Back to Journals » Journal of Pain Research » Volume 19
Minimally Invasive Interventions for Cervicogenic Headache: A Systematic Review of Targeted Anatomical Approaches and Clinical Outcomes
Authors Jin X, Zhang Q, Lin J, Sun Y ![]() , Dong Z, Jin W
, Dong Z, Jin W ![]()
Received 24 June 2025
Accepted for publication 26 December 2025
Published 8 January 2026 Volume 2026:19 549239
DOI https://doi.org/10.2147/JPR.S549239
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rune Häckert Christensen
Xing Jin,1 Qingyu Zhang,1 Jia Lin,2 Ye Sun,3 Zhiting Dong,4 Wenzhe Jin1
1Department of Pain, Yanbian University Hospital, Yanji, Jilin, 133000, People’s Republic of China; 2Department of Internal Medicine 1, No. 965 Hospital, Jilin, Jilin, 132000, People’s Republic of China; 3Department of Anatomy, School of Medicine, Yanbian University, Yanji, Jilin, 133000, People’s Republic of China; 4Department of General Surgery II, Affiliated Hospital of Beihua University, Jilin, Jilin, 132000, People’s Republic of China
Correspondence: Wenzhe Jin, Department of Pain, Yanbian University Hospital, No. 119, Juzi Street, Yanji, Jilin, 133000, People’s Republic of China, Tel +860433-2660064, Email [email protected]
Objective: Cervicogenic headache (CEH) is a complex secondary headache arising from functional or structural abnormalities within the cervical spine. This systematic review summarizes and evaluates the clinical effectiveness and anatomical mechanisms of minimally invasive techniques targeting sites such as the C2 dorsal root ganglion (DRG) and C1– 2 joint in CEH management..
Methods: PubMed, Embase, Cochrane Library, and Web of Science were systematically searched from January 2004 to May 2025. Studies involving minimally invasive interventions for CEH were included. Data extraction and quality appraisal were independently performed by two reviewers using the Cochrane Risk of Bias (ROB) tool and Newcastle–Ottawa Scale (NOS). Owing to heterogeneity across studies, results were narratively synthesized.
Results: Twenty-three studies were included, comprising 4 randomized controlled trials (RCTs), 13 cohort studies, 1 case-control study, and 5 anatomical studies. Interventions targeting the C2 DRG, C1– 2 joint, cervical discs, deep cervical plexus, and greater occipital nerve showed consistent short-term pain relief and improved quality of life. However, substantial heterogeneity in treatment protocols and limited long-term data restrict definitive conclusions. Most studies demonstrated moderate-to-high methodological quality.
Conclusion: This review integrates clinical and anatomical evidence to clarify how target-specific interventions influence CEH outcomes. The findings highlight the importance of anatomical precision in guiding individualized interventional strategies and provide a theoretical framework for optimizing future treatment paradigms.
Keywords: cervicogenic headache, dorsal root ganglion, radiofrequency, minimally-invasive treatments, anatomical targets, ultrasound guidance
Introduction
Cervicogenic headache (CEH) is a secondary headache arising from pathological changes or dysfunctions in the cervical spine structures. Its etiology involves lesions of the cervical nerves, joints, intervertebral discs, and surrounding soft tissues.1 Because of its multifactorial origins and overlapping clinical features, distinguishing CEH from occipital neuralgia, migraine, and tension-type headache remains challenging.2 According to the latest diagnostic criteria of the International Headache Society (IHS), CEH is characterized by a cervical source of pain, accompanied by neck movement limitation, cervical tenderness, and supportive imaging findings.3 These criteria provide a more standardized basis for diagnosis and facilitate early clinical recognition. Clinically, CEH commonly presents as unilateral neck pain radiating to the occipital or temporal region.4 Epidemiological data indicate that CEH affects approximately 4.1% of the general population5 and up to 17.5% of patients with severe headache,6 underscoring its substantial clinical burden.
The pathophysiology of CEH primarily involves degenerative or inflammatory changes in the upper cervical segments (C1–3) and their related neural structures.7 Irritation of cervical nerve roots or joints, including the atlanto-axial joint and associated occipital nerves, can produce referred pain to the occipital region.8,9 Disc degeneration and soft-tissue dysfunction such as muscular spasm or myofascial inflammation may further contribute to symptom persistence.10–14
Based on these anatomical insights, several minimally invasive interventions have been developed for CEH management, including selective nerve block, pulsed radiofrequency (PRF), radiofrequency ablation (RFA), and coblation radiofrequency.15,16 These procedures aim to relieve pain by reducing local inflammation, modulating nociceptive transmission, or interrupting pathological neural activity. They have been increasingly adopted as promising alternatives to conservative therapy, offering rapid pain relief with minimal complications and high patient acceptability.
Despite increasing evidence supporting the efficacy of minimally invasive interventions for CEH.15–17 Previous reviews have mainly compared interventional techniques but often neglected the crucial role of anatomical target selection. We hypothesize that variations in anatomical targets may substantially influence treatment outcomes, as different neural or musculoskeletal structures may respond differently to the same intervention.
To date, no systematic review has comprehensively summarized clinical and anatomical evidence on minimally invasive interventions for CEH. Therefore, this systematic review integrates evidence from both clinical and anatomical studies to comprehensively evaluate the efficacy and mechanisms of minimally invasive treatments for CEH from an anatomical perspective. By comparing therapeutic outcomes associated with different anatomical targets, this review aims to provide a reference for optimizing individualized interventional strategies and improving clinical efficacy. It is expected that such an anatomy-based analytical framework will enhance understanding of CEH mechanisms and inform the refinement of future clinical treatment paradigms.
Materials and Methods
Reporting Guideline and Registration
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement.18 The protocol was prospectively registered in the PROSPERO database (Registration No. CRD420251183639).
Database Selection and Search Strategy
A comprehensive search was performed in PubMed, Embase, Cochrane Library, and Web of Science from January 2004 to May 30, 2025. Only English-language publications were included. The PubMed search strategy used a combination of the following terms: “cervicogenic headache”, “nerve block”, “radiofrequency”, “pulsed radiofrequency”, “coblation”, “anatomical”, and “minimally invasive”.
Equivalent search strategies were adapted for the other databases. The detailed search strings for each database are provided in Supplementary Table S1.
To enhance completeness, we additionally queried ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform (ICTRP) to identify ongoing or completed but unpublished trials relevant to CEH interventions; records lacking peer-reviewed outcome data were excluded from the evidence synthesis. Reference lists of included studies and related reviews were manually screened.
Eligibility Criteria
Eligibility criteria were defined a priori based on the PICOS framework. Studies were included if they met the following criteria:
(1) Population: Patients clinically diagnosed with CEH, regardless of specific diagnostic criteria;
(2) Intervention: Minimally invasive interventional procedures targeting cervical anatomical structures, such as nerve block, RFA, PRF, coblation, or steroid injection;
(3) Outcomes: Studies were required to report pain-related outcomes.
The primary outcome was pain improvement, expressed as either the change in pain intensity (eg, VAS, NRS, Izbicki score, NPS, or headache intensity scales) or the proportion of patients achieving ≥50% pain reduction (“responders”).
Secondary outcomes included functional disability (eg, Neck Disability Index [NDI]), quality of life (eg, SF-36, EORTC QLQ-C30), sleep or headache impact (eg, PSQI, HIT-6), adverse events, guidance modality–related differences, and durability of treatment effect across follow-up periods.
(4) Study design: Both randomized controlled trials (RCTs) and observational studies (retrospective or prospective cohort, case-control, or single-arm) with or without control groups were eligible.
Additionally, anatomical studies were included if they explicitly described or demonstrated the anatomical mechanisms or neural pathways related to the pathogenesis of CEH, such as nerve compression, joint innervation, or muscle–nerve interactions.
Exclusion Criteria Were
- Non-human or animal studies;
- Case reports or case series with fewer than 10 subjects;
- Studies that did not describe the anatomical mechanisms of CEH (for anatomical studies);
- Conference abstracts, reviews, or non-English publications.
Study Selection and Data Extraction
Two reviewers (X. Jin and Q. Zhang) independently screened the titles, abstracts, and full texts of all retrieved articles according to the eligibility criteria. Disagreements were resolved through discussion or consultation with a third reviewer (Y. Sun).
