of education achieved. We divided patients into groups according to low, intermediate, high, or very high income and according to basic education, youth education, or higher education.
Mortality and Causes of Death
We identified the date of death and the underlying cause of death from the DRCD, grouped by ICD-8/ICD-10 diagnosis codes (Supplementary Data 5).
Statistical Analyses
We followed all participants from the index date and until date of death, emigration, or December 31, 2018, whichever came first. We characterized patients with overweight/obesity and persons in the comparison cohort in terms of sex, age categories, and time period of diagnosis. We computed the median age with interquartile range (IQR) at inclusion and median follow-up time for both cohorts. We calculated the absolute mortality risk and the mortality rates (MRs) per 1000 person-years. We used Cox proportional-hazards regression analysis to compute mortality rate ratios (MRRs; specifically, hazard ratios) as measures of relative mortality risk, comparing patients with overweight/obesity to persons in the comparison cohort. In the Cox regression analysis, we dissolved the matching and instead included the matching factors as covariates in the model as the matching factors did not remain balanced over time. In addition to sex, age, and time period, we adjusted for prior diagnoses up to the index date of cancer, diabetes, stroke, acute myocardial infarction, or heart failure, educational level, and income.
To examine for effect modification, we repeated the adjusted MRR (aMRR) analyses, stratified by age (18 to <30, 30 to <40, 40 to <50, 50 to <60, 60 to <70, and ≥70 years), sex (female/male), time period (1979–1989, 1990–1999, 2000–2009, and 2010–2018), baseline CCI score (none, moderate, high), cancer (yes/no), diabetes (yes/no), stroke (yes/no), acute myocardial infarction (yes/no), heart failure (yes/no), education level (basic education/youth education/higher education), income (low/intermediate/high/very high), type of hospital contact (inpatient/outpatient), and type of diagnosis code (primary vs secondary and overweight vs obesity).
