Back to Journals » International Journal of Women's Health » Volume 14
Mirabegron in the Management of Overactive Bladder Syndrome
Authors O'Kane M ![]() , Robinson D, Cardozo L, Wagg A
, Robinson D, Cardozo L, Wagg A ![]() , Abrams P
, Abrams P
Received 18 May 2022
Accepted for publication 8 September 2022
Published 16 September 2022 Volume 2022:14 Pages 1337—1350
DOI https://doi.org/10.2147/IJWH.S372597
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Miriam O’Kane,1 Dudley Robinson,1 Linda Cardozo,1 Adrian Wagg,2 Paul Abrams3
1Department of Urogynaecology, King’s College Hospital, London, UK; 2Department of Medicine, University of Alberta, Edmonton, Alberta, Canada; 3Bristol Urological Institute, Bristol, UK
Correspondence: Dudley Robinson, Department of Urogynaecology, King’s College Hospital, London, SE5 9RS, UK, Tel +44 203 299 3568, Fax +44 203 299 3449, Email [email protected]
Abstract: Overactive bladder (OAB) negatively affects work productivity and quality of life in sufferers. Its overall impact is likely to increase as a result of increasing prevalence in an ageing population. The pathophysiology of OAB is not completely understood but the β 3-adrenoceptor, which is highly expressed in the urinary bladder, is thought to be important for mediating human detrusor relaxation during the storage phase. Clinical trial results have demonstrated that mirabegron, a selective β 3-adrenoceptor agonist offers substantial clinical efficacy and good adherence rates over 12 months. Furthermore, due to its different mechanism of action, it is likely to offer a favourable tolerability profile when compared with antimuscarinic agents, resulting in improved persistence over long-term treatment. Finally, from a health economic perspective, despite its higher drug acquisition cost, mirabegron has been found to be cost-effective, owing to the greater increase in quality-adjusted-life-years gained, when compared to antimuscarinic medications. The PubMed database was searched for English language articles published between 1 January 2005 to 31 January 2022, on the subject of mirabegron. Search terms included “mirabegron”, “overactive bladder”, “β 3-adrenoceptor agonist”, “urinary incontinence”. This review summarises the evidence for mirabegron as a treatment option for the management of OAB.
Keywords: β 3-adrenoceptor agonist, drug therapy, mirabegron, overactive bladder, urinary incontinence
Introduction
Overactive bladder (OAB) is characterised by urinary urgency, usually accompanied by urinary frequency and nocturia, with or without urgency incontinence, in the absence of urinary tract infection or any other obvious pathology.1,2 The worldwide prevalence of OAB in 2008 was estimated at 10.7%. Although no further epidemiological studies have been conducted since, this prevalence was projected to have risen to 20.1% by 2018, due to an increasing proportion of older people in the population. In numerical terms, this equates to an increase from 455 to 546 million in a single decade.3 This has important implications for active aging as OAB is associated with reduced work productivity, as well as a significant impact on health-related quality of life (HRQoL), decreased sexual satisfaction and increased anxiety and depression.4–7
The bladder is innervated by Aδ fibres in the detrusor smooth muscle layer, which respond to stretching of the bladder and unmyelinated C-fibres in the detrusor muscle, near to the urothelium in the lamina propria.8,9 Normal bladder emptying occurs following integration of afferent signalling to the micturition centre, modulation by frontal areas of the brain and activation of efferent activity via parasympathetic nerves ending in the urinary bladder wall to release acetylcholine, as well as via concomitant activation of relaxation mechanisms along the urethra.10,11 In OAB, abnormalities in the afferent pathway may lead to overactivity in the efferent pathway and thus cause involuntary detrusor contractions. Equally, OAB could be the cause of failure to suppress the afferent pathway in response to detrusor contractions. In addition, these involuntary contractions could be the result of hypersensitivity to cholinergic agonists via muscarinic M2/M3 receptors.10
Current treatment options for OAB include conservative strategies such as lifestyle advice, bladder retraining and pelvic floor muscle exercises for urgency suppression, followed by drug therapy, botulinum toxin injection, posterior tibial nerve stimulation, and sacral nerve stimulation. If these interventions prove ineffective, patients may progress to major surgery, such as augmentation cystoplasty. In terms of drug therapy, anti-muscarinic agents, including oxybutynin, tolterodine and solifenacin are currently the most widely used pharmacological agents.12,13 These drugs block muscarinic M2 and M3 receptors to modulate detrusor and urothelial neural activity. However, they also inhibit muscarinic receptors in other parts of the body, such as the salivary glands, tear ducts, brain and heart that can result in unwanted effects such as dry mouth, constipation, dry eyes and blurred vision.9 Relative intolerability could be the cause of the low adherence and persistence associated with these agents, and may lead to early discontinuation of treatment.13–15 In addition, there is concern that long-term exposure to high doses of anti-muscarinic agents may increase the risk of cognitive impairment, including dementia, in older persons.16,17
β-Adrenoceptors and OAB
Adrenoceptors are members of a family of seven transmembrane receptors, with two main groups, α and β, and several subtypes. β1-, 2- and 3-adrenoceptors have been identified in human urothelium and detrusor muscle, with β3 being highly expressed in the urinary bladder.18,19 β3-adrenoceptors have been demonstrated as the predominant subtype, with 95% of all β-adrenoceptor mRNA in the human bladder relating to this subtype; this receptor is thought to be important for mediating human detrusor relaxation.20,21 This is supported by animal studies in which β3-adrenoceptor agonists have been demonstrated to cause dose-dependent detrusor relaxation during the storage phase of the micturition cycle and to inhibit neurogenic detrusor overactivity during in vitro studies.22–24
Mirabegron
Mirabegron is the first commercially available selective, β3-agonist for the treatment of OAB. It was first approved for use in Japan (2011), the US, Canada and EU (2012)25–27 and Australia (2013).28
Pharmacokinetics and Pharmacodynamics
In a study to analyse the distribution of β-adrenoceptors in the cells of the human bladder, mirabegron was shown to induce increases in cAMP levels in human urothelial cells.29 This induction of cAMP accumulation was also observed in cells expressing rat and human β3-adrenoceptors, and in the same study, mirabegron was shown to induce a maximal relaxant effect on rat bladder strips.30 In an in vivo study, mirabegron decreased the mechanosensitive afferent activity of Aδ fibres and C-fibres of the rat bladder in a dose-dependent manner, as well as inhibiting bladder microcontractions.31 Furthermore, in a rat model of detrusor overactivity, mirabegron dose-dependently increased volume voided per micturition.30 Additional studies have shown that mirabegron reduces pre-constricted isolated rat detrusor muscle contraction, reduces distension-induced bladder contractions in rats, increases bladder capacity in water loaded rats and monkeys, and reduces intravesical pressure in dogs.32
In healthy volunteers, mirabegron at a dose of 25 mg has a bioavailability of 29% which increases to 35% at 50 mg, 40% at 100 mg and 45% at 150 mg.25,33,34 Mirabegron is rapidly absorbed and the time to reach maximum concentration is 3–4 hours with a terminal elimination half-life of 50 hours.25,35 The agent is widely distributed in the body with a volume of distribution of 1670 L.25,35 The metabolism of mirabegron involves de-alkylation, oxidation and glucuronidation, with two major metabolites, which are pharmacologically inactive, identified in human plasma representing 17% and 10% of the total exposure.25,33 Metabolism involves two cytochrome P450 enzymes (CYP3A4 and CYP2D6). Following metabolism, mirabegron is excreted in the urine (55%) and faeces (34%) mainly in the unchanged form.36 Further pharmacokinetic assessments and the impact of food on exposure of mirabegron have been conducted in healthy East Asian subjects.37 No significant differences in pharmacokinetics were observed among Japanese, Taiwanese, and Chinese populations. The exposure of mirabegron was found to be lower under fed-conditions than fasted-conditions in Japanese and Taiwanese subjects.37 Higher exposure levels of mirabegron were seen in female than male East Asian subjects, a trend that has previously been observed in Western subjects.37
Clinical Efficacy & Safety
Phase II Trials
The BLOSSOM trial was a proof-of-concept randomised, double-blind, phase IIa trial of mirabegron in patients with OAB.38 During the trial, 262 patients were randomised to receive placebo, mirabegron 100 mg twice daily (bid), mirabegron 150 mg twice daily or tolterodine 4 mg extended release (ER). Comparisons were only made between active treatment and placebo. When compared with placebo, mirabegron was associated with a statistically significant decrease in the mean number of micturitions per 24 hours (−2.19 and −2.21 for mirabegron 100 mg bid and 150 mg bid, respectively, versus −1.18 for placebo, p ≤ 0.01). Treatment-related adverse events were comparable for the mirabegron and placebo treatment groups. Following the positive results of the BLOSSOM trial, a 12-week double-blind dose-ranging phase IIb trial of 928 patients with OAB was conducted (DRAGON trial).39 Results demonstrated that mirabegron (50, 100 and 200 mg) showed significant dose-dependent reduction in micturition frequency versus placebo (p ≤ 0.05). In addition, a decrease in the mean total number of incontinence episodes, urgency incontinence episodes and urgency episodes per 24 hours compared with placebo was observed. Furthermore, in line with the criteria stated by the International Conference on Harmonisation E14 guidance proposal that, “a thorough QT/QTc study, including supratherapeutic doses, is conducted, for all new drugs to identify any cardiac effect of treatment”, mirabegron did not cause QTc interval prolongation in either sex at 50 or 100 mg doses (the upper boundary of the one-sided 95% CI for the QTc interval was <10 ms at all evaluated time points).40 The threshold of regulatory concern for drug effect on QTc interval prolongation is around 5 ms with an upper boundary of the one-sided 95% CI of 10 ms. Mirabegron at 200 mg dose did not exceed this threshold in males. However, in the female subpopulation, the largest mean ΔQTc effect was 10.42 ms (upper boundary of the one-sided 95% CI of 13.44 ms) occurring at 5 h. The EMA and FDA approved starting dose for mirabegron is 50 mg and 25 mg, respectively,25,26 and prolongation caused by the supratherapeutic dose of 200 mg in females is unlikely to be clinically significant.