Data were extracted into a standardized form, including: author, year, country, study design, sample size, diagnostic reference, anatomical target, intervention type, imaging guidance modality, outcome measures (pain intensity, pain relief rate, functional or quality-of-life indicators), follow-up duration, and adverse events.
Quality Assessment
Two reviewers (X. Jin and Q. Zhang) independently performed study-level risk-of-bias assessments. RCTs were appraised with the Cochrane Risk of Bias (ROB) tool (random sequence generation, allocation concealment, blinding of participants/personnel and outcome assessors, incomplete outcome data, selective reporting, and other bias). Observational studies were appraised with the Newcastle–Ottawa Scale (NOS) (Selection, Comparability, Outcome). Disagreements were resolved by discussion or adjudication by a third reviewer (Y. Sun).
The detailed risk-of-bias evaluations for all included studies are presented in Supplementary Figure 1.
Data Synthesis
Given the substantial heterogeneity among included studies in terms of study designs, populations, anatomical targets, techniques, and outcome measures, a narrative synthesis was undertaken, organized by anatomical target. Primary outcome findings are presented as reported changes in pain intensity; secondary outcomes include responder rates (eg, ≥50% pain reduction), functional and quality-of-life metrics, adverse events, and durability of effect during follow-up. For anatomical studies, results are narratively summarized in relation to the structural or neurophysiological mechanisms implicated in CEH pathogenesis.
Results
Study Selection
A total of 1883 records were retrieved from four databases (PubMed, Embase, Cochrane Library, and Web of Science). After removing duplicates and performing title, abstract, and full-text screening, 23 studies met the inclusion criteria and were included in the final qualitative synthesis. Among them, 18 were clinical studies and 5 were anatomical studies.
The detailed screening and selection process is illustrated in Figure 1 (PRISMA flow diagram). The PRISMA 2020 checklist is provided in Supplementary Table S2.
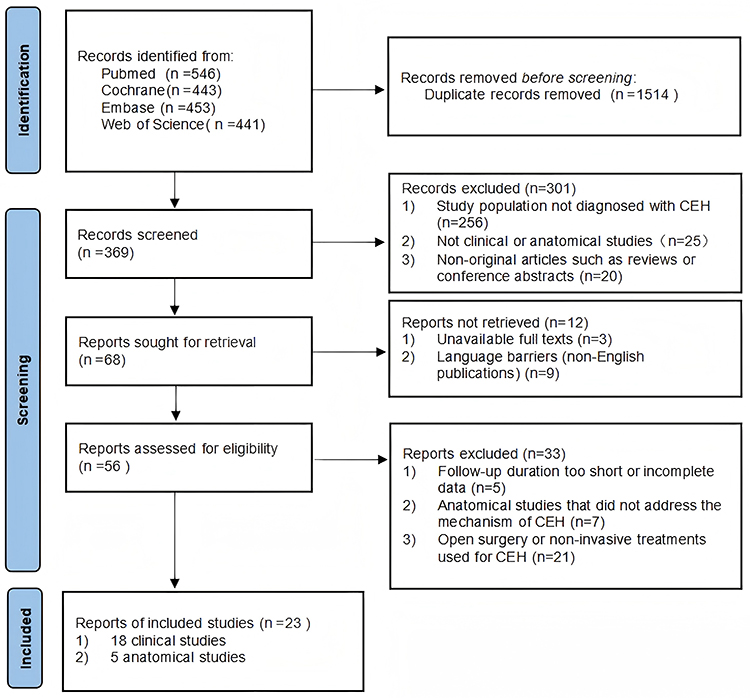 |
Figure 1 PRISMA 2020 flow diagram of literature selection process. |
Study Characteristics
A total of 23 articles were included in this review, comprising 4 RCTs, 1 case-control study, 13 retrospective cohort studies, and 5 anatomical studies (Tables 1 and 2).
