Back to Journals » International Journal of General Medicine » Volume 19
miR-1287-5p as a Biomarker for Predicting Lymph Node Metastasis in Gastric Cancer Patients
Authors Zhang J, Zhang M, Zhao W, Wu H, Wang R
Received 25 March 2026
Accepted for publication 31 May 2026
Published 9 June 2026 Volume 2026:19 609960
DOI https://doi.org/10.2147/IJGM.S609960
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ching-Hsien Chen
Jinjia Zhang,1 Min Zhang,1 Wenwen Zhao,1 Huadong Wu,2 Rongying Wang1
1Department of General Practice, The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 2Department of Gastrointestinal Surgery, The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China
Correspondence: Rongying Wang, Department of General Practice, The Second Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China, Tel +86 0311 66002805, Fax +86 0311 66002805, Email [email protected]
Background: The purpose of this study was to predict lymph node metastasis (LNM) in gastric cancer (GC) patients by constructing a nomogram.
Methods: A total of 416 GC patients from the TCGA database and the Second Hospital of Hebei Medical University were included. The TCGA cohort was used to develop the prediction model. Logistic regression was used to determine risk factors associated with LNM in GC patients. A nomogram model was then developed. Model performance was evaluated using the area under the curve (AUC) and calibration curves.
Results: In the multivariate analysis, the variables independently associated with LNM in GC patients were race (OR=1.820, 95% CI 1.060– 3.125), histologic grade (OR=0.587, 95% CI 0.354– 0.974), pathologic stage T3 or higher (OR=2.081, 95% CI 1.188– 3.647) and miR-1287-5p (OR=0.748, 95% CI 0.565– 0.992). A nomogram comprising the above four independent factors was constructed to calculate the possibility of LNM. The C-index values were 0.847 (95% CI 0.777– 0.917) and 0.755 (95% CI 0.565– 0.944) in the training and supportive cohorts, respectively.
Conclusion: We identified miR-1287-5p as a novel predictor of LNM in GC patients. We established a nomogram model for predicting LNM in GC patients, and evaluated its performance in a supportive cohort.
Keywords: miR-1287-5p, gastric cancer, lymph node metastasis, nomogram
Introduction
GC is the fifth most common cancer worldwide and ranks fourth in cancer-related mortality, according to Global Cancer Statistics 2020.1 China has the largest number of GC cases and deaths in the world.1 At present, the mortality rate of GC patients remains high, with a 5-year survival rate of about 30%, mainly related to the high recurrence and metastasis rates of GC.2
Following GC resection, LNM is one of the most important prognostic factors.3,4 Preoperative assessment of LNM currently relies mainly on MRI and CT, neither of which has high sensitivity or specificity for detecting LNM.5,6 Therefore, accurate prediction of LNM remains a clinical challenge. For gastric cancer patients, particularly those at high risk of LNM, accurate postoperative assessment of lymph node status is important for planning adjuvant therapy. Our nomogram, based on pathologic variables from surgical specimens, is designed for postoperative risk stratification.
MiRNAs are tiny noncoding RNAs that are around 20–25 nucleotides long. They bind to the 3’untranslated regions (3’UTRs) of targeted mRNAs to cause translational repression and perform biological functions in cancer.7–9 Accumulating evidence demonstrates that miR-1287-5p was vital regulators in the occurrence of colorectal cancer,pancreatic cancer, lung cancer, breast cancer, thyroid cancer and other cancers.10–14 For instance, by targeting SLC7A11, miR-1287-5p contributes to colorectal cancer cell growth, invasion, and ferroptosis suppression.10 miR-1287-5p had been found to suppress pancreatic carcinoma malignant properties by LAMTOR3 signalling.11 In non-small cell lung cancer cells,miR-1287-5p/PFN2 signaling reduced invasion and proliferation.12 Nevertheless, it is still unknown how miR-1287-5p and GC are related.
Thus, using data from the TCGA database, this study systematically examined 326 cases of gastric adenocarcinoma, focusing on miR-1287-5p and clinical features. To improve treatment precision and LNM assessment in GC patients, we aimed to construct a nomogram for predicting LNM in GC.
Materials and Methods
TCGA Data Gathering and Preparation
We downloaded the quantitative miRNA expression data of transcripts of GC and created matrix files after logging in to https://portal.gdc.cancer.gov/. The requirements for inclusion were: (1) Gastric adenocarcinoma was the histological diagnosis; (2) Full demographic information, including gender, age, race, histologic grade, and TNM stage, was required. These patients from TCGA were used as the training cohort for the nomogram.
Differentially Expressed miRNAs (DEMs) Identification
The edgeR package of the R software was used to calculate the DEMs between the GC and adjacent non-tumor tissues. The thresholds for the screening criteria were established at p < 0.05 and |log2(fold change)| > 1. To visualize DEMs, a volcano plot was used. After being normalized by edgeR, the raw count was then transformed into log2values (normalized values) for use in further analysis.
