Back to Journals » Advances in Medical Education and Practice » Volume 17
Mixed-Methods Evaluation of Programmatic Interventions on Academic Performance and Resident Perspectives in Internal Medicine Residency
Authors Al Alawi AM, Al Busaidi S, Kashoub M, Al Sarmi G, Al-Busaidi IS, Al Balushi NA, Al Rawahi M ![]()
Received 24 November 2025
Accepted for publication 6 March 2026
Published 18 March 2026 Volume 2026:17 583981
DOI https://doi.org/10.2147/AMEP.S583981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Abdullah M Al Alawi,1– 3 Salim Al Busaidi,2 Masoud Kashoub,2 Ghadeer Al Sarmi,3 Ibrahim S Al-Busaidi,4 Nujood Abdullah Al Balushi,5 Mohamed Al Rawahi1– 3
1Medical Research Center, Sultan Qaboos University, Muscat, Oman; 2Department of Medicine, Sultan Qaboos University Hospital, Muscat, Oman; 3Internal Medicine Residency Training Program, Oman Medical Specialty Board, Muscat, Oman; 4Department of Primary Care and Clinical Simulation, University of Otago, Christchurch, New Zealand; 5Department of Medicine, University of Galway, Galway, Ireland
Correspondence: Abdullah M Al Alawi, Medical Research Center, Sultan Qaboos University, PO Box: 141, PC: 123, Muscat, Oman, Tel +968-95384990, Email [email protected]
Background: The Oman Medical Specialty Board (OMSB) Internal Medicine Residency Program addressed challenges like fatigue, burnout, and academic stress by implementing programmatic changes. These interventions aimed to improve certification exam pass rates, scholarly productivity, and work-life balance, ultimately enhancing academic performance and resident well-being within the program.
Objective: To evaluate the impact of four integrated programmatic interventions—reduced duty hours (24-hour to 12-hour shifts), restructured academic days, simulation-based workshops, and enhanced research mentorship—on academic performance, scholarly productivity, well-being, and resident satisfaction in an IM residency program.
Methods: A mixed-methods study was conducted in the OMSB IM Residency Program during the 2022/23 academic year. Interventions included: (1) restructuring Internal Medicine Academic Days (IMAD) into full-day structured learning incorporating dedicated lectures (8 am-1 pm) and simulation-based workshops (1– 3 pm), (2) reducing duty hours from 24-hour to 12-hour shifts, and (3) enhancing research training and mentorship. The quantitative component analyzed 78 residents in the pre-intervention period and 114 residents in the post-intervention period, measuring OMSB Part 1, Part 2, and Objective Structured Clinical Examination (OSCE) pass rates, as well as annual peer-reviewed resident publications. Independent z-tests compared outcomes between periods (p < 0.05). The qualitative component included semi-structured interviews with 13 purposively selected residents (third and fourth-year trainees), analyzed using Braun and Clarke’s thematic framework.
Results: Part 2 exam pass rates significantly improved (85.0% to 98.0%, p = 0.014), and resident publications doubled (10.5 to 21.0 annually, p = 0.007). Interviews revealed reduced fatigue, better work-life balance, and improved satisfaction with academic days and simulations. However, concerns were raised regarding scheduling conflicts and continuity of care.
Conclusion: Structured educational and wellness-focused interventions improved academic outcomes, scholarly output, and resident well-being. These findings support integrating similar strategies into residency programs, though further research is needed to assess long-term sustainability and broader applicability.
Keywords: residency training, programmatic interventions, academic performance, resident well-being, simulation workshops, scholarly productivity
Background
Over the last few decades, there has been a shift in medical education toward competency-based frameworks as defined by the Accreditation Council for Graduate Medical Education (ACGME) in the United States.1,2 The ACGME identifies six core competencies: professionalism, patient care, medical knowledge, interpersonal and communication skills, system-based care, and practice-based learning and improvement. Recently, the ACGME has introduced milestones to guide progression and development aligned with these core competencies.3 However, several challenges impede the effective implementation of competency-based graduate (ie. specialty, residency) medical education, including the evaluation of certain competencies (eg., system-based practice) and the need for flexible timeframes to achieve these goals.1,4
Residency programs face a range of obstacles that hinder the achievement of optimal training outcomes. Fatigue remains one of the most prominent issues negatively impacting residents’ overall well-being and academic performance.5 Similarly, burnout represents a substantial threat to residents’ mental and emotional resilience.6 Balancing professional commitments with personal life continues to be a major challenge, compounded by pressures to engage in scholarly activities such as research and publication.7 Additionally, preparing for certification examinations demands strategic preparation and consistent dedication.8 Addressing these multifaceted challenges is crucial for optimizing residency training programs’ outcomes and overall success.
While individual interventions show promise, evidence suggests that comprehensive, multi-faceted approaches are most effective for promoting resident well-being and educational outcomes. Goldman et al (2018) developed an intervention framework demonstrating that programs addressing duty hours, fatigue management, well-being support, and educational quality simultaneously achieve better outcomes than single interventions.9 This comprehensive approach requires commitment from both programs and institutions to prioritize physician well-being, ensure protected time with patients, minimize non-physician obligations, and provide residents with access to support services.9
Tariq et al, in a study conducted in Pakistan, modified work hours and introduced structured educational activities such as Residents’ Hour, Residents’ Slide Session, Grand Rounds, Journal Clubs, and Clinicopathological conferences10 These interventions improved postgraduate examination pass rates from 59.2% to 86.4%.10 Similarly, Murakami et al, in a study conducted in Japan, demonstrated the benefits of combining simulation-based education and peer-assisted learning in enhancing residents’ satisfaction and knowledge retention during emergency duties, though no significant differences were noted in clinical performance.11
The Oman Medical Specialty Board (OMSB) manages 18 postgraduate residency training programs in Oman, including a four-year Internal Medicine (IM) Residency Training Program accredited by the ACGME. With a commitment to ensuring training excellence, the OMSB regularly evaluates the knowledge, skills, and attitudes of approximately 570 residents to ensure that individual residents are progressing satisfactorily and meeting the required competency standards for their respective training levels.12
The performance of the IM Residency Program is reviewed annually by the Program Evaluation Subcommittee, with periodic reviews by OMSB and ACGME. Data for these reviews are collected through surveys from trainers and trainees, academic records, reports, and assessments of residents’ scholarly achievements. Key areas for improvement include certification exam pass rates, scholarly performance, and managing residents’ fatigue and work-life balance. High OMSB exam failure rates were noted. Burnout and fatigue were highlighted due to excessive workload, prolonged duty hours, and insufficient recovery time, negatively impacting well-being and learning. Limited research engagement was also identified, with residents facing challenges in publishing their projects due to lack of structured mentorship, time constraints, and unclear research guidance.
