Back to Journals » Therapeutics and Clinical Risk Management » Volume 17
More Pronounced Muscle Loss During Immunochemotherapy is Associated with Worse Clinical Outcomes in Newly Diagnosed Patients with Diffuse Large B-Cell Lymphoma with Unfavorable Features
Authors Lucijanic M ![]() , Huzjan Korunic R, Sedinic M, Kusec R
, Huzjan Korunic R, Sedinic M, Kusec R ![]() , Pejsa V
, Pejsa V
Received 9 June 2021
Accepted for publication 13 August 2021
Published 24 September 2021 Volume 2021:17 Pages 1037—1044
DOI https://doi.org/10.2147/TCRM.S323749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Garry Walsh
Marko Lucijanic,1,2 Renata Huzjan Korunic,2,3 Martina Sedinic,1 Rajko Kusec,1,2 Vlatko Pejsa1,2
1Hematology Department, University Hospital Dubrava, Zagreb, Croatia; 2University of Zagreb School of Medicine, Zagreb, Croatia; 3Radiology Department, University Hospital Dubrava, Zagreb, Croatia
Correspondence: Marko Lucijanic
Hematology Department, University Hospital Dubrava, Av. Gojka Suska 6, Zagreb, 10000, Croatia
Email [email protected]
Introduction: Cancer-induced cachexia is associated with poor prognosis in patients with non-Hodgkin lymphoma, but it is unknown how and to what extent curable lymphoma treatments affect the musculoskeletal system.
Patients and Methods: We retrospectively analyzed 104 newly diagnosed diffuse large B-cell lymphoma (DLBCL) patients with unfavorable disease features treated with the R-DA-EPOCH regimen. Psoas muscle area (PMA) measured at L3 vertebra level was compared between staging (pre-therapy) and revision (end of treatment) computerized tomography (CT) scans.
Results: Small but significant decline in PMA was observed during the immunochemotherapy period (average loss 5%; P=0.016) with 57.7% of patients experiencing muscle loss. Higher body surface area (OR=17.98 for each m2; P=0.034), number of cycles with dose reduction (OR=2.86 for each cycle; P=0.039) and worse response to therapy (OR=3.09 for each response category; P=0.052) were recognized as independent contributors to the PMA loss in multivariate analysis. One quarter of patients had more pronounced PMA loss (≥ 21%), which was associated with significantly worse overall and progression-free survival. Both ≥ 21% PMA loss and non-achieving response to therapy remained independently associated with inferior OS (PMA loss HR=2.98; P=0.016 and achieving response HR=0.04; P< 0.001) and PFS (PMA loss HR=3.16; P=0.005 and achieving response HR=0.08; P=0.001) in multivariate analyses.
Discussion: Muscle loss occurs in approximately half of newly diagnosed DLBCL patients with unfavorable disease features during R-DA-EPOCH immunochemotherapy. If pronounced, this is associated with worse clinical outcomes irrespectively of achieved response to therapy. Muscle loss seems to be mostly affected by the efficacy and tolerability of the regimen.
