Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
More Physical Exercise is Beneficial to Glycemic Control in Late Pregnancy Among Women with Gestational Diabetes Mellitus: Findings Based on Trajectory Model in a Prospective Cohort in Shanghai
Authors Zhang X ![]() , Ding Y
, Ding Y ![]() , Duan Z
, Duan Z ![]() , Cai R, Gao X
, Cai R, Gao X ![]() , Zhang R, Wang R
, Zhang R, Wang R ![]()
Received 19 March 2025
Accepted for publication 20 May 2025
Published 27 May 2025 Volume 2025:18 Pages 1723—1737
DOI https://doi.org/10.2147/DMSO.S524237
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hillary Keenan
Xiuqi Zhang,1,2,* Yuning Ding,1,2,* Zhen Duan,3,* Ruiqi Cai,3 Xiangjin Gao,1 Rui Zhang,1 Ruiping Wang1– 4
1Clinical Research Center, Shanghai Skin Diseases Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2School of Medicine, Tongji University, Shanghai, People’s Republic of China; 3School of Public Health, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 4Office of Public Health Management, Songjiang Maternal and Children’s Health-Care Hospital, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ruiping Wang, Clinical Research Center, Shanghai Skin Diseases Hospital, School of Medicine, Tongji University, 1278 Baode Road, Jing’an District, Shanghai, 200443, People’s Republic of China, Email [email protected]
Purpose: Physical exercise effectively prevents the onset of gestational diabetes mellitus (GDM). However, the association between the daily physical exercise time (PET) and the overall trend in glycemic levels in late pregnancy among women with GDM is limited. This study aimed to explore this association using a group-based trajectory model (GBTM) among women with GDM.
Patients and Methods: We constructed two types of models (A and B) by applying GBTM analysis based on a series of abnormal plasma glucose (PG) prevalence values calculated at each prenatal checkup in the GDM cohort. Women with GDM were classified into good plasma glucose control (PGC) and bad PGC groups based on each trajectory model. Logistic regression was used to explore the association between daily PET and prevalence of good PGC among women with GDM. In this study, P value less than 0.05 was set as the statistical significance.
Results: Among 1122 GDM women, the average age was 26.9 years. The number of women with GDM in the good PGC group was 539 (48.0%) in Model A 644 (57.4%) in Model B. The median daily PET was longer in the good PGC group (70 min in both Models A and B) than in the poor PGC group (Model A, 65 min; Model B, 64 min). Logistic regression analysis indicated that GDM women with ≥ 120 min/day PET had a significantly higher PGC prevalence in late pregnancy (odds ratio (OR), 1.32 (95% confidence interval (CI): 1.12– 1.56) in Model A, and 1.24 (95% CI: 1.05– 1.46) in Model B, even after adjusting for potential confounders (age and BMI).
Conclusion: Women with GDM need ≥ 120 min/day PET to achieve glycemic control, especially for those who are older and have BMI ≥ 24kg/m2.
Keywords: physical exercise, gestational diabetes mellitus, trajectory model, abnormal plasma glucose prevalence
Introduction
Gestational diabetes mellitus (GDM) refers to varying degrees of abnormal glucose tolerance that first occurs during the gestational period,1 which is a common metabolic disorder during pregnancy. GDM can induce various complications and long-term adverse pregnancy outcomes, which have a serious impact on the health of both mothers and children.2,3 According to the International Diabetes Federation (IDF), the global prevalence of GDM is approximately 14.0% in 2021.4 In China, and with the implementation of three-child policies and improvement in living standards, the number of obese and elderly pregnant women affected by GDM is increasing.5,6 IDF data indicate that the overall prevalence of GDM In China is approximately 8.6% in 2021, affecting over 8.7 million live births. GDM has therefore become an important global public health issue.
Good glycemic control during pregnancy can reduce the incidence of GDM and significantly improve maternal and fetal prognosis.7 Currently, the optimal treatment method for GDM remains unclear. Previous studies demonstrate that lifestyle intervention including diet and physical exercise can maintain normal glycemic level and reduce hypoglycemic drugs use, and thereby alleviating side effects.8 In China, pregnancy is treated as a special state that requires extra attention and recuperation by Chinese women. It is usually unacceptable to control the glycemic level by dietary due to the fact that many GDM women express concerns that altering dietary patterns during pregnancy could potentially affect fetal development. However, GDM women may prefer physical exercise, because they can select physical activities tailored to their individual health status and personal preferences. Therefore, physical exercise is more acceptable for GDM women compared to dietary guidance in China. Physical exercise is widely recommended to achieve meaningful health benefits. The latest guidelines recommended by the American College of Obstetricians and Gynecologists (ACOG) and the Canadian Society for Exercise Physiology (CSEP) suggest that pregnant women without exercise contraindications should engage in ≥150 minutes of moderate-intensity physical exercise per week to prevent the occurrence of GDM.9,10 Furthermore, our previous studies indicated that GDM women require ≥60 min/day moderate-intensity physical exercise to achieve good glycemic control (<30%) in late pregnancy.11,12 However, data analysis in the aforementioned studies were based on logistic regression or repeated measures ANOVA, and the abnormal plasma glucose (PG) prevalence was calculated as the cumulative number of abnormal PG divided by the total number of prenatal checkups. A single point could not completely depict the trend of PG level changes in the subsequent 6–8 times of antenatal checkups and might have induced some bias. Therefore, the incorporation of a novel model to depict data with repeated measurements and analyze trend variation should be considered.
Group-based trajectory model (GBTM) is an analysis based on a longitudinal cohort, which identifies individuals exhibiting homogeneous changes in repeated measurement data and groups them by monitoring the dynamic trend of specific observation indicators over time to achieve group clustering.13,14 Currently, studies evaluating the trajectory of the changes in PG levels at different times of antenatal checkups among women with GDM by GBTM are still limited.15 Therefore, it is crucial to implement GBTM to explore the association between PET (physical exercise time) and glycemic control to propose an appropriate amount of exercise time for GDM women.
Materials and Methods
Study Design and Participants
In this study, participants came from a dynamic cohort of GDM established in Songjiang District, Shanghai in August 2019, and detailed information on the cohort was reported in our previous studies.11,16,17. We extracted data on 1122 women with GDM from this cohort recruited in 2019 and 2020. The inclusion criteria were as follows: 1) aged 18–45 years; 2) gestation weeks of 24–28; 3) singleton pregnancy; 4) without diabetes before pregnancy; 5) confirmed GDM by a diagnostic 75 g OGTT; 6) without exercise contraindications; 7) living in Shanghai without planning for migration in 2 years; and 8) able to read and sign the informed consent form. The exclusion criteria were as follows: 1) taking long-term medications that affect glucose metabolism; 2) intellectual disabilities, mental disorders, and inability to communicate normally or fully understand the questionnaire items; 3) history of habitual abortions, stillbirths, intrauterine fetal developmental delays, and postnatal hemorrhage; and 4) severe disorders of the heart, lung, liver, and kidney; hyperthyroidism; anemia; malignant tumors; acute and chronic infections; coagulation disorders; autoimmune diseases.
This study was reviewed and authorized by the Institutional Review Board of Songjiang Maternal and Children’s Healthcare Hospital (IRB#-201912003), and informed consent was obtained from each GDM patient before the interview. This study was conducted in accordance with the Declaration of Helsinki and registered in the Chinese Clinical Trial Registry (ChiCTR2000028832).
