")
Back to Journals » Infection and Drug Resistance » Volume 16
Molecular Epidemiology of Carbapenem Resistant Klebsiella Pneumoniae in Northern China: Clinical Characteristics, Antimicrobial Resistance, Virulence and Geographic Distribution
Authors Cai W, Kang J, Ma Y , Yin D, Song Y, Liu Y, Duan J
Received 17 September 2023
Accepted for publication 11 November 2023
Published 20 November 2023 Volume 2023:16 Pages 7289—7304
DOI https://doi.org/10.2147/IDR.S436284
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Wanni Cai,1– 3,* Jianbang Kang,4,* Yanbin Ma,1– 3 Donghong Yin,5 Yan Song,5 Yujie Liu,1– 3 Jinju Duan5
1School of Pharmacy, Shanxi Medical University, Taiyuan, 030001, People’s Republic of China; 2Medicinal Basic Research Innovation Center of Chronic Kidney Disease, Ministry of Education, Shanxi Medical University, Taiyuan, 030001, People’s Republic of China; 3Shanxi Provincial Key Laboratory of Drug Synthesis and Novel Pharmaceutical Preparation Technology, Shanxi Medical University, Taiyuan, 030001, People’s Republic of China; 4Department of Microbiology, Second Hospital of Shanxi Medical University, Taiyuan, 030001, People’s Republic of China; 5Department of Pharmacy, Second Hospital of Shanxi Medical University, Taiyuan, 030001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinju Duan, Department of Pharmacy, Second Hospital of Shanxi Medical University, No. 382, Wuyi Road, Xinghualing District, Taiyuan, 030001, Shanxi, People’s Republic of China, Tel +86 351 3365713, Email [email protected]
Purpose: In this article, we studied in detail 74 Carbapenem Resistant Klebsiella pneumoniae (CRKP) in Shanxi to provide essential insight into development of effective strategies for control of CRKP.
Patients and Methods: From 2018 to 2021, we collected 74 clinical CRKP from 11 hospitals in Shanxi Province. Clinical data were obtained from medical records, and all isolates were subjected to antimicrobial susceptibility testing, multi locus sequence typing, capsular serotypes, resistant gene profiles and virulence gene profiles. The synergistic activity was performed by microdilution checkerboard method.
Results: Our study found differences in the clinical characteristics of CRKP between regions in Shanxi. Sequence type (ST) 11 was the dominant ST in Shanxi; however, the ST types in Shanxi had become more diverse over time and the proportion of STs showed a more balanced distribution with a significant decrease in ST11. NDM was the most common carbapenemase in Shanxi. In addition, the STs, carbapenemases, serotypes and virulence gene distribution varied by region in Shanxi. Moreover, tigecycline in combination with carbapenems and aztreonam had an excellent synergistic effect on CRKP in vitro.
Conclusion: The results of this study provide essential insight into development of effective strategies for control of CRKP in Shanxi.
Keywords: Klebsiella pneumoniae, antimicrobial resistance, carbapenemase, virulence, synergistic effect, China
Introduction
Klebsiella pneumoniae is a common cause of nosocomial and community-acquired infections, such as urinary tract infections, pneumonias, bacteremia, liver abscesses and surgical wound infections.1 The ability of K. pneumoniae to adapt through gene transfer, as well as its virulence and the convergence of resistance, has led to the emergence of strains causing severe and untreatable invasive infections.2 Carbapenems, such as imipenem and meropenem, are the commonly used agents to treat severe K. pneumoniae infections, and are also the last resort drugs for the treatment of multidrug resistance (MDR) K. pneumoniae infections.3 However, carbapenem resistant K. pneumoniae (CRKP) has emerged as a global crisis, becoming one of the most important and challenging pathogens causing infections with high mortality.4
According to the China Antimicrobial Resistance Surveillance System (CARSS),5 K. pneumoniae resistance rate to carbapenems gradually increased from 6.4% in 2013 (269 secondary hospitals and 841 tertiary hospitals) to 11.3% in 2021 (363 secondary hospitals and 1010 tertiary hospitals). However, according to the China Antimicrobial Surveillance Network (CHINET) (only 71 hospitals),6 K. pneumoniae resistance rate to imipenem and meropenem has risen dramatically from 3.0% and 2.9% in 2005 to 26% and 27.5% in 2022, respectively. These findings indicate that CRKP had spread rapidly and broadly in China. Carbapenem resistance in K. pneumoniae is mainly due to the production of carbapenemases, such as the class A serine carbapenemase K. pneumoniae (KPC) and New Delhi metallo-beta-lactamase (NDM).7 In 2004, the first KPC-2-producing K. pneumoniae isolate recorded in China was found in Zhejiang Province.8 Since then, KPC-2-producing K. pneumoniae has spread widely in China, and blaKPC-2 has become the most prevalent carbapenemase in China,8 with sequence type (ST) 11 contributing significantly to the dissemination of blaKPC-positive K. pneumoniae.9
Apart from antimicrobial resistance, another worrisome development is related to the evolution of hypervirulent K. pneumoniae (HvKP).10 Hypervirulence of K. pneumoniae is associated with diagnostic virulence genes such rmpA and iroN as well as hypermucoviscosity. In addition to intrinsic resistance to ampicillin, hvKP strains are usually susceptible to a variety of antibiotics, including cephalosporins and carbapenems; however, a fatal carbapenem-resistant hypervirulent K. pneumoniae (CR-hvKP) ST11 outbreak clone has recently appeared in eastern China.11 This finding suggests a worrying convergence of carbapenem resistance and hypervirulence in the already prevalent K. pneumoniae lineage. Although incidence of CR-hvKP has remained low,12 it is essential to understand how this lineage appeared and evolved in controlling its further dissemination.
The epidemic dynamics of CRKP differ across geographical regions. Due to the vast territory of China, it is crucial to comprehend local evolutionary and epidemiological variation to establish the most appropriate strategies of surveillance, infection control, and antibiotic stewardship. Shanxi Province, one of the 34 provincial-level administrative regions in China, is located in the northern part of the country, with a population of 34.8 million and an area of 156,700 square kilometers. In this study, we described the clinical characteristics, clonal relationships, genetic mechanisms of resistance and virulence, and vitro synergistic effect of 74 CRKP isolates in Shanxi Province, hoping to provide essential insight into development of effective strategies for control of CRKP and reducing the rate of untreatable infections in clinical settings.
Materials and Methods
CRKP Isolates
From January 1, 2018, to December 31, 2021, we collected 74 non-repetitive clinical CRKP from 11 hospitals in 11 prefecture-level cities across Shanxi Province, including Taiyuan, Lvliang, Jinzhong, Yangquan, Xinzhou, Datong, Shuozhou, Yuncheng, Linfen, Jincheng, and Changzhi (Table S1). One representative hospital from each location (usually the largest general hospital in the location) was chosen for isolates collection. According to the geographical distribution, we divided the locations into four areas: central (Taiyuan, Lvliang, Jinzhong, and Yangquan), northern (Xinzhou, Datong, and Shuozhou), southern (Yuncheng and Linfen), and southeast (Jincheng and Changzhi).
The Second Hospital of Shanxi Medical University, as the lead organization, regularly asked other hospitals about multidrug-resistant bacteria every six months from 2018 to 2021 and collected strains to establish a multidrug-resistant bacteria database. CRKP with carbapenem-resistant phenotype (resistant to at least one carbapenem such as imipenem, ertapenem, or meropenem) were detected in each hospital, and were first temporarily stored in the hospital’s −80°C refrigerator. It was then sent to the Second Hospital of Shanxi Medical University (the strains were preserved by the paper sheet method and sent on dry ice after three layers of tight packaging) after confirmation of the researchers’ inquiries, but the local failure of timely preservation could not be excluded.
