Back to Journals » Risk Management and Healthcare Policy » Volume 16
Monkeypox Knowledge Investigation and Knowledge Gap Analysis: An Online Cross-Sectional Survey in China
Authors Wang H ![]() , Song W, Wang Y, Wu X
, Song W, Wang Y, Wu X
Received 17 October 2023
Accepted for publication 10 December 2023
Published 13 December 2023 Volume 2023:16 Pages 2741—2756
DOI https://doi.org/10.2147/RMHP.S442135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Gulsum Kaya
Han Wang,1,* Wei Song,2,* Yuwei Wang,1 Xiwen Wu3
1School of Journalism and Communication, Jinan University, Guangzhou, Guangdong, 510632, People’s Republic of China; 2School of Journalism and Information Communication, Huazhong University of Science and Technology, Wuhan City, Hubei, 430074, People’s Republic of China; 3School of Media and Communication, University of Leeds, Leeds, UK
*These authors contributed equally to this work
Correspondence: Xiwen Wu, School of Media and Communication, University of Leeds, Leeds, LS29JT, UK, Tel +44 7536 249140, Email [email protected]
Background: Monkeypox, as a significant public health concern, warrants a thorough investigation into public knowledge and understanding. Especially in non-endemic areas like China, exploring the factors contributing to knowledge and understanding gaps is crucial for effective disease management and prevention strategies.
Objective: This study aims to assess the level of monkeypox knowledge among the Chinese public and to identify the factors that influence this knowledge, particularly focusing on the knowledge gaps between different educational groups.
Methods: An online cross-sectional survey was conducted involving 720 participants stratified by age, between July and August 2023. The survey used a modified monkeypox knowledge questionnaire, and hierarchical regression analysis was employed to analyze the data.
Results: The study revealed a significant knowledge gap in the understanding of monkeypox among the Chinese public. Key factors influencing this knowledge included educational level, perceived relevance of information, interpersonal communication, and exposure to social media and official health websites. Notably, exposure to social media was found to widen the knowledge gap between different educational groups, with its positive impact more pronounced in individuals with at least a junior high school education.
Conclusion: The findings emphasize the need for varied communication strategies to effectively disseminate information about monkeypox and bridge the existing knowledge gaps. Tailoring health communication to different educational levels and utilizing diverse information sources are crucial for improving public understanding and containment of monkeypox.
Keywords: monkeypox, health knowledge, knowledge gap, online survey, media exposure, awareness, China
Introduction
Mpox (monkeypox) is a zoonotic orthopoxvirus infectious disease caused by the monkeypox virus.1 First identified in 1958 in research monkeys in Denmark, this enveloped double-stranded DNA virus belongs to the Orthopoxvirus genus within the Poxviridae family.2 The first documented human case was a 9-month-old boy in the Democratic Republic of the Congo in 1970.3 Historically endemic in several African countries, Mpox has been characterized by periodic outbreaks and sporadic cases. Although cases of monkeypox were reported globally, the virus primarily remained confined to specific African regions. However, in May 2022, a significant resurgence of Mpox occurred, leading to a global epidemic. This resurgence highlighted the disease’s potential for wider international spread beyond its traditional endemic regions. In response to this escalating situation, the World Health Organization declared the current monkeypox outbreak a Public Health Emergency of International Concern (PHEIC) on July 23, 2022.4 As of August 23, 2023, there have been 89,581 reported infection cases worldwide.5 In July 2022, mainland China reported a substantial increase in confirmed cases of monkeypox, with 491 new infections, a figure more than four times the number reported in June.6 This recent data, as reported by the China Centers for Disease Control and Prevention, underscores the continued global impact of this disease, which has now become an extra burden on global health.7
A significant barrier to preventing the recurrence of human monkeypox may be the lack of understanding about this infection. The lack of knowledge among the public, coupled with the widespread dissemination and rapid spread of misinformation about the disease, is one of the challenges in controlling the current epidemic.8 Appropriate levels of health knowledge in the community positively affect health promotion and disease prevention.9 In previous studies on infectious diseases such as AIDS10 and influenza,11 scholars generally believed that individuals with a comprehensive understanding of infectious diseases can accurately assess the threat of the virus and take proactive preventive measures. Similarly, public health knowledge is essential in reducing risky behaviors and adopting protective and preventive measures during public health emergencies.12 Assessing a general understanding of viral diseases can help determine how they seek health information and prepare adequately for the outbreak of infectious diseases.13 Therefore, investigating the factors influencing the acquisition of public knowledge about monkeypox is of great importance. However, according to our understanding, more research is needed on monkeypox knowledge measurement instruments, factors influencing monkeypox knowledge, and studies on the knowledge gap between different educational level groups. Further related research can assist healthcare professionals and health departments in conducting more effective health education and propaganda activities, raising public disease prevention awareness, and thereby better preventing and controlling the spread of monkeypox. Therefore, this study aims to optimize the measurement instrument for monkeypox knowledge, understand the factors influencing monkeypox knowledge, and explore the knowledge gap regarding monkeypox.
Background
Measurement of Health Knowledge and Monkeypox Knowledge Instrument
Health knowledge encompasses information about disease etiology, prevalence, risk factors, prevention, transmission, symptoms, treatment, health services, and patient rights.14 Recognized as crucial for influencing health behaviors and outcomes, health knowledge is particularly vital during public health emergencies, where it serves as a key strategy for safeguarding public health.15 Its measurement is instrumental in assessing the efficacy of health education and promotional campaigns and in tailoring health information to the public’s understanding.16
The emergence of human monkeypox as a sudden public health event necessitates the design of specific knowledge measurement instruments. Existing instruments for measuring monkeypox knowledge were developed by Harapan et al17 drawing on information from the US Centers for Disease Control and Prevention. This instrument comprises a knowledge survey questionnaire with 21 true/false questions. Correct answers are awarded one point, while incorrect ones receive zero points. The aggregate score, which can range from 0 to 21, indicates the level of knowledge, with higher scores indicating better knowledge. This survey tool has been deployed in Indonesia,17 the United Arab Emirates,18 and the Philippines8 to gauge monkeypox knowledge. However, the extant research has not delved deeply into categorizing health knowledge. Given that the definition of health knowledge reveals its multifaceted categorization, and these categories, derived from authorized external sources, are deemed definitive and factual.12 Given health knowledge’s multifaceted nature, a detailed categorization is critical for pinpointing gaps in health promotion efforts. Consequently, refining and optimizing monkeypox knowledge measurement tools is essential for a more accurate assessment of public understanding in diverse knowledge areas of the disease.
Predictive Factors of Monkeypox Knowledge
Many factors influence the acquisition and comprehension of health knowledge. Among them, socio-economic determinants stand out as one of the pivotal predictive factors. For instance, the educational level has been established to correlate with dental health knowledge.19 Furthermore, research indicated that socio-economic variables, such as ethnicity and social class, affect how individuals acquire, seek, process, and utilize health information and with eventual health outcomes.20 Such findings underscore the potential influence of socio-economic factors on health knowledge.
