Back to Journals » International Journal of General Medicine » Volume 14
Modern Contraceptive Use and Associated Factors During Extended Postpartum Period Among Women Who Gave Birth in the Last 12 Months at Northwest Ethiopia
Authors Getaneh M, Jara D, Alle A ![]() , Arora A, Tsegaye TB
, Arora A, Tsegaye TB ![]() , Birhanu MY
, Birhanu MY ![]()
Received 4 May 2021
Accepted for publication 21 June 2021
Published 12 July 2021 Volume 2021:14 Pages 3313—3325
DOI https://doi.org/10.2147/IJGM.S317649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mekonnen Getaneh,1 Dube Jara,2 Atsede Alle,2 Amit Arora,3 Tesfa Birlew Tsegaye,2 Molla Yigzaw Birhanu2
1Department of Midwifery, Medicine and Health Science College, Wolkite University, Wolkite, Ethiopia; 2Department of Public Health, Medicine and Health Science College, Debre Markos University, Debre Markos, Ethiopia; 3School of Health Sciences, Western Sydney University, Penrith, NSW, 2751, Australia
Correspondence: Molla Yigzaw Birhanu; Tesfa Birlew Tsegaye
Department of Public Health, Medicine and Health Science College, Debre Markos University, Debre Markos, Ethiopia
Tel +251910614947
; +251913310476
Email [email protected]; [email protected]
Background: The extended postpartum period is a one-year follow-up period after giving birth, and it is critical for women to prevent unintended pregnancy and reduce the risk of maternal and child mortality by ensuring safe birth intervals. Many women, however, are unaware that they are at risk for pregnancy throughout this period. Hence, the aim of this study was to assess the utilization and associated factors of modern contraceptives during extended postpartum family planning (EPPP) in northwest Ethiopia.
Methods: A community-based cross-sectional study design was conducted using 630 samples from October 01 to October 30, 2020, in northwest Ethiopia. The study participants were drawn through a multistage sampling technique and data were collected using structured questionnaires via interview. The collected data were entered into EpiData version 4.2 and exported into SPSS version 25.0 for management and further analysis. A bivariable logistic regression model was used to identify variables having an association with the outcome variable. In bivariable analysis, variables having P ≤ 0.25 were selected and entered into multivariable logistic regression analysis. Finally, in multivariable analysis, variables having P ≤ 0.05 with a 95% CI were declared as significantly associated with the outcome variable.
Results: About 60.6% of women were using modern contraceptive during extended postpartum period. Mothers to partner discussion (AOR= 7.6, 95% CI: 4.20– 14.05), secondary educational status (AOR= 3.8, 95% CI: 1.36– 10.93), college and above educational status (AOR= 7, 95% CI: 1.92– 25.57), menstrual resumption (AOR= 9.2, 95% CI: 5.66– 15.12), sex resumed (AOR=8.5, 95% CI: 2.19– 33.58), fertility desire (AOR= 3.9, 95% CI: 1.99– 6.15), linkage to FP during child immunization (AOR= 2.7, 95% CI: 1.67– 4.50), and FP counseling during pregnancy (AOR=2, 95% CI: 1.25– 3.34) were significantly associated with outcome variable.
Conclusion: Associating factors were identified as partner discussion, education, menstrual resumption, fertility desire, sexual resumption, FP counseling, and FP during child immunization. Improving mothers’ education and informing couples about the dangers of becoming pregnant before menstruation are critical.