Phase III Trials
SCORPIO was a European-Australian multicentre, randomised, double-blind, phase III trial of 1987 patients who received mirabegron 50 mg, mirabegron 100 mg, tolterodine ER 4 mg or placebo once daily for 12 weeks.41,42 During the study, mirabegron 50 mg and 100 mg significantly decreased the mean number of micturitions (−1.93 and −1.77, respectively) and incontinence episodes (−1.57 and −1.46, respectively) per 24 hours compared with placebo (p < 0.05, Table 1). In addition, post-hoc analysis indicated both doses of mirabegron resulted in similar improvements in the primary endpoints (change from baseline to final visit (end of treatment) in mean number of incontinence episodes and mean number of micturitions/24 h.) in patients who were either anti-muscarinic naïve or had received prior anti-muscarinic therapy. An additional multicentre, randomised, double-blind, placebo-controlled phase III study of mirabegron (ARIES) was conducted in North America and included 1328 patients with OAB.43 Patients received mirabegron 50 mg, 100 mg, or placebo for 12 weeks. In line with previous results, both doses of mirabegron resulted in reduced incontinence episodes and number of micturitions per 24 hours compared with placebo (Table 1). A further European-North American key trial, CAPRICORN, was a randomised, double-blind, placebo-controlled trial comparing mirabegron 25 mg and 50 mg to placebo in 1306 patients with OAB.44 During this study, mirabegron significantly reduced the number of incontinence episodes and number of micturitions per 24 hours compared with placebo (p < 0.05, Table 1). In these studies, mirabegron was associated with a more favourable tolerability profile than antimuscarinic therapies among patients ≥65 years; over 12 weeks, the incidence of dry mouth was 6-fold higher in tolterodine ER 4mg treated patients compared with mirabegron 25 mg or 50 mg. Furthermore, the incidence of serious AEs and treatment-emergent AEs that led to discontinuation of mirabegron 50 mg in patients aged ≥65 years was lower than with tolterodine ER over 12 months.45 Mirabegron treatment led to improved HRQoL in older patients with OAB compared to those receiving placebo.45
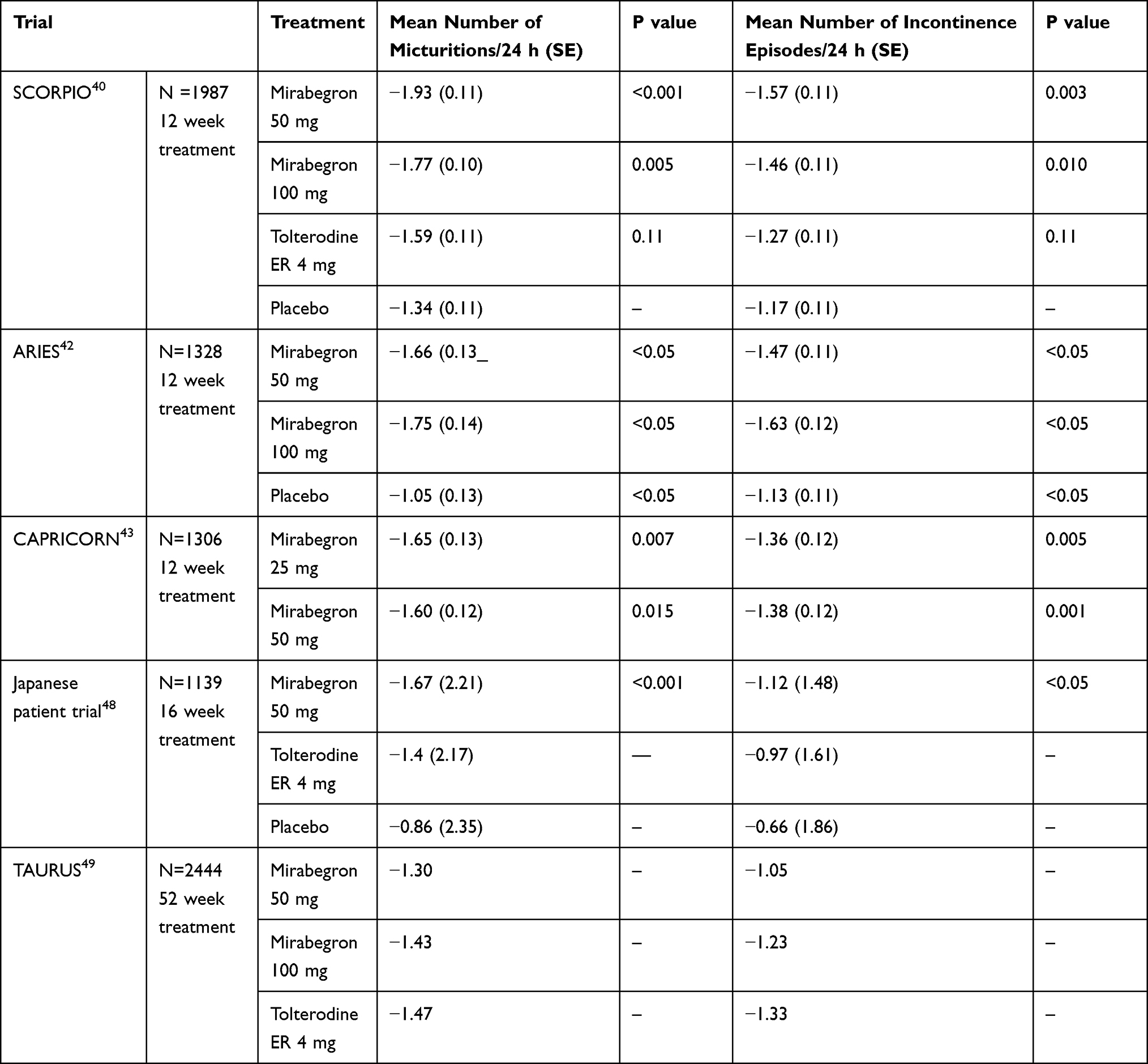 |
Table 1 Primary Endpoints for Phase III Trials Evaluating Mirabegron in Patients with OAB |
Treatment with mirabegron (25, 50 and 100 mg) significantly improved symptoms in Japanese patients with OAB compared to placebo. Improvements were observed in mean number of micturitions/24h as well as incontinence episodes/24h, urgency episodes/24h, mean volume voided and storage function, including first desire to void and maximum cystometric capacity.46,47 The efficacy of mirabegron in Asian patients has been further demonstrated in a 12-week, randomised, double-blind study, patients received mirabegron (50 mg) or tolterodine ER (4 mg) or placebo.48 Patients treated with mirabegron (n = 311) had significant improvement compared to placebo (n = 300) in the mean number of micturitions/24 hr compared to placebo.48 The incidence of treatment emergent adverse events (TEAE) was similar to that observed in the larger trials. This study supports the previous phase III trials conducted in Europe, North America, and Japan.48 During a longer, 16-week randomised phase III trial of Japanese patients with OAB, patients (n = 1139) received either placebo, mirabegron 50 mg or tolterodine ER 4 mg.49 Mirabegron statistically significantly reduced the mean number of micturitions (p < 0.001), urgency episodes (p = 0.025) and incontinence episodes per 24 hours (p = 0.003), compared with placebo. The overall distribution of treatment-related adverse events was broadly similar, however dry mouth was more common in the tolterodine treated patients than placebo and mirabegron treated patients. In a post hoc analysis of pooled data from two of these earlier studies, Takahashi et al substantiated the use of mirabegron in OAB wet populations, illustrating a statistically significant improvement in mean micturitions/24h and incontinence episodes at EoT, as well as other secondary endpoints, for women with urgency urinary incontinence or mixed urinary incontinence.50
In order to evaluate the long-term efficacy and safety of mirabegron (50 and 100 mg) and tolterodine ER 4 mg, a large, global, double-blind, placebo-controlled randomised phase III trial was conducted over 12 months (TAURUS).51 The study included 2444 patients randomised to one of four treatment arms, and included patients who had previously received mirabegron as part of an earlier phase III trial (81%). Results demonstrated a similar prevalence of adverse events across all the treatment groups and the discontinuation rate due to such events was low (6.4%, 5.9% and 6.0% for mirabegron 50 mg, mirabegron 100 mg and tolterodine ER 4 mg, respectively). The efficacy of mirabegron treatment was maintained for 12 months. The long-term (52-week) efficacy of mirabegron (50 mg and 100 mg) in Japanese patients with OAB (n = 204) was further assessed.52 Mirabegron treatment was well tolerated with 34% (51/152) and 30% (15/50) of patients experiencing adverse events with 50 mg and 100 mg, respectively. Common adverse events in patients treated with 50 and 100 mg included constipation (6% and 1%, respectively) and increased blood pressure (3% and 1%, respectively). An improvement in frequency and urgency of micturition was observed from week 8 and remained stable until the end of treatment, and was accompanied by improvements in QoL in the 193 patients remaining in the study.52 Furthermore, prospective pooled analysis of three of the 12-week phase III trials and the 1-year trial demonstrated a favourable tolerability profile of mirabegron in patients with OAB.53 The mirabegron tolerability profile was similar to that seen with placebo and tolterodine ER 4 mg, except for dry mouth, which occurred up to five times less frequently with mirabegron.