For the time periods 1979–1989, 1990–1999, 2000–2009, and 2010–2018 we present the cumulative mortality graphically according to age group. We computed MRs, crude MRR, and aMRRs using Cox proportional-hazards regression analysis for the time periods 0–364 days, 1–10 years, 11–20 years, 21–30 years, 31–40 years, and 0–40 years after the index date. We used log-log plots to test the proportionality of hazards visually and found that the assumptions were fulfilled for each of the follow-up periods.
Finally, we calculated MRs and crude and adjusted MRRs for the most frequent causes of death and compared cause-specific mortality rates in the two cohorts. We tested for secular trends using the Wald χ2 test with a significance level of <0.0001.
We conducted all statistical analyses using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Descriptive Data
In the overweight/obesity cohort (N = 331,185 patients; 2,997,960 person-years; median follow-up time 7.7 years) and the comparison cohort (N = 1,655,925 persons; 16,407,090 person-years; median follow-up time 8.1 years), 75.6% were female and the median age was 45 years (Table 1). More patients in the overweight/obesity cohort vs the comparison cohort had a CCI score of ≥1: 38.1% vs 17.3%, respectively. Frequent comorbidities included diabetes (14.2% vs 2.0%), cancer (5.9% vs 4.1%), and heart failure (4.2% vs 0.8%). Patients with overweight/obesity had a lower educational level than persons in the comparison cohort: basic education: 35.1% vs 26.0%.
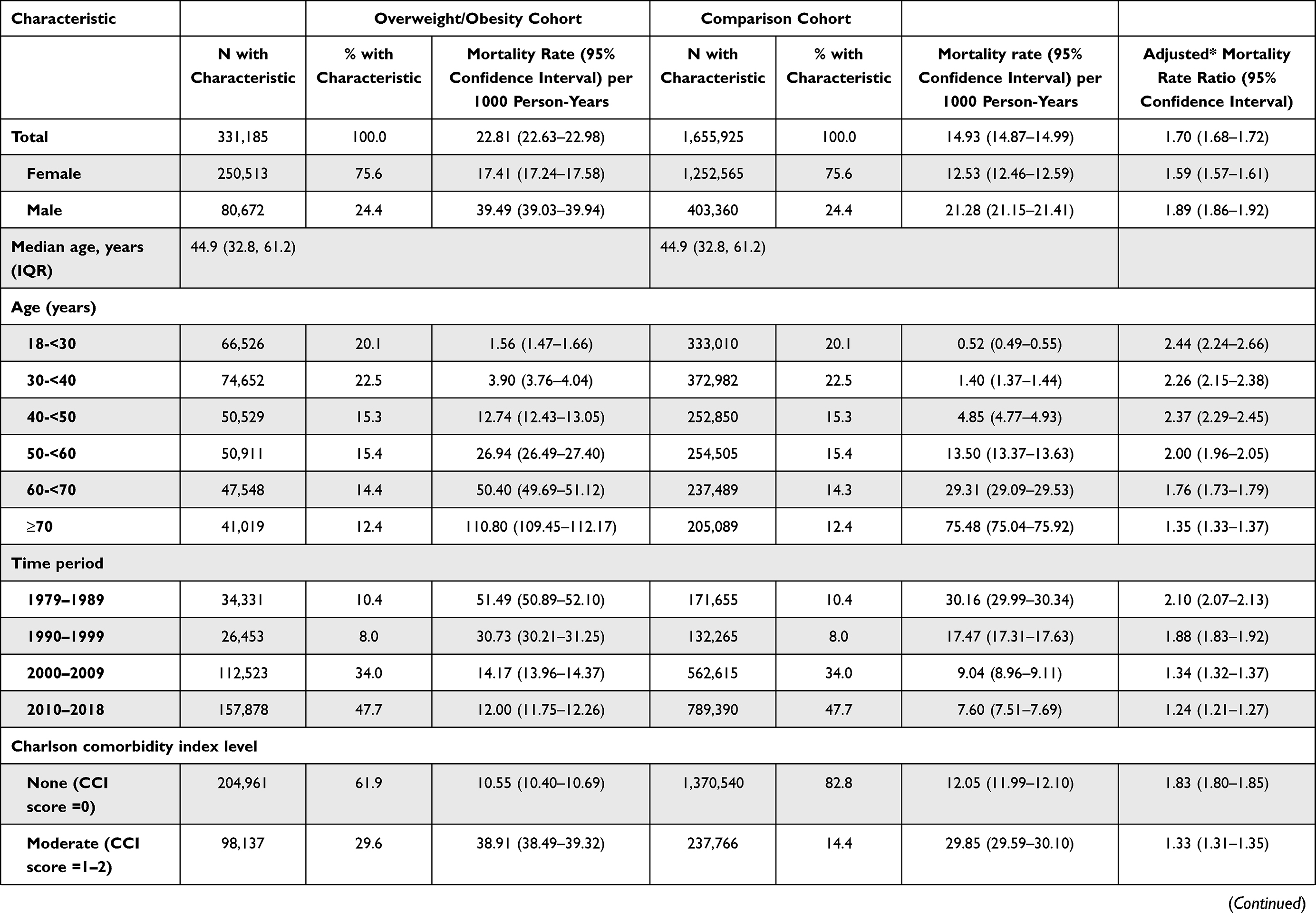 | 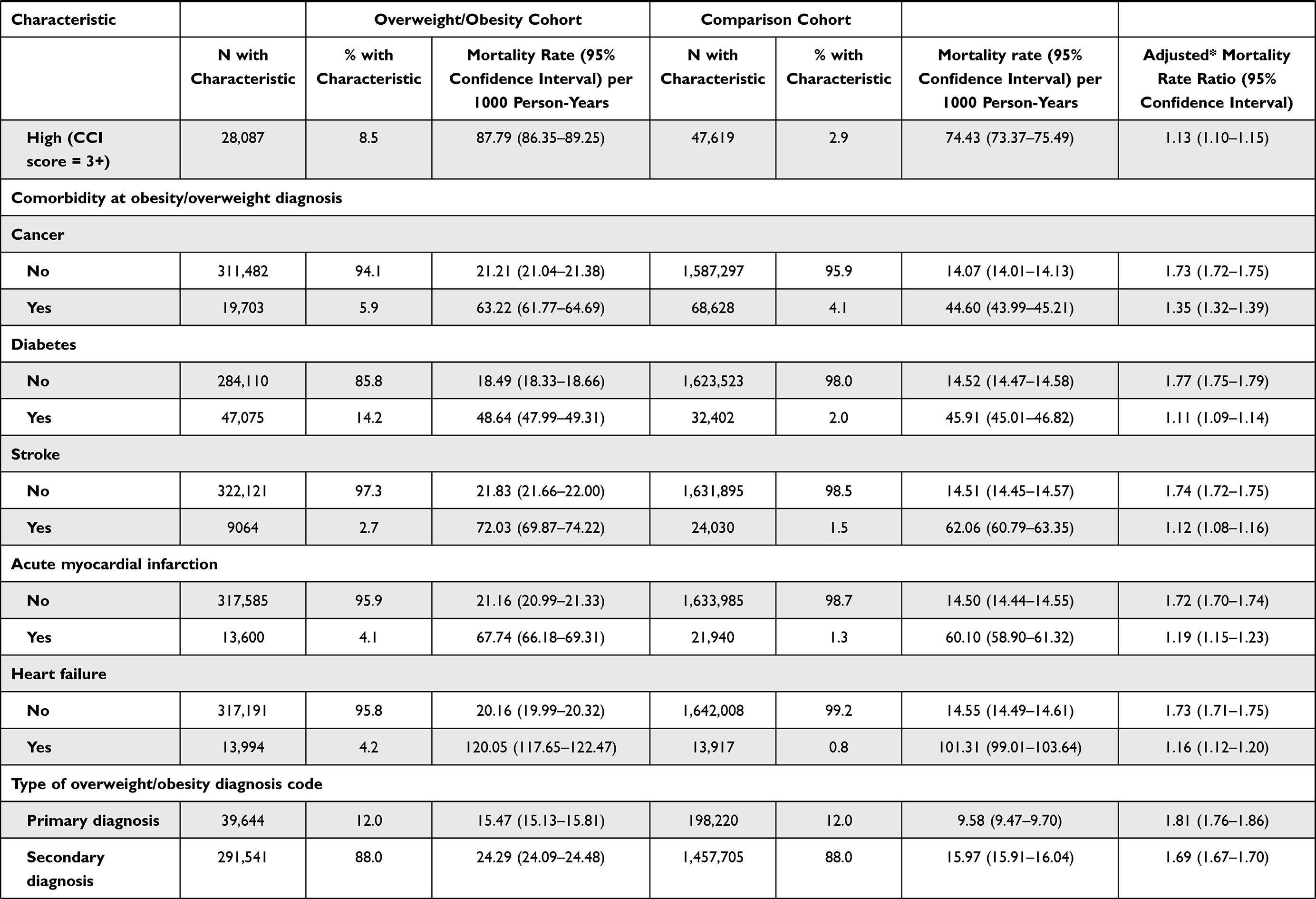 | 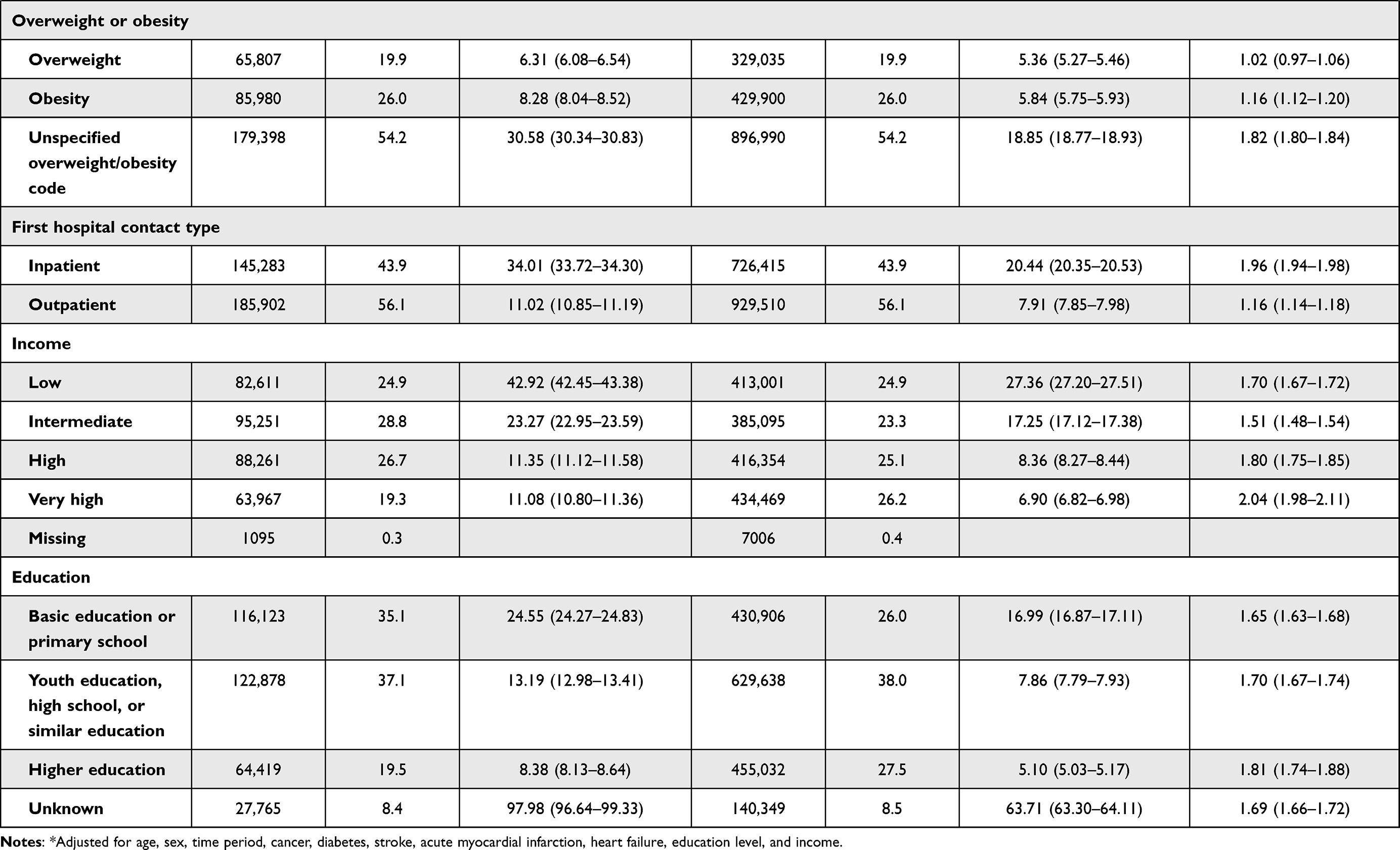 |
Table 1 Characteristics of Patients with Overweight/Obesity and the General Population Cohort, and Mortality Rates and Rate Ratios Overall and by Subgroups |
In total, 291,541 (88.0%) patients had a secondary diagnosis code of overweight/obesity (Supplementary Data 5), with almost half (145,283; 43.9%) having an inpatient hospital code. We found a large increase in the absolute number of patients with overweight/obesity during our study period, with 157,878 of all patients (47.7%) diagnosed in the final 9 years.