Keywords: postpartum, modern contraceptive, utilization, reproductive age, Ethiopia
Background
Postpartum family planning (PFP) is a means of preventing unintended pregnancy and closely spaced pregnancies for one year following childbirth.1 The World Health Organization (WHO) recommends that after giving birth, a woman stay for at least two years before having another child to avoid the risks of maternal, prenatal, and infant health.2
According to the Global Burden of Disease study, there are 265 million unwanted pregnancies, 110 million unnecessary abortions, 590,000 avoidable maternal deaths, and 8 million preventable infant deaths worldwide, with developing countries accounting for 99% of maternal deaths.3,4 Women account for 69% of the unmet need for modern contraception in three regions (Sub-Saharan Africa (SSA), South Central Asia, and South East Asia), with 49 million unintended pregnancies accounting for 21 and 15 million induced abortions and the loss of healthy years of women’s lives, respectively.5
The total contraceptive prevalence rate (CPR) for currently married women aged 15–49 years in Ethiopia is 42% (41% using modern methods and 1% using traditional methods).6 Although the recommended time for initiation of contraceptives in the postpartum period is 6 weeks after delivery, most women do not receive contraceptives as recommended.7
Most women start sexual activity without using contraceptive methods, although more than 90% of them want to postpone a future pregnancy in the first year of postpartum period.1 As a result of low use of modern contraceptives, high rates of unintended pregnancies, unsafe abortions and unplanned births occur in the SSA.8 The risk of low birth weight is doubled if pregnancy occurs less than six months after previous delivery and children who are born less than two years previous birth.9
Shorter birth intervals are associated with an increased risk of negative maternal, perinatal, infant, and child health outcomes, which can prevent approximately 33% and 10% of maternal and under-five child deaths, respectively.10–12 FP improves the health and social outcomes of women and families, as well as the environmental benefits at different levels.13
Maternal mortality related to pregnancy and child birth complications in Ethiopia is the highest among SSA countries and it represents about 412 per 100,000 live births.7 The unmet need for postpartum family planning in Ethiopia is still high, ranging from 86% in the first 5 months to 76% by the end of the first year after delivery and 81% of women do not use PPFP due to not realizing they could get pregnant one year after delivery.14,15
Resumption of menses, limited knowledge of available choices, confusion when fertility comes back and unpredictability of the timing of the onset of intercourse, and not discussing family planning methods with partners, were the factors identified by previous studies.16,17
Improving contraceptive counseling efforts may be one strategy to prevent adverse pregnancy outcomes and unsafe abortion among young women, reduce risks of maternal mortality, and promote achieving reproductive rights.18 So, to enhance postpartum utilization of contraceptives, health education at home or community level, counseling, provision of the full range of family planning methods and treatment of medical conditions and side effects should be considered.19 The introduction of modern contraceptives during the postpartum period is very crucial, yet less emphasis is given on the first year after birth. Therefore, this study aimed to assess extended postpartum period modern contraceptive methods’ utilization and identify the factors affecting their utilization.
Materials and Methods
Study Design, Area and Period
A community-based cross-sectional study was conducted from October 01, 2020, to October 30, 2020, in Goncha Siso Enese, which is one of the districts in the Amhara Regional State of Ethiopia. The district is located 335 kms from Addis Ababa, the capital city of Ethiopia, 154 kms from Bahir Dar, the capital city of Amhara regional state, and 159 kms from Debre Markos, the administrative city of the East Gojjam Zone. The current total population of Goncha Siso Enese District is 211,894, of which 106,159 are women of reproductive age, and estimated live births are 5007 (23.6%) and 7141 (3.37%) respectively. There are 8 health centers, 8 private clinics, and 5 pharmacies providing maternal and other health services to the population.
Populations
All reproductive age (18–49) women who gave birth in the previous year were the source population, and all reproductive age women who gave birth in the previous year and lived in randomly selected Kebeles in the district were the study population.
Sample Size Determination and Sampling Procedures
A single population proportion formula was used to get the minimum required sample size using the following assumption and information: 95% CI, 5% margin of error, and prevalence of EPPP modern contraceptive (P=46.7%),20 1.5 design effect,21,22 and adding 10% non-response rate, was calculated and the final sample size for this study was 630.
Of the total of 43 (Rural 41, Urban 2) Kebeles in the district, 13 Kebeles (12 rural, 1 urban Kebeles) were selected through a lottery and a simple random sampling method. The study participants were drawn via a multistage sampling technique. Health extension workers in each country compiled a list of mothers who gave birth in the previous 12 months. Before data collection, the sampling frame was designed by numbering the list of households using the registration book. When there are two or more eligible women in the same household, the lottery method is used to select one of them, and if the selected postpartum woman is absent at the time of data collection, the data collector is returned the following time. When the interviewer was unable to find the woman for a second time, the next postpartum woman was included in the study (Figures 1 and 2).
 |
Figure 1 Conceptual framework for study done on EPPP modern contraceptive utilization and its associated factors among reproductive age women in Goncha Siso Enesie district, East Gojjam Zone, Ethiopia, 2020. |
 |
Figure 2 Schematic representation of the sampling procedure among extended postpartum women in Goncha Siso Enesie district, East Gojjam Zone, Ethiopia, 2020 (“K” stands for kebele). |
Variables
Dependent Variables
Extended postpartum period modern contraceptive utilization.