Keywords: diffuse large B-cell lymphoma, sarcopenia, psoas muscle, R-DA-EPOCH, survival
Plain Language Summary
Patients with aggressive lymphoid malignancies receive intensive immunochemotherapeutic therapies that result with a cure in a majority of patients. Our paper is the first to provide an overview of the extent and clinical associations of muscle loss during therapy with one of the standard immunochemotherapy regimens (R-DA-EPOCH) for aggressive diffuse large B-cell lymphoma with unfavorable disease features. Our data show that muscle loss is common in these patients but detrimental only if very pronounced. Factors that affect muscle loss are mostly related to immunochemotherapy and not disease features prior to therapy per se.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common subset of aggressive non-Hodgkin lymphomas (NHL). It is curable in a majority of newly diagnosed patients using the R-CHOP immunochemotherapy regimen which is a current standard of care. Still, a substantial proportion of DLBCL patients with very aggressive and poor prognostic disease features have unsatisfactory outcomes when treated with R-CHOP regimen and these patients might benefit from more intensive therapeutic approaches.1 Although no significant improvement could be demonstrated for the R-DA-EPOCH regimen in a randomized controlled trial in comparison to R-CHOP in unselected DLBCL patients,2 a number studies reported improved outcomes with the R-DA-EPOCH regimen in patients with unfavorable disease features.3–5
Hematologic malignancies are often characterized by presence of constitutional symptoms driven by high cytokine activity like involuntary body weight loss and profound night sweating. Cancer-induced cachexia, ie loss of muscle and fat tissue, and sarcopenia, ie loss of skeletal muscle tissue, present at baseline have been associated with more advanced disease features, functional impairment and inferior prognosis in patients with various malignancies, including Hodgkin lymphoma and NHL patients.6–8 Loss of skeletal muscle mass during chemotherapy was shown to have negative prognostic implications in patients with gastrointestinal malignancies.9–11 It is unknown, however, how and to what extent curable lymphoma treatments affect the musculoskeletal system and might they improve or further deteriorate muscle tissues. Computerized tomography (CT) scans done at the times of pre-therapy DLBCL staging and at the end of treatment (EOT) revision offer a unique opportunity to assess chemotherapeutic effects on muscle mass dynamics without exposing patients to additional harm. Psoas muscle is a large skeletal muscle that is easy to assess and quantify when assessing lymphadenopathy. Thus, we aimed to investigate how immunochemotherapy affects psoas muscle mass and whether this has prognostic consequences in our cohort of newly diagnosed DLBCL patients with unfavorable disease features treated with the R-DA-EPOCH regimen through assessment of baseline and EOT CT scans.
Patients and Methods
The primary goal was to assess the extent and predictors of the PMA loss. The secondary goal was to investigate prognostic associations of PMA loss.
We retrospectively analyzed a single institution cohort of 104 newly diagnosed DLBCL patients who were treated with the R-DA-EPOCH immunochemotherapy regimen in the period from 2005 to 2019 and had available baseline and end of treatment CT scans. All patients were adult, Caucasian and had unfavorable prognostic features (a very high proliferative index Ki-67+ ≥80% and/or International Prognostic Index (IPI) ≥2 points). Prednisolone dose was reduced in the majority of patients to improve tolerability. A subset of patients underwent autologous stem cell transplantation as a part of the first-line therapy and a subset of patients received concomitant radiotherapy. Psoas muscle area (PMA) was assessed from transversal scans at L3 vertebra level from baseline and EOT CT scans. EOT measurements were divided by baseline measurements to obtain the percentage of muscle mass loss/improvement. Patients with tumor infiltration of psoas muscle were excluded from the study. Clinical characteristics and outcomes were obtained from paper and electronic medical records. The study was approved by the Institutional review board. All procedures followed the Helsinki Declaration. Due to the retrospective nature of the study based on routine clinical procedures, informed consent was not required. All patients gave informed consent for procedures included in the study.
Statistical Methods
Normality of distribution of numerical variables was tested using the Shapiro–Wilk test. Normally distributed numerical variables were presented as mean±standard deviation and were compared between groups using the t-test. Non-normally distributed numerical variables were presented as median and interquartile range (IQR) and were compared between groups using the Mann–Whitney U-test and Kruskal–Wallis one-way analysis of variance. Correlations between numerical variables were assessed using the Spearman rank correlation. Psoas muscle measurements before and after chemotherapy were compared using the Wilcoxon test for paired data. Categorical variables were presented as ratios and percentages and were compared between groups using the χ2 test. Independent associations with the loss of psoas muscle mass were analyzed using the logistic regression via backward approach (enter P criterion <0.1, exclusion P criterion >0.2). The ROC curve analysis was used to define optimal cut-off values of numerical variables for survival outcomes. Survival analyses were performed using the methods of Kaplan and Meier. Survival curves were compared between groups using the log rank test. Univariate associations of continuous variables with survival were assessed using the Cox regression analysis. Multivariate survival analyses were performed using the Cox regression analysis, using the backward approach (enter P criterion <0.1, exclusion P criterion >0.2) for exploratory assessment of different survival predictors and simultaneously controlling for PMA and clinically relevant parameters for assessing relationship of PMA loss with outcomes in the context of age, sex, response to therapy and the R-IPI score. Initial screening for survival associations was performed using the custom-made MS Excel workbook.12 P values <0.05 were considered to be statistically significant. All presented analyses were performed using the MedCalc statistical software version 19.8 (MedCalc Software Ltd, Ostend, Belgium).