The source of information emerges as another crucial factor impacting health knowledge. Empirical evidence substantiates that mass media profoundly alter individual health behaviors21 and enhance the public’s cognizance of disease symptoms and signs.22 Confronted with unfamiliar viruses or diseases, people must use relevant knowledge. Various media channels have risen to prominence as primary avenues for health knowledge acquisition. In this digital age, the internet and social media platforms are progressively establishing themselves as pivotal sources of health information.23 For the elderly demographic, however, traditional media outlets such as magazines, television, and radio persist as vital conduits of health-related information.24 Beyond media consumption, interpersonal communication has significantly influenced one’s perceptions of diseases.25 For instance, a study on a rural community in eastern Nigeria revealed that interpersonal dialogue effectively heightened the community’s awareness of COVID-19.26
Beyond the avenues of information, individuals’ reception and processing of information are influenced by many psychological factors. Notably, perceived fear and the salience of information have been demonstrated to significantly impact the acceptance and utilization of health knowledge. Numerous studies have confirmed that perceived fear and information salience can amplify attention to, comprehension of, and retention of health information, thereby predicting health knowledge acquisition. For instance, Tannenbaum et al found that health advertisements employing fear-based strategies garnered more attention and retention from viewers than those without such tactics.27 Research by Robert J. Griffin and colleagues postulated that the perceived salience of information inclines individuals to seek and process health-related information in diverse ways.28 Furthermore, when this information is deemed highly pertinent to an individual’s life, they are more likely to embrace it.
While some studies have ventured into the predictive factors of monkeypox knowledge, the existing body of research remains insufficient and does not encapsulate all relevant predictive elements. As such, a more comprehensive exploration of the predictive determinants underpinning monkeypox knowledge is imperative.
The Monkeypox Knowledge Gap
Tichenor et al proposed the “knowledge gap” hypothesis in the 1970s, arguing that disseminating media information would increase the knowledge gap between people of different socio-economic statuses (classes).29 People with higher education levels are more capable of acquiring new information than those with lower education levels. With increased media information over time, people with higher education levels will obtain more helpful information, widening the “knowledge gap” between the two classes. This framework is particularly salient in health communication, shedding light on the potential to mitigate health disparities.30 Vulnerable societal groups that bear the brunt of subpar health outcomes are often the most deprived of knowledge acquisition opportunities, perpetuating health inequalities.31
With continuous refinement and development of the “knowledge gap” hypothesis, an increasing body of research has focused on the “knowledge gap” in health-related topics. For instance, a study investigating the correlation between media consumption and HIV/AIDS awareness among residents in Northwestern Ethiopia indicated that increasing media usage narrowed the knowledge gap between those with high and low educational attainment.32 Conversely, a study on media use and COVID-19 awareness among the Chinese populace demonstrated that frequent internet media usage widened the knowledge gap between these two educational cohorts. In contrast, other media forms were inconclusive in predicting variations in the knowledge gap among these educational groups.16
Monkeypox, a pivotal health concern due to its recurrent outbreaks, has increasingly threatened human health. Public awareness and accurate knowledge are quintessential for controlling its spread and mitigating its impact. The knowledge gap hypothesis offers a theoretical framework to understand and address health disparities. Specific to the monkeypox knowledge gap, research findings can equip public health agencies with strategies for effective communication, aiming to reduce health inequities. Overall, more discussions are needed regarding the monkeypox knowledge gap, especially the role of the media in either widening or narrowing the knowledge gap between different educational level groups. A deeper exploration of this knowledge gap is paramount to addressing health disparities stemming from information dissemination imbalances. Based on the research background, this study proposes the following research hypotheses and research questions:
H1: The level of education can significantly and positively predict scores on monkeypox knowledge.
H2: Exposure to different sources of information can significantly and positively predict scores on monkeypox knowledge.
H3: Psychological factors (perceived fear and perceived significance of information) can significantly and positively predict scores on monkeypox knowledge.
H4: Exposure to different sources of information can significantly predict the knowledge gap of monkeypox among different educational level groups.
RQ1: If there is a significant prediction, how does exposure to different sources of information affect the knowledge gap of monkeypox among various educational groups? Does it widen or narrow the gap?
Materials and Methods
Study Design
This study employed a cross-sectional design in accordance with the STROBE statement33 and aimed to optimize the measurement instrument for monkeypox knowledge, investigate the factors influencing monkeypox knowledge among healthcare professionals, and explore the knowledge gap regarding monkeypox in a diverse population sample.
Study Setting and Participants
From July to August 2023, we conducted a cross-sectional survey using the services of the professional data survey company “Tencent Questionnaire”. The company was tasked with distributing paid online questionnaires, with a budget of approximately 2000 RMB. Tencent Questionnaire possesses a database of 3 million potential respondents, distributed reasonably across gender, age, occupation, and region. For sample selection, we entrusted “Tencent Questionnaire” to distribute 1349 questionnaires using stratified sampling, referencing the age data structure of China’s Seventh National Population Census. Participants for the study were exclusively individuals aged 18 and above, as those under 18 were excluded due to ethical concerns regarding the participation of minors.
Sample Size
Ultimately, 755 valid samples were collected for this study, with an effective recovery rate of 55.96%. Throughout the process, the company ensured the data’s quality and validity. After distributing and collecting the data, the company provided the final valid data to the researchers, but the detailed recruitment process was not disclosed. During the final analysis of this study, samples of participants under 18 years of age, totaling 35, were excluded. The sample of this study covers all provincial administrative regions in China. According to the Kendall sample estimation method for multivariate analysis, the minimum sample size should be ten times the number of scale items.34 For our survey, which includes 41 scale items, this method recommends a minimum sample size of 410. Our study achieved a final sample size of 720, substantially exceeding this recommended minimum.
Ethical Approval
The research was approved by the Ethical Committee for Social Sciences at Jinan University (IRB No. A2207001-029) on July 19, 2022, and was conducted in accordance with the principles of the Declaration of Helsinki, the principles of bioethics, relevant domestic laws and regulations, and internationally recognized ethical and safety guidelines.
Informed Consent
The informed consent process in this study was conducted online. Prior to participating in the survey, individuals were presented with an informed consent statement. This statement outlined the study’s purpose, assured confidentiality and anonymity of responses, and emphasized that participation was entirely voluntary and without any repercussions for withdrawal. Participants were informed that by clicking the “next” button after reading the consent statement, they were agreeing to participate in the survey. Additionally, it was made clear that they could withdraw from the survey at any point without any obligation to explain their reasons for doing so. This process ensured that participants were well-informed about the nature of the study and their rights as participants, in line with ethical research standards.
Instrument
Monkeypox Knowledge
The study utilized a monkeypox knowledge survey questionnaire, originally developed by Harapan et al, which was based on the Centers for Disease Control and Prevention (CDC) guidelines from 2020.17 This questionnaire consists of 22 multiple-choice questions, each scored with 1 point for a correct answer, allowing for a total score range of 0 to 22 points. The optimization of this instrument in our study focused on three main aspects: incorporating the local context and diverse academic literature sources about monkeypox,35–37 segmenting knowledge into six categories (current status of monkeypox, basics, transmission modes, symptoms, prevention, and treatment), and modifying the response options by adding a “Don’t know” choice to minimize guesswork. This study retained some of the question designs from the existing monkeypox knowledge measurement scale. Three linguists translated them from the original English into Chinese for retained questions. Throughout the translation process, semantic equivalence standards and procedures were consistently used to ensure effective and accurate translation of the questions.38 The translated instrument underwent a pilot test among 30 participants to identify errors and inconsistencies. Ultimately, the instrument’s Cronbach’s alpha was 0.93, indicating high reliability.39
Media Exposure
This variable assesses individuals’ exposure to various media sources (Online News, Official Health Websites, Print Media, Radio, and Television) for information related to Monkeypox. The period of interest spans from the initial recognition of the outbreak to a defined endpoint. Following the practices in past research,16 we employed a seven-level scale (Cronbach’s alpha = 0.71) consisting of four items to measure this exposure. Participants were asked, “In the past two months, how often have you been exposed to information about Monkeypox through the following media?” Response options ranged from “1. Never” to “7. Always”.
Interpersonal Communication
The interpersonal communication variable was measured by a mature seven-level scale31,32 with two items (Cronbach’s alpha = 0.92): 1. How often do you participate in discussions related to monkeypox information or aimed at enhancing your understanding of monkeypox? 2. How often do you initiate a conversation with others about monkeypox?
