")
Back to Journals » OncoTargets and Therapy » Volume 15
Molecular Characteristics and the Effect of KRAS Mutation on the Prognosis of Immunotherapy in Non-Small Cell Lung Cancer in Xinjiang, China
Authors Gu G, Yu B, Wan H , Lu S, Zhu X, Zhao Y, Fuxi Y, Liu C
Received 15 July 2022
Accepted for publication 10 September 2022
Published 21 September 2022 Volume 2022:15 Pages 1021—1032
DOI https://doi.org/10.2147/OTT.S381825
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Gaetano Romano
Guomin Gu,1 Bo Yu,2 Hua Wan,2 Suqiong Lu,1 Xiaodan Zhu,1 Yan Zhao,1 Yujing Fuxi,1 Chunling Liu1
1Department of Pulmonary Medicine, Affiliated Cancer Hospital of Xinjiang Medical University, Urumqi, Xinjiang, 830011, People’s Republic of China; 2Department of Medicine, Beijing USCI Medical Laboratory, Beijing, 100195, People’s Republic of China
Correspondence: Chunling Liu, Department of Pulmonary Medicine, Affiliated Cancer Hospital of Xinjiang Medical University, No. 789 Suzhou East Street, Urumqi, Xinjiang, 830011, People’s Republic of China, +Tel/Fax +86-991-7819352, Email [email protected]
Purpose: Non-small cell lung cancer (NSCLC) is a malignant tumor with high mortality. The Kirsten rat sarcoma vial oncogene (KRAS) gene can affect patient prognosis. In this study, we aim to explore the impact of KRAS mutation status on the clinical prognosis of NSCLC immunotherapy.
Patients and Methods: Collected tumor samples from the Affiliated Cancer Hospital of Xinjiang Medical University and 220 patients with stage III–IV NSCLC were included the study. All patients are on first- or second-line therapy and not on targeted therapy. Based on the molecular profiles and clinical features, we analysis of the effect of KRAS mutation on the treatment outcome of NSCLC.
Results: In this study, the main mutant subtypes of KRAS were G12C, G12D, and G12V. In the KRAS mutation group, the highest mutation frequency other than KRAS was TP53, followed by STK11 and KMT2C. We found that among patients received immunotherapy, KRAS-mutant patients were more sensitive to immunotherapy, with an objective response rate (ORR) of 65% and a disease control rate (DCR) of 80%. Survival analysis found that patients with KRAS mutation had better prognosis with immunotherapy than the non-KRAS mutation patients by comparing the overall survival (OS) (median OS: 18.1 months vs 12.2 months, p=0.0032) and progression-free survival (PFS) (media PFS: 7.9 months vs 3.6 months, p=0.01). We found that the patients with KRAS mutation had better prognosis with immunotherapy than with chemotherapy (median OS: 18.1 months vs 12.3 months, p=0.039, PFS 7.9 months vs 4.1 months, p=0.001). Patients with the KRAS G12C mutation had better results with immunotherapy than chemotherapy, but there was no significant difference in outcome between the two groups (OS: p=0.26 PFS: p=0.055). KRAS and TP53 co-mutation and KRAS and KMT2C co-mutation may improve response to immunotherapy.
Conclusion: Our results suggested that the gene mutation profile of NSCLC in KRAS mutation group and non-KRAS mutation group were different. The patients with KRAS mutation will have better prognosis with immunotherapy.
Keywords: NSCLC, KRAS, mutation, immunotherapy, prognosis
Introduction
Non-small cell lung cancer (NSCLC), one of the major histological classes of lung cancer, is approximately 85% of all lung cancer.1 With the tumor gene detection becoming the recommended method among national guidelines for the diagnosis and treatment of cancer patients,2 Kirsten rat sarcoma vial oncogene (KRAS) gene has been shown to be one of the most prevalent oncogenic drivers of human cancer.3 KRAS, along with NRAS, and HRAS genes, members of the Ras superfamily, is the first identified human oncogene in 1982.4 Several meta-analyses have shown that the frequency of KRAS mutations is associated with regions, accounting for 26.1% of individual mutation rates in lung adenocarcinoma (LUAD) among Western and about 11.2% of Asian patients.5 The human KRAS gene is located in chromosome 12.p12.1, and the most frequent mutations that occur in condon 12 in NSCLC are G12C, G12D, and G12V. Those common G12 mutations are commonly associated with poor prognosis.6–8
For more than three decades, there have not been highly efficient promising drugs targeting KRAS mutations developed, untill sotorasib (AMG510) being approved by FDA for the treatment of patients with advanced KRAS G12C-mutant NSCLC following at least one prior systemic therapy in 2021.9,10 However, chemotherapy is yet the standard treatment for advanced NSCLC patients with KRAS mutations. The development of immune checkpoint inhibitors (ICIs) immunotherapy should be a rising therapy in curing KRAS mutation patients.11–14 A meta-analysis by Lee et al reported that ICIs appeared to improve survival compared to docetaxel, in the subgroup of KRAS mutant patients but not in KRAS wt ones.15–17 Another subgroup analysis of a randomized Phase III study, CheckMate057, shows that nivolumab monotherapy has a higher Overall Survival (OS) benefit than docetaxel monotherapy during second-line therapy in patients with KRAS mutations.18 Results of the OS analysis in the OAK study, a randomized, double-blind phase III study, according to KRAS mutation status, suggest that patients with KRAS-mutant NSCLC may also benefit from atezolizumab in terms of OS.19 However, a study showed regardless of the KRAS mutation status, the Progression-Free-Survival (PFS), OS, and objective response rate (ORR) benefits are similar in pembrolizumab combined with platinum-containing chemotherapy.20 In a study of multiple lines of nivolumab in patients with KRAS-mutant NSCLC, response rates were similar regardless of KRAS status.17 These disparities indicate that the impact of KRAS mutation status on the immune response of NSCLC patients remains controversial, and the effect of immunotherapy in KRAS-mutant NSCLC patients needs more detailed research and analysis.
In this study, we explored the impact of KRAS mutation status on the clinical prognosis of NSCLC immunotherapy and inspect the correlation of KRAS mutation subtypes with clinical characteristics, immunotherapy efficacy and prognosis, and determine whether KRAS mutation can act as an independent factor affecting immunotherapy efficacy.
