Back to Journals » Cancer Management and Research » Volume 18

Mindfulness, Psychological Resilience, and Social Function Deficits in Young and Middle-Aged Lymphoma Patients: A Latent Profile and Mediation Analysis
Authors Zhang L ![]() , Li F, Wu Y, Zhang Y, Xu C, Zhu W
, Li F, Wu Y, Zhang Y, Xu C, Zhu W ![]()
Received 25 September 2025
Accepted for publication 4 March 2026
Published 19 March 2026 Volume 2026:18 570129
DOI https://doi.org/10.2147/CMAR.S570129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Javier-David Benitez-Fuentes
Li Zhang,1 Fengyi Li,1 Yaru Wu,1 Yuting Zhang,1 Chunyan Xu,2,3 Wei Zhu3,4
1School of Nursing, Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 2Department of Gynecologic Surgery, The Affiliated Cancer Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 3Health Care Research Center for Xinjiang Regional Population, Urumqi, Xinjiang, People’s Republic of China; 4Department of Lymphoma, The Affiliated Cancer Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China
Correspondence: Wei Zhu, Department of Lymphoma, The Affiliated Cancer Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China, Email [email protected]
Objective: This study aims to identify distinct mindfulness profiles among young and middle-aged lymphoma patients and to examine the mediating role of psychological resilience in the relationship between these mindfulness profiles and social function deficits.
Methods: From November 2024 to June 2025, a total of 324 young and middle-aged lymphoma patients were recruited using convenience sampling from a tertiary cancer hospital in Urumqi, Xinjiang, China. Participants completed the Mindful Attention Awareness Scale, the 10-item Connor-Davidson Resilience Scale, and the Social Dysfunction Screening Scale. We used latent profile analysis (LPA) to identify distinct mindfulness profiles and tested the mediating role of psychological resilience with the Bootstrap method.
Results: Latent profile analysis identified three distinct mindfulness profiles among the patients: a low mindfulness type (29.3%), a moderate mindfulness type (40.1%), and a high mindfulness type (30.6%). Furthermore, psychological resilience partially mediated the relationship between these mindfulness profiles and social function deficits.
Conclusion: Young and middle-aged lymphoma patients exhibit heterogeneous mindfulness profiles. Higher mindfulness can enhance psychological resilience, which in turn alleviates social function deficits. Therefore, healthcare providers should develop personalized interventions targeting psychological resilience based on patients’ specific mindfulness profiles to improve their social function.
Keywords: young and middle-aged lymphoma, mindfulness, psychological resilience, social function deficit, latent profile, mediation analysis
Introduction
Lymphoma is a malignant tumor originating in the lymphoid hematopoietic system. In recent years, the incidence of lymphoma in China has continued to rise, with a trend toward younger age at onset.1 Meanwhile, advances in medical technology have substantially improved survival and cure rates among lymphoma patients.2 However, a considerable number of patients still experience treatment failure or relapse after remission,3,4 leading to a protracted disease course. Such long-term and recurrent disease progression can severely impair their social function. As a crucial indicator of recovery, impaired social function primarily manifests as difficulties in social interaction and role fulfillment. This issue is particularly acute among young patients.5 Young and middle-aged individuals face intense family and career pressures, making them particularly vulnerable to social dysfunction caused by the physical and psychological burden of lymphoma.6 This directly impedes their return to normal social roles. Furthermore, it increases the risk of depression and impaired quality of life,7 as well as leading to social isolation.8 Notably, social isolation itself is a significant risk factor for increased all-cause mortality.9 Therefore, addressing social function deficits is crucial for promoting the holistic recovery of these patients.
Mindfulness is a mental state characterized by non-judgmental attention to and awareness of present-moment experiences.10 It reflects patients’ capacity for psychological adaptation and emotional regulation during illness, and is closely associated with quality of life.11 As a positive psychological trait, mindfulness not only helps alleviate perceived stress and enhance interpersonal satisfaction, thereby promoting the recovery of social function in domains such as work,12,13 but also fosters prosocial behavior,14 thus further exerting a positive influence on social function. However, previous studies have predominantly adopted variable-centered approaches, overlooking individual heterogeneity.15 Therefore, this study uses latent profile analysis (LPA), a person-centered method that identifies homogeneous subtypes based on observable indicators.16 By examining how these distinct mindfulness profiles relate to social function deficits, we aim to improve clinical assessment and supportive care for this population.
Psychological resilience, defined as the capacity to adapt effectively to adversity,17 is significantly associated with social function deficits. Specifically, low resilience represents a key risk factor for impaired social function,18 which is typically manifested as marked social withdrawal and reduced social engagement.19 Furthermore, mindfulness is positively associated with psychological resilience, as it enhances self-regulation and reduces rumination.20,21 However, it remains unclear how distinct mindfulness profiles influence social function deficits through the mediating mechanism of psychological resilience. Clarifying this mediating role would help elucidate their differential pathways and facilitate the development of precise, profile-based psychosocial interventions.
Mindfulness-Based Meaning Theory posits that mindfulness serves as a buffer against stress by promoting decentering and broadening attentional focus, allowing for more adaptive reappraisal of adverse events.22,23 This process fosters psychological resilience, which in turn supports both psychological well-being and active social participation.22 Specifically, mindfulness enhances psychological resilience through improved cognitive-emotional regulation.23 This increased resilience thereby acts as an internal mechanism that improves social function by facilitating adaptive coping.24 Grounded in this theory, this study aims to explore the relationships among mindfulness, psychological resilience, and social function deficits in young and middle-aged lymphoma patients, to provide a theoretical basis for targeted interventions. The following hypotheses are proposed:
H1. Mindfulness is heterogeneous among young and middle-aged lymphoma patients. H2. Distinct latent mindfulness profiles predict social function deficits, and this association is partially mediated by psychological resilience.
The theoretical framework is presented in Figure 1.
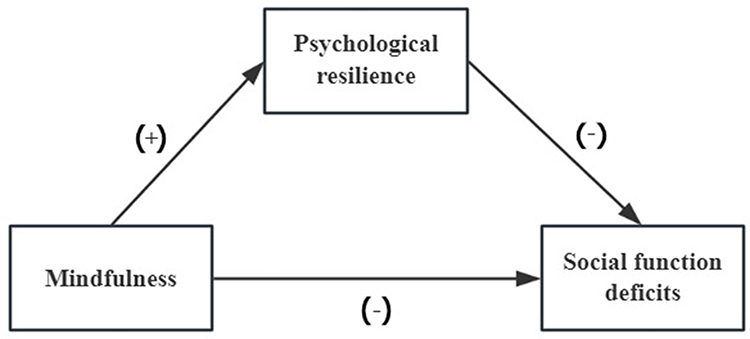 |
Figure 1 The hypothesis framework. Notes: “+” indicates positive correlation; “-” indicates negative correlation. |
Study Subjects and Methods
Study Subjects
Lymphoma patients who were treated at a tertiary cancer hospital in Urumqi, Xinjiang, between November 2024 and June 2025 were recruited using convenience sampling. Inclusion criteria were as follows: (1) histopathologically confirmed lymphoma; (2) aged 18–59 years; and (3) voluntary provision of written informed consent. Additionally, only patients with documented current efficacy assessment data in their electronic medical records were included. Exclusion criteria were: (1) a history of psychiatric disorders or cognitive impairment; (2) other concurrent malignancies; or (3) being too critically ill to complete the questionnaires.
