Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Mismatch Negativity and Auditory Brain Stem Response in Children with Autism Spectrum Disorders and Language Disorders
Authors Kabil SE ![]() , Abdelshafy R, Ahmed AIA
, Abdelshafy R, Ahmed AIA ![]() , Zahran AM, Attalah M, Sallam Y
, Zahran AM, Attalah M, Sallam Y ![]() , El Lateef AGA
, El Lateef AGA
Received 18 December 2022
Accepted for publication 3 March 2023
Published 27 March 2023 Volume 2023:16 Pages 811—817
DOI https://doi.org/10.2147/JMDH.S401937
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shaimaa E Kabil,1 Rania Abdelshafy,1 Ahmed Ismail Abbas Ahmed,1 Alhassan Mostafa Zahran,2 Mahmoud Attalah,2 Yossra Sallam,1 Aisha Ghanem Abd El Lateef3
1E. N. T Department, Faculty of Medicine Cairo, Al-Azhar University, Cairo, Egypt; 2Pediatric Department, Faculty of Medicine Cairo, Al-Azhar University, Cairo, Egypt; 3Psychiatric Department, Faculty of Medicine Cairo, Al-Azhar University, Cairo, Egypt
Correspondence: Shaimaa E Kabil, Email [email protected]
Objective: Language disorders (LD) in autism spectrum disorders (ASD) are highly variable and has a severe impact on the level of functioning in autistic children. Early diagnosis of these language disorders is essential for early interventions for children at risk. The electrophysiological measurements are considered valuable tools for determining language disabilities in children with ASD. This study aimed to study and compare ABR and MMN in autistic children with language disorders.
Methods: This study included a group of typically developing children and a group of children diagnosed with autistic spectrum disorders and language disorders. Both groups were matching according to age and gender. After confirming bilateral normal peripheral hearing sensitivity, ABR was done and both absolute and interpeak wave latencies were correlated. MMN using frequency oddball paradigms were also obtained and correlated.
Results: More abnormalities were reported in ABR test results in the form of delayed absolute latencies and prolonged interpeak intervals. Also, we reported prolonged latencies of MMN. Consequently, both ABR and MMN are complementary test in evaluating autistic children with language disorders.
Conclusion: Our results support the hypothesis of remarkable dysfunction in basic auditory sound processing that may impact the linguistic development of autistic children.
Keywords: Autism spectrum disorders, Language Disorders, Auditory brain stem response, Mismatch negativity
Introduction
The term ‘autism spectrum disorders’ (ASD) refers to a neurodevelopmental disorder, characterized by limitations in social communication and everyday functioning.1 It is a developmental disability; biologically based and unclear how biological variants connect to the symptoms of this condition. In some way, the central processing of stimuli may be disturbed.2 Delayed language development (DLD) occurs when children present language maturation, at least 12 months behind their chronological age due to either sensory or intellectual deficits, autism spectrum disorders, evident cerebral damage, and/or inadequate social and emotional conditions.3
Language disabilities in ASD may vary from mild to severe impairments,4 and consequently affect the level of functioning in autistic children. About 34% of young children with ASD are nonverbal.5 Early diagnosis is essential for early interventions for children who are at risk. Electrophysiological measures have the advantage of being objective tools with no need for language abilities to comply, so they are valuable for evaluating the central auditory system and identify the auditory processing deficits that may affect language development in autistic children.6,7
It was declared that both the cerebral cortex and the subcortical area are involved in language processing.8,9 Auditory brain stem response (ABR) is one of the electrophysiological measures that reflects the synchrony of the brain stem electrical activity in response to acoustic stimuli,10 while mismatch negativity testing (MMN) reflects the integrity of the auditory sensory memory.11 This memory is essential in mapping meaning for language.12,13
Several studies assessed the auditory pathway at the level of the brainstem in individuals with ASD using ABR.14,15 Generally, the literature showed that those subjects may present alterations in ABR. The most common findings were increased latency of waves III and V14,16,17 and an increase in the interpeak intervals of I–III and I–V, suggesting brainstem affection.14,17
While ABR reflects synchronized electrical activity of the brainstem’s neural elements in response to acoustic stimulation,10 a mismatch negativity (MMN) paradigm is used to study the preconscious automatic auditory processing. Findings on MMN in children with autism are highly variable. Some studies reported larger MMN and/or shorter latencies in children with autism, whereas other studies reported smaller or even normal MMN and/or longer latencies in children with ASD.18,19
Lepistö et al,20 reported some MMN amplitude changes with no differences in regard to latency measurements in autistic children diagnosed with language impairment. Since it was declared by Green et al 20206 to be the only MMN study of ASD with language impairment to typically developing children,6 and it did not study ABR in comparison with MMN.