Materials and Method
Patients and Samples
In this retrospective study, from January 2017 to January 2022, we analyzed the NGS results of 930 NSCLC patients who came to Affiliated Cancer Hospital of Xinjiang Medical University. Of these patients, 91 had KRAS mutations. Then we selected patients who had undergone 616 tumor-related gene panel sequencing, first- and second-line treatment, advanced NSCLC, and no targeted therapy for research. The patients who received immunotherapy or immunotherapy combined with chemotherapy were classified into the immunotherapy group. These patients were reviewed for medical records, pathology data, molecular test results, survival, and associated therapy effect assessments. Follow-up was closed on May 31, 2022. All participants signed informed consent to provide medical records and related data for research purposes with ethical standards. This study was approved by the committee of Ethics Committee of Cancer Hospital Affiliated to Xinjiang Medical University, and conducted in accordance with the Declaration of Helsinki principle. The stage was according to the 8th edition tumor, node, and metastasis (TNM) criteria. Histological classification was assessed according to the latest World Health Organization criteria.
Targeted Sequencing and Bioinformatics Analysis
All the samples were performed on NGS test with a pan-cancer panel, which spans 2.2 MB of human genome and consists of all exons and critical introns of 616 cancer-related genes (The list of genes was provided in Table S1). DNA was extracted from tissue and centrifugation of hydrothorax samples using QIAamp DNA FFPE Tissue Kit (Qiagen, Germany), and from peripheral blood samples using QIAamp DNA Blood Mini Kit (Qiagen, Germany). And cfDNA was extracted from plasma using MagMAX™Cell-Free DNA Isolation Kit (Life, USA). DNA concentration was estimated using a Qubit fluorometer and Qubit dsDNA High Sensitivity (HS) Assay Kit (Invitrogen, USA). 50–100ng of sheared genomic DNA was subjected to library construction with an MGIEasy universal DNA library kit (MGI, China), then followed by hybrid capture using an xGen Hybridization and Wash Kit (IDT, USA). The qualified libraries were sequenced with 2×100bp paired-end reads on a MGISEQ-2000 (MGI, China) platform.
The paired-end reads were aligned to human reference genome GRCh37/hg19 using BWA-MEM (v0.7.17). SNVs and InDels were called by VarScan (v 2.4.3) by verified settings. SNVs and InDels from tissue and plasma were filtered by mean depths >800X and 1000X, respectively. At least 5 supporting reads were needed for InDels, while 8 supporting reads were needed for SNVs to be called. CNVs were analyzed with an in-house algorithm based on sequencing depth of coverage data of capture intervals. The minimum threshold of copy number gain or loss was CN >2.75 or CN <1.75 for hotspot genes, and CN >3 or CN <1.5 for others. Gene fusion was analyzed using FACTERA. Tumor mutation burden (TMB) was assessed as described by Chalmers and colleagues.
Statistical Analysis
R software was performed for statistical analyses. Chi-squared test was used to calculate the significance of differences in each cancer type separately. P value were adjusted through Benjamini and Hochberg (BH) procedure to control the false discovery rate (FDR). For correlation analyzing, Chi-squared test and fisher test was used to calculate the significance of differences. The Kaplan–Meier method was used to map disease free survival. P < 0.05 indicated statistical significance.
Results
Clinical Characteristics