Study Size
The sample size was determined based on the typical range of profiles (3–5) identified in latent profile analysis.25 With at least 50 cases per profile and allowing for a 20% attrition rate, the required sample size was calculated as 313. The final sample comprised 324 participants, which met this requirement.
Instruments
General Information Questionnaire
The questionnaire was developed by the researchers based on a literature review and consisted of two sections. The first section collected demographic information, including gender, age, marital status, education level, monthly per capita household income, residence, type of health insurance, and number of children. The second section collected disease-related information, including tumor type, cancer stage, transplantation status, duration of illness, and current disease status.
Mindful Attention Awareness Scale (MAAS)
This study used the Chinese version of the scale, which was originally developed by Brown and Ryan26 and translated and validated by Chen27 et alIt is a unidimensional scale comprising 15 items, each rated on a 6-point Likert scale ranging from 1 (“almost never”) to 6 (“almost always”). Higher total scores indicate greater levels of present-moment awareness and attention in daily life. In the present study, the scale demonstrated excellent internal consistency, with a Cronbach’s α coefficient of 0.920.
10-Item Connor-Davidson Resilience Scale (CD-RISC-10)
Psychological resilience was measured using the Chinese version of the 10-item Connor-Davidson Resilience Scale. The original 25-item scale was developed by Connor and Davidson28 and later shortened to 10 items by Campbell-Sills and Stein.29 This study used the Chinese version translated and revised by Ye et al,30 which has been validated in Chinese populations and measures two dimensions: adaptability and resilience Items are rated on a 5-point Likert scale ranging from 0 (almost never) to 4 (“almost always”). Total scores range from 0 to 40, with higher scores indicating greater psychological resilience. In this study, the scale demonstrated acceptable internal consistency with a Cronbach’s α of 0.767.
Social Dysfunction Screening Scale (SDSS)
Social function deficits were assessed using the Chinese version of the Social Dysfunction Screening Scale. The scale was originally developed by the World Health Organization and later revised by the 12 Provincial/Municipal Collaborative Group on Psychiatric Epidemiology in China.31 It consists of 10 items, each evaluating a distinct aspect of the patient’s social behavior or role performance. Items are rated on a 3-point scale from 0 (“normal”) to 2 (“severely impaired”). The total score ranges from 0 to 20, with a score of <2 indicating normal social function and a score of ≥2 indicating social dysfunction. Higher scores reflect greater severity of impairment. In the present study, the scale demonstrated good internal consistency, with a Cronbach’s α of 0.780.
Data Collection
Prior to data collection, research staff received standardized training and provided participants with a detailed explanation of the purpose and significance of the study. Written informed consent was obtained before administration of the questionnaire. Questionnaires were completed via face-to-face interviews. During the investigation, researchers clarified any questions on site, and all questionnaires were completed and collected immediately. To ensure data quality, each returned questionnaire was rigorously reviewed. Invalid questionnaires, including those with incomplete responses, uniform responses across all items, or logical inconsistencies, were excluded. A total of 340 questionnaires were distributed, and 324 valid questionnaires were recovered, with a valid response rate of 95.29%.
Statistical Analysis
This study used SPSS 26.0 and Mplus 8.3 for statistical analyses. First, descriptive statistics and correlation analyses were performed using SPSS 26.0. Subsequently, LPA was conducted in Mplus 8.3 to identify mindfulness subtypes. The optimal number of profiles was determined by comparing model fit indices, including the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and adjusted Bayesian Information Criterion (aBIC), as well as entropy. Smaller AIC, BIC, and aBIC values indicate better model fit, with BIC serving as the primary selection criterion. Entropy values closer to 1 represent higher classification accuracy. The Lo-Mendell-Rubin likelihood ratio test (LMRT) and Bootstrapped Likelihood Ratio Test (BLRT) were used to compare the fit of nested models. A P-value < 0.05 indicates that the k-profile model fits the data better than the (k-1)-profile model.25 Second, univariate and multivariate analyses were used to explore factors associated with different mindfulness subtypes, with results visualized using forest plots.Third, the Bolck-Croon-Hagenaars (BCH) method was applied to examine differences in social function deficits across the identified latent profiles.Fourth, Harman’s single-factor test was conducted to assess potential common method bias.32 Finally, a mediation model was tested with the mindfulness latent profile as the independent variable, psychological resilience as the mediator, and social function deficits as the dependent variable, while controlling for relevant demographic and clinical variables. Using the PROCESS macro (Model 4) in SPSS 26.0, the indirect effect was tested via the bias-corrected bootstrap method with 5,000 resamples.
Results
Demographic Characteristics
The study cohort consisted predominantly of males (60.5%) and individuals aged 18–44 years (64.2%). Regarding education level, most participants (39.5%) had completed junior high school or below. In terms of monthly per capita household income, 36.1% reported an income of 3,000–5,000 RMB. Clinically, 37.0% had a duration of illness shorter than 6 months, and 63.6% were in remission or had controlled disease. Social function deficit scores differed significantly across groups defined by gender, age, education level, monthly per capita household income, and duration of illness (P<0.05). Detailed data are presented in Table 1.