Results
A total of 104 patients with available data were included in the study. There were 57/104 (54.8%) males and 47/104 (45.2%) females. Median age was 63 years, IQR (50–71). Median R-IPI score was 3 points, IQR (2–3) and median od R-DA-EPOCH cycles received was 6, IQR (6–7.25). Patients’ characteristics and their relationship with the psoas muscle mass dynamics during treatment are shown in Table 1.
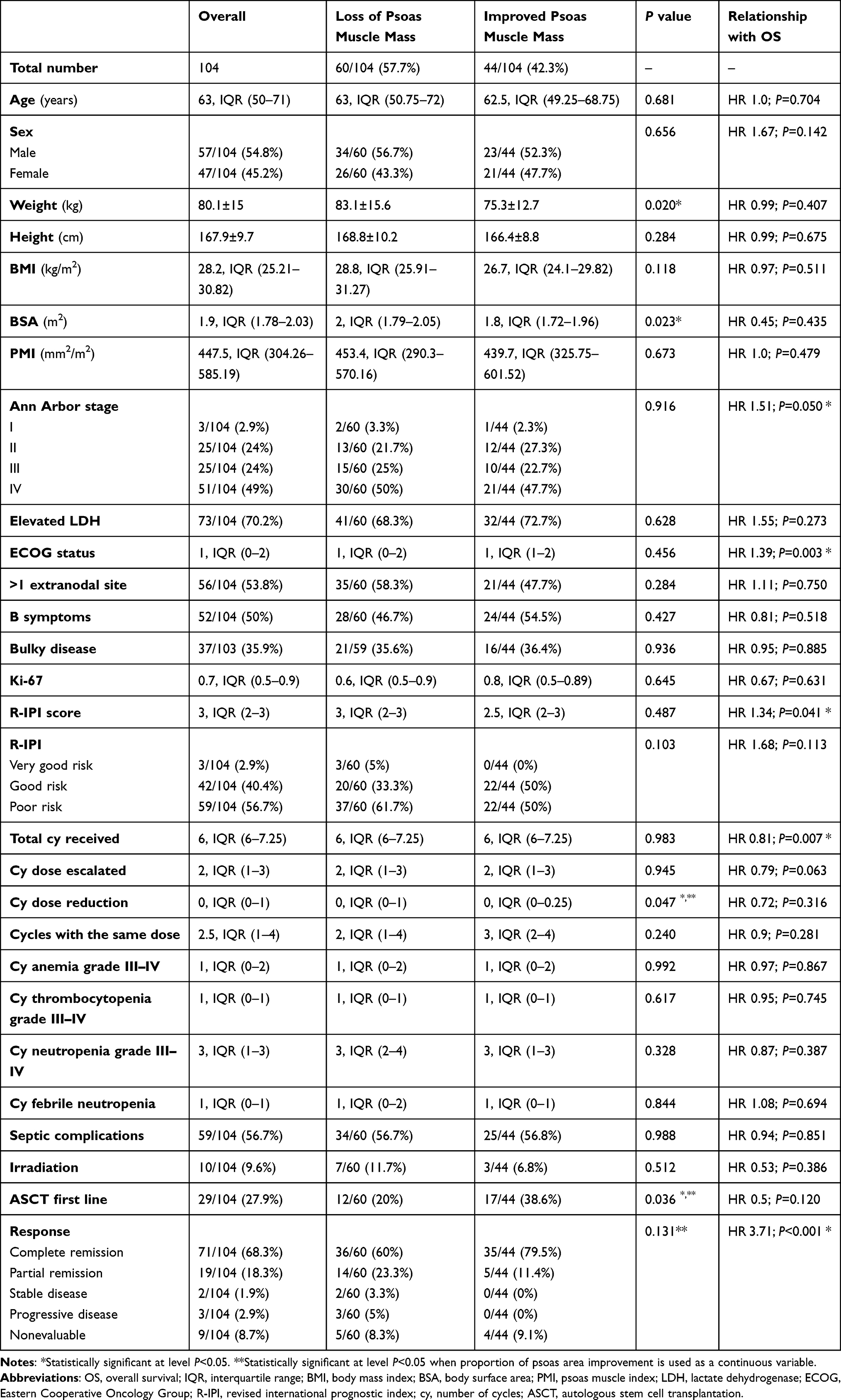 |
Table 1 Patients’ Characteristics Stratified According to the Psoas Muscle Mass Dynamics During Immunochemotherapy Treatment |
Median psoas area measurements before and after R-DA-EPOCH therapy were 1238 and 1099 mm2, respectively, with small but significant decline during the immunochemotherapy period (P=0.016; Figure 1A). Average PMA loss was 5% with slightly more than half of the patients experiencing the loss during the treatment period [60/104 (57.7%)]. Factors univariately associated with the PMA loss (either stratified as a categorical variable or analyzed as a continuous psoas area ratio) were higher patient body weight (P=0.020), higher body surface area (P=0.023), higher number of chemotherapy cycles with required dose reduction (P=0.047) and worse disease response to therapy (P=0.008; Figure 1B). Age, sex, baseline psoas muscle index, BMI, Ki-67, Ann Arbor and R-IPI staging systems had no significant association with the extent of PMA loss (P>0.05 for all analyses). In the multivariate logistic regression analysis investigating independent contribution of univariately associated and other disease specific variables, the backward model building process recognized higher body surface area (OR 17.98 for each m2; P=0.034), number of cycles with dose reduction (OR 2.86 for each cycle; P=0.039) and worse response to therapy (OR 3.09 for each response category; P=0.052) as independent contributors to the PMA loss as shown in Table 2.
 |