The β adrenoceptors are expressed in the cardiovascular system and, as a consequence, the effects of mirabegron on cardiovascular (CV) safety have been closely monitored in the key registration trials.54 Over 1/3 of patients with OAB in these trials had hypertension at baseline, however, CV safety profile of mirabegron has been found to be acceptable at therapeutic doses and comparable with that of anitmuscarinic agents.54 That notwithstanding, mirabegron should not be given to those patients with severe uncontrolled hypertension, in line with both FDA and EMA directions.
Recently, the efficacy of mirabegron compared to solifenacin has been examined in a randomised non-inferiority phase IIIb trial of patients dissatisfied with previous antimuscarinic treatment due to lack of efficacy.55 Patients (n = 1887) were randomised to receive mirabegron (50 mg, n = 943) or solifenacin (5 mg, n = 944) for 12 weeks. The mean difference in mean number of micturitions/24h between the two groups was −0.18 (−0.42, 0.06); therefore, the non-inferiority of mirabegron was not demonstrated since the lower limit of the 95% CI was not > −0.20. Nervertheless, improvements in OAB symptoms were observed but there was no significant difference between the two treatments. Both therapies were well tolerated, but with a numerically lower incidence of dry mouth with mirabegron.
Phase IV Trials
The PILLAR trial was a Phase IV, double-blind, randomised, placebo-controlled, multicentre study specifically designed to assess the efficacy and safety of mirabegron in patients aged >65 years with OAB-wet.56 Eight hundred and eighty-eight patients were randomised to receive either mirabegron 25 mg, mirabegron 50 mg or placebo once daily for 12 weeks. The study was not designed to detect a difference between individual doses of mirabegron and placebo. Mirabegron treatment was associated with a statistically significant improvement in change from baseline to EOT in the mean number of micturitions/24h (−0.7) and mean number of incontinence episodes/24h (−0.6) vs placebo (P < 0.001). However, the change was greater in those patients aged <75 years vs those aged >75 years (−2.09 and –1.98 respectively) for the mean change in incontinence episodes at EOT in the mirabegron group.
An in-depth examination of the safety and tolerability of mirabegron among the participants in the PILLAR study demonstrated a frequency of TEAEs (47%) similar to that of previously reported phase III studies enrolling patients aged >65 years.57 Those TEAEs most frequently reported (UTI, headache, and diarrhoea) were in line with the known mirabegron safety profile, and did not appear to be either age, or dose dependent. Furthermore, a pre-planned analysis aimed to detect potential cognitive decline related to treatment with mirabegron, using a rapid screening instrument for mild cognitive impairment, the Montreal Cognitive Assessment (MoCA), was conducted as part of the PILLAR study.58 There was no statistically significant change in adjusted mean MoCA total score from baseline to EOT in either the mirabegron group (−0.2) or the placebo group (−0.1), indicating that the pattern of change in cognition over time in an older OAB population receiving mirabegron does not appear to differ from that of subjects receiving placebo.
Children
OAB is also prevalent in paediatric patients and can negatively affect self-esteem and child development. Mirabegron has been assessed in a prospective trial of 58 patients (median age 10.1 years) without symptom improvement following behavioural and medical interventions.59 Mirabegron treatment improved median bladder capacity (150 mL to 200 mL, p < 0.001) and continence in 90% (52/58) of patients, with 13 becoming completely dry. Eight patients reported side effects and three discontinued treatment because of them.59
A retrospective observational study of 16 patients, aged 8 to 11 years, showed a statistically significant increase in age-adjusted bladder capacity ratio from 0.57 to 0.97 after mirabegron use. This study compared solifenacin (n = 29) to mirabegron (n = 16), and although it found no significant difference in efficacy between the two groups, drug-induced adverse effects were only reported in the solifenacin group.60 Similarly, a prospective, single-blind study comparing mirabegron 50 mg (n = 64), solifenacin 5 mg (n = 65), and placebo (n = 61), in children aged 5 to 14 years, who reported ongoing bothersome urgency symptoms after at least 3 months of behavioural therapy, reported comparable efficacy for both mirabegron and solifenacin.61 There was a significant improvement in the number of incontinence episodes per day, mean number of voids per day, and mean void volume, in both groups, but the frequency of adverse effects was lower in those taking mirabegron.
A Phase III, dose-titration study evaluated the efficacy and safety of mirabegron in children and adolescents with neurogenic detrusor overactivity using clean intermittent catheterisation.62 Mirabegron treatment resulted in a statistically significant increase in maximum cystometric capacity by week 24 (mean change from baseline 87.2mL, p < 0.001) in the total population and in both age groups (p < 0.001). Statistically significant improvements were also found for secondary endpoints including all urodynamic assessments and the Patient Global Impression of Severity (PGI-S) questionnaire. This study identified no new safety concerns in the paediatric population and demonstrated that the pharmacokinetic profile of mirabegron can be predicted by body weight alone, and is not affected by age.
Patient Reported Outcomes
Patient-reported outcomes (PROs) directly collect the responses of the patient to treatment to provide further information on its effectiveness. It is important to address this area in diseases and treatments that are associated with an impact on daily routines and HRQoL, as these can adversely affect adherence and persistence with drug therapy. Pre-specified analysis of PROs from the phase III SCORPIO trial of patients with OAB receiving placebo, mirabegron (50 or 100 mg) or tolterodine ER (4 mg) for 12 weeks was performed.63 Patients treated with mirabegron (50 mg) had significant improvement of disease perception and QoL, with improvements in coping, concern and perception of their condition compared with placebo (p < 0.05). Patients on mirabegron presented with improved overall work productivity and reduced the number of absences from work compared to placebo or tolterodine.63 However, PERSPECTIVE, a prospective, non-interventional registry found similar improvements in OAB-q SF symptom bother score and HRQoL total score for both mirabegron and antimuscarinic initiators, concluding that there are no differences between mirabegron and antimuscarinics in terms of these patient-reported outcomes.64 A post hoc analysis of pooled data from the three, randomised, double-blind, placebo-controlled 12-week trials have examined the patient experience with mirabegron.65 In this analysis, mirabegron (50 mg) treated patients had greater improvement in PROs than placebo. Mirabegron significantly improved OAB-q symptom bother scale and patient perception of bladder condition (p < 0.05) as well as the OAB-q total HRQoL and OAB-q subscales of coping, concern and sleeping (p < 0.05) from baseline to final visit.65 This improvement in objective outcomes with mirabegron translated into a meaningful clinical benefit with the OAB-q and PPBC appearing to provide a clinically relevant view on OAB management.65
Persistence and Adherence
Persistence with long-term medication is typically low in patients with chronic diseases66 and is often a leading cause of rising health-care costs and preventable morbidity and mortality.67 The chronic nature of OAB usually requires persistent treatment for effective management and involves a careful balance between efficacy and tolerability. A number of studies examining clinical practice and medication compliance have found that patients quickly discontinue OAB medication with continuation rates in one study found to be <25% at 1 year.14,68
The different tolerability profile of mirabegron compared to the widely used anti-muscarinic treatments may improve patients’ adherence and persistence to their treatment. Two recent studies have provided early evidence that patients with OAB treated with mirabegron have improved persistence (defined by a gap in therapy of at least 30 days or switching to another medication) and adherence (calculated as the proportion of days the patient received the prescribed medication compared to their overall time on therapy) to their treatment compared to patients receiving anti-muscarinics.69–71
In one retrospective, exploratory analysis, data from 19,485 patients were analysed. Treatment-experienced patients who received mirabegron had greater 12-month persistence (39%) compared with patients receiving solifenacin (35%; HR 1.220; CI: 1.013–1.469; p = 0.037) patients taking oxybutynin ER (17%; HR 1.838; CI: 1.409–2.398; p < 0.001) or oxybutynin IR (14%; HR 2.160; CI: 1.759–2.652; p < 0.001). In treatment-naïve patients, mirabegron continued to have the highest rates of persistence at 12 months (30%) compared with antimuscarinics (13.8–21.0%), with the lowest persistence in patients taking oxybutynin (14%; HR 1.786; CI: 1.663–1.997; p < 0.001).70,71 In the treatment-naïve cohort, patients <46 years were more likely to discontinue OAB treatment than those aged ≥65 years. Patients taking mirabegron had significantly better adherence than those taking antimuscarinics (64.5% vs 18.6–49.2%, P < 0.001). Adherence was greater in treatment-experienced patients than treatment-naïve, with patients <46 years the least adherent.71 In contrast, Carlson et al found no difference in persistence rates between the unadjusted cohorts in those taking mirabegron versus antimuscarinics. However, once adjusted for age, sex and prior OAB medication use, persistence was higher for mirabegron.72
In a prospective case series, long-term persistence with mirabegron was investigated in 354 women who received mirabegron. A quarter of all patients (90/354) continued to receive mirabegron at 1 year.73 Those patients who were still on medication continued to derive benefit in terms of QoL. The most common reasons for discontinuation were lack of efficacy and side effects. Continuation rates of mirabegron were similar to anticholinergic therapies. The higher discontinuation rates are consistent with the real-world nature of this series.73 This is further supported by a study of hospital prescription data in 197 patients who were prescribed mirabegron for OAB. At 3 months, 69% persisted with treatment, falling to 48% at 6 months; persistence rates were similar between sexes. Lack of efficacy and adverse events were the most common reasons given for discontinuation.74 As with other studies many patients had previously received pharmacotherapy, with only 19% of patients receiving mirabegron as the first-line treatment, reflecting guideline-driven clinical practice. The difference in persistence rates may be affected by heterogeneous groups of patients, the majority of whom have failed previous therapies and thus they may not be comparable to treatment-naïve populations.74 Optimal efficacy with mirabegron can take up to 4 weeks to achieve, hence those patients (19%) discontinuing before 1 month, should be encouraged to persevere with treatment.