Clinical Samples
A total of 90 GC patients who had surgery at the Second Hospital of Hebei Medical University were examined, and their paired tumor tissues and adjacent normal tissues (three to four centimeters away from the tumor tissue) were collected between August 2024 and November 2024. Age, gender, race, histologic grade, and TNM stage were among the clinical data collected, along with written informed consent from each participant. Histologic grade was determined from the postoperative pathological report of the surgical specimen. The ethics committee of the Second Hospital of Hebei Medical University granted ethical approval for this investigation. These patients served as the supportive cohort.
Real-Time Quantitative Reverse Transcription Polymerase Chain Reaction (RT-qPCR)
RT-qPCR was performed to detect miR-1287-5p expression in 90 paired tissue samples. Total RNA was extracted using TRIzol reagent (Tiangen, Beijing, China), and RNA quality and concentration were measured with a Nanodrop 2000 (Thermo Fisher Scientific, USA). Reverse transcription was carried out using the All-in-One™ miRNA qRT-PCR Detection Kit 2.0 (GeneCopoeia, Rockville, MD, USA). qPCR was performed on an Applied Biosystems 7500 Real Time PCR System (Thermo Fisher Scientific, Waltham, MA, USA) using SYBR Premix Ex Taq II (Takara). U6 served as an internal control. Relative expression of miR-1287-5p was calculated using the 2−ΔΔCt method. Primer sequences are listed below.
miR-1287-5p-F: 5′-TGCTGGATCAGTGGTTCGAGTC-3′;
miR-1287-5p-R: 5′-TGGTGTCGTGGAGTCG-3′;
U6-F: 5′-CAAATTCGTGAAGCGTT-3′;
U6-R: 5′-TCACTGGTGTCGTGG-3′.
miR-1287-5p Target Genes Prediction and Functions Analysis
The possible target genes of miR-1287-5p were predicted using the online databases TargetScan (https://www.targetscan.org/), mirDIP (https://ophid.utoronto.ca/mirDIP/index.jsp), and miRWalk (https://mirwalk.umm.uni-heidelberg.de/). The miR-1287-5p target genes were those that the three tools predicted. To further understand the underlying molecular mechanism of miR-1287-5p, GO functional annotations and KEGG pathway enrichment of the consensus genes were constructed using DAVID (https://david.ncifcrf.gov/) with a demarcation threshold of P < 0.05.15 Key KEGG pathways and GO function annotations were defined as those pathways or annotations with the highest count value or the lowest P-value. Three components make up GO function annotations: biological process (BP), cellular component (CC) and molecular function (MF).
Statistical Analysis
Statistical analyses were performed using R software (version 4.1.0) and SPSS version 26.0 (IBM Corp., Armonk, NY, USA). The mean ± standard deviation was used to express continuous variables. Percentages were used to represent categorical variables. To examine the risk factors for LNM in GC patients, univariate and multivariate logistic regression analyses were performed. A nomogram was then constructed based on the results of the multivariate logistic regression analysis using the training cohort. For miR-1287-5p expression, a median split was performed separately within each cohort. Patients with expression above the median were classified as the “high” group, and those below as the “low” group. Thus, miR-1287-5p was entered into the logistic regression model as a binary categorical variable. The supportive cohort was used to evaluate the model’s performance. The same logistic regression coefficients derived from the training cohort were applied to the supportive cohort’s variables. The predicted probability of LNM was then computed for each patient, and the area under the curve (AUC) and calibration curve were generated based on these predicted probabilities versus observed LNM status.Statistical significance was defined as p < 0.05.
Results
DEMs Between GC and Normal Samples Based on TCGA
We collected miRNA information from a TCGA data set, including 436 tumor tissues and 41 normal tissues. 242 DEMs, comprising 178 upregulated and 64 downregulated miRNAs, were found between GC and normal control samples based on the selected criteria. Volcano plots and heat maps were created for these 242 DEMs, as shown in Figures 1a and b.
 |
Figure 1 Differentially expressed miRNAs in GC. The DEMs in GC and adjacent non-tumor tissues were shown in the volcano plot (a) and heatmap (b) based on TCGA database. The red parts represented the upregulated genes; the green parts represented the downregulated genes, and the black parts represented the genes without significant difference. FDR < 0.05, log2 | FC | >1 and P < 0.05. |
Expression of miR-1287-5p in GC From TCGA and Clinical Samples
From the TCGA database, 436 GC patients and 41 normal cases were gathered. In the GC group, the relevant expression value of miR-1287-5p (log2x) by microRNA-Seq was 4.20 ± 0.90, while in the normal group, it was 4.79 ± 0.69. miR-1287-5p expression was significantly lower in the GC group when compared to the normal group (Figure 2a). 90 GC cases and adjacent non-cancer cases were gathered from the Second Hospital of Hebei Medical University. The relevant expression value of miR-1287-5p by RT-qPCR in the GC tissues was 0.63 ± 0.12 and that of the related adjacent tissues was 1.01 ± 0.15. The results demonstrated that, in contrast to the related adjacent tissues, miR-1287-5p expression was significantly lower in the GC tumor tissues (Figure 2b).