Table 2 Multivariate Logistic Regression Model Investigating Independent Associations of Clinical Parameters with the Loss of Psoas Muscle Mass |
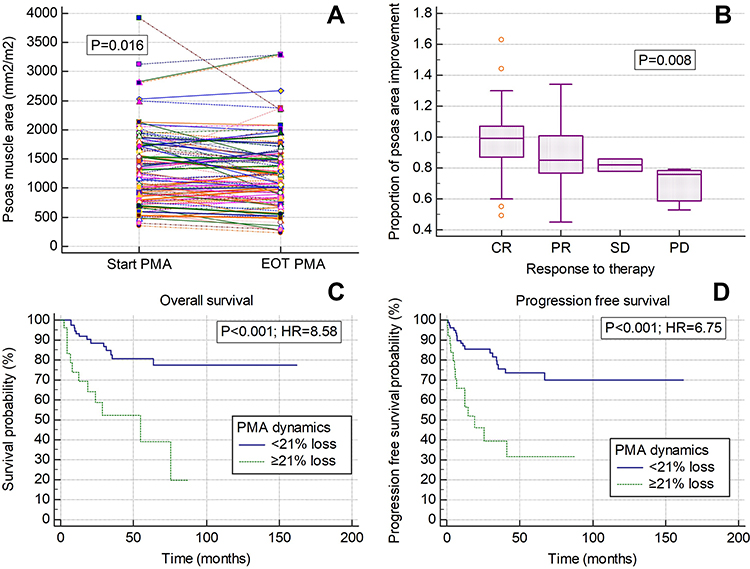 |
Figure 1 (A) Psoas muscle area (PMA) dynamics between start and end of treatment (EOT) computerized tomography scans. (B) PMA dynamics stratified according to the response to the R-DA-EPOCH immunochemotherapy. (C) Overall survival and (D) progression-free survival stratified according to the degree of PMA loss. Abbreviation: HR, hazard ratio. |
Median follow-up of our cohort was 46 months with 25 patients dying and 22 progressing during the follow-up period. Median overall survival (OS) and progression-free survival (PFS) were not reached. Univariate associations of assessed clinical variables with OS are presented in Table 1. Using the ROC curve analyses we have defined an optimal cut-off level for PMA loss of ≥21% for OS and PFS discrimination (AUC 0.649 and 0.624, respectively). A total of 25/104 (24%) patients fulfilled this criterion. Patients with ≥21% PMA loss experienced significantly worse OS (HR=8.58; P<0.001) and PFS (HR=6.75; P<0.001) as shown in Figure 1C and D. These phenomena remained statistically significant in multivariate Cox regression analyses after adjustments for age, sex, R-IPI score and achieved response as shown in Table 3. Both ≥21% PMA loss and non-achieving response to therapy were independently associated with inferior OS and PFS. Similar was observed in additional exploratory analyses where all variables that were univariately significantly associated with OS were included into the backward model building process. A ≥21% PMA loss and non-response to therapy were retained in both OS and PFS models and were mutually significantly associated with inferior OS and PFS. R-IPI was the only additional variable that was retained in the OS model but was insignificant in this context similarly as in the model from Table 3.
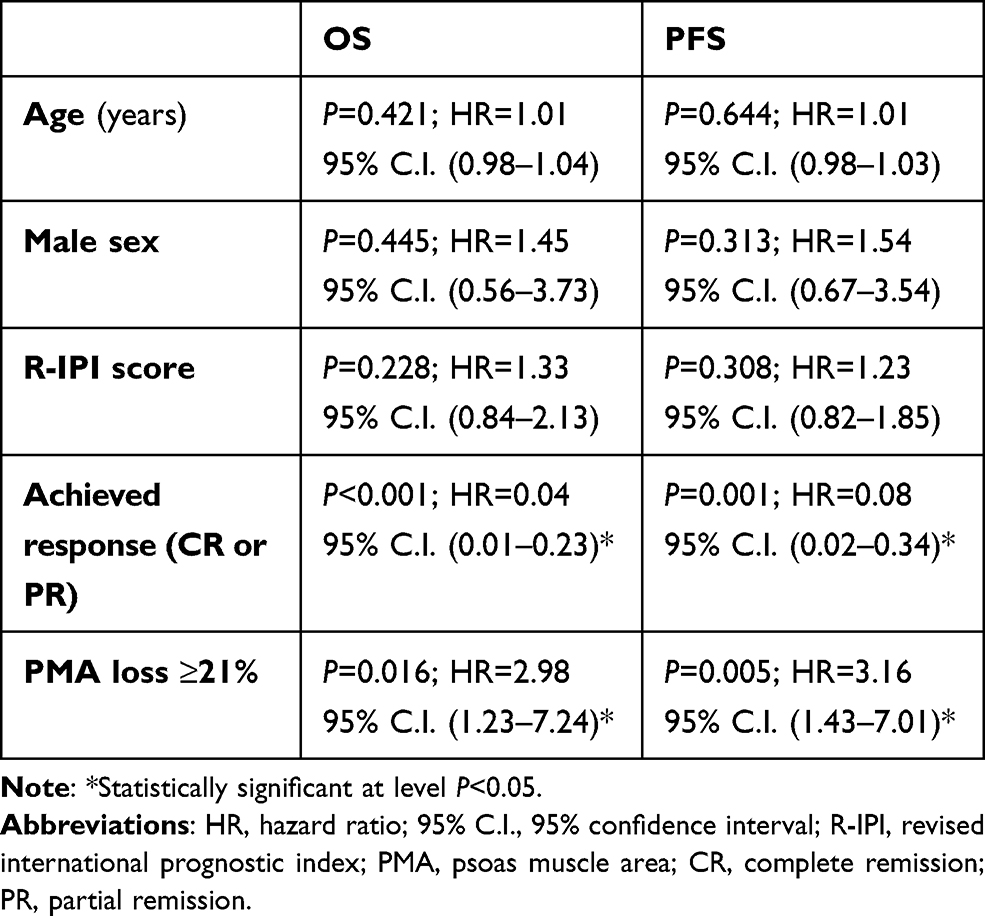 |
