Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Monitoring And Managing Depression In Adolescents With Epilepsy: Current Perspectives
Authors Coppola G ![]() , Operto FF, Matricardi S, Verrotti A
, Operto FF, Matricardi S, Verrotti A
Received 9 June 2019
Accepted for publication 2 September 2019
Published 24 September 2019 Volume 2019:15 Pages 2773—2780
DOI https://doi.org/10.2147/NDT.S192714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Giangennaro Coppola,1 Francesca Felicia Operto,1 Sara Matricardi,2 Alberto Verrotti3
1Child and Adolescent Neuropsychiatry, Department of Medicine, Surgery, and Odontoiatry, University of Salerno, Salerno, Italy; 2Department of Pediatric Neurology, Ospedali Riuniti, Ancona, Italy; 3Department of Pediatrics, University of L’Aquila, L’Aquila, Italy
Correspondence: Giangennaro Coppola
Child and Adolescent Neuropsychiatry, Department of Medicine, Surgery and Odontoiatry, University of Salerno, Largo d’Ippocrate, 1, Salerno 84100, Italy
Tel/Fax +39 089672578
Email [email protected]
Abstract: Epilepsy is associated with a significantly increased risk of developing depressive disorder during adolescence. On the other hand, depression is highly detected in adolescents with epilepsy. These findings highlight the importance of early identification and proper management of comorbid depression in adolescent age. The prevalence of depressive disorders in adolescents with epilepsy ranges between 8 and 35% and is higher than the general population of the same age. The relationship between epilepsy and depression is complex and potentially bidirectional, thereby suggesting a common underlying pathophysiology. Furthermore, failure to detect and treat depressive disorder mostly in adolescence could lead to several negative implications such as an increased risk of suicidal ideation or behavior and poor quality of life. A number of methods are available to detect depressive disorder, such as psychiatric or psychological assessments, structured or semi-structured interviews, and self-report screening tools. Thus, physicians should be able to regularly screen depressive symptoms in youths with epilepsy. Recently, the NDDI-E-.Y inventory has been developed from the adult NDDI-E, and has been validated in many countries. NDDI-E-Y has showed reliable validity, being a brief screening tool (12 items) that can be easily included in routine epilepsy care. The first step to be considered for the management of depressive disorder in adolescents with epilepsy is to consider potential reversible causes of anxiety and depression (i.e., a new AEDs; seizure control). Secondly, great attention has to be given to the education of the child/adolescent and his/her family, trying to improve knowledge about epilepsy as well as to decrease parental stress and improving the child’s sense of competence. Pharmacological treatment should also be considered in adolescents diagnosed with depression.
Keywords: depression, adolescents, monitoring, management, epilepsy
Introduction
Epilepsy is associated with a significantly increased risk of developing depressive disorder during adolescence. On the other hand, depression is highly detected in adolescents with epilepsy. These findings highlight the importance of early identification and proper management of comorbid depression in adolescent age. Depressive disorders are the most frequent psychiatric disturbances associated with epilepsy in adolescents and include a broad and heterogeneous spectrum of conditions that share hallmark features and symptoms such as sadness, irritability, decreased motivation or interests, fatigue, withdrawal, hopelessness, anhedonia, changes in appetite and weight, and sleep disturbances that are persistent and pervasive most days for at least 2 weeks. The chapter describing Depressive disorders in Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)1 comprises disruptive mood dysregulation disorder, major depressive disorder (including major depressive episode), and persistent depressive disorder (dysthymia). In adolescents, other possible symptoms include psychomotor agitation, regressive behaviors (eg separation anxiety), vegetative and somatic symptoms (eg, stomachaches, lethargy), difficulty in thinking, concentrating or making decisions, recurrent thoughts of death or suicidal ideation, plans or attempts, and an increased risk of substance abuse. The severity of depression must be specified and defined as mild, moderate, or severe, according to the number of key symptoms, their severity, and the degree of functional impairment. Other specifiers for depressive disorders must be assessed and detected to improve tailored management. The most frequent associated specifiers that could occur in adolescents are anxiety symptoms, psychotic features, and manic/hypomanic symptoms. About the latter, the manic/hypomanic specifier in DSM-5 allows us to code major depressive disorder without also diagnosing bipolar disorder. Likewise, the presence of manic symptoms has been found in the interictal dysphoric disorder (IDD) which is a proposed epilepsy-specific mood disorder characterized by both depressive and manic symptoms in adults.2
It is of paramount importance to carefully detail the presence and severity of these specifiers for management planning and monitoring of treatment response.1 A major depressive episode before the age of 15 years old leads to a 50% increased risk of developing bipolar disorder. This possible evolution into bipolar disorder has important treatment implications. Foremost, antidepressants should be avoided even when they are administered with mood-stabilizers, which do not fully “protect” patients from switching to mania.