To address these concerns, the OMSB IM Residency Program implemented a series of targeted interventions during the 2022/23 academic year. Prior to restructuring, academic days were conducted on a weekly basis (1–3 pm) at the training sites. However, these sessions lacked protected time and were scheduled alongside other clinical work, resulting in poor attendance and inconsistent participation. Additionally, these sessions were delivered by faculty without a comprehensive, structured curriculum. The program restructured these into dedicated, full-day Internal Medicine Academic Days (IMAD) with protected time, clearly defined learning objectives, and comprehensive content including lectures, case-based problem-solving sessions, simulation workshops, and dedicated sessions on research methods, wellness, and leadership development.
Despite the growing body of evidence supporting individual interventions, significant gaps remain in the literature. Few studies have simultaneously evaluated the impact of comprehensive programmatic interventions on multiple outcome domains including academic performance, scholarly productivity, resident well-being, and satisfaction.9,13 Additionally, most research on residency interventions has been conducted in Western contexts, with limited evidence from Middle Eastern residency programs. Furthermore, while duty hour restrictions and educational interventions have been extensively studied, long-term sustainability of comprehensive interventions and their broader applicability across diverse settings remain unclear. Finally, qualitative research exploring residents lived experiences with programmatic changes is limited, particularly in non-Western educational contexts.
The Oman Medical Specialty Board (OMSB) Internal Medicine (IM) Residency Program, accredited by the ACGME, identified specific performance gaps that prompted this comprehensive evaluation. These included: (1) historically high certification exam failure rates, particularly in OMSB IM Part 1 and Part 2 examinations; (2) limited scholarly productivity with few residents publishing in peer-reviewed journals; and (3) resident reports of fatigue, burnout, and poor work-life balance. To address these interconnected challenges, the program implemented a comprehensive intervention package combining reduced duty hours (from 24-hour to 12-hour shifts), restructured academic days, simulation-based learning, and enhanced research support. This study was conducted to systematically evaluate whether these programmatic changes could simultaneously improve academic outcomes, scholarly productivity, and resident well-being—outcomes that are rarely evaluated together in the literature, particularly in Middle Eastern medical education contexts.
Methods
Study Design
This study adopted a pragmatic research paradigm focused on practical solutions and real-world outcomes. We employed a mixed-methods approach combining quantitative methods (examination pass rates and publication metrics) with qualitative methods (semi-structured interviews). The integration of methods occurred at the design level (concurrent data collection), analysis level (separate statistical and thematic analysis), and interpretation level (synthesis of findings). This approach enabled triangulation of findings to comprehensively evaluate the programmatic interventions’ impact on academic performance, scholarly activities, well-being, and work-life balance.
Programmatic Interventions
The IM Residency Program implemented targeted programmatic changes during the 2022/23 academic year to address several identified challenges. These interventions aimed to enhance academic performance, reduce fatigue, and promote scholarly activities, while fostering a better work-life balance among residents. These changes included:
The programmatic interventions included the following four main components:
- Internal Medicine Academic Days (IMAD): IMAD sessions are conducted weekly on Mondays, with residents divided into four groups by training level (R1+R2 Groups A and B; R3+R4 Groups A and B). Each resident attends one IMAD per academic block (4 weeks). Each full-day session includes: (a) Dedicated lectures and case-based problem-solving (8 am-1 pm) covering clinical skills, research methods, wellness, and leadership; and (b) Simulation-based workshops (1–3 pm) for clinical skill development. Content is recorded and made available on the Tebyan academic platform for asynchronous access. The IMAD curriculum includes integrated exam preparation activities designed to enhance residents’ readiness for OMSB certification examinations. These activities include faculty-led board review sessions, regular quizzes, and mock examinations. Board reviews are structured, faculty-led sessions that focus on high-yield topics and key content areas covered in the OMSB certification examinations (OMSB IM Part 1, Part 2, and OSCE). Routine multiple-choice questions (MCQs) aligned with ongoing education are administered, and mock examinations familiarize residents with board exam formats and enhance both clinical skills and confidence. The IMAD employs a blended pedagogical approach combining, case-based problem-solving discussions, and simulation-based active learning, ensuring that residents engage in active learning and collaborative problem-solving rather than passive knowledge reception.
- Reduced working hours: Working hours were restructured from 24-hour continuous shifts followed by one day off to a maximum of 12-hour shifts with increased frequency of days off, while maintaining similar total weekly working hours (35–45 hours per week). The program identified peak-demand clinical periods and adjusted the frequency and distribution of on-call duties accordingly. For night-shift coverage, residents work two consecutive night shifts in rotation, ensuring adequate staffing while maintaining protected rest periods.
- Research training and support: To promote research and scholarly activity, the program redesigned the research manual. Previously, the manual focused on stating program requirements and completion criteria. The redesigned manual now provides comprehensive, step-by-step guidance covering research idea selection, proposal writing, data analysis, manuscript preparation, and publication processes. The program also introduced dedicated IMAD sessions on research proposal and manuscript writing with structured mentorship and expert feedback. Residents are encouraged to participate in local and international conferences and contribute to peer-reviewed journals. Recognition of scholarly contributions is provided through certificates awarded at the annual Internal Medicine Research Day.
Setting
The study was conducted within the OMSB IM Residency Program, a four-year postgraduate training program accredited by the ACGME in the United States. The program accommodates up to 30 residents per training level (Residency year 1–4: R1, R2, R3, R4), with a total capacity of 120 residents across the program. Its curriculum integrates rigorous academic, clinical, and research training through the four main programmatic interventions: structured IMAD with integrated simulation-based workshops, reduced working hours, and enhanced research training and support, preparing residents for comprehensive IM practice.