Table 3 Multivariate Cox Regression Models Investigating Associations of PMA Dynamics with Overall (OS) and Progression-Free Survival (PFS) |
Discussion
There are several important points emerging from our data that we would like to emphasize. To the best of our knowledge, there are no previous studies assessing muscle mass dynamics during immunochemotherapy and its prognostic associations in patients with lymphoid malignancies. Our data show that muscle mass loss occurs in approximately half of R-DA-EPOCH treated newly diagnosed DLBCL with unfavorable disease features, and if pronounced, this is associated with worse clinical outcomes independently of achieved response to therapy.
Associations of tumor cachexia and reduced muscle mass present at baseline with adverse clinical outcomes are well described in patients with various solid and hematologic malignancies.7,8,13–16 In cohorts of R-CHOP-treated DLBCL patients, patients presenting with sarcopenia prior to immunochemotherapy were shown to have worse OS and PFS.8,13,14,16,17 However, as we have previously reported,18 immunochemotherapeutic regimens like R-DA-EPOCH might moderate these associations through personalized dose adjustments tailored to the hematopoietic reserve. Despite being associated with older age, female gender and worse R-IPI stage, baseline psoas muscle index did not affect response to therapy or survival outcomes in our cohort of patients.18 As we report in the current study, baseline psoas muscle index also does not seem to predict loss of muscle mass during immunochemotherapy. Similarly, parameters reflecting more aggressive tumor behavior like higher Ann Arbor or R-IPI stage, Ki-67 index, and general characteristics like body mass index, age and gender also did not show significant association with muscle mass dynamics despite some of them having associations with baseline presence of sarcopenia. Similar to our observations are reports in patients with metastatic colorectal cancer and foregut malignancies among whom a decrease in skeletal muscle index/area was associated with poor survival as opposed to baseline sarcopenia that showed no significant associations with survival.9,10