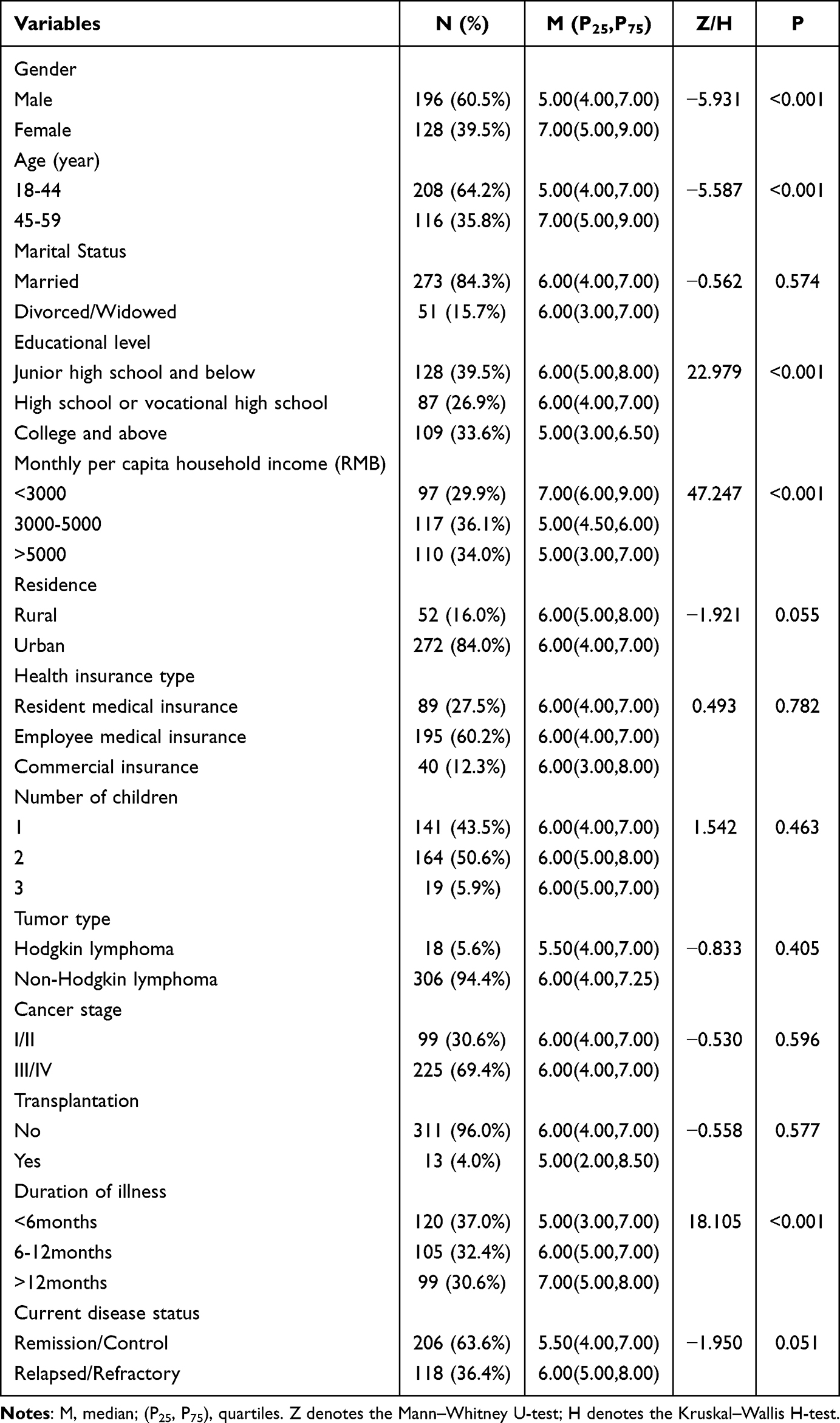 |
Table 1 Differences in Social Function Deficit Scores Across Demographic and Disease-Related Variables (n=324) |
Correlation Analysis of Mindfulness, Psychological Resilience, and Social Function Deficits
First, the normality of the distributions for mindfulness, psychological resilience, and social function deficits was tested. As the data violated the assumption of normality (P<0.05), Spearman’s rank correlation analysis was employed. The results showed a strong positive correlation between mindfulness and psychological resilience (r=0.638, P<0.001), as well as strong negative correlations between mindfulness and social function deficits (r=–0.640, P<0.001) and between psychological resilience and social function deficits (r=–0.707, P<0.001) (Figure 2).
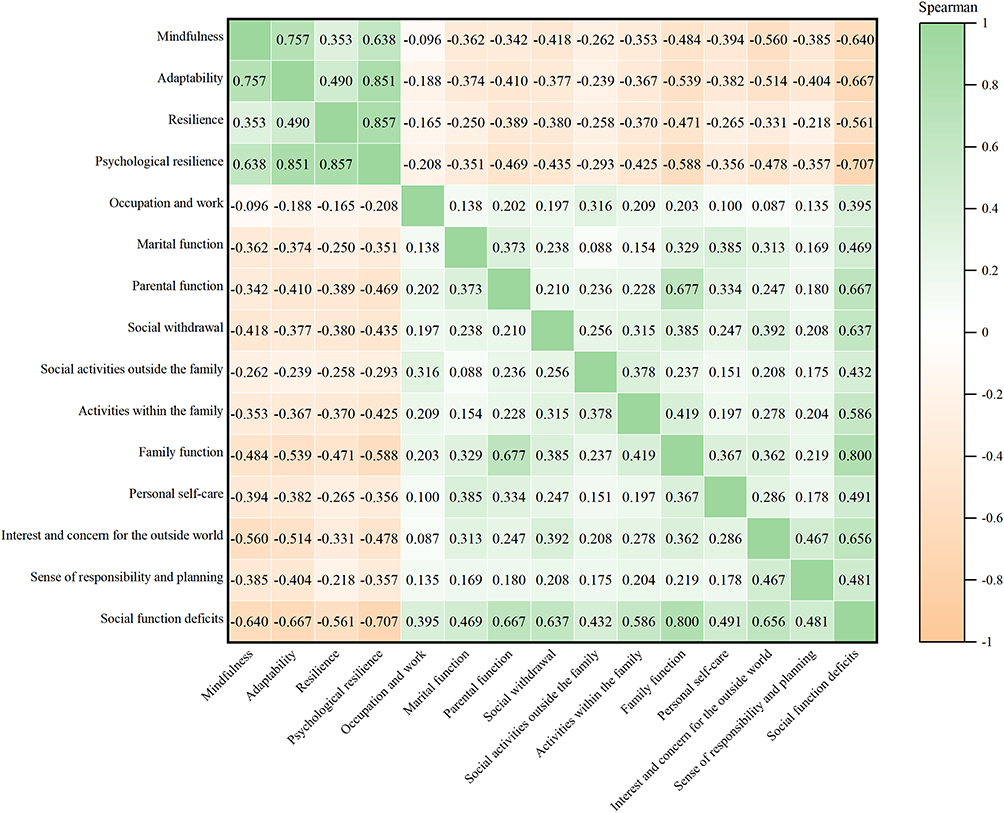 |
Figure 2 Spearman correlation heatmap of mindfulness, psychological resilience, and social function deficits. |
LPA of Mindfulness
To determine the optimal latent profile architecture for mindfulness, models with 1 to 5 profiles were estimated sequentially. The choice was guided by the principles of model parsimony and classification accuracy. Both the 4- and 5-profile solutions were rejected because their LMRT tests were non-significant (P>0.05), and each contained at least one profile with a sample proportion below 5%, indicating insufficient interpretability and stability. Compared with the 2-profile model, the 3-profile solution showed a lower BIC value and higher entropy (0.979). The average posterior probabilities for class assignment all exceeded 0.95 (0.994, 0.987, 0.997), indicating excellent classification accuracy. Therefore, the 3-profile model was ultimately selected as optimal (Table 2). Figure 3A illustrates the characteristic score patterns of the three mindfulness latent profiles. Based on the scores across profiles, the first profile was labeled the “low mindfulness type” (n=95, 29.3%); the second, the “moderate mindfulness type” (n=130, 40.1%); and the third, the “high mindfulness type” (n=99, 30.6%). The specific meanings of the mindfulness items are detailed in Supplementary Material. Univariate and multivariate analyses revealed that age and number of children were factors distinguishing Profile 1 from Profile 2. Gender, age, number of children, duration of illness, and current disease status were factors distinguishing Profile 1 from Profile 3 (Figure 3B).