Clinical Data Collection
Clinical data and patient information were obtained from medical records and included demographic characteristics, hospitalization, clinical diagnosis, antimicrobial therapy, invasive treatments and outcomes. This study was reviewed and approved by the research ethics committee of each participating hospital. We had hidden the patient’s information. The patients’ written informed consent was exempt.
Multilocus Sequence Typing (MLST)
We performed MLST as described on the Pasteur Institute MLST website (http://www.pasteur.fr/recherche/genopole/PF8/mlst/Kpneumoniae.html). The sequences of seven housekeeping genes (gapA, mdh, phoE, tonB, infB, pgi, and rpoB) were compared with those in the MLST databases (Institute Pasteur MLST Database; https://bigsdb.pasteur.fr/Klebsiella).
CRKP Definition and Antimicrobial Susceptibility Testing
K. pneumoniae strains that resistant to at least one carbapenem such as imipenem, ertapenem, or meropenem were defined as CRKP, according to the recommendation of the Clinical and Laboratory Standards Institute (CLSI) 2021.13 Strain identity was confirmed by MALDI-TOF mass spectrometry (BrukerDaltonik GmbH, Bremen, Germany). Antimicrobial susceptibilities were determined by the VITEK-2 compact system (bioMérieux). Susceptibilities to colistin and tigecycline were determined by the broth dilution method according to CLSI 2021.13 In this study, the minimum inhibitory concentration (MIC) results were interpreted according to the breakpoints defined by the CLSI 2021,13 with the exception of tigecycline, which were based on the US Food and Drug Administration (FDA) breakpoints (≤2 mg/liter was susceptible, 4 mg/liter was intermediate, and ≥8 mg/liter was resistant). Multiple antibiotic resistance index (MARI) was measured as a/b, where a = the total number of antibiotics to which an isolate was resistant and b = the total number of antibiotics tested.14
Phenotypic Confirmation of Carbapenemases
All CRKP were screened for carbapenemase production using the modified carbapenem inactivation method (mCIM) together with EDTA-modified carbapenem inactivation method (eCIM), according to CLSI 2021.13 The mCIM and eCIM results were interpreted as follows: only mCIM positive: serine carbapenemase positive (Ambler A and D group carbapenemase); both mCIM/eCIM positive: metallo-beta-lactamases positive (Ambler B group carbapenemase). It should be noted that eCIM was only valid for isolates that tested positive for mCIM.
Molecular Detection of Carbapenemases and Other Resistant Genes
The polymerase chain reaction (PCR) was performed with specific primers to detect the presence of Ambler A carbapenemase (blaKPC, blaNMC, blaSME, blaIMI, blaGES), Ambler B group carbapenemase (blaNDM, blaIMP, blaVIM, blaSPM, blaGIM, blaSIM), Ambler D group carbapenemase (blaOXA-48, 23, 24, 58, 51-like), Extended-spectrum β-lactamases (ESBLs) (blaCTX−M, blaSHV, and blaTEM), and AmpC enzyme gene (blaDHA, blaCMY and blaACT). The sequence of primers for each gene are listed in Table S2. The results of whole genome sequencing of the four novel ST CRKP strains (ST4564, ST5365, ST5647, and ST5587) identified in this study were described in detail in previous studies.15,16
Identification of Serotypes
The serotypes were detected by wzi locus. The sequences of wzi were compared with the pasteur databases (https:// bigsdb.pasteur.fr/Klebsiella). Positive PCR products were visualized by agarose gel electrophoresis, purified with a QIAquick PCR Purification Kit (Qiagen, Valencia, CA, USA) and sequenced by Sanger sequencing on an ABI PRISM 3730XL system (Applied Biosystems, Foster City, CA, USA).
Detection of Virulence Genes and Hypermucoviscosity Phenotype
Multiplex PCR for virulence genes including iucA, iutA, iroN, rmpA, rmpA2, ureA, ugeA, fimH, mrkD, kfu, peg344 and peg589 was performed. The sequence of primers for each gene are listed in Table S2. We used the string test to detect hypermucoviscosity phenotype as described previously.16 The positive for the string test was defined as the formation of a viscous string exceeding 5 mm in length, as previously described.
Tigecycline Combinations Checkerboard Assay
Synergistic activity of tigecycline–imipenem (TGC+IPM), tigecycline–meropenem (TGC+MEM), and tigecycline– aztreonam (TGC+ATM) combinations were performed by microdilution checkerboard method using 96-well microtiter plates (Corning Corporation, America). The concentration ranges were based on the MICs determined above. The effects of antibiotics in combination were quantified by the fractional inhibitory concentration (FIC) index. The FIC index ≤0.5 was interpreted as synergy, >0.5 to ≤1.0 as additive, >1.0 to ≤4.0 as irrelevant and >4.0 as antagonism. The cation adjusted Mueller-Hinton broth (CAMHB) served as negative control (Hepebio, Qingdao Hope Biotechnology, Qingdao, Shandong, China) and bacterial suspension served as positive control.
Statistical Analysis
Statistical analysis was performed using SPSS 25.0 software (IBM Corporation, Armonk, NY, USA). Continuous variables were assessed by independent sample t-test or variance analysis. The comparison of the categorical variables was calculated by Chi-square test or Fisher’s exact test. The linear-by-linear association test were used to assess the changes in CRKP over the calendar year. P value <0.05 was considered to be statistically significant.
Results
General Clinical Characteristics
A total of 74 CRKP strains were collected in this study, 31 strains from central Shanxi, 22 from northern Shanxi, 12 from southern Shanxi and 9 from southeast Shanxi (Table 1). The differences in the patient demographic and clinical characteristics among the various region were not statistically significant, except for wards distribution and indwelling device use (Table 1). The mean age of the included patients was 55.9 ± 19.6 years, ranging from 1 to 95 years (Table 1, Table S1). The majority of patients were males (n = 52, 70.2%), but this ratio was lower in the southern district (n = 6, 50.0%). CRKP isolates were obtained from 17 different wards, mainly from intensive care unit (ICU; n = 15, 20.3%), hematology unit (n = 13.17.6%), and neurosurgery unit (n = 12, 16.2%). Nearly half of the patients in northern Shanxi and southern Shanxi were from ICU (P = 0.008) and neurosurgery unit (P = 0.043), respectively; however, only central Shanxi and southeast Shanxi had patients from the blood transplantation unit (P = 0.009). Most isolates were from sputum (n = 38, 51.4%), blood (n = 14, 18.9%) and secretion (n = 8, 10.8%), which accounted for predominant sources of CRKP in various regions of Shanxi Province. The most prevalent infections were pneumonia (n = 43, 58.1%) and bloodstream infection (n = 13, 17.6%), which were also the most common types of infections in various regions of Shanxi. Surgical treatments were performed in 59.5% (n = 44) of the patients, and this ratio was higher in the southern Shanxi (n = 9, 75.0%). The majority of patients were exposure to antibiotics (n = 69, 93.2%), and all patients in the northern and southern Shanxi received antibiotics prior to isolation of CRKP. There were 36.5% of patients isolated with CRKP using central venous catheter, particularly, 59.1% of patients in the northern Shanxi used central venous catheter, compared to less than 36% in the other regions (P = 0.021). In contrast to more than 50% of patients in the other regions, only 22.2% of patients in southeast Shanxi used gastrostomy tube (P = 0.016).
 |
Table 1 Demographic and Clinical Characteristics of Patients with Carbapenem-Resistant Klebsiella Pneumoniae |
Among 74 patients, 67.6% (n = 50) presented clinical improvement at discharge, and 32.4% (n = 24) died or abandoned treatment due to the severity of condition. Half of patients in northern Shanxi died or abandoned treatment, compared to less than 26% in other regions, although there were no significant differences between regions.
