")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Mindfulness and Chronic Musculoskeletal Pain: An Umbrella Review
Authors Cardle P , Kumar S , Leach M , McEvoy M , Veziari Y
Received 18 November 2022
Accepted for publication 23 December 2022
Published 28 February 2023 Volume 2023:16 Pages 515—533
DOI https://doi.org/10.2147/JMDH.S392375
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Paul Cardle,1 Saravana Kumar,1 Matthew Leach,2 Maureen McEvoy,1 Yasamin Veziari1
1Allied Health and Human Performance Unit, The University of South Australia, Adelaide, SA, Australia; 2National Centre for Naturopathic Medicine, Southern Cross University, Lismore, New South Wales, Australia
Correspondence: Paul Cardle, Email [email protected]
Background: Chronic musculoskeletal pain (CMSP) disorders are a leading cause of disability globally, affecting up to one in three people. Mindfulness-based interventions (MBI) have become a popular treatment for CMSP. The aim of this umbrella review was to synthesise the best available research evidence for the effectiveness of MBI for adults with CMSP.
Methods: Eight databases were searched from inception to 30th June 2021 for systematic reviews that examined the use of MBI in CMSP (pain experienced > 3 months) in adult populations. Two reviewers independently conducted screening and selection, data extraction, and assessment of methodological quality using The Assessing the Methodological Quality of Systematic Reviews tool (AMSTAR 2). Outcomes examined were pain, sleep quality, depression, quality of life, physical functioning, and mindfulness. Furthermore, definitions of mindfulness, and intervention parameters (mindfulness practices used, length, frequency of sessions, duration) were also reported.
Results: Nineteen systematic reviews (n = 1 rated high quality, n = 1 moderate quality, n = 2 low quality and n = 15 critically low quality) examining 194 primary studies met the review criteria. Although some promising evidence was identified for the use of MBI in CMSP, the general low quality and widespread heterogeneity of included SRs and made it difficult to reach a definitive conclusion. Differences in results and outcomes amongst systematic reviews that, in many cases, had a high overlap of included RCTs, suggests fundamental differences in critical design elements that make data difficult to compare.
Conclusion: This umbrella review found mixed results on the effectiveness of MBI for the management of CMSP across a range of outcomes (pain, sleep quality, depression, quality of life, physical functioning, mindfulness). Definitions of MBI varied as did parameters, which may have contributed to these mixed results. More rigorous research with stringent MBI protocols is required.
Keywords: mindfulness, chronic pain, musculoskeletal disorders, chronic musculoskeletal pain, systematic reviews
Background
Musculoskeletal disorders (MSD) are one of the leading causes of disability globally, second only to mental health disorders1 to which MSD are also a contributor2. Musculoskeletal disorders relate to conditions of the joints, bones, muscles, spine, and regional pain areas and are comprised of over 150 conditions, typically categorised by pain and disorders of physical functioning.2 For the purposes of this review, chronic musculoskeletal pain (CMSP) refers to any chronic MSD that causes persistent or recurring pain lasting three months or longer. It is estimated that 1.17 billion people suffer from CMSP globally, with a greater prevalence reported in higher income countries;2 although, both prevalence and burden of CMSP are likely to be underestimated.1
The international association for the study of pain defines pain as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage”.3 This definition is supported by a growing body of knowledge that suggests chronic pain may have multiple contributing factors that include elements relating to the three domains (biological, psychological, social) of the biopsychosocial model.4 The biopsychosocial approach to disease examines how these elements of biology, psychology, and sociology intersect to affect the experiences and presentations of disorders such as chronic pain.5
Several biopsychosocial interventions have been trialled for the management of CMSP, with varying degrees of success.6 One intervention that has shown promise in many aspects associated with CMSP is mindfulness,7–9 a type of meditation practice that has its origins in Buddhism.10 Mindfulness has been defined as “the awareness that arises from paying attention, on purpose, in the present moment and non-judgmentally”.11 There is evidence to indicate that mindfulness-based interventions (MBI) may positively impact a range of biological, psychological, and social outcomes. For example, some research has shown that MBI may improve immune function, increase regional brain grey matter density,12 support early childhood self-regulation, and reduce early childhood anxiety leading to the development of greater moment-to-moment awareness, and improved socioemotional competence.13 There is also evidence supporting the use of MBI for diverse health conditions such as anxiety, depression, and chronic pain.14–16
There have been many systematic reviews examining the effectiveness of MBI for CMSP. Although several of these reviews reported positive results supporting the use of MBI, other reviews have been inconclusive or have shown no effect.17–19 For example, while seemingly investigating the same interventions for the same conditions, Chiesa et al32 reported finding no benefits for the use of MBI for pain, Cramer18 et al reported mixed findings and Veehof et al43 reported a clear benefit to pain outcomes. The inconsistent findings warrant further investigation to determine whether the conflicting results can be explained by differences in methodological design, definitions of chronic pain and mindfulness, and the application, and practice of MBI. These inconsistencies can pose a barrier to evidence implementation22 which could in turn, delay improvements in clinical practice and patient outcomes. Gaining further clarification of the parameters and methodologies to explore inconsistencies in the effectiveness may add greater confidence for clinicians in where and how mindfulness interventions may be most effectively included in management. This umbrella review aims to address this barrier by synthesising the findings of systematic reviews to answer two research questions:
- What parameters and methodologies are used within systematic reviews to investigate the effectiveness of MBI for CMSP?