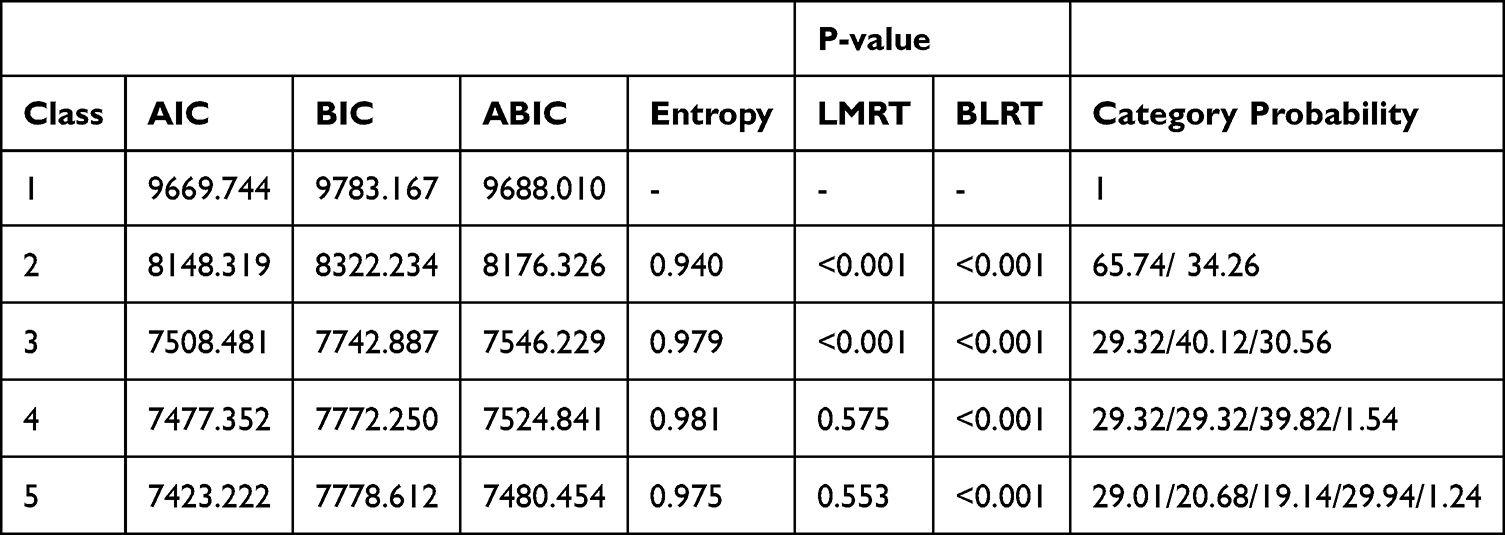 |
Table 2 Latent Profile Analysis Fit Indices and Classification Probabilities for Mindfulness |
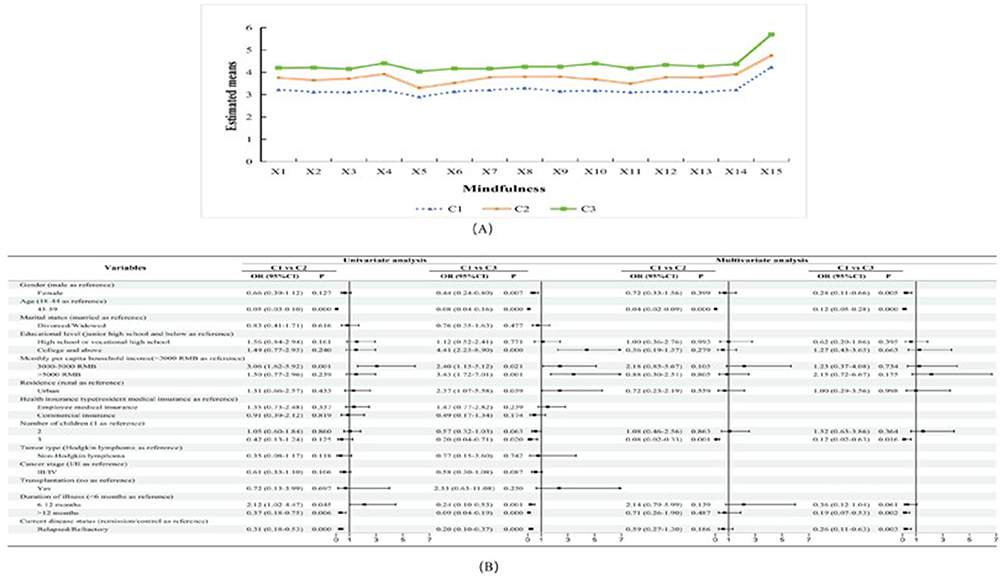 |
Figure 3 Characteristic score patterns of mindfulness latent profiles and associated logistic regression analysis results. Notes: (A) Distributions of characteristic scores for three mindfulness latent profiles. C1 = Low Mindfulness Type; C2 = Moderate Mindfulness Type; C3 = High Mindfulness Type. (B) Logistic regression analysis results for the associated factors of mindfulness latent profiles. |
Differences in Social Function Deficits Across Mindfulness Latent Profiles
Building on the three identified mindfulness latent profiles, differences in social function deficits across these profiles were examined using the Bolck-Croon-Hagenaars (BCH) method. The overall test was significant (=158.014, P<0.001), indicating that social function deficit scores differed among the profiles. Post-hoc pairwise comparisons revealed a graded pattern: C1 (low mindfulness type) had the highest deficit scores, followed by C2 (moderate mindfulness type), and then C3 (high mindfulness type), with all pairwise differences being statistically significant (P<0.05; see Table 3).
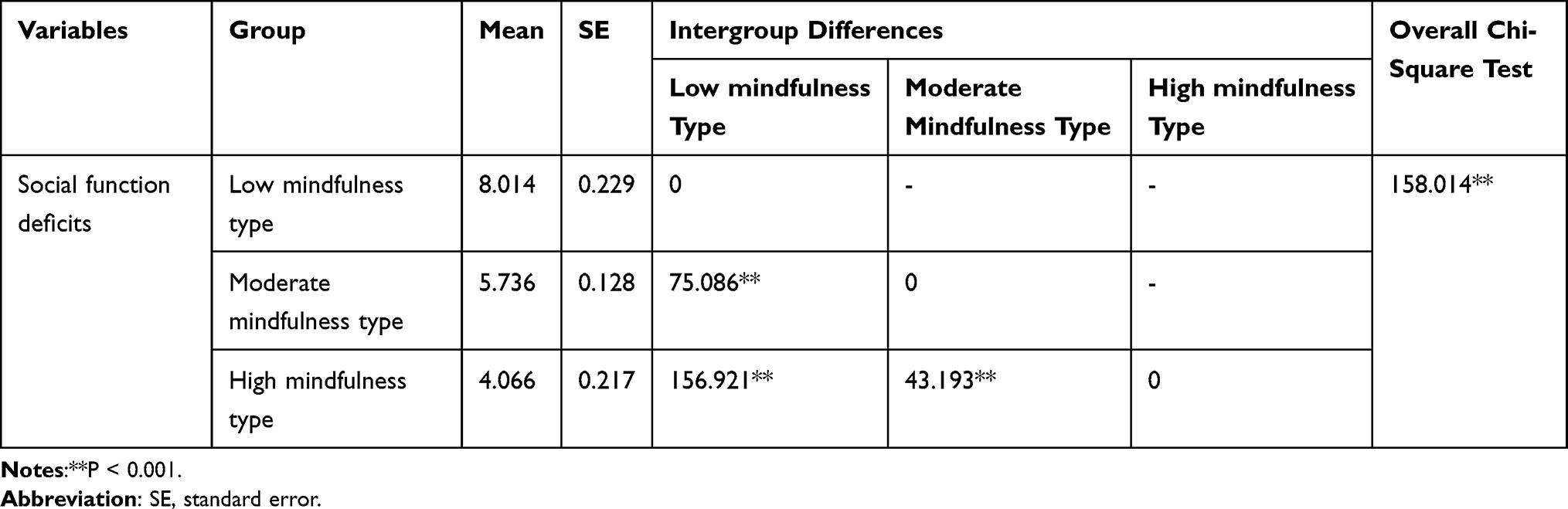 |
Table 3 Intergroup Comparisons of Social Function Deficit Scores Across Mindfulness Latent Profiles (N = 324) |
The Mediating Role of Psychological Resilience Between Mindfulness Latent Profiles and Social Function Deficits
Harman’s single-factor test showed that the variance explained by the first common factor was 31.87%, which was less than 40%, indicating no serious common method bias in this study. We controlled for several covariates associated with social function deficits and mindfulness latent profiles, including gender, age, education level, monthly per capita household income, number of children, duration of illness, and current disease status.