CRKP Sequence Types (STs)
Overall, 74 CRKP in this study belonged to 32 different STs, with ST11 being the predominant ST (n = 33, 44.5%), followed by ST15 (n = 4, 5.4%), ST37 (n = 3, 4.0%), ST485 (n = 3, 4.0%), ST17 (n = 2, 2.7%), ST307 (n = 2, 2.7%) and ST462 (n = 2, 2.7%). Single isolates were also recovered in 25 other STs (Figure 1).
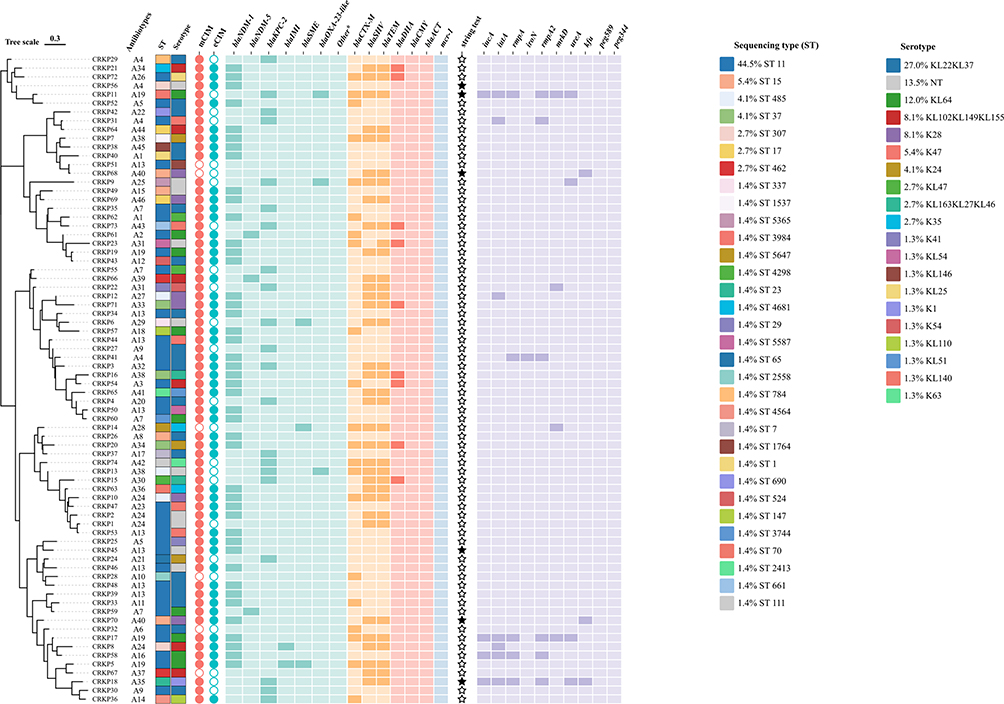 |
Figure 1 Phenotype and Genetic characteristics of Antimicrobial and Virulence of Carbapenem-Resistant Klebsiella pneumoniae. *Other carbapenemase genes included blaNMC, blaGES, blaIMP, blaVIM, blaSPM, blaGIM, blaSIM, and blaOXA48, 24, 58, 51-like. Abbreviations: ST, sequencing type; NT, non typable. |
Notably, 11 STs were found in 32 CRKP of 2018, 4 STs in 7 strains of 2019,11 STs in 18 strains of 2020, and 12 STs in 17 strains of 2021 (Figure 2A). In addition, one (ST4564), two (ST5365 and ST5647) and one novel ST (ST5587) were found in 2018, 2020 and 2021, respectively (Figure 2A). The proportion of ST11 decreased significantly over time, from 65.6% in 2018 to 11.7% in 2021 (P-trend < 0.001), although ST11 had always been the dominant ST, while the percentage of ST37, ST17, and ST462 increased significantly by 11.8% from 2018 to 2021 (P-trend < 0.05) (Figure 2A).
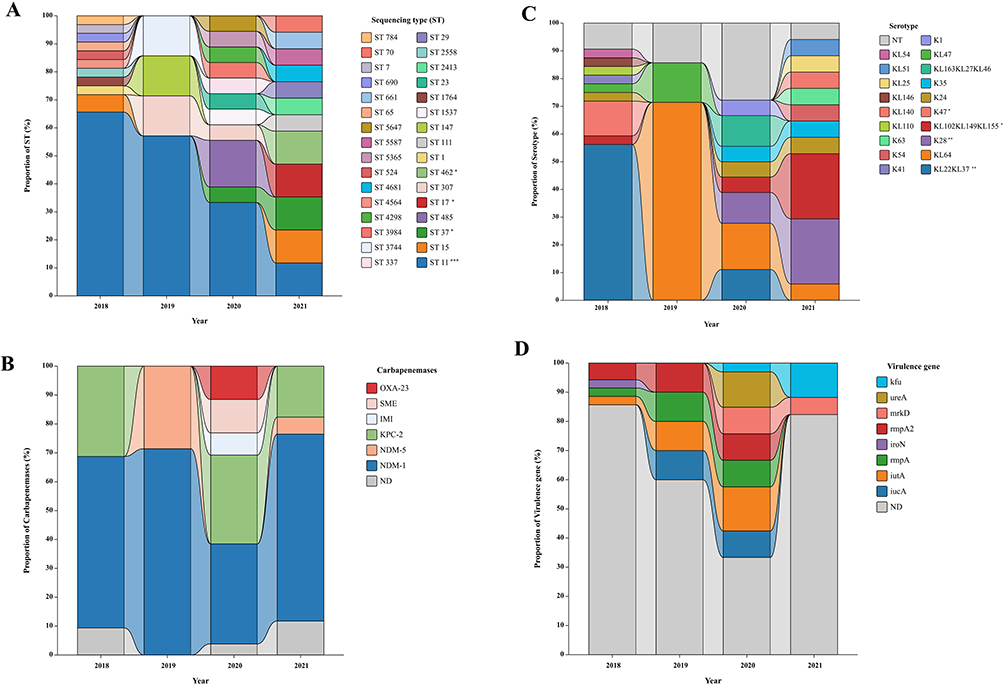 |
Figure 2 Distribution of ST (A), carbapenemase (B), serotype (C) and virulence gene (D) of Carbapenem-Resistant Klebsiella pneumoniae from 2018 to 2021. 32 CRKP strains were included in 2018, 7 in 2019, 18 in 2020, and 17 in 2021. *P-trend<0.05, **P-trend<0.01, ***P-trend<0.001. Abbreviations: ST, sequencing type; NT, non typable. ND, none detected. |
CRKP ST types were geographically diverse. Central Shanxi had 18 ST types (mainly ST11, ST485 and ST307), followed by 10 STs in southern Shanxi (mainly ST11 and ST15), 7 STs in northern Shanxi (mainly ST11), and 5 STs in southeast Shanxi (mainly ST11 and ST37) (Figure 3A, Table S1). Although ST11 was the most prevalent type in various regions of Shanxi, the percentage of ST11 in northern Shanxi was 68.2%, while other regions were less than 45% (Figure 3A). Notably, no ST11 CRKP was found in Shuozhou, a city in northern Shanxi, but instead consisted of one strain each of ST15, ST17 and ST462 (Figure S1A).