In another prospective study, tolerability of mirabegron was shown to be significantly higher than that of tolterodine (PREFER).75 In this 8-week crossover, double-blind, phase IV study, 358 patients with OAB were randomised to one of four treatment sequences: mirabegron/tolterodine, tolterodine/mirabegron, mirabegron/mirabegron, or tolterodine/tolterodine. The mean OAB-S Medication Tolerability score of 86.29 for mirabegron (CI: 83.50, 89.08) was significantly higher than 83.40 for tolterodine (CI: 80.59, 86.20; p < 0.004), with any potential effect of sequence on tolerability scores being excluded by a nonsignificant period-by-treatment interaction (p = 0.955). In addition, the percentage of patients achieving a clinically meaningful benefit from treatment, as measured by a minimal important difference (MID) of ≥90 in OAB-S Medication Tolerability score or ≥10-point improvement in OABq scale, was higher for mirabegron (52.5%) vs tolterodine ER (48.5%). However, patient preference, improvements in OAB symptoms and improvements in PROs (OAB Satisfaction, OABq and PPBC) were comparable between groups.76
The improved persistence and adherence rates in those taking mirabegron has been supported by a large systematic review and network meta-analysis conducted by Song et al. Persistence trials, involving 237,602 participants, demonstrated a significantly higher persistence rate for mirabegron compared to all other anticholinergics. Among adherence trials, with 46,731 participants, mirabegron also had the highest adherence rate at 12 months, although the difference in adherence rates compared to all other anticholinergics was not statistically significant.
Combination of Mirabegron with Anti-Muscarinic Agents
In order to examine whether combining mirabegron with anti-muscarinic treatments could improve efficacy in patients with OAB a randomised, double-blind, phase II trial (SYMPHONY) evaluated the efficacy of combination of solifenacin (2.5, 5 and 10 mg) with mirabegron (25 and 50 mg) compared to solifenacin and mirabegron monotherapy (n = 1306).77 The mean volume voided per micturition was significantly improved in patients treated with combination therapy with the adjusted difference compared with solifenacin 5 mg monotherapy ranging from 18.0 mL (95% CI 5.4–30.0) for solifenacin 5 mg plus mirabegron 25 mg to 26.3mL (95% CI 12.0–41.0) for solifenacin 10 mg plus mirabegron 50 mg. Micturition frequency was significantly reduced in patients treated with solifenacin 5 mg plus mirabegron 50 mg, solifenacin 10 mg plus mirabegron 25 mg and solifenacin 10 mg plus mirabegron 50 mg groups (p < 0.05) compared with solifenacin 5 mg monotherapy. All combinations were well tolerated with the incidence and type of treatment-emergent adverse events similar between patients treated with monotherapy or combination therapies. This study demonstrated that combination therapy significantly improved efficacy compared with solifenacin 5 mg monotherapy. The lack of any additive effects on safety parameters, of these two treatments, is important, and no new clinically relevant safety concerns arose.
Where subjective efficacy assessments were considered, improvement in PROs (OABq and PPBC) and the proportion of patients achieving clinically relevant improvement in efficacy and PROs (responder analysis) was significantly greater with combination treatment (mirabegron 25 or 50mg and solifenacin 5 or 10mg) compared to solifenacin 5mg monotherapy or placebo.78 To further identify whether the combination of mirabegron and solifenacin maximises the efficacy and minimises the side effects of anti-muscarinics and results in improved persistence and adherence, a multinational Phase III study comparing the efficacy and safety of solifenacin succinate and mirabegron taken together, compared to each medicine alone (SYNERGY), in subjects with symptoms of OAB, was conducted.79 In this 12-week trial, 3398 patients with wet OAB were randomised to solifenacin 5 mg + mirabegron 25 mg (combined S5 + M25 group), solifenacin 5 mg + mirabegron 50 mg (combined S5 + M50 group), solifenacin 5 mg, mirabegron 25 mg, mirabegron 50 mg, or placebo. The combination of solifenacin 5 mg and mirabegron 50 mg resulted in a statistically superior reduction in incontinence episodes/24h at end of treatment compared to solifenacin 5 mg (P = 0.033). Unfortunately, this was not demonstrated when compared to mirabegron 50 mg monotherapy. There was, however, a significant change from baseline to EoT for micturitions/24h, (the other co-primary endpoint) for both combination therapy groups vs monotherapies (combined S5 + M50 group, nominal P values 0.006 and <0.001 vs solifenacin 5 mg and mirabegron 50 mg, respectively; combined S5 + M25 group, nominal P values 0.040 and 0.001 vs solifenacin 5 mg and mirabegron 25 mg, respectively).79 Combined therapy demonstrated consistent improvements across all secondary efficacy parameters compared to monotherapy, with effect sizes being additive. 36% of patients experienced ≥1 TEAE (highest (40%) in combination 5+25mg group and lowest (32%) in the mirabegron 25mg group). However, the majority of these were mild to moderate in severity, and there was no meaningful difference between treatment groups in the incidence of TEAEs. A subanalysis from the study reported generally comparable cardiovascular safety with combination and monotherapy treatment.80 This was supported by the results of a further sub-study analysing ambulatory BP monitoring in 715 patients. This showed that combination therapy produced no meaningful changes in BP or heart rate over 12 weeks of treatment.81
The promising results from SYNERGY were reproduced in an extension of the study, SYNERGY II, which evaluated the safety and efficacy of solifenacin 5 mg in combination with mirabegron 50 mg compared to solifenacin or mirabegron monotherapy over a 12-month period.82 Once again, combination therapy was statistically superior to mirabegron and solifenacin for the number of incontinence episodes and micturitions. Overall, 47% of patients experienced ≥1 TEAE, and again the frequency was slightly higher in the combination group. Although serious TEAEs were reported by 3.7%, only one was considered possibly treatment-related (mirabegron group, atrial fibrillation). When patients were stratified according to age, TEAEs, most notably UTIs, were more common in older age groups, regardless of treatment.