Overall 40-Year Mortality
The absolute mortality risks over the maximum 40 years of follow-up were 75.6% (95% CI: 74.6–76.6%) in the overweight/obesity cohort vs 70.3% (95% CI: 69.8–70.7%) in the comparison cohort (Supplementary Data 7).
The MRs and the MRRs for the overweight/obesity cohort were markedly higher than for the comparison cohort during the entire study period (Table 2). The overall MR was 22.81 (95% CI: 22.63–22.98) per 1000 person-years for the overweight/obesity cohort vs 14.93 (95% CI: 14.87–14.99) per 1000 person-years for the comparison cohort. The overall MRR was 2.22 (95% CI: 2.20–2.24), when adjusting for matching factors only, and 1.70 (95% CI: 1.68–1.72) when adjusting for matching factors, baseline comorbidities, and educational level (Supplementary Data 6).
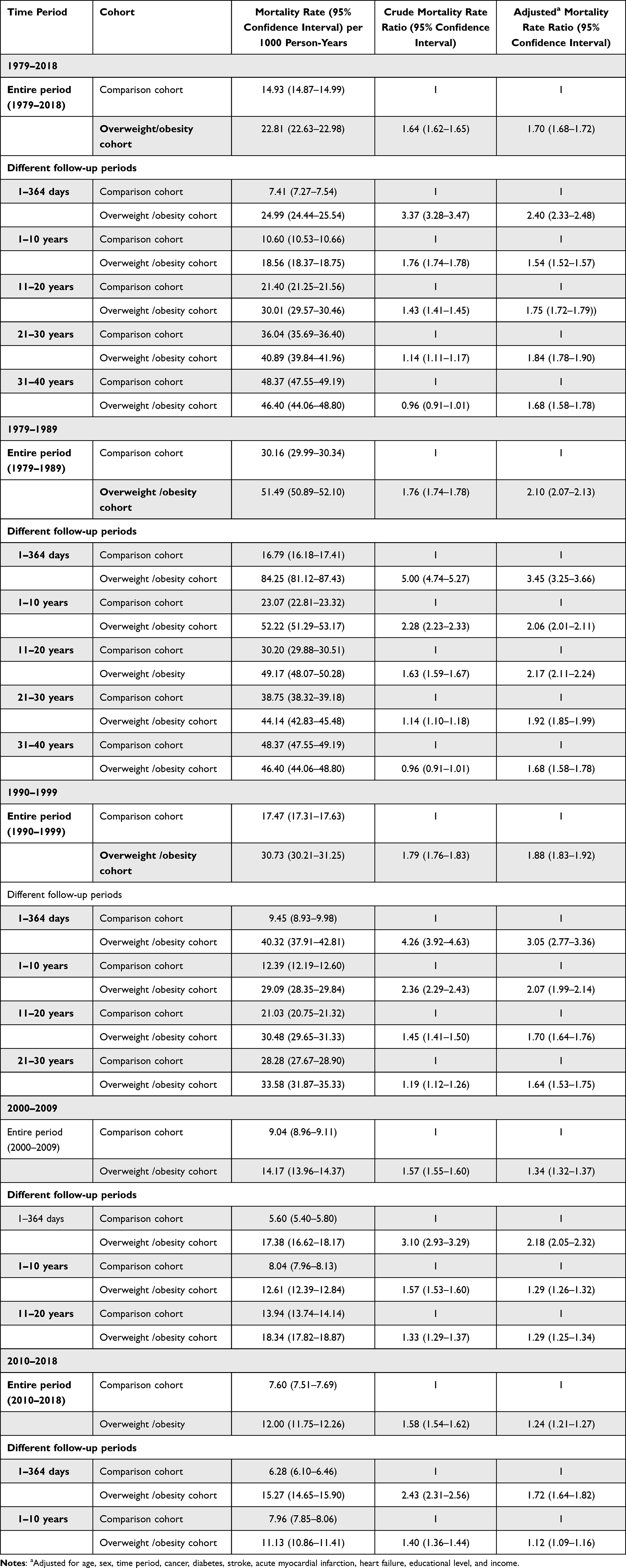 |
Table 2 Mortality Rates and Rate Ratios Associated with Overweight/Obesity, by Different Time Periods and Durations of Follow-Up |
1-Year Mortality
During the first year of follow-up, the absolute mortality risks were 2.5% (95% CI: 2.4–2.5%) in the overweight/obesity cohort vs 0.7% (95% CI: 0.7–0.8%) in the comparison cohort (Supplementary Data 7). The aMRR was high during the first year following an overweight/obesity diagnosis: 2.43 (95% CI: 2.36–2.51) (Table 2). The 1-year aMRR declined for patients with overweight/obesity from the beginning of the study period in 1979–1989 (aMRR = 3.45 [95% CI: 3.25–3.66]) and until 2010–2018 (aMRR = 1.72 [95% CI: 1.64–1.82]) (Table 2, Figure 1).