Aim
This study was designed to assess auditory processing, by investigating and comparing the brain stem auditory evoked potentials (ABR) and an event-related potential mismatch negativity (MMN) in a group of children diagnosed with ASD & language impairment in spite of apparent normal peripheral hearing sensitivity.
Patients and Methods
A total of 120 children between the ages of 8 and 12 who were chosen from the pediatric and phoniatric clinics of Al Zahraa University Hospital and AL Hussein University Hospital participated in this observational case–control study. They were divided into two groups:
- Study group: consisted of 60 children with varying degrees of autism spectrum disorders. Their mean age was 9.8 ± 1.19 ranged from 8 to 12 years and 61.7% were males. All ASD groups recruited in this study completed the tests and their language age was below 2 years.
- Control group: consisted of 65 typically developing children. However, 5 children did not complete the evaluation so they were excluded from the analyses. Consequently, 60 typically developing children with average intellectual ability and fully developed language were included in the statistical analyses. They were matched for age and sex with the study group with mean age 10.03 ± 1.28 ranged from 8 to 12 years and 55% were males.
All participants in this study had undergone general, neurological and otorhinolaryngological examination to exclude other systemic, psychological and neurological diseases. In addition, patients with history of otological diseases, head trauma and ototoxic medications were excluded.
Diagnosis of autism was carried out according to DSM-5 (diagnostic and statistical manual – fifth edition)1 and graded according to CARS (childhood autism rating scale).20 Language evaluation was done by Arabic PLS4 (preschool language scale – fourth edition).21 According to DSM-5 autistic children must have persistent deficit in each area of social communication plus at least two types of repetitive behaviors. On the other hand, classification of severity was done according to CARs because it provides clear cutoff points for each level of severity (children who got score below 30% are considered non-autistic, children with score between 30 and 36.5 suffer from mild to moderate autism, and others who scored 37 up to 60 are considered severely autistic), whereas psychometric evaluation was done by SBIS5 (Stanford-Binet intelligence scale-fifth edition).22
Audiological Examination
To verify normal peripheral hearing and intact acoustic reflexes, a basic audiological assessment was conducted:
- Otoscopy is used to examine the tympanic membrane and external auditory canal.
- By using an immitancemeter (Maico, Diagnostic GmbH, MI 44), 226 Hz tympanometry and ipsilateral acoustic reflex thresholds at 1, 2, and 4 kHz were obtained.
- An audiometer was used to get pure-tone audiometry (PTA) in a sound treated room (Piano Plus INVENTIS), using calibrated TDH39 headphones. Air conduction thresholds were obtained between 0.25 and 8 kHz. Play conditioning audiometry has sometimes been employed.
A threshold of up to 20 dBnHL for all tested frequencies was considered normal.
- Interacoustics Eclipse (EP25, Inc., Middelfart, Denmark), in a calm, dark room with the participant seated comfortably in a recliner, was used to conduct electrophysiological measurements.
Auditory brain stem response using click stimuli was obtained for all children. The subjects were tested following the oral administration of chloral hydrate to avoid interference caused by excessive muscle activity. The following parameters were applied: 100 μs, 80 dBnHL, rarefaction, and broadband click, given at a rate of 21.1/s, with 1200 total sweeps, and a 20 ms time window. The absolute latencies of waves I, III, and V on both sides as well as the IPLs of waves I–III and III–V were identified manually.
Tone burst stimuli were delivered in an odd-ball paradigm while the patients watching silent videos, to produce mismatch negative responses. The Probability for the standard was 80% and 20% for the deviant stimuli. The deviants (250 in total) were presented in an alternating polarity, with an intensity of 80 dBpeSPL and at a rate of 1.1/s. 300 sweeps for each ear were obtained and averaged. Time analysis was set at 500 ms, and included 50 ms pre-stimulus onset. Recording of two replications from each ear was made with an amplification of 50, artifact rejection at 100 μV, and a band-pass filter of 1–30 Hz.