Quantitative Component
The quantitative analysis included 78 residents in the pre-intervention period (2020/2021 and 2021/2022 academic years), representing the total resident population in the OMSB IM Residency Program prior to the intervention. In the post-intervention period (2022/2023 and 2023/2024 academic years), 114 residents were active in the program, reflecting program growth and expansion during this period. For OMSB examinations, only first-time exam takers were analyzed to ensure consistency across the dataset. This approach minimized potential bias from repeat test-takers, who may have had varied levels of prior exposure and preparation, ensuring a fair and reliable comparison of academic performance before and after the interventions. Research productivity data were retrieved from the IM office and supplemented by conducting a comprehensive PubMed search using initials (first and last name) and affiliations (OMSB) to capture all publications by residents included in this study. Descriptive statistics were calculated for performance metrics, including OMSB IM Part 1, Part 2, and OSCE pass rates, as well as the number of peer-reviewed journal publications per year, before and after the intervention. Independent z-tests for proportions were used to compare pass rates between groups. Statistical significance was set at p < 0.05. Statistical analyses were performed using STATA version 17.0 (STATA Corporation, College Station, TX, USA).
Qualitative Component
The qualitative component was designed to align with the study’s primary objectives by exploring residents’ experiences with recent programmatic changes and their perceived effects on academic performance, scholarly productivity, well-being, and satisfaction. This qualitative analysis complements the quantitative findings by providing a deeper understanding of how residents experienced the interventions and their impact on training outcomes.
Residents were purposively selected using the following criteria: representation across different training levels (R3 and R4), both genders, and varying family structures and life circumstances. An interview guide was used, piloted on three residents excluded from the study, and the interview guide was finalized ensuring question validity and accuracy through input from the research team and is provided in (supplementary material 1).
One-on-one, in-person semi-structured interviews were conducted by an independent research assistant trained explicitly for the task and uninvolved in the programmatic changes. All interviews were recorded and transcribed using Otter.AI (Otter.AI, California, United States). These transcriptions were later corroborated for accuracy.
Qualitative data were analyzed using Braun and Clarke’s six-phase thematic analysis framework, employing an inductive approach. The analysis process involved the following steps: (1) Familiarization: Researchers became familiar with the data through repeated reading of transcripts and initial note-taking. (2) Initial coding: Systematic, line-by-line coding of interesting features across the entire dataset, generating initial codes that were data-driven and inductive. (3) Theme development: Collating codes into potential themes and sub-themes that captured meaningful patterns related to the study objectives. (4) Theme review: Reviewing and refining themes to ensure they were coherent, distinct, and well-supported by the data. (5) Theme definition and naming: Clearly defining each theme and assigning descriptive names. (6) Report production: Selecting compelling illustrative quotations and writing the analysis report.
A review of interview transcript was conducted until new interviews ceased to uncover new insights. Following the first three interviews, we performed a preliminary thematic analysis using Braun and Clarke’s framework, which included familiarization with the data and initial coding.14
The research team reviewed and refined the initial codes, themes, and sub-themes iteratively. This process produced an initial thematic map, which guided the analysis of subsequent interviews, with revisions made in a recursive manner throughout the data analysis. All interviews were coded and analysed by a research team member. Final themes were supported by illustrative quotations and detailed textural descriptions, with structural descriptions exploring underlying patterns.
Ethics
Residents in their third or fourth year of training, who had experienced the programmatic changes, were invited to participate by S.B.
Informed consent was obtained from all participants, allowing for the publication of anonymized responses and direct quotes. Residents provided written informed consent in person at the training sites before interviews began. They were informed that participation was voluntary, they could withdraw at any time without penalty, and their responses would remain confidential and anonymous.
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki and adheres to ethical guidelines for research involving human participants. The study received ethical approval from the Research and Innovation Committee of the Oman Medical Specialty Board (Ref. No.:RIC/03/2024).
Results
Characteristics of Interview Participants
A total of 13 residents participated in the qualitative interviews. The sample included residents from different training levels, with 8 R3 residents (third-year residents) representing, 5 R4 residents (fourth-year residents). Gender representation included 7 female residents,6 male residents. Participants ranged in age from 28 to 37 years, with a mean age of approximately 31 years. Regarding marital status, 7 residents were married, including those with children ranging from infants to school-age, 6 residents were single. Of the residents with confirmed parental status, five had children while three did not.
Quantitative Analysis
The quantitative analysis compared outcomes between the pre-intervention period (2020/2021 and 2021/2022, n=78 residents) and the post-intervention period (2022/2023 and 2023/2024, n=114 residents). The increase in resident numbers from 78 to 114 reflects program growth and expansion during the study period (Table 1 and Figure 1).
 |
Table 1 Comparison of Oman Medical Specialty Board (OMSB) Examination Pass Rates and Publication Metrics Before and After Programmatic Interventions |
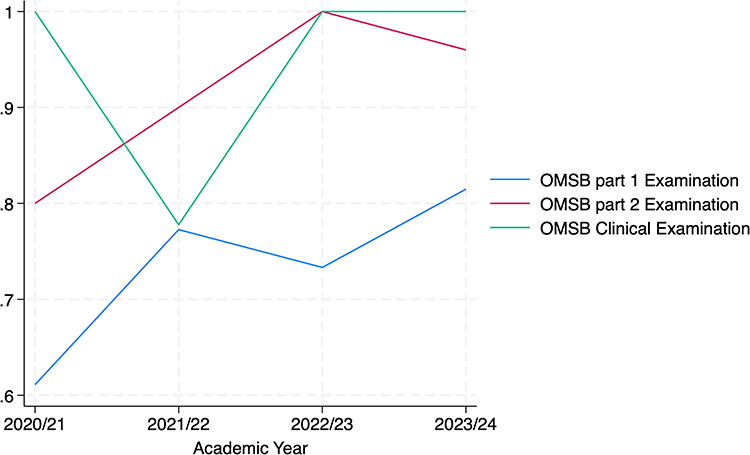 |
Figure 1 Trends in Oman Medical Specialty Board (OMSB) Examination Pass Rates Across Academic Years (2020/21–2023/24). Notes: Sample sizes represent first-time exam takers per academic year: 2020/21 (n=18 for Part 1, n=15 for Part 2, n=11 for OSCE), 2021/22 (n=22 for Part 1, n=10 for Part 2, n=9 for OSCE), 2022/23 (n=30 for Part 1, n=12 for Part 2, n=12 for OSCE), 2023/24 (n=27 for Part 1, n=25 for Part 2, n=24 for OSCE). |
The intervention led to notable improvements in several areas. The pass rate for OMSB IM Part 1 remained stable, with a slight increase from 70.0% (95% CI: 54.6–81.9%) pre-intervention to 77.2% (95% CI: 64.8–86.2%) post-intervention (p=0.25). However, the OMSB IM Part 2 pass rate showed a significant improvement, rising from 84.0% (95% CI: 65.3–93.6%) to 97.3% (95% CI: 86.2–99.5%) post-intervention (p=0.01). Additionally, OSCE pass rates increased from 90.0% (95% CI: 69.9–97.2%) to 100.0% (95% CI: 90.4–100.0%) post-intervention (p=0.05). Furthermore, the number of publications in peer-reviewed journals where residents contributed per year doubled from 10.5 to 21 (p=0.01), indicating enhanced scholarly activity (Table 2).