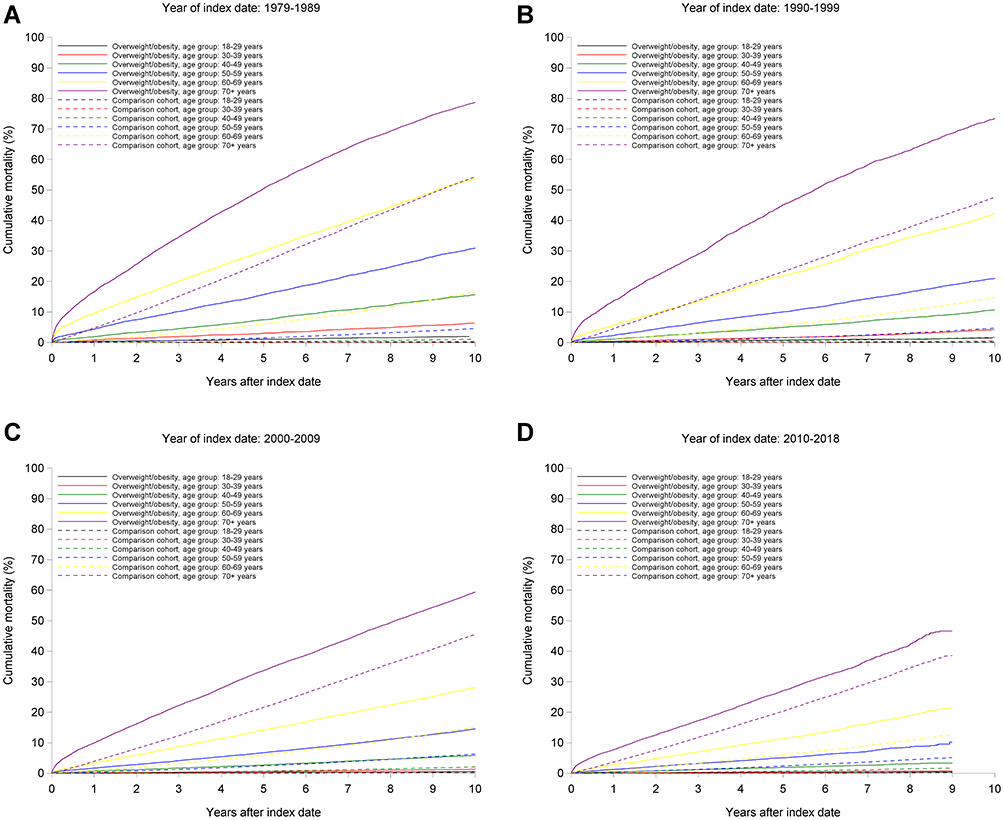 |
Figure 1 Mortality in the overweight/obesity cohort and in the comparison cohort. (A) Mortality in the overweight/obesity cohort and in the comparison cohort. Year of index date: 1979–1989. (B) Mortality in the overweight/obesity cohort and in the comparison cohort. Year of index date: 1990–1999. (C) Mortality in the overweight/obesity cohort and in the comparison cohort. Year of index date: 2009–2009. (D) Mortality in the overweight/obesity cohort and in the comparison cohort. Year of index date: 2010–2018. |
Relative Mortality Beyond 1 Year and Secular Time Trends
The aMRRs of the overweight/obesity cohort vs the comparison cohort remained elevated during the entire follow-up (1–10 year aMRR = 1.54 [95% CI: 1.52–1.57]; 11–20 year aMRR = 1.75 [95% CI: 1.72–1.79]; 21–30 year aMRR = 1.84 [95% CI: 1.78–1.90]; and 31–40 year aMRR = 1.68 (95% CI: 1.58–1.78]) (Table 2, Figure 1). The longest-term aMRRs represent exclusively patients diagnosed early in our 40-year study period, and thus potentially mix time period of diagnosis effects with follow-up duration effects. When following subcohorts, the 1–10-year aMRRs clearly decreased over time (from 2.06 [95% CI: 2.01–2.11] in 1979–1989 to 1.29 [95% CI: 1.26–1.32] in 2000–2009). P-values for secular time trends were < 0.0001.
Causes of Death
Compared with the general population, patients with obesity/overweight had markedly higher all-time death rates for diabetes and other endocrine diseases (aMRR= 2.68 [95% CI: 2.57–2.81]). The absolute number of deaths and the aMRR were high for cardiovascular diseases: aMRR=1.95 [95% CI: 1.91–1.98], respiratory diseases: aMRR=1.83 [95% CI: 1.77–1.89]; and cancer: aMRR=1.44 [95% CI: 1.41–1.46] (Table 3). The aMRRs were also increased due to skin diseases (aMRR=2.81 [95% CI: 2.21–3.58]), genitourinary diseases (aMRR = 2.34 [95% CI: 2.18–2.52), gastrointestinal diseases (aMRR= 2.14 [95% CI: 2.05–2.23]), and infectious diseases (aMRR=1.59 [95% CI: 1.52–1.66]) (Table 3). Patients with overweight/obesity had an aMRR of 1.28 (95% CI: 1.19–1.36) for death due to accidents, an aMRR of 1.60 (95% CI: 1.44–1.78) for suicide, and an aMRR for death due to psychiatric diseases of 0.90 (95% CI: 0.84–0.95).