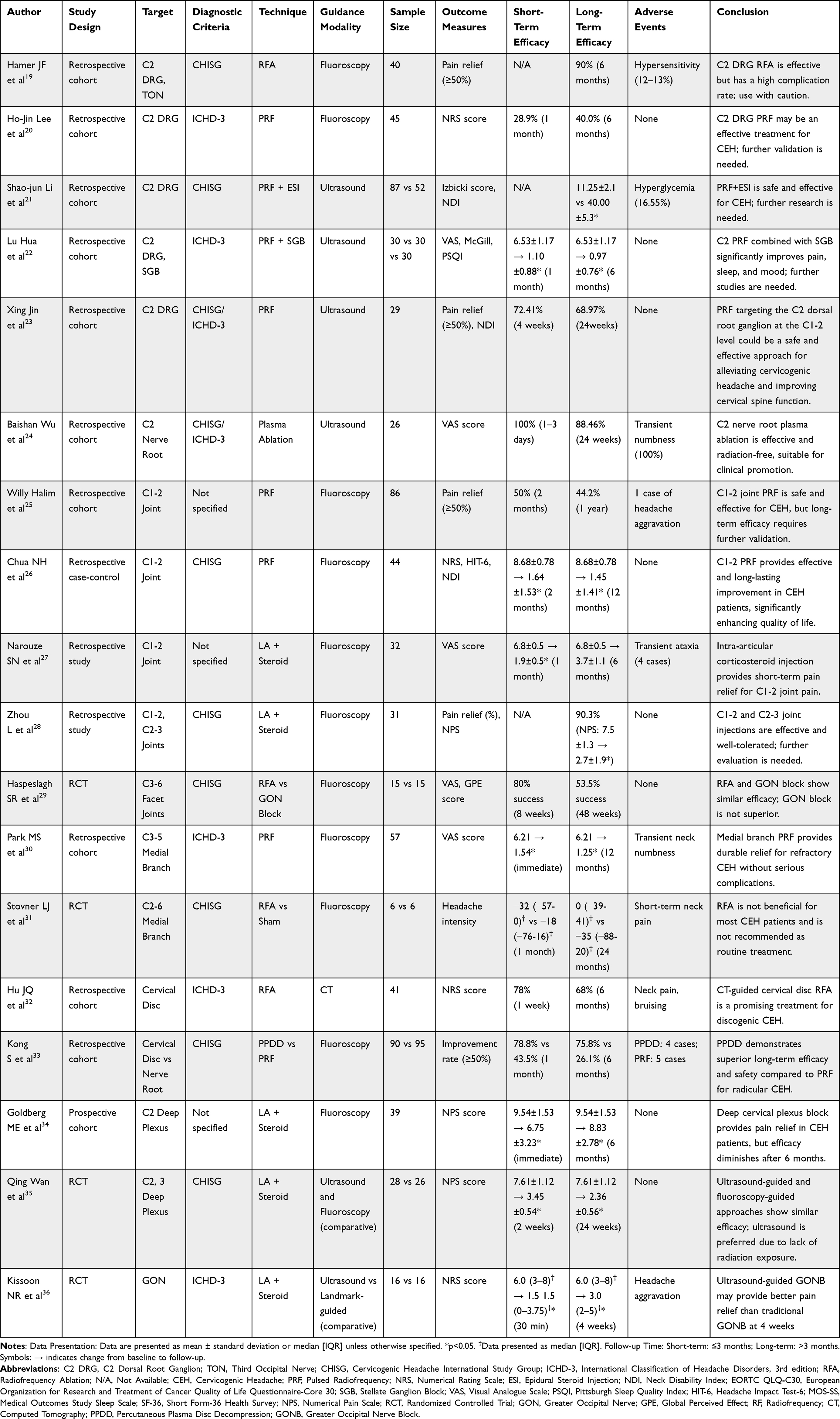 |
Table 1 Summary of Clinical Studies on Anatomical Target-Based Minimally Invasive Techniques for Cervicogenic Headache |
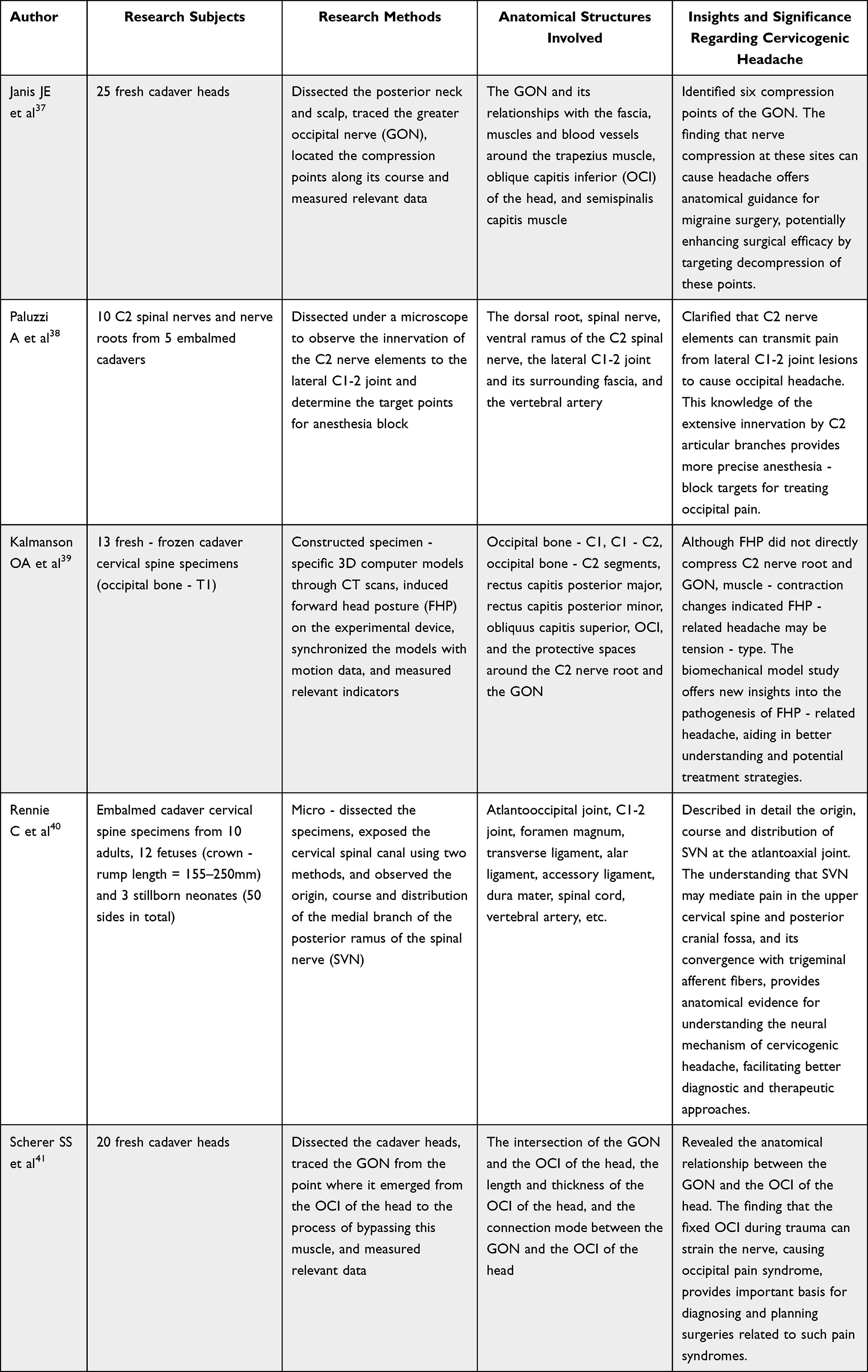 |
Table 2 Summary of Studies on Anatomical - Related Mechanisms of Cervicogenic Headache |
Most clinical studies investigated minimally invasive interventional techniques, including RFA, PRF, coblation, or nerve block, targeting specific cervical anatomical structures.
The anatomical studies, on the other hand, primarily explored neural innervation, compression points, and biomechanical alterations implicated in the pathogenesis of CEH.
The distribution of anatomical targets investigated across clinical studies is visually summarized in Figure 2.
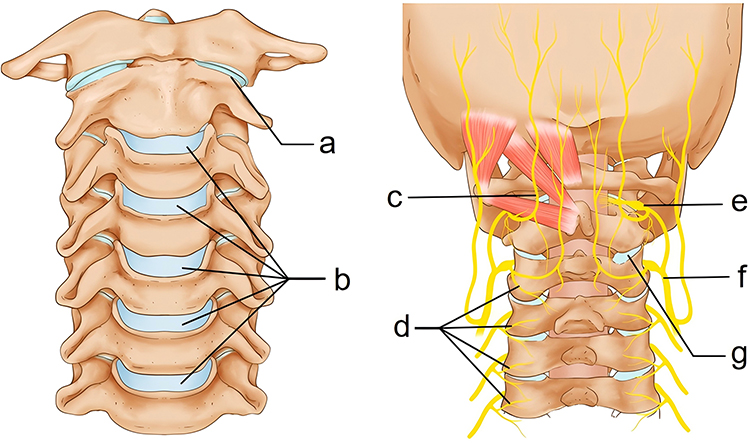 |
Figure 2 Anatomical targets for minimally invasive treatment of cervicogenic headache (anterior and posterior views). The illustration summarizes anatomical targets reported in the included clinical and anatomical studies. (a) C1–2 joint; (b) cervical intervertebral disc; (c) greater occipital nerve; (d) medial branch of cervical nerve; (e) C2 dorsal root ganglion; (f) deep cervical plexus; (g) C2–3 facet joint. |
Quality Assessment
The methodological quality of the included studies varied across study designs.
Among the four RCTs, which were evaluated using the Cochrane ROB tool, two were rated as low risk of bias, one as unclear, and one as high risk, mainly due to incomplete blinding and selective outcome reporting (Figure 3).
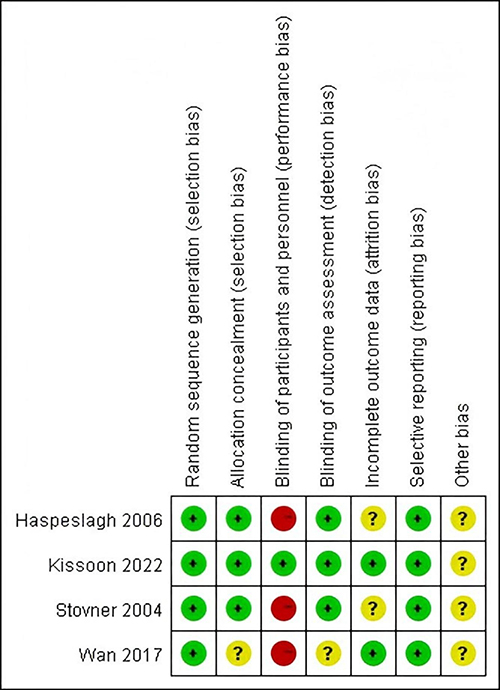 |
Figure 3 Risk of bias assessment of included randomized controlled trials. This figure presents the risk of bias assessment for the included randomized controlled trials using the Cochrane Risk of Bias tool. Each domain represents a potential source of bias: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other bias. Green (+): low risk of bias; Yellow (?): unclear risk of bias; Red (−): high risk of bias. |
For the observational studies, the overall quality assessed using the NOS ranged from 5 to 7 points, indicating moderate to high methodological quality (Table 3).
Overall, the methodological quality of the included studies was acceptable, though the limited number of RCTs and variability in study design warrant cautious interpretation. The detailed results for each anatomical target are presented below.
