")
Back to Journals » Research and Reports in Urology » Volume 15
Vibegron 50 mg Once Daily Improves OABSS, OAB-q SF Score in OAB Patients ≥80 Years Old in Real-World Clinical Settings and Switching from Other OAB Drugs May Reduce Residual Urine Volume
Authors Kuno T, Tamura K , Shimizu N , Fukuhara H, Fukata S, Ashida S, Karashima T, Satake H, Sawada K, Yamasaki I, Komatsu F, Kuroiwa H , Saito M, Inoue K
Received 9 March 2023
Accepted for publication 16 May 2023
Published 22 May 2023 Volume 2023:15 Pages 157—164
DOI https://doi.org/10.2147/RRU.S411841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Guglielmo Mantica
Takahira Kuno,1,2 Kenji Tamura,1,3 Nobutaka Shimizu,1 Hideo Fukuhara,1 Satoshi Fukata,1 Shingo Ashida,1 Takashi Karashima,1 Hirofumi Satake,3 Kohji Sawada,4 Ichiro Yamasaki,5 Fumito Komatsu,2 Hajime Kuroiwa,6 Motoaki Saito,7 Keiji Inoue1
1Department of Urology, Kochi Medical School, Kochi University, Nankoku, Japan; 2Department of Urology, Tosa Municipal Hospital, Tosa, Japan; 3Department of Urology, Chikamori Hospital, Kochi, Japan; 4Department of Urology, Kochi Prefectural Hata Kenmin Hospital, Sukumo, Japan; 5Department of Urology, Kubokawa Hospital, Takaoka-gun, Japan; 6Integrated Center for Advanced Medical Technologies (ICAM-Tech), Kochi Medical School, Nankoku, Japan; 7Department of Pharmacology, Kochi Medical School, Kochi University, Nankoku, Japan
Correspondence: Kenji Tamura, Email [email protected]
Objective: The treatment effects of vibegron have not previously been evaluated in a prospective, non-interventional observational study of elderly Japanese patients, particularly those ≥ 80 years old. In addition, no reports have referred to residual urine volume in switching cases. We therefore grouped patients by condition and investigated the treatment effects of vibegron on Overactive Bladder Symptom Score (OABSS), Overactive Bladder Questionnaire Short Form (OAB-q SF), and residual urine volume in each group.
Methods: This multicenter, prospective, non-interventional, observational study consecutively enrolled OAB patients with total OABSS score ≥ 3 and OABSS question 3 score ≥ 2. Sixty-three patients from six centers were recruited. Vibegron 50 mg once daily was administered for 12 weeks as first-line monotherapy (first-line group), monotherapy switching from antimuscarinics or mirabegron due to failure of prior therapy (no washout period), or combination therapy with antimuscarinics (second-line group). OABSS, OAB-q SF, and residual urine volume were collected after 4 and 12 weeks. Adverse events were also recorded at each visit.
Results: Of the 63 patients registered, 61 were eligible for analysis (first line, n=36; second line, n=25). The OABSS, excluding daytime frequency scores, and OAB-q SF scale showed significant improvement in all conditions. Switching from mirabegron to vibegron significantly reduced residual urine volume. No serious treatment-related adverse events were encountered.
Conclusion: Vibegron 50 mg once daily significantly improved OABSS and OAB-q SF even in patients ≥ 80 years old. Notably, switching from mirabegron to vibegron resulted in significant improvements to residual urine volume.
Keywords: selective β 3-adrenoreceptor agonist, overactive bladder, residual urine volume, vibegron, mirabegron
Introduction
Overactive bladder (OAB) is a syndrome involving symptoms such as “urinary urgency”, “pollakiuria”, and “nocturia” due to causes such as aging and neurological disease.1,2 OAB interferes with daily life and acts to deteriorate quality of life (QOL). Pharmacotherapy, usually using anticholinergics or β3-adrenergic receptor agonists, is the mainstay of treatment for OAB.3 However, anticholinergic drugs are often poorly tolerated, leading to low adherence and discontinuation.4,5 The continuation rate for oral administration of anticholinergic drugs is reportedly 8–25%.6,7 Mirabegron, a β3-adrenergic receptor (AR) agonist, improves adherence as an alternative to antimuscarinic drugs.6 A network meta-analysis revealed that mirabegron 50 mg was significantly more therapeutic than placebo and comparable to common antimuscarinic drugs, with fewer anticholinergic side effects such as dry mouth and constipation, and was well tolerated.8 However, mirabegron is known to inhibit CYP2D6, a cytochrome P450 (CYP450) enzyme, so drug-drug interactions need to be considered.9 In September 2018, vibegron, a selective β3 adrenoreceptor agonist, was approved in Japan for the treatment of OAB.10 Vibegron does not appear to be metabolized by CYP3A4 or CYP2D6,11 reducing the risk of drug interactions.