After screening, we selected 220 patients who had undergone 616 tumor-related gene panel sequencing, first- and second-line treatment, advanced NSCLC, and no targeted therapy into the study. The cohort average age was 60.8 years. Patients had a median age of 61 years at surgery, ranging from 26 to 83 years. There were 138 (138/220, 62.7%) male and 54 (82/220, 37.3%) female patients. There were 185 (185/220, 84.1%) cases of LUAD and 26 (26/220, 11.8%) cases of LUSC, 9 (9/220, 4.1%) cases of other histology subtypes. There were 40% of patients (88/220) with smoking history. Among all, 32 (14.5%) patients were in stage III and 171 (77.7%) in stage IV. Clinical characteristics of this cohort were summarized in Table 1. The clinical and pathological characteristics of NSCLC patients with KRAS mutation and non-KRAS mutations were compared. The median ages of the KRAS mutation and non-KRAS mutation patients were 63 and 59 years old, respectively. The proportion of male patients was higher in the KRAS mutation group than that in the non-KRAS mutation subgroup (69.6% vs 57.8%). Most of the G12C and non-G12C subtype patients were diagnosed with adenocarcinoma. 51.1% and 32.0% were former or current smokers in KRAS mutation and non-KRAS mutation, respectively. 28.6% of patients in this study cohort received ICIs immunotherapy, and the ratio turned to 26.4% for patients with KRAS mutations and 30.2% for patiensts without KRAS mutations. The main ICIs drugs used were sintilimab (30.2%) and tislelizumab (36.5%), and other drugs including pembrolizumab (14.3%) and carelizumab (12.7%)(Tables 1 and S2).
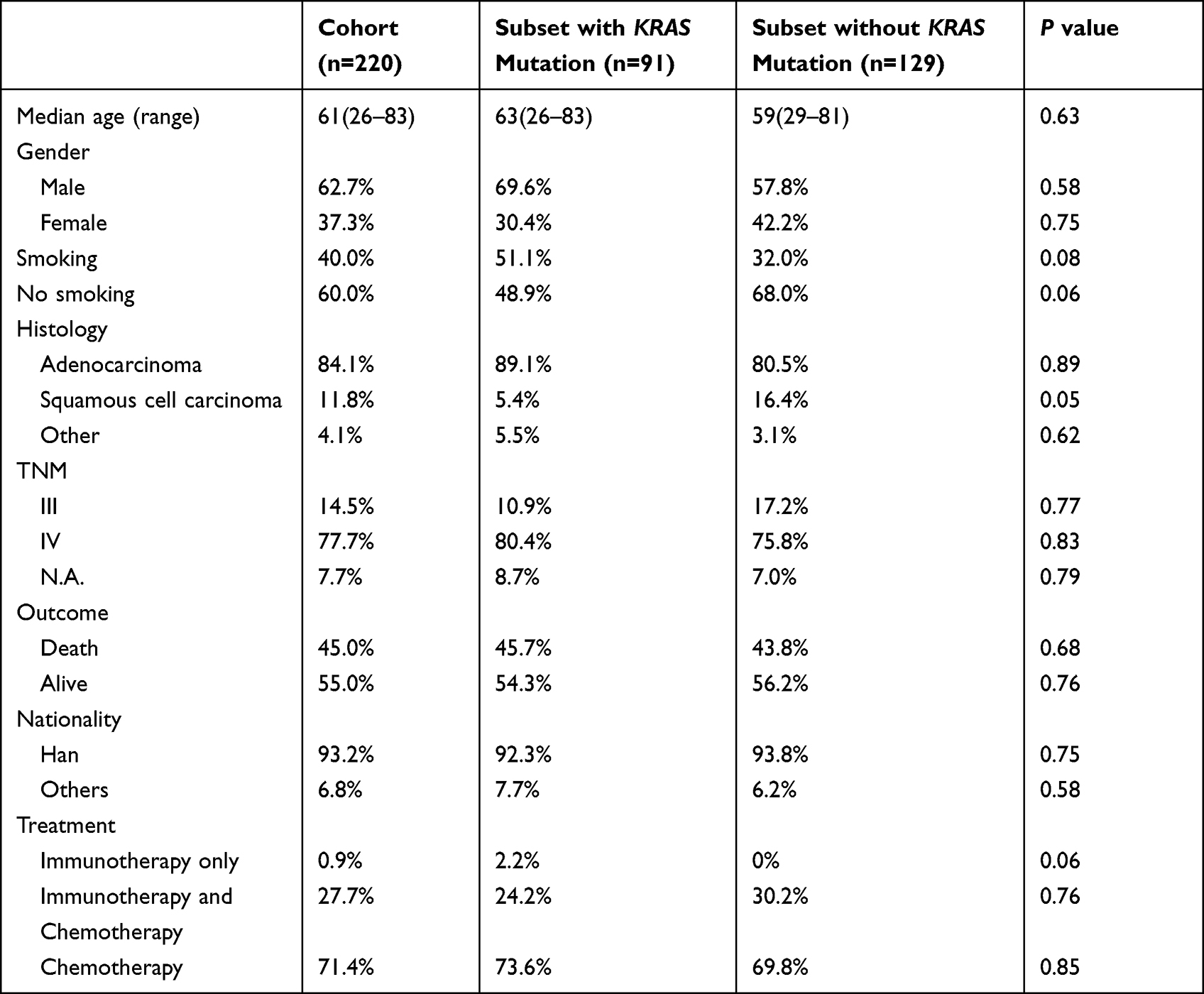 |
Table 1 Summary of Baseline Patient Characteristics |
Sequencing and Variant Detection
In this study, 91 patients had KRAS mutation, accounting for 9.78% of the samples sent for inspection in Affiliated Cancer Hospital of Xinjiang Medical University. We analyzed the sequencing data of the enrolled patients who underwent 616-gene panel sequencing and found that the main mutant subtype of KRAS was G12C, which account for 41.76% (38/91) of the total number of KRAS mutations. The proportions of the other three major KRAS codon 12 subtypes were as follows: G12D, 29.67% (27/91); G12V, 16.48% (15/91); and G12A, 3.3% (3/91) (Figure 1A). Only one KRAS subtype was in per KRAS postive patient, except two patients mutated in two sites.
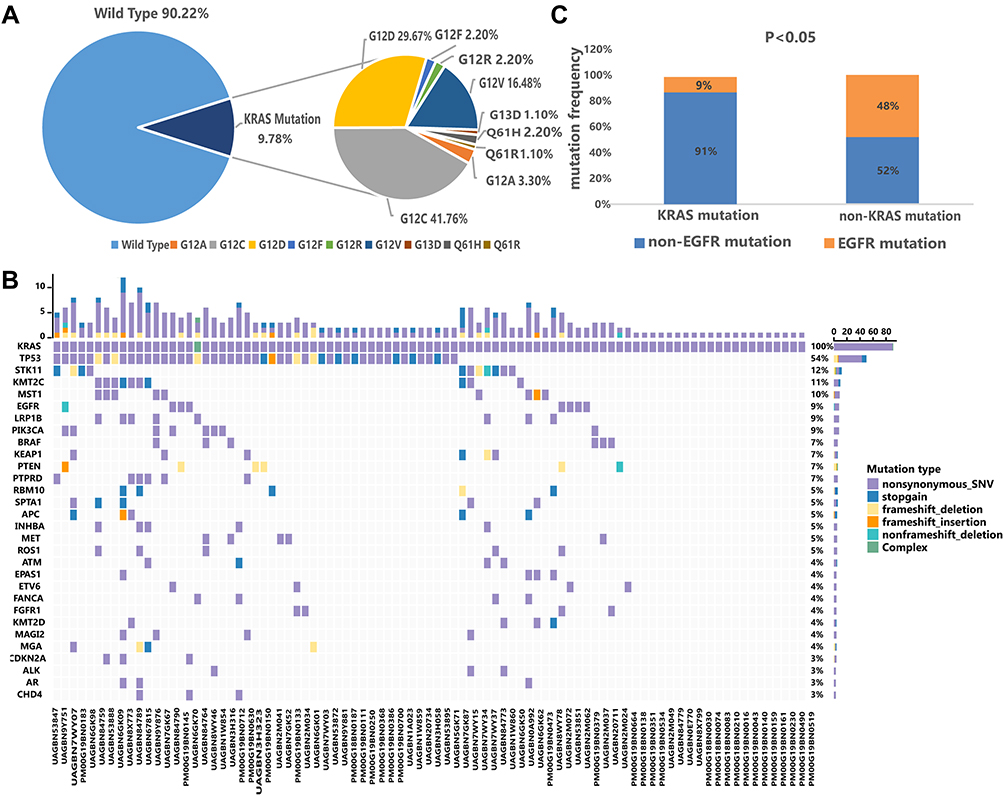 |
Figure 1 The summary of the KRAS mutation. (A) p Pie charts of NSCLC patients with KRAS mutations. Pie charts showing the proportions of KRAS mutation and wildtype tumors (left) and the proportions of different KRAS mutation subtypes (right). (B) Landscape of somatic mutations identified in the 91 NSCLC patients with KRAS mutation, the top 30 genes with mutation frequency are shown on the graph. (C) EGFR mutation statistics between KRAS-mutant patients and non-KRAS-mutant patients. |
In the KRAS mutation group, the top three co-mutant gene were was TP53, STK11 and KMT2C, with mutation frequencies of 54%, 12%, and 11%, respectively. While EGFR mutation frequency was relatively low (9%, Figure 1B). In the non-KRAS mutation group, the top mutation frequency gene was also TP53 with the mutation frequency of 56%, followed by EGFR with the frequency of 48%, and MST1 with the frequency of 27% (Supplementary Figure 1). EGFR mutation frequency is significantly lower in KRAS-mutant patients than in non-KRAS-mutant patients (Figure 1C).
Analysis of PD-L1 Expression and TMB
Tumor PD-L1 protein expression in 220 patients was analyzed. Although PD-L1 expression in KRAS-mutant NSCLC was numerically higher than in non-KRAS-mutant patients, there was no significant difference between the two groups (Figure 2A). We set PD-L1 ≥1% as positive. The positive rate of PD-L1 expression was 39.6% in KRAS-mutant patients and 29.5% in non-KRAS-mutant patients. No significant differences were observed between the KRAS-mutant and non-KRAS-mutant groups. We also found that KRAS-mutant patients had higher TMB values than non-KRAS-mutant patients, The mean TMB of patients with KRAS mutations was 10.2, while the mean TMB of patients with non-KRAS mutations was only 9.5 (Figure 2B).