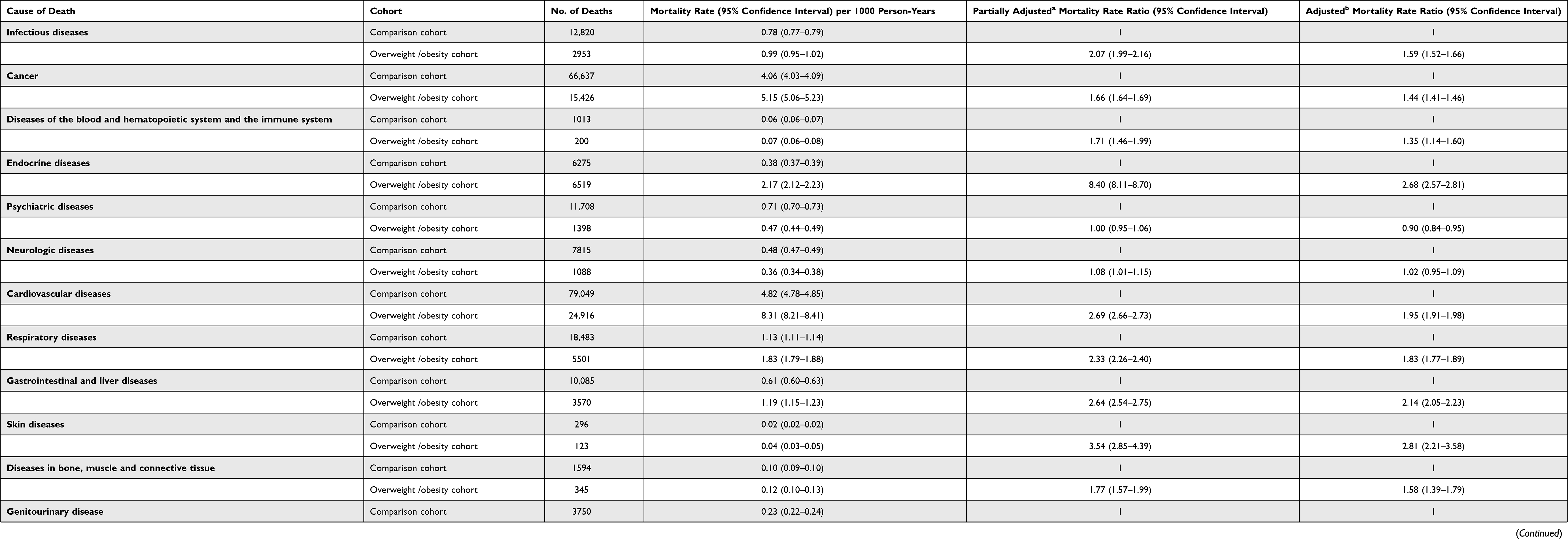 |
Table 3 Mortality Rates and Rate Ratios for Specific Causes of Death Among Patients with Overweight/Obesity and Persons in the General Population Cohort, 1979–2018 |
Stratified Analyses
The impact of overweight/obesity decreased with increasing age: age 18 to <30 years: aMRR=2.44 (95% CI: 2.24–2.66) and ≥70 years; aMRR=1.35 (95% CI: 1.33–1.37) (Table 1). Overweight/obesity had a smaller relative impact on mortality in those with pre-existing comorbidities: CCI score=3+: aMRR: 1.13 (95% CI: 1.10–1.15) vs those without comorbidities: aMRR: 1.83 (95% CI: 1.80–1.85). Findings were similar for diabetes: patients with diabetes: aMRR=1.11 (95% CI: 1.09–1.14) vs patients without diabetes: aMRR=1.77 (95% CI: 1.75–1.79), for cancer; patients with cancer: aMRR=1.73 (95% CI: 1.72–1.75) vs patients without cancer; aMRR=1.36 (95% CI: 1.32–1.40), and stroke: patients with stroke: aMRR=1.74 (95% CI: 1.72–1.75) vs patients without stroke aMRR=1.12 (95% CI: 1.08–1.16) (Table 1). The aMRR was 1.59 (95% CI: 1.57–1.61) women and 1.89 (95% CI: 1.86–1.92) for men, and the aMRR for was 1.96 (95% CI: 1.94–1.98) patients with an inpatient diagnosis code and 1.16 (95% CI: 1.14–1.18) for patients with an outpatient diagnosis code.
The aMRR was higher among patients with obesity (1.16 [95% CI: 1.12–1.20]), than for those with overweight (1.02 [95% CI: 0.97–1.06]).
The aMRR associated with overweight/obesity was 1.81 (95% CI: 1.74–1.88) among patients with a higher education compared to 1.65 (95% CI: 1.63–1.68) among those with basic education (Table 1). Among patients with a very high income, the aMRR was 2.04 (95% CI: 1.98–2.11) vs 1.70 (95% CI: 1.67–1.72) among those with a low income.
Discussion
Principal Findings
In this hospital-based 40-year cohort study, we found that inpatients and outpatients with a hospital diagnosis for overweight/obesity had a 1.7-fold increased relative mortality risk compared with that expected from the general population. Over the past four decades we observed gradual reductions in excess 10-year mortality for patients with overweight/obesity. We showed that findings from general population studies on increased diabetes, cardiovascular disease, and cancer risk associated with overweight/obesity could be extended to a hospital care setting. Other aspects of our findings are novel, including the strong association of overweight/obesity with mortality due to respiratory, genitourinary, and skin diseases. We also provide evidence of a large relative impact of obesity on mortality in people of young age, without pre-existing comorbidities, and with high income and a high level of education.
Overall Mortality Risk Was Elevated, but Declined Over the Last Decades
Although the findings of increased long-term mortality risk associated with hospital-diagnosed overweight/obesity are similar to those of general population studies, direct comparisons are difficult, as comorbidities, lifestyle, and other confounding factors impacting mortality may be more frequent in hospitalized persons.4–8,36 Our hospital-based population is an important subset of the general population, and it is plausible that the same social, clinical, and biological mechanisms mediate the increased long-term mortality in the two populations. Previous hospital-based studies have mainly examined short-term mortality, with conflicting results.22–25,27 We found that mortality risk was increased during the entire follow-up period, including the first year of follow up.
In parallel with rising obesity rates, population-level cardiovascular disease incidence and mortality have decreased over the past decades.37 The decline in mortality associated with overweight/obesity since 1979 may be attributable to earlier and better primary prevention and treatment of the overweight/obesity-related comorbidities the general population.37–40 However, increased longevity may be at the expense of a greater proportion of life lived with comorbidities including cardiovascular disease.41 Since the overweight/obesity hospital coding has improved over time, less severe cases of overweight/obesity with lower mortality risk may have been registered in the latest decades. Furthermore, obesity status may change with higher age and long follow-up time. For these reasons, this encouraging result needs to be interpreted carefully.
Effect Modification by Age, Comorbidities, and Socio-Economic Factors
Our finding of a relatively higher relative mortality associated with overweight/obesity among younger persons is in agreement with previous studies.42,43 Our findings add to the evidence that increasing age and baseline comorbidities dilute the association between overweight/obesity and mortality.2,42,43
The association between adverse socioeconomic factors and increased mortality is well established.44 We found a greater relative impact of overweight/obesity on mortality in people with high income and a high level of education. In patients with high socioeconomic status, other comorbidities may be less frequent, leading to a greater isolated impact of obesity.44 In general, the association between socioeconomic status and obesity has weakened over time with the increasing prevalence of obesity.45
New Aspects of Cause-Specific Mortality Risk
In the absence of broad evidence summarizing cause-specific mortality outcomes after hospital admission for overweight/obesity, we analysed the long-term mortality according to major disease categories. Thus, we provide an analysis of the main causes of death that may be associated with overweight/obesity. For the cause-specific mortality from cardiovascular disease, diabetes, and cancer, our risk estimates were in the same direction and of greater magnitude than those derived from previous general population studies.4–8 Our results provide new evidence of hospital-diagnosed overweight/obesity as a harbinger of mortality due to infectious diseases,46–49 respiratory diseases,5,50–52 genitourinary diseases,53 trauma,54,55 and skin diseases,47,56 which have been inconsistently reported in the previous literature.