 |
Figure 2 miR-1287-5p expression is decreased in TCGA samples and clinical GC samples. (a) miR-1287-5p expression is decreased in TCGA GC samples by microRNA-Seq. (b) miR-1287-5p expression is decreased in clinical GC samples by RT-qPCR. (***P<0.001). |
Baseline Data of GC Population
326 patients from the TCGA database and 90 patients from the Second Hospital of Hebei Medical University were included in this study based on the inclusion and exclusion criteria. Among the patients in the TCGA database, there were 436 patients with the diagnosis of GC. We excluded patients with incomplete clinical and pathological data. After screening, 326 patients remained. The median age was 64.71 years, with 205 (62.9%) males and 121 (37.1%) females. For patients in our hospital, the median age was 65.20 years, with 60 (66.7%) males and 30 (33.3%) females. Table 1 provided a summary of the clinicopathological features. Furthermore, we specifically analyzed the expression level of miR-1287-5p in relation to lymph node metastasis status in the supportive cohort. The expression level of miR-1287-5p was significantly lower in patients with lymph node metastasis compared to those without (p < 0.05) (Table 2).
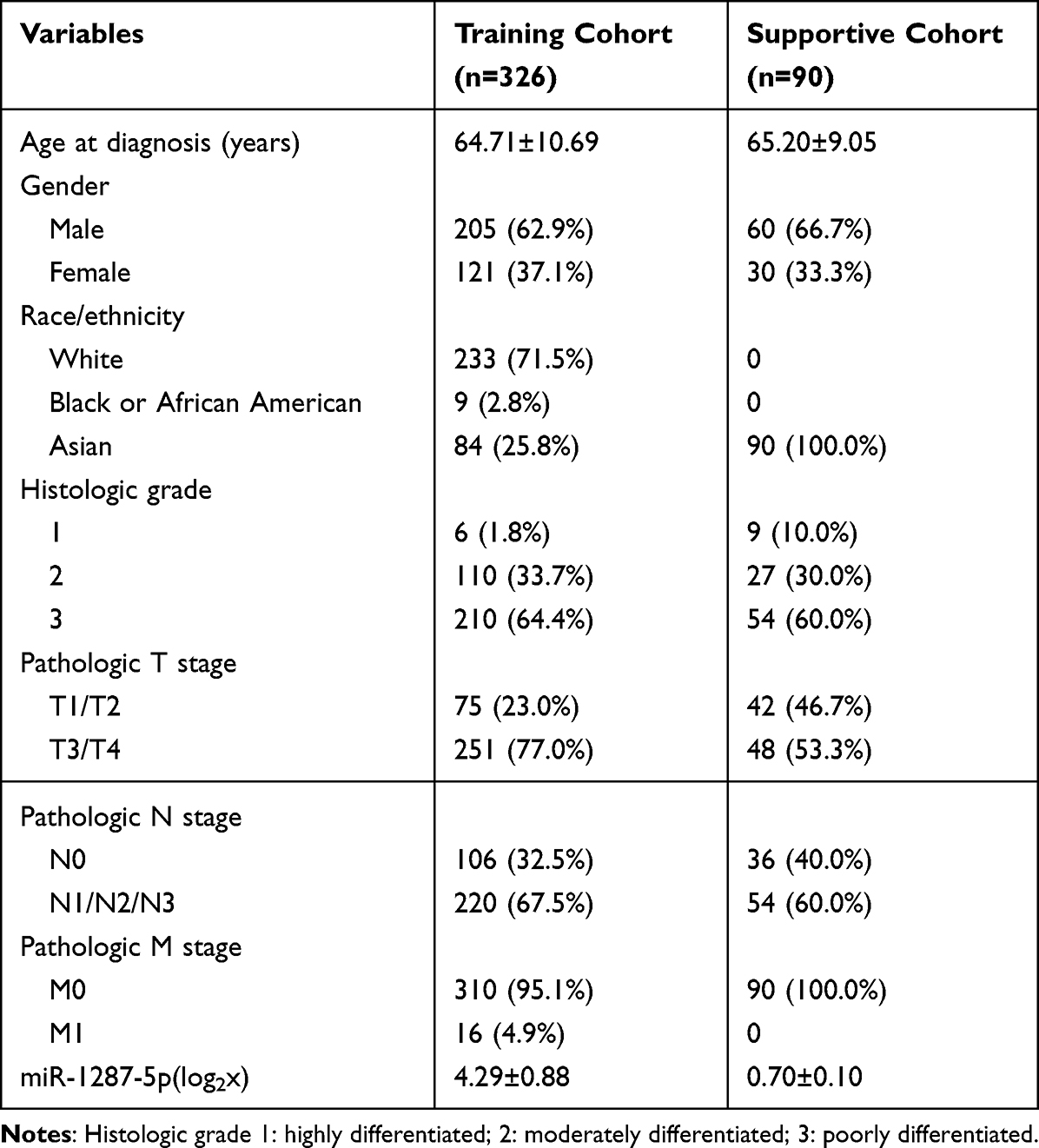 |
Table 1 Summary of Clinicopathological Characteristics of GC Patients in the Training and Supportive Cohorts. (n=416) |
 |
Table 2 Association of miR-1287-5p Expression with Lymph Node Metastasis in the Supportive Cohort |
Univariate and Multivariate Analysis of Risk Factors for LNM in GC Patients in the Training Cohort
Based on the presence or absence of LNM, we separated GC patients into two groups. There were 220 GC patients with LNM. The univariate analyses were performed, showing that race, histologic grade, pathologic T stage and miR-1287-5p were linked to LNM (Table 3). In multivariate analysis, factors that had a P value of less than 0.05 in univariate analysis were included. Results showed that the variables independently associated with LNM were race (OR=1.820, 95% CI 1.060–3.125), histologic grade (OR=0.587, 95% CI 0.354–0.974), pathologic stage T3 or higher (OR=2.081, 95% CI 1.188–3.647) and miR-1287-5p (OR=0.748, 95% CI 0.565–0.992) (Table 3).