Adolescence is a peculiar neurodevelopmental period marked by rapid and profound changes in various domains such as biological, social, and psychological domains. Coping with these rapid changes could be challenging. Also, the developmental trajectories during this period of life are at a higher risk of distortion. The prevalence of depressive disorders in adolescents with epilepsy is higher than the general population at the same age.3–12 In fact, the reported prevalence of depression in adolescents with epilepsy ranges between 8-35% with a broad heterogeneity between estimates. This broad variability could be attributed to different and heterogeneous methods of depression assessment (eg, self-report, questionnaires, clinical assessment, or specific diagnostic scales) and the presence of potential confounders. Population-based studies have revealed a prevalence of lifetime depression in epilepsy of almost 13-20%.4,10,11 Also, the risk of depression in adolescents is higher when epilepsy is also associated with lower cognitive functioning, language disorders and lower scores in specific neuropsychological domains.13,14 Other specific epilepsy related-factors, such as age at seizure onset and seizure type or syndrome, seem to be less involved in the development of depression, even if poor seizure control and seizure relapses could be highly associated with major depressive mood episodes.3 The relationship between epilepsy and depression is complex and potentially bidirectional, thereby suggesting a common underlying pathophysiology between these conditions.15–21 Patients suffering from epilepsy can show depressive disorders due to the uncertainty and unpredictability of seizures, mostly at epilepsy onset and diagnosis or in the case of poor seizure control with antiepileptic drugs (AEDs). Furthermore, numerous other factors related to the epileptic disease could interfere with the development of depressive mood in an adolescent beyond seizure burden and seizure control. These factors include the stigma and the adverse psychosocial impact that epilepsy entails due, for instance, to diminished social relationships with peers and engagements, as well as lower educational programs and poorer academic achievement, the need for supervision in particular circumstances, specific restrictions on activities, and parental overprotection that further limit the acquisition of independence. All these factors linked to epilepsy could affect self-esteem, behavior, and mood dysregulation during adolescence.
On the other hand, depression could increase the development of epileptic activity by several mechanisms of action including the hyperactivity of the hypothalamic-pituitary-adrenal axis and alterations in the balance of release and re-uptake of excitatory and inhibitory neurotransmitters as glutamate and γ-aminobutyric acid. These changes have been found in both epilepsy and depression and could also cause cortical structural alterations, including volume reduction of the hippocampus and frontal lobes.22,23 Furthermore, failure to detect and treat depressive mood mostly in adolescence age could lead to several negative implications such as an increased risk of suicidal ideation or behavior, poor quality of life, poor compliance to AED therapy and, as a consequence, an increased risk of seizure recurrence.24
On the other hand, although a clear causal correlation between mood disorders and psychogenic non-epileptic seizures (PNES) has not been demonstrated, adolescents with PNES, both epileptic and non-epileptic, report high rates of depression, anxiety and somatoform symptoms. In this perspective, particular attention should also be paid to the monitoring of depressive symptoms in this group of patients.25,26
Depression could be under-diagnosed and inadequately treated particularly during adolescence. In adolescents with epilepsy depression could interfere with the overall management and quality of life, leading to poor scholar and social functioning, as well as to increased health care system requirements, poorer seizure control, and increased AED adverse events. Therefore, comorbid depressive disturbances represent a heavier burden of the disease, particularly at this age.
Physicians that are responsible for the management of adolescents with epilepsy should be aware of the increased risk of depressive mood in these patients. Thus, physicians should screen patients regularly with appropriate assessment tools for an early detection of depressive symptoms and targeted treatment.
Monitoring
Numerous methods are available to detect depression or depressive symptoms, such as psychiatric or psychological assessments, structured or semi-structured interviews, and self-report screening tools.27 The use of screening tools can be effective because they are often brief, standardized, and a less resource-intensive means for assessing depressive symptoms. Many depression-screening tools have been developed for the general population, such as the Beck Depression Inventory (BDI),28 the Hospital and Anxiety and Depression Scale (HADS),29 the Child Depression Inventory-2 (CDI-2),30 and the Hamilton Rating Scale for Depression (HRSD),31 and have been validated by using gold and/or reference standards various screening tools such as SCID-I (Structured Clinical Interview for DSM-IV-TR Axis I Disorders)32 or MINI (Mini International Neuropsychiatric Interview).33 However, the only so far validated epilepsy-specific tool is the Neurological Disorders Depression Inventory for Epilepsy (NDDI-E).34 Considering that depression in youths with epilepsy is a common comorbidity that is characterized by poorer psychosocial and healthy-related outcomes and increased risk of suicide, a brief, free measure of specific depressive symptoms in youths with epilepsy would be beneficial. Recently, the NDDI-E-Y inventory has been developed from the adult NDDI-E,35 and has been validated in many countries. NDDI-E-Y has showed reliable and construct validity, being a brief screening tool (12 items) that can be easily included in routine epilepsy care (Table 1).