The prevalence of OAB tends to increase with age, and the 2012 population in Japan included an estimated 10.4 million OAB patients. In addition, the number of OAB patients is expected to increase with the continued aging of the population.12 In a previous study, the efficacy of vibegron treatment was confirmed in not only patients ≥65 years old, but also patients ≥75 years old.13 In clinical settings, aging populations provide more opportunities to prescribe to older age groups. However, no reports appear to have evaluated the therapeutic effects of vibegron in older patient populations in clinical settings. In addition, residual urine volume in patients switching from mirabegron has yet to be clarified. We therefore grouped patients by condition and investigated the treatment effect of vibegron on the Overactive Bladder Symptom Score (OABSS), Overactive Bladder Questionnaire Short Form (OAB-q SF), and residual urine volume in each group.
Materials and Methods
Study Design and Patients
This prospective, non-interventional, observational study investigated Japanese men and women treated with vibegron 50 mg once daily and was conducted in an ambulatory care setting. Patients were followed-up to the last treatment (if treatment was discontinued prior to 12 weeks) for surveillance periods of 12±2 weeks. The study population for effectiveness analyses included all patients with both baseline (0 weeks) and endpoint observations (at 12±2 weeks or at an early discontinuation visit).
Ethics Statement
The institutional review board at each participating center approved this study. All patients provided written informed consent, in accordance with the guiding principles of the Declaration of Helsinki. Treatment for OAB was prescribed according to the usual standard of care and was not provided by the study sponsor.
Inclusion and Exclusion Criteria
Patients included in the study were men and women ≥40 years old who had been diagnosed with OAB (selection criteria: total OABSS ≥ 3 and OABSS question 3 score ≥ 2) and who had been newly prescribed vibegron at 50 mg once daily. Patients with any of the following contraindications were excluded: hypersensitivity to vibegron; urinary tract cancer; judgment as ineligible by the attending physician; or no provision of consent. The decision to enroll a patient was made at the discretion of the investigator.
Endpoints
Data were obtained from case report forms by investigators. The primary endpoints were changes in OABSS, OAB-q SF and residual urine output. The secondary endpoint was to evaluate the safety of vibegron 50 mg once daily treatment by analyzing adverse events. Investigators used the verified Japanese-language versions of the OABSS and OAB-q SF questionnaires14–16 to assess the severity of symptoms at study baseline (0 weeks), 4 weeks and 12 weeks. Safety and efficacy were evaluated according to patient age, comorbidities, concomitant medications, and conditions of vibegron use (ie, monotherapy, etc) for more than 12 weeks.
Statistical Analyses
Descriptive statistics are presented as mean ± standard deviation for continuous variables, unless otherwise indicated, and frequency and percentage are presented for categorical variables. Statistical analyses were performed using the paired t-test. We evaluated the efficacy of vibegron in patients with OAB ≥80 years old and in patients switched from mirabegron. No imputation was applied for missing or discontinuous data. Two-sided values of p<0.05 were considered to indicate statistical significance. Statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (R Foundation for Statistical Computing, Vienna, Austria).17
Results
Analysis Populations
A total of 63 patients were included in the safety analysis. The baseline demographics of participants are shown in Figure 1. Of these, 61 patients were included in the 12-week surveillance effectiveness analysis. One patient chose to withdraw from the study and one patient forgot to visit to hospital in the 12th week. After excluding these two cases, 61 patients remained in the final statistical analysis. Of the 61 eligible patients, 36 and 25 received vibegron in the first- and second-line (post-OAB drug) groups, respectively (Figure 1). Forty-two participants (68.9%) were female and 21 (34.4%) were ≥80 years old (Table 1).