 |
Figure 3 Distribution of ST (A), carbapenemase (B), serotype (C) and virulence gene (D) of Carbapenem-Resistant Klebsiella pneumoniae in different regions of Shanxi Province, China. *P<0.05, ***P<0.001. Abbreviations: ST, sequencing type; NT, non typable. ND, none detected. |
Antimicrobial Susceptibility Testing Results
The detailed antimicrobial susceptibility testing results of the 18 drugs is listed in Table 2. The CRKP isolates showed high susceptibility to colistin (98.6%), followed by amikacin (78.4%), tigecycline (67.6%), fosfomycin (64.1%), and minocycline (42.5%), while the susceptibility to other antibiotics was below 23%. Notably, fewer than 5.5% of the CRKP were susceptible to meropenem, imipenem and ertapenem. The 74 CRKP had 44 (A1-A44) different antibiotypes (antibiotic resistance patterns) (Table S3). A14 (n = 9, 12.2%) was the most frequent pattern. Also, MARI ranged from 0.3 to 0.9 and the majority of isolates (n = 66, 89.2%) had MARI of ≥0.5 (Table S3). However, only 66.7% of CRKP in southern Shanxi (n = 8) had MARI of ≥0.5, while other regions were greater than 90%, especially in southeast Shanxi (n = 9, 100%) (Table S1).
 |
Table 2 Antimicrobial Susceptibility Testing Results of Carbapenem-Resistant Klebsiella Pneumoniae |
Antimicrobial Susceptibility Comparison Between ST11 and Non-ST11 CRKP
There were clear variations in susceptibility between ST11 CRKP and non-ST11 isolates (Figure 4). For ST11 CRKP, imipenem, ertapenem, cefaclor, ceftriaxone, ceftazidime, cefepime, aztreonam, cefoperazone sulbactam, ciprofloxacin, levofloxacin and chloramphenicol were all unsusceptible. The susceptibility of ST11 CRKP to drugs other than cephalosporin, minocycline and tigecycline was lower than that of non-ST11 isolates (Figure 4). The 2 groups of CRKP (ST11 vs non-ST11) differed significantly in terms of susceptibility to aztreonam (0% vs 22%, P < 0.01), cefoperazone sulbactam (0% vs 17.1%, P < 0.05), ciprofloxacin (0% vs 45.5%, P < 0.001), levofloxacin (0% vs 34.1%, P < 0.001), piperacillin tazobactam (3.0% vs 33.3%, P < 0.01) and minocycline (60% vs 13.3%, P < 0.01). The most common antibiotype of ST11 CRKP was A14 (n = 9, 27.2%), while A31 (n = 3, 7.3%) and A39 (n = 3, 7.3%) were the most frequent patterns in non-ST11 isolates (Figure 1, Table S1).
 |
Figure 4 Comparison of susceptibility between ST11 and non-ST11 Carbapenem-Resistant Klebsiella pneumoniae. *P<0.05, **P<0.01, ***P<0.001. Abbreviation: ST, sequencing type. |
Phenotypic Confirmation and Molecular Detection of Carbapenemase
In phenotypic evaluation, 24.3% (n = 18) and 66.2% (n = 49) of CRKP were serine carbapenemase producers (only mCIM positive) and MBL producers (both mCIM/eCIM positive), respectively (Figure 1). However, molecular detection showed that 32.4% (n = 24) and 63.5% (n = 47) of CRKP carried at least one serine carbapenemase (blaKPC, blaIMI, blaSME and blaOXA-23) and MBL gene (blaNDM), respectively (Figure 1).
Overall, carbapenemase genes were detected in 68 isolates (91.9%). The NDM-type carbapenemase gene was the most abundant type, with blaNDM-1 accounting for the majority (n = 44, 59.5%) and blaNDM-5 for the minority (n = 3, 4.1%), whereas blaKPC-2 was identified in 21 isolates (n = 21, 28.4%), and blaOXA-23, blaSME and blaIMI in 3 (n = 3, 4.1%), 3 (n = 3, 4.1%) and 2 (n = 2, 2.7%), respectively (Figure 1, Table S1). The distribution of carbapenemases was not significant from 2018 to 2021 (Figure 2B). Nevertheless, we found an increase in the type of carbapenemases produced from 2020 onwards and the emergence of isolates that coproduced carbapenemases (Figure 2B, Table S1). Seven CRKP strains coproduced at least two carbapenemase genes (n = 7, 9.5%). Coproduction of blaKPC-2+OXA-23 was found in 3 isolates (ST3984, ST5365, ST485) and co-production of blaNDM-1+KPC-2 in 1 isolate (ST11), blaNDM-1+IMI in 1 isolate (ST307), blaNDM-1+IMI+SME in 1 isolate (ST11), and blaKPC-2+SME in 1 isolate (ST337), respectively (Figure 1).
The distribution of carbapenemase differed significantly among regions in Shanxi (P = 0.049). All CRKP (n = 9) in southeast Shanxi, 96.8% (n = 30) in central Shanxi, 91.7% (n = 11) in southern Shanxi and 81.8% (n = 18) in northern Shanxi carried carbapenemase genes (Figure 3B, Figure S1B). A variety of carbapenemase genes (blaNDM-1, blaKPC-2, blaIMI, blaSME, blaOXA-23) were detected in central Shanxi, while in other regions only blaNDM and blaKPC were detected. The blaNDM-5 was only found in southern Shanxi and southeast Shanxi (P = 0.011). In addition, all seven coproduction CRKP strains were found in central Shanxi (Taiyuan) (Table S1).
Molecular Detection of Other Resistance Genes
More than half of CRKP (n = 44, 59.5%) harbored ESBL gene, including blaCTX-M (n = 21, 28.4%), blaSHV (n = 34, 45.9%) and blaTEM (n = 35, 47.3%). A total of 45.9% (n = 34) of CRKP carried more than one ESBL, of which all strains coproduced blaSHV+TEM (n = 34) and 32.4% coproduced blaCTX-M+SHV+TEM (n = 11).
Only 12.2% of isolates (n = 9) carried AmpC gene, all blaDHA. The frequency of co-occurrence of various beta-lactamases was as follows: AmpC/ESBL/carbapenemase (n = 9, 12.2%) and ESBL/carbapenemase (n = 31, 41.9%).
CRKP Serotypes
Of 19 different serotypes identified, KL22KL37 (n = 20, 27%) was dominant serotype in this study, followed by KL64 (n = 9, 12.0%), K28 (n = 6, 8.1%), KL102KL149KL155 (n = 6, 8.1%), K47 (n = 4, 5.4%) and K24 (n = 3, 4.1%) (Figure 1). There was a progressive enrichment of serotypes, but the dominant serotype varied from year to year (Figure 2C). In 2018, it was mainly KL22KL37 (n = 18, 56.2%) and K47 (n = 4, 12.5%), KL64 was popular in 2019 (n = 5, 71.4%) and 2020 (n = 3, 16.7%), and in 2021 it became dominated by K28 (n = 4, 23.5%) and KL102KL149KL155 (n = 4, 23.5%). In particular, KL22KL37 and K47 decreased significantly by 56.2% and 12.5%, respectively, from 2018 to 2021 (P-trend < 0.001 and P-trend = 0.035), while K28 and KL102KL149KL155 increased significantly by 23.5% and 20.4%, respectively (P-trend = 0.004 and P-trend = 0.029).
CRKP serotypes were also geographically diverse. Central Shanxi had 12 serotypes, followed by 8 serotypes in southern Shanxi, 6 serotypes in northern Shanxi, and 5 serotypes in southeast Shanxi (Table S1, Figure 3C, Figure S1C). KL22KL37 was the most prevalent type in northern Shanxi (n = 10, 45.5%), southern Shanxi (n = 3, 25.0%) and central Shanxi (n = 7, 22.6%), while KL64 (n = 5, 55.6%) was the most prevalent type in southeast Shanxi and KL22KL37 was not found in this area (P < 0.001) (Figure 3C). Moreover, K47 only detected in northern Shanxi (P = 0.026).