Independent Variables
Age, educational status, marital status, religion, occupation, income, and discussion with husband are socio-demographic characteristics. Contact with health care professionals (ANC, FP counseling during pregnancy, PNC, place of delivery, link to family planning during child immunization); knowledge of FP (awareness of contraceptive use after birth, source of knowledge, source of FP, benefit of FP); and reproductive health-related characteristics (sexual resumption, menstrual resumption, fertility desire, time of starting a postpartum period, time of starting a postpartum period, time of starting a postpartum contraceptive).
Operational Definitions
Extended Postpartum Modern Contraceptive Utilization
When a postpartum woman’s currently use of any modern contraception methods (pill, IUD, injectable, condom (male or female), sterilization (male or female), implants during the 12 months following her most recent childbirth.23
Extended Postpartum Period
The 12 month period after a live birth.23
Menstrual Resumption
Women who started to see menstruation after birth during data collection time within one year.15
Knowledge of Family Planning
A women was considered as “knowledgeable about family planning by using 10 question, if a respondent answered mean score and above from knowledge-related questions” and “below mean score had poor knowledge”.24
Modern Contraceptive
It includes male and female sterilization, intrauterine devices (IUCDs), implants, injections, pills, emergency contraception, vaginal barriers, and mechanical male and female condoms.
Traditional Contraceptive (Natural Methods)
It includes withdrawal, rhythm (periodic abstinence), and the lactational amenorrhea method (LAM).
Data Collection Tools and Procedure and Quality Control
The data were collected using a pre-tested structured questionnaire via face-to-face interviewer administration. To maintain consistency, the questionnaire was prepared first in the English language and translated to Amharic (local language translated back to English by language experts.
About eight diploma clinical nurses women and two public health officers were recruited as data collectors and supervisors respectively. To keep data quality, one-day training was given to the data collectors and supervisors on the objective, confidentiality of information, respondent rights, and the techniques of interview, and close supervision of the data collectors and pre-tested was made. The collected data was checked for completeness and consistency by the principal investigator to ensure the quality of the data every day.
Data Management and Analysis
The collected data was entered into the computer software EpiData version 4.2 by the principal investigator, then exported to SPSS version 25.0 for further management and analysis. To describe the study population in relation to the relevant variables, descriptive statistics such as frequencies, percentages, meaning, and standard deviation were computed based on the distribution and nature of the variables. Bivariable and multivariable logistic analysis was executed to identify associated factors with EPPP modern contraceptive utilization. In bivariable analysis, variables having p < 0.25 were recruited as candidates for multivariable analysis. In multivariable logistic analysis, variables having P < 0.05 were declared as significantly associated with modern contraceptive utilization during the extended postpartum period.