We observed significant clinical associations of muscle mass loss with higher body surface area, higher number of cycles with required chemotherapy dose reduction and worse disease response to immunochemotherapy. Since R-DA-EPOCH and other immunochemotherapeutic regimens are initially dosed according to the body surface area, we interpret these findings as a consequence of higher delivered absolute drug doses of antiproliferative agents and corticosteroids that are known to have myopathic/neuropathic properties. R-DA-EPOCH dose reduction is mandated in patients developing deep and prolonged cytopenias or septic complications between cycles of therapy and higher number of cycles requiring dose reduction might indicate poor immunochemotherapy tolerance/weaker hematopoietic reserve that seems to be an important predictor of psoas muscle loss/improvement. Similar was observed in patients with myelofibrosis treated with ruxolitinib who were more likely to experience muscle mass improvement with better baseline hematopoietic status.19 The role and function of the musculoskeletal system in patients with hematologic malignancies and its relationship with disease pathophysiology, hematopoiesis, patient mobility and energy metabolism are insufficiently understood to draw clear conclusions. Also, inadequate disease response to therapy that is associated with prolonged pro-cachectic tumor effects and further functional deterioration is an important independent predictor of muscle loss. Summarized, our data suggest that most relevant predictors of muscle loss seem to be immunochemotherapy related, ie associated with the dose, tolerability and efficacy of the immunochemotherapy regimen.