Data Collection
Data on women with GDM were collected through face-to-face interviews. The questionnaire consisted of four parts. Part A concerned demographic information (age, education, employment, residency status, and monthly income). Part B concerned pregnancy history data (number of pregnancies and number of births), routine antenatal checkup information, height and weight before pregnancy, and PG test records. Part C concerned newborn delivery information (gestational week, delivery mode, sex and birth weight of baby, adverse pregnancy outcomes (macrosomia, postpartum hemorrhage, polyhydramnios, etc.)). Part D included 20 types of physical exercise (walking, house cleaning, stationary riding, jogging, swimming, climbing stairs, Tai Chi, soft gymnastics, yoga, oxygen dance, etc.) in late pregnancy, recording the frequency and duration of each physical exercise on an average on a monthly basis during Weeks 27–40 of gestation. The form for exercise was designed through the combination of exercise types recommended by international guidelines with Chinese guidelines for GDM women, and its reliability (the split-half reliability coefficient was 0.89) and validity (the content validity coefficient was 0.86) were evaluated and validated in our pilot study. In this study, Data in Parts A, B, and C were directly extracted from prenatal examination records saved by the hospital. Data in Part D were obtained through face-to-face interviews with GDM women after delivery conducted by trained investigators.
In this study, records with missing values were flagged and double-checked with reference to original paper records. Each investigator received training to ensure record accuracy. All the data were encrypted and accessed only by the principal investigators; therefore, they could not be linked to any specific individual.
Definition and Index Calculation
In this study, we use the International Association of Diabetes and Pregnancy Study Group (IADPSG) criteria to diagnose GDM, a diagnostic 75 g OGTT at 24–28 gestational weeks when any one of the following values met or exceed the threshold is diagnosed as GDM: 0-hour PG (fasting for over 8 hours) ≥5.1 mmol/L, 1-hour PG ≥10.0 mmol/L and 2-hour PG ≥8.50 mmol/L. PG was evaluated in gestational Weeks 27–28, Weeks 29–30, Weeks 31–32, Weeks 33–34, Weeks 35–36, Weeks 37–38, and Weeks 39–40 (pre-birth), and an abnormal PG was defined as the morning fasting PG ≥5.3 mmol/L or (and) 2h PG following a standard breakfast ≥6.7 mmol/L in each of the following routine prenatal checkups.
In this study, we constructed two types of trajectory models by applying a GBTM-based series of eight abnormal PG prevalence in the GDM cohort. Abnormal PG prevalence at each prenatal checkup was calculated as the cumulative time of abnormal PG during the first and current prenatal checkups divided by the total 8 times of prenatal checkups (Model A) or the total number of prenatal checkups (Model B). For example, a woman with GDM visited the hospital for the 5th prenatal checkup in gestational Weeks 33–34, if she had three episodes of abnormal PG in total during the five prenatal checkups, the abnormal PG prevalence at the 5th prenatal checkup was 37.5% in Model A (3/8) and 60% in Model B (3/5). A higher prevalence of abnormal PG indicates poorer glycemic control. Women with GDM were then classified into the good and bad PGC groups.
Moderate-intensity PET (the intensity of increasing respiratory rate while one can still hold a conversation) was evaluated using the reported total daily activity time. First, the physical activity time was calculated as the monthly activity frequency multiplied by the average duration of each activity and then divided by 30 days. Thereafter, the 20 types of physical activity times were combined to provide the total daily time of physical activity with moderate-intensity with or without metabolic equivalence (METS) conversion for each participant. For example, if a woman with GDM reported three types of physical activity (bicycle riding, walking, and line dancing) during gestation Weeks 27–40, the average frequency and duration were 12, 20, and 12 times per month and 20, 30, and 25 minutes, respectively, and the total daily activity time was 40.7 min ((12 × 20 + 20 × 30 + 12 × 25)/30). We then classified GDM women into dichotomous groups according to their total daily physical activity time: “<30 min/day” and “≥30 min/day”, “<60 min/day” and “≥60 min/day” “<90 min/day” and “≥90 min/day” and “<120 min/day” and “≥120 min/day”, and we also classified them into groups of “<60 min/day”, “60–89 min/day”, “90–119 min/day” and “≥120 min/day”.
Age was classified as <35 and ≥35 years. Education was documented as the completed years of schooling and classified into three categories: 6–9 years (primary or junior high), 10–12 years (senior high), and >12 years (college and above). Body mass index (BMI) before pregnancy was classified as “<24 kg/m2” and “≥24 kg/m2”, monthly income (RMB) was categorized into 3 groups: “<5000”, “5001–10,000” and “>10,000”.
Data Analysis
The R software (version 4.3.2) and SPSS software (version 23.0) were used for data analysis. Means and standard deviations (SD) were calculated for quantitative data with a normal distribution, and median and interquartile range (IQR, [P25-P75]) were calculated for quantitative data with a skewed distribution. Frequency counts and proportions were calculated for qualitative variables, and χ2 test was used to analyze the differences between women with GDM and different demographic features.
The GBTM adopts a semi-parametric trajectory grouping strategy which assumes that there are a finite number of potential developmental trajectories in the GDM cohort, GDM women in each trajectory groups exhibit similar developmental patterns over the same temporal dimension. Different developmental trajectories of the indicators were described using polynomial function equations, and the model parameters were estimated using the maximum likelihood method (MLM). The ggplot package in R was used to explore the original development curve of the series of abnormal PG prevalence among GDM women at each prenatal checkup, and the HLME package was used to sequentially fit nine developmental trajectories. The models can estimate the probability of each GDM woman belonging to different trajectory groups by using four objective indicators. The Bayesian Information Criterion (BIC) is close to zero, serving as an indicator to confirm the goodness of fit of the data, which also reflects the consistency between group members in each trajectory after classification. The average posterior probability (AvePP) of each trajectory group is used as the basis for judging whether the model accurately reflects the sample data (a higher AvePP indicates better accuracy in the model), and it is generally regarded as AvePP >0.7. Entropy ≥0.7, with closer proximity to 1, was set as the criterion for determining the certainty and acceptability of the group classification, and the proportion of GDM women in each trajectory group should not be less than 5% of the total number of GDM women. This study assumed that only one group of trajectories gradually increased in number and finally fitted a maximum of three groups. After the number of groups was determined, the estimated values of each parameter were adjusted to reach a significant level by changing the order of variation for each group (repeatedly fitting the linear, quadratic, and cubic terms), thereby determining the shape of the trajectories for the final model.
Odds ratios (OR) and 95% confidence intervals (CI) were calculated using logistic regression to explore the association between daily PET and good PG prevalence among women with GDM based on Models A and B, respectively. Moreover, potential confounders adjusted for in the multivariate logistic regression model were identified using a directed acyclic graph (DAG). In this study, a P-value less than 0.05 (two tailed) was considered as statistical significance.
Results
In this study, 1122 women with GDM included 362 local residents (32.3%), and their ages ranged from 18 to 45 with an average age of 26.9 years (SD = 5.4). 60.6 Of the women with GDM, 60.6% had an educational level of college or above, and the majority of women with GDM were employed (1045, 93.1%) and had a monthly income of >5000 RMB (861, 76.7%). Moreover, 35.2% of women with GDM were overweight or obese (BMI ≥24kg/m2) before pregnancy, and 40.6% had a balanced diet with doctors’ suggestions after the confirmation of GDM, which was based on the “Dietary guide for patients with gestational diabetes mellitus (GDM)” formulated by The National Health Commission of the People’s Republic of China (version 2018). Table 1.
 |
Table 1 Demographic Features of Women with Gestational Diabetes Mellitus (GDM) |
Abnormal PG Prevalence and Trajectory Groups Classification Based on GBTM Model
The abnormal PG prevalence in Model A was 12.5% at antenatal Weeks 24–26 for GDM confirmation, and subsequently increased in the following seven antenatal checkups (ranging from 25% to 60%). Model B indicated that the abnormal PG prevalence was 100% at Weeks 24–26, and descended gradually during subsequent antenatal checkups (ranging from 55% to 73%). Figure 1.
