Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Mobile App Psychoeducation for Dementia Caregivers In Vietnam: A Randomized Controlled Trial
Authors Nguyen TTT ![]() , Vu LDT
, Vu LDT ![]() , Nguyen TC, Truong KT, Thai TT
, Nguyen TC, Truong KT, Thai TT ![]() , Than THN, Nguyen HT
, Than THN, Nguyen HT
Received 1 August 2025
Accepted for publication 15 October 2025
Published 23 October 2025 Volume 2025:18 Pages 6871—6885
DOI https://doi.org/10.2147/JMDH.S557573
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Charles V Pollack
Tran To Tran Nguyen,1,2 Lan Duong Tuyet Vu,2 Tuan Chau Nguyen,3 Khoa Tri Truong,1,4 Truc Thanh Thai,5 The Ha Ngoc Than,6 Huan Thanh Nguyen1,7
1Department of Geriatrics and Gerontology, School of Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 2Department of Geriatrics, Nhan dan Gia Dinh Hospital, Ho Chi Minh City, Vietnam; 3Department of Rheumatology, University Medical Center Ho Chi Minh City, Ho Chi Minh City, Vietnam; 4Tam Anh Ho Chi Minh City General Hospital, Ho Chi Minh City, Vietnam; 5Department of Medical Statistics and Informatics, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 6Medical Ethics – Social Medicine – Palliative Care Department, School of Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 7Department of Cardiology, Thong Nhat Hospital, Ho Chi Minh City, Vietnam
Correspondence: Tran To Tran Nguyen, Department of Geriatrics and Gerontology, School of Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, 217 Hong Bang, Ward Cho Lon, Ho Chi Minh City, 700000, Vietnam, Tel +84979635889, Email [email protected]; [email protected]
Purpose: This study aimed to evaluate the effectiveness of a smartphone app–based psychoeducational intervention for caregivers of people with dementia (PwD). Primary outcomes included levels of depression, anxiety, and stress. Secondary outcomes were dementia knowledge, caregiving burden, and perceived social support.
Participants and methods: This randomized controlled trial was conducted at the Geriatrics Department of a public hospital in Ho Chi Minh City, Vietnam. Eligible participants were family caregivers of PwD with at least a fifth-grade education, a caregiving duration of six months or more, a smartphone with the Zalo app (a free messaging platform in Vietnam), and a Stress Thermometer score of 4 or higher. Participants were randomly assigned to the intervention or usual care group in a 1:1 ratio. The intervention was delivered over seven weeks via Zalo and consisted of seven short videos covering dementia progression, daily care, behavioral symptoms, comorbidities, self-care, and caregiver preparation. The intervention was delivered individually to ensure personalized support. Outcomes were assessed at baseline, post-intervention, and three-month follow-up.
Results: A total of 172 participants were randomized. Compared to the control group, the intervention group showed significant reductions in depression (β = − 4.5, p < 0.001), anxiety (β = − 5.2, p < 0.001), and stress (β = − 6.5, p < 0.001), with effects maintained at the three-month follow-up. Significant improvements were also observed in dementia knowledge (β = 2.3, p < 0.001), perceived social support (β = 0.5, p < 0.001), and caregiving burden (β = − 2.9, p < 0.001), which were sustained over time.
Conclusion: This smartphone-based psychoeducational intervention had a positive impact on caregiver mental health and caregiving capacity. Its accessible and scalable design may help overcome geographical and resource barriers in Vietnam and other resource-limited countries.
Trial Registration: https://clinicaltrials.gov/study/NCT06700551.
Keywords: digital intervention, burden, low-resource settings, social support, stress reduction, Zalo app
Introduction
With the ongoing increase in the aging population, dementia has become one of the leading causes of dependence and disability among older adults worldwide.1,2 Current estimates show that over 55 million people are affected by dementia, and nearly 10 million new cases are diagnosed each year.1 The financial burden is substantial,3,4 with worldwide costs hitting around USD 1 trillion in 2018 and projected to almost double by 2030. Notably, more than 60% of people with dementia (PwD) live in low- and middle-income countries (LMICs), where care is primarily provided at home by family members.2,5
Caring for older adults with dementia becomes more demanding as the disease advances.6 In the early stages, family caregivers may dedicate around 37 hours per week to caregiving tasks; however, this can increase to nearly 109 hours per week during the advanced stages.7,8 As dementia progresses, the type of care shifts from help with instrumental activities of daily living to providing complete personal care.9,10 Beyond the physical effort, caregivers often encounter behavioral issues and comorbidities in PwD.11,12 As a result, they face significant physical and psychological stress compared to those caring for older adults without dementia.13,14 Research has shown notable rates of depression (30–40%) and anxiety (32–44%) among caregivers of PwD, including in Asian populations.8,15,16 Moreover, caregivers of PwD often experience physical health issues such as fatigue, musculoskeletal pain, and sleep disturbances, which are linked to the long-term physical and emotional demands of caregiving.17,18 Despite these challenges, many family caregivers in LMICs often lack sufficient support systems and training, which further increases their caregiving burden.19–21 This not only compromises the quality of care provided to PwD but also significantly increases the risk of caregivers’ burnout.22,23
Vietnam is one of the fastest-aging countries in Asia, with over 650,000 people currently living with dementia.1,24 In 2021, Vietnam recorded age-standardized incidence and prevalence rates of 110.09 (95% uncertainty interval [UI]: 96.21–126.57) and 649.42 (95% UI: 556.89–744.39) per 100,000 population for Alzheimer’s disease and other dementias. These estimates are broadly consistent with those observed across Southeast Asia and globally.25 Most of these individuals are cared for at home by family members.26,27 Research shows that 92.1% of family caregivers have limited knowledge about dementia, and 74.2% report needing help with caregiving.28 However, support systems for PwD and their caregivers are still limited, often leaving family members to manage the complex demands of caregiving alone.29 This situation leads to increased burden and psychological distress.
Psychoeducational interventions are crucial for supporting family caregivers of individuals with dementia, as they provide essential knowledge, practical caregiving skills, and psychological support.30,31 Research has shown that these interventions can significantly decrease caregiver burden, reduce symptoms of anxiety and depression, improve overall well-being, and foster better mental health among caregivers.32,33 However, access to these programs remains limited in many LMICs, including Vietnam.
In recent years, technology-based interventions have emerged as innovative solutions, providing more accessible and flexible methods for delivering educational content and emotional support.34,35 Among these, mobile applications have grown increasingly popular because of their accessibility, flexibility, and adaptability across various healthcare settings. They have been effectively used for managing chronic diseases, supporting mental health, and caring for dementia. Additionally, the integration of artificial intelligence (AI) into mobile platforms has further improved personalization and user engagement, opening up new possibilities for tailored caregiver support.36,37
Importantly, using digital health technologies to support dementia caregivers aligns with the strategic priorities outlined in the World Health Organization’s Global Action Plan on the Public Health Response to Dementia 2017–2025, which highlights the importance of developing technology-based caregiver interventions to reduce the burden and enhance support systems.38 Despite these encouraging advances, few digital interventions have been culturally adapted or thoroughly evaluated in LMIC settings like Vietnam, where the need for scalable, context-appropriate caregiver support remains urgent.