Psychological Factors
This section primarily measures two psychological factors: perceived fear and perceived salience of information. Based on the relevant literature,40 two statements about perceived fear were set: 1. The monkeypox virus makes me feel afraid. 2. My family might get infected with the monkeypox virus. The scale has good internal consistency (Cronbach’s alpha = 0.84). According to relevant literature,28 three statements were set concerning the perceived salience of information: 1. I believe the information related to the monkeypox virus communicated through different channels is highly relevant. 2. I think the information about the monkeypox virus communicated through different channels is highly relevant to my friends, family, and community members around me. 3. The information about the monkeypox virus communicated through various channels is helpful for my current situation. Respondents were asked to choose from “1. Strongly Disagree” to “7. Strongly Agree”, and the scale has good internal consistency (Cronbach’s alpha = 0.94, M = 4.98, SD = 1.73).
Level of Education
In previous studies on knowledge gaps, educational level was often used to measure socio-economic status (SES),41 so this study adopted the same practice. The question in the survey was: “What is your highest level of education?” 1. Primary school and below 2. Junior High School 3. High school/Secondary vocational school/Technical school 4. Associate degree 5. Bachelor’s degree 6. Master’s degree 7. Doctoral degree.
Control Variables
Following the practices in past research,16 several demographic variables were set as control variables. The individual characteristic control variables are as follows:1. Gender (Males were coded as 1, females as 0). 2. Age. 3. Place of residence (Urban was coded as 1, rural was coded as 0). 4. Personal monthly income (No income/2000 yuan and below/2001-5000 yuan/5001-10,000 yuan/10,001–20,000 yuan/Over 20,000 yuan).
Statistical Analysis
The study used IBM SPSS Statistics (v27) for statistical analysis. A total of 720 valid samples were used for data analysis. Before analysis, we checked for outliers and multicollinearity and re-coded and standardized variables to fit the research design. Cronbach’s alpha was used to assess the internal consistency and reliability of the redesigned tool. The respondents’ demographic profiles and the core variables’ overview were reported using frequencies, percentages, and averages. Hierarchical regression analysis was employed to assess the predictors of monkeypox knowledge and the knowledge gap related to monkeypox. The monkeypox knowledge gap was visualized using simple slope plots and the Johnson-Neyman technique. P-values are two-tailed, with values < 0.05 considered statistically significant.
Results
Demographic Characteristics of Samples
This study recruited 720 participants, with an average age of 35. Among them, 57.2% of the participants were female, and 84.4% resided in urban areas. Regarding educational background, 50.3% of the participants held a bachelor’s degree. Professionally, 18.1% of the participants were students, while 16.9% were corporate employees. Economically, 34.2% of the participants had a personal monthly income ranging from 5001 to 10,000 RMB, and 31.4% had a monthly income between 2001 and 5000 RMB. Detailed demographic characteristics can be seen in Table 1.
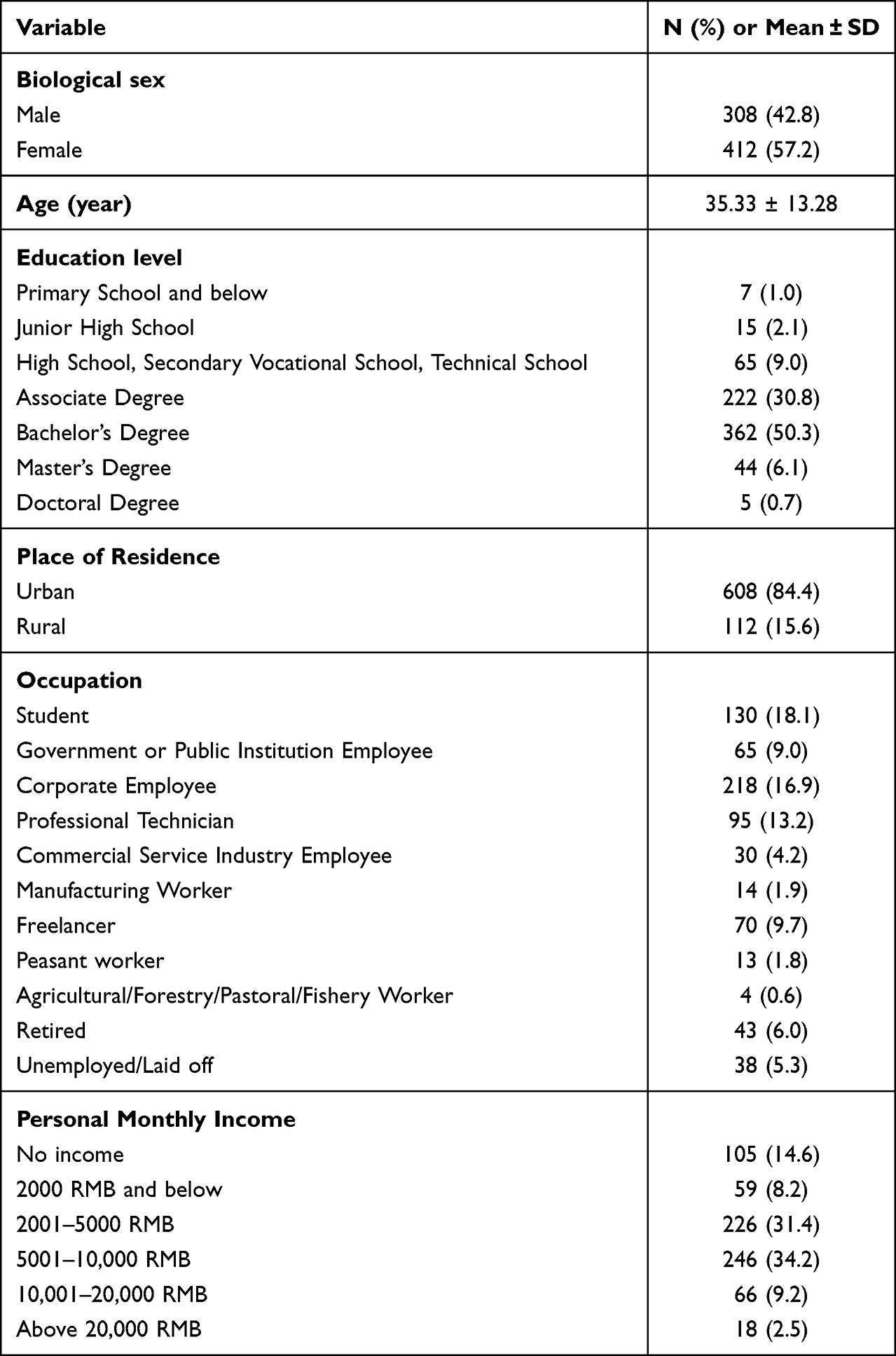 |
Table 1 Demographic Characteristics of the Participants |
Descriptive Analysis Results
Table 2 lists the public’s response selection rates and accuracy rates. The answer options are divided into three categories: “True”, “False”, and “Do not Know”. The correct answer options are marked with an asterisk (*). The mean and median scores of the participants’ knowledge about monkeypox are 10.07 and 11, respectively. Among all participants, using 80% and 70% of the knowledge domain as evaluation standards, 3.61% and 9.72% of people have good knowledge, respectively (as shown in Figure 1). Specifically, in the subdivided knowledge categories, the public has the highest understanding of the transmission mode, with an accuracy rate of 63.75%. The understanding of monkeypox prevention comes next, with a rate of 59.65%. However, the understanding of basic knowledge about monkeypox is the lowest, with only a 35.35% accuracy rate. Regarding sources of monkeypox information (Table 3), social media is the most common source of information, followed by online news and official health websites. Television and print media follow. Interpersonal communication is the least common source for obtaining monkeypox information. Overall, the perceived salience of information and perceived fear are relatively high.