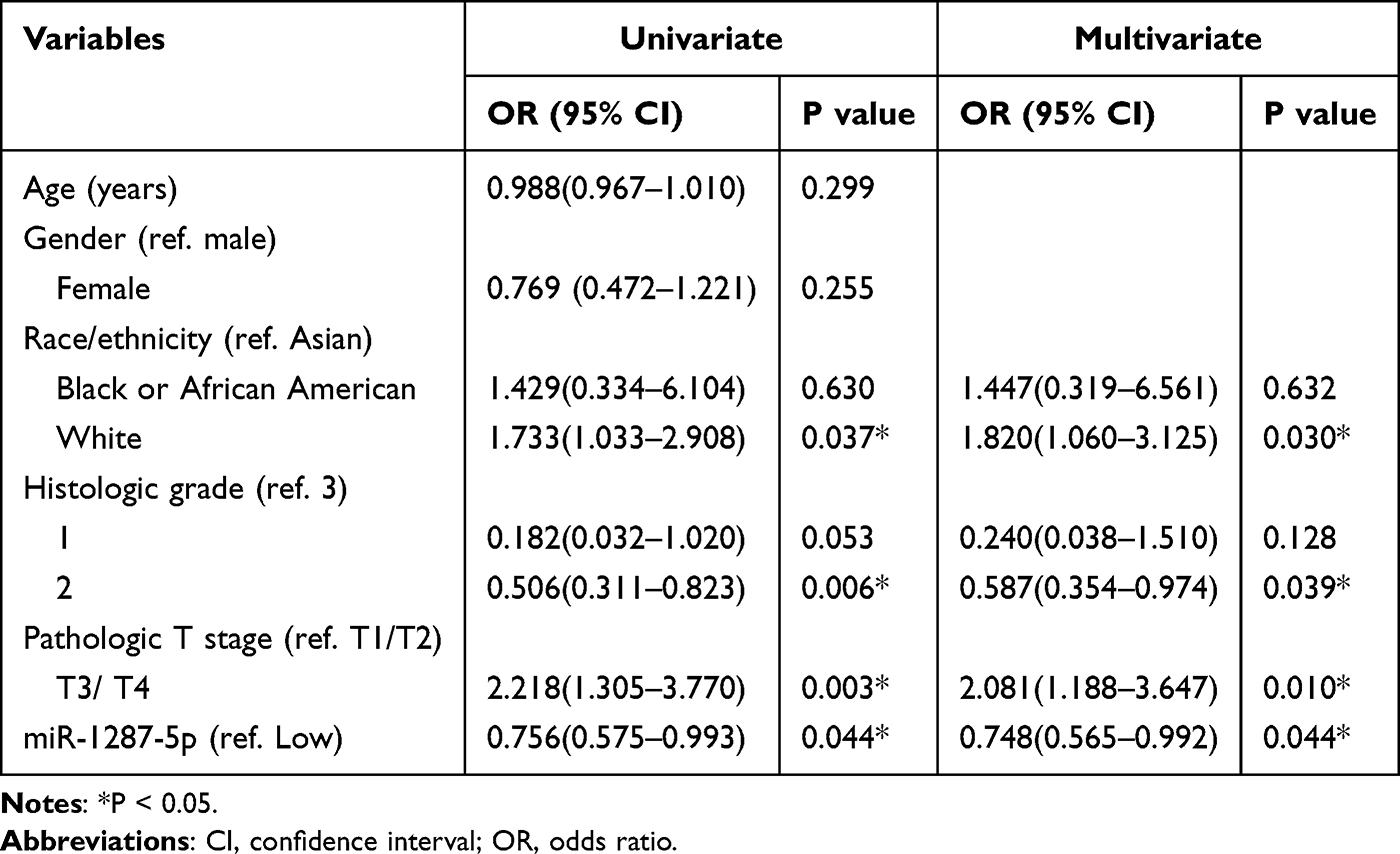 |
Table 3 Univariate and Multivariate Analysis of Risk Factors for LNM in 326 GC Patients |
Nomogram Model for Predicting LNM in GC Patients
The nomogram model was established using the important predictors in the multivariate logistic analysis of training set (Figure 3). One score for each risk factor could be obtained by applying the rule above the nomogram that corresponds to it. Each score was added together, and the sum of the scores indicated the likelihood of LNM in this patient.