- What is the evidence of the effectiveness of MBI for the treatment of CMSP and its sequelae?
Methods
Design
This was an umbrella review of systematic reviews investigating the effectiveness of MBI for CMSP. The review protocol was registered with Prospero (CDR number CRD42021246913).
Participants
This review included adults (aged ≥18 years) suffering from CMSP. For the purposes of this umbrella review, chronic pain was defined as pain persisting for >3 months, beyond the normal tissue healing time.23 Participants aged <18 years, with acute pain, and types of pain not included in the World Health Organisation (WHO) classification of CMSP (eg, pelvic or cancer pain) were excluded.
Types of Exposure
Interventions needed to be a form of mindfulness training and/or practice specifically used to manage pain. This could include, but was not necessarily limited to, mindfulness-based stress relief (MBSR), acceptance and commitment therapy (ACT), mindfulness-based cognitive therapy (MBCT), traditional or spiritual mindfulness practice, secular mindfulness practices, Yoga, Tai qi (Tai chi) and Qigong. Other forms of meditation and practices, such as compassion-based interventions, analytical type meditation, and cognitive behavioural therapy (CBT) were excluded. Mindfulness used for the purposes of improving academic or physical performance (eg, athletics) was also excluded.
Context
MBI that were taught/practiced within a health care, religious or traditional setting were included; practitioner must have been trained in mindfulness practice(s) to be included. Mindfulness practiced in an education or athletic context, (eg, martial arts clubs, primary schools) were excluded.
Comparators
Eligible comparators included waitlist control, education support group, no treatment, active treatment, relaxation, and stretching.
Outcomes
Outcomes examined in this review were pain, sleep quality, depression, quality of life, physical functioning, mindfulness, definitions of mindfulness, and intervention parameters (eg, mindfulness practices used, duration of intervention, frequency of sessions).
Types of Studies
The review included systematic reviews, with and without meta-analyses. For the purposes of this research, systematic reviews were defined as any review that uses explicit, systematic methodology to collate evidence that fits pre-specified eligibility criteria in order to answer a specific research question.24
Search Strategy
Databases
A preliminary search was initially conducted to determine whether there were any systematic reviews on this topic. Initial keywords were identified following analysis of the text words contained in the title and abstract, and of the index terms to describe relevant reviews. The following electronic databases were searched from inception to 30th June 2021; MEDLINE, EMBASE, EMCARE (OVID), PsycINFO, the Cochrane Library, and the PROSPERO register. A grey literature search of non-commercially published literature or reports was undertaken using ProQuest Dissertations, Scopus, and Google Scholar. The Google search engine was also searched (up to the first 10 pages). No search limits were applied. Secondary searching of reference lists in all included studies was also undertaken. Table 1 details the search terms used for the search in the Medline database, on which all other searches were based.