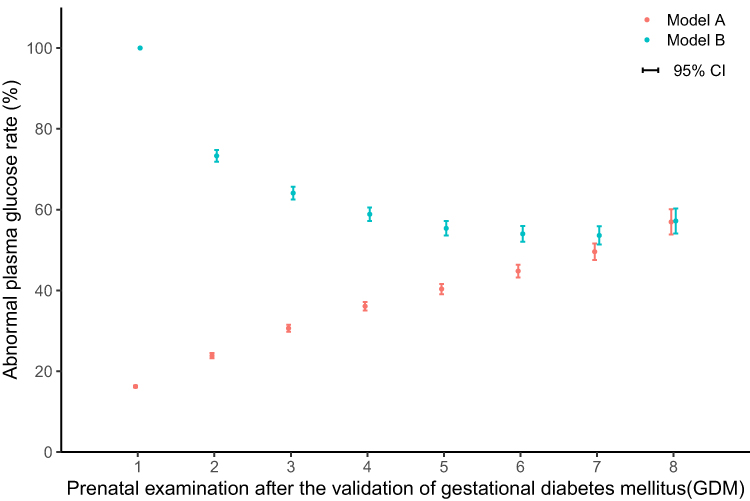 |
Figure 1 The abnormal rate of plasma glucose in each preset time-point for prenatal examination after the validation of gestational diabetes mellitus (GDM) among women in different Models. Abbreviation: CI, confidence interval. |
Based on GBTM, 1122 GDM women were classified into the good PGC group (n = 539) and bad PGC group (n = 583) in Model A, and into the good PGC group (n = 644) and bad PGC group (n = 478) in Model B. Detailed information on the abnormal PG prevalence at each time of routine antenatal checkups in the two groups, both in Models A and B, is depicted in Figure 2 Detailed information on the overall development curve for abnormal PG prevalence as well as the model fitting evaluation indicators in the two models is depicted in Supplementary Figure 1, Supplementary Table 1, Supplementary Table 2 and Figure 2.
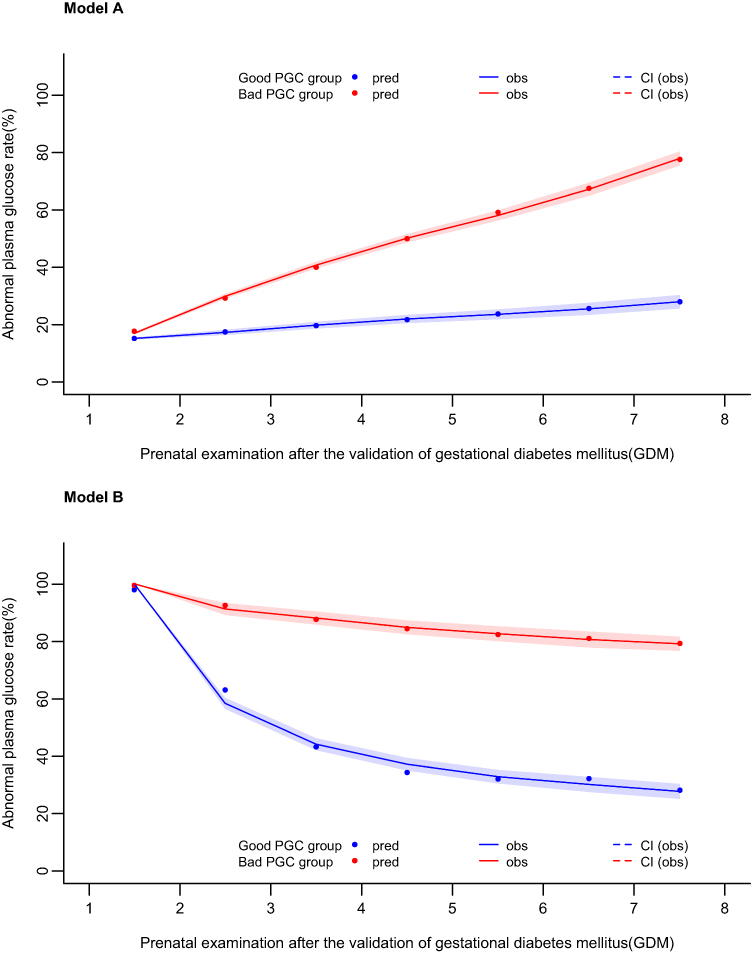 |
Figure 2 Trajectories of abnormal plasma glucose rate from prenatal examination after the validation of gestational diabetes mellitus (GDM) in Model A and Model B. Abbreviations: PGC, plasma glucose control; pred, prediction; obs, observation; CI, confidence interval. |
Prevalence of Good PGC Among Women with GDM
In this study, the prevalence of good PGC in Model A 48.0% (539/1122) and that in Model B was 57.4% (644/1122), demonstrating a lower abnormal PG rate in late pregnancy. In Model A, good PGC prevalence was higher in women with GDM with college or above education (53.8%), with >10000 RMB monthly income (52.2%), local residency status (52.5%), and BMI <24kg/m2 (53.5%), and the differences were all statistically significant (P < 0.05). In Model B, the prevalence of good PGC was higher in GDM women aged <35 years (59.0%), those with college and higher education (62.8%), with >10000 RMB monthly income (63.5%), and those with a BMI <25 kg/m2 (63.7%); the differences were also statistically significant (P < 0.05). Table 2.