CRKP Virulence Gene and String Test
Eight virulence genes were detected in 13 CRKP isolates (n = 13, 17.6%): iutA (n = 7, 9.4%), rmpA2 (n = 6, 8.1%), rmpA (n = 5, 6.7%), iucA (n = 4, 5.4%), mrkD (n = 4, 5.4%), ureA (n = 4, 5.4%), kfu (n = 3, 4.0%) and iroN (n = 1, 1.3%) (Figure 1, Table S1). Nine of the 13 isolates carried more than one virulence gene. Five virulence gene combinations were identified, as follows: iutA + rmpA2 (n = 1, 1.3%), rmpA + iroN + rmpA2 (n = 1, 1.3%), iucA + iutA + rmpA + rmpA2 (n = 1, 1.3%), iucA + iutA + rmpA + rmpA2 + urea + kfu (n = 1, 1.3%), and iucA + iutA + rmpA + rmpA2 + mrkD + kfu (n = 2, 2.7%). In addition, the variety of virulence genes detected gradually increased from 2018 to 2020, but only two virulence genes (mrkD and kfu) were detected in 2021 (Figure 2D). Most of the detected virulence genes were distributed in the central and southeast Shanxi; three cities (Xinzhou, Linfen and Changzhi) did not detect any virulence genes (Figure 3D, Figure S1d).
Only 6 CRKP (8.1%) showed phenotype of hypermucoviscousity with positive string test, belonging to genetic lines ST15/K28 (n = 2), ST23/K1 (n = 1), ST3984/KL64 (n = 1), ST11/KL-NT (n = 1), and ST307/KL-NT (n = 1) (Figure 1). Isolates of ST15/K28 carried kfu; isolate of ST23/K1 harbored iucA + iutA + rmpA + rmpA2 + urea + kfu; isolate of ST3984/KL64 carried iucA + iutA + rmpA + rmpA2 + mrkD + kfu; isolate of ST11/KL-NT and ST307/KL-NT did not detect the aforementioned virulence genes.
Synergistic Effects of Tigecycline with Other Antibiotics
Half of CRKP (n = 37, 50.0%) were selected to evaluate the combined therapeutic effects of TGC with MEM, IPM, and ATM, of which 48.6% (n = 18) from northern Shanxi, 27.0% (n = 10) from central Shanxi, 16.2% (n = 6) from southern Shanxi and 8.1% (n = 3) from southeast Shanxi (Figure S2). The MICs of TGC were reduced by 17–25 fold on average in the TGC+IPM, TGC+MEM, and TGC+ATM combinations. The MICs of IPM and ATM decreased by 6-fold (2 ~ 2048-fold) and 16-fold (2 ~ 64-fold), respectively. In particular, the MIC of MEM dramatically decreased by an average of 134-fold (2~256-fold). TGC+IPM, TGC+MEM, and TGC+ATM combinations were high synergistic against 97.3% (36/37), 91.9% (34/37), and 91.9% (34/37) of CRKP isolates, respectively. Moreover, neither of the combinations of these isolates showed signs of irrelevant or antagonism. The results of the FICs are shown in Table 3.
 |
Table 3 Combined Therapeutic Effects of Tigecycline with Other Antibiotics |
Discussion
The continual emergence of CRKP strains is a major threat to public health worldwide. According to the CARSS,5 the rate of K. pneumoniae resistance to carbapenems in Shanxi Province increased from 1.2% in 2014 to 3.1% in 2021, while the data from CHINET showed that the detection rate of CRKP in Shanxi Province increased from 2.5% in 2017 to 4.7% in 2021.6 The gradual increase of CRKP in Shanxi Province needs to be alerted. Therefore, local epidemiologic data on the prevalence of specific CRKP clones are indispensable for developing clinical treatment regimens and evaluating the outcomes of various treatment strategies.
In this study, nearly half of the patients isolated from CRKP were older than 60 (n = 33, 44.6%), with 9.5% of them older than 80 years (n = 7, 9.5%) (Table S1), which may result from the decreased immune function of elderly patients.8 This finding is consistent with a study from Zhejiang, China, which reported that the detection rate of CRKP increased along with age and the highest proportion of resistant isolates was observed among those ≥60 years.8 In addition, most of the patients in our study were hospitalized in ICUs, which is considered as an important risk factor associated with CRKP in previous studies.17,18 The patients admitted to ICU are usually in a more severe condition, who also often have other coexisting health issues, may make them more susceptible to CRKP. Moreover, the ICU is a relatively confined space, and the poor ventilation makes it easier for CRKP to colonize and contaminate environmental surfaces in ICU wards, increasing the likelihood of transmission among patients, ICU staff, and the environment.19
In this study, 32.4% of patients isolated CRKP eventually died, including those who abandoned treatment due to the severity of disease because many Chinese chose to be discharged home at the end of life. The mortality of CRKP in this study was comparable to that in North America (33.2%), but higher than in previous studies in China (19.1–19.7%) and lower than in South America (46.7%) and Europe (50.1%).20–23 These differences may be due to differences in inclusion criteria and study design chosen by different investigators. In addition, patient conditions, co-morbidities, as well as geographic variations, should be taken into account. It is worth noting that the mortality rates in our study also varied by region, with mortality rates as high as 50% in northern Shanxi and less than 26% in other regions. We speculate that the high mortality rate in northern Shanxi may be relate to the high proportion of ICU patients (45.5%), the history of antibiotic exposure in all patients and the high use of invasive devices (50–81.8%), which are risk factors for death in patients isolated with CRKP reported in previous studies.17,18,24
Clonal lineages of K. pneumoniae differ in their ability to acquire resistance and virulence genes, and in their propensity to spread within hospital and community environments.2 In our study, CRKP had 32 STs, revealing polyclonality of Shanxi Province. ST11 of CRKP, but not ST258, a common strain type reported worldwide, is the dominant CRKP type in Shanxi Province, which has exhibited signs of multiclonal dissemination in China.25 Other STs are relatively rare and sporadically distributed, with ST15 being the next most common type. Notably ST15 is of growing concern given its characterization as both MDR and hypervirulent,26 which had led to the unfavorable prognosis of one patient in our study and in-hospital mortality in other study.27 Therefore, attention should be focused on the identification of sporadic STs and surveillance of the most prevalent clonal complexes.
In addition, the type of ST varied in each region of Shanxi Province, which may be relate to the geographical characteristics and location of Shanxi. Shanxi Province is roughly parallelogram shaped with a long north-south spacing of about 682 km, with Shaanxi to the south and Inner Mongolia to the north, which may explain the ST differences between the north and south of Shanxi Province in our study. Moreover, differences in climate and altitude in different regions will also screen for bacteria adapted to different growth environments. The insufficient strains in this study could also have an impact on the results. In particular, Taiyuan, located in central Shanxi, had the most abundant STs, probably due to its high traffic flow as the provincial capital and the fact that most of the patients with serious diseases in inferior hospitals are referred to Taiyuan, and this causes different ST of CRKP from different regions to cluster in here. Notably, carbapenemase genes, serotypes, and virulence genes also showed regional differences similar to ST types in this study, which may be related to the differences between STs in terms of fitness, epidemicity, and host-related factors, as well as the ability to acquire resistance and virulence genes.28 Therefore, molecular identification of specific high-risk clones in a region is of the utmost importance to implement appropriate infection control programs.