Ethical Considerations
The study objectives, design and all details were fully explained to all participants. The study procedure was in accordance with the Declaration of Helsinki and was approved by the institutional review board (IRB), faculty of medicine, Al-Azhar University, Cairo, Egypt. Participation was voluntary; after obtaining informed consents from parents and guardians. Each participant had the right to refuse participation or withdraw from the study at any time without giving any reasons and without any interference with their rights of medical care. Data were anonymous and coded to assure confidentiality of participants.
Statistical Analysis
It was carried out using the SPSS computer package (IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp., USA). The Shapiro–Wilk test was used to examine the normality of quantitative data. For descriptive statistics: the mean ± SD or median (interquartile range 25th–75th percentile (IQR)) were used for quantitative variables while frequency and percentage was used for qualitative variables. Fisher’s exact test was used to assess the differences in frequency of qualitative variables, while Independent samples or Mann–Whitney U-tests were used to assess the differences in means of quantitative variables between both groups. The statistical methods were verified, assuming a significant level of two-sided p values <0.05.
Results
Regarding auditory brainstem evoked response, the median (mean) values of absolute and interpeak latencies in both ears were significantly delayed (prolonged) in children with autism compared to controls except for wave I in both ears, wave I–III in the right ear, and wave III in the left ear that were delayed (prolonged) but with no significant differences (Table 1 and Table 2).
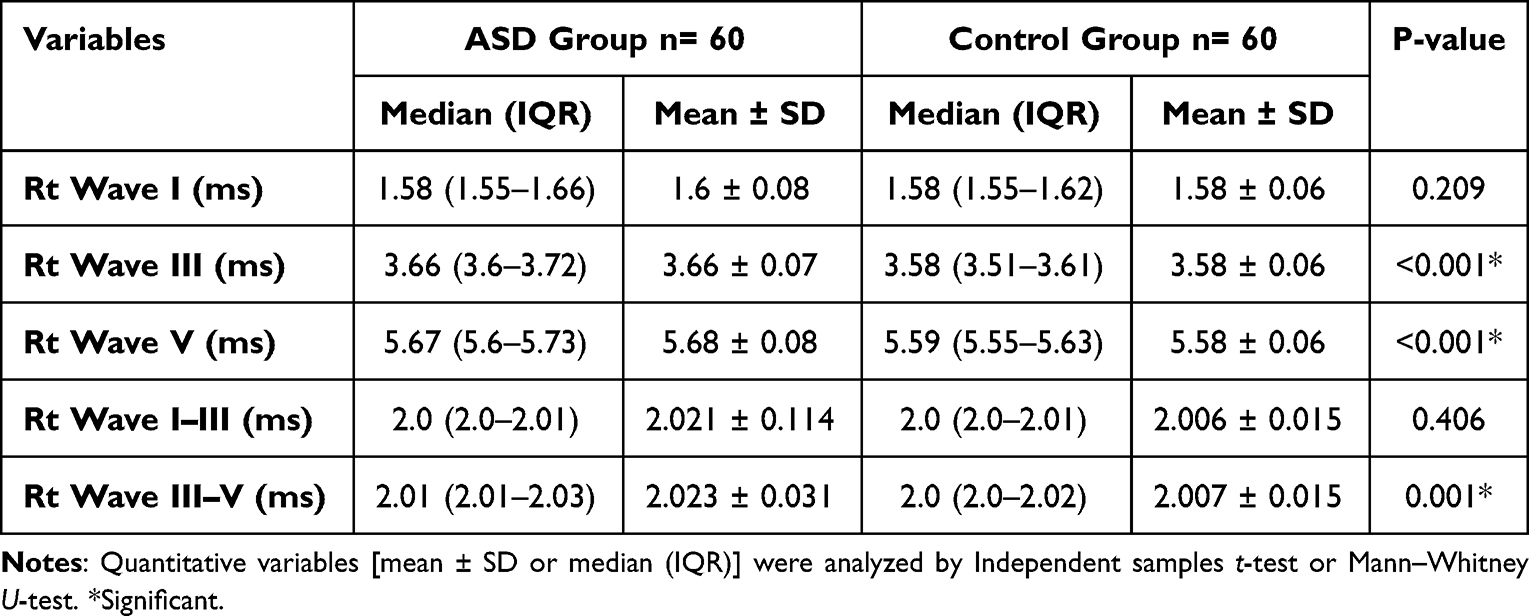 |
Table 1 Absolute and Interpeak Latencies in the Right Ear of the Studied Groups |
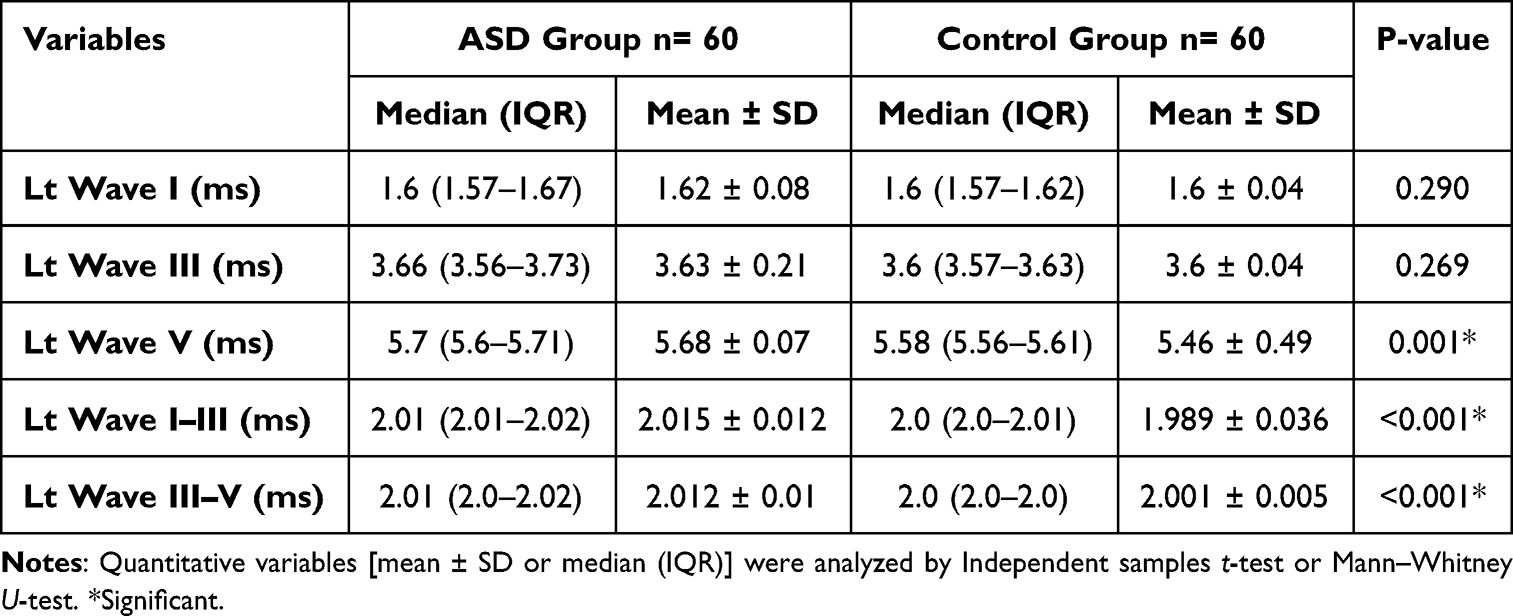 |
Table 2 Absolute and Interpeak Latencies in the Left Ear of the Studied Groups |
Regarding mismatch negativity, the median (mean) values of latency measures in both ears were significantly delayed (prolonged) in autistic children in comparison to controls (P=0.035 in the right ear and P=0.005 in the left ear) while regarding amplitudes, no substantial variation was detected between both groups in both ears (P=0.995 in the right ear and P=0.644 in the left ear) (Table 3).
 |
Table 3 Mismatch Negativity Test in Both Ears of the Studied Groups |
Significantly, the ASD group showed a total of 43.3% of abnormal auditory brainstem evoked response and a total of 30% showed significant changes in mismatch negativity latency measurements on comparing with the control group (P<0.001) (Figure 1).