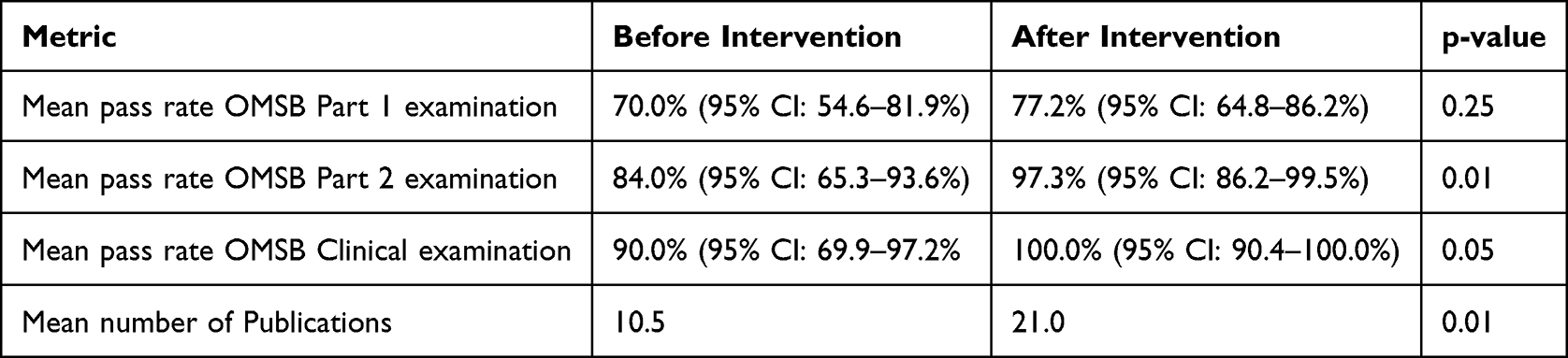 |
Table 2 Comparison of Performance Metrics Before After Implementation of the Programmatic Interventions |
Qualitative Analysis
Qualitative analysis of feedback from IM residents identified common themes which related to the perceived positive and negative effects of the interventions on their wellbeing, work-life balance, academic performance, and professional development. These are outlined below.
Academic Performance
Residents consistently reported that the shift from a half academic day to a full academic day enhanced their learning experience considerably, primarily by offering dedicated, uninterrupted time for education. This change allowed them to focus better on learning without the constant pull of clinical duties. As one resident noted:
Having a full day made us learn better and be more prepared.
The structured, distraction-free environment of the full academic day was particularly appreciated. Another resident shared:
We now have a full day and usually we know what our objective is… we are free to focus.
A key improvement was the timing of academic sessions. Previously scheduled in the late afternoon or after work hours, half-day sessions often conflicted with clinical responsibilities and were attended when residents were already fatigued. One resident reflected:
When it was half day, it was by the end of the day when we were already exhausted.
In contrast, with sessions now scheduled in the morning, residents felt more mentally prepared and engaged:
From morning when we’re fresh… we’re eager to learn.
Residents described the previous half-day format as being frequently interrupted, particularly for junior residents:
It was full of interruptions, especially when you are an R1 [first year resident] … you are the first encounter with the nurses and the patients.
This issue was greatly reduced in the new format:
You go there, and you can even switch off your phone… no more interruptions from the hospital.
The positive impact on academic performance and participation was another common theme. Residents reported better attendance, improved engagement, and stronger decision-making skills. One participant observed:
My attendance was poor when it was a half day… now the attendance is better, and the material quality has improved.
The full academic day also introduced a varied and engaging learning environment, including lectures, simulation sessions, and interactive workshops. One resident described the structure:
From eight we’ll start Lecture Series… later we’ll have simulations some of the weeks, which is really good.
Beyond the academic perspective the intervention also had a positive impact on resident well-being. Residents felt the program had become more supportive of their mental and physical health:
The program is more supportive now… the environment is healthier.
Finally, the full academic day facilitated stronger social and professional relationships, offering more opportunities for interaction and collaboration:
It has both educational and social benefits… it improved all relationships together.
Residents widely recognized the value of simulation sessions and hands-on workshops in improving their clinical performance, procedural confidence, and preparedness for real-life scenarios. These sessions were described as closely mirroring real-world situations, helping residents gain both technical skills and mental readiness for acute care settings.
One resident summarized this impact by stating:
Simulation sessions are great—they simulate whatever we face in reality.
Another highlighted how these activities translated into better performance during critical times:
Learning these techniques and doing hands-on sessions improved our work during on-calls and stressful times.
The sessions were also credited with increasing residents’ confidence:
They made us more confident during procedures and helped us do them better.
Furthermore, the simulations helped residents feel more equipped to handle emergencies and critically ill patients:
The simulations of stressful and crashing patients were really helpful in preparing us for those real situations.
Overall, these reflections suggest that simulation-based education significantly enhanced clinical readiness, reduced anxiety during high-pressure encounters, and strengthened procedural competence.
Scholarly Productivity
Residents emphasized the positive impact of enhanced research support, particularly the introduction of dedicated research sessions during academic days and the redesign of the research manual. These changes were seen as making research more accessible and organized, especially for new residents.
One Resident Shared
The redesigned research manual made it very easy to find a supervisor. Trainers posted their topics, and you could sign up, which exposed us to a variety of research areas.
Residents also appreciated the targeted research skills training integrated into the academic program:
We had sessions on how to write a manuscript, critical appraisal, and how to validate research questions—it helped me a lot.
This structured support was especially valued by newer residents:
The new R1s are lucky—they have clear guidance on how to write proposals, do analysis, and prepare manuscripts. These sessions are essential in residency.