Results
Sociodemographic Characteristics of the Study Population
The response rate for this study was 98.2%. The mean age of the respondents was 30.28 years (± 5.82 SD) with an 18–49 range of years. One-third of those polled (18.2%) were between the ages of 25 and 29. When it comes to ethnicity, they all belong to the Amhara ethnic group and are Orthodox Christians. About 580 (993.7%) were married, and 545 (8.88%) were housewives. Regarding their educational status, 246 (39.7%) of them had no formal education. Only about 450 (72.7%) had conversations with their husbands, and only 36 (5.8%) worked for the government (Table 1).
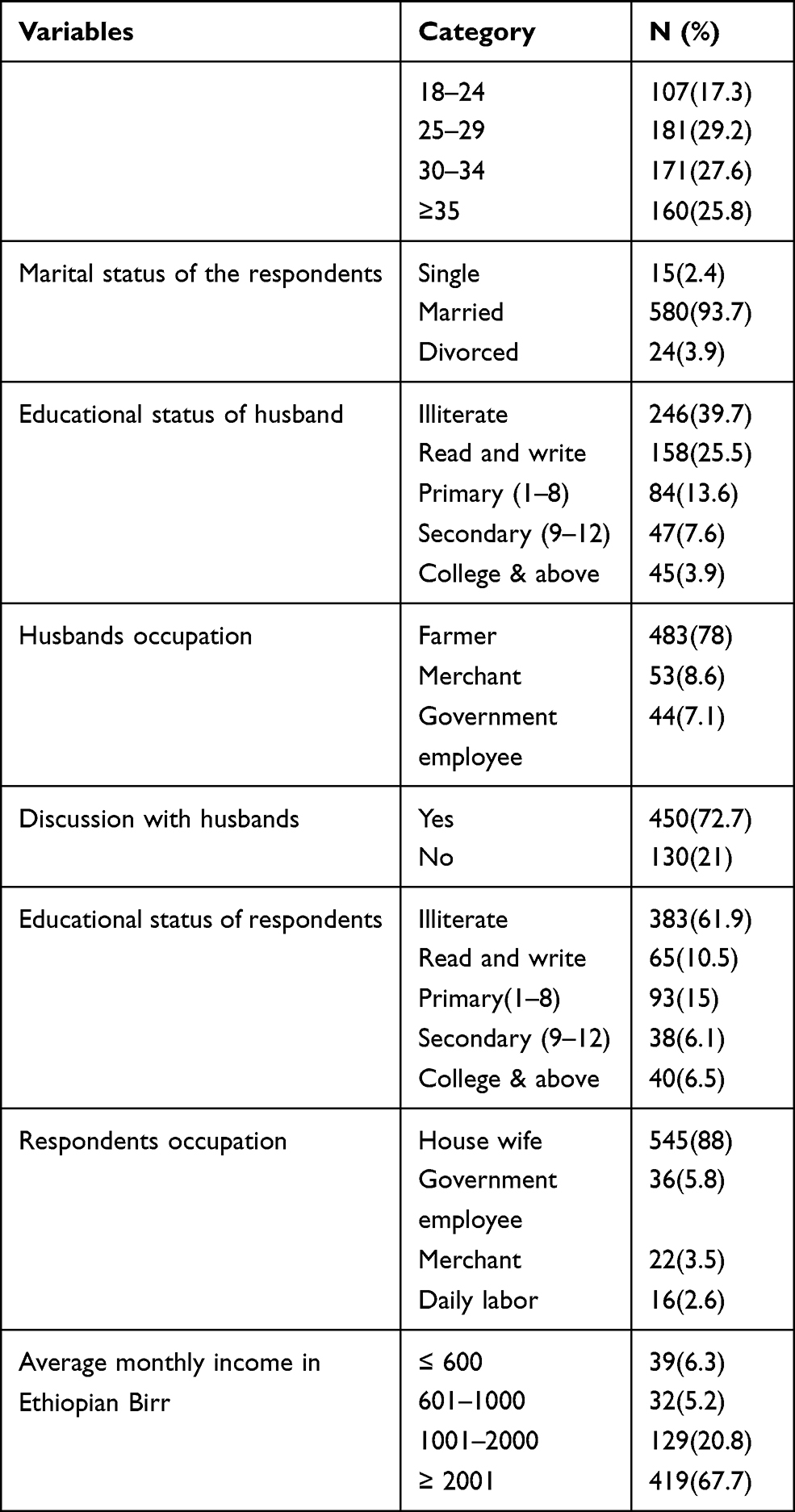 |
Table 1 Socio-Demographic Characteristics of Women in the Extended Postpartum Period in Goncha Siso Enese District, Ethiopia, 2020 (N= 619) |
Reproduction Preference and Characteristics of Study Population
The majority of 537 (86.8%) respondents said their recent pregnancy was planned, 307 (49.6%) said they wanted to have their next child in two years, and 94 (15.2%) said they did not want to have any more children. On the other hand, 353 (57%) of the respondents’ menstruation had returned and 574 (92.7%) of those had resumed sex after delivery (Table 2).
 |
Table 2 Reproductive History and Preference of Women in Goncha Siso Enese District, Ethiopia, 2020 |
Contraceptive Use During the Extended Postpartum Period
In this study, 375 (60.6%; 95% CI: 57–64%) of women used contraceptive methods in the extended postpartum period. Among those who used a contraceptive method, 292 (47.2%) began using it >3 months after childbirth, while 83 (22.1%) began using it after 3 months of childbirth. Within one year of delivery, the most commonly used methods were injectables (329) and implants (36) (0.8%). The majority of methods were obtained from the government health institute (366 (59.1%) and a private clinic (9 [1.5%]) (Figure 3). The main reason for non-use of contraceptive method in the EPPP was feeling not susceptible to pregnancy 107 (17.3%) followed by feeling of not at risk due to amenorrhea 90 (14.5%), pregnancy due to breast feeding 28 (4.5%), fear of side effect 19[3.1%)] (Figure 4).
 |
Figure 3 The most commonly used modern contraceptive methods in the EPPP, in Goncha Siso Enesie district, East Gojjam Zone, Ethiopia, 2020. |
 |
Figure 4 Reasons for modern contraceptive non-use in the EPPP, in Goncha Siso Enesie district, East Gojjam Zone, Ethiopia, 2020. |
Postpartum Women Knowledge on Contraceptive Methods
About 481 (77.7%) of the study participants had good knowledge. Whereas, 138 (22.3%) of the respondents had poor knowledge on postpartum contraceptive utilizations (Table 3).