To date, only one pilot cluster randomized controlled trial has been published in northern Vietnam, evaluating a multicomponent intervention that included problem-solving techniques, mood regulation through cognitive restructuring, stress reduction strategies, and communication skills training.39 However, the intervention was delivered face-to-face, either at clinics or in caregivers’ homes, which may limit its scalability in settings with limited healthcare staff. Compared to other methods, smartphone-based interventions offer a more practical and scalable option, given the widespread use of mobile phones and internet access in Vietnam.40,41 Therefore, we created and implemented a psychoeducational program delivered via Zalo,42 a free and widely used messaging platform among Vietnamese adults. In Phase 1, we conducted a qualitative study to understand caregivers’ needs and identify the key information and skills required for support.29 In Phase 2, we developed the intervention content and assessed the feasibility of both the approach and the intervention. In Phase 3 (the current study), we performed a randomized controlled trial to assess the effectiveness of the intervention.
The primary aim of this randomized controlled trial was to evaluate the effectiveness of a smartphone-based psychoeducational intervention in reducing psychological distress among family caregivers of PwD. The secondary aim was to assess the intervention’s effects on dementia-related knowledge, caregiver burden, and perceived social support.
Methods
Trial Design
This study employed a randomized controlled trial design, with participants randomly assigned to the intervention and control groups (1:1 ratio). The trial was conducted following the CONSORT (Consolidated Standards of Reporting Trials) guidelines, and a detailed checklist is included in Supplementary 1.
Participants
Family caregivers who were primarily responsible for the daily care of older adults with dementia hospitalized in the Geriatrics Department at Nhan dan Gia Dinh Hospital were eligible for inclusion. Inclusion criteria were: (1) Vietnamese citizenship; (2) age ≥18 years; (3) completion of at least a fifth-grade education; (4) ownership of or willingness to install Zalo, a free and commonly used messaging application in Vietnam; and (5) a score ≥4 on the Stress Thermometer (range: 0–10). Exclusion criteria included: a current diagnosis of a mental health disorder (eg, major depressive disorder, bipolar disorder); a Mini-Cog score ≤4; or a serious physical illness such as metastatic cancer. Recruitment was conducted from October 2024 to March 2025 and written informed consent was required prior to participation.
Intervention
The intervention was delivered through the Zalo mobile application. Participants in the intervention group received weekly psychoeducational videos via the app’s messaging feature. Before sending each video, a research member who administered the intervention asked participants which topics they were most interested in. A total of seven videos were shared, covering essential knowledge about dementia, caregiving skills, and support for caregivers. The topics included: (1) understanding dementia and its progression, (2) the role of the caregiver, (3) self-care strategies, (4) feeding and managing incontinence, (5) addressing behavioral changes in PwD, (6) fall prevention, and (7) pressure ulcer prevention and management. These educational materials were developed based on findings from a qualitative study involving 20 in-depth interviews, which explored the information and skills caregivers need when caring for PwD.29 The development of the intervention content was mainly guided by the World Health Organization’s iSupport program,43 with input from experts in dementia and geriatric care. Additionally, participants were encouraged to submit caregiving-related questions throughout the program. The program administrator answered these questions after consulting with relevant specialists. Importantly, the intervention was delivered individually, providing personalized support tailored to each caregiver’s specific needs.
Usual Care
Caregivers in the usual care group received standard care without any extra intervention. They had access to an educational website specifically designed for caregivers of individuals with dementia (https://www.alz.org/asian/about/what_is_alzheimers.asp?nL=VI&dL=VI) and were encouraged to explore the content independently. The intervention did not impact or alter the medical treatment of PwD during hospitalization or after discharge.
Measures
All study data were collected and managed using REDCap, a secure web-based platform hosted by the University of Medicine and Pharmacy at Ho Chi Minh City. Data collection was through face-to-face interviews using a structured, pre-defined questionnaire.
Demographics
Demographic information of participants, including age, sex, education level, occupation, marital status, income, relationship to the care recipient, and duration of caregiving, was gathered from participants. Data on participants’ chronic health conditions were also recorded. Additionally, demographic and clinical characteristics of care recipients, including age, sex, functional status, dementia severity, and comorbidities, were collected.
Outcomes
The primary outcome of the study was the level of depression, anxiety, and stress among caregivers, assessed using the 21-item Depression, Anxiety, and Stress Scale (DASS-21). This instrument includes three subscales, each measuring one of the emotional states. Scores for each subscale range from 0 to 42, while the overall score ranges from 0 to 126, with higher scores reflecting greater psychological distress.44 Assessments were conducted at three time points: before the intervention (baseline), immediately following the intervention, and three months post-intervention.
The secondary outcomes included participants’ knowledge of dementia, caregiving burden, and perceived social support: (1) Dementia knowledge was measured using a seven-item questionnaire from the Northern Ireland Life and Times Survey.45 Scores range from 0 to 7, with higher scores reflecting greater knowledge; (2) The burden of caregiving46 was assessed using the 4-item version of the Zarit Burden Interview (ZBI), in which each item is rated on a 5-point Likert scale from 0 to 4. The total score ranges from 0 to 16, with higher scores indicating a greater perceived burden; (3) Perceived social support was assessed using the Multidimensional Scale of Perceived Social Support (MSPSS), which includes 12 items measuring support from three sources: a significant other, friends, and family.47 Each item is rated on a 7-point Likert scale, from 1 (very strongly disagree) to 7 (very strongly agree), resulting in a total score that ranges from 12 to 84. Higher scores reflect greater levels of perceived social support. These instruments had been previously translated into Vietnamese and culturally adapted.28,48–50 In this study, they were assessed at three time points: before the intervention (baseline), right after the intervention, and three months post-intervention.
Sample Size
The sample size was calculated based on a superiority design with continuous outcomes (DASS-21 scores). The formula used was:

Where n1 and n2 are the required sample sizes per group, S is the pooled standard deviation, δ is the expected mean difference, and δ0 is the clinically meaningful difference. The calculation was based on several assumptions: (1) a moderate effect size (standardized difference of 0.5) between the intervention and control groups for both primary outcomes at the post-intervention stage; (2) statistical power of 80%; (3) an anticipated attrition rate of 10% within the intervention group; (4) a 1:1 allocation ratio between the control and intervention groups, assuming a similar attrition rate of approximately 10% in the control group; and (5) expected variability in DASS-21 scores post-intervention, informed by prior research.51 Based on these parameters, the final adjusted sample size was determined to be 86 participants per group. The computation was performed using Stata version 16.0.
Randomization
Participants who met the eligibility criteria were randomly allocated to either the intervention or control group through block randomization with varying block sizes. The randomization process was conducted by an independent statistician to ensure allocation concealment. A total of 172 sealed, sequentially numbered envelopes (from 1 to 172) were prepared in advance. Each participant was assigned a number in the order of enrollment. Following the baseline interview, the envelope with the corresponding number was opened. An assignment letter inside determined group allocation: “A” indicated placement in the intervention group, while “B” indicated assignment to the control group.
Blinding
The team members conducting the outcome assessments were blinded to the participants’ group assignments and were unaware of whether individuals belonged to the intervention or control group.
Statistical methods
Independent sample t-tests or Mann–Whitney U-tests were used to compare continuous variables between the intervention and control groups, depending on the normality of the data distribution. Categorical variables were analyzed using Chi-squared tests or Fisher’s exact tests, as appropriate.
An intention-to-treat (ITT) approach was applied for the primary analysis. To assess the effects of the intervention on repeated measures outcomes, linear mixed-effects models were employed, including a random intercept for participants and fixed effects for group, time, and the group-by-time interaction. Statistical significance was set at p <0.05. All analyses were conducted using Stata version 16.0 (StataCorp LLC, College Station, TX, USA).