However, the research matching system, where incoming residents are paired with consultants based on pre-set topics, received mixed feedback. Some felt it limited flexibility and ownership:
When I was an R1, I approached a consultant myself and we created a title. Now they just get matched with projects the consultants want to do.
Residents also pointed out areas needing improvement, particularly in the timing and structure of research activities:
It’s scheduled very wrong—we don’t get the full benefit, and it definitely still needs improving.
It’s good overall, but there should be more emphasis on data collection and analysis.
Well-Being and Satisfaction
A prominent theme among residents was the positive impact of reducing duty hours from 24-hour to 12-hour shifts, particularly in relation to fatigue, mental well-being, work-life balance, academic performance, and patient safety.
Residents consistently described 24-hour calls as exhausting and mentally taxing. One remarked,
The 24-hour duty is more hectic.
The shift to 12-hour duties was seen as relieving both physical and emotional burden, with residents reporting more time for rest, family, and studying. One resident noted,
We have much more time for studying and family time.
Another emphasized the reduction in fatigue and improved focus:
With the shortened duty calls, the fatigue is much less.
The psychological benefits were also highlighted:
Mentally, it’s a lot more relaxed, less stress, more time for socializing.
In terms of academic performance, residents felt better equipped to concentrate and prepare for exams:
It helps improve academic performance in different ways.
We’re able to make decisions in a good amount of time because we’re not exhausted.
The impact extended to patient care and safety, as reduced fatigue was perceived to enhance attentiveness and reduce medical errors. One resident reflected:
Patient care has improved—you’re giving these doctors a 50% reduction in the time and more focus on their patients.
Another shared a critical incident illustrating the risks of exhaustion under the previous 24-hour model:
I gave a patient potassium, and he had advanced kidney disease. The next day, his potassium level was almost seven—it was really dangerous.
Despite overall satisfaction with the reduced shifts, some residents expressed concerns about team dynamics, continuity of care, and workload distribution—particularly with the introduction of the night floater system. One resident explained:
This year, because of the night floater and double shift system, we had fewer residents during working hours as some were on night call.
Others noted mixed experiences regarding continuity of care and handovers. One resident expressed a preference for the continuity offered by longer shifts, stating:
“For me, I like to have control of my 24 hours to minimize the handover time,” indicating a preference for continuous patient care management over the new fragmented shift system.
Some residents felt that communication and teamwork had improved under the new system:
Actually, it improved the team dynamics. There’s more communication and better organization than before.
Overall, the reduction in duty hours was viewed as a beneficial intervention that improved well-being, academic engagement, and patient care. However, a nuanced perspective emerged, with some residents—particularly seniors—valuing longer shifts for continuity, and others highlighting operational challenges related to team structure and on-call coverage.
As part of the restructured Internal Medicine Academic Days (IMAD), residents participated in integrated exam preparation activities including faculty-led board review sessions, regular quizzes, and mock examinations. Residents shared generally positive feedback regarding these exam preparation strategies, particularly the board reviews, quizzes, and mock exams, which were introduced as core components of the academic restructuring. These tools were seen as instrumental in orienting residents to exam content, identifying knowledge gaps, and building confidence ahead of high-stakes assessments.
Board review sessions were widely valued for highlighting key topics and helping residents focus their study efforts. As one resident explained:
Board reviews help us to orient ourselves on the most important topics to study, and they supported our preparation very much.
Others emphasized the benefit of repetition and structured review:
It was very helpful to go through the board review last year—attending it the first time and reviewing it again a second or third time helped a lot.
However, some residents raised concerns about session length and delivery, suggesting the format could be improved:
I’m not a fan of the current board review sessions. They are too long and often not finished. They should be condensed and more structured.
There was strong consensus on the need to record sessions to improve accessibility for residents on duty:
They need to be recorded and held regularly. If they’re limited to three hours and accessible anytime, that would help everyone.
Regular quizzes were appreciated by many residents for promoting self-assessment and consistent study habits:
Quizzes are really good—they give me insight into where I stand and what I need to study more.
Even when we were tired, quizzes encouraged us to keep reading.
However, not all residents found quizzes as beneficial. One shared a more individual preference:
I didn’t benefit much from quizzes. I found them stressful. Maybe allowing residents to study in their own preferred way would be better.
Mock exams received unanimous praise for simulating the exam environment and familiarizing residents with question types. As one participant stated:
Mock exams were very useful—they helped a lot in exam preparation and reduced anxiety about the real test.
Unlike the positive perceptions of research support, feedback on professional development sessions was less favorable. Residents felt these sessions were often too general and not practically helpful, with some needing to seek individual support to get their questions answered. As one participant noted:
These sessions were not very beneficial. I still had to go one-on-one to the research people and ask the same questions again.
Residents consistently reported that the programmatic interventions, especially the shift to 12-hour duty schedules, had a positive effect on their mental, emotional, and physical well-being. Despite some increase in the number of on-call days, residents described feeling less stressed and more in control of their time.
One Resident Noted
Physically and emotionally, I feel much better now.
Another Shared
Even with more on-calls, the stress has been less.
Time for rest, family, and personal life significantly improved, leading to better work-life balance and reduced burnout:
With the 12-hour shift, I have more free time. I can now visit my parents and have time for myself.
Social time is much better—we still have time to meet our family and practice hobbies before our shifts.
Residents also described improved time management and academic performance, suggesting that the reduction in fatigue had spillover benefits in other areas:
My stress has significantly reduced, and my time management has improved with the changes in duty hours.
It helped in academic performance and studying.
Finally, several participants expressed overall satisfaction with the interventions, emphasizing the broader impact on their quality of life:
This is affecting our personal life positively.
Mentally, it’s more relaxed, less stress, and more time for family and socializing.
Discussion
This mixed-methods study assessed the impact of a comprehensive programmatic intervention on Internal Medicine residents, focusing on academic performance, scholarly productivity, well-being, and satisfaction. The intervention led to stable pass rates for OMSB IM Part 1, while OMSB IM Part 2 and OSCE pass rates showed significant improvements. Scholarly productivity, as measured by peer-reviewed publications, increased substantially. Qualitative findings highlighted residents’ perceived improvements in well-being, work-life balance, and overall satisfaction with the program. Key elements valued by residents included protected academic time, simulation-based learning, reduced duty hours, and enhanced research support. However, some concerns were raised about team dynamics and continuity of care under the new shift system. The study uniquely integrates academic performance, well-being, and scholarly activities to evaluate residency training holistically. It emphasizes innovative interventions like 12-hour shift rotations and academic days, balancing educational and clinical demands. By focusing on residents lived experiences, the study adds a humanistic perspective often missing in quantitative research. Situated within an accredited program in Oman, it offers valuable insights into regional residency training challenges and solutions.