A large body of research has identified a bidirectional association between obesity and mental disorders,18,57–60 possibly following from inflammation, stigmatization, and adverse lifestyle and self-care, or side effects of antipsychotic drugs.18,61–63 We found no increased mortality due to psychiatric diseases, but our results support an association between overweight/obesity and suicide risk.62,63
Possible Biological Mechanisms
Several interacting factors might explain the increased mortality risk. Overweight/obesity exerts adverse impacts on systemic low-grade inflammation, oxidative stress, insulin resistance, lipid profile, and endothelial dysfunction secondary to adipose tissue-derived pro-inflammatory mediators.9 This leads to a greater risk of diabetes, hypertension, cardiovascular disease, and site-specific cancers. These above-mentioned factors may also, together with decreased lung function, increase susceptibility to infections and their severity.9
Obesity-associated restrictive ventilation and decreased residual volumes, in addition to inflammation, may exacerbate respiratory diseases.64,65 This may outweigh the potentially protective effect of a lower smoking prevalence in patients with overweight/obesity.47 Diagnostic delay and sub-optimal treatment of these comorbidities may still occur in patients with overweight/obesity, due to stigmatization,66 social isolation,67 and related mental disorders.18
Methodological Considerations
The accuracy of our findings depends on the data quality, and our study has several limitations in addition to its strengths. A main limitation is its reliance on overweight/obesity diagnosis codes with no information on exact Body Mass Index (BMI) values. Whereas the completeness of overweight/obesity coding in the DNPR is low: 11% of patients with a BMI ≥25 kg/m2 measured in hospital may receive an overweight/obesity diagnosis code, the positive predictive value of an overweight/obesity diagnosis was 88%.68 The low likelihood of being assigned an overweight/obesity code despite elevated BMI may raise a concern of selection bias. For example, women may more likely be assigned an overweight/obesity code than men (76% of our patients were female). If women had a higher likelihood of having even mild cases of overweight/obesity registered, eg according to the Danish pregnancy care program where routine BMI screening is mandatory,69 while predominantly the more severe cases of overweight/obesity were registered and coded for men, this may have contributed to the aMRR from overweight/obesity being lower in women than men.
Similar mechanisms may have biased the observed aMRRs for overweight/obesity diagnoses downwards in the most recent years (possibly due to increased completeness in the registration of milder cases) versus earlier study years. Furthermore, elderly patients with comorbidity may have a higher likelihood of being assigned a code for mild overweight/obesity, due to their frequent health care encounters. It is possible that predominantly more severe cases of overweight/obesity were registered in young people with otherwise little comorbidity. Such a bias may have contributed to the overweight/obesity aMRRs being lower in older persons with comorbidity than in younger people without comorbidity.
Unfortunately, our registry data did not allow us to further examine the exact BMI associated with overweight/obesity diagnoses. However, we made extensive adjustment for pre-existing comorbidities and type of hospital contact or diagnosis code, when comparing any associations between overweight/obesity and mortality. If for example more severe cases of overweight/obesity were registered for men than for women due to differential coding, men with overweight/obesity would also appear more comorbid on average, and these differences would then be adjusted for in our mortality analyses.
The most commonly used overweight/obesity ICD diagnosis codes were unspecific codes (ie ICD-10 E660 Obesity due to excess calories, or E669 Obesity not specified elsewhere), and thus data on the exact degree and clinical severity of obesity was unfortunately unavailable. Moreover, onset of overweight/obesity likely occurs many years before a hospital contact and thus prevalent and incident cases may be mixed, and left truncation may be a concern.70 Our risk estimates may be conservative, due to both the code’s low sensitivity and the increasing prevalence of overweight and obesity over time in Denmark’s general population, with recent survey data suggesting that 34% are overweight and 17% are obese.71
Finally, all deaths are registered in the DRCD, as a person cannot be declared dead unless a diagnosis code is provided and reported to the registry.31 However, the diagnosis code is assigned by a physician who might not have known the patient’s medical history thoroughly.
Conclusion
Our study raises the need to rethink and revise the clinical handling of obesity, as societal prevention of obesity and its complications is fundamental. A hospital contact is a potential window of opportunity to initiate clinically preventive interventions like treatment of hypertension, hypercholesterolemia, and diabetes, and lifestyle changes.72 Taking these actions would reduce the burden of obesity. Socioeconomic factors may be treated as a target for local and global health strategies, with important implications for mortality.
Importantly, excess mortality declined during the 40-year study period, providing evidence that the prevention and treatment of obesity-related comorbidities are effective and should be extended.
Abbreviations
BMI, body mass index; CCI, the Charlson comorbidity index; CRS, The Danish Civil Registration System; DNPR, The Danish National Patient Registry; DRCD, The Danish Register of Causes of Death; ICD-8, Eighth Revision of the International Classification of Diseases; ICD-10, Tenth Revision of the International Classification of Diseases; IQR, interquartile range; MR, mortality rates; MRR, mortality rate ratios.
Ethics
Data in the Danish public registries are available to researchers. According to Danish legislation, purely registry-based studies do not require informed consent or separate approval from the Danish Scientific Ethics Committee. Data permission: The study was reported to the Danish Data Protection Agency (registration number: KEA–2015–57–0002, 605).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Obesity and overweight; 2018. Available from: http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
2. Collaboration NCDRF. Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet. 2016;387(10026):1377–1396. doi:10.1016/S0140-6736(16)30054-X
3. Mackenbach JP. Nordic paradox, Southern miracle, Eastern disaster: persistence of inequalities in mortality in Europe. Eur J Public Health. 2017;27(suppl_4):14–17. doi:10.1093/eurpub/ckx160
4. Di Angelantonio E, Bhupathiraju SN, Wormser D. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016;388(10046):776–786. doi:10.1016/S0140-6736(16)30175-1
5. Whitlock G, Lewington S, Sherliker P, et al. Body-mass index and cause-specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet. 2009;373(9669):1083–1096. doi:10.1016/S0140-6736(09)60318-4
6. Flegal KM, Kit BK, Orpana H, Graubard BI. Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA. 2013;309(1):71–82. doi:10.1001/jama.2012.113905
7. Collaborators GBDO, Afshin A, Forouzanfar MH, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377(1):13–27.
8. Bhaskaran K, Dos-Santos-Silva I, Leon DA, Douglas IJ, Smeeth L. Association of BMI with overall and cause-specific mortality: a population-based cohort study of 3·6 million adults in the UK. Lancet Diabetes Endocrinol. 2018;6(12):944–953. doi:10.1016/S2213-8587(18)30288-2
9. Holt R, Cockram C, Flyvbjerg A, Goldstein B. Obesity and Diabetes. Textbook of Diabetes. John Wiley & Sons, Incorporated; 2017.