 |
Figure 1 The deviant results on auditory brainstem response and mismatch negativity among the studied groups. |
Discussion
The click-ABR is a noninvasive and objective test method. It does not rely on the participant’s active responses, so it became a conventional tool to evaluate auditory functions in children, who are difficult to assess behaviorally. A strong relationship between abnormalities in the click-ABR and ASD has been reported in the literatures.23–25
In this work, we intended to study the click ABR in autistic children with language disorders and reported significantly increased absolute latencies of waves (III, V) and the interpeak intervals (Table 1 and Table 2). However, the ABR findings are variable within the scientific literature. Some studies have shown that there have been no changes to the actual wave latencies of ABR.15,26,27 Controversely, some authors reported prolonged absolute latencies for waves III and IV,16 increased latencies for waves I and V,17 and prolonged latencies for waves V in the right ear and wave I in the left ear28,29 in ASD. This electrophysiologic variability supports the hypothesis of perceptual inconstancy.16
Magliaro et al,14 worked on a group of autistic children and revealed that the latencies of waves III and V as well as the I–III interpeak interval were prolonged.
This inconstancy among studies can be due to methodological differences, as regarding different diagnostic criteria for autism, variability in stimulus presentation rate and differences in the studied groups’ age range.30 Also, autism is a heterogeneous disorder with several subgroups,31,32 which suggests that this latency prolongation may occur in a subgroup of autism cases. These latency differences and prolonged interpeak intervals of ABR are supposed to be due to defects in the myelination, axon diameter, and synaptic efficacy of the auditory pathways at the brainstem level.33
Regarding the mismatch negativity, there was no statistically substantial variation between the two groups regarding amplitude measurements; however, the latencies were substantially increased in the ASD group. This agrees with Roberts et al,34 who declared that on comparison with neurotypical developing children, autistic children with delayed language had a considerably longer mismatch magnetic field (magnetic analog of MMN) latencies.
Jansson-Verkasalo et al,35 worked on a group of children diagnosed with Asperger’s syndrome and exhibited greater MMN latencies. They saw this as a sign of auditory discriminating issues, most likely the consequence of inadequate temporary memory storage processes. However, Kemner et al,36 reported that regarding the MMN, there were no variations between the autistics and the normal controls.
Findings on MMN in ASD are quite variable.18 Some studies revealed enhanced MMN and/or shorter latencies,37 while others showed smaller or even normal MMN amplitude and/or longer latencies in comparison to age-matched normally developing children.34 These discrepancies between researchers may be due to variable methodology and inadequate measuring reliability, and statistical power.38 Also, as mentioned above autism is a heterogeneous disorder with several subgroups.31,32
In our study, a total of 43.3% and 30% of the ASD group showed significant changes in the ABR and MMN test results, respectively, on comparing with the control group (Figure 1).
Conclusions
Both ABR and MMN are complementary tests in evaluating language development in ASD. Our work may give some clinical evidence of remarkable dysfunction in basic auditory sound processing at the brain stem, this impacts the linguistic development of autistic children and may be partially to blame for their atypical development. The significance of this finding needs further in-depth studies with larger sample size, considering the subgroups of autistic children with language impairment and multiple settings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
2. Gillberg C. Autism and pervasive developmental disorders. J Child Psychol Psychiatry. 1990;31(1):99–119. Erratum in: J Child Psychol Psychiatry 1991 Jan;32(1):213.PMID: 2179250. doi:10.1111/j.1469-7610.1990.tb02275.x