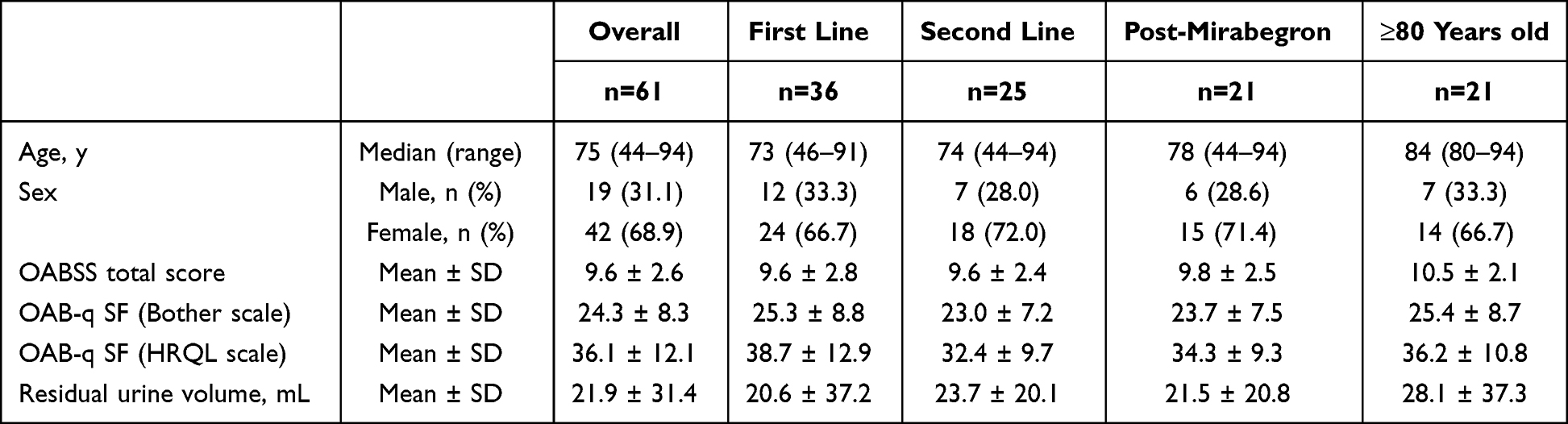 |
Table 1 Baseline Demographics and Clinical Characteristics |
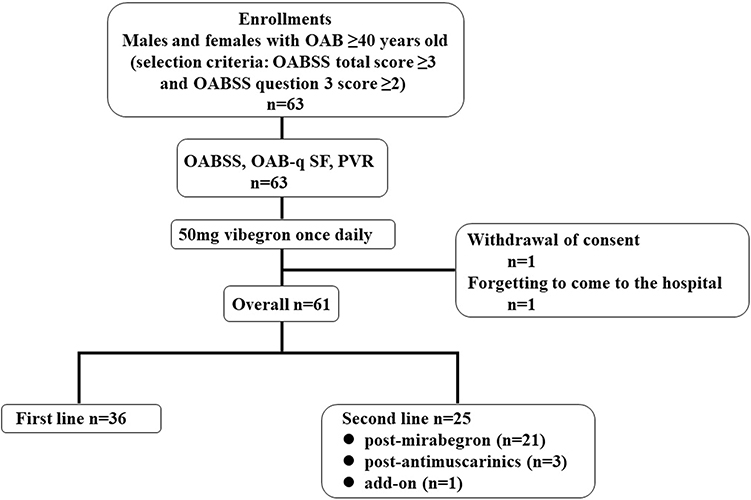 |
Figure 1 Study flow-chart. OAB patients ≥40 years old with an OABSS total score of 3 or more and an OABSS Question 3 score of 2 or more were enrolled. A total of 63 patients were included in the safety analysis and of these, 61 patients (males, n=19; females, n=42) were included in the 12-week surveillance efficacy analysis (first line, n=36; post-antimuscarinics, n=3; post-mirabegron, n=21; add-on, n=1). One patient chose to discontinue the study and one patient forgot to go to the hospital at the 12th week. Abbreviations: OABSS, Overactive Bladder Symptom Score; OAB-q SF, Overactive Bladder Questionnaire Short-Form; PVR, Post Residual Void. |
Demographics, Baseline Clinical Characteristics, and Concomitant Medications
Median age of the safety population was 75 years (range; 44–94 years) for the overall cohort, 78 years (range; 44–94 years) for patients who had switched from mirabegron, and 84 years (range; 80–94 years) for patients ≥80 years old (Table 1). The most common comorbidities were cardiovascular disease (including hypertension, 59%), diabetes mellitus (18%), and a history of cerebrovascular accidents (11%) (data not shown). Twenty-five people were already taking OAB medications, 21 of whom had switched from mirabegron (two of whom were also continuing to take anticholinergic drugs that had already been used in combination pharmacotherapy), three had switched from anticholinergic drugs, and one added vibegron to anticholinergic drugs already being taken (data not shown). Concomitant anticholinergic agents were not changed or added before or after administration of vibegron. Fourteen of the 19 men were already taking medications for benign prostatic hyperplasia (BPH) (phosphodiesterase-5 inhibitors, n=5; alpha blockers, n=9). No additional or modified medications were added during the observation period. We believe that interference from other drugs could be ruled out, because no contraindicated agents were administered in combination with vibegron and no additions or changes were made during the observation period, including drugs for comorbidities.