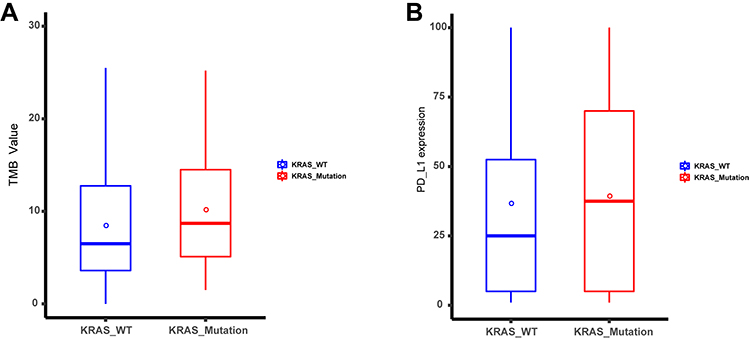 |
Figure 2 The PD-L1 expression and TMB value analysis. (A) Analysis of the difference between the expression of the KRAS mutation group and the non-KRAS mutation group. (B) Analysis of the difference between the TMB value of the KRAS mutation group and the non-KRAS mutation group. |
Patients with KRAS Mutations are More Sensitive to Immunotherapy
Next, we investigated the impact of KRAS mutations on immunotherapy. We found that among patients receiving immunotherapy, KRAS-mutant patients were more sensitive to immunotherapy, with an objective response rate (ORR) of 65% and a disease control rate (DCR) of 80%. While in the non-KRAS mutation group, the ORR and DCR were 37.9% and 82.8%, respectively (Figure 3A and B, Table S2). The ORR of KRAS-mutant patients was significantly higher than that of non-KRAS-mutant patients (P<0.05), suggesting that KRAS-mutant patients are more sensitive to immunotherapy.
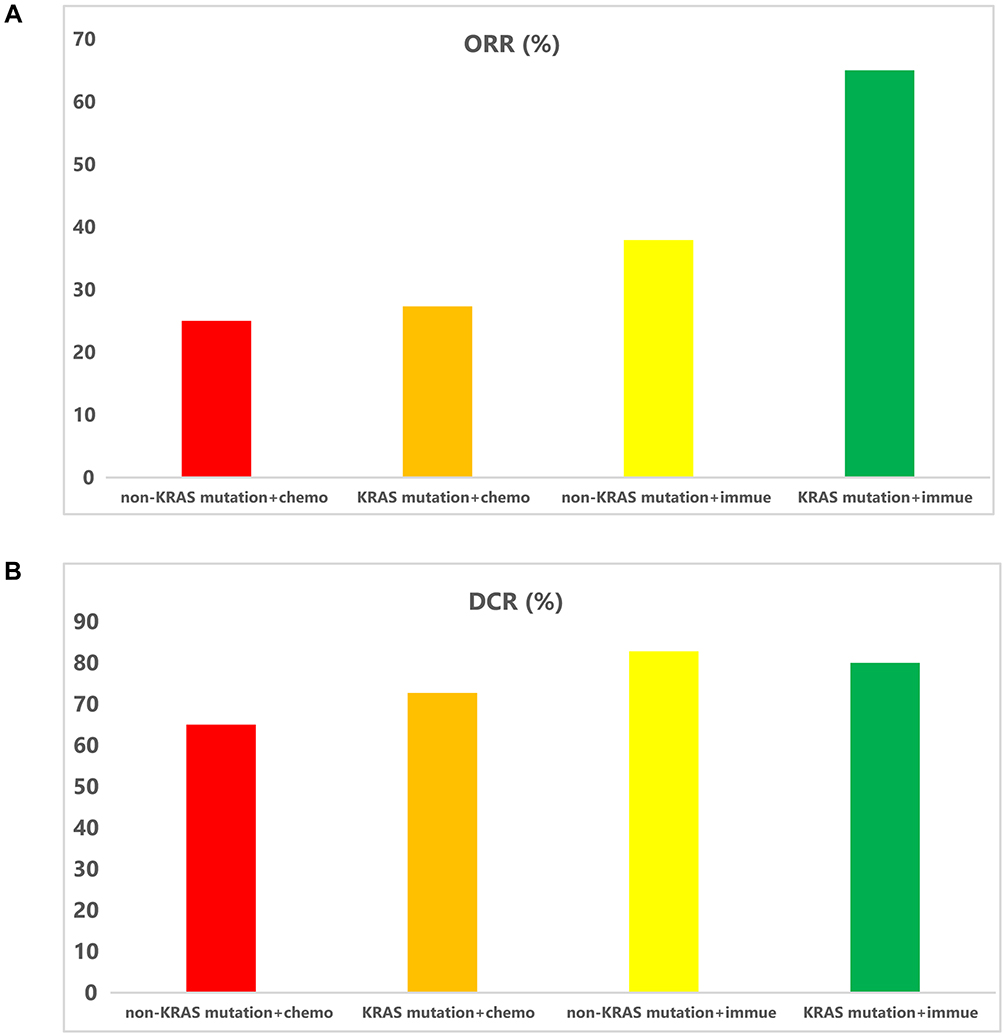 |
Figure 3 Association between KRAS mutation and Immunotherapy. (A) The ORR of different treatments between the KRAS mutation and non-KRAS mutation. (B) The DCR of different treatments between the KRAS mutation and non-KRAS mutation. |
Then, we explored the prognostic value of KRAS mutations. Survival analysis were conducted with the patients who had complete clinical information and follow-up information. In the Kaplan-Meier analysis, we found the results revealed a significant difference in prognosis between the two groups. Patients with KRAS mutations had better prognosis with immunotherapy than the non-KRAS-mutant patients by comparing the overall survival (OS) and progression-free survival (PFS) (Figure 4A and B). The mean duration of PFS was 7.9 months and 3.6 months for KRAS-mutant patients and non-KRAS-mutant patients, respectively (P=0.01) (Figure 4A and Table S3). The median duration of OS was 18.1 months for immunotherapy-treated KRAS-mutant patients and 12.2 months for non-KRAS-mutant patients (P=0.003) (Figure 4B and Table S3).