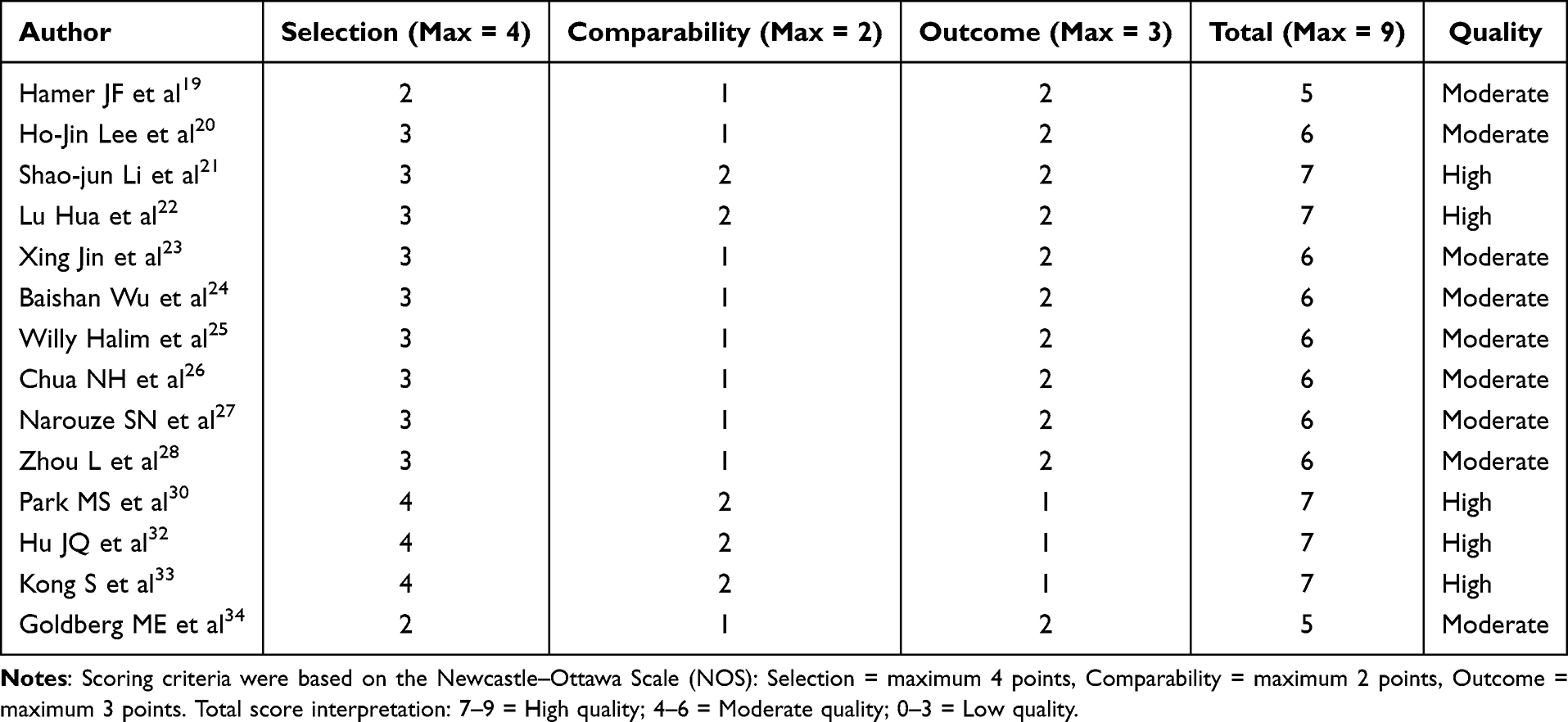 |
Table 3 Quality Assessment of Included Observational Studies Using the Newcastle–Ottawa Scale (NOS) |
Clinical Studies
Primary outcomes (pain intensity or proportion achieving ≥50% pain reduction) and secondary outcomes (functional improvement, quality of life, and adverse events) were narratively summarized according to anatomical target.
C2 Dorsal Root Ganglion (DRG)/C2 Nerve Root
(6 Studies; All Retrospective Cohorts)
Six studies19–24 targeted the C2 DRG or C2 nerve root for treatment. Among them, five studies19–23 focused on the C2 DRG, with four applying the PRF technique20–23 and one using RFA.19 Another study targeted the C2 nerve root and employed the coblation radiofrequency technique.24
Regarding the guiding methods, four studies used X-ray fluoroscopy, and two adopted ultrasound guidance. In terms of treatment effects, Hamer et al19 reported that 90% of patients achieved ≥50% pain relief at six months, though the complication rate reached 12–13%. Ho-Jin Lee et al20 found that 28.9% of patients achieved ≥50% relief at one month and 40.0% at six months, with no complications. Shao-jun Li et al21 demonstrated that PRF of the C2 DRG combined with epidural steroid injection was superior to steroid injection alone in improving pain and quality of life, with the median Izbicki pain score decreasing from 78.5 to 11.25 after two years. Lu Hua et al22 showed that ultrasound-guided PRF of the C2 DRG combined with stellate ganglion block was more effective than either method alone; the Visual Analogue Scale (VAS) score decreased from 6.53 ± 1.17 to 1.10 ± 0.88 at one month, and to 0.97 ± 0.76 at six months. X Jin et al23 reported that ultrasound-guided PRF at the C2 DRG produced ≥50% pain relief in 72.41% of patients at 4 weeks and 68.97% at 24 weeks, with no serious adverse events observed. Collectively, these findings support the C2 DRG as a key anatomical target for neuromodulatory intervention in CEH.
In addition, Wu et al24 targeted the C2 nerve root using ultrasound-guided coblation radiofrequency. All patients experienced ≥50% pain relief within 1–3 days, and 88.46% maintained this level at 24 weeks, with only mild, transient numbness reported. Although the C2 nerve root and C2 DRG are anatomically adjacent, their responses to intervention may differ, warranting further comparative investigation.
In summary, the current evidence supports the C2 DRG as the most reliable and effective anatomical target for neuromodulatory intervention in CEH, while the efficacy of C2 nerve root–based treatments requires further validation.
Quality profile: Five studies rated moderate to high quality (NOS 5–7); overall moderate-certainty evidence supports C2 DRG-targeted interventions.
C1-2 Joint
(3 Studies; 2 Retrospective Cohorts, 1 Case-Control)
Three studies25–27 targeted the C1–2 joint as the anatomical site for treating CEH. Willy Halim et al25 and Chua et al26 applied the PRF technique, while Narouze et al27 utilized intra-articular steroid injection. All three employed X-ray fluoroscopic guidance.
In terms of clinical outcomes, Willy Halim et al25 reported that 50% of patients achieved ≥50% pain relief two months post-treatment, and 44.2% maintained this level at one year, with only one mild complication. In a case-control study by Chua et al26 involving 45 patients, 25 (55.6%) were classified as responders. In this group, the Numeric Rating Scale (NRS) score decreased from 8.68 ± 0.78 to 1.64 ± 1.53 at two months, and further to 1.45 ± 1.41 at twelve months. Narouze et al27 observed a reduction in VAS score from 6.8 ± 0.5 to 1.9 ± 0.5 one month after treatment; however, at six months, the score rose to 3.7 ± 1.1, and the improvement was not statistically significant. Some patients experienced transient headache exacerbation during injection, but most demonstrated a positive response overall.
In summary, interventions targeting the C1–2 joint have shown moderate efficacy and favorable safety profiles, though small sample sizes and technique variability limit the strength of current evidence.
Quality profile: All three studies rated moderate quality (NOS 6); overall moderate-certainty evidence.
Cervical Facet Joints/Medial Branches of Cervical Nerves
(4 Studies: 2 RCTs + 2 Retrospective Cohorts)
Four studies28–31 investigated interventions for CEH targeting the cervical facet joints or the medial branches of cervical nerves.
Zhou et al28 performed zygapophyseal joint injections combined with posterior ramus block of spinal nerves under X-ray fluoroscopic guidance in 31 refractory patients, targeting the C1–2 and C2–3 zygapophyseal joints and the posterior ramus of the C2–3 spinal nerve. A total of 90.3% (28 patients) achieved >50% headache relief, and the Numeric Pain Scale (NPS) score decreased from 7.5 ± 1.3 to 2.7 ± 1.9 after treatment, with an average pain-free duration of 21.7 days. Relapsed patients also responded favorably to repeat treatment, and no complications were reported.
Haspeslagh et al29 applied RFA to the medial branches of the C3–6 zygapophyseal joints under X-ray fluoroscopy. Thirty patients were randomly divided into groups, and compared with the greater occipital nerve (GON) block, there were no significant differences in pain intensity, headache days, or quality-of-life scores across multiple follow-up points. The treatment success rate was also not significantly different between groups.
Park et al30 employed PRF targeting the bilateral medial branches of the C3–5 cervical nerves under X-ray fluoroscopy in 57 refractory patients. The VAS score decreased from 6.21 at baseline to 1.54 immediately post-treatment and further to 1.25 at 12 months. Most patients maintained good long-term relief and were able to discontinue analgesics. Adverse effects were mild and transient.
Stovner et al31 conducted RFA on the medial branches of the C2–6 zygapophyseal joints under fluoroscopic guidance. Twelve patients were randomized equally to RFA or sham groups. One month after treatment, the RFA group showed a median change in headache intensity of −32 [interquartile range (IQR) −57 to 0] compared to −18 [IQR −76 to 16] in the sham group. However, at 24 months, no significant difference was observed (0 [IQR −39 to 41] vs −35 [IQR −88 to 20]), and some patients reported transient neck pain. Owing to methodological variability and limited efficacy, this technique was recommended for research use only.