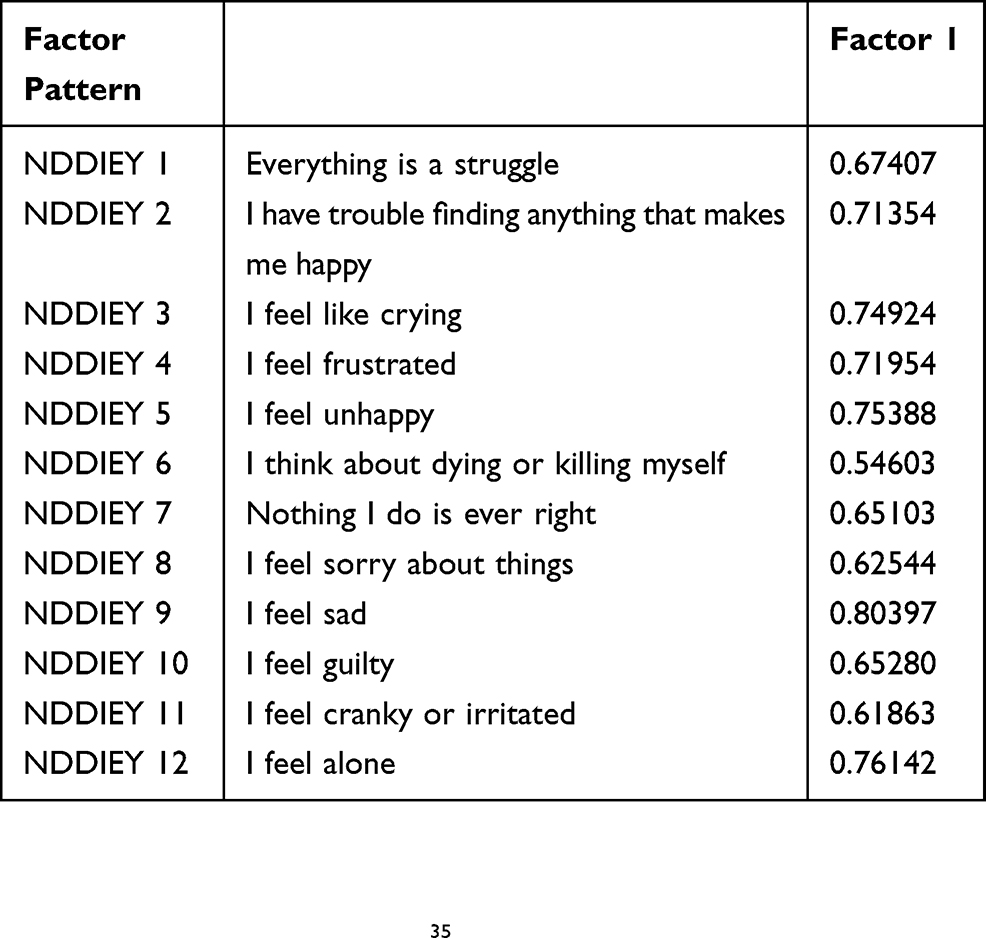 |
Table 1 The 12-Item Revised NDDI-E-Y For Children And Adolescents With Epilepsy, Aged 12–17 Years |
More in detail, the content for the original NDDI-E-Y was developed from the adult NDDI-E, with an input from a panel of experts and as a result of cognitive interviewing with 17 youths. An 11-item NDDI-E-Y was administered to 93 youths. Several revisions were made to the NDDI-E-Y based on preliminary findings. Three new items were added. Given the prevalence of suicidal ideation in youths with epilepsy,36,37 the item “I think about dying” which was dropped following cognitive interviewing due to confusion over the question, (i.e., whether it was referring to death in general or the relevant participant’s death) was revised as “I think about dying or killing myself.” Also the item “I feel cranky or irritated” was added because irritation is a seminal symptom of depression in the general population of youths as indicated by the DSM-5. Finally, the item “I feel alone” was added to represent the domain of interpersonal difficulties or loneliness in depression27,38 and frequent endorsement in youths with epilepsy.39 Indeed, loneliness is not likely to be related to AED adverse effects. These revisions resulted in the 12-item measure that has been validated in the present study. In the aim to establish the reliability and construct validity of the NDDI-E-Y, 143 youths with epilepsy aged 12–17 years were asked to fill in the NDDI-E-Y questionnaires during a routine ambulatory visit at two different Epilepsy Care centers. At one center, adolescents were also asked to complete the 32-items CDI-2, a well-known gold-standard questionnaire for detecting depressive symptoms in children and adolescents.30 In the present study, the NDDIE-Y resulted to be a reliable and valid instrument to screen depressive symptoms in youths with epilepsy. Psychometric properties of the NDDI-E-Y were strong, including internal consistency, sensitivity/specificity, which were similar to the CDI-2. A cut-off score of 32 on the NDDI-E-Y demonstrated high sensitivity and specificity in predicting a clinical score on the CDI-2 (T ≥ 65). Another cross-sectional study40 examined the predictive utility of the Neurological Disorders Depression Inventory-Epilepsy for Youth (NDDI-E-Y) and the Neuro-QOL Depression Short Form (Neuro-QOL SF) in explaining variance in overall depressive symptoms and specific symptom clusters on the gold standard Children’s Depression Inventory-2 (CDI-2). Ninety-nine YWEs (female 68, mean age 14.7 years) during a routine epilepsy visit, completed self-report measures of depressive symptoms, including the NDDI-E-Y, CDI-2, and the Neuro-QOL SF. Concurrently, caregivers completed a measure of seizure severity. All sociodemographic and medical information was evaluated through electronic medical record review. In this study with a sample of youths with chronic treatment-resistant epilepsy (56% have had a seizure in the past year, 57% on polytherapy), 20% of participants reported elevated depressive symptoms on the CDI-2 and 23% of them reported elevated depressive symptoms on the NDDI-E-Y. These results suggest that NDD-E is brief, reliable and sensitive as a depressive screening tool for YWE during routine epilepsy care.
Thus, once adolescents with depressive symptoms have been identified, diagnosis should always be confirmed by a thorough clinical psychometric measure.