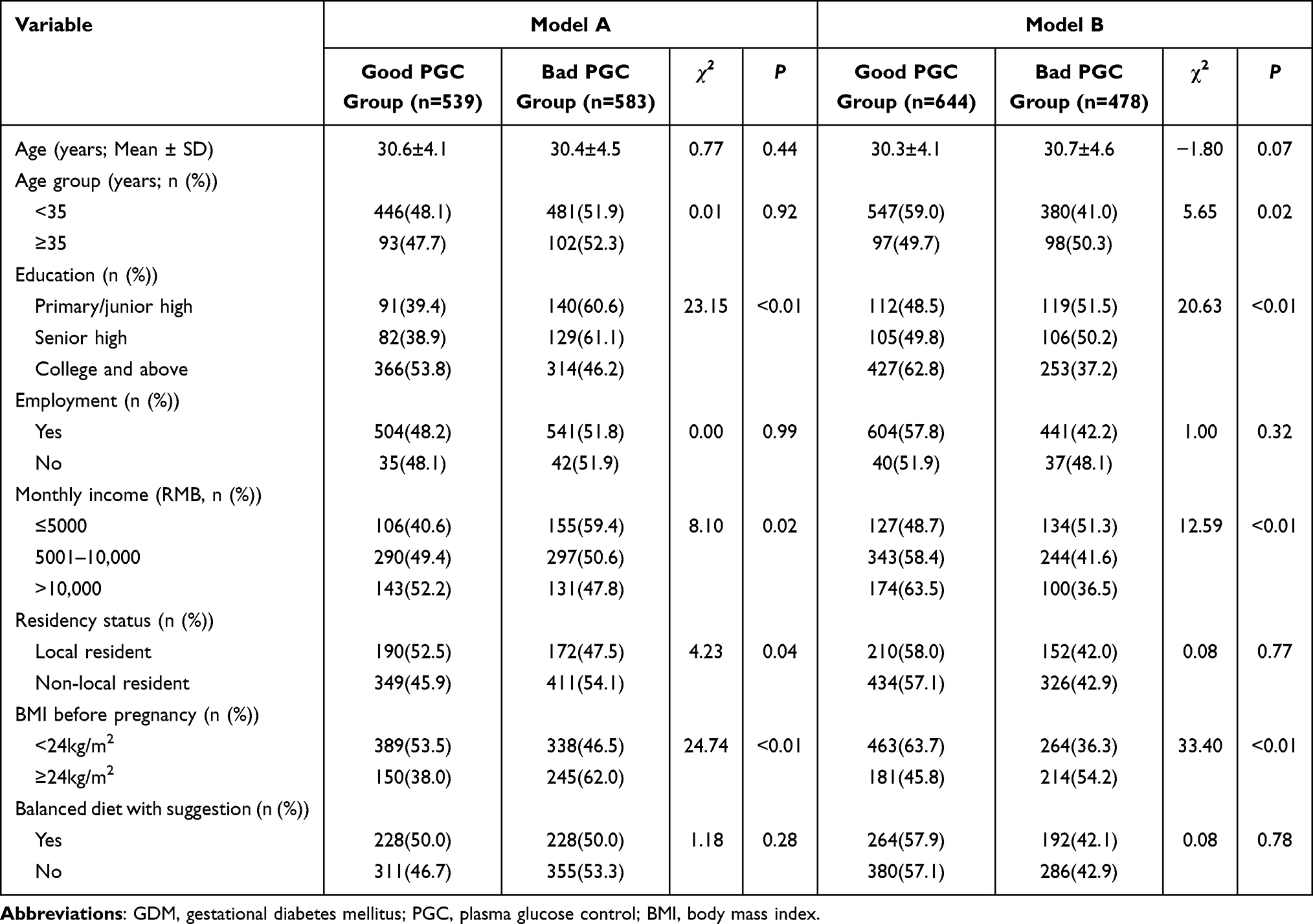 |
Table 2 Demographic Features among GDM Women with or without Good Plasma Glucose Control Classified Based on the Trajectory Analysis in Different Models (n = 1122) |
Association Between Physical Exercise Time and Good PGC in GDM Women
In this study, the median daily moderate-intensity exercise time among 1122 GDM women was 65 min (IQR = 45.0–90.0), with 38.9% of women with GDM exercising <60 min/day and 27.5% exercising ≥90 min/day. Regarding the dichotomized classification of daily PET based on different cutoff values, the proportion of GDM women with PET ≥30, 60, 90, and 120 min/day was 95.4%, 61.1%, 27.5%, and 7.9%, respectively. Table 3.
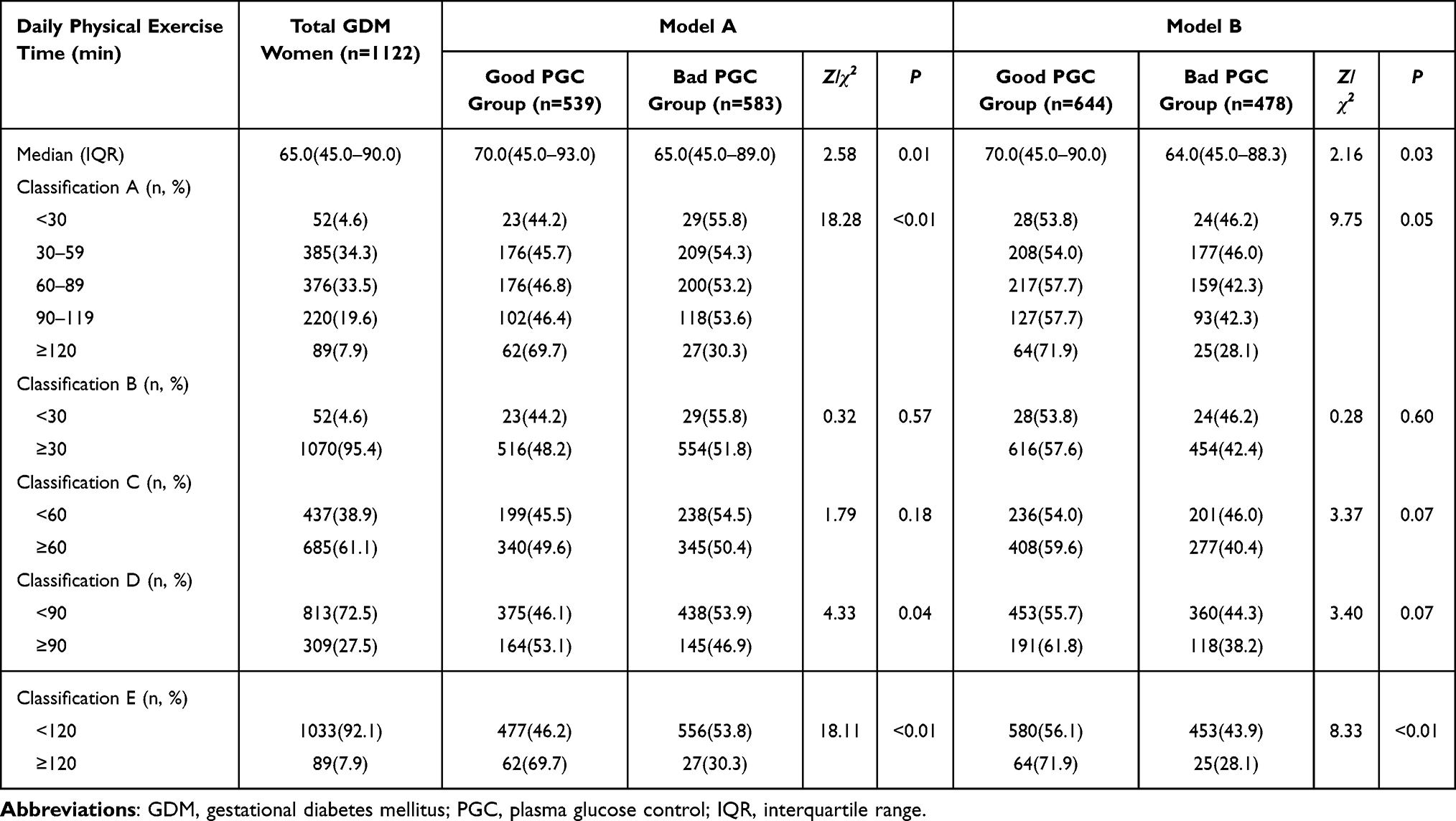 |
Table 3 Daily Physical Exercise Time among GDM Women with or without Good Plasma Glucose Control Classified Based on the Trajectory Analysis in Different Models (n = 1122) |
The median PET among GDM women in the good PGC group (70 min in both Models A and B) was significantly higher than that in the bad PGC group (65 min in Model A and 64 min in Model B) (P < 0.05). The prevalence of PG increased from 44.2% (<30 min/day group) to 69.7% (≥120 min/day group) in Model A 53.8% to 71.9% in Model B, which was statistically significant (P < 0.05). Furthermore, in the dichotomized classification groups, women with GDM in Model A with exercise time ≥90 min/day had a significantly higher PG prevalence than those with exercise time <90 min/day (53.1% vs 46.1%, P < 0.05), which was the same in the ≥120 min/day group compared with the <120 min/day group (69.7% vs 46.2%, P < 0.05). In Model B, women with GDM who exercised for ≥120 min/day also had a higher PG prevalence than those with an exercise time <120 min/day (71.9% vs 56.1%, P < 0.05). Table 3.