Recently, addition of mirabegron (50 mg) to solifenacin (5 mg) has been shown to further improve OAB symptoms compared to solifenacin 5 mg or 10 mg alone in patients who remain incontinent after initial solifenacin 5 mg (4-week run-in) treatment in a 12-week study (BESIDE).83 Change from baseline in mean number of incontinence episodes/24h was −1.80 for combination therapy compared to −1.53 for solifenacin 5 mg (difference −0.26 CI: −0.47, −0.05; p = 0.01) and change from baseline in mean number of micturitions/24h was −1.59 for combination treatment compared to −1.14 for solifenacin 5 mg (difference −0.45; CI: −0.67, −0.22; p < 0.001).83 All treatments were well tolerated with dry mouth and constipation were the most common TEAEs. The incidence of TEAEs was lowest with solifenacin 5 mg (33.1%), highest with solifenacin 10 mg (39.4%), and 35.9% with combination. The incidence of dry mouth was lower with combination (5.9%) compared to solifenacin 10 mg (9.5%) and similar to solifenacin 5 mg (5.6%). Combination treatment resulted in higher hypersensitivity reactions compared to solifenacin 5 and 10 mg (1.5% and 0.8%, respectively). There was no significant increase in cardiovascular-related TEAE, changes in vital signs or ECG parameters with the addition of mirabegron to solifenacin 5 mg or 10 mg compared to solifenacin monotherapy at either dose.84 The lack of synergistic effect of combination treatment on cardiovascular safety outcomes supports the earlier findings of both the Symphony and MILAI studies.
A subanalysis of this study, stratified according to age group, demonstrated that efficacy of combination treatment is maintained in older (≥65 years) and elderly (≥75 years) patients without an associated increase in the incidence of TEAEs.85 Change from baseline in the mean number of daily incontinence episodes was –1.75 and –1.73, respectively, in the ≥65 years and ≥75 years age groups. However, when compared to solifenacin 5 mg monotherapy, the treatment difference was not significant (−0.32 [95% CI: −0.69, 0.06] for ≥65 years, and –0.26 [95% CI: −0.94, 0.42] for ≥75 years age groups). Improvements in secondary outcomes were consistently greater with combination treatment versus solifenacin 5 mg or 10 mg, but again, treatment differences did not reach statistical significance.85 The incidence of overall TEAEs was comparable between combination (39% in ≥65 years and 39.7% in ≥75 years age groups) and solifenacin 5 mg (39.4% in ≥65 years and 40.9% in ≥75 years) groups but numerically higher in the solifenacin 10 mg group (48.7% in ≥65 years and 49.1% in ≥75 year age groups). Once again, the most common TEAE was dry mouth which was highest in the solifenacin 10 mg group.
The Japanese MILAI study was an open-label study to examine the safety and efficacy of mirabegron as an “add-on” to solifenacin in patients with OAB.86 Patients (n = 223) continued to receive solifenacin 2.5 or 5 mg and mirabegron 25 mg (escalated to 50 mg) was added. The study demonstrated that mirabegron add-on therapy to solifenacin was well tolerated by Japanese patients, with drug-related adverse events experienced by 23.3%. Common adverse events were consistent with the safety profile of mirabegron and solifenacin monotherapy. The add-on therapy was again associated with improvement in OAB symptoms from baseline to end of treatment.86
In a slight reversal of the MILAI study, the MILAI II study, a multicentre, open-label, phase IV trial, evaluated the safety and efficacy of antimuscarinic add-on therapy over 52 weeks in patients with OAB symptoms treated with mirabegron.87 Six hundred and forty-seven patients were randomised to receive one of four antimuscarinics including solifenacin (SOLI) 5 mg, propiverine (PRO) 20 mg, imidarifenacin (IMI) 0.2 mg or tolterodine (TOL) 4 mg, in addition to current treatment of mirabegron 50 mg. The incidence of drug-related TEAEs was similar across all groups (MIRA+SOLI 45.8%, MIRA+PRO 50.3%, MIRA+IMI 44.7%, MIRA+TOL 46.5%), and in line with previous long-term Japanese studies investigating the use of antimuscarinic monotherapies.88,89 Once again dry mouth and constipation were the most common drug-related adverse events. The cardiovascular safety profile of long-term treatment with mirabegron in combination with antimuscarinics was found to be favourable.90 Overall, 36 TEAEs of interest related to the CV system that were possibly/probably related to treatment were reported, with similar incidences for each group. The majority of these were mild in severity and most had resolved by the end of the study. Higher overall incidences of CV-related TEAEs were reported in the MIRA+SOLI group (6.6%) compared to previous BESIDE and SYNERGY trials, but this may be because of the difference in the length of treatment between the studies (52 weeks compared to 12 weeks in both BESIDE and SYNERGY). Treatment efficacy, measured using changes from baseline in overactive bladder symptom total score and its associated parameters, was demonstrated in all treatment groups (P < 0.001).87
OAB has a negative impact on the QoL of older persons but not all elderly patients have a satisfactory response to treatment with antimuscarinics. A randomised, placebo-controlled trial examined the efficacy and safety of mirabegron (50 mg) and solifenacin (10 mg) in older patients (average age 71.2 years) with OAB.91 Combination treatment provided therapeutic benefit within a short period of time with episodes of incontinence per day decreasing by 3.8 episodes and mean micturition frequency decreasing by 4.0 episodes (p ≤ 0.01). The incidence of adverse events in the combination treatment group was not significantly different to that in patients treated with monotherapy.91
Cost-Effectiveness
In order to evaluate its efficacy and cost effectiveness, the National Institute for Health and Care Excellence (NICE) conducted a Health Technology Assessment of mirabegron.92 As a result of this evaluation, mirabegron was recommended as an option for treating the symptoms of overactive bladder for people in whom anti-muscarinic drugs are contraindicated, clinically ineffective, or have unacceptable side effects. However, due to the small differences in cost between mirabegron and anti-muscarinic agents, the committee concluded it would be difficult to reliably estimate a cost-effectiveness ratio without further evidence.
Cost-equivalence was further examined in an analysis from a UK NHS perspective, which compared mirabegron 50 mg with tolterodine ER 4 mg in adult patients with OAB.93 Total 5-year costs per patient were £1645.62 for mirabegron 50 mg/day and £1607.75 for tolterodine ER 4 mg/day. However, mirabegron was associated with a gain of 0.009 quality-adjusted life years (QALYs) at an additional cost of £37.88. The probability of mirabegron being cost-effective relative to tolterodine ER 4 mg was 89.4% at willingness-to-pay threshold of £20,000 QALY gained (the accepted NICE threshold). Mirabegron is therefore, likely to be cost-effective compared with tolterodine for adults with OAB. Recently, the cost-effectiveness of mirabegron (50 mg) has been compared with oral antimuscarinic agents in adults with OAB from a UK NHS perspective.94 Base case incremental cost-effectiveness ratios (ICERs) ranged from £367 (vs solifenacin 10 mg) to £15,593 (vs oxybutynin IR 10 mg) per QALY gained. Additional sensitivity analysis showed that at a willingness-to-pay threshold of £20,000/QALY gained the probability of mirabegron (50 mg) being cost-effective ranged from 70.2% vs oxybutynin IR 10 mg to 97.8% vs darifencin 15 mg.94
Patients may require several pharmacotherapies for OAB. Previous analyses have evaluated the costs of individual drug therapies for OAB; however, the costs of sequences of drugs, incorporating recently approved agents such as mirabegron, have not previously been conducted. The cost and outcomes associated with different sequences of oral anti-muscarinic agents and mirabegron has recently been evaluated.95 A sequence consisting of two generics and third-line branded therapy (eg, oxybutynin or tolterodine followed by branded treatment) was less effective and associated with costs similar to a sequence consisting of three branded agents (eg, mirabegron first-line and solifenacin second and third-line) with the cost per patient of the standard treatment sequence £1299/patient compared with £1385/patient with the new treatment sequence.95 These drugs are associated with better efficacy, tolerability and persistence, which can lower overall treatment costs.
Conclusions
Mirabegron, is a β3-agonist that selectively targets β3-adrenoceptors over β1 and β2-adrenoceptors. Clinical trial results have demonstrated that mirabegron is clinically effective. Furthermore, due to mirabegron’s specificity of action it offers an additional treatment option for those patients who have discontinued anti-muscarinic therapy. As tolerability is known to be an important factor defining adherence to, or persistence with drug therapy, mirabegron is likely to improve persistence and adherence when compared with other anti-muscarinic agents, due to its low side-effect profile. Economic analysis has also shown mirabegron to be cost-effective when compared to other anti-muscarinic agents, with an acceptable incremental cost justified by an increase in QALYs gained.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
DR has received financial support from Astellas, Pfizer, Allergan, Ferring, and Ixaltis. LC has received funding for research, consultancy and speaker fees from Allergan, Astellas, BMR, Pfizer and Syner-Med. AW has received financial support from Astellas Pharma, SCA, Duchesnay (Canada), Urovant sciences, and Easily hygiene & health; Pfizer Corp for research, consultancy, and speaker fees. PA has received financial support from Astellas, Ferring, Ipsen, Sun Pharma, Cipla, Chiltern, Sanofi, Procter and Gamble, and Pfizer for research, consultancy, and speaker fees. The authors report no other conflicts of interest in this work.