Management
The first step to consider for the management of depressive symptoms in adolescent with epilepsy is the potential reversible causes of anxiety and depression (ie. a new AEDs; seizure control). The detection of depressive mood in an adolescent with epilepsy has to be taken into account when prescribing AEDs, and the susceptibility to epileptic seizures has to be carefully considered when selecting drugs to treat depression. An appropriate recognition of depressive symptoms is crucial for planning appropriate treatment. However its management is often challenging. Depression in adolescents with epilepsy is most commonly the expression of an underlying spontaneous inter-ictal condition, but it may also represent peri-ictal symptomatology that occurs in specific relation to seizure timing such as a dysphoric mood that could precede a seizure several hours before and could persist for a few days after. Depression could also result from a para-ictal phenomenon due to forced normalization or may be due to iatrogenic conditions that are triggered by pharmacological or surgical treatment of the epileptic condition. All these different scenarios have to be taken into account before starting any therapeutic regimen.41–43 Many AEDs could have iatrogenic potential and negatively affect mood and behavior in epileptic adolescents. This iatrogenic potential is also due to pharmacodynamic mechanisms and pharmacokinetic interactions with other concurrent treatments in patients receiving polytherapy. Depressive symptoms more likely occur with AEDs with known negative psychotropic actions, including GABAergic drugs as barbiturates, benzodiazepines, vigabatrin, and tiagabine; or with topiramate, levetiracetam, zonisamide, felbamate, and perampanel.42,44,45 An increased risk of depression has been observed when these types of AEDs are administered at a high dose since the beginning of the treatment or titrated rapidly.46 Iatrogenic depressive symptoms usually occur more frequently in specific groups of adolescents: those who have a personal or family history of mood disorders, those who discontinue AEDs with antidepressant properties, or those who are on psychotropic drugs to manage depression and started an enzyme-inducer AED that increases the clearance of the psychotropic drug metabolized in the liver. On the other hand, many AEDs contain known antidepressant and mood-stabilizing properties like valproic acid, carbamazepine, oxcarbazepine, and lamotrigine (Table 2). However, the use of valproic acid, despite its broad spectrum efficacy in epilepsy and its mood-stabilizing and anxiolytic actions, must be limited in female adolescents due to its known iatrogenic effects in women of childbearing age.47 Furthermore, vagus nerve stimulation, a palliative treatment for drug resistant epilepsy, has been proved to have a positive effect on depressive symptoms. On the other hand, epilepsy surgery is often the best therapeutic alternative for treating seizures, but the current evidence concerning its effects on mood is inconclusive: surgery could improve presurgical depressive symptoms or cause a relapse or de novo episodes of depression.42 A recent prospective controlled study on patients with refractory epilepsy showed that epilepsy surgery resulted in an improvement in depressive symptoms after 12 months follow-up compared to a control group.48
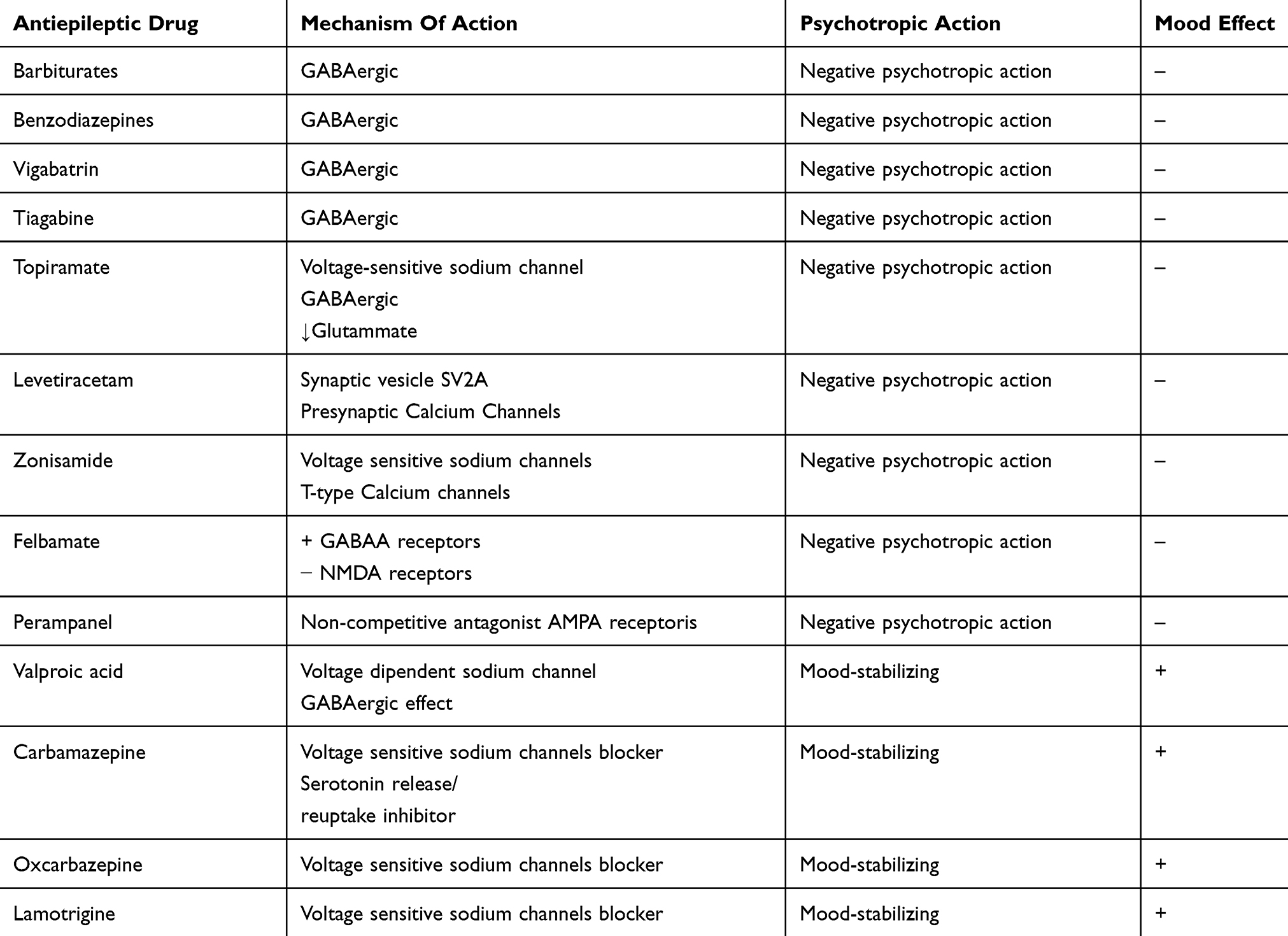 |
Table 2 Psychotropic Proprieties Of Antiepileptic Drugs |
Secondly, great attention has to be given to the education of the child/adolescent and his/her family, with the aim to improve their knowledge about epilepsy and decrease parental stress as well as to improve the child’s sense of competence. Interventions can be distinguished in non-pharmacological and pharmacological (Table 3). The former include psychoeducation, which should be utilized to explain to adolescents and their parents the main features of the epileptic disorder, the side effects of antiepileptic drugs, treatment modalities, as well as to cope with learning and social difficulties, in order to improve the quality of their life. Psychological and psychosocial treatments can help patients to cope with their limited independence, engagement, and relationships due to the epileptic illness. Family therapy is another important key component in the overall treatment; parents should be involved with supportive therapy that addresses negative feelings towards the stigma of epilepsy and reduces their anxiety.30 Furthermore, a better understanding of epilepsy and of the potential benefits and side effects of its treatment could improve the compliance