Treatment options for CRKP infections are very limited, cephalosporins, beta-lactamase inhibitor combinations, and fluoroquinolones were not suitable treatment options for most isolates owing to high levels of resistance (Table 2). These findings were consistent with recent reports of increasing emergence of highly resistant K. pneumoniae strains in different studies from Iran, India, Colombia and China.2,9,14,28 Moreover, ST11 showed a higher resistance than non-ST11 strains, which was similar with a previous nationwide study in China.9 Although most CRKP isolates were susceptible to colistin and tigecycline, monitoring in this study reported a 27.0% resistance rate for tigecycline but only a 1.4% resistance rate for colistin in CRKP isolates. Such a result was actually not unexpected, as in our region colistin is not usually part of the standard treatment regimen due to the severe nephrotoxicity and neurotoxicity, but is only used as a last resort and for MDR K. pneumoniae infections. However, the efficacy of colistin for treating CRKP infections has recently been questioned following clinical monotherapy trials.8 Another interesting finding of the current study was the high susceptibility of CRKP to fosfomycin (64.1%) and amikacin (78.4%), in contrast to previous reports of 21–50.7% sensitivity to fosfomycin and 27–47.7% sensitivity to amikacin.9,10,14,25 Notably, the resistance patterns were different in each region of Shanxi Province, with A23 and A18 predominating in central Shanxi, A14 and A4 in northern Shanxi, A31 and A2 in southern Shanxi, and A7 and A34 in southeast Shanxi (Table S1). There are a number of reasons that could explain these inconsistencies, including the source of isolates, sample type and size, different patient populations, and treatment regimens commonly prescribed in the region. This result provides important data for selecting specific drugs for the clinical therapy of infections caused by CRKP.
Carbapenemase-producing CRKP strains carry resistance genes on mobile plasmids that can shuttle between resistant and susceptible strains.9 The blaKPC-2 has become the most widely spread carbapenemase gene in China,9 while our data showed that blaNDM-1 was the main drug resistance factor of CRKP in Shanxi (found in 59.5% of isolates). Alarmingly, NDM-1 has prevalent in K. pneumoniae in China, India, and Pakistan.2,29,30 In addition, the OXA-lactamases in K. pneumoniae strains were usually blaOXA-48,31 however, in our study, no such enzyme was found. Instead, we detected three strains harbored blaOXA-23, which are scarcely found in K. pneumoniae but more commonly in Acinetobacter baumannii.31 A review of the medical records revealed that one patient (CRKP11) was detected for CRKP carrying blaOXA-23 along with MDR A. baumannii (resistant to carbapenem, penicillin, penicillin with enzyme inhibitors, cephalosporin, cephalosporin with enzyme inhibitors, aminoglycoside, quinolone, tetracycline, sulfonamide), which probably led to the transmission of blaOXA-23 located in the plasmid.31 The blaOXA-23 of the other two CRKP strains were probably from other patients infected with A. baumannii in the same unit or ward. Furthermore, IMI or SME-producing strains were rarely reported. In this study, two IMI-producing strains and three SME-producing strains were detected. IMI carbapenemases have been reported to be associated with a gene encoding a LysR-type transcriptional regulator, conferring high resistance to imipenem and meropenem; it has mainly been identified in Enterobacter cloacae and Enterobacter asburiae.32 And the SME enzymes have been found only infrequently and sporadically worldwide in Serratia marcescens.33 The blaIMI or blaSME -mediated carbapenem resistance is an infrequent mechanism but it has been reported both in hospitals and community environments in China.32 However, the exact origin of IMI and SME enzymes and how they emerged in K. pneumoniae still remain unclear. Notably, a recent single center study conducted locally in Shanxi showed that CRKP carrying blaIMI and blaSME also emerged from a hospital in Taiyuan,34 reminding us that transmission of this type of strain may have occurred in Shanxi and requires close attention and continuous monitoring.
Of note, a CRKP strain coproducing blaNDM-1+KPC-2 was identified in this study, and co-occurrence of blaKPC-2 and blaNDM-1 has rarely been reported yet. The conjugation assay in a study reflected that blaNDM-1 plasmid is more prone to transfer than blaKPC-2 plasmid;35 therefore, it is possible that the emergence of KPC-2-NDM-1-CRKP was owing to blaNDM-1 plasmid transferred into blaKPC-2 plasmid, which can increase resistance of this type of bacteria. This also raised an alarm on the increased prevalence of co-existing blaKPC-2 and blaNDM-1 CRKP isolates with characteristics of high stability and non-inferior fitness, which may increase the difficulty of treating and prolonging infections.35 Our study also identified other strains that produced at least two genes, including blaKPC-2+OXA-23, blaNDM-1+IMI, blaKPC-2+SME, and blaNDM-1+IMI+SME, which have been rarely reported worldwide. Monitoring the dynamics of CRKPs with coproductions in the surveillance program is essential because of the potential risks they present, and because the way they emerge and whether they are only transient or have transmission capacity remain uncertain.28
However, six CRKP were negative for the carbapenemase gene detection and only one strain was positive for the carbapenemase production via mCIM experiment, which means the other five CRKP strains have other mechanisms for carbapenem resistance. Possible explanations include the existence of mutations or loss of outer membrane porins (especially for the OmpK35 and OmpK36), or the active drug efflux.27 The relative detections of the six CRKP strains could be performed in the further study.
Although the positive rate of ESBL genes was >59% in CRKP in this study, we were unable to confirm this by phenotypic testing because the ESBL phenotype is no longer sensitive to carbapenemase.9 In our study, 45.9% and 47.2% CRKP carried blaSHV and blaTEM, respectively, while only 28.3% of CRKP with blaCTX-M. This finding is contrary to previous studies in China as well as in other countries that reported that blaCTX-M is the most popular ESBL.9,14,36 Antibiotic use plans differ in each region, which may cause selection pressure for the circulation of ESBL producing isolates and explain these inconsistencies. Also, the origin of collected samples and the geographical variances may contributed to these differences. There is evidence for the role of AmpC beta-lactamase in resistance to carbapenems and increasing their MIC.37 In our study, only 12.2% of isolates carried AmpC gene, all blaDHA. In a previous observation from Iran,14 higher prevalence rates of blaDHA (34.4%) were found in K. pneumoniae isolates.
The emergence of hypervirulent lineages carrying antimicrobial resistance genes including carbapenemases is now being increasingly reported: with limited treatment measures and high mortality, they are considered a “super-bug”.27 The differentiate of hvKP is usually based on phenotypic and genotypic characteristics, but so far there are no standard methods.14
A total of 19 serotypes were identified in our study, with KL22KL37 accounting for the majority. The most common serotypes of hvkP in China are KL64 and KL47,38 while KL22KL37 has rarely been reported, but a hospital in Taiyuan, Shanxi, also isolated CRKP identified as KL22KL37 in 2018.39 And most strains of KL22KL37 in this study were isolated in 2018, with only 2 sporadic strains appearing in 2020. This suggests that KL22KL37 may have undergone transmission between hospitals in Taiyuan and from Taiyuan to other regions of Shanxi in 2018. Nine CRKP strains in this study were identified as KL64, second only to KL22KL37, and were highly correlated with ST11 (n = 6, 66.6%), similar to previous studies.40
In our study, 6 of 74 CRKP isolates were string test positive, but only two strains carried rmpA and rmpA2, which were previously associated with the hypermucoviscous phenotype in K. pneumoniae strains.41 And one string test positive strain was negative for the virulence gene detection, which required the second- or third-generation sequencing to demonstrate the presence of other genes. Moreover, the string test only describes the phenotypic characteristics, but cannot represent the hypervirulent of the strains. In this study, only eight virulence genes were detected in 13 strains, including genes encoding capsular polysaccharides (rmpA, rmpA2, ureA), siderophores (iucA, iutA, iroN and kfu) and type III fimbriae (mrkD). However, 69.2% (n = 9) of isolates carrying gene markers had a negative string test. This phenomenon has also been reported in previous studies from Iran and China.10,14 This may be due to the presence of mutations in the studied genes that prevent their function to produce the hypervirulent phenotype.10 It is worth noting that in our study, a strain with the genetic line ST23/K1 was identified that was positive for string test and carried multiple virulence genes including iucA + iutA + rmpA + rmpA2 + ureA + kfu. Studies have shown that K1 is strongly related to ST23 and is the most predominant type of hvkP in Asia.41 Several studies have suggested that K1 strains have higher virulence than the strains of other serotypes, which could be attributed to the distinct compositions that confer survival advantages.42 A recent study showed that a surface-exposed protein, fructose-1, 6-bisphosphate aldolase, was identified in K1 hvKP, and its enhanced expression could protect bacteria against neutrophil killing under high glucose condition.43 Therefore, we must pay close attention to such strains to prevent the further spread.