Ethics Approval and Informed Consent
The study was approved by the Institutional Review Board of the University of Medicine and Pharmacy at Ho Chi Minh City (Approval No. 557/HĐĐĐ-ĐHYD) and conducted in accordance with the principles of the Declaration of Helsinki.
To maintain ethical standards and protect participant data, informed consent was secured from all participants before enrollment. For confidentiality, individuals in the intervention group were only identified by coded numbers rather than personal details, and all communication data on Zalo will be permanently deleted within three months after the follow-up period.
Trial Registration
Mobile-Phone-Based Psychoeducation for Dementia Caregivers in Vietnam. ID: NCT06700551. URL: https://clinicaltrials.gov/study/NCT06700551.
Results
During the study period, 174 eligible participants were invited to participate; however, two declined due to time constraints. A total of 172 participants were subsequently randomized into the intervention and usual care groups. During the intervention period, three participants in the intervention group and three in the usual care group withdrew due to the death of the care recipient. During the follow-up period, an additional three participants in the intervention group were lost due to the death of the care recipient, and two participants in the usual care group were lost to follow-up due to loss of contact. Finally, 172 participants were included in the analysis. The flow of participants is illustrated in the CONSORT flow diagram (Figure 1). The recruitment process spanned five months, from October 2024 to February 2025. The intervention phase concluded on April 5, 2025, followed by a three-month follow-up period that ended on July 5, 2025.
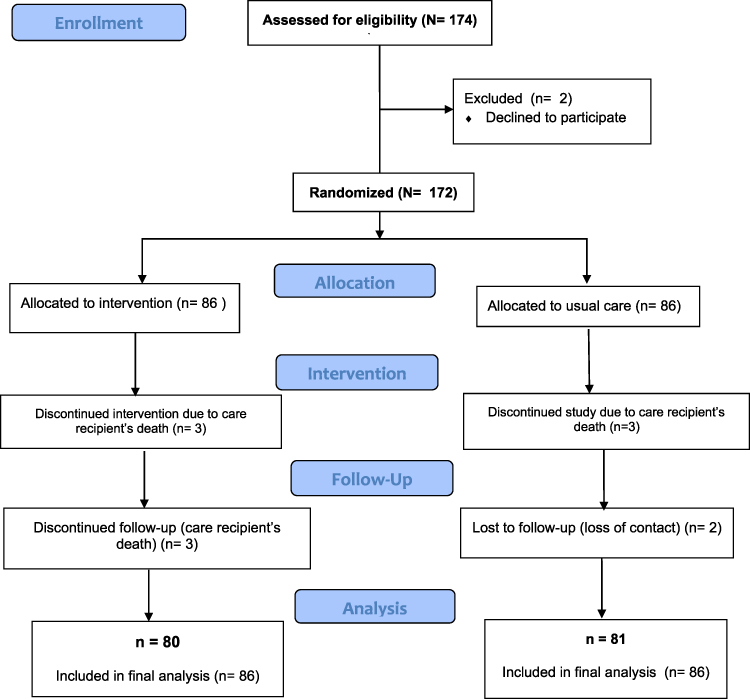 |
Figure 1 CONSORT Flow Diagram. |
Tables 1 and 2 show the baseline characteristics of participants and care recipients (PwD). Overall, the demographics of participants in the intervention and usual care groups were similar. Over 70% of the caregivers were female, and roughly three-quarters were the daughter or son of the PwD. Notably, a higher percentage of individuals in the intervention group reported spending more than 9 hours on caregiving compared to those in the usual care group. Similarly, the care recipients in both groups had comparable characteristics, with about 80% of PwD in each group classified as having a severe stage of dementia.
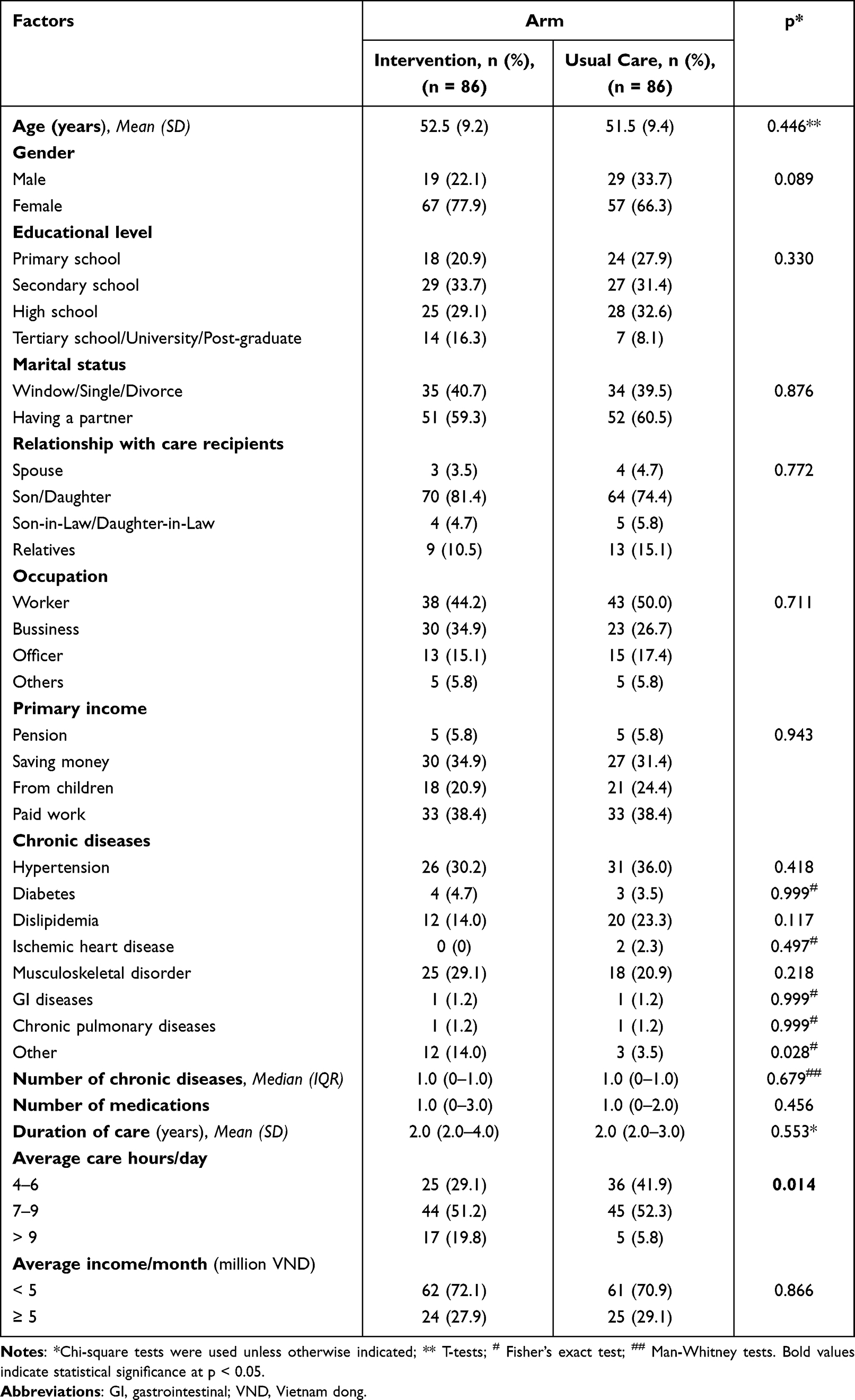 |
Table 1 Baseline Characteristics of Participants (N = 172) |
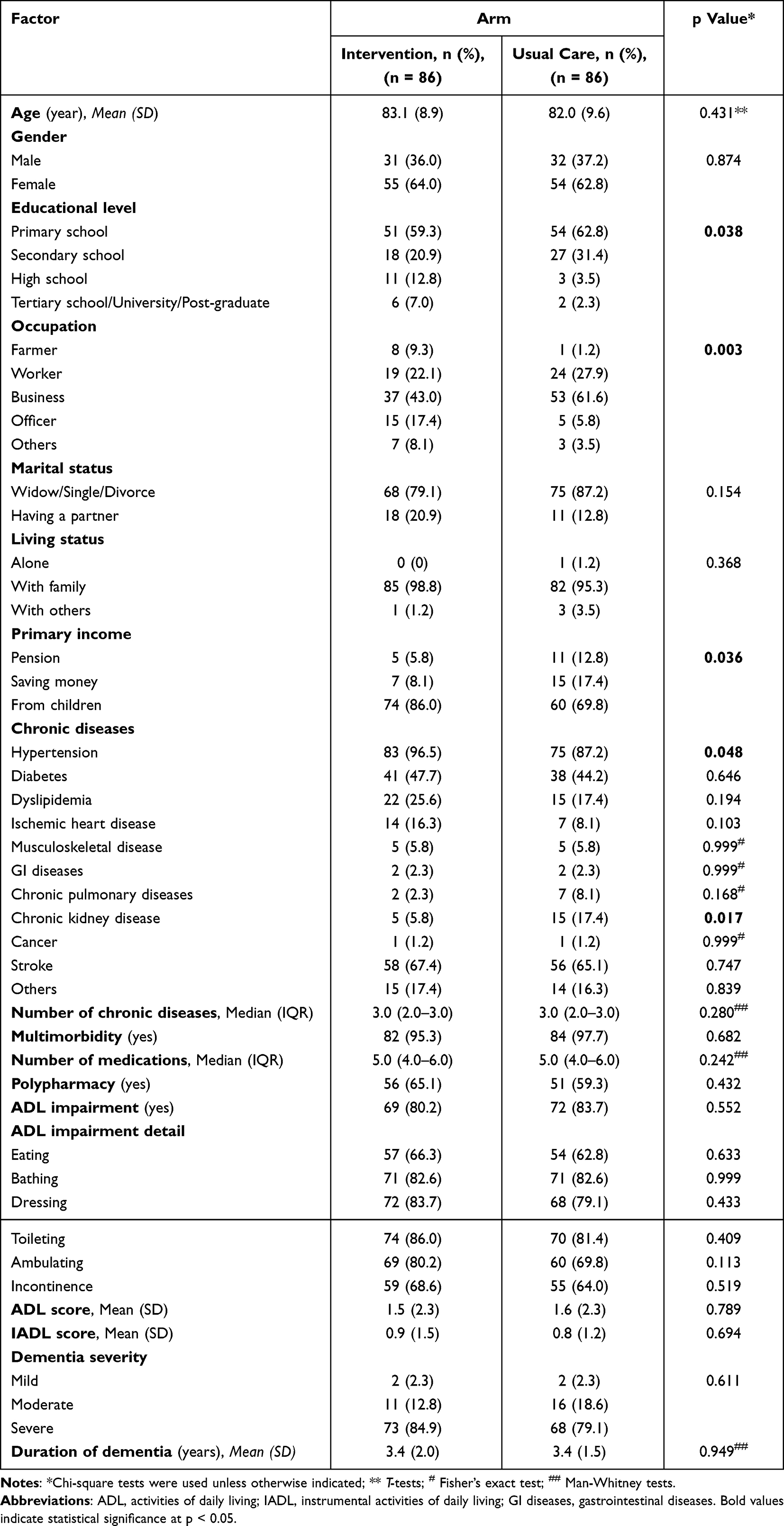 |
Table 2 Baseline Characteristics of Care Recipients (N = 172) |