Safety: Treatment-Emergent Adverse Events
Only one man experienced grade 1 dizziness (CTCAE v5.0), but he recovered spontaneously while taking vibegron. The causality of the relationship with vibegron is therefore unclear. Dizziness is a known adverse event, observed in 0.9% of participants in Phase III trials.18
Effectiveness
Figure 2 shows symptomatic changes by group. Mean values of each score and changes from baseline were plotted at 4 weeks and 12 weeks. Comparisons from baseline at 4-week time points and the 12-week endpoint showed significant improvements in all parameters except residual urine volume (Figure 2A and Figure 2). Interestingly, the second-line group (Figure 2C) showed a significant improvement in residual urine volume when comparing baseline and the 12-week endpoint. Next, since a significant improvement was observed in the second-line group (n=25), we narrowed down patients to the group of 21 patients who had switched from mirabegron, which accounted for the majority of the second-line group, and performed the evaluations again. We also evaluated the group of 21 patients ≥80 years old, as a group that should be noted clinically. Table 2 shows changes in subjective symptoms under each condition. Similar to the results for the second-line group, switching from mirabegron resulted in significant improvements to all parameters, including residual urine volume. In patients ≥80 years old, significant improvements were confirmed in each score except daytime frequency score and residual urine volume (Table 2).
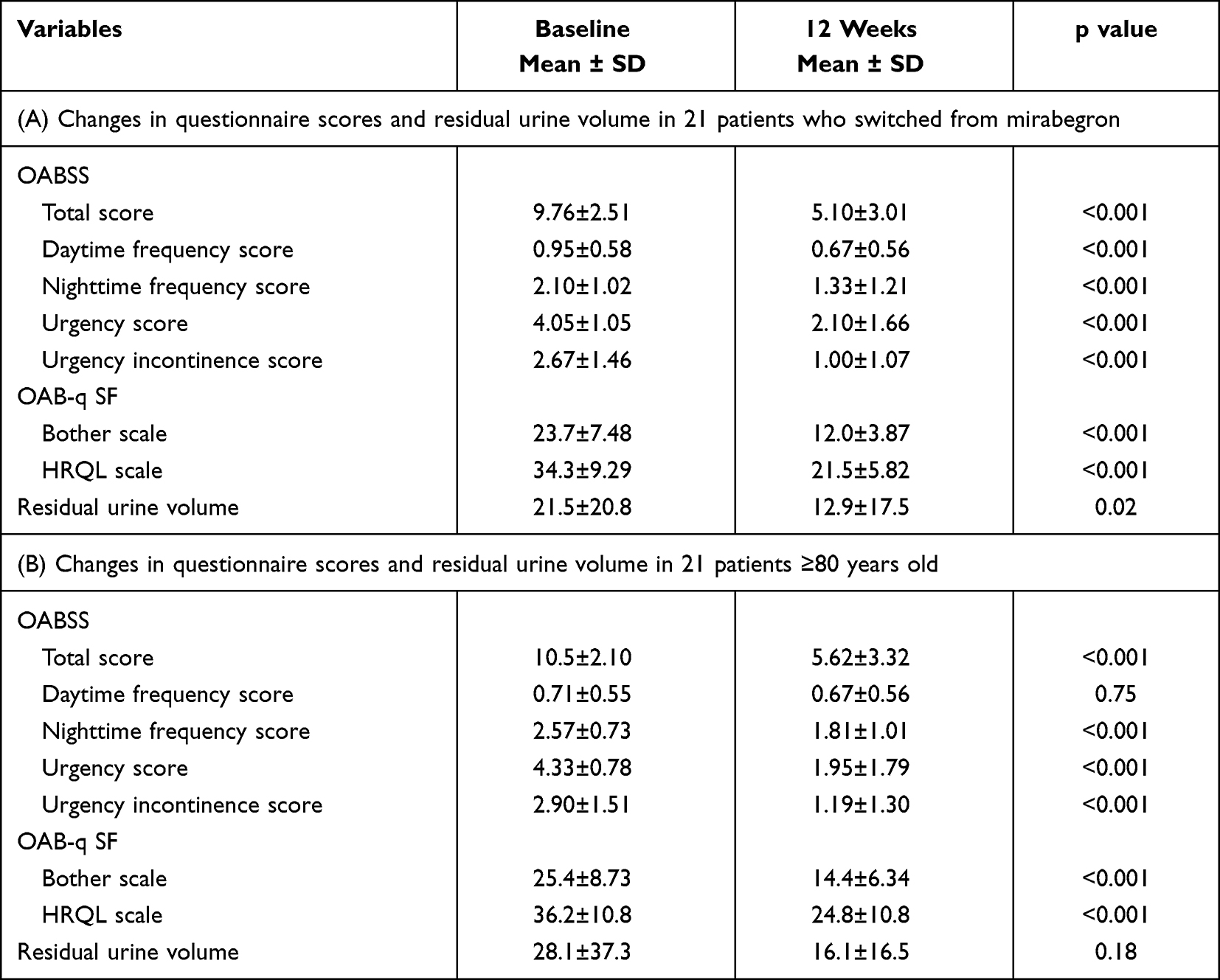 |
Table 2 Changes in Subjective Symptoms and Residual Urine Volume in Each Condition |
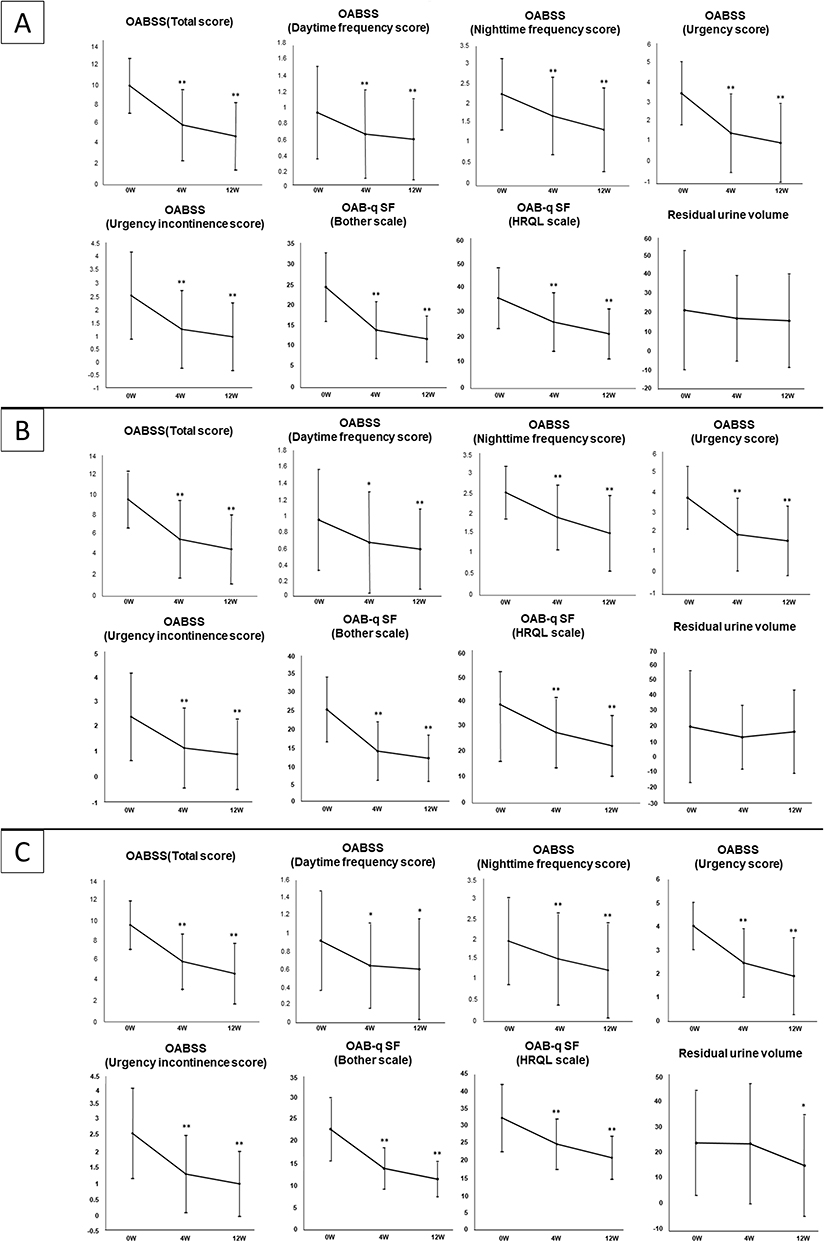 |