 |
Figure 3 Nomogram for predicting LNM in GC patients. Grade,race,T stage, hsa-miR-1287-5p are the variables of the prediction model. |
Evaluation of Nomogram Performance
A ROC curve was drawn for the training model (AUC 0.847, 95% CI 0.777–0.917, Figure 4a). For the supportive cohort, the same logistic regression coefficients from the training model were applied to calculate predicted LNM probabilities. The resulting AUC was 0.755 (95% CI 0.565–0.944, Figure 4b), indicating acceptable discrimination. The Hosmer-Lemeshow test (χ2=11.099, P=0.196) and the calibration curve (Figure 4c and d) showed acceptable agreement between predicted and observed LNM. In the supportive cohort, the prediction accuracy was slightly lower than in the training cohort, possibly related to the fact that the supportive cohort had a smaller sample size and only included Asian patients but not white and black patients.
 |
Figure 4 The ROC curves and calibration curves of the nomogram model. (a) indicates the ROC curve of the training set, (b) indicates the ROC curve of the supportive set, (c) represents the calibration curve of the training set, and (d) represents the calibration curve of the supportive set. |
Molecular Mechanism of miR-1287-5p
717 target genes of miR-1287-5p were found using the prediction results in conjunction with TargetScan, mirDIP, and miRWalk. A portion of the KEGG pathway and GO enrichment analysis results for 717 target genes by DAVID (https://david.ncifcrf.gov/) were displayed in Figure 5. The dot plot (Figure 5a–c) showed the GO enrichment findings for the top 20 terms, including biological process (BP), cellular component (CC), and molecular function (MF). The three most significant of the 196 items in GO-BP were actin cytoskeleton organization, positive regulation of transcription by RNA polymerase II and positive regulation of canonical Wnt signaling pathway. Among the 67 items in GO-CC, cytosol, nucleoplasm, and glutamatergic synapses were the most crucial. The target genes in GO-MF, which had 60 items, were primarily involved in protein binding, guanyl-nucleotide exchange factor activity and virus receptor activity. Findings from the KEGG pathways analysis were primarily enriched in focal adhesion, proteoglycans in cancer and PI3K-Akt signaling pathway (Figure 5d and Table 4).
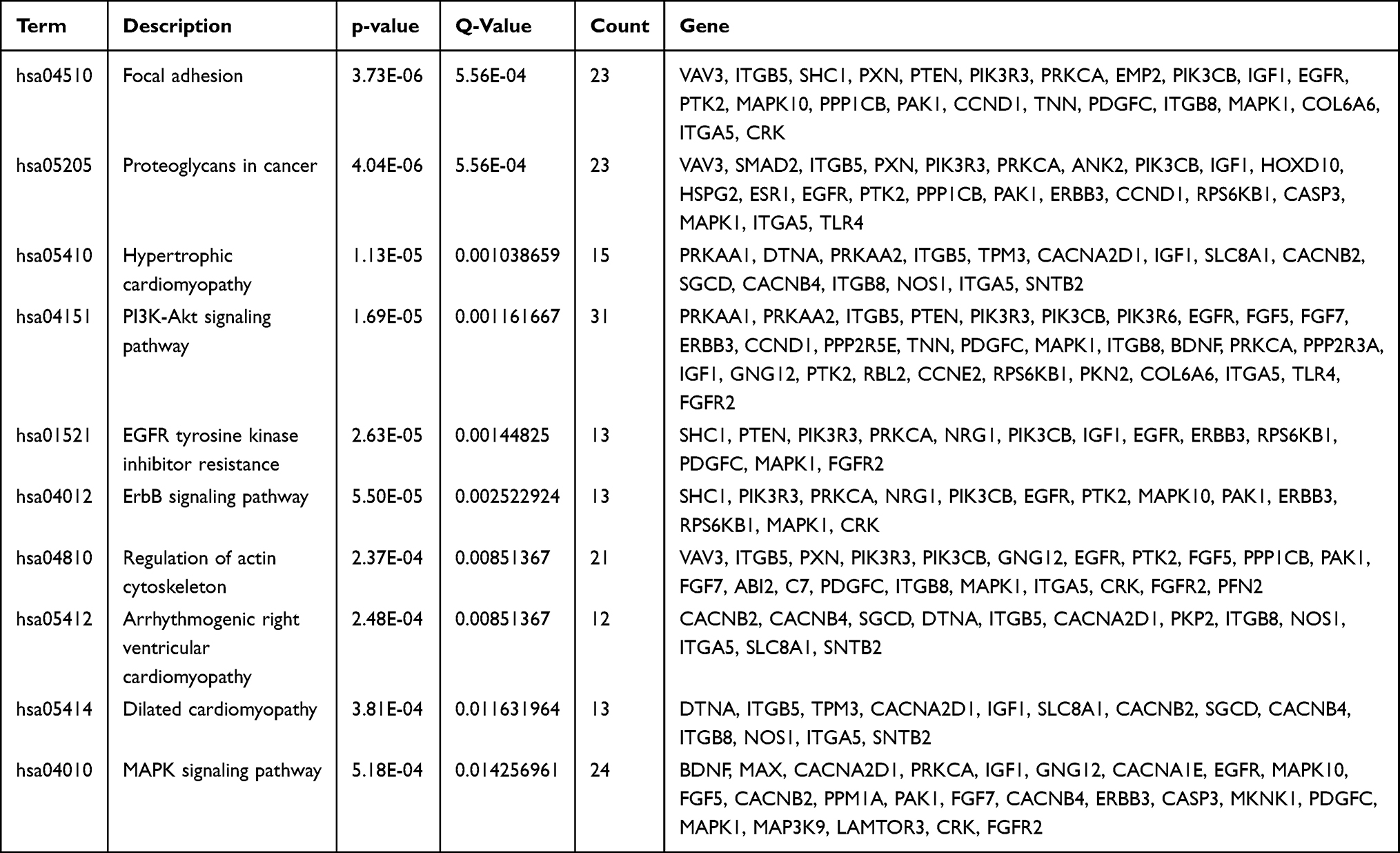 |
Table 4 KEGG Signaling Pathways of the Target Genes |
 |
Figure 5 Functional enrichment analysis of target genes. (a) BP; (b) CC; (c) MF; (d) KEGG signaling pathways. |
Discussion
In this study, we developed a nomogram to predict lymph node metastasis (LNM) in gastric cancer (GC) patients using four independent risk factors: race, histologic grade, pathologic T stage, and miR-1287-5p expression. The model showed good discrimination in the training cohort (AUC 0.847) and was evaluated in an supportive cohort (AUC 0.755). The lower AUC in the supportive cohort may reflect its smaller sample size and homogeneous racial composition, underscoring the need for multi-ethnic evaluation.