 |
Table 3 Knowledge About Modern Contraceptive Among Extended Postpartum Women in Goncha Siso Enese District, Ethiopia, 2020 |
Having Information About Postpartum Women on Contraceptive Methods
Among all women, five hundred eighty two (94%) of the respondents had information about modern contraceptive methods and knew at least one modern contraceptive method. Among those women, the main source of information about the contraceptive method was from health extension workers. The majority of respondents knew about modern contraceptive methods, with 551 (89%) knowing about injectable methods and 236 [38.1%] knowing about implants (Table 4).
 |
Table 4 Having Information About Modern Contraceptive Among Extended Postpartum Women in Goncha Siso Enesie District, Ethiopia, 2020 |
Contact with Health Care Professionals During Maternal and Child Health Care Services
Only 343 (55.4%) and 344 (55.6%) received family planning counseling during antenatal care and delivery, respectively, out of 599 (96.8%) who had an antenatal care check up in their previous pregnancy. Regarding the place of delivery for the last birth of respondents, 97 (15.7%) gave birth in government hospitals, 438 (70.8%) gave birth in government health centers, and 84 (13.6%) were at home. Doctors, midwives, nurses, untrained traditional birth attendants, and trained traditional birth attendants assisted the majority of deliveries, assisting 94 (15.2%), 441 (71.2%), 69 (11.1%), and 15 (2.4%) of the women, respectively. Sixty six (10.7%) were waiting in the maternity waiting room and among these 41 women counseling about modern contraceptive use. Postnatal care was received by 481 (777.1%) of the respondents. Only 463 (774%.8%) of women who had a postnatal checkup received family planning counseling. The majority of women, 590 (953%), visit health institutes to get vaccines for their children, while 321 [1.9%] have been linked to the EPPP service by health (Table 5).
 |
Table 5 Contact with Health Care Professionals Among Postpartum Women in Goncha Siso Enese District, Ethiopia, 2020 |
Factors Associated with EPPP Modern Contraceptive FP Method Utilization
About 15 variables with a p-value of ≤ 0.25 were included in the multivariable logistic regression. In multivariable logistic analysis, discussion with the husband, educational status of respondents, fertility desire, resumption of menses, sexual resumption, FP counseling at ANC, and getting linkage to FP during child immunization were significantly associated with EPPP modern FP utilization at p < 0.05 (Table 6).
 |
Table 6 Factor Associated with Extended Postpartum Modern Contraceptive Use, in Goncha Siso Enese District, Ethiopia, 2020 |
Women who had discussions about modern contraceptives with their husbands were 7.6 times (AOR = 7.65, 95% CI: 4.20–14.05) more likely to use modern contraceptive methods in the extended postpartum period compared to their counterparts. The odds of using modern contraceptive methods in the EPPP among women with secondary educational status were 3.8 times (AOR = 3.85, 95% CI: 1.36–10.93) more likely than for women whose educational status was college level and above.
Women who resumed menstruation after birth were 9.2 times more likely to use contraception in the EPPP than those who were amenorrheic in the postpartum period (AOR = 9.25, 95% CI: 5.66–15.12). The odds of using modern contraceptives among women who had resumed sexual activity were 8.5 times (AOR = 8.57, 95% CI: 2.19–33.58) more likely than for those who had not resumed sexual activity after birth. Women who have not decided when to have children 3.4 times (AOR 3.49, 95% CI: 1.99, more likely to use during EPPP compared to those who had desire to have children after two. Women who received FP counseling during their ANC visit were twice as likely (AOR = 2.04, 95% CI: 1.25–3.34) to use contraception in the EPPP as their counterparts.
Women who had linked to FP service by health professional during child immunization visit were 2.7 times [AOR 2.74, 95% CI; 1.67–4.50] more likely during postpartum period compared to those who not linked (Table 6).
Discussion
One of the interventions for reducing maternal and child morbidity and mortality is postpartum modern contraception. In developing countries such as Ethiopia, women in the postpartum period do not have access to services that address their desire to delay childbirth and avoid an unintended pregnancy and its consequences.