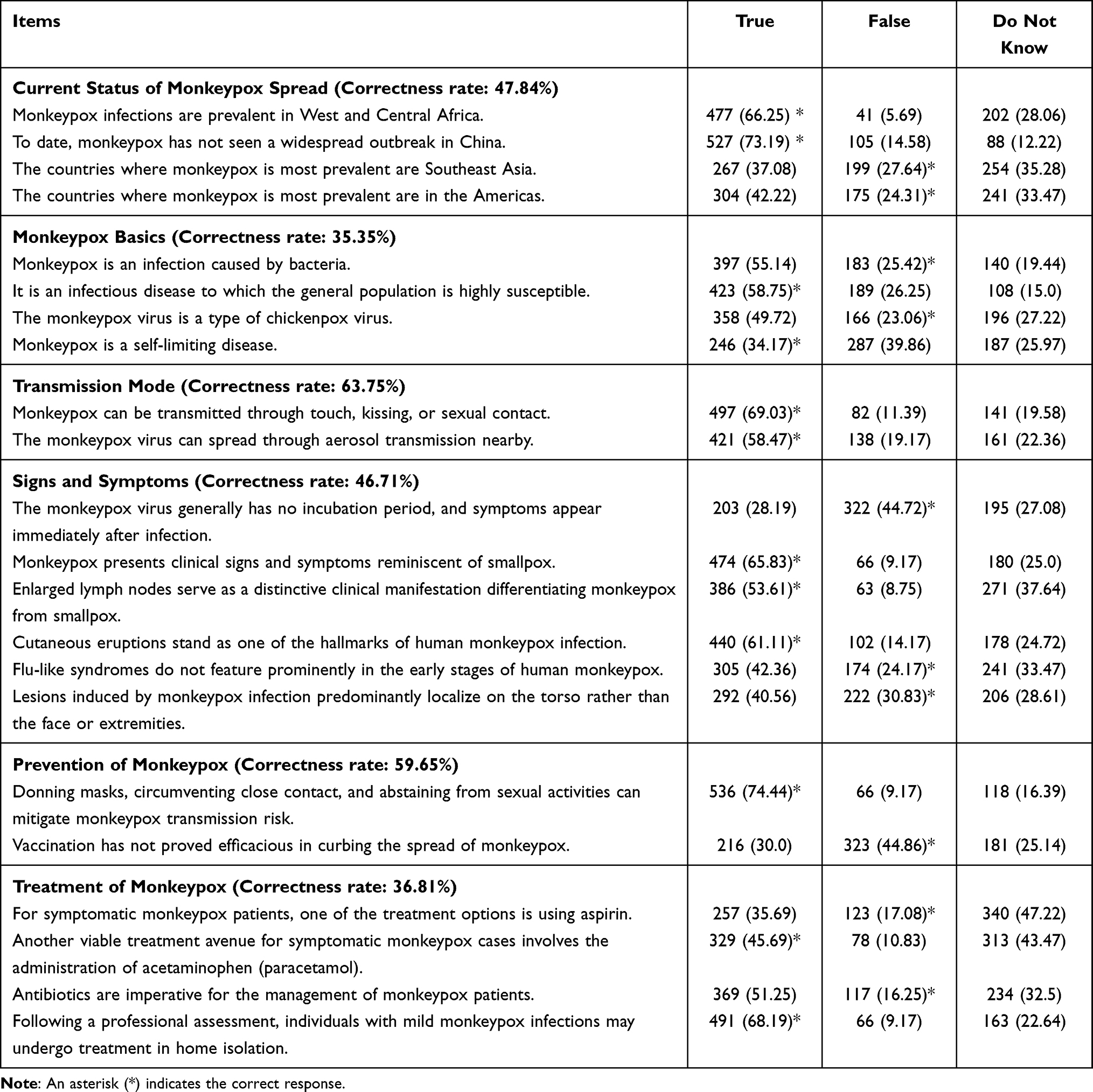 |
Table 2 Participants’ Selection Rates for Different Options and Accuracy Rates for Various Knowledge Categories |
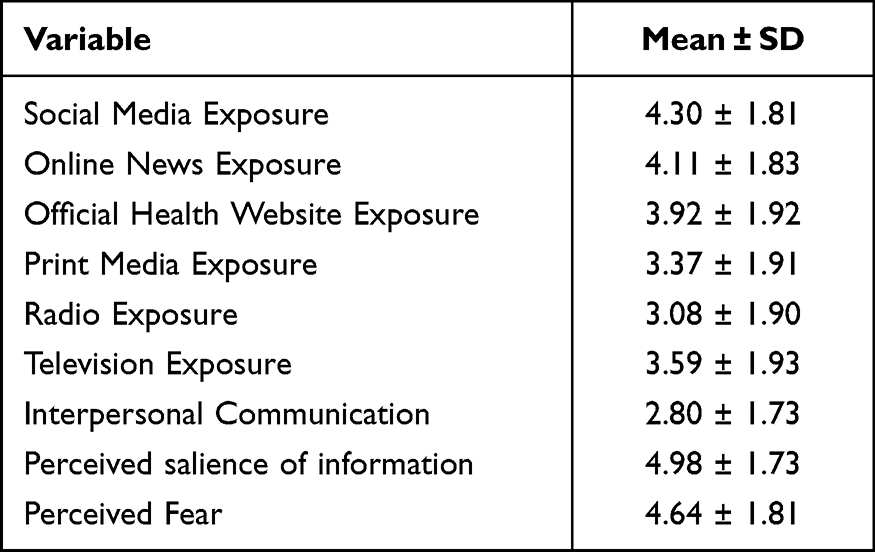 |
Table 3 Mean and Standard Deviation of Core Variables |
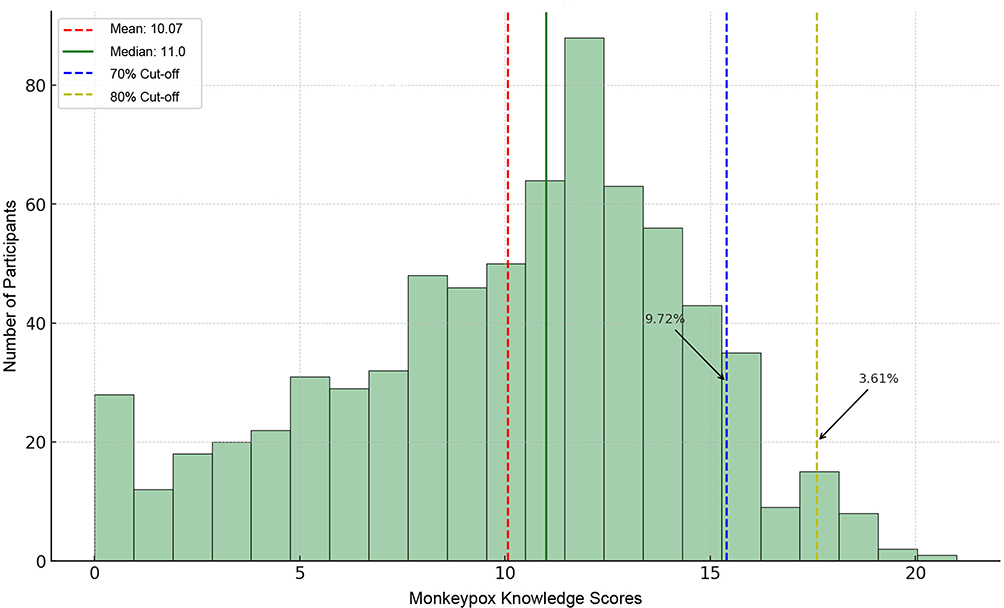 |
Figure 1 Participants’ mastery level of monkeypox knowledge. |
Hierarchical Regression Analysis
The results of the hierarchical regression analysis are shown in Table 4. Research Hypothesis 1 received full support, while Research Hypotheses 2 and 3 received partial support. Specifically, the first level consists of control variables, and the second level comprises predictor variables. Upon the inclusion of predictor variables based on Model 1, the change in F value displayed significance (p < 0.05), suggesting that the inclusion of predictor variables contributes explanatory value to the model. Additionally, the R-squared value increased from 0.022 to 0.244, implying that the predictor variables can account for 22.2% of the variance in knowledge scores. Among them, educational level (B = 0.613, p < 0.01), perceived salience of information (B = 0.326, p < 0.01), interpersonal communication (B = 0.291, p < 0.05), social media exposure (B = 0.303, p < 0.05), and official health websites exposure (B = 0.354, p < 0.05) have a significant positive relationship with monkeypox knowledge scores. Conversely, perceived fear, online news websites exposure, print media exposure, radio exposure, and television exposure do not significantly impact monkeypox knowledge scores (p > 0.05).