Consistent with previous research, White GC patients have a significantly higher LNM rate than Asian patients.16,17 The underlying etiologies remain poorly defined, but possible explanations include less aggressive tumor biology in Asians,18 differences in disease location, environmental factors, tumor histological type, and Helicobacter pylori status.19–23 Additionally, effective lymph node assessment requires close cooperation between pathologists and surgeons.24 The number of lymph nodes analyzed can be influenced by the extent of disease, surgical technique of lymph node dissection, and specimen preparation. Notably, in the United States, pathology technicians often remove lymph nodes during formalin fixation, whereas Asian surgeons typically do so immediately after gastrectomy before fixation. Other ethnic-related factors, such as body mass index, may also affect the adequacy of lymphadenectomy.25
The presence of LNM in GC is strongly correlated with tumor invasion depth, which generally reflects tumor progression from the mucosal layer.26,27 Our findings align with this, confirming pathologic T stage as a significant clinical predictor of LNM. The role of histologic grade remains controversial. Some researchers have found no significant relationship between differentiation type and LNM;28,29 however, most studies demonstrate that poorly differentiated GC has a higher incidence of LNM.30,31 This discrepancy may be because some studies focus on specific GC stages or subtypes, such as undifferentiated-type GC28 or signet ring cell-type intramucosal GC.29
We identified 717 putative target genes of miR-1287-5p using three prediction platforms.Then we conducted a bioinformatics analysis using the KEGG pathway and GO enrichment. GO enrichment analysis revealed significant enrichment in “actin cytoskeleton organization” and “positive regulation of transcription by RNA polymerase II”. The former suggests that miR-1287-5p may regulate cell migration and invasion, key processes in metastasis. KEGG pathway analysis highlighted “focal adhesion”, “proteoglycans in cancer”, and the “PI3K-Akt signaling pathway” as the top enriched pathways. Notably, the PI3K-Akt pathway is frequently dysregulated in gastric cancer and is known to promote cell survival, proliferation, and metastasis. The enrichment of “focal adhesion” further supports a role for miR-1287-5p in tumor cell-extracellular matrix interactions, which are critical for lymph node dissemination. These bioinformatic findings provide a mechanistic basis for the observed association between low miR-1287-5p expression and increased LNM risk. Future functional studies, such as luciferase reporter assays and in vitro invasion assays, are needed to validate these predicted targets.
In the future, we will develop a web-based or mobile application calculator that would integrate the nomogram’s algorithm. This would allow a clinician to input the patient’s data (race, histologic grade, T stage, miR-1287-5p expression) and instantly receive the predicted probability of LNM, eliminating even the minimal step of manually plotting points on a nomogram. This addition frames the nomogram as a robust foundation for future digital health tools.