3. de Vasconcelos Hage SR, Cendes F, Montenegro MA, Abramides DV, Guimarães CA, Guerreiro MM. Specific language impairment: linguistic and neurobiological aspects. Arq Neuropsiquiatr. 2006;64(2A):173–180. PMID: 16791351. doi:10.1590/s0004-282x2006000200001
4. Anderson DK, Lord C, Risi S, et al. Patterns of growth in verbal abilities among children with autism spectrum disorder. J Consult Clin Psychol. 2007;75(4):594–604. PMID: 17663613. doi:10.1037/0022-006X.75.4.594
5. Tager-Flusberg H, Joseph R, Folstein S. Current directions in research on autism. Ment Retard Dev Disabil Res Rev. 2001;7(1):21–29. PMID: 11241879. doi:10.1002/1098-2779(200102)7:1<21::AID-MRDD1004>3.0.CO;2-3
6. Green HL, Shuffrey LC, Levinson L, et al. Evaluation of mismatch negativity as a marker for language impairment in autism spectrum disorder. J Commun Disord. 2020;87:105997. PMID: 32521234. doi:10.1016/j.jcomdis.2020.105997
7. Ramezani M, Lotfi Y, Moossavi A, Bakhshi E. Auditory brainstem response to speech in children with high functional autism spectrum disorder. Neurol Sci. 2019;40(1):121–125. PMID: 30284655. doi:10.1007/s10072-018-3594-9
8. Ahissar E, Nagarajan S, Ahissar M, Protopapas A, Mahncke H, Merzenich MM. Speech comprehension is correlated with temporal response patterns recorded from auditory cortex. Proc Natl Acad Sci U S A. 2001;98(23):13367–13372. PMID: 11698688; PMCID: PMC60877. doi:10.1073/pnas.201400998
9. Johnson KL, Nicol TG, Kraus N. Brain stem response to speech: a biological marker of auditory processing. Ear Hear. 2005;26(5):424–434. PMID: 16230893. doi:10.1097/01.aud.0000179687.71662.6e
10. Junqueira CAO, Colafêmina JF. Investigation of inter and intra-examiner stability to P300 auditory identification: analysis of errors. Braz J Otorhinolaryngol. 2002;4:468–478. doi:10.1590/S0034-72992002000400004
11. Näätänen R. The role of attention in auditory information processing as revealed by event-related potentials and other brain measures of cognitive function. Behav Brain Sci. 1990;13(2):201–233. doi:10.1017/S0140525X00078407
12. Cowan N. Sensory memory and its role in information processing. In: Karmos G, Csepe V, Czigler I, editors. Perspectives of Event-Related Potentials Research. Amsterdam: Elsevier; 1995a.
13. Cowan N. Attention and Memory: An Integrated Framework. New York: Oxford Psychology Series; 1995b.
14. Magliaro FC, Scheuer CI, Assumpção Júnior FB, Matas CG. Estudo dos potenciais evocados auditivos em autismo [Study of auditory evoked potentials in autism]. Pro Fono. 2010;22(1):31–36. Portuguese. Portuguese. doi:10.1590/s0104-56872010000100007
15. Ververi A, Vargiami E, Papadopoulou V, Tryfonas D, Zafeiriou D. Brainstem auditory evoked potentials in boys with autism: still searching for the hidden truth. Iran J Child Neurol. 2015;9(2):21–28. PMID: 26221159; PMCID: PMC4515337.
16. Rosenblum SM, Arick JR, Krug DA, Stubbs EG, Young NB, Pelson RO. Auditory brainstem evoked responses in autistic children. J Autism Dev Disord. 1980;10(2):215–225. PMID: 6927688. doi:10.1007/BF02408472
17. Rosenhall U, Nordin V, Brantberg K, Gillberg C. Autism and auditory brain stem responses. Ear Hear. 2003;24(3):206–214. PMID: 12799542. doi:10.1097/01.AUD.0000069326.11466.7E
18. Dunn MA, Gomes H, Gravel J. Mismatch negativity in children with autism and typical development. J Autism Dev Disord. 2008;38:52–71. doi:10.1007/s10803-007-0359-3
19. Näätänen R, Paavilainen P, Rinne T, Alho K. The mismatch negativity (MMN) in basic research of central auditory processing: a review. Clin Neurophysiol. 2007;118(12):2544–2590. PMID: 17931964. doi:10.1016/j.clinph.2007.04.026
20. Lepistö T, Kajander M, Vanhala R, et al. The perception of invariant speech features in children with autism. Biol Psychol. 2008;77(1):25–31. PMID: 17919805. doi:10.1016/j.biopsycho.2007.08.010
21. Chlebowski C, Green JA, Barton ML, Fein D. Using the childhood autism rating scale to diagnose autism spectrum disorders. J Autism Dev Disord. 2010;40(7):787–799. PMID: 20054630; PMCID: PMC3612531. doi:10.1007/s10803-009-0926-x
22. Abu Haseeba A, El Sady S, Elshobary A, Gamal N, Ibrahim M, Abd El-Azeem A Standardization, Translation and Modification of the Preschool Language Scale [unpublished MD thesis]. Phoniatric unit, Ain Shams University; 2011.