to therapy and the overall outcome. Among the various forms of psychotherapy, cognitive-behavioral therapy (CBT) is an individual therapy targeting cognitive errors such as overgeneralizations, catastrophizing, and selective abstraction. It focuses on the relationships between feelings, thoughts, behaviors, and body sensations. The patient learns self-regulation skills including behavioral activation, self-monitoring, relaxation, problem-solving, and cognitive adaption to improve mood and reduce anxiety. This therapeutic approach has been successfully performed in adolescents with mild or moderate depression, resulting in an improvement of their quality of life, psychosocial well-being, and reduction of depressive symptoms.6,8,49,50 Indeed, CBT has been reported as effective in preventing depression in 30 adolescents51 with depressive symptoms. After a 9-month follow-up, three patients with depression were found in the control group (which was treated with the usual therapy), while no patient was found in the group treated with psychoeducation combined with CBT. Psychopharmacology for depressive disorders should be considered only after a deep assessment of prior and current antiepileptic and/or psychopharmacologic treatment. The elements that have to be considered when deciding on medication versus psychotherapy include the severity of the depression, risk of suicidality, recurrence of depressive symptoms or their chronicity, lack of response to psychotherapy, family preferences, and the presence of psychosocial stressors.
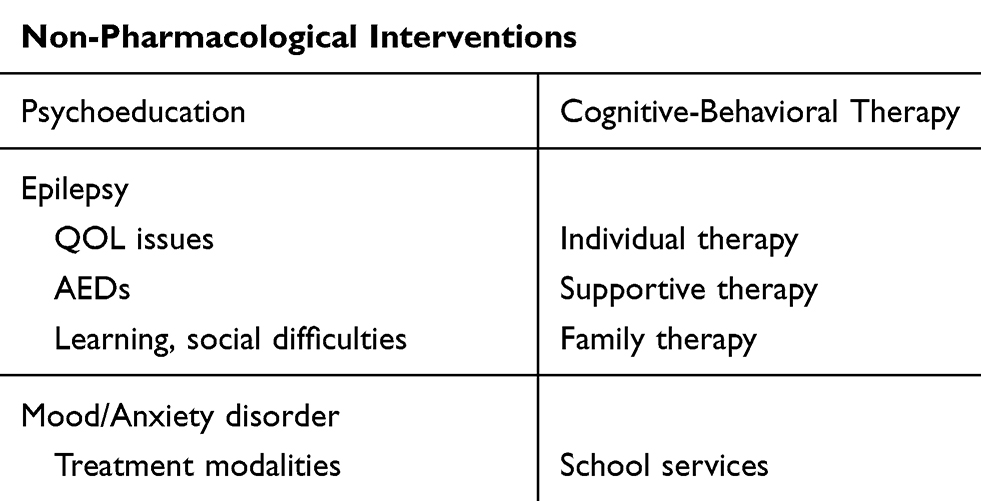 |
Table 3 Non-pharmacological Interventions For Adolescents With Epilepsy And Depressive Symptoms |
In general, pharmacologic treatment should be considered in adolescents with moderate to severe depression.6,8 Prior to start with therapy, a good rule is to optimize AEDs treatment. Since no controlled studies in adolescents with epilepsy and depression are available so far, general guidelines for mood psychopharmacotherapy in adolescents without epilepsy should be applied. Selective serotonin re-uptake inhibitors (SSRIs), such as fluoxetine, fluvoxamine, paroxetine, sertraline, citalopram, and escitalopram are the first-line medications in adolescents with epilepsy and comorbid depression.52 Although fluoxetine for depression in youths without an unsuccessful trial period of psychotherapy is outside of the licensed indications, physicians should consider starting antidepressants and psychotherapy simultaneously with adolescents with moderate to severe depression notably with those with severe depression as an alternative to psychotherapy followed by combined therapy.53 Furthermore, the risk of treatment emergent adverse events should be weighed against the risk that depression is unresponsive to non-pharmacologic interventions. The pharmacotherapy of depression has often a multi-step approach. Treatment planning must ensure an adequate trial of the selected drug with careful monitoring of its effectiveness, considering a second-step medication when the first fails. Fluoxetine is the antidepressant of choice in monotherapy; switching to alternate SSRI in monotherapy (as escitalopram, sertraline, and citalopram) should be considered for youths who do not exhibit an adequate improvement. In adolescents who do not respond to SSRIs, a third-step is to switch to venlafaxine, which belongs to the SNRI class.54 Data coming from experimental studies in animals and humans seem to confirm no decrease of seizure threshold by SSRI adjunctive therapy. The misconception about the proconvulsant potential of many psychotropic drugs still represents a high obstacle in the prescription of these medications to treat depression in adolescents with epileptic seizures. This question was mostly based on anecdotal case reports and small case series. To better understand this phenomenon, multicenter randomized placebo-controlled trials that compared the incidence of seizures in patients randomly assigned to a psychotropic drug or to a placebo were performed.55 Trials with antidepressant drugs included: tricyclic agents, SSRIs, serotonin-noradrenaline reuptake inhibitors (SNRIs) venlafaxine, α2-antagonist mirtazapine, and noradrenaline-dopamine reuptake inhibitor bupropion. Seizure frequency was significantly lower in patients who received antidepressants compared to patients who received a placebo (standardized incidence ratio: 0.48; 95% CI 0.36–0.61); furthermore, in patients who received a placebo, seizures occurred more often compared to the general population. Seizure recurrence was higher both in patients treated with antidepressants