The mediating effect was examined using the bias-corrected bootstrap method with 5,000 resamples in SPSS PROCESS. Latent class membership derived from LPA was entered into the mediation model as a categorical independent variable, with the low mindfulness type automatically set as the reference group by the PROCESS macro, psychological resilience as the mediator, and social function deficits as the dependent variable. Mediation analysis (bias-corrected bootstrap, 95% CI) revealed that, compared with the low mindfulness type, both the moderate and high mindfulness types exhibited significant direct, indirect (via psychological resilience), and total effects on social function deficits, with all 95% CIs excluding zero (Table 4). Specifically, for the moderate type: direct (−1.882 to −0.845), indirect (−1.341 to −0.566), total (−2.870 to −1.723); for the high type: direct (−2.406 to −1.116), indirect (−2.625 to −1.480), total (−4.401 to −3.162). These results demonstrated that psychological resilience partially mediated the association between mindfulness latent profiles and social function deficits (Figure 4).
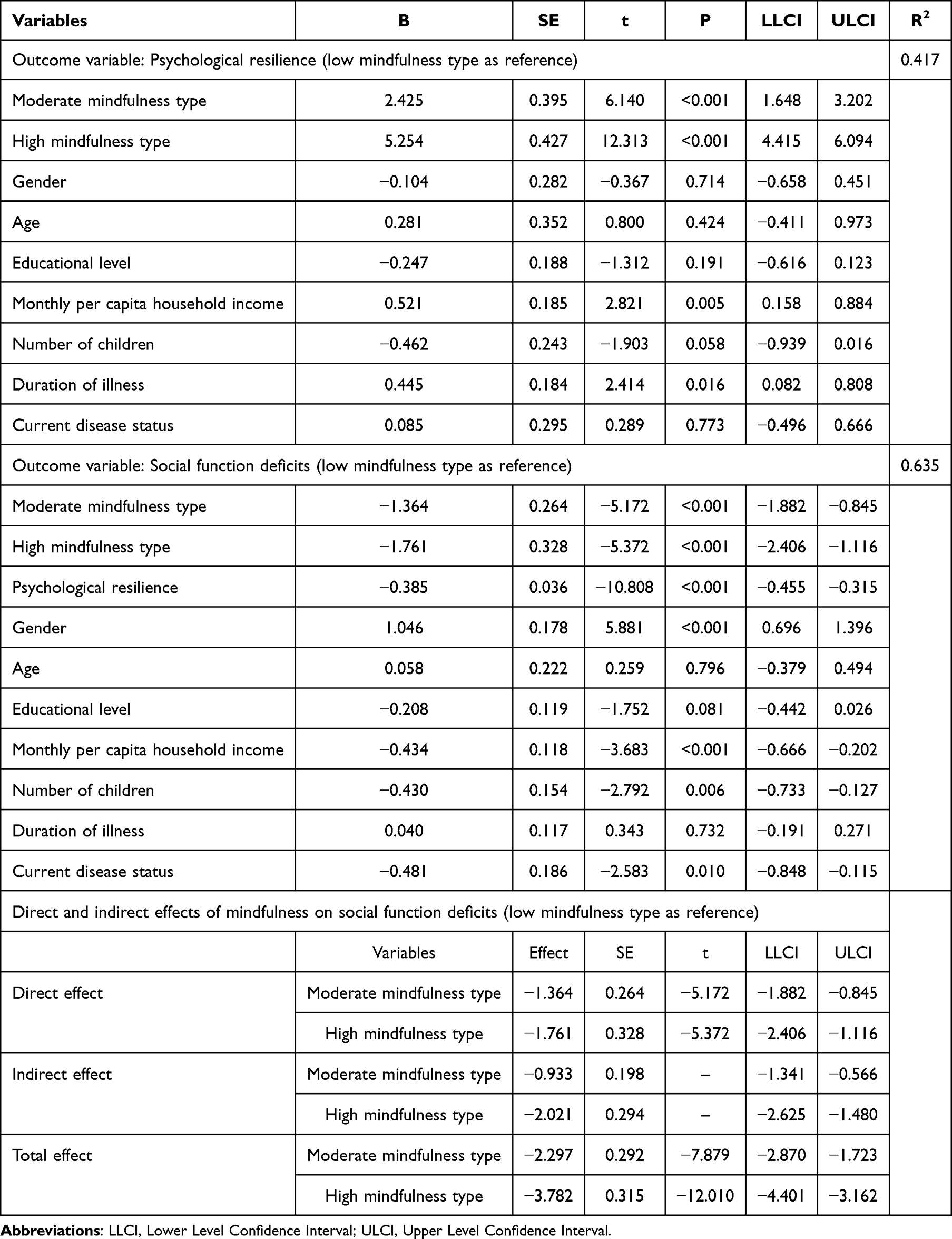 |
Table 4 Mediating Role of Psychological Resilience Between Mindfulness Latent Profiles and Social Function Deficits |
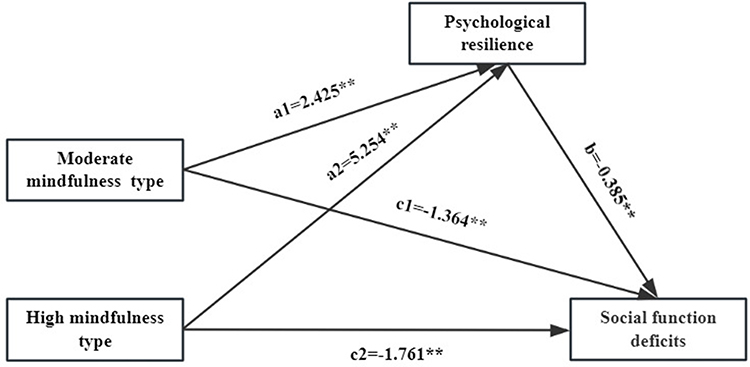 |
Figure 4 Mediation model of psychological resilience between mindfulness latent profiles and social function deficits. Notes: **P<0.001. The “Low Mindfulness Type” was used as the reference group. Path coefficients are unstandardized. |
Discussion
Among young and middle-aged lymphoma patients, mindfulness was best characterized by three distinct latent profiles. Social function deficit scores differed significantly across these profiles. After adjusting for key demographic and clinical covariates, psychological resilience was found to partially mediate the association between mindfulness profiles and social function deficits.