Factors Associated with Good PG Control in GDM Women
Seven factors were adopted to explore their independent and mutual influence on glycemic control in women with GDM. The variable assignment for each factor is shown in Supplementary Table 3.
Univariate logistic regression (LR) indicated that good PG prevalence in Model A was higher in women with GDM with exercise time ≥120 min/day (OR = 1.29, 95% CI: 1.08–1.52), college and higher education (OR = 1.16, 95% CI: 1.07–1.24), and higher monthly income (OR = 1.09 [95% CI: 1.02–1.17] for 5001–10000 RMB, OR = 1.12 [95% CI: 1.03–1.22] for >10000 RMB), but was lower in GDM women with non-local residency status (OR = 0.94, 95% CI: 0.88–1.00), and BMI ≥24kg/m2(OR=0.86, 95% CI: 0.81–0.91). Multivariate LR indicated that GDM women with PET ≥120 min/day had good PG control (OR = 1.32, 95% CI: 1.12–1.56), even after adjusting for age, education, monthly income, BMI, and dietary habits. Table 4.
 |
Table 4 The Influence of Physical Exercise Time on the Prevalence of GDM Women with Good Plasma Glucose Control Classified Based on the Trajectory Analysis in Model A (n = 1122) |
In Model B, univariate LR indicated that good PG prevalence was higher in women with GDM with exercise time ≥120 min/day, college and above education (OR = 1.15, 95% CI: 1.07–1.24), and higher monthly income (OR = 1.10 [95% CI: 1.03–1.18] for 5001–10000 RMB, and OR = 1.16 [95% CI: 1.07–1.26] for >10000 RMB), but was lower in GDM women aged ≥35 years (OR = 0.91, 95% CI: 0.84–0.98), and with BMI ≥24kg/m2 (OR = 0.84, 95% CI: 0.79–0.89). Multivariate LR indicated that GDM women with PET ≥120 min/day had good PG control (OR = 1.24, 95% CI: 1.05–1.46), even after adjusting for the aforementioned factors. Table 5.
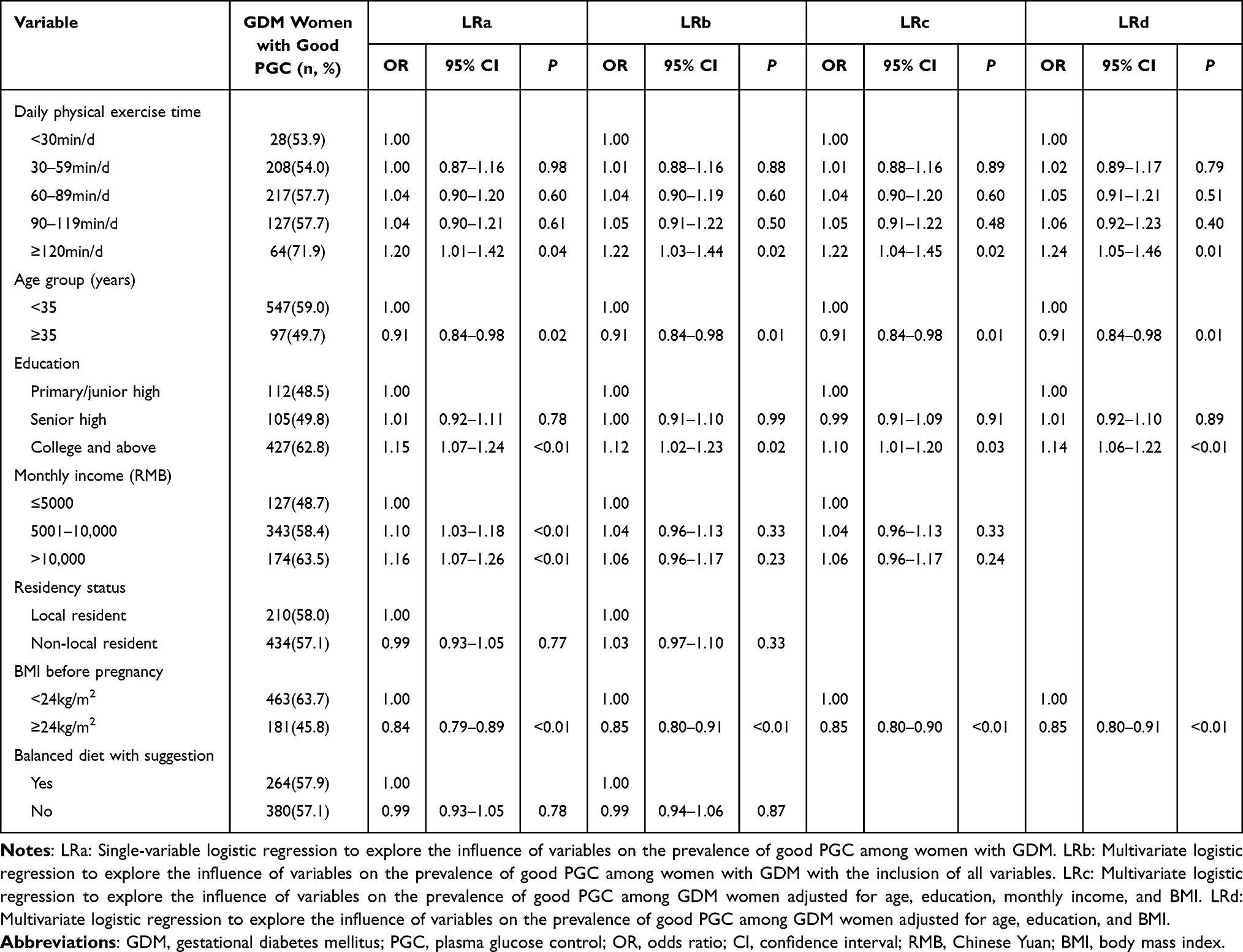 |
Table 5 The Influence of Physical Exercise Time on the Prevalence of GDM Women with Good Plasma Glucose Control Classified Based on the Trajectory Analysis in Model B (n = 1122) |
Subgroup Analyses
The impact of stratified population heterogeneity in different age levels was assessed in subgroup analyses. As depicted in the forest figures, multivariate logistic regression (LR) based on data among GDM women aged <35 years indicated that GDM women with PET ≥120 min/day had good PG control (Model A: OR = 1.41, 95% CI: 1.16–1.71; Model B: OR = 1.33, 95% CI: 1.09–1.61), with the adjustment of potential confounders. For GDM women aged ≥35 years, multivariate LR with the adjustment of potential confounders indicated that GDM women with PET ≥120 min/day also had good PG control (Model A: OR = 1.17, 95% CI: 0.82–1.66; Model B: OR = 1.22, 95% CI: 0.86–1.75), but without statistically significant. Figures 3 and 4.