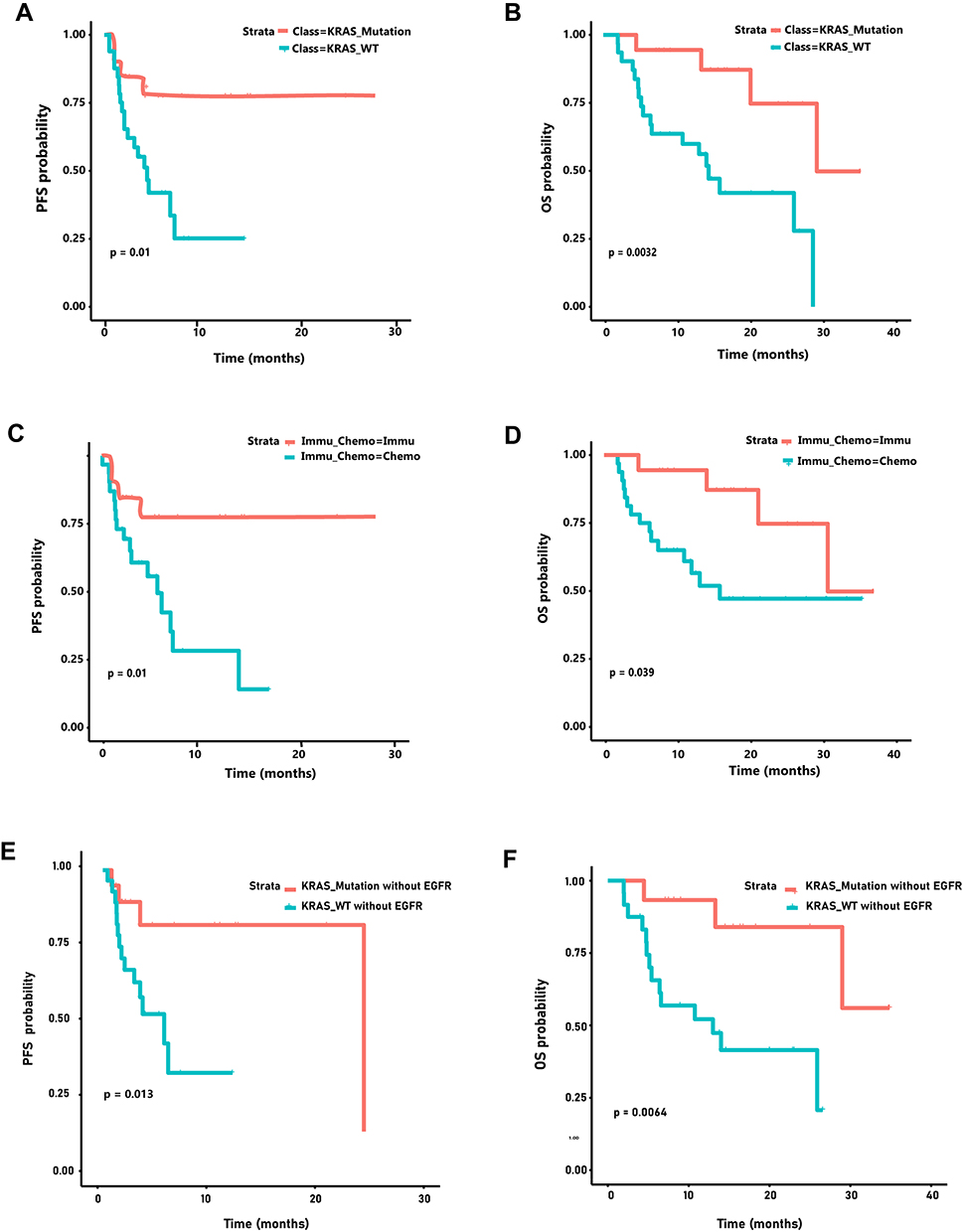 |
Figure 4 The Kaplan-Meier analysis for the prognostic value of KRAS mutations. (A) Kaplan-Meier analyses of the PFS (HR 0.20; 95% CI: 0.019–2.17) between KRAS mutation and non-KRAS mutation group that with immunotherapy. (B) Kaplan-Meier analyses of the OS (HR 0.25; 95% CI: 0.014–4.43) between KRAS mutation and non-KRAS mutation group that with immunotherapy. (C) Kaplan-Meier analyzes PFS (HR 0.25; 95% CI: 0.013–4.17) of immunotherapy and chemotherapy in KRAS mutation patients. (D) Kaplan-Meier analyzes OS (HR 0.22; 95% CI: 0.016–3.17) of immunotherapy and chemotherapy in KRAS mutation patients. (E) At the no-EGFR mutation group, Kaplan-Meier analyses of the PFS between KRAS mutation and non-KRAS mutation group that with immunotherapy. (F) At the no-EGFR mutation group, Kaplan-Meier analyses of the OS between KRAS mutation and non-KRAS mutation group that with immunotherapy. |
Comparative analysis of the prognosis of immunotherapy and chemotherapy in KRAS mutation-positive patients. We found that patients with KRAS mutations had a better prognosis with immunotherapy than with chemotherapy (Figure 4C). The mean survival time were 18.1 months and 12.3 months for the KRAS mutation and non-KRAS mutation patients, respectively (P=0.039) (Figure 4D). The mean duration of PFS for the KRAS mutation group and for the non-KRAS group were 7.9 months and 4.1 months, respectively (P=0.01) (Table S4). It has been reported that EGFR may affect the outcome of immunotherapy, so we studied the effect of KRAS mutation on immunotherapy in patients without EGFR mutation, and found that patients with KRAS mutation had better immunotherapy efficacy, with significant differences in PFS and OS (PFS: P=0.013; OS: P=0.006) (Figure 4E and F).
Prognostic Value of the KRAS G12C and G12D Mutation
Because G12C mutation is the predominant subtype of KRAS mutation, we investigated the effect of G12C mutation on prognosis. Patients with the G12C mutation subtype had better results with immunotherapy than chemotherapy, with the mean PFS and OS of 10.4 months days and 19.3 months for immunotherapy, respectively, compared with 5.9 months and 14.6 months for chemotherapy. Survival with immunotherapy was longer than with chemotherapy, but there was no significant difference in treatment between the two groups (PFS: P=0.055; OS: P=0.26) (Figure 5A and B). When examining the effects of KRAS G12C mutations and non-G12C mutations on immunotherapy, it was found that KRAS mutation subtypes did not affect immunotherapy outcomes (OS: G12C vs non-G12C P=0.85; PFS: G12C vs non-G12C P=0.98) (Figure 5C and D, Table S5). While the G12D mutation may also affect immunotherapy outcomes, so we investigated the effect of G12D mutation and found a significant difference in PFS in immunotherapy outcomes between G12D-mutated and non-G12D-mutated patients (media PFS: G12D-mutated 1.9 months VS non-G12D-mutated 10.2 monthsP=0.007), but not in OS (G12D-mutated 12.9 months VS non-G12D-mutated 17.9 months P=0.29;) (Figure 5E and F).