Descriptive statistics for the primary and secondary outcomes are presented in Tables 3 and 4, respectively. Overall, participants in the intervention group demonstrated improvements in outcomes from baseline to the post-intervention assessment.
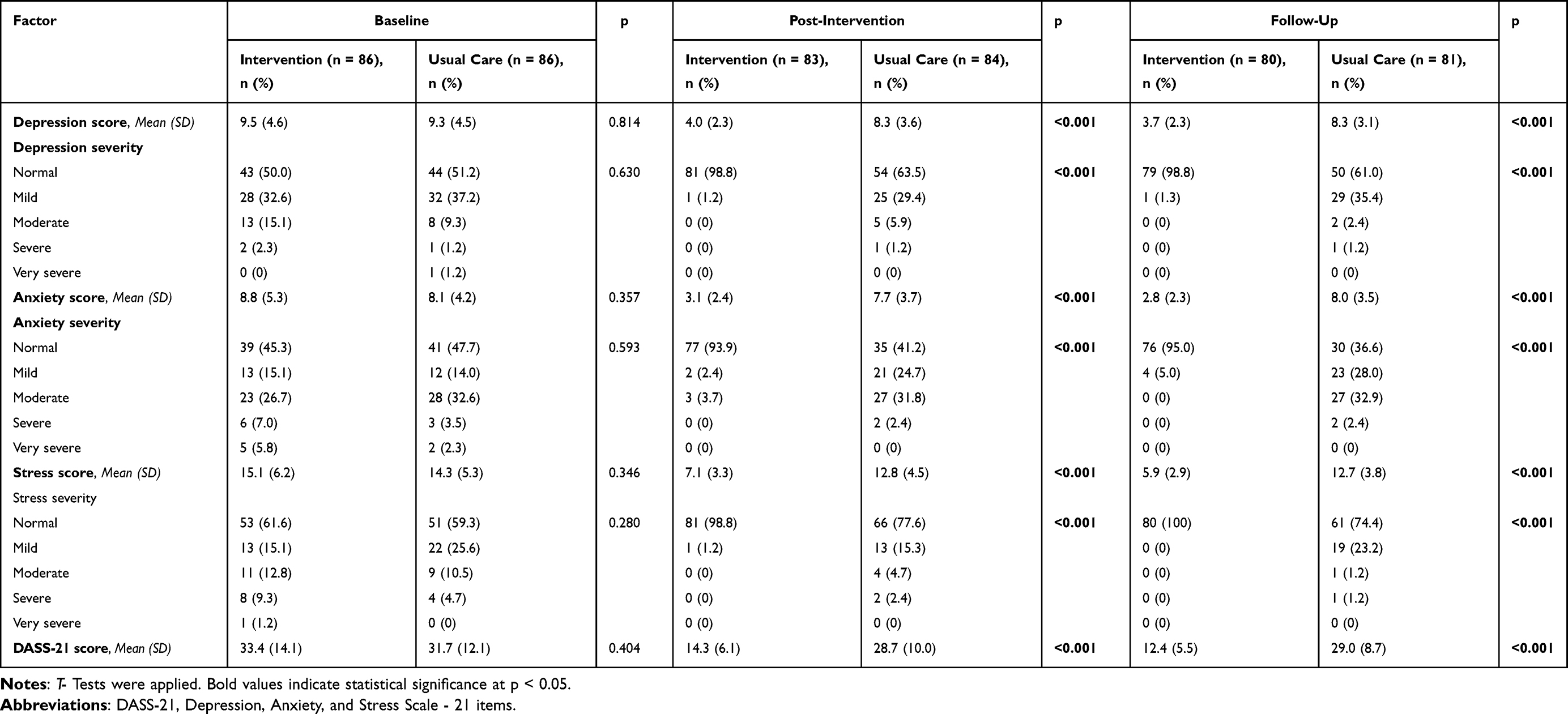 |
Table 3 Depression, Anxiety, and Stress Scores of Participants in the Two Groups at Baseline, Post-Intervention, and Three-Month Follow-Up |
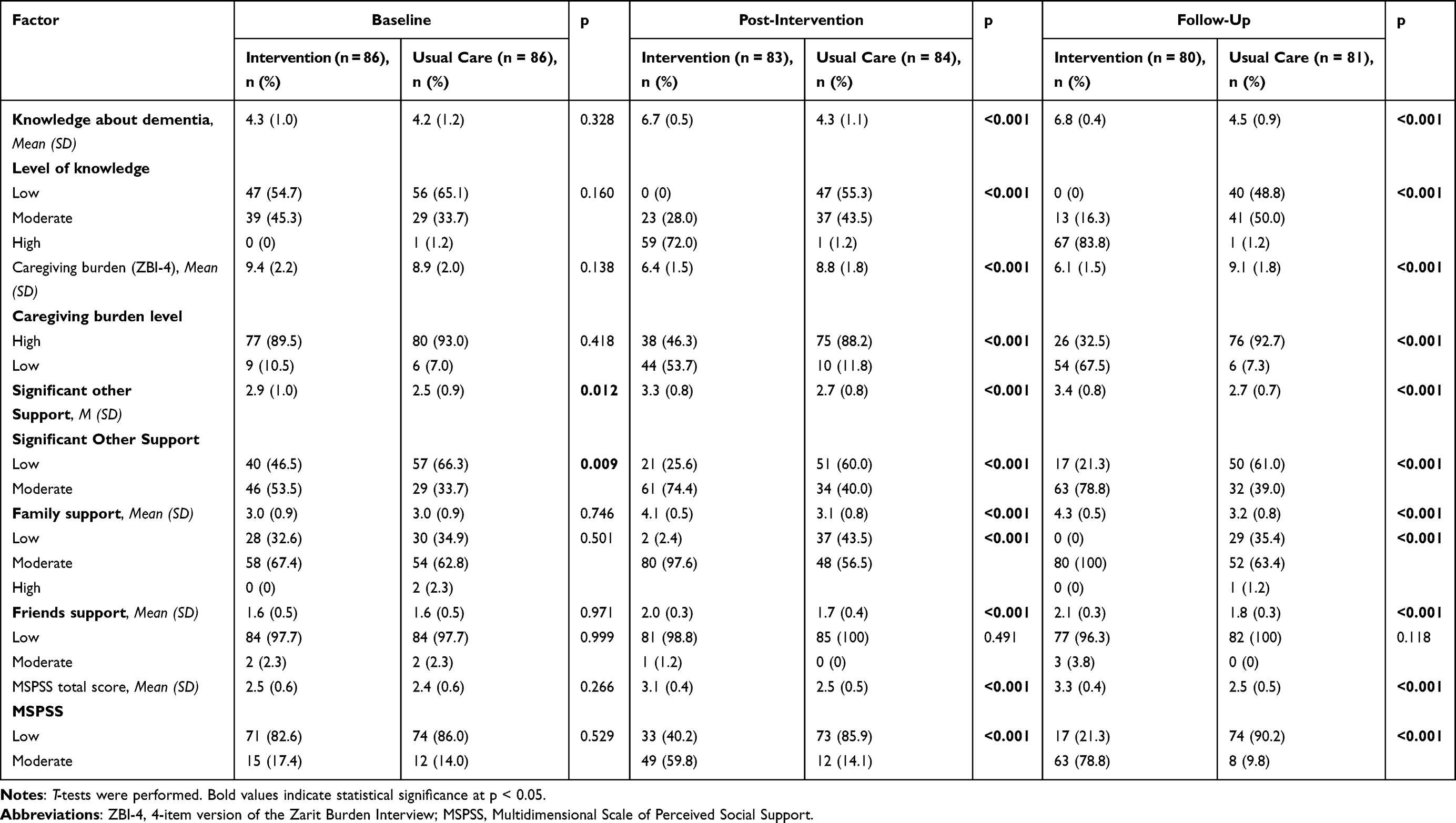 |
Table 4 Secondary Outcomes of The Two Groups at Baseline, Post-Intervention, and Three-Month Follow-Up |
The effects of the intervention over time in both the intervention and usual care groups are shown in Table 5 and depicted in Supplementary 2. Compared to the control group, the intervention group showed significant reductions in depression (β = −4.5, p <0.001), anxiety (β = −5.2, p <0.001), and stress (β = −6.5, p <0.001), with effects maintained at the three-month follow-up. Significant improvements were also observed in dementia knowledge (β = 2.3, p <0.001), perceived social support (β = 0.5, p <0.001), and caregiving burden (β = −2.9, p <0.001), which were sustained over time.
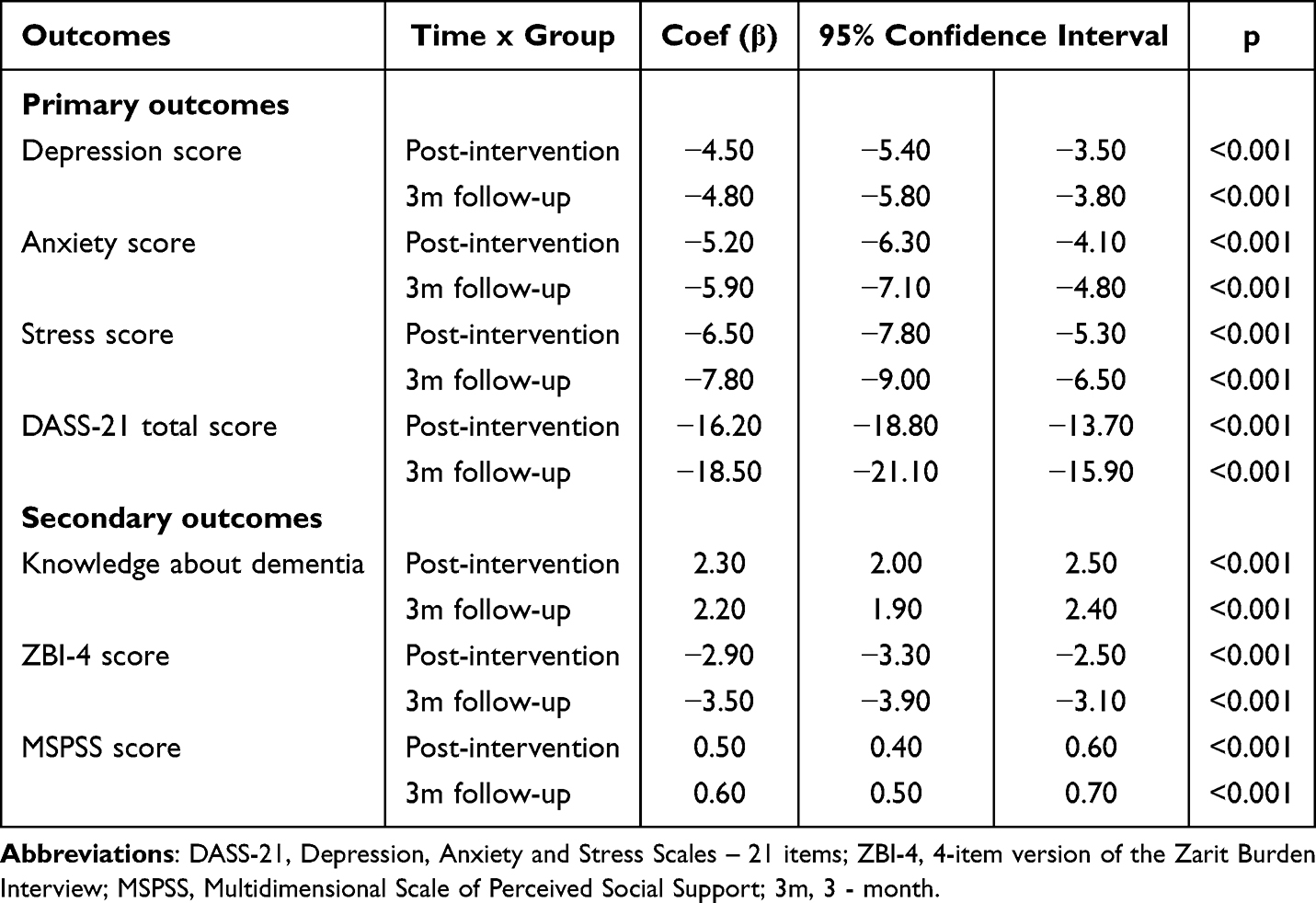 |
Table 5 Estimated Intervention Effects on Outcome Measures Over Time From Linear Mixed-Effects Models |
No adverse effects or harms were reported by participants in the intervention group during the study period.