References
1. Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J. 2010;21(1):5–26. doi:10.1007/s00192-009-0976-9
2. Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21(2):167–178. doi:10.1002/nau.10052
3. Irwin DE, Kopp ZS, Agatep B, Milsom I, Abrams P. Worldwide prevalence estimates of lower urinary tract symptoms, overactive bladder, urinary incontinence and bladder outlet obstruction. BJU Int. 2011;108(7):1132–1138. doi:10.1111/j.1464-410X.2010.09993.x
4. Coyne KS, Payne C, Bhattacharyya SK, et al. The impact of urinary urgency and frequency on health-related quality of life in overactive bladder: results from a national community survey. Value Health. 2004;7(4):455–463. doi:10.1111/j.1524-4733.2004.74008.x
5. Coyne KS, Sexton CC, Irwin DE, Kopp ZS, Kelleher CJ, Milsom I. The impact of overactive bladder, incontinence and other lower urinary tract symptoms on quality of life, work productivity, sexuality and emotional well-being in men and women: results from the EPIC study. BJU Int. 2008;101(11):1388–1395. doi:10.1111/j.1464-410X.2008.07601.x
6. Coyne KS, Sexton CC, Kopp ZS, Ebel-Bitoun C, Milsom I, Chapple C. The impact of overactive bladder on mental health, work productivity and health-related quality of life in the UK and Sweden: results from EpiLUTS. BJU Int. 2011;108(9):1459–1471. doi:10.1111/j.1464-410X.2010.10013.x
7. Coyne KS, Sexton CC, Thompson C, Kopp ZS, Milsom I, Kaplan SA. The impact of OAB on sexual health in men and women: results from EpiLUTS. J Sex Med. 2011;8(6):1603–1615. doi:10.1111/j.1743-6109.2011.02250.x
8. Kanai A, Andersson KE. Bladder afferent signaling: recent findings. J Urol. 2010;183(4):1288–1295. doi:10.1016/j.juro.2009.12.060
9. Andersson KE. New developments in the management of overactive bladder: focus on mirabegron and onabotulinumtoxinA. Ther Clin Risk Manag. 2013;9:161–170. doi:10.2147/TCRM.S33052
10. Imran M, Najmi AK, Tabrez S. Mirabegron for overactive bladder: a novel, first-in-class beta3-agonist therapy. Urol J. 2013;10(3):935–940.
11. Abrams P. Describing bladder storage function: overactive bladder syndrome and detrusor overactivity. Urology. 2003;62(5Suppl 2):
12. Andersson KE, Chapple CR, Cardozo L, et al. Pharmacological treatment of overactive bladder: report from the International Consultation on Incontinence. Curr Opin Urol. 2009;19(4):380–394. doi:10.1097/MOU.0b013e32832ce8a4
13. Wagg A, Compion G, Fahey A, Siddiqui E. Persistence with prescribed antimuscarinic therapy for overactive bladder: a UK experience. BJU Int. 2012;110(11):1767–1774. doi:10.1111/j.1464-410X.2012.11023.x
14. Brubaker L, Fanning K, Goldberg EL, et al. Predictors of discontinuing overactive bladder medications. BJU Int. 2009;105(9):1283–1290. doi:10.1111/j.1464-410X.2009.09035.x
15. Sicras-Mainar A, Rejas J, Navarro-Artieda R, et al. Antimuscarinic persistence patterns in newly treated patients with overactive bladder: a retrospective comparative analysis. Int Urogynecol J. 2014;25(4):485–492. doi:10.1007/s00192-013-2250-4
16. Gray SL, Anderson ML, Dublin S, et al. Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med. 2015;175(3):401–407. doi:10.1001/jamainternmed.2014.7663
17. Staskin DR, Zoltan E. Anticholinergics and central nervous system effects: are we confused? Rev Urol Fall. 2007;9(4):191–196.
18. Andersson KE, Arner A. Urinary bladder contraction and relaxation: physiology and pathophysiology. Physiol Rev. 2004;84(3):935–986. doi:10.1152/physrev.00038.2003
19. Otsuka A, Shinbo H, Matsumoto R, Kurita Y, Ozono S. Expression and functional role of beta-adrenoceptors in the human urinary bladder urothelium. Naunyn Schmiedebergs Arch Pharmacol. 2008;377(4–6):473–481. doi:10.1007/s00210-008-0274-y
20. Takeda M, Obara K, Mizusawa T, et al. Evidence for beta3-adrenoceptor subtypes in relaxation of the human urinary bladder detrusor: analysis by molecular biological and pharmacological methods. J Pharmacol Exp Ther. 1999;288(3):1367–1373.
21. Nomiya M, Yamaguchi O. A quantitative analysis of mRNA expression of alpha 1 and beta-adrenoceptor subtypes and their functional roles in human normal and obstructed bladders. J Urol. 2003;170(2 Pt 1):649–653. doi:10.1097/01.ju.0000067621.62736.7c
22. Sacco E, Bientinesi R, Tienforti D, et al. Discovery history and clinical development of mirabegron for the treatment of overactive bladder and urinary incontinence. Expert Opin Drug Discov. 2014;9(4):433–448. doi:10.1517/17460441.2014.892923
23. Hicks A, McCafferty GP, Riedel E, et al. GW427353 (solabegron), a novel, selective beta3-adrenergic receptor agonist, evokes bladder relaxation and increases micturition reflex threshold in the dog. J Pharmacol Exp Ther. 2007;323(1):202–209. doi:10.1124/jpet.107.125757
24. Takasu T, Ukai M, Sato S, et al. Effect of (R)-2-(2-aminothiazol-4-yl)-4’-{2-[(2-hydroxy-2-phenylethyl)amino]ethyl} acetanilide (YM178), a novel selective beta3-adrenoceptor agonist, on bladder function. J Pharmacol Exp Ther. 2007;321(2):642–647. doi:10.1124/jpet.106.115840
25. US Food and Drug Administration [homepage on intranet]. Approved drug products with therapeutic equivalence evaluations; 2020. Available from: https://www.fda.gov/media/136324/download.
26. European Medicines Agency [homepage on the intranet]. Amsterdam: human medicine European public assessment report (EPAR): betmiga; 2012. Available from: https://www.ema.europa.eu/en.
27. Astellas [press release]. FDA approves overactive bladder treatment myrbetriqTM (mirabegron) from Astellas; 2012. Available from: https://www.astellas.com/en/.
28. Australian Therapeutic Goods Administration [homepage on the intranet]. Australian public assessment report: mirabegron; 2014. Available from: https://www.tga.gov.au.
29. Limberg BJ, Andersson KE, Aura Kullmann F, Burmer G, de Groat WC, Rosenbaum JS. beta-Adrenergic receptor subtype expression in myocyte and non-myocyte cells in human female bladder. Cell Tissue Res. 2010;342(2):295–306. doi:10.1007/s00441-010-1053-x
30. Hatanaka T, Ukai M, Watanabe M, et al. Effect of mirabegron, a novel beta3-adrenoceptor agonist, on bladder function during storage phase in rats. Naunyn Schmiedebergs Arch Pharmacol. 2013;386(1):71–78. doi:10.1007/s00210-012-0814-3
31. Aizawa N, Homma Y, Igawa Y. Effects of mirabegron, a novel beta3-adrenoceptor agonist, on primary bladder afferent activity and bladder microcontractions in rats compared with the effects of oxybutynin. Eur Urol. 2012;62(6):1165–1173. doi:10.1016/j.eururo.2012.08.056
32. US Food and Drug Administration [homepage on intranet]. Center for drug evaluation and research pharmacology review(s); 2012. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/202611Orig1s000PharmR.pdf.
33. Krauwinkel W, van Dijk J, Schaddelee M, et al. Pharmacokinetic properties of mirabegron, a beta3-adrenoceptor agonist: results from two Phase I, randomized, multiple-dose studies in healthy young and elderly men and women. Clin Ther. 2012;34(10):2144–2160. doi:10.1016/j.clinthera.2012.09.010
34. Iitsuka H, Tokuno T, Amada Y, et al. Pharmacokinetics of mirabegron, a beta3-adrenoceptor agonist for treatment of overactive bladder, in healthy Japanese male subjects: results from single- and multiple-dose studies. Clin Drug Investig. 2014;34(1):27–35. doi:10.1007/s40261-013-0146-1
35. US Food and Drug Administration [homepage on intranet]. Center for drug evaluation and research clinical pharmacology and biopharmaceutics review(s); 2012. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/202611Orig1s000ClinPharmR.pdf.