A substantial subset (24%) of patients with pronounced muscle loss ≥21% had approximately three-fold higher risk of death and progression or death in comparison to other patients irrespectively of achieved response to therapy. Considering predictors of muscle mass loss, this might be due to sub-optimal dose density due to higher number of cycles with chemotherapy dose reduction. Since development of sarcopenia during treatment has such profound negative prognostic implications, a question emerges whether active strategies aimed at muscle mass improvement like physiotherapy and intensive nutritional support might improve outcomes in this subgroup of patients. It is also unknown would such interventions have effects if performed during or after immunochemotherapy. These important questions deserve further investigations in prospectively conducted interventional studies that are highly needed. Retrospective studies comparing the extent and consequences of muscle loss in patients with other types of lymphoid malignancies and DLBCL patients treated with other immunochemotherapy regimens would help to better describe and understand this very interesting clinical phenomenon. Relationships of muscle loss with baseline nutritional risk, comorbidities and PET-CT defined metabolic response are yet to be determined.
Limitations of our study are the single center experience, retrospective study design and inability to discriminate between different DLBCL subsets. Also, we investigated a selected cohort of patients with unfavorable disease features uniformly treated with the R-DA-EPOCH immunochemotherapeutic regimen and we do not know do our findings translate to DLBCL patients with lower risk disease who receive other immunochemotherapeutic regimens like R-CHOP. Inclusion criteria based on both R-IPI and high proliferation index probably resulted in diminished prognostic properties of R-IPI in both univariate and multivariate settings as patients having lower IPI had tendency for having higher tumor proliferation index. Also, we did not have available data to properly investigate how were underlying comorbidities, general nutritional conditions and PET-CT metabolic response related to the PMA loss. Nevertheless, extent of the loss of muscle mass during immunochemotherapy period in newly diagnosed DLBCL patients and its clinical consequences have not been previously reported and our results call for planning of specific interventions and future studies on this very interesting topic.
In conclusion, muscle loss is common in DLBCL patients during the R-DA-EPOCH immunochemotherapy period and if pronounced, might negatively reflect on prognosis.
Ethical Approval
The study was approved by the University Hospital Dubrava Institutional Review Board.
Funding
The study was funded by the Foundation of the Croatian Cooperative Group for Hematological Diseases – CROHEM research grant.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Karlin L, Coiffier B. Improving survival and preventing recurrence of diffuse large B-cell lymphoma in younger patients: current strategies and future directions. Onco Targets Ther. 2013;6:289–296.
2. Bartlett NL, Wilson WH, Jung SH, et al. Dose-adjusted EPOCH-R compared with R-CHOP as frontline therapy for diffuse large B-cell lymphoma: clinical outcomes of the phase III intergroup trial alliance/CALGB 50303. J Clin Oncol. 2019;37(21):1790–1799. doi:10.1200/JCO.18.01994
3. García-Suárez J, Bañas H, Arribas I, De Miguel D, Pascual T, Burgaleta C. Dose-adjusted EPOCH plus rituximab is an effective regimen in patients with poor-prognostic untreated diffuse large B-cell lymphoma: results from a prospective observational study. Br J Haematol. 2007;136(2):276–285. doi:10.1111/j.1365-2141.2006.06438.x