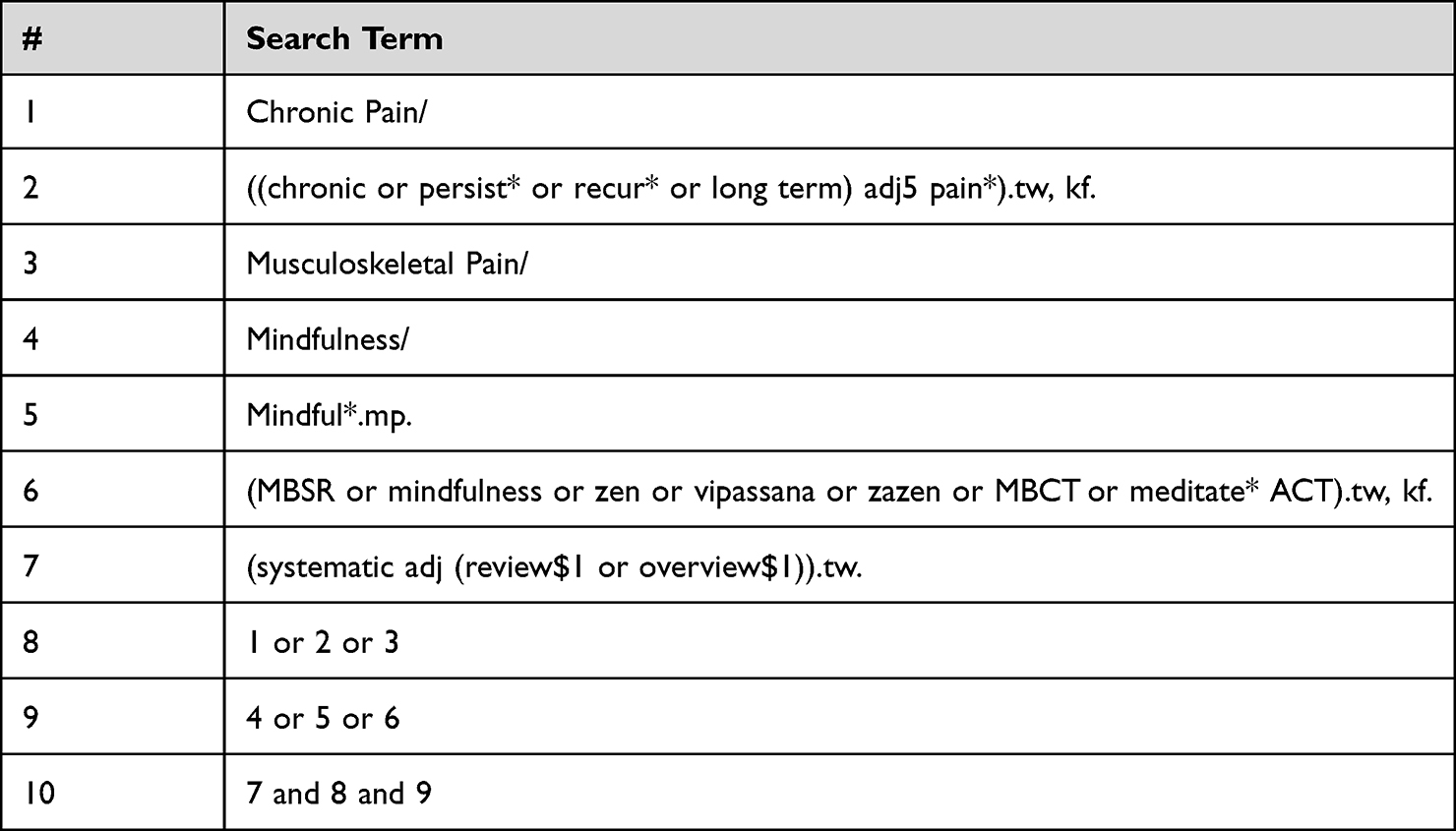 |
Table 1 Medline Search Terms |
Selection Process
The initial search was undertaken by two reviewers (PC, YV). Search results were initially imported into EndNote™25 as a referencing management tool. Citations were then exported into Covidence™26 to assist with citation screening and deduplication. Title/abstract and full-text screening were undertaken by two reviewers (PC, YV), with the arbitration of disputes carried out by a third reviewer (SK, ML, MM).