23. Santos M, Marques C, Nóbrega Pinto A, Fernandes R, Coutinho MB, Almeida E Sousa C. Autism spectrum disorders and the amplitude of auditory brainstem response wave I. Autism Res. 2017;10(7):1300–1305. PMID: 28371266. doi:10.1002/aur.1771
24. Matsuzaki J, Ku M, Dipiero M, et al. Delayed auditory evoked responses in autism spectrum disorder across the life span. Dev Neurosci. 2019;41(3–4):223–233. PMID: 32007990; PMCID: PMC7044064. doi:10.1159/000504960
25. Rapin I, Tuchman RF. Autism: definition, neurobiology, screening, diagnosis. Pediatr Clin North Am. 2008;55(5):1129–46, viii. PMID: 18929056. doi:10.1016/j.pcl.2008.07.005
26. Tas A, Yagiz R, Tas M, Esme M, Uzun C, Karasalihoglu AR. Evaluation of hearing in children with autism by using TEOAE and ABR. Autism. 2007;11(1):73–79. PMID: 17175575. doi:10.1177/1362361307070908
27. Roth DA, Muchnik C, Shabtai E, Hildesheimer M, Henkin Y. Evidence for atypical auditory brainstem responses in young children with suspected autism spectrum disorders. Dev Med Child Neurol. 2012;54(1):23–29. PMID: 22142282. doi:10.1111/j.1469-8749.2011.04149.x
28. Azouz HG, Kozou H, Khalil M, Abdou RM, Sakr M. The correlation between central auditory processing in autistic children and their language processing abilities. Int J Pediatr Otorhinolaryngol. 2014;78(12):2297–2300. PMID: 25468467. doi:10.1016/j.ijporl.2014.10.039
29. Kamita MK, Silva LAF, Magliaro FCL, Kawai RYC, Fernandes FDM, Matas CG. Brainstem auditory evoked potentials in children with autism spectrum disorder. J Pediatr. 2020;96(3):386–392. PMID: 30802422; PMCID: PMC9432277. doi:10.1016/j.jped.2018.12.010
30. Wang X, Wang S, Fan Y, Huang D, Zhang Y. Speech-specific categorical perception deficit in autism: an event-related potential study of lexical tone processing in Mandarin-speaking children. Sci Rep. 2017;7:43254. PMID: 28225070; PMCID: PMC5320551. doi:10.1038/srep43254
31. Doshi-Velez F, Ge Y, Kohane I. Comorbidity clusters in autism spectrum disorders: an electronic health record time-series analysis. Pediatrics. 2014;133(1):e54–e63. PMID: 24323995; PMCID: PMC3876178. doi:10.1542/peds.2013-0819
32. Karmel BZ, Gardner JM, Meade LS, et al. Early medical and behavioral characteristics of NICU infants later classified with ASD. Pediatrics. 2010;126(3):457–467. PMID: 20679296; PMCID: PMC3494479. doi:10.1542/peds.2009-2680
33. Amato CA, Santos TH, Barbosa MR, Fernandes FD. Longitudinal study of language therapy in 142 children and adolescents with autism spectrum disorders. Codas. 2013;25(4):388–390. Portuguese. PMID: 24408489. doi:10.1590/s2317-17822013000400015
34. Roberts TP, Cannon KM, Tavabi K, et al. Auditory magnetic mismatch field latency: a biomarker for language impairment in autism. Biol Psychiatry. 2011;70(3):263–269. PMID: 21392733; PMCID: PMC3134608. doi:10.1016/j.biopsych.2011.01.015
35. Jansson-Verkasalo E, Ceponiene R, Kielinen M, et al. Deficient auditory processing in children with Asperger syndrome, as indexed by event-related potentials. Neurosci Lett. 2003;338(3):197–200. PMID: 12581830. doi:10.1016/s0304-3940(02)01405-2
36. Kemner C, Verbaten MN, Cuperus JM, Camfferman G, van Engeland H. Auditory event-related brain potentials in autistic children and three different control groups. Biol Psychiatry. 1995;38(3):150–165. PMID: 7578658. doi:10.1016/0006-3223(94)00247-Z
37. Kujala T, Tervaniemi M, Schröger E. The mismatch negativity in cognitive and clinical neuroscience: theoretical and methodological considerations. Biol Psychol. 2007;74(1):1–19. PMID: 16844278. doi:10.1016/j.biopsycho.2006.06.001
38. Bishop DV. Using mismatch negativity to study central auditory processing in developmental language and literacy impairments: where are we, and where should we be going? Psychol Bull. 2007;133(4):651–672. PMID: 17592960. doi:10.1037/0033-2909.133.4.651
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.