and in the placebo group compared with the known incidence of seizures in the general population. These findings highlight the conception that depression itself represents a risk factor for the development of new onset epilepsy and provide supporting evidence that SSRIs and SNRIs could have an antiseizure action potential. Likewise, data on animal models seem to support this assumption;56,57 however, high-quality evidence controlled studies in humans have not yet been performed. A recent meta-analysis of clinical trials did not detect any evidence of increased seizures risk in epileptic patients receiving SSRIs, however, their safety profiles data were not fully definite particularly in long-term treatments.58 A lower seizure threshold has been reported to be related to high daily doses of antidepressants.42,49,59 Thus, the choice of administering a specific AED and, if needed, of an antidepressant drug should take into account all these caveats, including the tolerability, the potential side effects, and the pharmacokinetic and pharmacodynamic profiles. Non-enzyme levels of phenytoin, carbamazepine and valproic acid. Enzyme-inducing drugs like carbamazepine and phenytoin can, in turn, lower SSRI and other psychotropic blood levels, while non enzyme-inducing AEDs like valproic acid may inhibit the metabolism of some psychotropic agents. AEDs that do not induce or inhibit the CYP isoenzyme system include levetiracetam, lamotrigine, gabapentin, pregabalin, tiagabine, zonisamide, lacosamide, and perampanel. In general, many neurologists are moving toward the use of the newer- generation AEDs, due to their more favorable side effects and pharmacokinetic profile. Furthermore, in case of adolescents with comorbid anxiety and/or depressive symptoms, mood stabilizing AEDs like lamotrigine or valproic acid are often preferred. Conversely, drugs like Phenobarbital, topiramate and levetiracetam may worsen underlying mood disorders.
In conclusion, monitoring of depressive symptoms in adolescents with epilepsy is highly beneficial. NDDI-E-Y inventory is a brief, free useful tool to detect depressive symptoms with high sensitivity and specificity. Youths that are screened to be at risk of depression should be further evaluated and carefully followed-up. Thus, each child and adolescent epilepsy service should routinely administer screening questionnaires for anxiety and depression symptoms at each ambulatory visit. It is important to highlight that screening is generally used to detect disorders not symptoms. Hence, when a patient is screened positive, a clinical interview and a follow-up examination should be mandatory, since a mood disorder may develop throughout the clinical course. Furthermore, an early family and individual psychoeducation and psychological intervention may itself be effective in preventing a depressive disorder.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
2. Wiglusz MS, Landowski J, Cubała WJ. Interictal dysphoric disorder of epilepsy: a continuing diagnostic challenge. Epilepsy Behav. 2019;95:34–38. doi:10.1016/j.yebeh.2019.03.036
3. Berg AT, Caplan R, Hesdorffer DC. Psychiatric and neurodevelopmental disorders in childhood-onset epilepsy. Epilepsy Behav. 2011;20(3):550–555. doi:10.1016/j.yebeh.2010.12.038
4. Davies S, Heyman I, Goodman R. A population survey of mental health problems in children with epilepsy. Dev Med Child Neurol. 2003;45(5):292–295. doi:10.1017/s0012162203000550
5. Dunn DW, Austin JK, Perkins SM. Prevalence of psychopathology in childhood epilepsy: categorical and dimensional measures. Dev Med Child Neurol. 2009;51(5):364–372. doi:10.1111/j.1469-8749.2008.03172.x
6. Dunn DW, Besag F, Caplan R, Aldenkamp A, Gobbi G, Sillanpaa M. Psychiatric and behavioral disorders in children with epilepsy (ILAE task force report): anxiety, depression and childhood epilepsy. Epileptic Disord. 2016;18(Suppl. 1):S24–S30.
7. Ettinger AB, Weisbrot DM, Nolan EE, et al. Symptoms of depression and anxiety in pediatric epilepsy patients. Epilepsia. 1998;39(6):595–599. doi:10.1111/j.1528-1157.1998.tb01427.x
8. Reilly C, Agnew R, Neville BG. Depression and anxiety in childhood epilepsy: a review. Seizure. 2011;20(8):589–597. doi:10.1016/j.seizure.2011.06.004
9. Roeder R, Roeder K, Asano E, Chugani HT. Depression and mental health help-seeking behaviors in a predominantly African American population of children and adolescents with epilepsy. Epilepsia. 2009;50(8):1943–1952. doi:10.1111/j.1528-1167.2009.02046.x
10. Russ SA, Larson K, Halfon N. A national profile of childhood epilepsy and seizure disorder. Pediatrics. 2012;129(2):256–264. doi:10.1542/peds.2010-1371