In summary, evidence regarding cervical facet joint and medial branch interventions remains inconsistent, particularly for targets below the C3 level, suggesting that their therapeutic value for CEH is still uncertain.
Quality profile: Two RCTs showed unclear/high risk of bias; cohorts rated NOS 6–7. Overall low-certainty evidence due to methodological inconsistency.
Cervical Intervertebral Discs
(2 Studies; Both Retrospective Cohorts)
Two included studies32,33 targeted the cervical intervertebral discs as anatomical sites for treating CEH. Hu et al32 used the RFA technique. Under Computed Tomography (CT) guidance, they treated 41 refractory patients by targeting the cervical intervertebral discs. One week after the treatment, 78% of the patients experienced a pain relief of ≥50%, among which 46% had a complete relief. Six months after the treatment, 68% of the patients had a pain relief of ≥50%, with 41% having a complete relief. Moreover, compared with RFA of a single-level cervical intervertebral disc, RFA of multiple-level cervical intervertebral discs showed better results. Although there were mild complications, there were no serious problems. Kong et al33 employed percutaneous coblation disc decompression and the PRF technique. Under X-ray fluoroscopy guidance, they conducted a study on relevant patients. The results showed that the percutaneous coblation disc decompression group had a better CEH remission rate, neck disability index score, etc. at multiple time points after the operation compared with the PRF group, and there was no difference in the incidence of postoperative complications. This indicates that percutaneous coblation disc decompression via the lower cervical approach has a significant effect on relieving CEH pain in patients with combined nerve root type cervical spondylosis and has a better long-term curative effect.
In summary, cervical disc–related interventions appear to provide meaningful symptom relief in selected patients with lower cervical involvement, but further studies are needed to confirm their anatomical relevance to CEH.
Quality profile: Both high-quality observational studies (NOS 7); overall moderate-certainty evidence.
Deep Cervical Plexus
(2 Studies: 1 Prospective Cohort + 1 RCT)
Two included studies34,35 targeted the deep cervical plexus nerves as the anatomical sites for treating CEH. Goldberg et al34 used a modified method of injecting local anesthetics and glucocorticoids at the deep cervical plexus (at the transverse process of C2 on the affected side). Under fluoroscopy guidance, they treated 39 patients. The average treatment cycle for the patients was 59±61 days, and they received an average of 3±1.7 injections. There was a significant change in the NPS score before and after the injection, which decreased from 9.54±1.53 before the treatment to 6.75±3.23. However, the pain returned to the baseline level six months later, with an NPS of 8.83±2.78, suggesting that this technique is effective in the initial stage but its long-term effect needs to be improved. Wan et al35 used both ultrasound guidance and fluoroscopy guidance to inject local anesthetics and glucocorticoids at the deep cervical plexus (at the transverse processes of C2 and C3 on the affected side). They randomly divided 54 patients into an ultrasound group and a fluoroscopy group. Two weeks after the treatment, the NPS score of the ultrasound group decreased from 7.61±1.12 before the treatment to 3.45±0.54, and the NPS score of the fluoroscopy group decreased from 7.50±1.06 before the treatment to 3.40±0.58. At 24 weeks after the treatment, the NPS of the ultrasound group was 2.36±0.56, and the NPS score of the fluoroscopy group was 2.43±0.59. There was no significant difference in the degree of pain relief between the two groups at each follow-up time point, indicating that the two guiding methods have comparable effects. Moreover, the patients in both groups tolerated the procedures well, with only a few experiencing mild discomfort and no serious complications. In addition, ultrasound guidance has an obvious advantage of no radiation exposure and can be used as an effective alternative method for deep cervical plexus block in the treatment of CEH.
In summary, deep cervical plexus block appears effective in reducing pain and improving short- to mid-term outcomes in CEH, though its long-term efficacy and durability remain uncertain.
Quality profile: One moderate-quality cohort (NOS 5) and one RCT with mainly unclear risk of bias; overall low-to-moderate-certainty evidence.
GON
(1 Study; 1 RCT)
One included study36 investigated the treatment of CEH and occipital neuralgia with the GON as the anatomical target under different imaging guidance. Kissoon et al36 randomly divided 32 patients into two groups. The two groups received injections of local anesthetics and steroid hormones at the GON on the affected side, guided by ultrasound and anatomical landmarks, respectively. The results showed that for all patients, the NRS score decreased from 6.0 [IQR 3 to 8] before the treatment to 1.5 [IQR 0 to 3.75] 30 minutes after the treatment, and further decreased to 3.0 [IQR to–5] four weeks after the treatment. There was no significant difference in adverse events between the two groups, and only a few patients presented with mild and transient symptoms.
In summary, although GON-targeted injections demonstrated short-term pain relief with good tolerability, the evidence remains limited because the only available study included a mixed cohort of CEH and occipital neuralgia patients with short follow-up duration.
Quality profile: Single small RCT with unclear risk of bias; low-certainty evidence.
Across-Target Summary
Across anatomical targets, the most consistent and durable improvements were observed for C2 DRG and cervical disc–related interventions (moderate-certainty observational evidence). Evidence for facet joint/medial branch, deep cervical plexus, and GON interventions remains limited or inconsistent (low to low-moderate certainty).
Anatomical Studies
Anatomical studies were narratively summarized to elucidate the structural mechanisms underlying the clinical targets identified above.
Anatomical Characteristics of the Compression Points of the GON
According to the study by Janis et al,37 there are six main compression points along the pathway of the GON. These points are mainly related to the compression sites of the fascia, muscles, and blood vessels. These compression points include the entrance and exit points where the GON passes through the semispinalis and trapezius muscles, as well as the location where it crosses the occipital artery. The study proposed that the anatomical data of these compression points provide crucial references for surgical or non-invasive decompression treatments. By surgically releasing these compression points, some patients can achieve significant relief of headache symptoms.
The Role of the Articular Branches of the C2 Nerve in Occipital Pain
The anatomical study by Paluzzi et al38 has shown that the branches of the C2 nerve extensively innervate the C1-2 joint. These articular branches may be important neural pathways that trigger occipital pain. The study also pointed out that by precisely locating the articular branches of the C2 nerve and injecting anesthetic drugs, it is possible to effectively relieve headaches caused by degenerative diseases or neck trauma. This study further provides the target points for anesthetic injection treatment based on anatomical landmarks.
Biomechanical Changes in the Suboccipital Triangle Area
In the biomechanical study by Kalmanson et al,39 the Forward Head Posture (FHP) leads to a significant reduction (approximately 18.7%) in the area of the suboccipital triangle region. Meanwhile, it increases the tension of the rectus capitis posterior major and minor muscles. However, the study found that the bony structures of the cervical spine protect the GON and the C2 nerve root, and there is no obvious nerve compression. This suggests that headaches associated with FHP are more likely to be related to the cause of muscle tension rather than direct nerve compression.
The Contribution of the Sinus Vertebral Nerves
The study by Rennie et al40 revealed the role of the C1–C3 sinuvertebral nerves in CEH. These nerves, by innervating the dura mater, ligaments, and other structures in the cranio-cervical junction area, may serve as a crucial anatomical basis for headache symptoms. This finding provides the feasibility of using the sinuvertebral nerves as an intervention target and offers a more in-depth perspective for understanding the complex mechanisms of neck pain.
The Interaction Between the Oblique Capitis Inferior (OCI) and the GON
The study by Scherer et al41 focused on the interaction between the GON and the OCI of the head. The results showed that there was a close connection between the two in more than 80% of the specimens. Some nerves passed through the muscle, and the connection patterns were classified into three types: loose type, tight type, and intramuscular type. This anatomical study indicated that the OCI of the head may play a key role as a mechanical pivot point when the GON passes through the soft tissues of the neck. During traumatic movements such as head flexion and extension, this fixed point is likely to be the main cause of occipital headache.
In summary, anatomical studies collectively highlight the convergence of cervical and occipital neural pathways, the potential compression points of the GON, and the mechanical interactions among suboccipital muscles, joints, and sinuvertebral nerves. These findings provide crucial structural evidence supporting the anatomical targets identified in clinical interventions for CEH.