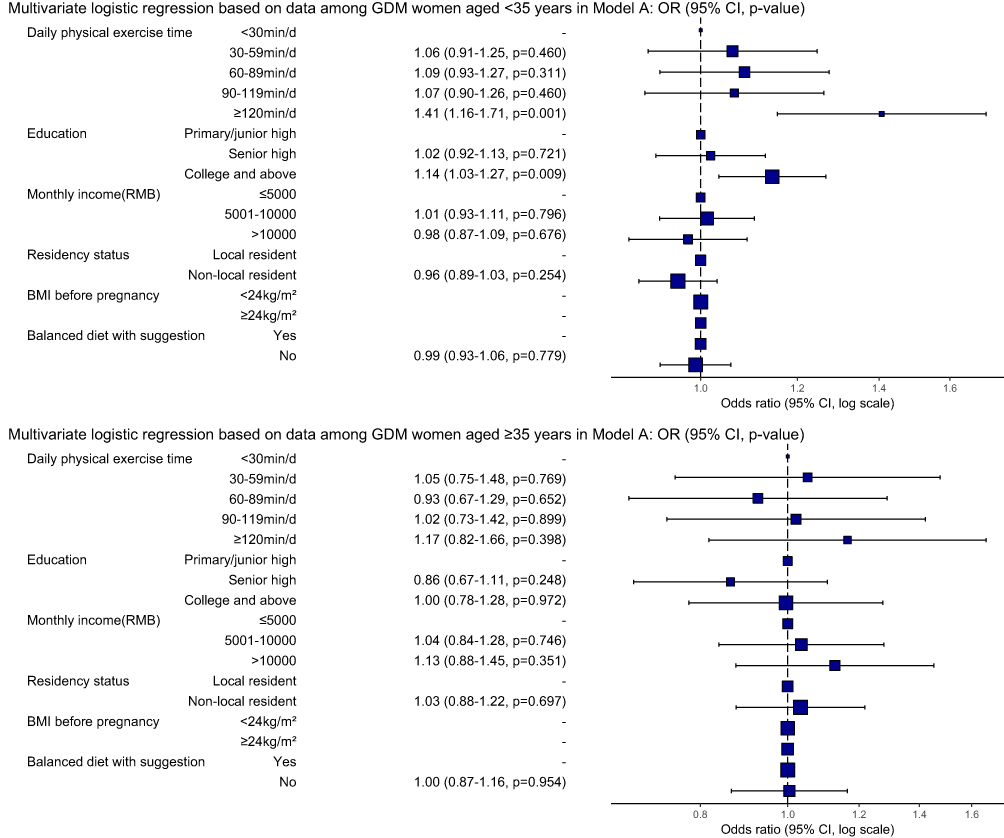 |
Figure 3 The influence of age on the association between physical exercise time and good plasma glucose prevalence among GDM women classified based on the trajectory analysis in Model A. Abbreviations: GDM, gestational diabetes mellitus; OR, odds ratio; CI, confidence interval; RMB, Chinese Yuan; BMI, body mass index. |
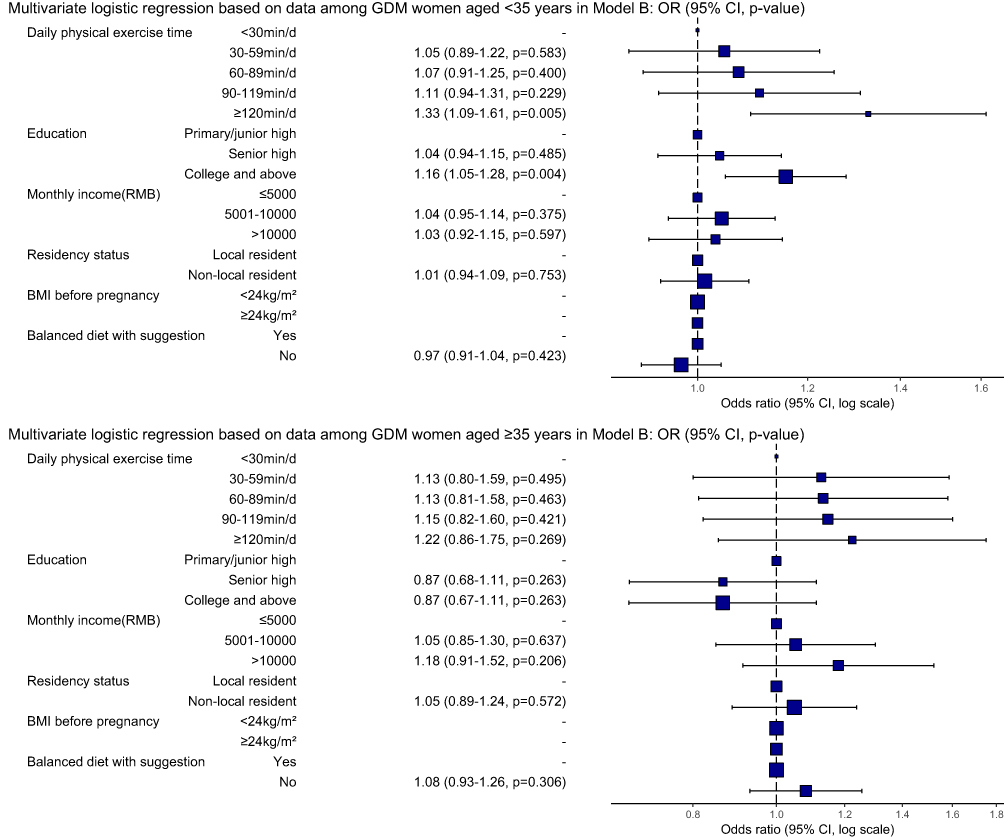 |
Figure 4 The influence of age on the association between physical exercise time and good plasma glucose prevalence among GDM women classified based on the trajectory analysis in Model B. Abbreviations: GDM, gestational diabetes mellitus; OR, odds ratio; CI, confidence interval; RMB, Chinese Yuan; BMI, body mass index. |
Discussion
To our knowledge, this is the first study to explore the association between long-daily PET and a low prevalence of glycemic abnormalities based on a series of abnormal PG rates collected through antenatal checkups by applying GBTM analysis among GDM women in China.
As a special type of diabetes, GDM has a complex pathogenesis, and its exact etiology is still unclear.18 Early prevention, diagnosis, and treatment are beneficial for glycemic control and complication prevention. Previous studies have shown that approximately 70–85% of women with GDM can effectively maintain normal PG levels through lifestyle interventions focused on diet and exercise.8,19 Due to the cultural disparity in China, it is difficult to implement dietary behavior change measures in women with GDM; therefore, physical exercise is more acceptable for them. Numerous studies have provided clinical evidence of the benefits of physical exercise during pregnancy. In this study, we found that GDM women with more daily PET tended to have a lower abnormal PG prevalence, which is in line with previous studies. Physical exercise can promote an increase in glycogen synthase, improve insulin sensitivity.20 Meanwhile, it can also enhance muscle glucose utilization.21
There is still a lack of multi-center, large-scale and high-quality clinical studies concerning the physical exercise and glycemic control during pregnancy in China. Therefore, unified consensus regarding the level of physical exercise among GDM women has not been established in China. So the guidelines stated in ACOG and CESP are weak recommendations and not suitable for GDM women in China. Moreover, Chinese and foreign GDM women are significantly different in physical fitness; some of them in China usually performed low-intensity physical exercise, which had an inferior glycemic control effect even with longer exercise time for METS compensation. In addition, evidence regarding exercise is beneficial during pregnancy is clear and valid.22 However, there is no consensus on the recommended physical exercise standard for women with GDM, especially with respect to the type, duration, and frequency of exercise, which further indicates the importance of proposing suitable guidance for Chinese GDM women.