Discussion
This study assessed the effectiveness of a Zalo-based psychoeducational intervention for caregivers of PwD. Regarding the primary outcomes, the intervention significantly lowered participants’ levels of depression, anxiety, and stress immediately after the program, with these improvements sustained at the three-month follow-up. The intervention also showed notable benefits across secondary outcomes. Compared to those receiving usual care, participants in the intervention group experienced greater improvements in dementia-related knowledge, perceived social support, and reductions in caregiver burden at both post-intervention and three-month follow-up. All observed changes were statistically significant (p <0.001) and associated with clinically meaningful effect sizes.
The consistent improvements seen in psychological and related outcomes likely result from both the relevance of the intervention content and the mode of delivery. The intervention was developed based on the specific needs of caregivers identified through in-depth interviews, with a focus on key areas such as dementia progression, caregiver preparedness, daily care skills, management of behavioral symptoms, and common comorbidities in care recipients.29,43 This content likely helped reduce psychological distress, increased knowledge about dementia, boosted perceived social support, and lowered caregiver burden. Additionally, using Zalo, a familiar and widely used messaging platform among Vietnamese adults, provided a user-friendly and accessible way to deliver the intervention. Content was delivered through short videos, which fit the busy schedules of caregivers. The one-on-one format also offered more privacy and helped participants feel more comfortable asking questions about their caregiving experiences. Additionally, the digital format allowed caregivers to participate without traveling to healthcare facilities, overcoming a common barrier to attending traditional face-to-face interventions. These factors together enhanced the overall effectiveness of the program.
Our results are consistent with previous research on mobile app–based psychoeducational interventions. For example, a study in Australia using the Stress Less app over five weeks showed significant reductions in stress (β = −2.07, p =0.04) and depression (β = −1.36, p =0.05) immediately after the intervention and at the three-month follow-up.51 However, there was no notable change in anxiety levels observed in that study. Similarly, a study conducted in Malaysia evaluating a mobile phone–based psychoeducational program for caregivers of PwD found significant reductions in caregiver burden, anxiety (β = −2.46, p = <0.001), and stress (β = −2.98, p =0.011) levels following the intervention.52 Compared to the two aforementioned studies, the intervention in our study resulted in relatively greater reductions in psychological outcomes. This may be attributed to the use of Zalo, a widely used and familiar platform among Vietnamese users, which likely enhanced participant engagement and adherence.53 The consistent findings across diverse delivery platforms and geographic regions underscore the value of digital and remote psychoeducational interventions as scalable and accessible tools for improving the psychological well-being of caregivers of PwD. A systematic review of 22 randomized controlled trials evaluating the effectiveness of internet-based or mobile app interventions for dementia caregivers reported significant benefits, including reductions in caregiver burden, improved perceived social support, and increased knowledge about dementia. Building on this evidence, our study offers new insights from an LMIC setting by using a locally developed and widely used digital platform (Zalo) to deliver the intervention.
Today, ChatGPT offers significant advantages in providing medical information to patients and caregivers. It can produce quick, human-like responses, making it easier for users to access information, especially when healthcare access is limited. Additionally, it helps caregivers understand symptoms, possible diagnoses, or treatment options, which can reduce anxiety and aid decision-making. However, relying only on ChatGPT comes with many risks. Since it is not trained with curated medical datasets and lacks clinical validation, it might give inaccurate information. This can mislead users, delay proper care, or even threaten patient safety.54 Furthermore, users may not fully recognize the chatbot’s limitations and might mistakenly see it as a medical expert.55 Therefore, using trusted sources of health information validated by professionals remains essential for caregiver education.
Several implications can be learnt from our study. The findings offer a novel and practical approach to supporting caregivers of PwD in Vietnam and other LMICs, where healthcare resources and infrastructure are often limited. This mobile app–based intervention is convenient for both caregivers and healthcare providers, especially those facing time constraints. The intervention content was tailored to the needs of participants, contributing to high adherence and engagement. Moreover, the digital format offers substantial potential for scalability across both urban and rural settings, making it a promising strategy for broader implementation.
However, several limitations should be acknowledged. Participants in this study were required to have at least a primary level of education, which excluded individuals with low literacy, who may experience greater caregiving challenges and higher levels of psychological distress. These individuals might require alternative forms of support tailored to their specific needs. Moreover, we were unable to verify whether participants consistently watched the video content. To enhance engagement, weekly reminder phone calls were made to encourage participants to view the materials. Notably, before conducting this randomized controlled trial, we carried out a pilot randomized controlled trial to assess the feasibility of both the intervention and the study methodology.56,57 The preliminary phase helped refine the intervention delivery process, contributing to the reliability of the present findings. This study was conducted at a single center and used a specific platform (Zalo), which may limit how broadly the findings can apply to the general population. Future research should include multicenter studies with diverse digital platforms to assess the effectiveness and relevance of the intervention more accurately.
Conclusions
The smartphone-based psychoeducational intervention delivered through the Zalo app showed positive effects on caregivers of PwD. It resulted in significant reductions in depression, anxiety, and stress, increased dementia-related knowledge, decreased caregiver burden, and improved perceived social support. These results indicate that this type of intervention is a convenient and practical option that could be used in hospital settings or other community-based services in Vietnam and similar LMICs. By utilizing mobile technology, the intervention can help overcome geographical barriers, resource shortages, and time constraints that both caregivers and healthcare providers face. Looking ahead, the psychoeducation videos developed in this study could be further adapted into a public platform or an independent mobile app, thereby increasing access for more caregivers and supporting the sustainability of caregiver assistance programs.
Abbreviations
DASS-21, Depression, Anxiety and Stress Scale - 21 items; ZBI-4, 4-item version of the Zarit Burden Interview; MSPSS, Multidimensional Scale of Perceived Social Support; PwD, People with Dementia.