Figure 2 Changes in each parameter (OABSS, OAB-q SF) and residual urine volume in each group of (A) Overall, (B) First line, (C) Second line. Each score is shown for the 4- and 12-week surveillance time points. Error bars represent ± SD. *p<0.05, when compared with paired t-test to 0 weeks in each group. **p<0.01, when compared with paired t-test to 0 weeks in each group. Abbreviations: OABSS, Overactive Bladder Symptom Score; OAB-q SF, Overactive Bladder Questionnaire Short-Form; SD, standard deviation. |
Discussion
In this study, administration of vibegron 50 mg once daily for 12 weeks was effective for the entire OAB population, including elderly patients ≥80 years old. In reports of vibegron, comparisons are often made between groups using a threshold age of 65 years. In addition, vibegron 75 mg has been reported as effective even in patients ≥75 years old.13 The aging of the population is a global phenomenon, and Japan is aging ahead of the rest of the world. By 2030, one-third of the Japanese population is expected to be ≥65 years old and 20% will be ≥75 years old.19 Currently, the average life expectancy in Japan exceeds 80 years for both women and men.19 Given that the prevalence of OAB increases with age,20 confirming the efficacy of vibegron in elderly populations is clinically important.
In this study, we examined each parameter in the overall cohort and in both first- and second-line groups (Figure 2). The second-line group had no washout period when switching from other OAB drugs, and immediate switching was performed because the previous treatment was ineffective. Three patients switched from antimuscarinics and one patient started vibegron as an add-on drug. These patients were grouped as a second-line group along with those who switched from mirabegron because they could not be statistically evaluated as a separate group. Baseline scores in the first- and second-line groups were comparable. Across all groups, vibegron 50 mg achieved significant improvements in each parameter. From early on, significant improvements in QOL were seen for all groups (Figure 2). Improvements in urinary