We acknowledge several limitations. Exclusion of patients with incomplete data may introduce selection bias. Factors such as tumor size, ulceration, vascular invasion, and neural invasion were not included due to missing records. The supportive cohort was collected over a short period at a single institution, raising concerns about representativeness; multi-center and multi-ethnic validation is needed. Additionally, our nomogram relies on pathologic variables from surgical specimens and is therefore intended for postoperative risk stratification. Future models for pre-treatment prediction should incorporate preoperative variables such as endoscopic ultrasound findings, biopsy-based grade, or circulating miRNAs. Finally, the association between miR-1287-5p and long-term prognosis was not evaluated, which will be a focus of subsequent studies.
Conclusions
This study identifies miR-1287-5p as a novel predictor of lymph node metastasis in gastric cancer. A nomogram incorporating race, histologic grade, pathologic T stage, and miR-1287-5p expression was successfully constructed and tested in a supportive cohort for consistency. This nomogram may serve as a practical tool for postoperative risk assessment and individualized treatment planning.
Data Sharing Statement
The data used during the present study are available from the corresponding author on reasonable request.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. This study was approved by the institutional review boards of The Second Hospital of Hebei Medical University (No.2024-R445). All the experiments in this study were carried out in accordance with relevant guidelines and regulation for human study.
Informed consent: Written informed consent was obtained from all participants or their clients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Medical Science Research Project of Hebei (No.20250066).
Disclosure
The authors declared that they have no conflicts of interest for this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–11. doi:10.3322/caac.21660
2. Banks M, Graham D, Jansen M, et al. British Society of Gastroenterology guidelines on the diagnosis and management of patients at risk of gastric adenocarcinoma. Gut. 2019;68(9):1545–1575. doi:10.1136/gutjnl-2018-318126
3. Imamura T, Komatsu S, Ichikawa D, et al. Early signet ring cell carcinoma of the stomach is related to favorable prognosis and low incidence of lymph node metastasis. J Surg Oncol. 2016;114:607–612. doi:10.1002/jso.24377
4. Zu H, Wang H, Li C, et al. Clinicopathologic characteristics and prognostic value of various histological types in advanced gastric cancer. Int J Clin Exp Pathol. 2014;7:5692–5700.
5. Hallinan JT, Venkatesh SK. Gastric carcinoma: imaging diagnosis, staging and assessment of treatment response. Cancer Imaging. 2013;13:212–227. doi:10.1102/1470-7330.2013.0023
6. Hasbahceci M, Akcakaya A, Memmi N, et al. Diffusion MRI on lymph node staging of gastric adenocarcinoma. Quant Imaging Med Surg. 2015;5:392–400. doi:10.3978/j.issn.2223-4292.2015.03.06
7. Lara-Barba E, Araya MJ, Hill CN, et al. Role of microRNA shuttled in small extracellular vesicles derived from mesenchymal stem/stromal cells for osteoarticular disease treatment. Frontiers in Immunology. 2021;12:768771. doi:10.3389/fimmu.2021.768771
8. Di Leva G, Garofalo M, Croce CM. MicroRNAs in cancer. Annu Rev Pathol. 2014;9:287–314. doi:10.1146/annurev-pathol-012513-104715
9. Peng Y, Croce CM. The role of microRNAs in human cancer. Signal Transduct Target Ther. 2016;1:15004. doi:10.1038/sigtrans.2015.4
10. Wang J, Zhang Z, Zhuang J, et al. CircCOL5A1 is involved in proliferation, invasion, and inhibition of ferroptosis of colorectal cancer cells via miR-1287-5p/SLC7A11. J Biochem Mol Toxicol. 2024;38(8):e23772. doi:10.1002/jbt.23772
11. Zhang X, Xue C, Cui X, et al. Circ_0075829 facilitates the progression of pancreatic carcinoma by sponging miR-1287-5p and activating LAMTOR3 signalling. J Cell Mol Med. 2020;24(24):14596–14607. doi:10.1111/jcmm.16089
12. Jin M, Yuan T, Tian K, et al. Oncogenic circ-SLC16A1 promotes progression of non-small cell lung cancer via regulation of the miR-1287-5p/profilin 2 axis. Cell Mol Biol Lett. 2024;29(1):43. doi:10.1186/s11658-024-00549-x
13. Schwarzenbacher D, Klec C, Pasculli B, et al. MiR-1287-5p inhibits triple negative breast cancer growth by interaction with phosphoinositide 3-kinase CB, thereby sensitizing cells for PI3Kinase inhibitors. Breast Cancer Res. 2019;21(1):20. doi:10.1186/s13058-019-1104-5