Methodological Quality Assessment
The AMSTAR 2 (Assessing the Methodological Quality of Systematic Reviews) was used to critically appraise the included systematic reviews. The AMSTAR 2 tool uses a confidence rating score of sixteen items from high, moderate, low, and critically low. Higher scores on this critical appraisal tool are indicative of higher methodological quality. Two independent reviewers (PC, YV) critically appraised each included study and then compared their results. Disagreements between reviewers were discussed until consensus was reached; any disagreements that could not be resolved were discussed, and determined by the rest of the review team (SK, ML, MM).
Data Extraction
A customised data extraction form was developed à priori and conducted in duplicate in accordance with the JBI Manual for Evidence Synthesis.27 The form was also pilot tested on three studies. The extraction form was designed to capture the following data from each included study: author, date, country, study design, participants, sample size, description of intervention/mindfulness practice, description of comparator, parameters of mindfulness interventions and comparator, outcomes, context, effectiveness of MBI for the treatment of CMSP, definitions of mindfulness, and definitions of chronic pain. Two reviewers (PC, YV) independently conducted data extraction of all the included reviews and compared the results. Disagreements between reviewers were discussed and any conflicts were resolved through consensus. These findings were then shared with the rest of the review team (SK, ML, MM) and any outstanding disagreements were resolved as team. This process ensured the entire review team had oversight of the data extraction process and final decisions were made as a team.
Data Synthesis
Given the nature of the review (umbrella review), a meta-analysis was not feasible and hence a descriptive synthesis was undertaken using summary tables of review characteristics and findings. Data were synthesised into one of three categories based on the strength of the evidence for each of the six outcomes: pain, quality of life (QoL), depression, sleep quality, physical functioning, and mindfulness measures. A “Green” classification was indicative of positive findings across all included studies (within the systematic review), including all comparators (both inactive and active) and at all time points. A “Red” classification indicated that all included studies found no effects or negative effects. An “Amber” classification represented mixed findings, where some studies reported positive findings, and some studies reported inconclusive findings, negative findings, or no significant difference between groups. This included reviews where positive results were found when compared with inactive controls and no difference was found when compared with active comparators. This also included differences in findings at different time points.
As a means of bringing together these diverse bodies of research, we also used the National Health and Medical Research Council (NHMRC) FORM framework.28 This framework was chosen as it has been previously used in other umbrella reviews,29 and it provides a well-established, consistent, and transparent process for data synthesis. The FORM framework comprises five components that are used to formulate and grade recommendations. These components include: (1) evidence base, (2) consistency, (3) clinical impact, (4) generalisability, and (5) applicability (for the purpose of this review, the applicability component was excluded as this review was not confined to Australian contexts). Each component could be rated as follows: A (excellent), B (good), C (satisfactory) or D (poor). The components were rated by two reviewers (PC and SK) and discussed until consensus was reached on each of the component scores and an overall recommendation.
Results
Search Findings
A total of eight-hundred and thirty-two records were identified from databases and the reference lists of included records. Of these, one-hundred and forty-eight duplicates were removed in Endnote™, and twenty-nine duplicates were removed in Covidence™. Five-hundred and ninety-six records were excluded at the title and abstract screening stage. Full text review of the remaining fifty-nine articles resulted in the exclusion of a further forty articles. Reasons for exclusion included: incorrect study design (n = 9), incorrect population (n = 17), incorrect intervention (n = 8), and duplicates (n = 6). As a result, nineteen systematic reviews17–19,30–45 were included in this umbrella review. Figure 1 provides an overview of the study selection process.