The magnitude of postpartum modern contraceptive use was 375 (60.6%, 95% CI: 57–64%) in this study. The result of this study is in line with the study done in Debre Tabor town (63%) and Injibara town (58.5%),7,25 and the finding is lower than study done in Kenya 86.3%,26 Addis Ababa (80.3%) and Hosanna town (72.9%),27,28 This discrepancy might be due to the socio-demographic characteristics of the respondents. That means there is higher health service coverage in Addis Ababa and Hosanna town than in the Goncha Siso Enese district. And the findings of this study are far superior to those of a study conducted in Parakou, a city in Northern Benin 13%,29 Somalia region Kebribeyah town, 12.3%,30 Dello Mena district 14.3%,22 East Gojjam zone, Gozamen district 46.7%.20 The discrepancy could be due to the time gap between the studies and the presence of some dissimilar sociodemographic and reproductive characteristics among the participants. According to the literature, discussion with partners about modern contraceptive use was lower (50.3%) in Parakou, a city in Northern Benin, than in this study.29 Other possible causes of religion in the Somalia region, Muslims in Kebribeyah town and Dello Mena district, were higher (91.7%, 89.7%) than those in this study.22,30 However, all of the respondents in this study were Orthodox. The other possible reason for the difference might be the difference in the educational level of the study participants. In the study conducted in the Gozamen district, the proportion of women who were illiterate was higher (67.3%) than that of this study (39.7%).20 The most frequently utilized modern contraceptive methods were injectable followed by implant.
Mothers’ educational status was found to have a significant association with postpartum contraceptive use in a multivariable analysis. This might be due to the fact that educated women have a better understanding of the benefits of contraception and the risks of a short interval of pregnancy. As a result, they have a better understanding of visiting health facilities and receiving services than those with no formal education or who are illiterate. The findings of this study are consistent with those of previous studies conducted in Bangladesh, Axum, and Injibara.7,23,31 Having discussion about modern FP methods with partner was significantly associated with postpartum modern contraceptive use. This is supported by reports from Urban Ghana,32 Kebri Beyah Ethiopia.30 This might be due to women who discuss modern FP with their partners, who are more likely to get acceptance and support. Resumption of menstruation was found to be significantly related to postpartum family planning. This could be due to mothers’ perceptions that once menstruation has resumed, the risk of pregnancy increases, motivating them to use contraceptive methods. This is in line with the studies conducted in Aksum town,23 and Gozamen District.20
Resumed sexual activity is one variable that showed statistically significant association with postpartum contraceptive use. This might be due to the fact that women who resume sexual activity have a fear of getting pregnant. As a result, they seek contraception more than those who have not resumed sex. This finding is consistent with study done in Urban Ghana,32 Hosanna town,27 Aksum town.23 Fertility desire is another variable which is positively associated with modern contraceptive use during the extended postpartum period. This finding is consistent with the findings of a study conducted in rural Ghana, which found that women with a high parity may be satisfied with the number and sex of their children and may wish to limit their births.33
This study also showed that family planning counseling during antenatal care was associated with modern contraceptive use during the extended postpartum period. Women who had received family planning counseling during the ANC had approximately 2 times higher odds of using modern contraceptives in the extended postpartum period than their counterparts. This may be because women who receive family planning counseling during the ANC might be highly motivated to use modern contraceptive methods. This finding is in line with study done Kebribeyah town, Somali region,30 Aksum,23 and Gondar city.34 The possible reason for this may be that counseling during ANC would create an opportunity for women to have more exposure to information and awareness regarding birth spacing by the use of contraceptives after giving each birth.
In this study, 52% of women had linkage to family planning service by professionals while coming to health institute for child immunization service. Those who were linked have higher odds of using postpartum contraceptives. This could be explained by the fact that the recommended infant vaccination schedule allows multiple health care contacts with women during the first year of life, so this makes it easy to screen women who do not use family planning and to link them to an FP clinic. This finding is supported by another study reported in Butajira,15 as a result, child immunization has a significant association with the use of postpartum contraception.
Conclusions
This study showed a high prevalence of postpartum modern contraceptive use in the Goncha Siso Enese district. Injectables and implants are the most commonly used methods during the postpartum period. Discussion with the husband, the educational status of the respondent, menstrual resumption, sexual resumption, fertility desire, FP counseling during ANC, linkage to FP during child immunization, were positively associated factors with postpartum contraceptive use. Improving women’s education in collaboration with various stakeholders, as it is critical to increasing access to postpartum family planning. Health providers must put great emphasis on transferring messages during maternal health care services about postpartum contraceptive use and should better strengthen intensive counseling on postpartum contraceptive use.