Discussion
CEH is a complex type of headache, and its pathogenesis involves multiple anatomical structures and pathophysiological processes. Through the systematic induction and summary of the included clinical studies on minimally invasive treatment of CEH and the anatomical studies related to CEH, this study found that the C2 DRG, C2 nerve root, C1-2 joint, cervical intervertebral disc, deep cervical plexus nerve, and GON are all effective anatomical targets for the minimally invasive treatment of CEH.
In the pathogenesis of CEH, the C2 DRG plays an extremely crucial role at the anatomical level. Existing studies have shown that some branches of the GON and the Lesser Occipital Nerve (LON) originate from the C2 nerve, which makes most of the occipital pain closely related to the C2 DRG or the C2 nerve.7,42 Janjua et al confirmed through an anatomical study that the OCI of the head in the suboccipital triangle area is innervated by a branch of the dorsal ramus originating from the C2 nerve.43 Therefore, when the OCI of the head causes pain, the pain signals are conducted through the C2 nerve. The studies by Lu Hua et al,22 Xing Jin et al23 and Baishan Wu et al,24 with the help of ultrasound-guided images, found that the C2 DRG or the C2 nerve root is located deep in the OCI of the head and is closely adjacent to this muscle.21–23 Given that the OCI of the head is an important muscle involved in head rotation,44 once it is strained or inflamed, it is highly likely to directly stimulate the C2 DRG or the C2 nerve root, thereby inducing occipital pain symptoms.
The clinical studies19–24 included in this research, which targeted the C2 DRG for treatment, showed that regardless of whether RFA, PRF, or coblation radiofrequency was used, these techniques could effectively relieve patients’ headache symptoms and significantly improve their cervical spine function. However, it should be noted that these studies generally lack long-term follow-up records for more than six months. As a result, the long-term curative effect of using the C2 DRG as a treatment target still needs to be further evaluated in future research. Nevertheless, these research findings further convincingly confirm the crucial role of the C2 DRG in the pathogenesis of CEH. In recent years, with the development of ultrasound-guided techniques, there have been an increasing number of studies on using ultrasound to guide the puncture of the C2 DRG. Traditional fluoroscopy is gradually being replaced, which further improves the precision, safety, and effectiveness of the treatment.45,46 Mechanistically, modulation of the C2 DRG and adjacent C2 root may suppress aberrant afferent discharges from upper cervical segments, leading to relief of occipital referred pain. This process mainly involves reduction of peripheral sensitization within the C2 distribution, while central convergence pathways might also contribute to symptom modulation.
The C1-2 joint, as a joint structure connecting the skull and the neck, plays a crucial role in the rotational, flexion, and extension movements of the neck. However, due to its unique anatomical structure and high mobility, it is extremely prone to problems such as degeneration, strain, and inflammation under the influence of factors such as long-term overloading, trauma, or poor posture.47 According to the anatomical study by Paluzzi et al, the nerves of the C1-2 joint originate from the C1-2 articular branches of the C2 nerve.38 Therefore, when the C1-2 joint is diseased, such as in the case of arthritis or degenerative changes, pain signals can be conducted through the C2 nerve, triggering radiating headaches in the occipital region or the neck. Evidently, the pathological changes of the C1-2 joint are closely related to CEH.
In this study, among the three studies that targeted the C1-2 joint as the anatomical site, two studies using PRF showed good therapeutic effects both in the short term and the long term. In the one study that employed the block treatment (local anesthetic + steroid), the short-term pain treatment effect was quite remarkable, but the therapeutic effect in the long term (> 6 months) was not satisfactory. The possible reason is that, compared with the block treatment, PRF not only treats the degeneration and strain of the C1-2 joint but also regulates the sensory nerves on the C1-2 joint. It effectively inhibits the conduction of pain signals to the C2 nerve root, thus achieving long-term and effective treatment of CEH.25,26
The study by Zhou et al28 demonstrated that injecting into the C1-2 and C2-3 zygapophyseal joints, combined with blocking the posterior rami of the C2 and C3 spinal nerves, could provide most patients with good pain relief, and this effect could be sustained for a certain period. However, because this study involved multiple treatment combinations, it was impossible to determine which specific treatment target played a crucial role.
Most of the studies29–31 on radiofrequency treatment of the medial branches of the posterior rami of spinal nerves below the C3 level have yielded inconsistent results. Therefore, it remains uncertain whether the medial branches of the posterior rami of spinal nerves below the C3 level are effective anatomical targets for the treatment of CEH. This indicates that the treatment effect of this target is influenced by various factors, such as treatment techniques and individual patient differences. More in-depth research is needed to clarify the optimal treatment strategy.
In this study, the anatomical research by Rennie et al revealed the important role of the C1-3 sinuvertebral nerves in the occurrence of CEH.40 Existing studies have shown that sinuvertebral nerves are present in the intervertebral discs and will abnormally grow into them during disc degeneration. They are extremely vulnerable to stimulation, which can then trigger pain.48,49 However, in the clinical study by Hu et al included in this research, most of the patients received RFA treatment of the cervical intervertebral discs below the C4 level;32 in the clinical study by Kong et al, all the included patients had nerve root type cervical spondylosis, and the treatment site was the coblation radiofrequency of the cervical intervertebral discs below the C5 level.33 It is worth noting that these two clinical studies on CEH patients both achieved good therapeutic effects, but during the treatment process, the handling of the sinuvertebral nerves of the upper cervical spine (C1-3) was rarely involved. In addition, in some anterior cervical discectomy and fusion surgeries, most cases mainly dealt with the cervical intervertebral discs below C4, and successfully treated CEH.11,50 Although the main pathogenesis of CEH is usually closely related to the lesions of the upper cervical spine (C1-3), the specific mechanism of why treating the lower cervical intervertebral discs can effectively treat CEH remains unclear at present. This phenomenon provides an important research direction and a point for reflection for further in-depth exploration of the treatment mechanism of CEH in the future, and more research is needed to reveal the mysteries behind it.
In the two clinical studies included in this research, which targeted the deep cervical plexus for the treatment of CEH, the deep cervical plexus block was performed at the location of the transverse process of C2 or C3 on the affected side.34,35 In essence, this is a paravertebral nerve block of C2 and C3. The GON, the LON, and the Third Occipital Nerve (TON) that innervate the head all originate from C2 and C3.51,52 In the past, cervical plexus block was used to provide sufficient anesthesia and analgesia for head and neck surgical procedures.53 The therapeutic effect of deep cervical plexus block may be attributed to the interruption of nociceptive transmission from the GON, LON, and TON, which arise from the C2–C3 plexus and radiate toward the occipital region. In addition, corticosteroids contained in the injectate can alleviate sterile inflammation around these nerves, reducing perineural irritation and thereby relieving headache symptoms in patients with CEH.
In the two anatomical studies37,41 included in this research, it is clearly pointed out that the compression of the GON by the surrounding muscles, fascia, and blood vessels is a key pathogenic factor leading to headache. The mechanism by which the GON mediates headache serves as the pathological basis for two types of headache diseases, namely CEH and occipital neuralgia.54, Moreover, both of these diseases belong to secondary headaches, and their clinical manifestations are extremely similar. Precise differentiation between CEH and occipital neuralgia has always been a difficult point in clinical practice.55,56 The study conducted by Kissoon et al36 included both patients with CEH and those with occipital neuralgia as the research subjects. It is undeniable that there is a certain flaw in the rigor of this method of selecting research subjects. However, the conclusion of this study indicates that, regardless of the disease type, the GON block therapy guided by ultrasound can achieve relatively remarkable therapeutic effects.36
Across these anatomical targets, the converging evidence suggests that minimally invasive interventions primarily act by reducing abnormal nociceptive input from the upper cervical segments (C1–C3), relieving nerve entrapment, and alleviating local aseptic inflammation around affected structures. These mechanisms together may attenuate peripheral sensitization and referred occipital pain, which explains the clinical effectiveness observed in many studies. Nevertheless, the exact neurophysiological processes remain incompletely understood, and the anatomical mechanisms of CEH require further research.