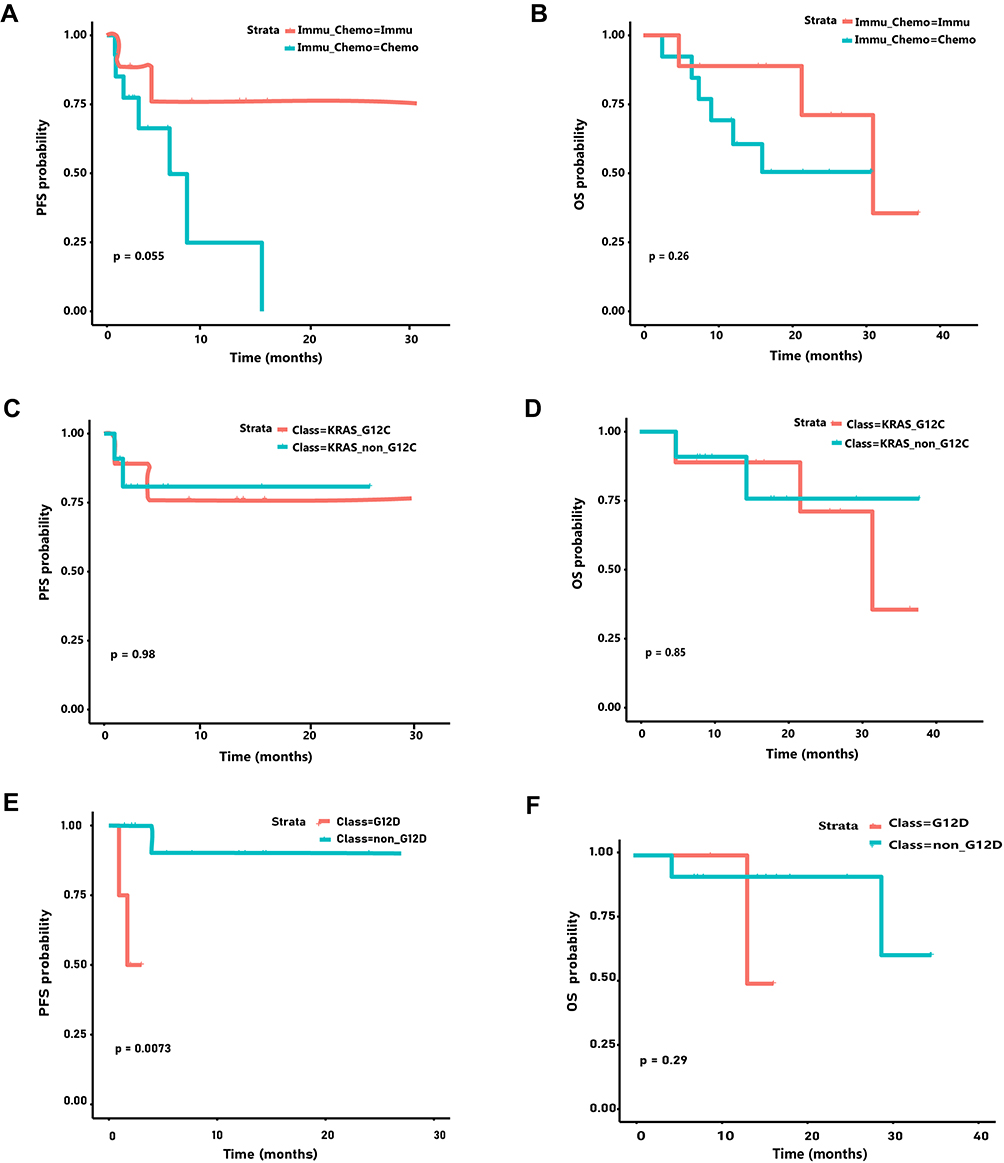 |
Figure 5 The Kaplan-Meier analysis for the prognostic value of KRAS G12C mutations. (A) Kaplan-Meier analyses of the PFS between the immunotherapy and chemotherapy in KRAS G12C mutation patients. (B) Kaplan-Meier analyses of the OS between the immunotherapy and chemotherapy in KRAS G12C mutation patients. (C) Kaplan-Meier analysis of PFS of G12C mutation and non-G12C mutation patients with immunotherapy. (D) Kaplan-Meier analysis of OS of G12C mutation and non-G12C mutation patients with immunotherapy. (E) Kaplan-Meier analysis of PFS of G12D mutation and non-G12D mutation patients with immunotherapy. (F) Kaplan-Meier analysis of OS of G12D mutation and non-G12D mutation patients with immunotherapy. |
The Impact of Co-Mutated Genes on Immunotherapy
We also studied the impact of genes co-mutated with KRAS on immunotherapy, and found that the hotspot mutations associated with KRAS mutations were mainly TP53, STK11 and KMT2C through the gene mutation map. Due to the lack of STK11 survival data, we analyzed TP53 and KMT2C, and found that patients with KRAS mutation had better immunotherapy effect, while patients with TP53 and KRAS co-mutation had the best immunotherapy effect, which was better than KRAS mutation alone (Supplementary Figure 2A and B). Likewise, patients with KRAS and KMT2C co-mutations responded best to immunotherapy, better than those with KRAS mutations alone (Supplementary Figure 2C and D).
Discussion
The treatment of different genetically mutated subgroups of NSCLC has greatly advanced over the past few years but remains to be the leading cause of cancer-related death worldwide.21 As KRAS mutation being one of the common oncogenic factors in NSCLC, in addition to traditional chemotherapy, scientists also maintain the development of variable therapies targeting KRAS mutation.22 However, current studies have shown that compared with KRAS mutation-negative patients, the prognosis and OS of KRAS mutation-positive patients are relatively insufficient,23 and the clinical effects of these treatments need to be further evaluated.
In this study, we investigated the impact of KRAS mutations on immunotherapy, and also explored the role of mutant subtypes on immunotherapy. The impact of KRAS mutation on immunotherapy has been studied from various aspects. By comparing the efficacy of immunotherapy between patients with or without KRAS mutation, the impact of hot spot mutations on immunotherapy, the impact of co-mutation on immunotherapy, etc., the impact of KRAS mutation on immunotherapy was comprehensively analyzed from multiple perspectives.