Latent Profile Analysis of Mindfulness
The results revealed three distinct mindfulness profiles among young and middle-aged lymphoma patients. Among them, 95 patients (29.3%) were classified into the low mindfulness profile, which was characterized by relatively weaker nonjudgmental attention and awareness. The moderate mindfulness profile comprised 130 patients (40.1%), representing the largest subgroup and indicating that a substantial proportion of young and middle-aged lymphoma patients exhibit a moderate level of mindfulness. The remaining 99 patients (30.6%) constituted the high mindfulness profile, demonstrating strong mindful traits. Mindfulness, defined as the process of maintaining nonjudgmental, present-moment awareness, is known to influence psychosocial and physical function.10 However, its cultivation may be particularly challenging in this population. Chemotherapy, as the primary treatment for lymphoma, can induce neurotoxicity that directly damages the central nervous system, leading to cognitive impairments such as distractibility and diminished awareness.33 Furthermore, disease- and treatment-related fatigue and psychological distress can exacerbate such cognitive dysfunction.34 This combined burden likely undermines patients’ ability to sustain mindful awareness. Consequently, healthcare providers should develop personalized interventions based on the distinct mindfulness profiles identified in this study. Tailoring strategies to these specific profiles offers a targeted approach to enhancing mindfulness, which may in turn facilitate the recovery of social function.
Factors Associated with Mindfulness Latent Profiles
The present study identified specific demographic and clinical factors associated with distinct mindfulness profiles. Notably, female patients tended to be classified into profiles characterized by lower mindfulness. This observation may be linked to the established tendency for women to engage in more ruminative thinking and deeper processing of negative emotions, which can divert attentional resources away from present-moment experiences.35 Furthermore, middle-aged patients were more likely than their younger counterparts to belong to lower-mindfulness profiles. This difference could be related to known age-related changes in cognitive function, such as declining attentional control and potential shifts in prefrontal cortex activation patterns associated with mindfulness.36 The burden of caring for multiple children may exacerbate patients’ psychological stress, potentially scattering attentional resources and reducing their capacity for present-moment awareness.37 Furthermore, the persistent stress of long-term illness (duration > 12 months) can deplete cognitive-regulatory resources, contributing to executive dysfunction and a weakened ability to sustain mindful attention.38 For patients facing relapse or refractory disease, profound uncertainty and fear often dominate their experience, with high anxiety directing attention toward anticipated negative outcomes and further eroding present-moment awareness.39 Therefore, in designing interventions, healthcare professionals should consider these multifaceted stressors. Developing tailored strategies that address these specific challenges could more effectively enhance patients’ mindfulness and, consequently, improve their social function.
Differences in Social Function Deficits Across Mindfulness Latent Profiles
The findings reveal significant differences in social function deficit scores among patients with distinct mindfulness profiles, which indicates that mindfulness is a significant predictor of social function deficits. This result is consistent with previous research.40 Mindfulness, through its cultivation of nonjudgmental present-moment awareness, facilitates the regulation of negative emotions. This process alleviates anxiety and depression and improves overall quality of life,41 while also buffering the negative impact of such emotions on social behavior and aiding in the maintenance of social support networks.42 Collectively, these pathways contribute to the restoration of social function. Moreover, low mindfulness is commonly linked to impairments in attentional control.43 The resulting scarcity of attentional resources can directly compromise an individual’s ability to engage effectively in social interactions.44 Research indicates that mindfulness training enhances not only subjective well-being but also prosocial behavior, thereby promoting improved social function.45 Targeted interventions, such as Social Cognitive Training Based on Mindfulness (SocialMIND), are designed to restore social function by improving social cognitive abilities.46 Additionally, evidence-based therapies like Acceptance and Commitment Therapy (ACT)47 and Mindfulness-Based Stress Reduction (MBSR)48 effectively elevate mindfulness levels, which in turn positively influence patients’ social function.
The Mediating Role of Psychological Resilience in the Relationship Between Mindfulness Latent Profiles and Social Function Deficits
This study found that psychological resilience partially mediated the relationship between mindfulness profiles and social function deficits in young and middle-aged lymphoma patients, thereby supporting Hypothesis 2. This suggests that higher levels of psychological resilience may mitigate the adverse effects of low mindfulness on social function. The underlying mechanism could involve treatment-related cognitive decline, which may directly impair social function by reducing mindfulness and compromising an individual’s capacity to fulfill social roles.49 Meanwhile, mindfulness enhances individuals’ nonjudgmental awareness and acceptance of the present moment, reduces negative rumination, strengthens stress adaptation and psychological recovery, and ultimately improves psychological resilience.21 In addition, this study showed that psychological resilience was negatively correlated with social function deficits, which is consistent with the findings of Wang et al.19
The Meaning Mindfulness Theory emphasizes nonjudgmental awareness of present-moment experiences. Individuals with high psychological resilience can employ such awareness to regulate their emotions more effectively when facing stress and conflicts in social interactions, thereby maintaining favorable interpersonal relationships and social adaptation.40 Second, when confronted with adversity, individuals with high psychological resilience can adopt a mindful cognitive style to view difficulties positively and regard them as opportunities for growth and learning. This positive meaning-making process not only enhances individuals’ psychological adjustment but also significantly increases their willingness to participate socially, further promoting the favorable recovery and maintenance of social function.23 Therefore, healthcare professionals can help patients with social function deficits improve their social function by implementing interventions centered on psychological resilience. Positive Psychology Interventions (PPI) can enhance positive outcomes such as optimism and resilience in patients and effectively improve their social function.Jin et al50 found that PPI effectively improved life satisfaction among patients with permanent stomas by enhancing their resilience. Meanwhile, studies have shown that PPI can significantly increase resilience, reduce depression, and improve quality of life in cancer patients.51 In addition, attention and interpretation therapy, peer support interventions,52,53 and other similar approaches have also been shown to effectively improve psychological resilience, alleviate negative emotions, and consequently enhance the social function and quality of life of cancer patients.
Clinical Significance
This study identified distinct mindfulness subtypes among young and middle-aged lymphoma patients using LPA and found significant differences in social function deficits across these profiles, with the relationship between mindfulness profiles and social function deficits being partially mediated by psychological resilience. These results provide a solid clinical basis for precise intervention: profiling mindfulness can help identify high-risk patients for social function deficits, thereby informing targeted supportive care. Understanding the factors associated with distinct mindfulness profiles enables the development of personalized care strategies, while leveraging psychological resilience offers a novel intervention pathway to improve patients’ social function. Overall, the findings of this study support the development of integrated intervention models focused on mindfulness subtypes and resilience training, which may ultimately promote the holistic recovery of young and middle-aged lymphoma patients.
Limitations
This study has several limitations. First, its single-site design, conducted at a tertiary hospital in Urumqi, may limit the representativeness and generalizability of the findings regarding mindfulness, psychological resilience, and social function deficits. Second, the cross-sectional nature of this study precludes causal inference among these key variables. Third, the reliance on self-reported measures may introduce common method bias, despite the Harman’s single-factor test indicating that such bias was not a severe concern. Future research should expand to multi-center and more diverse samples to enhance generalizability, adopt longitudinal or experimental designs to establish causal relationships among the variables, and incorporate objective assessments to complement self-report data, thereby improving the validity and reliability of the findings.