36. Takusagawa S, van Lier JJ, Suzuki K, et al. Absorption, metabolism and excretion of [(14)C]mirabegron (YM178), a potent and selective beta(3)-adrenoceptor agonist, after oral administration to healthy male volunteers. Drug Metab Dispos. 2012;40(4):815–824. doi:10.1124/dmd.111.043588
37. Iitsuka H, van Gelderen M, Katashima M, Takusagawa S, Sawamoto T. Pharmacokinetics of mirabegron, a beta3-adrenoceptor agonist for treatment of overactive bladder, in Healthy East Asian Subjects. Clin Ther. 2015;37(5):1031–1044. doi:10.1016/j.clinthera.2015.02.021
38. Chapple CR, Amarenco G, Lopez Aramburu MA, et al. A proof-of-concept study: mirabegron, a new therapy for overactive bladder. Neurourol Urodyn. 2013;32(8):1116–1122. doi:10.1002/nau.22373
39. Chapple CR, Dvorak V, Radziszewski P, et al. A phase II dose-ranging study of mirabegron in patients with overactive bladder. Int Urogynecol J. 2013;24(9):1447–1458. doi:10.1007/s00192-013-2042-x
40. Malik M, van Gelderen EM, Lee JH, et al. Proarrhythmic safety of repeat doses of mirabegron in healthy subjects: a randomized, double-blind, placebo-, and active-controlled thorough QT study. Clin Pharmacol Ther. 2012;92(6):696–706. doi:10.1038/clpt.2012.181
41. Khullar V, Amarenco G, Angulo JC, et al. Efficacy and tolerability of mirabegron, a beta(3)-adrenoceptor agonist, in patients with overactive bladder: results from a randomised European-Australian Phase 3 trial. Eur Urol. 2013;63(2):283–295. doi:10.1016/j.eururo.2012.10.016
42. Khullar V, Cambronero J, Angulo JC, et al. Efficacy of mirabegron in patients with and without prior antimuscarinic therapy for overactive bladder: a post hoc analysis of a randomized European-Australian Phase 3 trial. BMC Urol. 2013;13:45. doi:10.1186/1471-2490-13-45
43. Nitti VW, Auerbach S, Martin N, Calhoun A, Lee M, Herschorn S. Results of a randomized phase III trial of mirabegron in patients with overactive bladder. J Urol. 2013;189(4):1388–1395. doi:10.1016/j.juro.2012.10.017
44. Herschorn S, Barkin J, Castro-Diaz D, et al. A phase III, randomized, double-blind, parallel-group, placebo-controlled, multicentre study to assess the efficacy and safety of the beta(3) adrenoceptor agonist, mirabegron, in patients with symptoms of overactive bladder. Urology. 2013;82(2):313–320. doi:10.1016/j.urology.2013.02.077
45. Wagg A, Nitti VW, Kelleher C, Castro-Diaz D, Siddiqui E, Berner T. Oral pharmacotherapy for overactive bladder in older patients: mirabegron as a potential alternative to antimuscarinics. Curr Med Res Opin. 2016;32(4):621–638. doi:10.1185/03007995.2016.1149806
46. Yamaguchi O, Marui E, Igawa Y, et al. Efficacy and safety of the selective beta3 -adrenoceptor agonist mirabegron in Japanese patients with overactive bladder: a randomized, double-blind, placebo-controlled, dose-finding study. Low Urin Tract Symptoms. 2015;7(2):84–92. doi:10.1111/luts.12053
47. Matsukawa Y, Takai S, Funahashi Y, Yamamoto T, Gotoh M. Urodynamic evaluation of the efficacy of mirabegron on storage and voiding functions in women with overactive bladder. Urology. 2015;85(4):786–790. doi:10.1016/j.urology.2015.01.002
48. Kuo HC, Lee KS, Na Y, et al. Results of a randomized, double-blind, parallel-group, placebo- and active-controlled, multicenter study of mirabegron, a beta3-adrenoceptor agonist, in patients with overactive bladder in Asia. Neurourol Urodyn. 2015;34(7):685–692. doi:10.1002/nau.22645
49. Yamaguchi O, Marui E, Kakizaki H, et al. Phase III, randomised, double-blind, placebo-controlled study of the beta3-adrenoceptor agonist mirabegron, 50 mg once daily, in Japanese patients with overactive bladder. BJU Int. 2014;113(6):951–960. doi:10.1111/bju.12649
50. Takahashi S, Mishima Y, Kuroishi K, Ukai M. Efficacy of mirabegron, a beta3 -adrenoreceptor agonist, in Japanese women with overactive bladder and either urgency urinary incontinence or mixed urinary incontinence: post-hoc analysis of pooled data from two randomized, placebo-controlled, double-blind studies. Int J Urol. 2022;29(1):7–15. doi:10.1111/iju.14700
51. Chapple CR, Kaplan SA, Mitcheson D, et al. Randomized double-blind, active-controlled phase 3 study to assess 12-month safety and efficacy of mirabegron, a beta(3)-adrenoceptor agonist, in overactive bladder. Eur Urol. 2013;63(2):296–305. doi:10.1016/j.eururo.2012.10.048
52. Yamaguchi O, Ikeda Y, Ohkawa S. Phase III study to assess long-term (52-week) safety and efficacy of mirabegron, a β3-adrenoceptor agonist, in Japanese patients with overactive bladder. Low Urin Tract Symptoms. 2015. doi:10.1111/luts.12107
53. Nitti VW, Chapple CR, Walters C, et al. Safety and tolerability of the beta3 -adrenoceptor agonist mirabegron, for the treatment of overactive bladder: results of a prospective pooled analysis of three 12-week randomised Phase III trials and of a 1-year randomised Phase III trial. Int J Clin Pract. 2014;68(8):972–985. doi:10.1111/ijcp.12433
54. Rosa GM, Ferrero S, Nitti VW, Wagg A, Saleem T, Chapple CR. Cardiovascular safety of beta3-adrenoceptor agonists for the treatment of patients with overactive bladder syndrome. Eur Urol. 2016;69(2):311–323. doi:10.1016/j.eururo.2015.09.007
55. Batista JE, Kolbl H, Herschorn S, et al. The efficacy and safety of mirabegron compared with solifenacin in overactive bladder patients dissatisfied with previous antimuscarinic treatment due to lack of efficacy: results of a noninferiority, randomized, phase IIIb trial. Ther Adv Urol. 2015;7(4):167–179. doi:10.1177/1756287215589250
56. Wagg A, Staskin D, Engel E, Herschorn S, Kristy RM, Schermer CR. Efficacy, safety, and tolerability of mirabegron in patients aged >/=65yr with overactive bladder wet: a phase IV, double-blind, randomised, placebo-controlled study (PILLAR). Eur Urol. 2020;77(2):211–220. doi:10.1016/j.eururo.2019.10.002
57. Herschorn S, Staskin D, Schermer CR, Kristy RM, Wagg A. Safety and tolerability results from the PILLAR study: a Phase IV, double-blind, randomized, placebo-controlled study of mirabegron in patients >/= 65 years with overactive bladder-wet. Drugs Aging. 2020;37(9):665–676. doi:10.1007/s40266-020-00783-w
58. Griebling TL, Campbell NL, Mangel J, et al. Effect of mirabegron on cognitive function in elderly patients with overactive bladder: moCA results from a Phase 4 randomized, placebo-controlled study (PILLAR). BMC Geriatr. 2020;20(1):109. doi:10.1186/s12877-020-1474-7
59. Blais AS, Nadeau G, Moore K, Genois L, Bolduc S. Prospective pilot study of mirabegron in pediatric patients with overactive bladder. Eur Urol. 2016;70(1):9–13. doi:10.1016/j.eururo.2016.02.007
60. Kim SC, Park M, Chae C, et al. Efficacy and tolerability of mirabegron compared with solifenacin for children with idiopathic overactive bladder: a preliminary study. Investig Clin Urol. 2021;62(3):317–323. doi:10.4111/icu.20200380
61. Soliman MG, El-Abd S, El-Gamal OM, Raheem AA, Abou-Ramadan AR, El-Abd AS. Mirabegron versus solifenacin in children with overactive bladder: prospective randomized single-blind controlled trial. Urol Int. 2021;105(11–12):1011–1017. doi:10.1159/000515992
62. Baka-Ostrowska M, Bolong DT, Persu C, et al. Efficacy and safety of mirabegron in children and adolescents with neurogenic detrusor overactivity: an open-label, phase 3, dose-titration study. Neurourol Urodyn. 2021;40(6):1490–1499. doi:10.1002/nau.24657
63. Khullar V, Amarenco G, Angulo JC, et al. Patient-reported outcomes with the beta -adrenoceptor agonist mirabegron in a phase III trial in patients with overactive bladder. Neurourol Urodyn. 2015. doi:10.1002/nau.22844
64. Carlson KV, Rovner ES, Nair KV, Deal AS, Kristy RM, Schermer CR. Factors associated with improvements in patient-reported outcomes during mirabegron or antimuscarinic treatment of overactive bladder syndrome: a registry study (PERSPECTIVE). Adv Ther. 2019;36(8):1906–1921. doi:10.1007/s12325-019-00994-7
65. Castro-Diaz D, Chapple CR, Hakimi Z, et al. The effect of mirabegron on patient-related outcomes in patients with overactive bladder: the results of post hoc correlation and responder analyses using pooled data from three randomized Phase III trials. Qual Life Res. 2015;24(7):1719–1727. doi:10.1007/s11136-014-0904-4
66. Yu YF, Nichol MB, Yu AP, Ahn J. Persistence and adherence of medications for chronic overactive bladder/urinary incontinence in the California medicaid program. Value Health. 2005;8(4):495–505. doi:10.1111/j.1524-4733.2005.00041.x
67. World Health Organization. Adherence to long-term therapies: evidence for action; 2003. Available from: http://www.who.int/chp/knowledge/publications/adherence_report/en/.