4. Pejsa V, Prka Z, Lucijanic M, et al. Rituximab with dose-adjusted EPOCH as first-line treatment in patients with highly aggressive diffuse large B-cell lymphoma and autologous stem cell transplantation in selected patients. Croat Med J. 2017;58(1):40–48. doi:10.3325/cmj.2017.58.40
5. Matsuda S, Suzuki R, Takahashi T, et al. Dose-adjusted EPOCH with or without rituximab for aggressive lymphoma patients: real world data. Int J Hematol. 2020;112(6):807–816. doi:10.1007/s12185-020-02984-w
6. Dunne RF, Loh KP, Williams GR, Jatoi A, Mustian KM, Mohile SG. Cachexia and sarcopenia in older adults with cancer: a comprehensive review. Cancers. 2019;11(12):1861. doi:10.3390/cancers11121861
7. Lucijanić M, Huzjan Korunic R, Ivić M, et al. Psoas muscle index at the time of diagnosis might reflect the prognosis of classical hodgkin’s lymphoma patients. Wien Klin Wochenschr. 2021. doi:10.1007/s00508-021-01850-x
8. Iltar U, Sözel H, Sözel YK, et al. Prognostic impact of the psoas muscle index, a parameter of sarcopenia, in patients with diffuse large B-cell lymphoma treated with rituximab-based chemoimmunotherapy. Leuk Lymphoma. 2021;62(5):1098–1106
9. Gallois C, Bourillon C, Auclin E, et al. Skeletal muscle loss under chemotherapy and its association with survival and systemic treatment toxicity in metastatic colorectal cancer: an AGEO prospective multicenter study. J Clin Oncol. 2020;38(15_suppl):4025. doi:10.1200/JCO.2020.38.15_suppl.4025
10. Daly LE, Ní Bhuachalla ÉB, Power DG, Cushen SJ, James K, Ryan AM. Loss of skeletal muscle during systemic chemotherapy is prognostic of poor survival in patients with foregut cancer. J Cachexia Sarcopenia Muscle. 2018;9(2):315–325. doi:10.1002/jcsm.12267
11. Park SE, Choi JH, Park JY, et al. Loss of skeletal muscle mass during palliative chemotherapy is a poor prognostic factor in patients with advanced gastric cancer. Sci Rep. 2020;10(1):17683. doi:10.1038/s41598-020-74765-8
12. Lucijanić M. Survival analysis in clinical practice: analyze your own data using an excel workbook. Croat Med J. 2016;57(1):77–79. doi:10.3325/cmj.2016.57.77
13. Lanic H, Kraut-Tauzia J, Modzelewski R, et al. Sarcopenia is an independent prognostic factor in elderly patients with diffuse large B-cell lymphoma treated with immunochemotherapy. Leuk Lymphoma. 2014;55(4):817–823. doi:10.3109/10428194.2013.816421
14. Nakamura N, Hara T, Shibata Y, et al. Sarcopenia is an independent prognostic factor in male patients with diffuse large B-cell lymphoma. Ann Hematol. 2015;94(12):2043–2053. doi:10.1007/s00277-015-2499-4
15. Rier HN, Kharagjitsing H, van Rosmalen J, et al. Prognostic impact of low muscle mass and low muscle density in patients with diffuse large B-cell lymphoma. Leuk Lymphoma. 2020;61(7):1618–1626. doi:10.1080/10428194.2020.1737686
16. Go SI, Park MJ, Song HN, et al. Prognostic impact of sarcopenia in patients with diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone. J Cachexia Sarcopenia Muscle. 2016;7(5):567–576.
17. Go S-I, Kim H-G, Kang MH, Park S, Lee G-W. Prognostic model based on the geriatric nutritional risk index and sarcopenia in patients with diffuse large B-cell lymphoma. BMC Cancer. 2020;20(1):439. doi:10.1186/s12885-020-06921-2
18. Lucijanić M, Korunić RH, Sedinić M, Kušec R, Pejša V. Prognostic impact of psoas muscle index in patients with diffuse large B-cell lymphoma might be dependent on the immunochemotherapy type. Leuk Lymphoma. 2021;1–4. doi:10.1080/10428194.2021.1919667
19. Lucijanic M, Galusic D, Soric E, et al. Ruxolitinib treatment improves muscle mass in patients with myelofibrosis. Ann Hematol. 2020;100(4):1105–1106. doi:10.1007/s00277-020-04243-8
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.