Data Sharing Statement
De-identified data will be available upon reasonable request to Tran To Tran Nguyen. The available data include demographic characteristics, baseline measurements, and outcomes. Data will be accessible starting 12 months after publication and for up to 2 years following the publication.
Acknowledgments
We want to sincerely thank Professor Penny Schofield and Associate Professor Tuan Anh Nguyen for their invaluable support. We also extend our warm thanks to the participants and the staff at Nhan dan Gia Dinh Hospital for their cooperation and assistance. We also acknowledge the use of ChatGPT (OpenAI) for assistance with language editing during the preparation of this manuscript.
Funding
This research received no external funding.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Nichols E, Steinmetz JD, Vollset SE, et al. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 2022;7(2):e105–e125. doi:10.1016/S2468-2667(21)00249-8
2. Word Health Organization. Dementia. May 17th, 2025. 2025.Available from: https://www.who.int/news-room/fact-sheets/detail/dementia.
3. Lastuka A, Bliss E, Breshock MR, et al. Societal Costs of Dementia: 204 Countries, 2000–2019. J Alzheimer’s Dis. 2024;101(1):277–292. doi:10.3233/jad-240163
4. Alzheimer’s Disease International. World Alzheimer Report 2018 The state of the art of dementia research: new frontiers. 2018:4–46. https://www.alzint.org/u/WorldAlzheimerReport2018.pdf.
5. Giebel C, Hanna K, Watson J, et al. A systematic review on inequalities in accessing and using community-based social care in dementia. Inter Psychogeria. 2024;36(7):540–563. doi:10.1017/S104161022300042X
6. Culberson JW, Kopel J, Sehar U, Reddy PH. Urgent needs of caregiving in ageing populations with Alzheimer’s disease and other chronic conditions: support our loved ones. Ageing Res Rev. 2023;90:102001. doi:10.1016/j.arr.2023.102001
7. Alzheimer’s Disease International. World Alzheimer Report 2019 Attitudes to dementia 2019:8–166. https://www.alzint.org/u/WorldAlzheimerReport2019.pdf.
8. Cheng ST, Au A, Losada A, Thompson LW, Gallagher-Thompson D. Psychological Interventions for Dementia Caregivers: what We Have Achieved, What We Have Learned. Curr Psychiatry Rep. 2019;21(7):59. doi:10.1007/s11920-019-1045-9
9. Cipriani G, Danti S, Picchi L, Nuti A, Fiorino MD. Daily functioning and dementia. Dementia & neuropsychologia. Apr-Jun. 2020;14(2):93–102. doi:10.1590/1980-57642020dn14-020001
10. Ingraham BC, Barthold D, Fishman P, Coe NB. Caregiving for dementia: trends pre-post onset and predictive factors of family caregiving (2002–2018). Health Affairs Scholar. 2024;2(3):qxae020. doi:10.1093/haschl/qxae020
11. García-Martín V, de Hoyos-Alonso MC, Delgado-Puebla R, Ariza-Cardiel G, Del Cura-González I. Burden in caregivers of primary care patients with dementia: influence of neuropsychiatric symptoms according to disease stage (NeDEM project). BMC Geriatr. 2023;23(1):525. doi:10.1186/s12877-023-04234-0
12. Feast A, Orrell M, Charlesworth G, Melunsky N, Poland F, Moniz-Cook E. Behavioural and psychological symptoms in dementia and the challenges for family carers: systematic review. Br J Psychiatry. 2016;208(5):429–434. doi:10.1192/bjp.bp.114.153684
13. Cerejeira J, Lagarto L, Mukaetova-Ladinska E. Behavioral and Psychological Symptoms of Dementia. Front Neurol. 2012;3. doi:10.3389/fneur.2012.00073
14. Riffin C, Van Ness PH, Wolff JL, Fried T. Family and Other Unpaid Caregivers and Older Adults with and without Dementia and Disability. J Am Geriatr Soc. 2017;65(8):1821–1828. doi:10.1111/jgs.14910
15. Abdelhalim DS, Ahmed MM, Hussein HA, Khalaf OO, Sarhan MD. Burden of Care, Depression, and Anxiety Among Family Caregivers of People With Dementia. J Primary Care & Commun Health. 2024;15:21501319241288029. doi:10.1177/21501319241288029
16. Liu S, Li C, Shi Z, et al. Caregiver burden and prevalence of depression, anxiety and sleep disturbances in A lzheimer’s disease caregivers in C hina. J Clin Nurs. 2017;26(9–10):1291–1300. doi:10.1111/jocn.13601
17. Sörensen S, Conwell Y. Issues in dementia caregiving: effects on mental and physical health, intervention strategies, and research needs. Ame J Geriatric Psychiatry. 2011;19(6):491–496. doi:10.1097/JGP.0b013e31821c0e6e
18. Sabatini S, Martyr A, Hunt A, et al. Health conditions in spousal caregivers of people with dementia and their relationships with stress, caregiving experiences, and social networks: longitudinal findings from the IDEAL programme. BMC Geriatr. 2024;24(1):171. doi:10.1186/s12877-024-04707-w
19. Mukadam N, Cooper C, Livingston G. Improving access to dementia services for people from minority ethnic groups. Curr Opin Psychiatry. 2013;26(4):409–414. doi:10.1097/YCO.0b013e32835ee668
20. Kumar GS, Thomas PT, Arun M, Mohandas RP, Arshad F, Alladi S. A Qualitative Exploration of Caregiving in Advanced Dementia: caregiver Perspectives on Unmet Needs in Low- and Middle-income Setting. Indian J Palliat Care. 2024. doi:10.25259/IJPC_362_2024
21. Fam J, Mahendran R, Kua EH. Dementia care in low and middle-income countries. Curr Opin Psychiatry. 2019;32(5):461–464. doi:10.1097/yco.0000000000000523
22. Lindeza P, Rodrigues M, Costa J, Guerreiro M, Rosa MM. Impact of dementia on informal care: a systematic review of family caregivers’ perceptions. BMJ Supportive Palliative Care. 2024;14(e1):e38. doi:10.1136/bmjspcare-2020-002242
23. Yurt N, Yavuz E. Assessment of the Burden of Care and Burnout Level in Caregivers of Dementia Patients in a Home Care Setting. Euras J Family Med. 2022;11(4):189–196. doi:10.33880/ejfm.2022110402
24. Nguyen TA, Pham T, Dang TH, et al. Towards the development of Vietnam’s national dementia plan-the first step of action. Australas J Ageing. 2020;39(2):137–141. doi:10.1111/ajag.12755
25. Vo QP, Dang BL, Luu BMT, et al. Burden and risk factors of Alzheimer’s disease and other dementias in Vietnam from 1990 to 2021 – a comprehensive analysis from global burden disease. Cerebral Circulation. 2025;9:100390. doi:10.1016/j.cccb.2025.100390
26. Huynh-Truong HL, Shyu Y-IL, Tran TKL, Huang H-L, Do VA. Dementia care practices among community healthcare workers in Vietnam: a qualitative descriptive study. BMC Geriatr. 2023;23(1):562. doi:10.1186/s12877-023-04199-0
27. Nguyen H, Nguyen T, Tran D, Hinton L, Werner P. “It’s extremely hard but it’s not a burden”: a qualitative study of family caregiving for people living with dementia in Vietnam. PLoS One. 2021;16(11):e0259788. doi:10.1371/journal.pone.0259788
28. Nguyen T, The T, McFarland P, et al. Dementia Prevalence Among Older Hospitalized Patients in Vietnam and Dementia Understanding of Their Caregivers. Aging Med Healthcare. 2019;10(4):128–132. doi:10.33879/AMH.2019.123-1902.003