11. Plioplys S. Depression in children and adolescents with epilepsy. Epilepsy Behav. 2003;4(Suppl. 3):S39–S45.
12. Scott AJ, Sharpe L, Hunt C, Gandy M. Anxiety and depressive disorders in people with epilepsy: a meta-analysis. Epilepsia. 2017;58(6):973–982. doi:10.1111/epi.13769
13. Austin JK, Perkins SM, Johnson CS, et al. Self-esteem and symptoms of depression in children with seizures: relationships with neuropsychological functioning and family variables over time. Epilepsia. 2010;51(10):2074–2083. doi:10.1111/j.1528-1167.2010.02575.x
14. Caplan R, Siddarth P, Gurbani S, Hanson R, Sankar R, Shields WD. Depression and anxiety disorders in pediatric epilepsy. Epilepsia. 2005;46(5):720–730. doi:10.1111/j.1528-1167.2005.43604.x
15. Adelöw C, Anderson T, Ahlbom A, Tomson T. Hospitalization for psychiatric disorders before and after onset of unprovoked seizures/epilepsy. Neurology. 2012;78(6):396–401. doi:10.1212/WNL.0b013e318245f461
16. Hesdorffer DC, Ishihara L, Mynepalli L, Webb DJ, Weil J, Hauser WA. Epilepsy, suicidality, and psychiatric disorders: a bidirectional association. Ann Neurol. 2012;72(2):184–191. doi:10.1002/ana.23601
17. Hesdorffer D. Comorbidity between neurological illness and psychiatric disorders. CNS Spectr. 2016;21(3):230–238. doi:10.1017/S1092852915000929
18. Hoppe C, Elger CE. Depression in epilepsy: a critical review from a clinical perspective. Nat Rev Neurol. 2011;7(8):462–472. doi:10.1038/nrneurol.2011.104
19. Josephoson CB, Lowerison M, Vallerand I, et al. Association of depression and treated depression with epilepsy and seizure outcomes: a multicohort analysis. JAMA Neurol. 2017;74(5):533–539.
20. Kanner AM. Depression and epilepsy: a bidirectional relation? Epilepsia. 2011;52(Suppl. 1):21–27. doi:10.1111/j.1528-1167.2010.02907.x
21. Martin R, Faught E, Richman J, et al. Psychiatric and neurologic risk factors for incident cases of new-onset epilepsy in older adults: data from U.S. medicare beneficiaries. Epilepsia. 2014;55(7):1120–1127. doi:10.1111/epi.12649
22. Bremner JD, Narayan M, Anderson ER, Staib LH, Miller HL, Charney DS. Hippocampal volume reduction in major depression. Am J Psychiatry. 2000;157(1):115–118. doi:10.1176/ajp.157.1.115
23. Bremner JD, Vythilingam M, Vermetten E, et al. Reduced volume of orbitofrontal cortex in major depression. Biol Psychiatry. 2002;51(4):273–279. doi:10.1016/s0006-3223(01)01336-1
24. Kanner AM, Barry JJ, Gilliam F, Herman B, Meador KJ. Depressive and anxiety disorders in epilepsy: do they differ in their potential to worsen common antiepileptic drug-related adverse events? Epilepsia. 2012;53(6):1104–1108. doi:10.1111/j.1528-1167.2012.03488.x
25. Kozlowska K, Chudleigh C, Cruz C, et al. Psychogenic non-epileptic seizures in children and adolescents: part II - explanations to families, treatment, and group outcomes. Clin Child Psychol Psychiatry. 2018;23(1):160–176. doi:10.1177/1359104517730116
26. Reilly C, Menlove L, Fenton V, Das KB. Psychogenic nonepileptic seizures in children: a review. Epilepsia. 2013;54(10):1715–1724. doi:10.1111/epi.12336
27. Fiest KM, Patten SB, Jette N. Screening for depression and anxiety in epilepsy. Neurol Clin. 2016;34:351–361. doi:10.1016/j.ncl.2015.11.003
28. Wang YP, Gorenstein C. Psychometric properties of the Beck Depression Inventory-II: a comprehensive review. Braz J Psychiatry. 2013;35(4):416–431. doi:10.1590/1516-4446-2012-1048
29. Wiglusz MS, Landowski J, Michalak L, Cubała WJ. Validation of the Hospital Anxiety and Depression Scale in patients with epilepsy. Epilepsy Behav. 2016;58:97–101. doi:10.1016/j.yebeh.2016.03.003
30. Kovacs M. Children’s Depression Inventory 2nd Edition (CDI2). North Tonawanda, NY: Multi-Health Systems Inc; 2010.
31. Wiglusz MS, Landowski J, Michalak L, Cubała WJ. Validation of the Polish Version of the Hamilton Rating Scale for Depression in patients with epilepsy. Epilepsy Behav. 2016;62:81–84. doi:10.1016/j.yebeh.2016.06.030
32. Sanchez-Villegas A, Schlatter J, Ortuno F, et al. Validity of a self-reported diagnosis of depression among participants in a cohort study using the Structured Clinical Interview for DSM-IV (SCID-I). BMC Psychiatry. 2008;17(8):43. doi:10.1186/1471-244X-8-43
33. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):22–33;quiz 34-57.
34. Gilliam FG, Barry JJ, Hermann BP, Meador KJ, Vahle V, Kanner AM. Rapid detection of major depression in epilepsy: a multicentre study. Lancet Neurol. 2006;5(5):399–405. doi:10.1016/S1474-4422(06)70415-X
35. Wagner JL, Kellermann T, Mueller M, et al. Development and validation of the NDDI-E-Y: a screening tool for depressive symptoms in pediatric epilepsy. Epilepsia. 2016;57(8):1265–1270. doi:10.1111/epi.13446
36. Zamani G, Mehdizadeh M, Sadeghi P. Attempt to suicide in young ages with epilepsy. Iran J Pediatr. 2012;22(3):404–407.