TGC is currently a commonly used antibiotic for the clinical treatment of CRKP, but its use as monotherapy has been reported in the literature to have poor efficacy with reduced sensitivity, and TGC combined carbapenems are often used in combination therapy against CRKP strains.39,44 In view of the relatively low sensitivity of the strains to TGC found in this study and the predominance of NDM production in Shanxi, we conducted an in vitro synergistic test using TGC as the primary drug. The data showed that TGC in combination with carbapenems and ATM had an excellent synergistic effect on CRKP in vitro. TGC combined with IPM was the most effective. Our results inform an available selection for clinical treatment.
This study had some limitations. The participation of hospital was all tertiary hospital, so our results should not be interpreted as being representative of CRKP epidemiology for all types of hospitalized patients in Shanxi. However, patients with CRKP are generally more complex and severe, so they are actually more common in tertiary hospitals. Additionally, we did not carry out a detailed analysis of drug-resistant plasmids, which should be examined at later stages by second- or third-generation sequencing. Finally, the data conclusions about trends and distributions that might be artifacts of an incomplete or biased sampling.
Conclusion
In conclusion, to our knowledge this is the first province-wide CRKP study in Shanxi Province. Key findings of this study are summarized as follows. First, the differences in the patient demographic and clinical characteristics among the various region were not statistically significant, except for wards distribution and indwelling device use. Second, both ST types and serotypes in Shanxi province have become more diverse over time, and varied in each region. Third, NDM-1 is the most common carbapenemase in Shanxi and carbapenemases distribution have significant regional variability. Last but not least, TGC in combination with carbapenems and ATM had an excellent synergistic effect on CRKP in vitro. TGC combined with IPM was the most effective. According to the results of this study, we propose that nosocomial CRKP infection control strategies should be reevaluated and adjusted. Although the economy in Shanxi Province is underdeveloped, CRKP treatment must be considered urgent. Therefore, the establishment of increased and improved CRKP surveillance in hospitals is crucially needed to prevent the further spread of CRKP.
Ethics Approval and Consent to Participate
Our study complied with the Declaration of Helsinki. This study was reviewed and approved by the research ethics committee of the Second Hospital of Shanxi Medical University (Code 2021 YX-182). The data of patients’ clinical variables were collected from their medical records and did not contain names, addresses, or other personal information. The patient’s written informed consent was exempt. Informed consent is waived in the study because this research uses previous medical records, and meets all the following conditions: (1) the purpose of the study is important; (2) the exemption of informed consent will not adversely affect the rights and health of the subjects; (3) the privacy and personal identity information of the subjects were protected; (4) the study could not be carried out if informed consent was required. In summary, the Ethics Committee of the Second Hospital of Shanxi Medical University has approved the exemption of the patient’s written informed consent.
Acknowledgments
The authors would like to acknowledge the contribution of all involved staff members in the participating hospitals. This work was supported by the Shanxi Province Natural Science Foundation (grant number 201803D31124). The funders had no role in study design, data collection and interpretation, or the decision to submit the work for publication.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Paczosa MK, Mecsas J. Klebsiella pneumoniae: going on the offense with a strong defense. Microbiol Mol Biol Rev. 2016;80(3):629–661. doi:10.1128/MMBR.00078-15
2. Nagaraj G, Shamanna V, Govindan V, et al. High-resolution genomic profiling of carbapenem-resistant Klebsiella pneumoniae isolates: a multicentric retrospective Indian study. Clin Infect Dis. 2021;73(Suppl_4):S300–S307. doi:10.1093/cid/ciab767
3. Holt KE, Wertheim H, Zadoks RN, et al. Genomic analysis of diversity, population structure, virulence, and antimicrobial resistance in Klebsiella pneumoniae, an urgent threat to public health. Proc Natl Acad Sci U S A. 2015;112(27):E3574–E3581. doi:10.1073/pnas.1501049112
4. Agyeman AA, Bergen PJ, Rao GG, Nation RL, Landersdorfer CB. A systematic review and meta-analysis of treatment outcomes following antibiotic therapy among patients with carbapenem-resistant Klebsiella pneumoniae infections. Int J Antimicrob Agents. 2020;55(1):105833. doi:10.1016/j.ijantimicag.2019.10.014
5. CARSS. China antimicrobial resistance surveillance system; 2022. Available from: http://carss.cn/.
6. CHINET China antimicrobial surveillance network; 2022. Available from: http://www.chinets.com/Chinet/Index.
7. Queenan AM, Bush K. Carbapenemases: the versatile beta-lactamases. Clin Microbiol Rev. 2007;20(3):440–458. doi:10.1128/CMR.00001-07
8. Hu Y, Liu C, Shen Z, et al. Prevalence, risk factors and molecular epidemiology of carbapenem-resistant Klebsiella pneumoniae in patients from Zhejiang, China, 2008–2018. Emerg Microbes Infect. 2020;9(1):1771–1779. doi:10.1080/22221751.2020.1799721
9. Wang Q, Wang X, Wang J, et al. Phenotypic and genotypic characterization of carbapenem-resistant Enterobacteriaceae: data from a longitudinal large-scale CRE Study in China (2012–2016). Clin Infect Dis. 2018;67(suppl_2):S196–S205. doi:10.1093/cid/ciy660
10. Yang X, Sun Q, Li J, et al. Molecular epidemiology of carbapenem-resistant hypervirulent Klebsiella pneumoniae in China. Emerg Microbes Infect. 2022;11(1):841–849. doi:10.1080/22221751.2022.2049458
11. Gu D, Dong N, Zheng Z, et al. A fatal outbreak of ST11 carbapenem-resistant hypervirulent Klebsiella pneumoniae in a Chinese hospital: a molecular epidemiological study. Lancet Infect Dis. 2018;18(1):37–46. doi:10.1016/S1473-3099(17)30489-9
12. Du P, Zhang Y, Chen C. Emergence of carbapenem-resistant hypervirulent Klebsiella pneumoniae. Lancet Infect Dis. 2018;18(1):23–24. doi:10.1016/S1473-3099(17)30625-4
13. CaLS I. Performance Standards for Antimicrobial Susceptibility Testing. Wayne, PA: Clinical and Laboratory Standards Institute; 2021.
14. Saki M, Amin M, Savari M, Hashemzadeh M, Seyedian SS. Beta-lactamase determinants and molecular typing of carbapenem-resistant classic and hypervirulent Klebsiella pneumoniae clinical isolates from southwest of Iran. Front Microbiol. 2022;2:13.