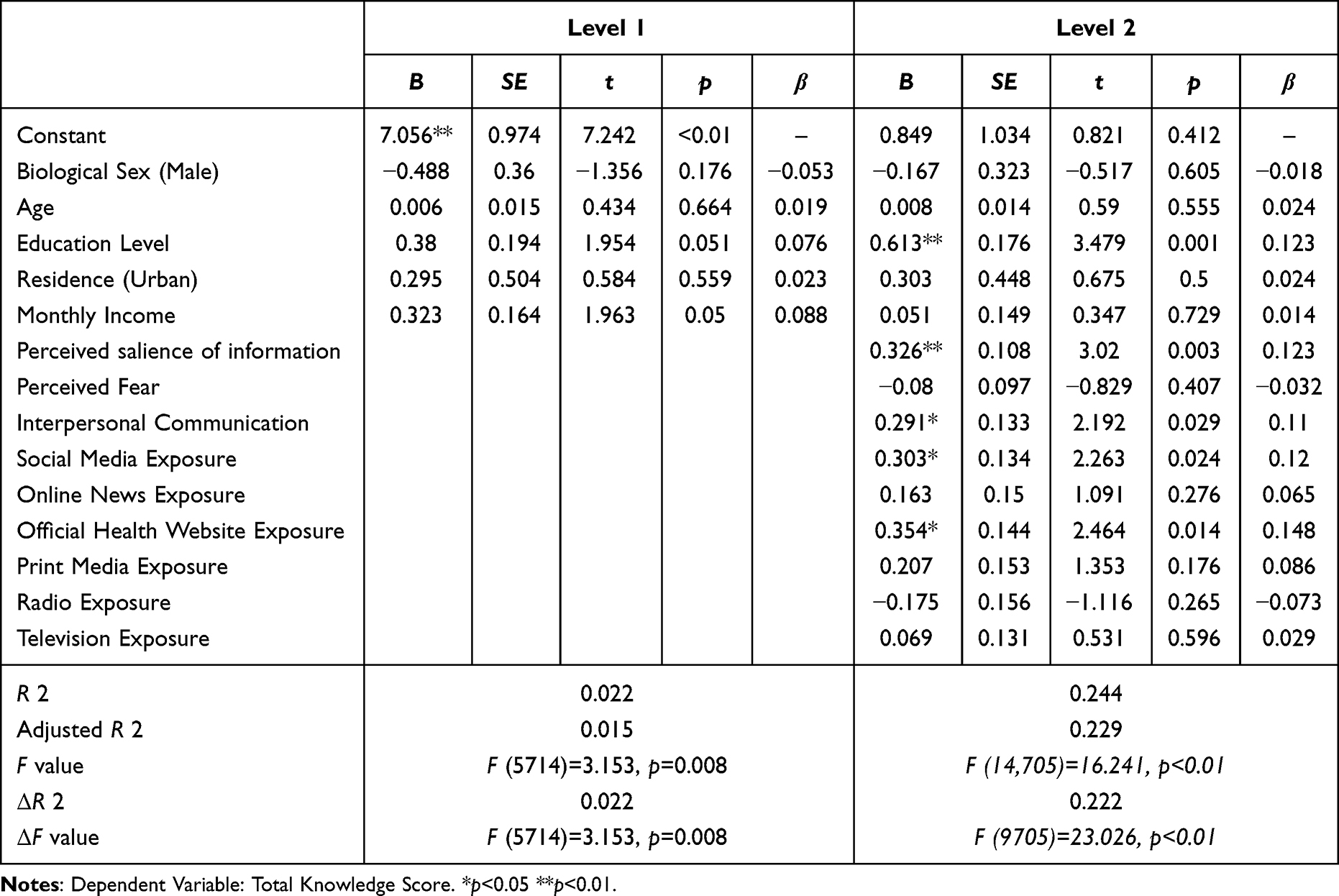 |
Table 4 Results of Hierarchical Regression Analysis |
Interaction Effect Test
The monkeypox knowledge gap was examined using a hierarchical regression model. Firstly, gender, age, personal monthly income, residence, and predictor variables were entered as control variables in Group 1. Next, the level of education was introduced to Group 2. Lastly, interaction terms (the product of predictor variables and level of education) were input into Group 3. The regression analysis results with the interaction variable indicated a significant interaction effect between the education level and social media exposure. No interaction effects were observed between other media exposure variables and the level of education. Thus, only these results from the hierarchical regression analysis are presented (Table 5). Hypothesis 4 received partial support. Social media exposure can significantly predict the monkeypox knowledge gap between different educational level groups.
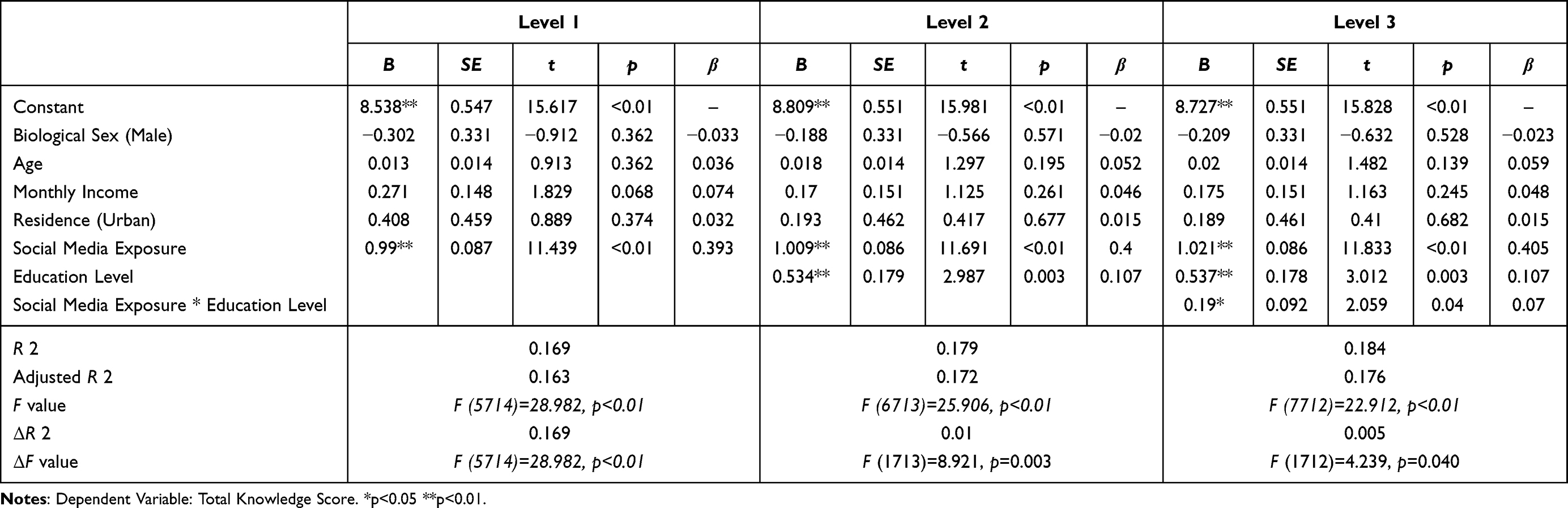 |
Table 5 Moderation Effect Analysis Results (n=720) |
Figure 2 further reveals the interaction model between social media exposure and the level of education. An increase in exposure to social media further widens the knowledge gap between groups with high educational qualifications and those with lower educational qualifications. In other words, the more exposure to monkeypox information on social media, the more significant the knowledge gap about monkeypox between the high-education and low-education groups (β = 0.07, p < 0.05).