37. Jones JE, Siddarth P, Gurbani S, Shields WD, Caplan R. Screening for suicidal ideation in children with epilepsy. Epilepsy Behav. 2013;29(3):521–526. doi:10.1016/j.yebeh.2013.09.020
38. Pettersson A, Bostrom KB, Gustavsson P, et al. Which instruments to support diagnosis of depression have sufficient accuracy? A systematic review. Nord J Psychiatry. 2015;69:497–508. doi:10.3109/08039488.2015.1008568
39. Lakkis NA, Mahmassani DM. Screening instruments for depression in primary care: a concise review for clinicians. Postgrad Med. 2015;127:99–106. doi:10.1080/00325481.2015.992721
40. Kellermann TS, Mueller M, Carter EG, et al. Prediction of specific depressive symptom clusters in youth with epilepsy: the NDDI-E-Y versus Neuro-QOL SF. Epilepsia. 2017;58(8):1370–1379. doi:10.1111/epi.13808
41. Barry JJ, Ettinger AB, Friel P, et al. Consensus statement: the evaluation and treatment of people with epilepsy and affective disorders. Epilepsy Behav. 2008;13(Suppl.1):S1–S29. doi:10.1016/j.yebeh.2008.04.005
42. Kanner AM. Management of psychiatric and neurological comorbidities in epilepsy. Nat Rev Neurol. 2016;12(2):106–116. doi:10.1038/nrneurol.2015.243
43. Mula M, Jauch R, Cavanna A. el at. Clinical and psychopathological definition of the interictaldysphoric disorder of epilepsy. Epilepsia. 2008;49(4):650–656. doi:10.1111/j.1528-1167.2007.01434.x
44. Chen B, Detyniecki K, Choi H, et al. Psychiatric and behavioural side effects of antiepileptic drugs in adolescents and children with epilepsy. Eur J Paediatr Neurol. 2017;21(3):441–449. doi:10.1016/j.ejpn.2017.02.003
45. Kanner AM, Dunn DW. Diagnosis and management of depression and psychosis in children and adolescents with epilepsy. J Child Neurol. 2004;19(Suppl.1):S65–S72. doi:10.1177/088307380401900108
46. Mula M, Hesdorffer DC, Trimble M, Sander JW. The role of titration schedule of topiramate for the development of depression in patients with epilepsy. Epilepsia. 2009;50(5):1072–1076. doi:10.1111/j.1528-1167.2008.01799.x
47. Tomson T, Marson A, Boon P, et al. Valproate in the treatment of epilepsy in girls and women of childbearing potential. Epilepsia. 2015;56(7):1006–1019. doi:10.1111/epi.13021
48. Ramos-Perdigués S, Baillés E, Mané A, et al. Psychiatric symptoms in refractory epilepsy during the first year after surgery. Neurotherapeutics. 2018;15(4):1082–1092. doi:10.1007/s13311-018-0652-1
49. Kanner AM. The treatment of depressive disorders in epilepsy: what all neurologist should know. Epilepsia. 2013;54(Suppl. 1):3–12. doi:10.1111/epi.12100
50. Sirven JI. Management of epilepsy comorbidities. Continuum (minneapminn). 2016;22(1Epilepsy):191–203.
51. Martinović Z, Simonović P, Djokić R. Preventing depression in adolescents with epilepsy. Epilepsy Behav. 2006;9(4):619–624. doi:10.1016/j.yebeh.2006.08.017
52. Thome-Souza MS, Kuczynski E, Valente KD. Sertraline and fluoxetine: safe treatments for children and adolescents with epilepsy and depression. Epilepsy Behav. 2007;10(3):417–425. doi:10.1016/j.yebeh.2007.01.004
53. National Institute for Health and Care Excellence. Depression in children and young people: identification and management in primary, community and secondary care. (Clinical guideline 28.). 2015. Available from: www.nice.org.uk/guidance/cg28.
54. Brent D, Emslie G, Clarke G, et al. Switching to another SSRI or venlafaxine with or without cognitive behavioral therapy for adolescents with SSRI-resistant depression: the TORDIA randomized controlled trial. JAMA. 2008;299(8):910–913. doi:10.1001/jama.299.8.901
55. Alper K, Schwartz KA, Kolts RL, Khan A. Seizure incidence in psychopharmacological clinical trials: an analysis of Food and Drug Administration (FDA) summary basis of approval reports. Biol Psychiatry. 2007;62(4):345–354. doi:10.1016/j.biopsych.2006.09.023
56. Jobe PC, Kanner AM, and Gilliam FG. In Depression and Brain Dysfunction. Gilliam F, editors. London, UK:Taylor & Francis; 2006:121–157.
57. Jobe Pc, Mishra Pk, Browning Ra, et al. Noradrenergic abnormalities in the genetically epilepsy-prone rat. Brain Res Bull. 1994;35(5–6):493–504. doi:10.1016/0361-9230(94)90163-5
58. Maguire MJ, Weston J, Singh J, Marson AG. Antidepressant for people with epilepsy and depression. Cochrane Database Syst Rev. 2014;3(12):CD010682.
59. Singh T, Goel RK. Managing epilepsy-associated depression: serotonin enhancers or serotonin producers? Epilepsy Behav. 2017;66:93–99. doi:10.1016/j.yebeh.2016.10.007
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.