incontinence are well known to result in improved QOL.21,22 Furthermore, the second-line group showed significant improvement in residual urine volume when comparing baseline and the 12-week endpoint. Interestingly, a significant improvement in residual urine volume was shown at the 12-week endpoint even when patients were limited to those who switched from mirabegron, accounting for 84% of the second-line group. To the best of our knowledge, this is the first report to confirm that switching from mirabegron to vibegron resulted in a significant reduction in residual urine volume. However, despite the significant reduction in residual urine volume, both baseline and 12-week residual urine volumes were within clinically normal ranges. The standard deviation was large and although the reduction in residual urine volume itself may not have been clinically meaningful, vibegron may have a lower risk of urinary retention. Mirabegron therapy for patients with OAB may be due not only to β3-adrenoceptor activation, but also to muscarinic receptor blockade.23 In addition, vibegron can bind to muscarinic receptors, as shown in the rat bladder, with a relatively higher affinity for the M2 subtype than for the M1 and M3 subtypes.24 Such findings suggest that mirabegron and vibegron might act through not only β3-adrenoreceptors, but also muscarinic receptors, in addition to direct or indirect suppression of C-fiber afferent activity to regulate bladder contractions. However, further verification and experimental evidence are required to confirm the exact mechanisms by which vibegron improves voiding efficiency. Clinical trial data have shown that vibegron does not affect the contractility of the detrusor muscle, which may lead to more efficient urination and less residual urine. Our findings suggest that vibegron is effective even in mirabegron-refractory patients and is a drug with a low risk of urinary retention.