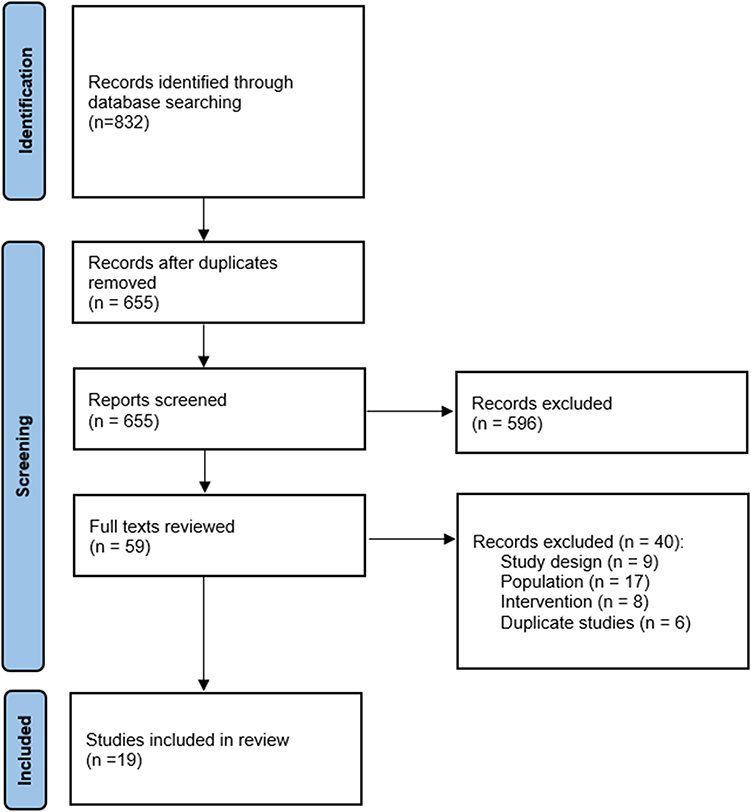 |
Figure 1 PRISMA flowchart. |
Review Characteristics and Description of Included Studies
The systematic reviews originated from 10 countries and were published between 2011 and 2021. Reviews included only adult populations (eg, aged >18 years). A broad range of chronic pain conditions were included within the umbrella category of CMSP such as, chronic low back pain, chronic back pain, fibromyalgia, headache, rheumatoid arthritis, osteoarthritis, failed back surgery syndrome, spine or joint pain, migraine headache, somatization, functional somatic syndrome, and temporomandibular disorder. Two hundred and seventeen randomized controlled trials were included in this review, and one hundred and twelve of these were unique and not repeated across the included systematic reviews. In nine reviews, there was a meta-analysis of at least one included outcome.
Methodological Quality of Included Reviews
Overall, the confidence rating of the critical appraisal scores were critically low (n = 15), low (n = 2), moderate (n = 1) and high (n = 1). Seven reviews did not report a research protocol, partial protocols were reported by eight reviews, and only four reviews reported complete protocols. The only criterion that was met by all included systematic reviews was the inclusion of a complete PICO question. By contrast, fifteen systematic reviews did not report inclusion criteria, eleven studies did not conduct a comprehensive search, eight systematic reviews conducted only a partial search, and fourteen systematic reviews did not report the impact of publication bias. Table 2 provides an overview of the AMSTAR 2 critical appraisal scores for the 19 included systematic reviews.
 |
Table 2 Methodological Quality of the Included Systematic Reviews |
Definitions, Interventions, and Parameters
A wide variety of unique definitions for mindfulness were utilised across all included systematic reviews, with few similarities. Six reviews18,32,33,39,40,44 did not provide a complete definition of mindfulness but did describe the included MBI. Four reviews19,30,38,45 did not report a definition. Where definitions provided an outline of included MBI in the reviews, there was a large variation. Many reviews opted to approach mindfulness from a complementary and alternative medicine perspective, with the inclusion for example of Tai chi and Qigong, while others adopted a more conventional approach by focusing on more clearly defined interventions such as MBSR and ACT. Table 3 summarises the definitions of mindfulness reported in the included systematic reviews.
 |
Table 3 Definitions for Mindfulness Reported in the Included Systematic Reviews |
Across all nineteen included reviews, there were no standardised interventions; and even for MBI such as MBSR, there were wide variations reported across reviews. Table 4 summarises the specific parameters of the interventions reported in each of the nineteen included systematic reviews. Fourteen reviews17,18,31–38,40,41,43,45 used MBSR alone as a treatment or in combination with at least one other treatment. Other MBI reported across multiple reviews included MBCT (n = 5 reviews) and ACT (n = 3 reviews). Where reported, session lengths varied from 1 to 3.5 hours, the number of sessions varied from 6 to 12, the frequency of sessions was either weekly or bi-weekly, and the duration of the intervention ranged from 1 day to 34 weeks.