15. Wang X, Li Q, Kang J, et al. Co-Production of NDM-1, CTX-M-9 Family and mcr-1 in a Klebsiella pneumoniae ST4564 Strain in China. Infect Drug Resist. 2021;14:449–457. doi:10.2147/IDR.S292820
16. Liu Y, Bai J, Kang J, et al. Three novel sequence types carbapenem-resistant Klebsiella pneumoniae strains ST5365, ST5587, ST5647 Isolated from two tertiary teaching general hospitals in Shanxi Province, in North China: molecular characteristics, resistance and virulence factors. Infect Drug Resist. 2022;15:2551–2563. doi:10.2147/IDR.S366480
17. Wu C, Zheng L, Yao J. Analysis of risk factors and mortality of patients with carbapenem-resistant Klebsiella pneumoniae infection. Infect Drug Resist. 2022;15:2383–2391. doi:10.2147/IDR.S362723
18. Chen J, Ma H, Huang X, et al. Risk factors and mortality of carbapenem-resistant Klebsiella pneumoniae bloodstream infection in a tertiary-care hospital in China: an eight-year retrospective study. Antimicrob Resist Infect Control. 2022;11(1):161. doi:10.1186/s13756-022-01204-w
19. Yan Z, Zhou Y, Du M, et al. Prospective investigation of carbapenem-resistant Klebsiella pneumonia transmission among the staff, environment and patients in five major intensive care units, Beijing. J Hosp Infect. 2019;101(2):150–157. doi:10.1016/j.jhin.2018.11.019
20. Pouch SM, Kubin CJ, Satlin MJ, et al. Epidemiology and outcomes of carbapenem‐resistant Klebsiella pneumoniae bacteriuria in kidney transplant recipients. Trans Infect Dis. 2015;17(6):800–809. doi:10.1111/tid.12450
21. Xu L, Sun X, Ma X. Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae. Ann Clin Microbiol Antimicrob. 2017;16(1):18. doi:10.1186/s12941-017-0191-3
22. Simkins J, Muggia V, Cohen HW, Minamoto GY. Carbapenem‐resistant Klebsiella pneumoniae infections in kidney transplant recipients: a case–control study. Trans Infect Dis. 2014;16(5):775–782. doi:10.1111/tid.12276
23. Hoxha A, Kärki T, Giambi C, et al. Attributable mortality of carbapenem-resistant Klebsiella pneumoniae infections in a prospective matched cohort study in Italy, 2012–2013. J Hos Infect. 2016;92(1):61–66. doi:10.1016/j.jhin.2015.06.018
24. Zhang H, Guo Z, Chai Y, et al. Risk factors for and clinical outcomes of carbapenem-resistant Klebsiella pneumoniae nosocomial infections: a retrospective study in a tertiary hospital in Beijing, China. Infect Drug Resist. 2021;14:1393–1401. doi:10.2147/IDR.S298530
25. Zhang R, Liu L, Zhou H, et al. Nationwide Surveillance of Clinical Carbapenem-resistant Enterobacteriaceae (CRE) Strains in China. EBioMedicine. 2017;19:98–106. doi:10.1016/j.ebiom.2017.04.032
26. David S, Reuter S, Harris SR, et al. Epidemic of carbapenem-resistant Klebsiella pneumoniae in Europe is driven by nosocomial spread. Nat Microbiol. 2019;4(11):1919–1929. doi:10.1038/s41564-019-0492-8
27. Zhao Y, Zhang S, Fang R, et al. Dynamic epidemiology and virulence characteristics of carbapenem-resistant Klebsiella pneumoniae in Wenzhou, China from 2003 to 2016. Infect Drug Resist. 2020;13:931–940. doi:10.2147/IDR.S243032
28. Saavedra SY, Bernal JF, Montilla-Escudero E, et al. Complexity of genomic epidemiology of carbapenem-resistant Klebsiella pneumoniae isolates in Colombia urges the reinforcement of whole genome sequencing-based surveillance programs. Clin Infect Dis. 2021;73(Suppl_4):S290–S299. doi:10.1093/cid/ciab777
29. Liu Z, Gu Y, Li X, et al. Identification and characterization of NDM-1-producing hypervirulent (Hypermucoviscous) Klebsiella pneumoniae in China. Ann Lab Med. 2019;39(2):167–175. doi:10.3343/alm.2019.39.2.167
30. Gondal AJ, Saleem S, Jahan S, Choudhry N, Yasmin N. Novel carbapenem-resistant Klebsiella pneumoniae ST147 coharboring bla (NDM-1), bla (OXA-48) and extended-spectrum beta-lactamases from Pakistan. Infect Drug Resist. 2020;13:2105–2115. doi:10.2147/IDR.S251532
31. Evans BA, Amyes SG. OXA beta-lactamases. Clin Microbiol Rev. 2014;27(2):241–263. doi:10.1128/CMR.00117-13
32. Zhang F, Wang X, Xie L, et al. A novel transposon, Tn6306, mediates the spread of bla(IMI) in Enterobacteriaceae in hospitals. Int J Infect Dis. 2017;65:22–26. doi:10.1016/j.ijid.2017.09.014
33. Dabos L, Patino-Navarrete R, Nastro M, et al. SME-4-producing Serratia marcescens from Argentina belonging to clade 2 of the S. marcescens phylogeny. J Antimicrob Chemother. 2019;74(7):1836–1841. doi:10.1093/jac/dkz115
34. Bai J, Liu Y, Kang J, et al. Antibiotic resistance and virulence characteristics of four carbapenem-resistant Klebsiella pneumoniae strains coharbouring bla(KPC) and bla(NDM) based on whole genome sequences from a tertiary general teaching hospital in central China between 2019 and 2021. Microb Pathog. 2023;175:105969. doi:10.1016/j.micpath.2023.105969
35. Gao H, Liu Y, Wang R, Wang Q, Jin L, Wang H. The transferability and evolution of NDM-1 and KPC-2 co-producing Klebsiella pneumoniae from clinical settings. EBioMedicine. 2020;51:102599. doi:10.1016/j.ebiom.2019.102599
36. Wang M, Earley M, Chen L, et al. Clinical outcomes and bacterial characteristics of carbapenem-resistant Klebsiella pneumoniae complex among patients from different global regions (CRACKLE-2): a prospective, multicentre, cohort study. Lancet Infect Dis. 2022;22(3):401–412. doi:10.1016/S1473-3099(21)00399-6
37. Kazemian H, Heidari H, Ghanavati R, et al. Phenotypic and genotypic characterization of ESBL-, AmpC-, and carbapenemase-producing Klebsiella pneumoniae and Escherichia coli Isolates. Med Princ Pract. 2019;28(6):547–551. doi:10.1159/000500311
38. Zhao L, Xia X, Yuan T, Zhu J, Shen Z, Li M. Molecular epidemiology of antimicrobial resistance, virulence and capsular serotypes of carbapenemase-carrying Klebsiella pneumoniae in China. Antibiotics. 2022;11:8.
39. Li Q, Zhu J, Kang J, et al. Emergence of NDM-5-producing carbapenem-resistant Klebsiella pneumoniae and SIM-producing hypervirulent Klebsiella pneumoniae isolated from aseptic body fluid in a large tertiary hospital, 2017–2018: genetic traits of blaNDM-like and blaSIM-like genes as determined by NGS. Infect Drug Resist. 2020;13:3075–3089. doi:10.2147/IDR.S261117
40. Zhou K, Xiao T, David S, et al. Novel subclone of carbapenem-resistant Klebsiella pneumoniae sequence type 11 with enhanced virulence and transmissibility, China. Emerg Infect Dis. 2020;26(2):289–297. doi:10.3201/eid2602.190594
41. Zhu J, Wang T, Chen L, Du H. Virulence factors in hypervirulent Klebsiella pneumoniae. Front Microbiol. 2021;12:642484. doi:10.3389/fmicb.2021.642484
42. Wang L, Shen D, Wu H, Ma Y. Resistance of hypervirulent Klebsiella pneumoniae to both intracellular and extracellular killing of neutrophils. PLoS One. 2017;12:3.
43. Lee CH, Chuah SK, Chang CC, Chen FJ. The surface protein fructose-1, 6 bisphosphate aldolase of Klebsiella pneumoniae Serotype K1: role of interaction with neutrophils. Pathogens. 2020;9(12):1009. doi:10.3390/pathogens9121009
44. Karah N, Sundsfjord A, Towner K, Samuelsen O. Insights into the global molecular epidemiology of carbapenem non-susceptible clones of Acinetobacter baumannii. Drug Resist Updat. 2012;15(4):237–247. doi:10.1016/j.drup.2012.06.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.