Immunotherapy has made progress in the treatment of many mutations lead cancer, and currently has become the standard treatment for advanced and difficult to be targeted NSCLC.24 While facing KRAS, the results of subgroup analysis of clinical trials showed that patients with KRAS mutations are more sensitive to PD-1/PD-L1 pathway-related inhibitory therapy, and the prognosis of treatment effect is also better. Compared with single standard chemotherapy, immunotherapy can improve patients’ PFS and OS,15 and this is also shown in our data. In our study, we found KRAS-mutant patients were more sensitive to immunotherapy, with ORR of 65% and disease control rate (DCR) of 80%. It was significantly higher than that of non-KRAS-mutant patients (p<0.05). Besides, the patients with KRAS mutations have better prognosis with immunotherapy through comparing the OS and PFS (Figure 4A and B). We speculated that the better prognosis of immunotherapy in patients with KRAS mutation may be due to the relatively high PD-L1 expression and TMB value in the KRAS mutation population. The correlation between KRAS mutation and PD-L1 and TMB was found, this may be one of the mechanisms by which immunotherapy is effective in KRAS-mutant NSCLC patients. Because PD-L1 and TMB are commonly used as biomarkers for predicting cancer response to immune checkpoint inhibitors.25–27
Several studies have demonstrated the relationship between smoking induction KRAS mutation, and it is believed that smoking leads to higher antigen load, and this is analyzed as a factor of KRAS mutation on the effect of immunotherapy,28 but there were no significant differences shown in our studies (Supplementary Figure 3A and B). Another frequently discussed studied component is the subtype of KRAS classifying by the difference in site of mutations. In our study, the variances in prognosis between mutations at different codons were not significant, but this may be due to the lack of data or populations. The average PFS of KRAS G12C immunotherapy patients in this study was 10.4 months, and the OS was 19.3 months. Currently, studies on KRAS G12C targeted inhibitors are underway, the most famous of which is Sotorasib. The average PFS of patients treated in its Phase II clinical trial was 6.8 months, and the OS was 12.5 months.29 In this study, the effect of immunotherapy is better, but due to fewer patients enrolled in this study, and there is a bias in the statistics. Therefore a larger sample size is needed for subsequent studies. For the KRAS G12D study, Liu et al’s study found that the efficacy of ICI in KRAS-G12D mutant NSCLC was poor.30 This result is also reflected in our results. We also found that the immunotherapy effect of non-KRAS G12D mutant patients better, although there was no significant difference in OS. The impact of mutation sites on different downstream signaling pathways may also lead to a different outcome of overall survival rate.31 Different molecular subtypes of KRAS mutations have different effects on underlying signaling pathways may result in immune evasion or ineffectiveness of immunotherapy.32 At present, research on the treatment of KRAS mutations is still in progress. In most studies, KRAS mutations alone are not considered suitable for analysis as a single factor affecting immunotherapy, but through the detection of KRAS subtypes may still be able to identified as a biomarker to help predict prognosis.14 But these all require the provision of larger cohorts and population to develop research in the future.
In the study of immunotherapy in KRAS-mutant patients, the study of co-mutation is essential. In previous studies, it was found that TP53 co-mutated with KRAS was more sensitive to ICI inhibitors and had better survival, while KRAS and SKT11 co-mutated patients were less sensitive to immunotherapy.33 In our study, we analyzed the immunotherapy susceptibility of patients with KRAS and TP53 co-mutation and KRAS and KMT2C co-mutation, and found that patients with KRAS and TP53 co-mutation were indeed more sensitive to immunotherapy and had a better prognosis than those with KRAS mutation alone and without KRAS mutation. Patients with KRAS and KMT2C co-mutations also showed good sensitivity to immunotherapy, and their treatment outcomes were better than those of patients with KRAS mutations alone and without KRAS mutations. However, due to the lack of clinical information on STK11 patient mutations, resulting in a small number of samples, the study could not be carried out here, and follow-up comparative studies are needed.
There are several limitations in our study: as a retrospective analysis, the provided information included patients from the Affiliated Cancer Hospital of Xinjiang Medical University, and the information contained long time span which might lead to inconsistent treatment plan; while some patients’ immunotherapy regimens included combination chemotherapy as could be a variable factor in our research; the design of the treatment plan and the use of drugs also vary from doctors to doctors, the use of different drugs may also bring some differences. Our findings should be better compared and further analyzed through larger prospective experimental studies.
In this study, the response of KRAS mutation-positive patients to immunotherapy was focused, and the different subtypes and PD-L1 expression of KRAS-mutant NSCLC patients were focused on the outcome of immunotherapy. Based on this result, more conclusively experiments in the future may lead to better outcomes and more clearly define the significance of TMB and PD-L1 expression as predictive biomarkers for immunotherapy, and the further develop of immunotherapy regimens and drug use guidance for KRAS mutations.
Conclusions
Our results suggested that the gene mutation profile of NSCLC in KRAS mutation group and non-KRAS mutation group were different. The patients with KRAS mutation will have better prognosis with immunotherapy. Detection of KRAS mutation in NSCLC patients can better guide immunotherapy.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study have been approved by the Affiliated Cancer Hospital of Xinjiang Medical University, and this study was conducted in accordance with the Declaration of Helsinki. A signed written informed consent was obtained from each patient.
Consent for Publication
Written informed consent for publication was obtained from each participant.
Funding
This work was supported by Department of Science and Technology of Xinjiang Uygur Autonomous Region, 2022D14010, Innovative team of Xinjiang Lung Cancer Immune Response Mechanism and Immunotherapy Advantageous Population Screening and Prognosis Related Research.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. ElOsta B, Behera M, Kim S., et al. Characteristics and Outcomes of Patients With Metastatic Kras-Mutant Lung Adenocarcinomas: the Lung Cancer Mutation Consortium Experience. J Thorac Oncol. 2019;14(5):876–889. doi:10.1016/j.jtho.2019.01.020
2. Jordan EJ, Kim HR, Arcila ME, et al. Prospective comprehensive molecular characterization of lung adenocarcinomas for efficient patient matching to approved and emerging therapies. Cancer Discov. 2017;7(6):596–609. doi:10.1158/2159-8290.CD-16-1337
3. Pylayeva GY, Grabocka E, Bar-Sagi D. RAS oncogenes: weaving a tumorigenic web. Nat Rev Cancer. 2011;11:761–774. doi:10.1038/nrc3106
4. Malumbres M, Barbacid M. RAS oncogenes: the first 30 years. Nat Rev Cancer. 2003;3:459–465. doi:10.1038/nrc1097
5. Dearden S, Stevens J, Wu Y, et al. Mutation incidence and coincidence in non small-cell lung cancer: meta-analyses by ethnicity and Histology (mutmap). Ann Oncol. 2013;24(9):2371–2376. doi:10.1093/annonc/mdt205