This study has several limitations that need to be addressed. Firstly, the literature search was limited to English-language publications, which may have resulted in the omission of important non-English studies and led to geographical bias. Secondly, there was significant heterogeneity in the intervention protocols (such as radiofrequency parameters and steroid dosages) and outcome assessment tools of the included studies, which hindered the feasibility of direct comparison and meta-analysis. It is worth noting that only 23.53% (4/17) of the clinical studies were RCTs. Most of the studies relied on small-sample retrospective designs, which may have weakened the robustness of the conclusions. Meanwhile, the anatomical studies on the pathogenesis of CEH are very limited, and more high-quality studies are needed in the future to further explore its mechanisms. In addition, there is a contradiction between the therapeutic effect of interventions on the lower cervical intervertebral discs (such as the C4-6 segments) for CEH and the current anatomical evidence (which mainly focuses on the upper cervical structures C1-3). Advanced neuroimaging techniques (such as diffusion tensor imaging, DTI) or electrophysiological techniques are required to elucidate the potential compensatory pathways. There is a lack of long-term safety data for nerve ablation techniques (such as RFA; PRF; and coblation radiofrequency), and the follow-up period of most studies did not exceed 12 months. Finally, inconsistency existed in the diagnostic criteria applied for CEH among the included studies—while most adopted either the Cervicogenic Headache International Study Group (CHISG) criteria or the International Classification of Headache Disorders, 3rd edition (ICHD-3) definitions, several did not specify their diagnostic approach. Moreover, one study included a mixed cohort comprising CEH and occipital neuralgia, which may have contributed to diagnostic heterogeneity and potential bias in the evaluation of treatment efficacy. In the future, multi-center RCT should be carried out, using standardized protocols and extending the follow-up period, to verify these findings and improve the reliability of the evidence.
Conclusion
The pathogenesis of CEH involves multiple interacting structures in the upper cervical spine, including nerves, joints, muscles, and intervertebral discs. This complexity contributes to the diversity of anatomical targets explored in minimally invasive treatments.
Current evidence suggests that interventions targeting structures such as the C2 DRG or C2 nerve root, C1–2 joint, cervical intervertebral disc, deep cervical plexus, and GON may provide pain relief and functional improvement in selected patients. However, these findings should be interpreted with caution given the heterogeneity of study designs, small sample sizes, and limited methodological quality across the available literature.
The overall body of evidence remains preliminary. Further high-quality, prospective, and multicenter randomized controlled trials are needed to validate these outcomes and clarify the underlying mechanisms of CEH. Future studies should also explore whether individualized treatment strategies based on anatomical evaluation and diagnostic confirmation can improve clinical outcomes.
Data Sharing Statement
All the data generated or analyzed during this study are included in this article. For further information, please contact the corresponding author.
Acknowledgment
We would like to express our sincere gratitude to all those who have contributed to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by grants from the Yanbian University School-Enterprise Collaboration Project (ydxq202314), Jilin Province Hygiene and Health Appropriate Technology Promotion Project (No. 2020S001; No. 2016S037), and Jilin Province Health and Family Planning Appropriate Technology for Poverty Alleviation Project (No. 2018FP047).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Bogduk N, Govind J. Cervicogenic headache: an assessment of the evidence on clinical diagnosis, invasive tests, and treatment. Lancet Neurol. 2009;8(10):959–19. doi:10.1016/S1474-4422(09)70209-1
2. Avijgan M, Thomas LC, Osmotherly PG, Bolton PS. A systematic review of the diagnostic criteria used to select participants in randomised controlled trials of interventions used to treat cervicogenic headache. Headache. 2020;60(1):15–27. doi:10.1111/head.13719
3. Headache classification committee of the international headache society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
4. Jull G. Cervicogenic headache. Musculoskelet Sci Pract. 2023;66:102787. doi:10.1016/j.msksp.2023.102787
5. Sjaastad O, Bakketeig LS. Prevalence of cervicogenic headache: vaga study of headache epidemiology. Acta Neurol Scand. 2008;117(3):173–180. doi:10.1111/j.1600-0404.2007.00962.x
6. Sjaastad O, Bakketeig LS. Migraine without aura: comparison with cervicogenic headache. Vågå study of headache epidemiology. Acta Neurol Scand. 2008;117(6):377–383. doi:10.1111/j.1600-0404.2007.00966.x
7. Bogduk N. Cervicogenic headache: anatomic basis and pathophysiologic mechanisms. Curr Pain Headache Rep. 2001;5(4):382–386. doi:10.1007/s11916-001-0029-7
8. Ferch RD, Zhang T, Bogduk N. Athrodesis of the lateral atlanto-axial joint for the relief of neck pain and cervicogenic headache. Pain Med. 2024;25(3):203–210. doi:10.1093/pm/pnad153
9. Hoppenfeld JD. Cervical facet arthropathy and occipital neuralgia: headache culprits. Curr Pain Headache Rep. 2010;14(6):418–423. doi:10.1007/s11916-010-0151-5
10. Jensen RK, Dissing KB, Jensen TS, Clausen SH, Arnbak B. The association between cervical degenerative MRI findings and self-reported neck pain, disability and headache: a cross-sectional exploratory study. Chiropr Man Therap. 2023;31(1):45. doi:10.1186/s12998-023-00517-w
11. Yang L, Li Y, Dai C, et al. Anterior cervical decompression and fusion surgery for cervicogenic headache: a multicenter prospective cohort study. Front Neurol. 2022;13:1064976. doi:10.3389/fneur.2022.1064976
12. Zhou J, Ho A, Ghaffari-Rafi A, Castillo J, Kim K. Headache relief 10 years after cervical disc arthroplasty: multicenter randomized clinical trial post hoc analysis. J Neurosurg Spine. 2023;40(1):54–61. doi:10.3171/2023.8.SPINE23524
13. Lu Z, Zou H, Zhao P, Wang J, Wang R. Myofascial release for the treatment of tension-type, cervicogenic headache or migraine: a systematic review and meta-analysis. Pain Res Manag. 2024;2024:2042069. doi:10.1155/2024/2042069
14. Núñez-Cabaleiro P, Leirós-Rodríguez R. Effectiveness of manual therapy in the treatment of cervicogenic headache: a systematic review. Headache. 2022;62(3):271–283. doi:10.1111/head.14278
15. Piovesan EJ, Utiumi MAT, Grossi DB. Cervicogenic headache - How to recognize and treat. Best Pract Res Clin Rheumatol. 2024;38(1):101931. doi:10.1016/j.berh.2024.101931
16. Goyal S, Kumar A, Mishra P, Goyal D. Efficacy of interventional treatment strategies for managing patients with cervicogenic headache: a systematic review. Korean J Anesthesiol. 2022;75(1):12–24. doi:10.4097/kja.21328
17. Suer M, Wahezi SE, Abd-Elsayed A, Sehgal N. Cervical facet joint pain and cervicogenic headache treated with radiofrequency ablation: a systematic review. Pain Physician. 2022;25(3):251–263.
18. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
19. Hamer JF, Purath TA. Response of cervicogenic headaches and occipital neuralgia to radiofrequency ablation of the C2 dorsal root ganglion and/or third occipital nerve. Headache. 2014;54(3):500–510. doi:10.1111/head.12295
20. Lee HJ, Cho HH, Nahm FS, Lee PB, Choi E. Pulsed radiofrequency ablation of the C2 dorsal root ganglion using a posterior approach for treating cervicogenic headache: a retrospective chart review. Headache. 2020;60(10):2463–2472. doi:10.1111/head.13759
21. Li SJ, Feng D. Pulsed radiofrequency of the C2 dorsal root ganglion and epidural steroid injections for cervicogenic headache. Neurol Sci. 2019;40(6):1173–1181. doi:10.1007/s10072-019-03782-x
22. Hua L, Sha K, Lu H, et al. Clinical efficacy evaluation of ultrasound-guided C2 dorsal root nerve pulsed radiofrequency combined with stellate ganglion block in the treatment of cervicogenic headache: a retrospective cohort study. J Pain Res. 2023;16:2655–2663. doi:10.2147/JPR.S409226
23. Jin X, Li C, Zhang Q, et al. Efficacy and safety of ultrasound-guided pulsed radiofrequency for cervicogenic headache: a retrospective study focusing on the C2 dorsal root ganglion at the C1–2 level. J Oral Facial Pain Headache. 2025;39(1):112–118. doi:10.22514/jofph.2025.010
24. Wu B, Yue L, Sun F, et al. The feasibility and efficacy of ultrasound-guided C2 nerve root coblation for cervicogenic headache. Pain Med. 2019;20(6):1219–1226. doi:10.1093/pm/pny227
25. Halim W, Chua NH, Vissers KC. Long-term pain relief in patients with cervicogenic headaches after pulsed radiofrequency application into the lateral atlantoaxial (C1-2) joint using an anterolateral approach. Pain Pract. 2010;10(4):267–271. doi:10.1111/j.1533-2500.2010.00360.x
26. Chua NH, Halim W, Evers AW, Vissers KC. Whiplash patients with cervicogenic headache after lateral atlanto-axial joint pulsed radiofrequency treatment. Anesth Pain Med. 2012;1(3):162–167. doi:10.5812/aapm.3590
27. Narouze SN, Casanova J, Mekhail N. The longitudinal effectiveness of lateral atlantoaxial intra-articular steroid injection in the treatment of cervicogenic headache. Pain Med. 2007;8(2):184–188. doi:10.1111/j.1526-4637.2006.00247.x
28. Zhou L, Hud-Shakoor Z, Hennessey C, Ashkenazi A. Upper cervical facet joint and spinal rami blocks for the treatment of cervicogenic headache. Headache. 2010;50(4):657–663. doi:10.1111/j.1526-4610.2010.01623.x
29. Haspeslagh SR, Van Suijlekom HA, Lamé IE, Kessels AG, Van kleef M, Weber WE. Randomised controlled trial of cervical radiofrequency lesions as a treatment for cervicogenic headache [ISRCTN07444684]. BMC Anesthesiol. 2006;6(1):1. doi:10.1186/1471-2253-6-1
30. Park MS, Choi HJ, Yang JS, Jeon JP, Kang SH, Cho YJ. Clinical efficacy of pulsed radiofrequency treatment targeting the mid-cervical medial branches for intractable cervicogenic headache. Clin J Pain. 2021;37(3):206–210. doi:10.1097/AJP.0000000000000911
31. Stovner LJ, Kolstad F, Helde G. Radiofrequency denervation of facet joints C2-C6 in cervicogenic headache: a randomized, double-blind, sham-controlled study. Cephalalgia. 2004;24(10):821–830. doi:10.1111/j.1468-2982.2004.00773.x
32. Hu JQ, Zhang J, Ru B, et al. Computed tomography-guided radiofrequency ablation of cervical intervertebral discs for the treatment of refractory cervicogenic headache: a retrospective chart review. Headache. 2022;62(7):839–847. doi:10.1111/head.14361
33. Kong S, Qian X, Cai J, Wang J, Wang K. Percutaneous plasma disc decompression through a lower surgical approach for the treatment of cervicogenic headache in patients with cervical spondylotic radiculopathy: a retrospective cohort study. Biomed Rep. 2024;21(5):152. doi:10.3892/br.2024.1840
34. Goldberg ME, Schwartzman RJ, Domsky R, Sabia M, Torjman MC. Deep cervical plexus block for the treatment of cervicogenic headache. Pain Physician. 2008;11(6):849–854. doi:10.36076/ppj.2008/11/849
35. Wan Q, Yang H, Li X, et al. Ultrasound-guided versus fluoroscopy-guided deep cervical plexus block for the treatment of cervicogenic headache. Biomed Res Int. 2017;2017:4654803. doi:10.1155/2017/4654803
36. Kissoon NR, O’Brien TG, Bendel MA, et al. Comparative effectiveness of landmark-guided greater occipital nerve (GON) block at the superior nuchal line versus ultrasound-guided GON block at the level of C2: a randomized clinical trial (RCT). Clin J Pain. 2022;38(4):271–278. doi:10.1097/AJP.0000000000001023
37. Janis JE, Hatef DA, Ducic I, et al. The anatomy of the greater occipital nerve: part II. Compression point topography. Plast Reconstr Surg. 2010;126(5):1563–1572. doi:10.1097/PRS.0b013e3181ef7f0c
38. Paluzzi A, Belli A, Lafuente J, Wasserberg J. Role of the C2 articular branches in occipital headache: an anatomical study. Clin Anat. 2006;19(6):497–502. doi:10.1002/ca.20206
39. Kalmanson OA, Khayatzadeh S, Germanwala A, et al. Anatomic considerations in headaches associated with cervical sagittal imbalance: a cadaveric biomechanical study. J Clin Neurosci. 2019;65:140–144. doi:10.1016/j.jocn.2019.02.003
40. Rennie C, Haffajee MR, Ebrahim MA. The sinuvertebral nerves at the craniovertebral junction: a microdissection study. Clin Anat. 2013;26(3):357–366. doi:10.1002/ca.22105
41. Scherer SS, Schiraldi L, Sapino G, et al. The greater occipital nerve and obliquus capitis inferior muscle: anatomical interactions and implications for occipital pain syndromes. Plast Reconstr Surg. 2019;144(3):730–736. doi:10.1097/PRS.0000000000005945
42. Wang L, Shen J, Das S, et al. Diffusion tensor imaging of the C1-C3 dorsal root ganglia and greater occipital nerve for cervicogenic headache. Korean J Pain. 2020;33(3):275–283. doi:10.3344/kjp.2020.33.3.275
43. Janjua MB, Zhou PL, Greenfield JP, Baaj AA, Frempong-Boadu A. C2 and greater occipital nerve: the anatomic and functional implications in spinal surgery. Cureus. 2017;9(3):e1074. doi:10.7759/cureus.1074
44. George T, Tadi P. Anatomy, head and neck, suboccipital muscles. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
45. He L, Zhao W, Su PP, et al. A novel ultrasonographic method to quickly and accurately access the C2 dorsal root ganglion. Pain Physician. 2024;27(8):E927–E935. doi:10.36076/ppj.2024.7.E927
46. Ma D, Maimaitimin A, Wang Y. A novel ultrasound-guided “three in one” approach plus interfascial plane blocks for the treatment of cervicogenic headache. Local Reg Anesth. 2024;17:1–8. doi:10.2147/LRA.S446667
47. Yin M, Ding X, Liu S, Ma J, Mo W. Research progress of atlantoaxial osteoarthritis: a narrative literature review. World Neurosurg. 2022;160:e573–e578. doi:10.1016/j.wneu.2022.01.081
48. Wu B, Yang L, Peng B. Ingrowth of nociceptive receptors into diseased cervical intervertebral disc is associated with discogenic neck pain [Published correction appears in pain med. 2020 Mar 1;21(3):654.]. Pain Med. 2019;20(6):1072–1077. doi:10.1093/pm/pnz013
49. Olmarker K, Blomquist J, Strömberg J, Nannmark U, Thomsen P, Rydevik B. Inflammatogenic properties of nucleus pulposus. Spine. 1995;20(6):665–669. doi:10.1097/00007632-199503150-00006
50. Pang X, Liu C, Peng B. Anterior cervical surgery for the treatment of cervicogenic headache caused by cervical spondylosis. J Pain Res. 2020;13:2783–2789. doi:10.2147/JPR.S275680
51. Li J, Szabova A. Ultrasound-guided nerve blocks in the head and neck for chronic pain management: the anatomy, sonoanatomy, and procedure. Pain Physician. 2021;24(8):533–548.
52. Cesmebasi A, Muhleman MA, Hulsberg P, et al. Occipital neuralgia: anatomic considerations. Clin Anat. 2015;28(1):101–108. doi:10.1002/ca.22468
53. Kim JS, Ko JS, Bang S, Kim H, Lee SY. Cervical plexus block. Korean J Anesthesiol. 2018;71(4):274–288. doi:10.4097/kja.d.18.00143
54. Lefel N, van Suijlekom H, Cohen SPC, Kallewaard JW, Van Zundert J. 11. Cervicogenic headache and occipital neuralgia. Pain Pract. 2025;25(1):e13405. doi:10.1111/papr.13405
55. Barmherzig R, Kingston W. Occipital neuralgia and cervicogenic headache: diagnosis and management. Curr Neurol Neurosci Rep. 2019;19(5):20. doi:10.1007/s11910-019-0937-8
56. Castillo-álvarez F, Hernando de la Bárcena I, Marzo-Sola ME. Greater occipital nerve block in the treatment of headaches. Review of evidence. Bloqueo anestésico del nervio occipital mayor en el tratamiento de las cefaleas. Revisión de la evidencia. Med Clin. 2023;161(3):113–118. doi:10.1016/j.medcli.2023.04.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.