68. Brostrom S, Hallas J. Persistence of antimuscarinic drug use. Eur J Clin Pharmacol. 2009;65(3):309–314. doi:10.1007/s00228-008-0600-9
69. Wagg A, Foley S, Peters J, Scrine L. Persistence with mirabegron, a beta-3 adrenoceptor agonist, versus antimuscarinics in patients with over-active bladder: early UK experience. Eur Urol. 2015;14(2):e267–e267a.
70. Wagg A, Franks B, Ramos B, Berner T. Persistence and adherence with mirabegron, a new beta-3 receptor agonist, versus antimuscarinics in overactive bladder: early experience in Canada. Value Health. 2014;17(7):A471. doi:10.1016/j.jval.2014.08.1336
71. Wagg A, Franks B, Ramos B, Berner T. Persistence and adherence with the new beta-3 receptor agonist, mirabegron, versus antimuscarinics in overactive bladder: early experience in Canada. Can Urol Assoc J. 2015;9(9–10):343–350. doi:10.5489/cuaj.3098
72. Carlson KV, Rovner ES, Nair KV, Deal AS, Kristy RM, Hairston JC. Persistence with mirabegron or antimuscarinic treatment for overactive bladder syndrome: findings from the PERSPECTIVE registry study. Low Urin Tract Symptoms. 2021;13(4):425–434. doi:10.1111/luts.12382
73. Duckett J, Balachandran A. Tolerability and persistence in a large, prospective case series of women prescribed mirabegron. Int Urogynecol J. 2016. doi:10.1007/s00192-016-2945-4
74. Pindoria N, Malde S, Nowers J, Taylor C, Kelleher C, Sahai A. Persistence with mirabegron therapy for overactive bladder: a real life experience. Neurourol Urodyn. 2015. doi:10.1002/nau.22943
75. Staskin D, Herschorn S, Fialkov J, Tu LM, Walsh T, Schermer CR. A prospective, double-blind, randomized, two-period crossover, multicenter study to evaluate tolerability and patient preference between mirabegron and tolterodine in patients with overactive bladder (PREFER study). Int Urogynecol J. 2018;29(2):273–283. doi:10.1007/s00192-017-3377-5
76. Herschorn S, Staskin D, Tu LM, et al. Patient-reported outcomes in patients with overactive bladder treated with mirabegron and tolterodine in a prospective, double-blind, randomized, two-period crossover, multicenter study (PREFER). Health Qual Life Outcomes. 2018;16(1):69. doi:10.1186/s12955-018-0892-0
77. Abrams P, Kelleher C, Staskin D, et al. Combination treatment with mirabegron and solifenacin in patients with overactive bladder: efficacy and safety results from a randomised, double-blind, dose-ranging, Phase 2 study (Symphony). Eur Urol. 2015;67(3):577–588. doi:10.1016/j.eururo.2014.02.012
78. Abrams P, Kelleher C, Staskin D, et al. Combination treatment with mirabegron and solifenacin in patients with overactive bladder: exploratory responder analyses of efficacy and evaluation of patient-reported outcomes from a randomized, double-blind, factorial, dose-ranging, Phase II study (SYMPHONY). World J Urol. 2017;35(5):827–838. doi:10.1007/s00345-016-1908-1
79. Herschorn S, Chapple CR, Abrams P, et al. Efficacy and safety of combinations of mirabegron and solifenacin compared with monotherapy and placebo in patients with overactive bladder (SYNERGY study). BJU Int. 2017;120(4):562–575. doi:10.1111/bju.13882
80. White WB, Chapple C, Gratzke C, et al. Cardiovascular safety of the beta3 -adrenoceptor agonist mirabegron and the antimuscarinic agent solifenacin in the SYNERGY trial. J Clin Pharmacol. 2018;58(8):1084–1091. doi:10.1002/jcph.1107
81. Weber MA, Chapple CR, Gratzke C, et al. A strategy utilizing ambulatory monitoring and home and clinic blood pressure measurements to optimize the safety evaluation of noncardiovascular drugs with potential for hemodynamic effects: a report from the SYNERGY trial. Blood Press Monit. 2018;23(3):153–163. doi:10.1097/MBP.0000000000000320
82. Mueller ER, van Maanen R, Chapple C, et al. Long-term treatment of older patients with overactive bladder using a combination of mirabegron and solifenacin: a prespecified analysis from the randomized, phase III SYNERGY II study. Neurourol Urodyn. 2019;38(2):779–792. doi:10.1002/nau.23919
83. Drake MJ, Chapple C, Esen AA, et al. Efficacy and safety of mirabegron add-on therapy to solifenacin in incontinent overactive bladder patients with an inadequate response to initial 4-week solifenacin monotherapy: a randomised double-blind multicentre Phase 3b study (BESIDE). Eur Urol. 2016. doi:10.1016/j.eururo.2016.02.030
84. Drake MJ, MacDiarmid S, Chapple CR, et al. Cardiovascular safety in refractory incontinent patients with overactive bladder receiving add-on mirabegron therapy to solifenacin (BESIDE). Int J Clin Pract. 2017;71(5). doi:10.1111/ijcp.12944
85. Gibson W, MacDiarmid S, Huang M, et al. Treating overactive bladder in older patients with a combination of mirabegron and solifenacin: a prespecified analysis from the BESIDE study. Eur Urol Focus. 2017;3(6):629–638. doi:10.1016/j.euf.2017.08.008
86. Yamaguchi O, Kakizaki H, Homma Y, et al. Safety and efficacy of mirabegron as ‘add-on’ therapy in patients with overactive bladder treated with solifenacin: a post-marketing, open-label study in Japan (MILAI study). BJU Int. 2015;116(4):612–622. doi:10.1111/bju.13068
87. Yamaguchi O, Kakizaki H, Homma Y, et al. Long-term safety and efficacy of antimuscarinic add-on therapy in patients with overactive bladder who had a suboptimal response to mirabegron monotherapy: a multicenter, randomized study in Japan (MILAI II study). Int J Urol. 2019;26(3):342–352. doi:10.1111/iju.13868
88. Takei M, Homma Y; Japanese Tolterodine Study G. Long-term safety, tolerability and efficacy of extended-release tolterodine in the treatment of overactive bladder in Japanese patients. Int J Urol. 2005;12(5):456–464. doi:10.1111/j.1442-2042.2005.01066.x
89. Homma Y, Yamaguchi O. Long-term safety, tolerability, and efficacy of the novel anti-muscarinic agent imidafenacin in Japanese patients with overactive bladder. Int J Urol. 2008;15(11):986–991. doi:10.1111/j.1442-2042.2008.02152.x
90. Katoh T, Igawa Y, Yamaguchi O, Kato D, Hamada T, Kuroishi K. Cardiovascular safety of antimuscarinic add-on therapy in patients with overactive bladder who had a suboptimal response to mirabegron monotherapy: a post hoc analysis from the Japanese MILAI II study. Low Urin Tract Symptoms. 2020;12(1):68–80. doi:10.1111/luts.12286
91. Kosilov K, Loparev S, Ivanovskaya M, Kosilova L. A randomized, controlled trial of effectiveness and safety of management of OAB symptoms in elderly men and women with standard-dosed combination of solifenacin and mirabegron. Arch Gerontol Geriatr. 2015;61(2):212–216. doi:10.1016/j.archger.2015.06.006
92. NICE. NICE technology appraisal guidance [TA290] Mirabegron for treating symptoms of overactive bladder; 2013. Available from: https://www.nice.org.uk/guidance/ta290.
93. Aballea S, Maman K, Thokagevistk K, et al. Cost effectiveness of mirabegron compared with tolterodine extended release for the treatment of adults with overactive bladder in the United Kingdom. Clin Drug Investig. 2015;35(2):83–93. doi:10.1007/s40261-014-0240-z
94. Nazir J, Maman K, Neine ME, et al. Cost-effectiveness of mirabegron compared with antimuscarinic agents for the treatment of adults with overactive bladder in the United Kingdom. Value Health. 2015;18(6):783–790. doi:10.1016/j.jval.2015.05.011
95. Nazir J, Posnett J, Walker A, Odeyemi IA, Hakimi Z, Garnham A. Economic evaluation of pharmacological treatments for overactive bladder from the perspective of the UK National Health Service. J Med Econ. 2015;18(5):390–397. doi:10.3111/13696998.2014.995300
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Vibegron 50 mg Once Daily Improves OABSS, OAB-q SF Score in OAB Patients ≥80 Years Old in Real-World Clinical Settings and Switching from Other OAB Drugs May Reduce Residual Urine Volume
Kuno T, Tamura K, Shimizu N, Fukuhara H, Fukata S, Ashida S, Karashima T, Satake H, Sawada K, Yamasaki I, Komatsu F, Kuroiwa H, Saito M, Inoue K
Research and Reports in Urology 2023, 15:157-164
Published Date: 22 May 2023