29. Nguyen TTT, Than THN, Nguyen TC, et al. Challenges, knowledge, and skills required for family caregivers of older adults with dementia: a qualitative study in Vietnam. Global Health Action. 2025;18(1):2526929. doi:10.1080/16549716.2025.2526929
30. Zhang N, Bai Y, Tao A, Zhao Y, Chan HYL. Effects of psychoeducation interventions on psychological outcomes among spousal caregivers of community-dwelling older adults: a systematic review and meta-analysis. Inter j nurs stud. 2025;166:105049. doi:10.1016/j.ijnurstu.2025.105049
31. Kishita N, Hammond L, Dietrich CM, et al. Which interventions work for dementia family carers?: an updated systematic review of randomized controlled trials of carer interventions. Inter Psychogeria. 2018;30(11):1679–1696. doi:10.1017/S1041610218000947
32. Cintoli S, Tommasini LL, Del Prete E, Cerri M, Ceravolo R, Tognoni G. The Psychoeducational Interventions: a valuable communication tool to support the caregiver of people with dementia. BMC Geriatr. 2024;24(1):1004. doi:10.1186/s12877-024-05562-5
33. Tawfik NM, Sabry NA, Darwish H, Mowafy M, Soliman SSA. Psychoeducational Program for the Family Member Caregivers of People with Dementia to Reduce Perceived Burden and Increase Patient’s Quality of Life: a Randomized Controlled Trial. J Primary Car Commun Health. 2021;12:21501327211014088. doi:10.1177/21501327211014088
34. Mao W, Qi X, Chi I, Wichinsky L, Wu B. Technology-Based Interventions to Address Social Isolation and Loneliness Among Informal Dementia Caregivers: a Scoping Review. J Ame Med Direct Assoc. 2023;24(11):1700–1707. doi:10.1016/j.jamda.2023.08.005
35. Wójcik D, Szczechowiak K, Konopka P, et al. Informal Dementia Caregivers: current Technology Use and Acceptance of Technology in Care. Int J Environ Res Public Health. 2021;18(6):3167. doi:10.3390/ijerph18063167
36. Pearse J, Chow J. An Internet of Things app for monitor unit calculation in superficial and orthovoltage skin therapy. IOP SciNotes. 2020;1(1):014002. doi:10.1088/2633-1357/ab8be0
37. Chow JCL, Li K. Large Language Models in Medical Chatbots: opportunities, Challenges, and the Need to Address AI Risks. Information. 2025;16(7):549. doi:10.3390/info16070549
38. World Health Organization. Global action plan on the public health response to dementia 2017–2025. 2017.
39. Hinton L, Nguyen H, Nguyen HT, et al. Advancing family dementia caregiver interventions in low- and middle-income countries: a pilot cluster randomized controlled trial of Resources for Advancing Alzheimer’s Caregiver Health in Vietnam (REACH VN). Alzheimers Dementia. 2021;6(e12063):1–8.
40. Brown E, Ruggiano N, Li J, Clarke P, Kay E, Hristidis V. Smartphone-Based Health Technologies for Dementia Care: opportunities, Challenges, and Current Practices. J Appl Gerontol. 2017;38:073346481772308. doi:10.1177/0733464817723088
41. Zgonec S. Mobile apps supporting people with dementia and their carers: literature Review and Research Agenda. IFAC-PapersOnLine. 2021;54(13):663–668. doi:10.1016/j.ifacol.2021.10.527
42. Statista. Penetration rate of leading social media apps among internet users in Vietnam as of 3rd quarter of 2024. 2025. July 9th, 2025. Updated June 24, Available from: https://www.statista.com/statistics/941843/vietnam-leading-social-media-platforms/.
43. Word Health Organization. iSupport For Dementia. Training and support manual for carers of people with dementia. 2019.
44. Lovibond S, Lovibond P. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy. 1995;33(3):335–343. doi:10.1016/0005-7967(94)00075-u
45. McParland P, Devine P, Innes A, Gayle V. Dementia knowledge and attitudes of the general public in Northern Ireland: an analysis of national survey data. Research Support, Non-U S Gov’t. Inter Psychogeria. 2012;24(10):1600–1613. doi:10.1017/S1041610212000658
46. Bédard M, Molloy DW, Squire L, Dubois S, Lever JA, O’Donnell M. The Zarit Burden Interview: a new short version and screening version. Gerontologist. 2001;41(5):652–657. doi:10.1093/geront/41.5.652
47. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The Multidimensional Scale of Perceived Social Support. JPersonal Asses. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
48. Tran TD, Tran T, Fisher J. Validation of the depression anxiety stress scales (DASS) 21 as a screening instrument for depression and anxiety in a rural community-based cohort of northern Vietnamese women. BMC Psychiatry. 2013;13(1):24. doi:10.1186/1471-244x-13-24
49. Thi Hue Man V, Nakamura K, Seino K, Nguyen HTL, Van Vo T. Fear of falling and cognitive impairment in elderly with different social support levels: findings from a community survey in Central Vietnam. BMC Geriatr. 2020;20(1):141. doi:10.1186/s12877-020-01533-8
50. Ta N, Nguyen H, Pham T, Nguyen TH, Hinton L. A cluster randomized controlled trial to test the feasibility and preliminary effectiveness of a family dementia caregiver intervention in Vietnam: the REACH VN study protocol. Medicine. 2018;97(42):e12553. doi:10.1097/md.0000000000012553
51. Fuller-Tyszkiewicz M, Richardson B, Little K, et al. Efficacy of a Smartphone App Intervention for Reducing Caregiver Stress: randomized Controlled Trial. JMIR Ment Health. 2020;7(7):e17541–e17541. doi:10.2196/17541
52. Ahmad SA, Kabir ZN, Tyrrell M, Craftman Å, Nasreen HE. Efficacy of a Telephone-Intervention on Caregiving Burden and Mental Health among Family Caregivers of Persons with Dementia in Malaysia: a Randomized Controlled Trial. Int J Environ Res Public Health. 2024;21(10). doi:10.3390/ijerph21101354
53. Eaton C, Vallejo N, McDonald X, et al. User Engagement With mHealth Interventions to Promote Treatment Adherence and Self-Management in People With Chronic Health Conditions: systematic Review. J Med Internet Res. 2024;26:e50508. doi:10.2196/50508
54. Chow JCL, Sanders L, Li K. Impact of ChatGPT on medical chatbots as a disruptive technology. Opin Front Artifi Intellig. 2023;2023:1.
55. Zada T, Tam N, Barnard F, Van Sittert M, Bhat V, Rambhatla S. Medical Misinformation in AI-Assisted Self-Diagnosis: development of a Method (EvalPrompt) for Analyzing Large Language Models. JMIR Form Res. 2025;9:e66207. doi:10.2196/66207
56. Than TN, Nguyen TT, Nguyen TC, et al. Smartphone app-based intervention for reducing stress, depression, and anxiety in caregivers of people with dementia in Vietnam: study protocol for a pilot randomized controlled trial. Digital Health Jan-Dec. 2023;9:20552076231163786. doi:10.1177/20552076231163786
57. Nguyen T, Nguyen H. Smartphone App-Based Psychoeducation for Caregivers of People with Dementia in Vietnam: a Pilot Randomized Controlled Trial. Clin Interventions Aging. 2025;20:1647–1660. doi:10.2147/CIA.S551994
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.