No significant improvement in daytime frequency score was seen among patients ≥80 years old. On further investigation, male sex appeared to have a negative impact on improving daytime frequency scores (Table S1). A closer look at daytime frequency scores for men revealed that this parameter alone was already low at baseline. We therefore concluded that the effect of vibegron was not attenuated by male sex, but rather that this study included a high proportion of men who originally had less problems with daytime frequency. In addition, we performed evaluations according to the presence or absence of BPH drugs (Table S2). Comparisons between BPH drugs were not possible due to the small number of patients for analysis. No significant difference in residual urine volume was seen between patients with and without BPH drugs. No significant improvements other than OABSS total score and OAB-q SF were seen in the group without treatment for BPH. In other words, when using vibegron in BPH patients, use in combination with BPH drugs appears desirable.
Key limitations of this study were the non-placebo design and the small number of patients. As we cannot rule out the possibility that the results were impacted by some degree of placebo effect, future placebo-controlled studies with more patients are warranted.
Conclusion
Patients of all age groups showed significant improvements in OABSS and OAB-q SF, with the exception of daytime frequency scores. We also found that switching from other OAB drugs, including mirabegron, can be expected to reduce residual urine volume. This study demonstrated that vibegron 50 mg once daily for the treatment of OAB offered favorable effectiveness in a real-world clinical setting. No serious treatment-related adverse events were observed in this study, and safety appeared to be sufficiently maintained regardless of age or sex. In conclusion, vibegron 50 mg once daily appears effective in clinical settings, regardless of age. In addition, this study augments data for vibegron 50 mg once daily as a safe, effective treatment for the management of OAB patients.
Data Sharing Statement
The data that support the findings of this study are not publicly available due to their containing information that could compromise the privacy of research participants, but are available from the corresponding author (K.T.) upon reasonable request.
Statement of Ethics
All patients have provided written informed consent. The research protocol was approved by the ethics review board of Kochi Medical School (registration number: ERB-105795).
Acknowledgments
We wish to thank the patients, research facilities, and research staff who participated in this observational study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Abrams P, Cardozo L, Fall M, et al.; Standardisation Sub-committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21(2):167–178. doi:10.1002/nau.10052
2. Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J. 2010;21(1):5–26. doi:10.1007/s00192-009-0976-9
3. Fogaing C, Mossa AH, Campeau L. Are beta 3 adrenergic agonists now the preferred pharmacologic management of overactive bladder? Curr Urol Rep. 2020;21(12):49. doi:10.1007/s11934-020-01003-z
4. Sexton CC, Notte SM, Maroulis C, et al. Persistence and adherence in the treatment of overactive bladder syndrome with anticholinergic therapy: a systematic review of the literature. Int J Clin Pract. 2011;65(5):567–585. doi:10.1111/j.1742-1241.2010.02626.x
5. Veenboer PW, Bosch JL. Long-term adherence to antimuscarinic therapy in everyday practice: a systematic review. J Urol. 2014;191(4):1003–1008. doi:10.1016/j.juro.2013.10.046
6. Chapple CR, Nazir J, Hakimi Z, et al. Persistence and adherence with mirabegron versus antimuscarinic agents in patients with overactive bladder: a retrospective observational study in UK clinical practice. Eur Urol. 2017;72(3):389–399. doi:10.1016/j.eururo.2017.01.037
7. Yeowell G, Smith P, Nazir J, Hakimi Z, Siddiqui E, Fatoye F. Real-world persistence and adherence to oral antimuscarinics and mirabegron in patients with overactive bladder (OAB): a systematic literature review. BMJ Open. 2018;8(11):e021889. doi:10.1136/bmjopen-2018-021889
8. Kelleher C, Hakimi Z, Zur R, et al. Efficacy and tolerability of mirabegron compared with antimuscarinic monotherapy or combination therapies for overactive bladder: a systematic review and network meta-analysis. Eur Urol. 2018;74(3):324–333. doi:10.1016/j.eururo.2018.03.020
9. Bragg R, Hebel D, Vouri SM, Pitlick JM. Mirabegron: a Beta-3 agonist for overactive bladder. Consult Pharm. 2014;29(12):823–837. doi:10.4140/TCP.n.2014.823
10. Keam SJ. Vibegron: first global approval. Drugs. 2018;78(17):1835–1839. doi:10.1007/s40265-018-1006-3
11. Edmondson SD, Zhu C, Kar NF, et al. Discovery of vibegron: a potent and selective β3 adrenergic receptor agonist for the treatment of overactive bladder. J Med Chem. 2016;59(2):609–623. doi:10.1021/acs.jmedchem.5b01372
12. Homma Y, Kakizaki H, Gotoh M, et al. Epidemiologic survey on lower urinary tract symptoms in Japan (written in Japanese). J Neurogenic Bladder Soc. 2003;14:266–277.