14. Sun H, Xu F, You D. CircPI4KA overexpression enhances carcinogenesis and glycolysis metabolism in papillary thyroid carcinoma by causing the miR-1287-5p-mediated NRP2 expression elevation. Horm Metab Res. 2023;55(10):701–710. doi:10.1055/a-2153-7428
15. Huang DW, Sherman BT, Lempicki RA. Systematic and integrative analysis of large gene lists using DAVID bioinformatics resources. Nat Protoc. 2009;4:44–57. doi:10.1038/nprot.2008.211
16. Ikoma N, Blum M, Chiang YJ, et al. Race is a risk for lymph node metastasis in patients with gastric cancer. Ann Surg Oncol. 2017;24(4):960–965. doi:10.1245/s10434-016-5645-x
17. Fukuhara S, Yabe M, Montgomery MM, et al. Race/Ethnicity is predictive of lymph node status in patients with early gastric cancer. J Gastrointest Surg. 2014;18:1744–1751. doi:10.1007/s11605-014-2590-5
18. Strong VE, Song KY, Park CH, et al. Comparison of gastric cancer survival following R0 resection in the United States and Korea using an internationally validated nomogram. Ann Surg. 2010;251(4):640–646. doi:10.1097/SLA.0b013e3181d3d29b
19. Schlemper RJ, Itabashi M, Kato Y, et al. Differences in diagnostic criteria for gastric carcinoma between Japanese and western pathologists. Lancet. 1997;349(9067):1725–1729. doi:10.1016/S0140-6736(96)12249-2
20. Theuer CP. Asian gastric cancer patients at a southern California comprehensive cancer center are diagnosed with less advanced disease and have superior stage-stratified survival. Am Surg. 2000;66(9):821–826. doi:10.1002/1097-0142(20001101)89:9<1883::aid-cncr3>3.3.co;2-8
21. Schwarz RE, Zagala-Nevarez K. Ethnic survival differences after gastrectomy for gastric cancer are better explained by factors specific for disease location and individual patient comorbidity. Eur J Surg Oncol. 2002;28:214–219. doi:10.1053/ejso.2001.1234
22. Bollschweiler E, Boettcher K, Hoelscher AH, et al. Is the prognosis for Japanese and German patients with gastric cancer really different? Cancer. 1993;71:2918–2925. doi:10.1002/1097-0142(19930515)71:10<2918::AID-CNCR2820711006>3.0.CO;2-V
23. Yao JC, Schnirer II, Reddy S, et al. Effects of sex and racial/ethnic group on the pattern of gastric cancer localization. Gastric Cancer. 2002;5:208–212. doi:10.1002/1097-0142(19930515)71:10<2918::aid-cncr2820711006>3.0.co;2-v
24. Smith AJ, Law CH, Khalifa MA, et al. Multimodal CME for surgeons and pathologists improves colon cancer staging. J Cancer Educ. 2003;18:81–86. doi:10.1207/S15430154JCE1802_09
25. Coburn NG, Swallow CJ, Kiss A, et al. Significant regional variation in adequacy of lymph node assessment and survival in gastric cancer. Cancer. 2006;107(9):2143–2151. doi:10.1002/cncr.22229
26. Zhang M, Ding C, Xu L, et al. A nomogram to predict risk of lymph node metastasis in early gastric cancer. Sci Rep. 2021;11(1):22873. doi:10.1038/s41598-021-02305-z
27. Bausys R, Bausys A, Vysniauskaite I, et al. Risk factors for lymph node metastasis in early gastric cancer patients: report from Eastern Europe country-Lithuania. BMC Surg. 2017;17(1):108. doi:10.1186/s12893-017-0304-0
28. Asakawa Y, Ohtaka M, Maekawa S, et al. Stratifying the risk of lymph node metastasis in undifferentiated-type early gastric cancer. World J Gastroenterol. 2015;21:2683–2692. doi:10.3748/wjg.v21.i9.2683
29. Pyo JH, Shin CM, Lee H, et al. A risk-prediction model based on lymph-node metastasis for incorporation into a treatment algorithm for signet ring cell-type intramucosal gastric cancer. PLoS One. 2016;11(5):e0156207. doi:10.1097/SLA.0000000000001602
30. Ding B, Luo P, Yong J. Model based on preoperative clinical characteristics to predict lymph node metastasis in patients with gastric cancer. Front Surg. 2022;9:976743. doi:10.3389/fsurg.2022.976743
31. Huang C, Hu C, Zhu J, et al. Establishment of decision rules and risk assessment model for preoperative prediction of lymph node metastasis in gastric cancer. Front Oncol. 2020;10:1638. doi:10.3389/fonc.2020.01638
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Integrating Machine Learning and the SHapley Additive exPlanations (SHAP) Framework to Predict Lymph Node Metastasis in Gastric Cancer Patients Based on Inflammation Indices and Peripheral Lymphocyte Subpopulations
Zhu Z, Wang C, Shi L, Li M, Li J, Liang S, Yin Z, Xue Y
Journal of Inflammation Research 2024, 17:9551-9566
Published Date: 23 November 2024
Relationship Between MIC-1, VEGF, and TGF-β1 and Clinicopathologic Stage and Lymph Node Metastasis in Gastric Cancer
Sheng J, Wang J, Ma T, He P
International Journal of General Medicine 2025, 18:955-965
Published Date: 21 February 2025