Conclusions
This study identified three distinct mindfulness latent profiles among young and middle-aged lymphoma patients and found that profile membership was significantly influenced by gender, age, number of children, duration of illness, and current disease status. It further revealed significant differences in social function deficits across these profiles, with this relationship partially mediated by psychological resilience. This suggests that mindfulness may improve social function by enhancing psychological resilience. Therefore, healthcare professionals could integrate mindfulness training with resilience-building strategies to effectively improve patients’ social participation and function. Despite certain limitations, these findings provide a novel, profile-based perspective for personalized interventions aimed at addressing social function deficits in this patient population.
Data Sharing Statement
Due to our commitment to protecting participant anonymity and confidentiality, the dataset generated and analyzed in this study is not publicly available. However, it can be obtained from the corresponding author upon reasonable request.
Ethics Statement
This study was conducted in strict accordance with the ethical principles of the Declaration of Helsinki and was approved by the Ethics Committee of The Affiliated Cancer Hospital of Xinjiang Medical University (Approval No. K-2024213). Written informed consent was obtained from all participants prior to their inclusion in the study.
Acknowledgments
We are sincerely grateful to all the young and middle-aged lymphoma patients who participated in this study for their valuable contribution.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the “Tianshan Talents” Medical and Health High‑level Talent Training Program.
Disclosure
All authors of this study do not have any conflicts of interest.
References
1. Luo J, Craver A, Bahl K, et al. Etiology of non-Hodgkin lymphoma: a review from epidemiologic studies. J Nat Cancer Center. 2022;2(4):226–14. doi:10.1016/j.jncc.2022.08.003
2. Maddocks K. Novel targets in aggressive lymphoma. Hematology Am Soc Hematol Educ Program. 2020;2020(1):101–106. doi:10.1182/hematology.2020000093
3. Kang J, Chae H, Hong JY, et al. Distinct clinical characteristics at diagnosis in patients with late relapses compared with early relapses of diffuse large B-cell lymphoma treated with R-CHOP. Leuk Lymphoma. 2020;61(5):1119–1125. doi:10.1080/10428194.2019.1709831
4. Wang J, Liu X, Wu Y, et al. Association of overall survival benefit of radiotherapy with progression-free survival after chemotherapy for diffuse large B-cell lymphoma: a systematic review and meta-analysis. J Natl Cancer Cent. 2024;4(3):249–259. doi:10.1016/j.jncc.2024.04.002
5. Drabbe C, Coenraadts ES, van Houdt WJ, et al. Impaired social functioning in adolescent and young adult sarcoma survivors: prevalence and risk factors. Cancer. 129(9):1419–1431. doi:10.1002/cncr.34689
6. Vena JA, Copel LC. Cancer survivorship and quality of life outcomes of adolescents and young adults with lymphoma: an integrative review. Eur J Oncol Nurs. 2021;52:101948. doi:10.1016/j.ejon.2021.101948
7. Patterson JM, Lu L, Watson LJ, et al. Associations between markers of social functioning and depression and quality of life in survivors of head and neck cancer: findings from the head and neck cancer 5000 study. Psychooncology. 2022;31(3):478–485. doi:10.1002/pon.5830
8. Anthony SJ, Robertson T, Selkirk E, et al. The social impact of early psychological maturity in adolescents with cancer. Psychooncology Mar. 2019;28(3):586–592. doi:10.1002/pon.4982
9. Wang F, Gao Y, Han Z, et al. A systematic review and meta-analysis of 90 cohort studies of social isolation, loneliness and mortality. Nat Hum Behav. 2023;7(8):1307–1319. doi:10.1038/s41562-023-01617-6
10. Kabat-Zinn J. Mindfulness-based interventions in context: past, present, and future. In: Clinical Psychology: Science & Practice. Vol. 10. Blackwell Publishing Ltd; 2003:144–156.
11. Garcia ACM, Camargos Junior JB, Sarto KK, et al. Quality of life, self-compassion and mindfulness in cancer patients undergoing chemotherapy: a cross-sectional study. Eur J Oncol Nurs. 2021;51:101924. doi:10.1016/j.ejon.2021.101924
12. Morin L, Laurin JC, Doucerain M, Grégoire S. Dyadic association between new parents’ mindfulness and relationship satisfaction: mediating role of perceived stress. J Soc Pers Relat. 2023;40(5):1448–1470. doi:10.1177/02654075231156404
13. Long HC, An HM, Dung PTP, Quy NLD. Mindfulness practice and work performance: the mediating role of emotional intelligence and psychological capital. Brain Behav. 2025;15(1):e70291. doi:10.1002/brb3.70291
14. Feruglio S, Panasiti MS, Crescentini C, Aglioti SM, Ponsi G. The impact of mindfulness meditation on social and moral behavior: does mindfulness enhance other-oriented motivation or decrease monetary reward salience? Front Integr Neurosci. 2022;16:963422. doi:10.3389/fnint.2022.963422
15. Al‐Hammouri MM, Rababah JA, Alfurjani AM. Factors influencing mindfulness among Jordanian nurses: a cross-sectional study. J Nurs Manag. 2022;30(7):3386–3392. doi:10.1111/jonm.13797
16. Mori M, Krumholz HM, Allore HG. Using latent class analysis to identify hidden clinical phenotypes. JAMA. 2020;324(7):700–701. doi:10.1001/jama.2020.2278
17. Bui MV, McInnes E, Ennis G, Foster K. Resilience and mental health nursing: an integrative review of updated evidence. Int J Ment Health Nurs. 2023;32(4):1055–1071. doi:10.1111/inm.13132
18. Bozikas VP, Parlapani E, Ntouros E, et al. Resilience predicts social functioning in clinically stable patients with bipolar disorder. J Nerv Ment Dis. 2018;206(7):567–574. doi:10.1097/nmd.0000000000000843
19. Wang M, Xu Y, Yang BX, Luo D, Hou H, Liu Q. A longitudinal study of resilience and social function in patients with colorectal cancer and stomas. J Psychosom Res. 2025;189:112013. doi:10.1016/j.jpsychores.2024.112013
20. Mei X, Mei R, Li Y, et al. Trait mindfulness, resilience, self-efficacy, and postpartum depression: a dominance analysis and serial-multiple mediation model. Psychol Res Behav Manag. 2025;18:743–757. doi:10.2147/prbm.S509684
21. Zhang J, Mao Y, Wang Y, Zhang Y. The relationship between trait mindfulness and resilience: a meta-analysis. Personal Ment Health. 2023;17(4):313–327. doi:10.1002/pmh.1581
22. Garland EL, Farb NA, Goldin P, Fredrickson BL. Mindfulness broadens awareness and builds eudaimonic meaning: a process model of mindful positive emotion regulation. Psychol Inq. 2015;26(4):293–314. doi:10.1080/1047840x.2015.1064294
23. Garland EL, Fredrickson BL. Positive psychological states in the arc from mindfulness to self-transcendence: extensions of the mindfulness-to-meaning theory and applications to addiction and chronic pain treatment. Curr Opin in Psychol. 2019;28:184–191. doi:10.1016/j.copsyc.2019.01.004
24. Hanley AW, de Vibe M, Solhaug I, et al. Modeling the mindfulness-to-meaning theory’s mindful reappraisal hypothesis: replication with longitudinal data from a randomized controlled study. Stress Health. 2021;37(4):778–789. doi:10.1002/smi.3035
25. Tein J-Y, Coxe S, Cham H. Statistical power to detect the correct number of classes in latent profile analysis. Struct Equation Model. 2013;20(4):640–657. doi:10.1080/10705511.2013.824781
26. Brown KW, Ryan RM. The benefits of being present: mindfulness and its role in psychological well-being. J Pers Soc Psychol. 2003;84(4):822–848. doi:10.1037/0022-3514.84.4.822
27. Chen SY, Cui H, Zhou RL, Jia YY. Revision and psychometric testing of the Mindful Attention Awareness Scale (MAAS). Chin J Clin Psychol. 2012;20(2):148–151.