GBTM is often applied in populations with significant heterogeneity.23 By modeling the development trajectory of a certain longitudinal indicator for individuals, it identifies potential trajectory groups within the population and studies whether there is a correlation between predictive factors and outcomes among these groups. In this study, GBTM analysis was used to classify GDM women into good PG and bad PG control groups in models A and B. When comparing the daily PET between trajectory groups in both models, we found that GDM women engaged in physical exercise for ≥120 min/day had optimal PG levels, even after adjusting for potential confounders, and confirmed the aforementioned association. Furthermore, we stratified the GDM women into <35 years group and ≥35 years group, and the association between PET and the prevalence of GDM women with good PG control was consistent in GDM women in <35 years group and ≥35 years group. Therefore, at least 120 min of moderate-intensity daily exercise is recommended for women with GDM to achieve good PG control in late pregnancy. A population survey in the United States showed that less than 15% of pregnant women met the widely accepted minimum recommendation of 150 minutes of exercise per week.24 In this study, the median daily PET was 65 minutes among GDM women in Shanghai, which was obviously a high level. This may due to the fact that after the diagnosis of GDM, obstetricians would explain the risks and benefits of physical exercise to GDM women through clinics and maternity schools, providing free professional guidance for them. Nevertheless, most women with GDM in China live with their parents, and pregnancy is usually treated as a special state that requires extra attention and recuperation by Chinese women and their parents. So when a GDM woman was recommended by the obstetrician to engage in more physical exercise, their parents would motivate them to do more daily physical exercise. Although parents are lack of expertise to provide a professional exercise guidance, their motivation could increase the amount of exercise times. All of these factors might explain why GDM women in China have more physical exercise time.
Previous studies have confirmed that women who are overweight or obese (BMI ≥24 kg/m2) before pregnancy have a higher risk of developing GDM,25 consistent with the findings of this study. This mechanism may be related to the sensitivity of BMI to serum leptin and insulin.26,27 When serum leptin levels are elevated, the responsiveness of the target organs or tissues to insulin decreases, leading to insulin resistance. Furthermore, the efficiency of insulin upon glucose uptake or utilization is lower than normal, leading to obesity and diabetes. Conversely, pregnant women with a high pre-pregnancy BMI have more fat accumulation in their bodies; however, insulin receptors in adipose tissue are relatively lower,28 and insulin secretion during pregnancy is insufficient, which ultimately results in glucose metabolism disorders. Min Zhao et al found that every 3kg/m2 increase in BMI before pregnancy increases the risk of GDM by 22% (adjusted OR, 1.22 (1.21,1.24)).29 Besides, this study also found that GDM in women aged ≥35 years had 1.10 times higher bad PG prevalence than that in women aged <35 years, which was also reported in previous studies, demonstrating that advanced gestational age is a prominent risk factor for GDM.30 The mechanism linking age with GDM is not yet conclusively established, which may be related to the decline in pancreatic β-cell function and insulin sensitivity with increasing age, as well as the regulation ability of glucose metabolism in elderly pregnant women, is not as effective as in young women.
The major strength of this study was the application of GBTM to depict the trend of PG levels with repeated measurements and to classify all patients into good and bad PGC groups to explore its association with PET based on a GDM prospective cohort. Additionally, this study defined new types of research indicators and applied two sets of formulas to calculate abnormal PG prevalence for sensitivity analysis, which ensured the credibility and consistency of the findings. Moreover, this study had relatively less recall bias because information about fasting and 2-hour postprandial glycemic values during each antenatal checkup and pregnancy and childbirth history was extracted directly from the delivery records. Finally, the use of DAG to identify potential confounders and then adjusting for them in the logistic regression analysis, which ensured a relatively unbiased assessment, was another strength of this study.
This study had some limitations. First, not all potential confounders were collected, including genetic factors (GDM family history, high expression of susceptibility genes, etc.), daily dietary information during pregnancy (supplementation of vitamins, minerals, etc.), and living environment factors, which may indicate that this study did not control for all potential confounders. Therefore, it is necessary to include more adjusted factors in the model and quantify each factor as specific indicators for objective evaluation in future studies. Second, information on exercise was collected through face-to-face interviews, which may have introduced over-reporting bias. Therefore, we should actively apply more rigorous research designs, including teaching pregnant women to wear devices to measure physiological parameters such as heart rate and blood oxygen saturation to evaluate their actual physical exercise level. Third, some of the 20 types of physical exercise were usually not moderate-intensity exercises, such as house cleaning, Tai Chi, and yoga, which might have induced a relatively longer physical exercise time but inferior glycemic control effect, even after METS conversion. Fourth, since most of participants in this study were young and active, the glycemic control due to physical exercise might favor the findings and induce some bias. Fifth, a detailed diet assessment of GDM women was not performed; therefore, we were unable to investigate and analyze the combined effects of exercise and diet in this study. Sixth, women with GDM were recruited from Songjiang District in Shanghai, which ensured higher internal authenticity, but lower generalizability of the findings. Therefore, further improvements should be considered in future studies.
Conclusion
This study based on a large prospective cohort and GBTM analysis demonstrates that exercise is beneficial for achieving glycemic control, and GDM women are required to engage in at least 120 minutes of daily physical exercise to maintain stable blood glucose levels, especially those of older age and with a BMI ≥24kg/m2. We recommend that women need to choose the appropriate type and intensity of exercise based on their actual physical conditions. And consider METS conversion of longer physical exercise time for activities with low intensity. Moreover, daily physical exercise plans should be formulated with the consultation of professional health workers.
Abbreviations
ACOG, American College of Obstetricians and Gynecologists; AvePP, average posterior probability; BIC, Bayesian information criterion; BMI, body mass index; CI, confidence interval; CSEP, Canadian Society for Exercise Physiology; DAG, directed acyclic graph; GBTM, Group-based trajectory model; GDM, gestational diabetes mellitus; MET, metabolic equivalent task; MLM, maximum likelihood method; IADPSG, International Association of Diabetes and Pregnancy Study Group; IDF, International Diabetes Federation; IQR, interquartile range; LR, logistic regression; OR, odds ratio; OGTT, oral glucose tolerance test; PET, physical exercise time; PG, plasma glucose; PGC, plasma glucose control; SD, standard deviations.
Data Sharing Statement
Data for this study are available upon request from the corresponding author. The request should state the title and aim of the research for which data were requested.
Ethical Approval and Informed Consent
This study was reviewed and authorized by the Institutional Review Board of Songjiang Maternal and Children’s Healthcare Hospital (IRB#-2019-12-003). Informed consent was obtained from each participant before the start of the study, which was strictly performed in accordance with the Declaration of Helsinki.
Acknowledgments
We thank Professor Michael Engelau (Center for Disease Control and Prevention, US) and Professor Klossi Chen (University of California, Los Angeles) for providing suggestions and comments on this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Clinical Research Program of the Shanghai Municipal Health Commission (202240371), Clinical Research Plan of SHDC (SHDC2022CRS053, SHDC2024CRX032), Intelligence Fund of Shanghai Skin Diseases Hospital (2021KYQD01), and the Shanghai Talent Development Fund (2021073). The funder had no role in the study design, data collection and analysis, decision to publish, or manuscript preparation.
Disclosure
The authors report no conflicts of interest in this work. This paper has been uploaded to SSRN as a preprint: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5050326.