10. Czech MP. Insulin action and resistance in obesity and type 2 diabetes. Nat Med. 2017;23(7):804–814. doi:10.1038/nm.4350
11. Lyall DM, Celis-Morales C, Ward J, et al. Association of body mass index with cardiometabolic disease in the UK Biobank: a Mendelian Randomization Study. JAMA cardiol. 2017;2(8):882–889. doi:10.1001/jamacardio.2016.5804
12. Dicker D, Feldman BS, Leventer-Roberts M, Benis A. Obesity or smoking: which factor contributes more to the incidence of myocardial infarction? Eur J Intern Med. 2016;32:43–46. doi:10.1016/j.ejim.2016.03.029
13. Janszky I, Romundstad P, Laugsand LE, Vatten LJ, Mukamal KJ, Morkedal B. Weight and weight change and risk of acute myocardial infarction and heart failure - the HUNT Study. J Intern Med. 2016;280(3):312–322. doi:10.1111/joim.12494
14. Wang J, Yang DL, Chen ZZ, Gou BF. Associations of body mass index with cancer incidence among populations, genders, and menopausal status: a systematic review and meta-analysis. Cancer Epidemiol. 2016;42:1–8. doi:10.1016/j.canep.2016.02.010
15. Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer. 2004;4(8):579–591.
16. Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet. 2008;371(9612):569–578. doi:10.1016/S0140-6736(08)60269-X
17. Kaspersen KA, Pedersen OB, Petersen MS, et al. Obesity and risk of infection: results from the Danish Blood Donor Study. Epidemiology. 2015;26(4):580–589. doi:10.1097/EDE.0000000000000301
18. Moussa OM, Ardissino M, Kulatilake P, et al. Effect of body mass index on depression in a UK cohort of 363 037 obese patients: a longitudinal analysis of transition. Clin Obes. 2019;9(3):e12305. doi:10.1111/cob.12305
19. Rajan TM, Menon V. Psychiatric disorders and obesity: a review of association studies. J Postgrad Med. 2017;63(3):182–190. doi:10.4103/jpgm.JPGM_712_16
20. Jagger C, Gillies C, Moscone F, et al. Inequalities in healthy life years in the 25 countries of the European Union in 2005: a cross-national meta-regression analysis. Lancet. 2008;372(9656):2124–2131. doi:10.1016/S0140-6736(08)61594-9
21. Livingston EH. Reimagining obesity in 2018: a JAMA theme issue on obesity. JAMA. 2018;319(3):238–240. doi:10.1001/jama.2017.21779
22. Barba R, Marco J, Ruiz J, et al. The obesity paradox in stroke: impact on mortality and short-term readmission. J Stroke Cerebrovasc Dis. 2015;24(4):766–770. doi:10.1016/j.jstrokecerebrovasdis.2014.11.002
23. Flanders WD, Eldridge RC, McClellan W. A nearly unavoidable mechanism for collider bias with index-event studies. Epidemiology. 2014;25(5):762–764. doi:10.1097/EDE.0000000000000131
24. Sakr Y, Alhussami I, Nanchal R, et al. Being overweight is associated with greater survival in ICU patients: results from the intensive care over nations audit. Crit Care Med. 2015;43(12):2623–2632. doi:10.1097/CCM.0000000000001310
25. Sharma A, Lavie CJ, Borer JS, et al. Meta-analysis of the relation of body mass index to all-cause and cardiovascular mortality and hospitalization in patients with chronic heart failure. Am J Cardiol. 2015;115(10):1428–1434. doi:10.1016/j.amjcard.2015.02.024
26. Hoogeveen EK, Rothman KJ, Voskamp PWM, et al. Obesity and risk of death or dialysis in younger and older patients on specialized pre-dialysis care. PLoS One. 2017;12(9):e0184007. doi:10.1371/journal.pone.0184007
27. Terada T, Forhan M, Norris CM, et al. Differences in short- and long-term mortality associated with BMI following coronary revascularization. J Am Heart Assoc. 2017;6(4). doi:10.1161/JAHA.116.005335
28. Schmidt M, Schmidt SAJ, Adelborg K, et al. The Danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
29. Schmidt M, Pedersen L, Sorensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
30. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
31. Helweg-Larsen K. The Danish register of causes of death. Scand J Public Health. 2011;39(7 Suppl):26–29. doi:10.1177/1403494811399958
32. Petersson F, Baadsgaard M, Thygesen LC. Danish registers on personal labour market affiliation. Scand J Public Health. 2011;39(7 Suppl):95–98. doi:10.1177/1403494811408483
33. Heide-Jørgensen U, Adelborg K, Kahlert J, Sørensen HT, Pedersen L. Sampling strategies for selecting general population comparison cohorts. Clin Epidemiol. 2018;10:1325–1337. doi:10.2147/CLEP.S164456