28. Connor KM, Davidson JRT. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
29. Campbell‐Sills L, Stein MB. Psychometric analysis and refinement of the connor–davidson resilience scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019–1028. doi:10.1002/jts.20271
30. Ye ZJ, Liu ML, Luo DM, et al. Validity and reliability of the 10-item Connor-Davidson Resilience Scale among parents of pediatric cancer patients. Nurs Res. 2016;30(33):4118–4122. doi:10.3969/j.issn.1009-6493.2016.33.008
31. Zhang MY. Manual of Mental Status Rating Scales. Changsha: Hunan Science & Technology Press; 1998:252.
32. Podsakoff PM, MacKenzie SB, Lee J-Y, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
33. Fayette D, Juríčková V, Kozák T, et al. Cognitive impairment associated with Hodgkin’s lymphoma and chemotherapy. 2023(797):137082. doi:10.1016/j.neulet.2023.137082
34. Ekels A, Oerlemans S, Schagen SB, et al. The course of self-perceived cognitive functioning among patients with lymphoma and the co-occurrence with fatigue and psychological distress. J Cancer Surviv. 2025;19(1):183–196. doi:10.1007/s11764-023-01458-2
35. Conradi HSW, Nguyen T, Lawal OA, Carlson LE. Mindfulness and psychosocial symptoms in people with cancer: testing rumination and experiential avoidance as mediators, and sex as a moderator. Glob Adva Integr Med Health. 2025;14:27536130251367051. doi:10.1177/27536130251367051
36. Shenoy S, Khandekar P, Sathe A. Young and middle-aged adults differ in neural correlate of sustained attention: a fNIRS study. Curr Aging Sci. 2021;14(3):201–213. doi:10.2174/1874609814666210716111022
37. Hong X, Zhu W, Zhao S. Type of family support for infant and toddler care that relieves parenting stress: does the number of children matter? Healthcare. 2023;11(3). doi:10.3390/healthcare11030421
38. Girotti M, Bulin SE, Carreno FR. Effects of chronic stress on cognitive function - From neurobiology to intervention. Neurobiol Stress. 2024;33:100670. doi:10.1016/j.ynstr.2024.100670
39. Wang C, Wu Y, Hu R. Managing uncertainty: a grounded theory study of restoring normality in young and middle-aged patients with lymphoma. Int J Nurs Sci. 2025;12(4):393–400. doi:10.1016/j.ijnss.2025.06.008
40. Wang Y, Zheng Z, Duan X, Li M, Li Y. The relationship between mindfulness and social adaptation among migrant children in china: the sequential mediating effect of self-esteem and resilience. Int J Environ Res Public Health. 19(23). doi:10.3390/ijerph192316241
41. Yin L. Effects of mindfulness-based stress reduction training on the negative emotions and social functioning of patients with laryngeal cancer. Clin Transl Oncol Apr. 2025;27(4):1760–1766. doi:10.1007/s12094-024-03622-1
42. Cooper DJ, Eckstein J, Sidiqi B, et al. Trait mindfulness and social support predict lower perceived stress burden in patients undergoing radiation therapy. Adv Radiat Oncol. 2024;9(8):101546. doi:10.1016/j.adro.2024.101546
43. Liu Y, Hou Y, Quan H, et al. Mindfulness training improves attention: evidence from behavioral and event-related potential analyses. Brain Topogr. 2023;36(2):243–254. doi:10.1007/s10548-023-00938-z
44. Achanccaray D, Sumioka H. Analysis of physiological response of attention and stress states in teleoperation performance of social tasks. Annu Int Conf IEEE Eng Med Biol Soc. 2023;2023:1–4. doi:10.1109/embc40787.2023.10340007
45. Zhou W, McLellan R. The effectiveness of taught, self-help mindfulness-based interventions on Chinese adolescents’ well-being, mental health, prosocial and difficult behavior, and coping strategy. Appl Psychol Health Well Being. 2024;16(3):1024–1045. doi:10.1111/aphw.12517
46. Mediavilla R, Muñoz-Sanjose A, Rodriguez-Vega B, et al. People with psychosis improve affective social cognition and self-care after a mindfulness-based social cognition training program (SocialMIND). Psychiatr Rehabil J. 2021;44(4):391–395. doi:10.1037/prj0000466
47. Latella D, Marafioti G, Formica C, et al. The role of acceptance and commitment therapy in improving social functioning among psychiatric patients: a systematic review. Healthcare. 13(13). doi:10.3390/healthcare13131587
48. Victorson D, Morgan T, Kutikov A, et al. Mindfulness-based stress reduction for men on active surveillance for prostate cancer and their spouses: design and methodology of a randomized controlled trial. Contemp Clin Trials. 2023;125:107059. doi:10.1016/j.cct.2022.107059
49. Franco-Rocha OY, Mahaffey ML, Matsui W, Kesler SR. Remote assessment of cognitive dysfunction in hematologic malignancies using web-based neuropsychological testing. Cancer Med. 2023;12(5):6068–6076. doi:10.1002/cam4.5331
50. Jin Y, Wang Y, Ma H, Tian X, Wang H. The efficacy and mechanism of positive psychological intervention on well-being for colostomy patients: a randomized controlled trial. Support Care Cancer. 2022;30(7):5747–5757. doi:10.1007/s00520-022-06951-5
51. Tian X, Zhou X, Sun M, et al. The effectiveness of positive psychological interventions for patients with cancer: a systematic review and meta-analysis. J Clin Nurs. 2024;33(9):3752–3774. doi:10.1111/jocn.17358
52. Lin C, Diao Y, Dong Z, Song J, Bao C. The effect of attention and interpretation therapy on psychological resilience, cancer-related fatigue, and negative emotions of patients after colon cancer surgery. Ann Palliat Med. 2020;9(5):3261–3270. doi:10.21037/apm-20-1370
53. Aizpurua-Perez I, Arregi A, Gonzalez D, et al. A randomized controlled trial of the effectiveness of a one-to-one peer support intervention on resilience, social support, and salivary cortisol in recently diagnosed women with breast cancer. Eur J Oncol Nurs. 2024;71:102616. doi:10.1016/j.ejon.2024.102616
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.