References
1. Sweeting A, Wong J, Murphy HR, Ross GP. A clinical update on gestational diabetes mellitus. Endocr Rev. 2022;43(5):763–793. doi:10.1210/endrev/bnac003
2. Ye W, Luo C, Huang J, Li C, Liu Z, Liu F. Gestational diabetes mellitus and adverse pregnancy outcomes: systematic review and meta-analysis. BMJ. 2022;377:e067946. doi:10.1136/bmj-2021-067946
3. Bellamy L, Casas JP, Hingorani AD, Williams D. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet. 2009;373(9677):1773–1779. doi:10.1016/s0140-6736(09)60731-5
4. Wang H, Li N, Chivese T, et al. IDF diabetes atlas: estimation of global and regional gestational diabetes mellitus prevalence for 2021 by international association of diabetes in pregnancy study group’s criteria. Diabet Res Clin Pract. 2022;183:109050. doi:10.1016/j.diabres.2021.109050
5. Wu S, Jin J, Hu KL, Wu Y, Zhang D. Prevention of gestational diabetes mellitus and gestational weight gain restriction in overweight/obese pregnant women: a systematic review and network meta-analysis. Nutrients. 2022;14(12). doi:10.3390/nu14122383
6. Zhang HX, Zhao YY, Wang YQ. Analysis of the characteristics of pregnancy and delivery before and after implementation of the two-child policy. Chin Med J. 2018;131(1):37–42. doi:10.4103/0366-6999.221268
7. Chehab RF, Ferrara A, Greenberg MB, Ngo AL, Feng J, Zhu Y. Glycemic control trajectories and risk of perinatal complications among individuals with gestational diabetes. JAMA Network Open. 2022;5(9):e2233955. doi:10.1001/jamanetworkopen.2022.33955
8. Rasmussen L, Poulsen CW, Kampmann U, Smedegaard SB, Ovesen PG, Fuglsang J. Diet and healthy lifestyle in the management of gestational diabetes mellitus. Nutrients. 2020;12(10):3050. doi:10.3390/nu12103050
9. Mottola MF, Davenport MH, Ruchat SM, et al. 2019 Canadian guideline for physical activity throughout pregnancy. Br J Sports Med. 2018;52(21):1339–1346. doi:10.1136/bjsports-2018-100056
10. Physical activity and exercise during pregnancy and the postpartum period: ACOG committee opinion, number 804. Obstet Gynecol. 2020;135(4):e178–188. doi:10.1097/AOG.0000000000003772
11. Wang R, Yang Q, Sun T, et al. Physical exercise is associated with glycemic control among women with gestational diabetes mellitus: findings from a prospective cohort in Shanghai, China. Diabetes Metab Syndr Obes. 2021;14:1949–1961. doi:10.2147/dmso.S308287
12. Zhang R, Gao X, Sun T, et al. Longer physical exercise duration prevents abnormal fasting plasma glucose occurrences in the third trimester: findings from a cohort of women with gestational diabetes mellitus in Shanghai. Front Endocrinol. 2023;14:1054153. doi:10.3389/fendo.2023.1054153
13. Yang F, Peng C, Peng L, et al. Group-based trajectory modeling of intracranial pressure in patients with acute brain injury: results from multi-center ICUs, 2008–2019. CNS Neurosci Ther. 2022;28(8):1218–1228. doi:10.1111/cns.13854
14. Nagin DS. Group-based trajectory modeling: an overview. Ann Nutr Metab. 2014;65(2–3):205–210. doi:10.1159/000360229
15. Chen S, Persson M, Wang R, et al. Random capillary glucose levels throughout pregnancy, obstetric and neonatal outcomes, and long-term neurodevelopmental conditions in children: a group-based trajectory analysis. BMC Med. 2023;21(1):260. doi:10.1186/s12916-023-02926-3
16. Gao X, Zhang X, Kuai L, et al. More physical exercise is required for overweight or obese women with gestational diabetes mellitus to achieve good plasma glucose control during pregnancy: finding from a prospective cohort in Shanghai. Diabetes Metab Syndr Obes. 2023;16:3925–3935. doi:10.2147/dmso.S439106
17. Wang R, Chen J, Yao F, et al. Number of parous events affects the association between physical exercise and glycemic control among women with gestational diabetes mellitus: a prospective cohort study. J Sport Health Sci. 2022;11(5):586–595. doi:10.1016/j.jshs.2022.03.005
18. Johns EC, Denison FC, Norman JE, Reynolds RM. Gestational diabetes mellitus: mechanisms, treatment, and complications. Trends Endocrinol Metab. 2018;29(11):743–754. doi:10.1016/j.tem.2018.09.004
19. American Diabetes Association. 13. Management of diabetes in pregnancy. Diabetes Care. 2017;40(Supply 1):S114–S119. doi:10.2337/dc17-S016
20. Dela F, Larsen JJ, Mikines KJ, Ploug T, Petersen LN, Galbo H. Insulin-stimulated muscle glucose clearance in patients with NIDDM. Effects of one-legged physical training. Diabetes. 1995;44(9):1010–1020. doi:10.2337/diab.44.9.1010
21. Goodyear LJ, Kahn BB. Exercise, glucose transport, and insulin sensitivity. Annu Rev Med. 1998;49:235–261. doi:10.1146/annurev.med.49.1.235
22. Song C, Li J, Leng J, Ma RC, Yang X. Lifestyle intervention can reduce the risk of gestational diabetes: a meta-analysis of randomized controlled trials. Obes Rev. 2016;17(10):960–969. doi:10.1111/obr.12442
23. Li L, Yang H. Heterogeneity in adolescents’ non-suicidal self-injury behaviour trajectories based on the group-based trajectory model and a decision tree analysis of family-related determinants. Psychol Res Behav Manag. 2023;16:3359–3371. doi:10.2147/prbm.S427090
24. Evenson KR, Wen F. Prevalence and correlates of objectively measured physical activity and sedentary behavior among US pregnant women. Prev Med. 2011;53(1–2):39–43. doi:10.1016/j.ypmed.2011.04.014
25. Wang MC, Shah NS, Petito LC, et al. Gestational diabetes and overweight/obesity: analysis of nulliparous women in the U.S. 2011–2019. Am J Prev Med. 2021;61(6):863–871. doi:10.1016/j.amepre.2021.05.036
26. Zheng X, Niu S. Leptin-induced basal Akt phosphorylation and its implication in exercise-mediated improvement of insulin sensitivity. Biochem Biophys Res Commun. 2018;496(1):37–43. doi:10.1016/j.bbrc.2017.12.161
27. Soheilykhah S, Mojibian M, Rahimi-Saghand S, Rashidi M, Hadinedoushan H. Maternal serum leptin concentration in gestational diabetes. Taiwan J Obstet Gynecol. 2011;50(2):149–153. doi:10.1016/j.tjog.2011.01.034
28. Saltiel AR, Kahn CR. Insulin signalling and the regulation of glucose and lipid metabolism. Nature. 2001;414(6865):799–806. doi:10.1038/414799a
29. Zhao M, Yang S, Hung TC, Zheng W, Su X. Association of pre- and early-pregnancy factors with the risk for gestational diabetes mellitus in a large Chinese population. Sci Rep. 2021;11(1):7335. doi:10.1038/s41598-021-86818-7
30. Li Y, Ren X, He L, Li J, Zhang S, Chen W. Maternal age and the risk of gestational diabetes mellitus: a systematic review and meta-analysis of over 120 million participants. Diabet Res Clin Pract. 2020;162:108044. doi:10.1016/j.diabres.2020.108044
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
More Physical Exercise is Required for Overweight or Obese Women with Gestational Diabetes Mellitus to Achieve Good Plasma Glucose Control During Pregnancy: Finding from a Prospective Cohort in Shanghai
Gao X, Zhang X, Kuai L, Yang Q, Li H, Zhang R, Li B, Wang R
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3925-3935
Published Date: 5 December 2023