34. Rothman KJ, Greenland S, Lash TL. Modern Epidemiology. Lippincott Williams And Wilkins; 2012.
35. Thygesen SK, Christiansen CF, Christensen S, Lash TL, Sorensen HT. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based Danish National Registry of Patients. BMC Med Res Methodol. 2011;11:83. doi:10.1186/1471-2288-11-83
36. Ju S-Y, Lee J-Y, Kim D-H. Association of metabolic syndrome and its components with all-cause and cardiovascular mortality in the elderly: a meta-analysis of prospective cohort studies. Medicine. 2017;96(45):e8491–e. doi:10.1097/MD.0000000000008491
37. Schmidt M, Jacobsen JB, Lash TL, Botker HE, Sorensen HT. 25 year trends in first time hospitalisation for acute myocardial infarction, subsequent short and long term mortality, and the prognostic impact of sex and comorbidity: a Danish nationwide cohort study. BMJ. 2012;344:e356. doi:10.1136/bmj.e356
38. Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis. 2016;252:207–274. doi:10.1016/j.atherosclerosis.2016.05.037
39. Mensah GA, Wei GS, Sorlie PD, et al. Decline in cardiovascular mortality: possible causes and implications. Circ Res. 2017;120(2):366–380. doi:10.1161/CIRCRESAHA.116.309115
40. Hahn RA, Chang M-H, Parrish RG, Teutsch SM, Jones WK. Trends in mortality among females in the United States, 1900–2010: progress and challenges. Prev Chronic Dis. 2018;15:E30–E. doi:10.5888/pcd15.170284
41. Khan SS, Ning H, Wilkins JT, et al. Association of body mass index with lifetime risk of cardiovascular disease and compression of morbidity. JAMA Cardiol. 2018;3(4):280–287. doi:10.1001/jamacardio.2018.0022
42. Stevens J, Cai J, Pamuk ER, Williamson DF, Thun MJ, Wood JL. The effect of age on the association between body-mass index and mortality. N Engl J Med. 1998;338(1):1–7. doi:10.1056/NEJM199801013380101
43. Kuk JL, Ardern CI. Influence of age on the association between various measures of obesity and all-cause mortality. J Am Geriatr Soc. 2009;57(11):2077–2084. doi:10.1111/j.1532-5415.2009.02486.x
44. Stringhini S, Carmeli C, Jokela M, et al. Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1·7 million men and women. Lancet. 2017;389(10075):1229–1237. doi:10.1016/S0140-6736(16)32380-7
45. Zhang Q, Wang Y. Trends in the association between obesity and socioeconomic status in U.S. adults: 1971 to 2000. Obes Res. 2004;12(10):1622–1632. doi:10.1038/oby.2004.202
46. Harpsoe MC, Nielsen NM, Friis-Moller N, et al. Body mass index and risk of infections among women in the Danish national birth cohort. Am J Epidemiol. 2016;183(11):1008–1017. doi:10.1093/aje/kwv300
47. Gribsholt SB, Pedersen L, Richelsen B, Dekkers O, Thomsen RW. Body Mass Index of 92,027 patients acutely admitted to general hospitals in Denmark: associated clinical characteristics and 30-day mortality. PLoS One. 2018;13(4):e0195853. doi:10.1371/journal.pone.0195853
48. Kornum JB, Norgaard M, Dethlefsen C, et al. Obesity and risk of subsequent hospitalisation with pneumonia. Eur Respir J. 2010;36(6):1330–1336. doi:10.1183/09031936.00184209
49. Wang S, Liu X, Chen Q, Liu C, Huang C, Fang X. The role of increased body mass index in outcomes of sepsis: a systematic review and meta-analysis. BMC Anesthesiol. 2017;17(1). doi:10.1186/s12871-017-0405-4
50. Wade KH, Carslake D, Tynelius P, Davey Smith G, Martin RM. Variation of all-cause and cause-specific mortality with body mass index in one million Swedish parent-son pairs: an instrumental variable analysis. PLoS Med. 2019;16(8):e1002868. doi:10.1371/journal.pmed.1002868
51. Braun N, Hoess C, Kutz A, et al. Obesity paradox in patients with community-acquired pneumonia: is inflammation the missing link? Nutrition. 2017;33:304–310. doi:10.1016/j.nut.2016.07.016
52. Sun YQ, Burgess S, Staley JR, et al. Body mass index and all cause mortality in HUNT and UK Biobank studies: linear and non-linear Mendelian randomisation analyses. BMJ. 2019;364:l1042. doi:10.1136/bmj.l1042
53. Nseir W, Farah R, Mahamid M, et al. Obesity and recurrent urinary tract infections in premenopausal women: a retrospective study. Int J Infect Dis. 2015;41:32–35. doi:10.1016/j.ijid.2015.10.014
54. Newell MA, Bard MR, Goettler CE, et al. Body mass index and outcomes in critically injured blunt trauma patients: weighing the impact. J Am Coll Surg. 2007;204(5):
55. Brahmbhatt TS, Hernon M, Siegert CJ, Plauché L, Young LS, Burke P. Trauma and BMI Mortality. Curr Obes Rep. 2017;6(2):211–216. doi:10.1007/s13679-017-0264-9
56. Falagas ME, Kompoti M. Obesity and infection. Lancet Infect Dis. 2006;6(7):438–446.
57. de Wit L, Luppino F, van Straten A, Penninx B, Zitman F, Cuijpers P. Depression and obesity: a meta-analysis of community-based studies. Psychiatry Res. 2010;178(2):230–235. doi:10.1016/j.psychres.2009.04.015
58. Apple R, Samuels LR, Fonnesbeck C, et al. Body mass index and health-related quality of life. Obes Sci Pract. 2018;4(5):417–426. doi:10.1002/osp4.292
59. Amiri S, Behnezhad S. Body mass index and risk of suicide: a systematic review and meta-analysis. J Affect Disord. 2018;238:615–625. doi:10.1016/j.jad.2018.05.028
60. Gravseth HM, Mehlum L, Bjerkedal T, Kristensen P. Suicide in young Norwegians in a life course perspective: population-based cohort study. J Epidemiol Community Health. 2010;64(5):407–412. doi:10.1136/jech.2008.083485
61. Magnusson PK, Rasmussen F, Lawlor DA, Tynelius P, Gunnell D. Association of body mass index with suicide mortality: a prospective cohort study of more than one million men. Am J Epidemiol. 2006;163(1):1–8. doi:10.1093/aje/kwj002
62. Schneider B, Lukaschek K, Baumert J, Meisinger C, Erazo N, Ladwig KH. Living alone, obesity, and smoking increase risk for suicide independently of depressive mood findings from the population-based MONICA/KORA Augsburg cohort study. J Affect Disord. 2014;152–154:416–421. doi:10.1016/j.jad.2013.10.007
63. Carrasco-Barrios MT, Huertas P, Martín P, et al. Determinants of suicidality in the European general population: a systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17(11):4115. doi:10.3390/ijerph17114115
64. Khalid F, Holguin F. A review of obesity and asthma across the life span. J Asthma. 2018;55(12):1286–1300. doi:10.1080/02770903.2018.1424187
65. Goto T, Hirayama A, Faridi MK, Camargo CA
66. World Health Organization. Weight bias and obesity stigma: considerations for the WHO European Region. World Health Organization; 2017.
67. Jung FU, Luck-Sikorski C. Overweight and lonely? A representative study on loneliness in obese people and its determinants. Obes Facts. 2019;12(4):440–447. doi:10.1159/000500095
68. Gribsholt SBP, Richelsen L, Thomsen B. Validity of ICD-10 diagnoses of overweight and obesity in Danish hospitals. Clin Epidemiol. 2019;11:845–854. doi:10.2147/CLEP.S214909
69. The Danish Health and Medicines Authorities. Anbefalinger for svangreomsorgen. [Recommendations for maternity care]; 2013. Available from: https://www.sst.dk/da/udgivelser/2015/~/media/C18BD8F183104A8384F80B73B155826D.ashx.
70. Cain KC, Harlow SD, Little RJ, et al. Bias due to left truncation and left censoring in longitudinal studies of developmental and disease processes. Am J Epidemiol. 2011;173(9):1078–1084. doi:10.1093/aje/kwq481
71. The Health of the Danes.Danskernes Sundhed. Tal fra Den Nationale Sundhedsprofil. [Figures from the National Health Profile]; 2018.
72. Caterson ID, Alfadda AA, Auerbach P, et al. Gaps to bridge: misalignment between perception, reality and actions in obesity. Diabetes Obes Metab. 2019;21(8):1914–1924. doi:10.1111/dom.13752
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.