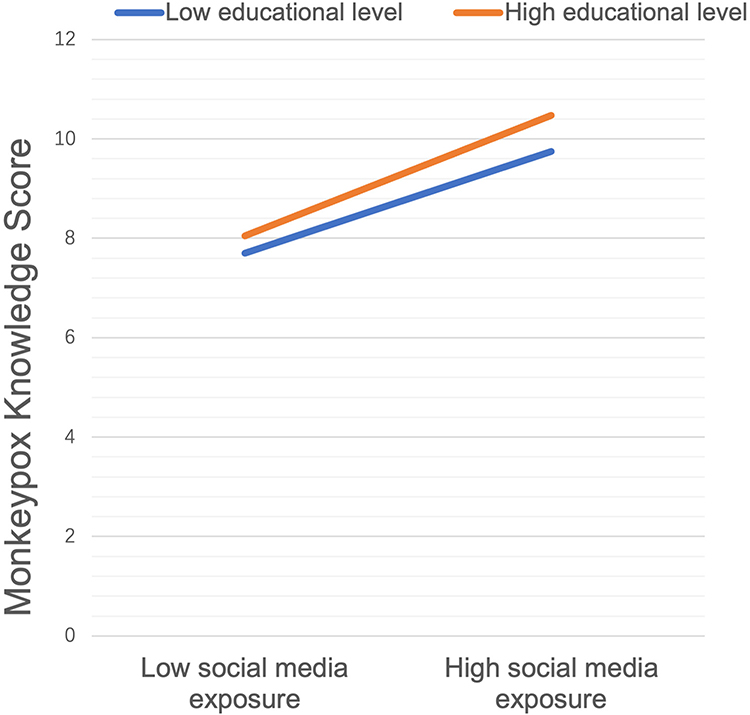 |
Figure 2 Simple slope plot illustrating the interaction effect between social media exposure and education level. |
Additional Exploratory Interaction Effect Analyses
We further probed the interaction effects using the interactions R package by employing the Johnson–Neyman technique. The results show (see Figure 3) that social media exposure significantly impacts the overall monkeypox knowledge score among groups with a junior high school education and above. Although this effect was observed in groups close to the junior high school education level, for most groups with an education level below junior high school, this effect was not significant.
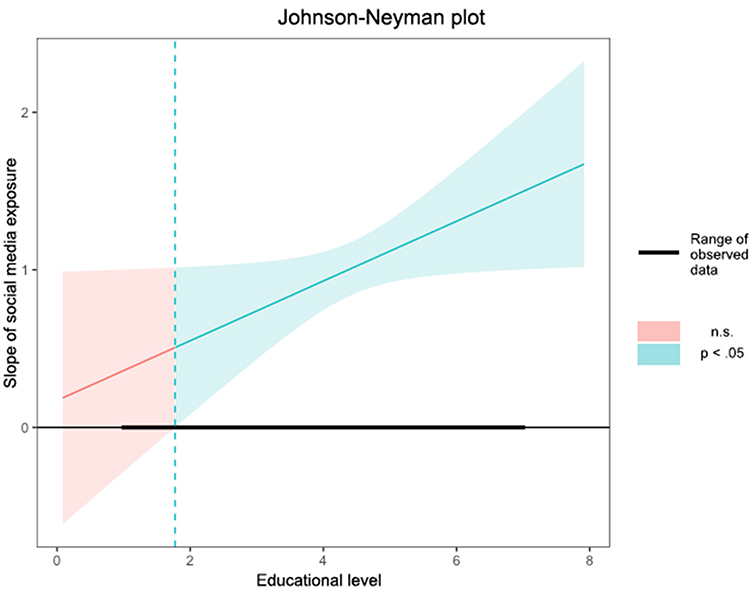 |
Figure 3 Johnson-Neyman plot illustrating the interaction effect between social media exposure and educational level. |
Discussion
This study builds on the optimization of the monkeypox knowledge measurement instrument and assesses monkeypox knowledge among the Chinese public, including predictive factors and knowledge gaps. Our findings reveal three significant insights. Firstly, most participants showed insufficient knowledge about monkeypox, with varied understanding across different knowledge categories. Secondly, educational level, perceived salience of information, interpersonal communication, social media exposure, and official health websites exposure significantly influenced monkeypox knowledge scores. Notably, social media exposure widened the knowledge gap among different educational groups, with a more pronounced positive effect on those educated to junior high school level or higher.
From the perspective of the Chinese public’s understanding of monkeypox, our study found that most respondents have insufficient knowledge about monkeypox infections, in line with findings from a survey in the Philippines.8 This result supports the perspective that rarity affects knowledge. This limited understanding is likely influenced by the disease’s rarity in China, which is not a hotspot for human monkeypox epidemics.42 Consequently, public awareness of monkeypox is somewhat limited. This study optimized the monkeypox knowledge survey questionnaire, focusing on sources of knowledge, knowledge categories, and response options, to uncover public “blind spots” in monkeypox knowledge. We discovered that participants are relatively more informed about the transmission mode and prevention methods of monkeypox, but less so about its basic knowledge and treatment. On one hand, this trend might be attributed to media agenda-setting, which often highlights the spread of a disease and its prevention, while basic knowledge and treatment details are less frequently reported.43,44 On the other hand, as emphasized by Goodall and Reed,45 when people face uncertainty, those exposed to higher levels of threat uncertainty are more likely to seek additional information about that threat. Consequently, as transmission channels and prevention information for monkeypox are perceived as urgently relevant and universally applicable, the public shows a greater interest in practical information on avoiding monkeypox infection. Overall, these findings highlight the public’s information needs and how media influence shapes understanding and response to health threats.