Prior research on residency interventions is sparse but indicates potential benefits from approaches such as structured reading and remedial programs to enhance exam performance, increasing interprofessional familiarity to boost team performance and communication, and shared decision-making training to enhance knowledge and attitudes.15,16 Additionally, burnout reduction techniques such as work-hour restrictions, self-care workshops, wellness initiatives incorporating peer support, and research productivity enhancements through leadership roles and structured curricula are effective.17,18
The quantitative analysis revealed notable improvements post-intervention, with OMSB IM Part 2 pass rates improving significantly and non- statistically significant improvement in OMSB IM Part 1 and OSCE examinations.
Academic Performance and Scholarly Activities
In the OMSB Internal Medicine Residency Program, improvements were noted in historically high failure rates, likely due to structured academic days, board review sessions, regular assessments, and simulation-based training. Reduced duty hours may have lessened fatigue, enhancing study and exam preparation. These findings highlight the importance of structured training, optimized duty hours, and educational reforms in enhancing certification outcomes and resident competency. Future studies should evaluate the long-term impact of these interventions and explore further refinements.
The intervention, including the revision of the research manual, dedicated lectures on conducting research, mentor support, and a program emphasis on publication, led to a remarkable improvement in the number of publications in peer-reviewed journals. Enhancing scholarly activities in training programs is crucial for developing research skills and academic productivity. Key strategies include a structured research curriculum with dedicated rotations and statistical training, effective mentorship, and faculty involvement.19 Providing protected time and funding for research boosts publication rates.19,20
Longitudinal initiatives—sustained programmatic activities spanning the entire residency training period with measurable milestones monitored at regular intervals—and peer-led initiatives, such as resident peer research leaders, foster a research culture. Integrating quality improvement and patient safety projects throughout training enhances engagement through practical applications.21
Duty Hours
The reduction of duty hours from 24 to 12 improved fatigue, stress, work-life balance, and academic performance. However, some senior residents preferred longer shifts for continuity, and the night floater system affected team dynamics by decreasing daytime resident presence. While duty hour restrictions for medical residents aim to improve well-being and patient safety, the evidence shows mixed outcomes.22 There are noted improvements in resident wellness, yet the benefits for education and patient care are less clear, with some negative perceptions and outcomes reported, especially in surgical programs where concerns have been flagged about limited operating room exposure due to restricted working hours.23,24 Our study did not explore faculty perceptions or assess patient safety metrics, such as incident reports, highlighting areas for future research.
Academic Days
The introduction of full academic days improved residents’ learning by providing uninterrupted study time, boosting engagement, and enhancing performance through diverse activities like lectures and simulations. This approach strengthened social and professional relationships, with studies indicating increased resident satisfaction and perceived educational value. However, the impact on exam performance is mixed, and operational challenges remain to optimize these benefits.25,26 However, the impact on exam performance is mixed, and operational challenges need to be addressed to optimize the benefits of such educational models.27
Knowledge Assessments
Programmatic intervention included regular knowledge assessment tasks, such as quizzes, which are part of the minimum progression criteria and assessed every six months by the clinical competence committee. Previous studies demonstrated that quizzes, whether gamified or not, enhance engagement, satisfaction, and knowledge retention in internal medicine programs.28
Research and Scholarly Activities
Programmatic interventions supporting research included guidance through sessions and a research manual, with mixed feedback on pairing residents with consultants but appreciation for structured guidance, particularly in manuscript writing and analysis. Despite concerns about scheduling and structure, there was an improvement in residents’ projects published in peer-reviewed journals post-interventions. Previous studies have shown that structured research programs encourage residents to engage in scholarly activities, leading to higher rates of research presentations and publications.29,30 Research activities during residency improve critical thinking, analytical reading skills, and the ability to conduct data-intensive research, essential for lifelong learning and quality patient care. Residents gain experience in research design, statistical analysis, and manuscript preparation, valuable skills for both academic and clinical careers.31
Future research should develop and evaluate additional programmatic interventions to enhance residents’ research engagement and output. This includes addressing challenges in scheduling and research activity structure, with a focus on improving support for data collection and analysis. Tailored interventions like expanded guidance sessions, optimized pairing systems, and enhanced resources could build on observed improvements in publication rates.
Professional Development Sessions
Professional development sessions on leadership, time management, exam preparation, and career planning were introduced, but feedback indicated they need improvement due to their limited number and perceived lack of benefit. Previous studies have shown that professional development sessions help residents develop essential non-technical skills, such as communication, leadership, and professionalism, often overlooked in traditional training.32 These sessions support the integration of personal and professional values, enhance wellness, reduce burnout, increase sensitivity to ethical issues, and improve career planning skills, fostering a sense of community and professional identity.33,34
Simulation and Workshops
Residents recognized the considerable impact of simulation sessions and workshops on their clinical practice, enhancing clinical skills, boosting confidence, and positively influencing patient management in acute situations. Previous medical education research shows that simulation sessions also improve communication skills and teamwork among medical and nursing students, fostering better interprofessional collaboration.35 They are vital for developing technical expertise, particularly in emergency and procedural skills, and enhance clinical decision-making by providing realistic practice scenarios.36 Regular simulations support skill retention and competence, offering opportunities for deliberate practice.
Resident Well-Being
Programmatic interventions improved substantially residents’ self-reported well-being, time management, life satisfaction, social opportunities, academic performance, and professional capabilities while reducing stress and enhancing personal and family life.
Burnout remains a prevalent issue in residency, particularly in surgical and high-stress specialties, leading to career dissatisfaction and increased medical errors.37,38 It causes emotional exhaustion and depersonalization, impacting mental health and performance. Factors such as heavy workloads, high stress, poor work-life balance, and night shifts contribute to burnout.39 Effective interventions include wellness training, stress management, mentoring, and organizational changes to reduce workload and enhance support.40 While this study highlights positive outcomes in resident well-being, further research should explore well-being in greater depth.