Abbreviations
ANC, antenatal care; AOR, adjusted odds ratio; COC, Combined Oral Contraceptive; CPR, contraceptive prevalence rate; DHS, Demographic Health Survey; EDHS, Ethiopian Demographic and Health Survey; EPPP, extended postpartum period; FP, family planning; HDSS, Health and Demographic Surveillance Site; HEW, health extension workers; IUCD, Intra Uterine Contraceptive Device; MNCH, Maternal, Newborn, and Child Health; MNH, Maternal and New born Health; OR, odds ratio; PNC, postnatal care; POP, Progesterone Only Pills; PPC, postpartum contraceptive; PPFP, postpartum family planning; WHO, World Health Organization.
Data Sharing Statement
The data sets generated during this study are available from the correspondences on reasonable request.
Ethical Consideration
Ethical clearance was obtained from the ethical review committee of the Debre Markos University institutional review board (IRB). An official letter was written from DMU to Goncha Siso Enese district Health office to get ethical clearance and a supportive letter to the selected Kebeles’ administration to get permission. During data collection, informed written consent was obtained from all women aged over 18 years. The information about the study participants was not disclosed to anyone other than the principal investigators in order to maintain their confidentiality. Generally, this study was conducted in accordance with the World Medical Association Declaration of Helsinki.
Acknowledgments
We are grateful to Debre Markos University, College of Medicine and Health Sciences for providing ethical clearance for this study. We would like to extend our thanks to Goncha Siso Enese District Health Office staffs, study participants, supervisors and data collectors for active participation and timely engaged data collection period.
Author Contributions
All authors made a significant contribution in the conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting, and gave final approval of the version to be published, and have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Also, there is no funding support for publication in a journal.
Disclosure
The authors have declared that no conflicting interests exist.
References
1. World Health Organization. Programming Strategies for Postpartum Family Planning. 2013.
2. Gaffield ME, Egan S, Temmerman M. It’s about time: WHO and partners release programming strategies for postpartum family planning. Glob Health Sci Pract. 2014;2(1):4–9.
3. Kassebaum NJ, Bertozzi-Villa A, Coggeshall MS, et al. Global, regional, and national levels and causes of maternal mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9947):980–1004. doi:10.1016/S0140-6736(14)60696-6
4. Cousens S, Blencowe H, Stanton C, et al. National, regional, and worldwide estimates of stillbirth rates in 2009 with trends since 1995: a systematic analysis. Lancet. 2011;377(9774):1319–1330. doi:10.1016/S0140-6736(10)62310-0
5. Darroch JE, Sedgh G, Ball H. Contraceptive Technologies: Responding to Women’s Needs. Vol. 201. New York: Guttmacher Institute; 2011:1–52.
6. EPHI I. Ethiopia Mini Demographic and Health Survey 2019: Key Indicators. Rockville, Maryland, USA: EPHI and ICF; 2019.
7. Belete GA, Getu AA, Belay G. Utilization and Associated Factors of Modern Contraceptives During Postpartum Period Among Women Who Gave Birth in the Last 12 Months in Injibara Town Awi Zone, North-West Ethiopia. 2019.
8. Apanga PA, Adam MA. Factors influencing the uptake of family planning services in the Talensi District, Ghana. Pan Afr Med J. 2015;20(1). doi:10.11604/pamj.2015.20.10.5301
9. RWANDA PSI. Family Planning Needs During the First Two Years Postpartum in Rwanda. 2010.
10. Conde-Agudelo A. Maternal morbidity and mortality associated with interpregnancy interval: Cross Sectional Study. BMJ. 2000;321(7271):1255–1259. doi:10.1136/bmj.321.7271.1255
11. Ahmed S, Norton M, Williams E, et al. Operations research to add postpartum family planning to maternal and neonatal health to improve birth spacing in Sylhet District, Bangladesh. Glob Health Sci Pract. 2013;1(2):262–276.
12. Tessema GA, Mekonnen TT, Mengesha ZB, Tumlinson K. Association between skilled maternal healthcare and postpartum contraceptive use in Ethiopia. BMC Pregnancy Childbirth. 2018;18(1):1–13. doi:10.1186/s12884-018-1790-5
13. Bakamjian L, Caruso S, Cianci S, Malandrino C, Cicero C. Programming Strategies for Postpartum Family Planning. Geneva, Switzerland: World Health Organization; 2013.
14. ICF C. Ethiopia Demographic and Health Survey 2016. Vol. 1. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016:6.
15. Fantahun M. Assessment of Postpartum Contraceptive Adoption and Associated Factors in Butajira Health and Demographic Surveillance Site (HDSS), in Southern Ethiopia. Addis Ababa University; 2015.