The second significant finding of our research is that the level of education, perceived salience of information, interpersonal communication, social media exposure, and official health website exposure are substantial predictors of the total score of monkeypox knowledge. Conversely, perceived fear, exposure to online news websites, print media, radio, and television do not significantly impact the total knowledge score. This underscores the complex ways in which the public acquires knowledge about monkeypox and offers key insights for public health communication strategies. Firstly, consistent with existing research,46 the level of education, a classic predictor of health knowledge, plays a significant role. Education enhances cognitive and information processing abilities, thus facilitating better understanding of complex health information.47 Consequently, individuals with higher education levels are likely to possess a deeper comprehension of monkeypox. Secondly, the study’s findings highlight the central role of interpersonal communication, social media, and official health organization websites in disseminating monkeypox knowledge. In contrast, traditional media seems to have a less significant role in this context. Interpersonal communication is particularly effective in health promotion, as information can be customized to the recipient’s needs.48 In addition, social media’s growing importance in public health information dissemination is evident.49 Official health websites, recognized as key predictors in our study, play a vital role due to their authoritative nature. However, it is suggested that their impact might be overestimated due to the higher reading level they require, potentially aligning them more with audiences possessing higher education levels.50 Furthermore, our results indicate that traditional media exposure does not significantly predict monkeypox knowledge, which may be due to the representative sample of our study. The effectiveness of traditional media in communicating knowledge might still be significant for specific groups, like the middle-aged and older populations. Therefore, in devising public health communication strategies, it’s essential to consider the diverse media preferences of different demographic groups. Third, from a psychological perspective, the results support that response efficacy better predicts change intention than fear emotion.51 When people perceive information as highly significant, they will be more motivated to protect themselves, increasing their understanding of monkeypox. However, if they are merely fearful, this fear might not increase their knowledge about monkeypox. In conclusion, understanding these predictors of monkeypox knowledge and incorporating them into public health communication strategies is paramount for health professionals and decision-makers.
The third significant finding of this study is that exposure to social media widens the knowledge gap between different educational groups. Specifically, the positive effect of social media exposure on the total score of monkeypox knowledge is mainly applicable to groups with a junior high school education or above. This effect is insignificant for most of those with an education level below junior high school. This finding aligns with existing research results, suggesting that new media exposure widens the knowledge gap.52 It highlights a critical societal issue: the development of information technology has not democratized knowledge but may be exacerbating societal stratification based on education and economic backgrounds. The study delves deeper into the reasons behind this and finds that the digital divide is related to people’s habits and abilities in using the internet. Those with higher education are better at actively seeking information online, emphasizing online media’s informative and instrumental use. In contrast, those with a lower educational background mostly see the internet as a relaxation tool, with their usage habits primarily focusing on its entertainment functions.53 Moreover, when faced with a vast amount of information on the internet, including misleading or false information, the more educated groups often demonstrate higher electronic health literacy (eHealth literacy).54 It implies they can find, discover, understand, and evaluate health information and apply the acquired knowledge to address or solve health issues.55 As a result, differences in media usage habits and eHealth literacy skills affect the amount and quality of information that both groups obtain and understand from the media, further widening the knowledge gap. In general, although social media serves as a primary source of information in the digital age, offering convenient opportunities for information sharing and access, it still needs to promote equitable knowledge dissemination from a fairness perspective. Therefore, public health organizations and related entities must recognize that education is a means of acquiring knowledge and a crucial factor in shaping how individuals interact with the world and understand information. Simply disseminating information is not enough; there needs to be a focus on ensuring that more people can access, understand, and effectively use this information. It might mean offering more media literacy training for those with lower educational levels, helping them develop more robust information filtering and assessment skills, and ensuring that even the less educated can benefit from the digital information era.
Conclusion
Most participants have insufficient knowledge about monkeypox, and there are discrepancies in their understanding across different categories of knowledge. Factors such as educational level, perceived salience of information, interpersonal communication, social media exposure, and official health website exposure have a significant positive relationship with the overall score of monkeypox knowledge. In contrast, perceived fear, online news website exposure, print media exposure, radio exposure, and television exposure do not influence the overall score of monkeypox knowledge. Social media exposure widens the knowledge gap between different educational groups. Notably, the positive effect of social media exposure on the overall monkeypox knowledge score mainly applies to those with a junior high school education or higher. This effect is insignificant for most of those with an education below junior high school. These findings provide critical insights for promoting the dissemination of monkeypox knowledge and bridging the knowledge gap. To effectively curb the further spread of the epidemic, it is crucial to use various information dissemination channels for targeted promotion and education. All parties need to work together to ensure that the public can access, understand, and apply knowledge related to monkeypox.
Abbreviations
WHO, World Health Organization; Mpox, Monkeypox; CDC, Centers for Disease Control and Prevention.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; they took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Fahrni ML, Sharma P, Sharma A, Choudhary OP. Monkeypox: prioritizing public health through early intervention and treatment. Int J Surg. 2022;104:106774. doi:10.1016/j.ijsu.2022.106774
2. World Health Organization. Mpox (monkeypox). Available form: https://www.who.int/news-room/fact-sheets/detail/monkeypox.
3. Dhawan M, Choudhary OP. Emergence of monkeypox: risk assessment and containment measures. Travel Med Infect Dis. 2022;49:102392. doi:10.1016/j.tmaid.2022.102392
4. World Health Organization. Second meeting of the International Health Regulations (2005) (IHR) Emergency Committee regarding the multi-country outbreak of monkeypox. Available form: https://www.who.int/news/item/23-07-2022-second-meeting-of-the-international-health-regulations-(2005)-(ihr)-emergency-committee-regarding-the-multi-country-outbreak-of-monkeypox.
5. U.S. Centers for Disease Control and Prevention. 2022-2023 Outbreak Cases and Data. Available form: https://www.cdc.gov/poxvirus/mpox/response/2022/index.html.
6. Chinese Centre for Disease Control and Prevention. Surveillance of monkeypox outbreak in July 2023. Available form: https://www.chinacdc.cn/jkzt/crb/qt/szkb_13037/gwjszl_13092/202308/t20230809_268502.html.
7. Saied AA, Metwally AA, Choudhary OP. Monkeypox: an extra burden on global health. Int J Surg. 2022;104:106745. doi:10.1016/j.ijsu.2022.106745
8. Berdida DJE. Population‐based survey of human monkeypox disease knowledge in the Philippines: an online cross‐sectional study. J Adv Nurs. 2023;79(7):2684–2694. doi:10.1111/jan.15635
9. Al-Shaikh GK, Syed SB, Fayed AA, et al. Effectiveness of health education programme: level of knowledge about prevention of cervical cancer among Saudi female healthcare students. J Pak Med Assoc. 2017;67(4):513–520.
10. Anderson JE, Kann L, Holtzman D, Arday S, Truman B, Kolbe L. HIV/AIDS knowledge and sexual behavior among high school students. Fam Plann Perspect. 1990;22(6):252–255. doi:10.2307/2135681
11. Abu-Rish EY, Elayeh ER, Mousa LA, Butanji YK, Albsoul-Younes AM. Knowledge, awareness and practices towards seasonal influenza and its vaccine: implications for future vaccination campaigns in Jordan. Fam Pract. 2016;33(6):690–697. doi:10.1093/fampra/cmw086
12. Manabe T, Hanh TT, Lam DM, et al. Knowledge, attitudes, practices and emotional reactions among residents of avian influenza (H5N1) hit communities in Vietnam. PLoS One. 2012. doi:10.1371/journal.pone.0047560
13. Bruns DP, Kraguljac NV, Bruns TR. COVID-19: facts, cultural considerations, and risk of stigmatization. J Transcult Nurs. 2020;31(4):326–332. doi:10.1177/1043659620917724
14. Trevethan R. Deconstructing and assessing knowledge and awareness in public health research. Front Public Health. 2017;5:194. doi:10.3389/fpubh.2017.00194
15. Balkhy HH, Abolfotouh MA, Al-Hathlool RH, Al-Jumah MA. Awareness, attitudes, and practices related to the swine influenza pandemic among the Saudi public. BMC Infect Dis. 2010;10(1):1–7. doi:10.1186/1471-2334-10-42
16. Wang H, Li L, Wu J, et al. Factors influencing COVID-19 knowledge-gap: a cross-sectional study in China. BMC Public Health. 2021;21:1826. doi:10.1186/s12889-021-11856-9
17. Harapan H, Setiawan AM, Yufika A, et al. Knowledge of human monkeypox viral infection among general practitioners: a cross-sectional study in Indonesia. Pathog Glob Health. 2020;114(2):68–75. doi:10.1080/20477724.2020.1743037
18. Jairoun AA, Al-Hemyari SS, Abdulla NM, et al. Awareness and preparedness of human monkeypox outbreak among university students: time to worry or one to ignore? J Infect Public Health. 2022;15(10):1065–1071. doi:10.1016/j.jiph.2022.08.015
19. Chen L, Hong J, Xiong D, et al. Are parents’ education levels associated with either their oral health knowledge or their children’s oral health behaviors? A survey of 8446 families in Wuhan. BMC Oral Health. 2020;20:1–12. doi:10.1186/s12903-020-01186-4
20. Viswanath K, Ramanadhan SR, Kontos EZ, Galea S. Macrosocial determinants of population health. In: Mass Media and Population Health: A Macrosocial View. Springer; 2007:275–294.