6. Sylwia J, Jiří D, Danuta R, et al. Clinical Relevance of KRAS in Human Cancers. Biomed Res Int. 2010;13:150960.
7. Helena AY, Sima CS, Shen R, et al. Prognostic impact of KRAS mutation subtypes in 677 patients with metastatic lung adenocarcinomas. J Thoracic Oncol. 2015;10(3):431–437. doi:10.1097/JTO.0000000000000432
8. Scheffler M, Ihle MA, Hein R, et al. K-ras Mutation Subtypes in NSCLC and Associated Co-occuring Mutations in Other Oncogenic Pathways. J Thorac Oncol. 2019;14(4):606–616. doi:10.1016/j.jtho.2018.12.013
9. Skoulidis F, Byers LA, Diao L, et al. Co-occurring Genomic Alterations Define Major Subsets of KRAS-Mutant Lung Adenocarcinoma with Distinct Biology, Immune Profiles, and Therapeutic VulnerabilitiesCo-occurring Genomic Alterations Define KRAS Subgroups. Cancer Discov. 2015;5(8):860–877. doi:10.1158/2159-8290.CD-14-1236
10. Bruno D, Dowlati A. Immunotherapy in EGFR mutant non-small cell lung cancer: when, who and how? Transl Lung Cancer Res. 2019;8(5):710–714. doi:10.21037/tlcr.2019.06.02
11. Ferrer I, Zugazagoitia J, Herbertz S, et al. KRAS-Mutant non-small cell lung cancer: from biology to therapy. Lung Cancer. 2018;124:53–64. doi:10.1016/j.lungcan.2018.07.013
12. Dong ZY, Zhong WZ, Zhang XC, et al. Potential Predictive Value of TP53 and KRAS Mutation Status for Response to PD-1 Blockade Immunotherapy in Lung Adenocarcinoma. Clin Cancer Res. 2017;23(12):3012–3024. doi:10.1158/1078-0432.CCR-16-2554
13. Arbour KC, Jordan E, Kim HR, et al. Effects of Co-occurring Genomic Alterations on Outcomes in Patients with KRAS-Mutant Non-Small Cell Lung Cancer. Clin Cancer Res. 2018;24(2):334–340. doi:10.1158/1078-0432.CCR-17-1841
14. Lee CK, Man J, Lord S, et al. Clinical and Molecular Characteristics Associated With Survival Among Patients Treated With Checkpoint Inhibitors for Advanced Non-Small Cell Lung Carcinoma: a Systematic Review and Meta-analysis. JAMA Oncol. 2018;4(2):210–216. doi:10.1001/jamaoncol.2017.4427
15. Liu C, Zheng S, Jin R, et al. The superior efficacy of anti-PD-1/PD-L1 immunotherapy in KRAS-mutant non-small cell lung cancer that correlates with an inflammatory phenotype and increased immunogenicity. Cancer Lett. 2020;470:95–105. doi:10.1016/j.canlet.2019.10.027
16. Huynh TG, Morales-Oyarvide V, Campo MJ, et al. Programmed Cell Death Ligand 1 Expression in Resected Lung Adenocarcinomas: association with Immune Microenvironment. J Thorac Oncol. 2016;11(11):1869–1878. doi:10.1016/j.jtho.2016.08.134
17. Passiglia F, Cappuzzo F, Alabiso O, et al. Efficacy of nivolumab in pre-treated non-small-cell lung cancer patients harbouring KRAS mutations. Br J Cancer. 2019;120(1):57–62. doi:10.1038/s41416-018-0234-3
18. Borghaei H, Paz-Ares L, Horn L, et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N Engl J Med. 2015;373(17):1627–1639. doi:10.1056/NEJMoa1507643
19. Rittmeyer A, Barlesi F, Waterkamp D, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a Phase 3, open-label, multicentre randomised controlled trial. Lancet. 2017;389(10066):255–265. doi:10.1016/S0140-6736(16)32517-X
20. Jeanson A, Tomasini P, Souquet-Bressand M, et al. Efficacy of immune checkpoint inhibitors in KRAS-mutant non-small cell lung cancer (NSCLC). J Thoracic Oncol. 2019;14(6):1095–1101. doi:10.1016/j.jtho.2019.01.011
21. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30. doi:10.3322/caac.21332
22. Adderley H, Blackhall FH, Lindsay CR. KRAS-mutant non-small cell lung cancer: converging small molecules and immune checkpoint inhibition. EBioMedicine. 2019;41:711–716. doi:10.1016/j.ebiom.2019.02.049
23. Winder T, Mündlein A, Rhomberg S, et al. Different types of K-Ras mutations are conversely associated with overall survival in patients with colorectal cancer. Oncol Rep. 2009;21(5):1283–1287. doi:10.3892/or_00000352
24. Landre T, Justeau G, Assié JB, et al. Anti-PD-(L) 1 for KRAS-mutant advanced non-small–cell lung cancers: a meta-analysis of randomized–controlled trials. Cancer Immunol Immunother. 2022;71(3):719–726. doi:10.1007/s00262-021-03031-1
25. Chen N, Fang W, Lin Z, et al. KRAS mutation-induced upregulation of PD-L1 mediates immune escape in human lung adenocarcinoma. Cancer Immunol Immunother. 2017;66(9):1175–1187. doi:10.1007/s00262-017-2005-z
26. Rosamaria P, Daniela P, Rosanna L, et al. KRAS-driven lung adenocarcinoma and B cell infiltration: novel insights for immunotherapy. Cancers. 2019;11(8):1145. doi:10.3390/cancers11081145
27. Arbour KC, Jordan E, Kim HR, et al. Effects of Co-occurring Genomic Alterations on Outcomes in Patients with KRAS-Mutant Non–Small Cell Lung CancerCo-occurring Genomic Alterations in KRAS-Mutant NSCLC. Clin Cancer Res. 2018;24(2):334–340.
28. Amanam I, Mambetsariev I, Gupta R, et al. Role of immunotherapy and co-mutations on KRAS-mutant non-small cell lung cancer survival. J Thorac Dis. 2020;12(9):5086. doi:10.21037/jtd.2020.04.18
29. Skoulidis F, Li BT, Dy GK, et al. Sotorasib for Lung Cancers with KRAS p.G12C Mutation. N Eng J Med. 2021;384(25):2371–2381. doi:10.1056/NEJMoa2103695
30. Liu C, Zheng S, Wang Z, et al. KRAS -G12D mutation drives immune suppression and the primary resistance of anti-PD-1/PD-L1 immunotherapy in non-small cell lung cancer. Cancer Commun. 2022;42(9):828–847. doi:10.1002/cac2.12327
31. Cai D, Hu C, Li L, et al. The prevalence and prognostic value of KRAS co‐mutation subtypes in Chinese advanced non‐small cell lung cancer patients. Cancer Med. 2020;9(1):84–93. doi:10.1002/cam4.2682
32. Ihle NT, Byers LA, Kim ES, et al. Effect of KRAS oncogene substitutions on protein behavior: implications for signaling and clinical outcome. J Natl Cancer Inst. 2012;104(3):228–239. doi:10.1093/jnci/djr523
33. Skoulidis F, Goldberg ME, Greenawalt DM, et al. STK11/LKB1 Mutations and PD-1 Inhibitor Resistance in KRAS -Mutant Lung Adenocarcinoma. Cancer Discov. 2018;8(7):822–835. doi:10.1158/2159-8290.CD-18-0099
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.