16. Ashebir W, Tadesse T. Associated factors of postpartum modern contraceptive use in Burie District, Amhara Region, Ethiopia. J Pregnancy. 2020;2020:2020. doi:10.1155/2020/6174504
17. Borda M, Winfrey W. Postpartum Fertility and Contraception: An Analysis of Findings from 17 Countries. Baltimore: Jhpiego; 2010.
18. Pasha O, Goudar SS, Patel A, et al. Postpartum contraceptive use and unmet need for family planning in five low-income countries. Reprod Health. 2015;12(2):1–7. doi:10.1186/1742-4755-12-S2-S11
19. World Health Organization. Packages of Interventions for Family Planning, Safe Abortion Care, Maternal, Newborn and Child Health. World Health Organization; 2010.
20. Gizaw W, Zewdu F, Abuhay M, Bayu H. Extended postpartum modern contraceptive utilization and associated factors among women in Gozamen district, East Gojam Zone, northwest Ethiopia, 2014. Insights Reprod Med. 2017;1(2):8.
21. Abera Y, Mengesha ZB, Tessema GA. Postpartum contraceptive use in Gondar town, Northwest Ethiopia: a Community Based Cross-Sectional Study. BMC Womens Health. 2015;15(1):19. doi:10.1186/s12905-015-0178-1
22. Niguse SG, Kuti KA, Belda SS. Contraceptive use and associated factors among women in the extended postpartum period in Dello Mena District, Bale Zone, Ethiopia: a Cross-Sectional Study.
23. Abraha TH, Teferra AS, Gelagay AA. Postpartum modern contraceptive use in northern Ethiopia: prevalence and associated factors. Epidemiol Health. 2017;39.
24. Dona A, Abera M, Alemu T, Hawaria D. Timely initiation of postpartum contraceptive utilization and associated factors among women of child bearing age in Aroressa District, Southern Ethiopia: a Community Based Cross-Sectional Study. BMC Public Health. 2018;18(1):1–9. doi:10.1186/s12889-018-5981-9
25. Taye EB, Mekonen DG, Debele TZ. Prevalence of post partum modern family planning utilization and associated factors among postpartum mothers in Debre Tabor Town, North West Ethiopia, 2018. BMC Res Notes. 2019;12(1):430. doi:10.1186/s13104-019-4464-0
26. Jalang’o R, Thuita F, Barasa SO, Njoroge P. Determinants of contraceptive use among postpartum women in a county hospital in rural Kenya. BMC Public Health. 2017;17(1):604. doi:10.1186/s12889-017-4510-6
27. Gejo NG, Anshebo AA, Dinsa LH. Postpartum modern contraceptive use and associated factors in Hossana town. PLoS One. 2019;14(5):e0217167. doi:10.1371/journal.pone.0217167
28. Gebremedhin AY, Kebede Y, Gelagay AA, Habitu YA. Family planning use and its associated factors among women in the extended postpartum period in Addis Ababa, Ethiopia. Contracept Reprod Med. 2018;3(1):1. doi:10.1186/s40834-017-0054-5
29. Hounkponou F, Ahanhanzo YG, Biaou COA, et al. Postpartum contraceptive use in Parakou (A city in northern Benin) in 2018: a Community Based Cross-Sectional Study. Open Access J Contracept. 2019;10:19. doi:10.2147/OAJC.S219709
30. Nigussie A, Girma D, Tura G. Postpartum family planning utilization and associated factors among women who gave birth in the past 12 months, Kebribeyah Town, Somali Region, Eastern Ethiopia. J Womens Health Care. 2016;5(340):2167–0420.1000340.
31. Baqui AH, Ahmed S, Begum N, et al. Impact of integrating a postpartum family planning program into a community-based maternal and newborn health program on birth spacing and preterm birth in rural Bangladesh. J Glob Health. 2018;8(2). doi:10.7189/jogh.08.020406
32. Coomson JI, Manu A. Determinants of modern contraceptive use among postpartum women in two health facilities in urban Ghana: a Cross-Sectional Study. Contracept Reprod Med. 2019;4(1):17. doi:10.1186/s40834-019-0098-9
33. Eliason SK, Bockarie AS, Eliason C. Postpartum fertility behaviours and contraceptive use among women in rural Ghana. Contracept Reprod Med. 2018;3(1):13. doi:10.1186/s40834-018-0066-9
34. Mekonnen BD, Gelagay AA, Lakew AM. Time to use modern contraceptives and associated factors among women in extended postpartum period in Gondar City, Northwest Ethiopia. Fam Med Med Sci Res. 2020.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.