13. Varano S, Staskin D, Frankel J, Shortino D, Jankowich R, Mudd PN. Efficacy and safety of once-daily vibegron for treatment of overactive bladder in patients aged ≥65 and ≥75 years: subpopulation analysis from the EMPOWUR randomized, international, Phase III study. Drugs Aging. 2021;38(2):137–146. doi:10.1007/s40266-020-00829-z
14. Coyne KS, Thompson CL, Lai JS, Sexton CC. An overactive bladder symptom and health-related quality of life short-form: validation of the OAB-q SF. Neurourol Urodyn. 2015;34(3):255–263. doi:10.1002/nau.22559
15. Homma Y, Gotoh M. Development and linguistic validation of the Japanese version of the overactive bladder questionnaire (OAB-q) (written in Japanese). J Neurogenic Bladder Soc. 2006;17:241–249.
16. Homma Y, Gotoh M, Yokoyama O, et al. Psychometric properties of the Japanese version of the overactive bladder questionnaire (OAB-q) (written in Japanese). J Neurogenic Bladder Soc. 2006;17:250–256.
17. Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. doi:10.1038/bmt.2012.244
18. Staskin D, Frankel J, Varano S, Shortino D, Jankowich R, Mudd PN. International Phase III, randomized, double-blind, placebo and active controlled study to evaluate the safety and efficacy of vibegron in patients with symptoms of overactive bladder: EMPOWUR. J Urol. 2020;204(2):316–324. doi:10.1097/JU.0000000000000807
19. Akiyama H. Aging well: an update. Nutr Rev. 2020;78(12 Suppl 2):3–9. doi:10.1093/nutrit/nuaa084
20. Coyne KS, Sexton CC, Bell JA, et al. The prevalence of lower urinary tract symptoms (LUTS) and overactive bladder (OAB) by racial/ethnic group and age: results from OAB-POLL. Neurourol Urodyn. 2013;32(3):230–237. doi:10.1002/nau.22295
21. Tang DH, Colayco DC, Khalaf KM, et al. Impact of urinary incontinence on healthcare resource utilization, health-related quality of life and productivity in patients with overactive bladder. BJU Int. 2014;113(3):484–491. doi:10.1111/bju.12505
22. Tapia CI, Khalaf K, Berenson K, Globe D, Chancellor M, Carr LK. Health-related quality of life and economic impact of urinary incontinence due to detrusor overactivity associated with a neurologic condition: a systematic review. Health Qual Life Outcomes. 2013;31(11):13. doi:10.1186/1477-7525-11-13
23. Yamada S, Chimoto J, Shiho M, et al. Possible Involvement of Muscarinic Receptor Blockade in Mirabegron Therapy for Patients with Overactive Bladder. J Pharmacol Exp Ther. 2021;377(2):201–206. doi:10.1124/jpet.120.000301.
24. Yamada S, Chimoto J, Shiho M, et al. Muscarinic receptor binding activity in rat tissues by vibegron and prediction of its receptor occupancy levels in the human bladder. Int J Urol. 2021;28(12):1298–1303. doi:10.1111/iju.14696
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.