21. Bala MM, Strzeszynski L, Topor‐Madry R. Mass media interventions for smoking cessation in adults. Cochrane Database Syst Rev. 2017. doi:10.1002/14651858.CD004704.pub4
22. Lecouturier J, Rodgers H, Murtagh MJ, White M, Ford GA, Thomson RG. Systematic review of mass media interventions designed to improve public recognition of stroke symptoms, emergency response and early treatment. BMC Public Health. 2010;10:1–10. doi:10.1186/1471-2458-10-784
23. Medlock S, Eslami S, Askari M, et al. Health information–seeking behavior of seniors who use the internet: a survey. J Med Internet Res. 2015;17(1):e10. doi:10.2196/jmir.3749
24. Taha J, Sharit J, Czaja S. Use of and satisfaction with sources of health information among older Internet users and nonusers. Gerontologist. 2009;49(5):663–673. doi:10.1093/geront/gnp058
25. Seo M, Matsaganis MD. How interpersonal communication mediates the relationship of multichannel communication connections to health-enhancing and health-threatening behaviors. J Health Commun. 2013;18(8):1002–1020. doi:10.1080/10810730.2013.768726
26. Ezeah G, Ogechi EO, Ohia NC, Celestine GV. Measuring the effect of interpersonal communication on awareness and knowledge of COVID-19 among rural communities in Eastern Nigeria. Health Educ Res. 2020;35(5):481–489. doi:10.1093/her/cyaa033
27. Tannenbaum MB, Hepler J, Zimmerman RS, et al. Appealing to fear: a meta-analysis of fear appeal effectiveness and theories. Psychol Bull. 2015;141(6):1178–1204. doi:10.1037/a0039729
28. Griffin RJ, Dunwoody S, Neuwirth K. Proposed model of the relationship of risk information seeking and processing to the development of preventive behaviors. Environ Res. 1999;80(2):S230–S245. doi:10.1006/enrs.1998.3940
29. Tichenor PJ, Donohue GA, Olien CN. Mass media flow and differential growth in knowledge. Public Opin Q. 1970;34(2):159–170. doi:10.1086/267786
30. Bao H, Lee EW. Knowledge Gap Hypothesis. Int Encycl Health Commun. 2023;1–6.
31. Braveman PA, Kumanyika S, Fielding J, et al. Health disparities and health equity: the issue is justice. Am J Public Health. 2011;101(Suppl 1):S149–S155. doi:10.2105/AJPH.2010.300062
32. Bekalu MA, Eggermont S. Media use and HIV/AIDS knowledge: a knowledge gap perspective. Health Promot Int. 2014;29(4):739–750. doi:10.1093/heapro/dat030
33. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296.
34. Wang JL. Clinical Epidemiology-Design, Measurement, and Evaluation of Clinical Scientific Research.
35. Choudhary OP, Fahrni ML, Saied AA, Chopra H. Ring vaccination for monkeypox containment: strategic implementation and challenges–Correspondence. Int J Surg. 2022. doi:10.1016/j.ijsu.2022.106873
36. Choudhary OP, Chopra H, Shafaati M, et al. Reverse zoonosis and its relevance to the monkeypox outbreak 2022. New Microbes New Infect. 2022:49. doi:10.1016/j.nmni.2022.101049
37. Chopra H, Choudhary OP. mRNA vaccines as an armor to combat infectious diseases. Travel Med Infect Dis. 2023;52:102550. doi:10.1016/j.tmaid.2023.102550
38. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. Lippincott Williams & Wilkins; 2008.
39. Taber KS. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res Sci Educ. 2018;48(6):1273–1296. doi:10.1007/s11165-016-9602-2
40. Melki J, Tamim H, Hadid D, et al. Media exposure and health behavior during pandemics: the mediating effect of perceived knowledge and fear on compliance with COVID-19 prevention measures. Health Commun. 2022;37(5):586–596. doi:10.1080/10410236.2020.1858564
41. Gaziano C. Forecast 2000: widening knowledge gaps. J Mass Commun Q. 1997;74(2):237–264. doi:10.1177/107769909707400202
42. Brown K, Leggat PA. Human monkeypox: current state of knowledge and implications for the future. Trop Med Infect Dis. 2016;1(1):8. doi:10.3390/tropicalmed1010008
43. McCombs ME, Shaw DL. The agenda-setting function of mass media. Public Opin Q. 1972;36(2):176–187. doi:10.1086/267990
44. Gupta M, Keshri VR, Konwar P, Cox KL, Jagnoor AJ. Media coverage of COVID-19 health information in India: a content analysis. Health Promot Int. 2022;37(2):daab116. doi:10.1093/heapro/daab116
45. Goodall CE, Reed P. Threat and efficacy uncertainty in news coverage about bed bugs as unique predictors of information seeking and avoidance: an extension of the EPPM. Health Commun. 2013;28(1):63–71. doi:10.1080/10410236.2012.689096
46. Gabriella C, James H, Sergio U. The education-health gradient. Am Econ Rev. 2010;100(2):234–238.
47. Eveland WP, Scheufele DA. Connecting news media use with gaps in knowledge and participation. Polit Commun. 2000;17(3):215–237. doi:10.1080/105846000414250
48. Storey D, Lee K. Achieving Lasting Impact at Scale: Social and Behavior Change and the Spread of Family Health Interventions in Low Income Countries. Report for The Bill & Melinda Gates Foundation; 2011.
49. Merchant RM. Evaluating the potential role of social media in preventive health care. JAMA. 2020;323(5):411–412. doi:10.1001/jama.2019.21084
50. Seitz CM, Shiplo S, Filippini T, Kabir Z, Lennon JL, Fowler D. The reading level of government and voluntary health organization smoking cessation websites: a descriptive analysis. Am J Health Educ. 2017;48(6):392–399. doi:10.1080/19325037.2017.1358122
51. Floyd DL, Prentice‐Dunn S, Rogers RW. A meta‐analysis of research on protection motivation theory. J Appl Soc Psychol. 2000;30(2):407–429. doi:10.1111/j.1559-1816.2000.tb02323.x
52. Gibson RK, McAllister I. New media, elections and the political knowledge gap in Australia. J Sociol. 2015;51(2):337–353. doi:10.1177/1440783314532173
53. Bonfadelli H. The Internet and knowledge gaps: a theoretical and empirical investigation. Eur J Commun. 2002;17(1):65–84. doi:10.1177/0267323102017001607
54. Lee J, Tak SH. Factors associated with eHealth literacy focusing on digital literacy components: a cross-sectional study of middle-aged adults in South Korea. Digital Health. 2022;8:20552076221102765. doi:10.1177/20552076221102765
55. Norman CD, Skinner HA. eHealth literacy: essential skills for consumer health in a networked world. J Med Internet Res. 2006;8(2):e9. doi:10.2196/jmir.8.2.e9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.