Strengths and Limitations
This study’s strengths include its comprehensive mixed-methods approach, integrating quantitative and qualitative insights to evaluate innovative, resident-centered interventions. It also contributes valuable data to the limited research on residency training in Oman and similar settings.
A key limitation is the inability to control for all potential confounders in a before-and-after intervention analysis. However, resident ability differences were unlikely to impact results, as the OMSB Internal Medicine Residency Program’s admission process remained unchanged throughout the study period. Candidate selection follows a rigorous, standardized process, including structured examinations and formal interviews, ensuring consistent competency levels across cohorts. Similarly, exam difficulty remained stable, as the OMSB assessments undergo a standardized review process, with centrally managed question banks, expert validation, and Angoff-based pass threshold determination. These factors minimize variability and support the interpretation that improvements were due to the interventions rather than cohort differences.
Other limitations include limited generalizability to other residency programs, the short follow-up period precluding long-term impact assessment, and the lack of faculty perspectives or patient safety evaluations. Future research should incorporate cohort-matching or prior academic performance adjustments and explore the long-term sustainability of these interventions.
Conclusion
This study highlights the transformative impact of targeted interventions in IM residency programs. This evaluation suggested that, by reducing duty shift lengths, introducing structured academic days, and promoting scholarly activity, the program resulted in improved exam performance, research output, and reported well-being. Qualitative analysis indicated positive effects on personal and professional lives. The study contributes to the medical education literature and provides a replicable framework for balancing academic rigor with personal and professional development. Future research should assess long-term sustainability and explore broader impacts, including faculty feedback and patient outcomes, to further validate these findings.
Abbreviations
ACGME, Accreditation Council for Graduate Medical Education; COREQ, Consolidated Criteria for Reporting Qualitative Research; IM, Internal Medicine; IMAD, Internal Medicine Academic Days; OMSB, Oman Medical Specialty Board; OSCE, Objective Structured Clinical Examination; R1, First-Year Resident; SQUH, Sultan Qaboos University Hospital.
Acknowledgments
We would like to express our heartfelt gratitude to the Internal Medicine Chief Residents for their dedication and hard work in achieving these programmatic interventions, which required immense effort and commitment. Our sincere thanks extend to the Internal Medicine Residents, the future of our healthcare system, for their active participation and contributions. We also deeply appreciate the support of the members of the Internal-Medicine Educational Committee, who played a pivotal role in supporting all interventions. Our gratitude goes to the Internal Medicine Faculty for their unwavering dedication and endless support throughout this journey. We acknowledge the Oman Medical Specialty Board for their support of this study and providing all data required, granting ethical approval, and to Sultan Qaboos University for funding this project. Finally, we extend special thanks to the Internal Medicine Residents who agreed to be interviewed, providing invaluable insights that enriched this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Ethical statement study received ethical approval from the Research and Innovation Committee of the Oman Medical Specialty Board (Ref. No: RIC/03/2024). Participation was voluntary, with participants free to withdraw at any time. Consent was obtained from those who chose to participate. To ensure privacy, participant data were de-identified and stored using a unique numbering system. The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Funding
This study received the Dean’s research grant from Sultan Qaboos University (Grant No. RF/MED/MEDE/24/04).
Disclosure
The authors declare that there are no competing interests. This paper has been uploaded to ResearchGate as a preprint: [https://www.researchgate.net/publication/389359537_Comprehensive_Evaluation_of_Programmatic_Interventions_in_Internal_Medicine_Residency_A_Mixed-Methods_Analysis_of_Academic_Performance_Well-being_and_Resident_Perspectives_Background].
References
1. Whitcomb ME. Internal medicine residency redesign: time to take stock. Ann Intern Med. 2010;153(11):759–16. doi:10.7326/0003-4819-153-11-201012070-00011
2. Norman G. Medical education: past, present and future. Perspect Med Educ. 2012;1(1):6–14. doi:10.1007/S40037-012-0002-7
3. Edgar L, Roberts S, Yaghmour NA, et al. Competency crosswalk: a multispecialty review of the accreditation council for graduate medical education milestones across four competency domains. Acad Med. 2018;93(7):1035–1041. doi:10.1097/ACM.0000000000002059
4. Baum KD, Axtell S. Trends in North American medical education. Keio J Med. 2005;54(1):22–28. doi:10.2302/kjm.54.22
5. Perez AR, Boscardin CK, Pardo M. Residents’ challenges in transitioning to residency and recommended strategies for improvement. J Educ Perioper Med. 2022;24(1):E679. doi:10.46374/volxxiv_issue1_boscardin
6. Taylor TS, Watling CJ, Teunissen PW, Dornan T, Lingard L. Principles of fatigue in residency education: a qualitative study. CMAJ Open. 2016;4(2):E200–204. doi:10.9778/cmajo.20150086
7. Nair SC, Ibrahim H, Almarzoqi F, Alkhemeiri A, Sreedharan J. Addressing research barriers and facilitators in medical residency. J Family Med Prim Care. 2019;8(3):1145–1150. doi:10.4103/jfmpc.jfmpc_38_19
8. Seaberg PH, Kling JM, Klanderman MC, et al. Resident factors associated with American board of internal medicine certification exam failure. Med Educ Online. 2023;28(1):2152162. doi:10.1080/10872981.2022.2152162
9. Goldman ML, Bernstein CA, Konopasek L, Arbuckle M, Mayer LES. An intervention framework for institutions to meet new ACGME common program requirements for physician well-being. Acad Psychiatry. 2018;42(4):542–547. doi:10.1007/s40596-018-0882-x
10. Tariq M, Syed NA, Motiwala A, et al. Effectiveness of educational interventions in improving clinical competence of residents in an internal medicine residency program in Pakistan. Educ Health. 2011;24(3):573. doi:10.4103/1357-6283.101420
11. Murakami T, Yamamoto A, Hagiya H, et al. The effectiveness of simulation-based education combined with peer-assisted learning on clinical performance of first-year medical residents: a case-control study. BMC Med Educ. 2023;23(1):859. doi:10.1186/s12909-023-04798-w
12. Al Rawahi A, Panchatcharam SM, Jose S. Research publications of the Oman medical specialty board. Oman Med Journal. 2021;36(2):e237. doi:10.5001/omj.2021.17
13. Fletcher KE, Reed DA, Arora VM. Patient safety, resident education and resident well-being following implementation of the 2003 ACGME duty hour rules. J Gen Intern Med. 2011;26(8):907–919. doi:10.1007/s11606-011-1657-1
14. Braun B CV.Using thematic analysis in psychology. In. Volume 2, edn. 2006
15. Iyasere CA, Wing J, Martel JN, Healy MG, Park YS, Finn KM. Effect of increased interprofessional familiarity on team performance, communication, and psychological safety on inpatient medical teams: a randomized clinical trial. JAMA Intern Med. 2022;182(11):1190–1198. doi:10.1001/jamainternmed.2022.4373
16. Funke Folorunsho E, Walsh C, Ostlundh L, et al. Understanding the impact of medical educational interventions in training shared decision making for residents. Int Med J. 2022;29(3).
17. Busireddy KR, Miller JA, Ellison K, Ren V, Qayyum R, Panda M. Efficacy of interventions to reduce resident physician burnout: a systematic review. J Graduat Med Educ. 2017;9(3):294–301. doi:10.4300/JGME-D-16-00372.1
18. Eskander J, Rajaguru PP, Greenberg PB. Evaluating wellness interventions for resident physicians: a systematic review. J Graduat Med Educ. 2021;13(1):58–69. doi:10.4300/JGME-D-20-00359.1
19. Abramson E, Weiss P, Mauer E, et al. 1. Scholarly activity training during fellowship: a national assessment. Academic Pediat. 2020;20.
20. Abramson E, Weiss P, Naifeh M, et al. Scholarly activity during pediatric fellowship. Pediatrics. 2020;20:147. doi:10.1186/s12887-020-02036-6
21. Suero-Abreu GA, Barajas-Ochoa A. The value of the chief resident in successful resident-led quality improvement and patient safety scholarly initiatives. J Gen Intern Med. 2021;36(12):3880–3881. doi:10.1007/s11606-021-07148-y
22. Ahmed N, Devitt KS, Keshet I, et al. A systematic review of the effects of resident duty hour restrictions in surgery: impact on resident wellness, training, and patient outcomes. Ann Surg. 2014;259(6):1041–1053. doi:10.1097/SLA.0000000000000595
23. Mauser NS, Michelson JD, Gissel H, Henderson C, Mauffrey C. Work-hour restrictions and orthopaedic resident education: a systematic review. Int Orthopaedics. 2016;40:865–873. doi:10.1007/s00264-015-3045-7
24. Weiss P, Kryger M, Knauert M. Impact of extended duty hours on medical trainees. Sleep Health. 2016;2(4):309–315. doi:10.1016/j.sleh.2016.08.003
25. DeBord JM, Schwartz A, King B, Frohna J, Shutak C, Borman-Shoap E. 38. Impact of academic half-day curricula on pediatric resident exam performance. Academic Pediat. 2020;20(7):e19. doi:10.1016/j.acap.2020.06.059
26. Randall MH, Schreiner AD, Clyburn EB, Rockey DC, Duckett A. Effects of an academic half day in a residency program on perceived educational value, resident satisfaction and wellness. Am J Med Sci. 2020;360(4):342–347. doi:10.1016/j.amjms.2020.05.013
27. Wagoner H, Seltz B. Attending physicians’ perspectives of resident academic half day. Teach Learn Med. 2019;31(3):270–278. doi:10.1080/10401334.2018.1551140
28. Romero‐Alemán M-D-M. Romero‐Alemán MdM: a pilot study on gamified and conventional e‐quizzes reinforcing human histology among first‐year medical and physiotherapy students. Anatomic Sci Educ. 2024;17(4):844–854. doi:10.1002/ase.2406
29. Haas DM, Hadaie B, Ramirez M, Shanks AL, Scott NP. Resident research mentoring teams: a support program to increase resident research productivity. J Graduat Med Educat. 2023;15(3):365–372. doi:10.4300/JGME-D-22-00499.1
30. Reulen H-J. The role of research in the training of residents. Eur Surg Res. 2002;34(1–2):13–17. doi:10.1159/000048881
31. Alguire PC, Anderson WA, Albrecht RR, Poland GA. Resident research in internal medicine training programs. Ann Internal Med. 1996;124(3):321–328. doi:10.7326/0003-4819-124-3-199602010-00007
32. Dijkhuizen K, Bustraan J, de Beaufort AJ, Velthuis SI, Driessen EW, van Lith JM. Encouraging residents’ professional development and career planning: the role of a development-oriented performance assessment. BMC Med Educ. 2018;18:1–8. doi:10.1186/s12909-018-1317-9
33. El Metwally D, Azzam M, Al‐Seoud A. Medical professionalism adapted to faith and cultural beliefs. Medical Education. 2012;46(5):524–525. doi:10.1111/j.1365-2923.2012.04249.x
34. Brauch RA, Goliath C, Patterson L, Sheers T, Haller N. A qualitative study of improving preceptor feedback delivery on professionalism to postgraduate year 1 residents through education, observation, and reflection. Ochsner J. 2013;13(3):322–326.
35. Bagnasco A, Pagnucci N, Tolotti A, Rosa F, Torre G, Sasso L. The role of simulation in developing communication and gestural skills in medical students. BMC Med Educ. 2014;14:1–7. doi:10.1186/1472-6920-14-106
36. Offiah G, Ekpotu LP, Murphy S, et al. Evaluation of medical student retention of clinical skills following simulation training. BMC Med Educ. 2019;19:1–7. doi:10.1186/s12909-019-1663-2
37. IsHak WW, Lederer S, Mandili C, et al. Burnout during residency training: a literature review. J Graduat Med Educ. 2009;1(2):236–242. doi:10.4300/JGME-D-09-00054.1
38. Shanafelt TD, Bradley KA, Wipf JE, Back AL. Burnout and self-reported patient care in an internal medicine residency program. Ann Internal Med. 2002;136(5):358–367. doi:10.7326/0003-4819-136-5-200203050-00008
39. Ogundipe O, Olagunju A, Lasebikan V, Coker A. Burnout among doctors in residency training in a tertiary hospital. Asian J Psych. 2014;10:27–32. doi:10.1016/j.ajp.2014.02.010
40. Lu F-I, Ratnapalan S. Burnout interventions for resident physicians: a scoping review of their content, format, and effectiveness. Arch Pathol Lab Med. 2023;147(2):227–235. doi:10.5858/arpa.2021-0115-EP
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.