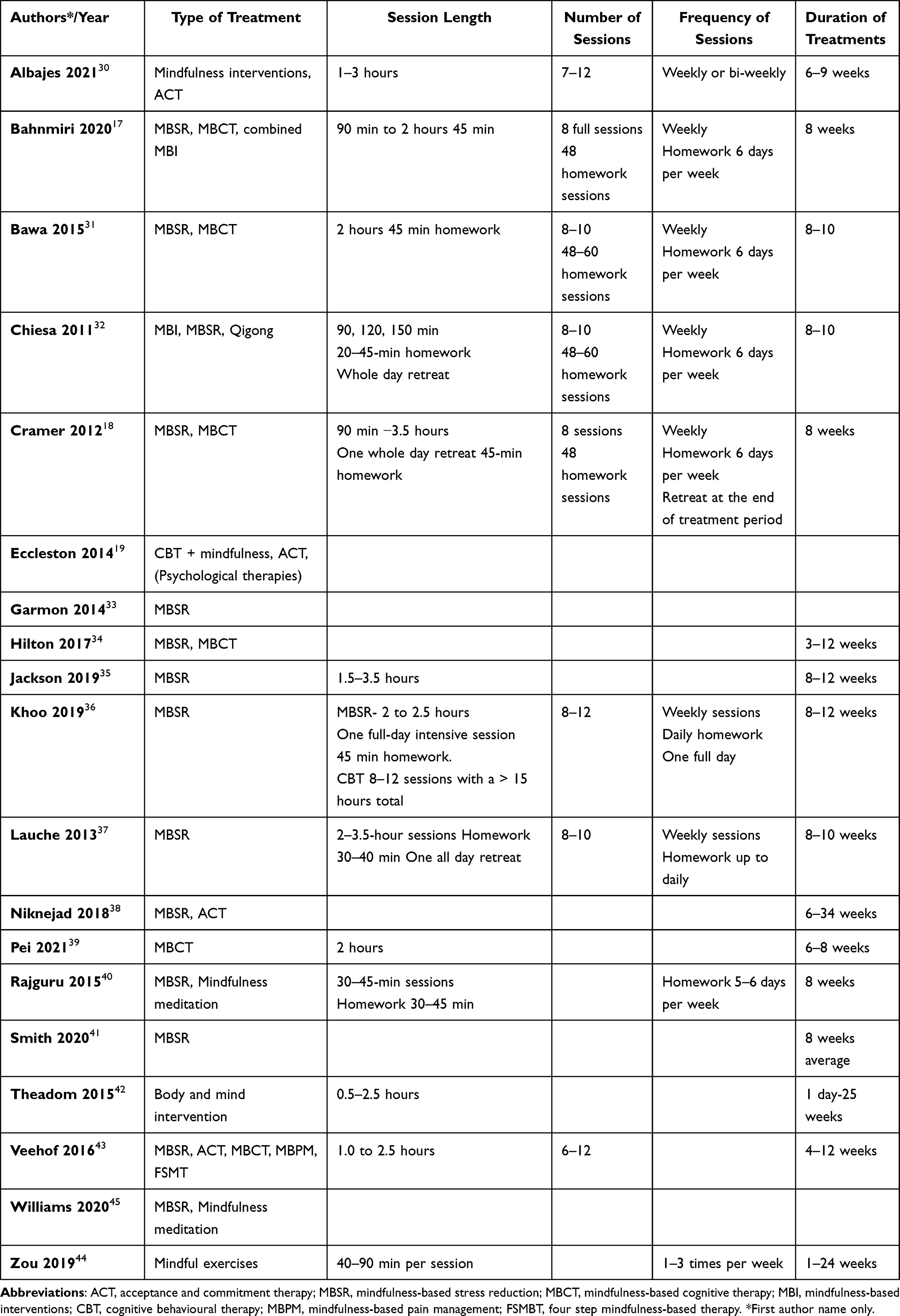 |
Table 4 Parameters of the Interventions Reported in the Included Systematic Reviews |
NHMRC FORM Framework
The findings from the NHMRC FORM framework,28 which was used to formulate and grade the results, are described in Table 5. These results should be interpreted with caution as several methodological concerns were noted, thereby lowering the grade of the evidence base. The fifth element of the FORM framework, applicability, was not used as the scope of this review was international and not restricted to an Australian population.28
 |
Table 5 NHMRC FORM Framework Analysis |
Evidence of Effectiveness
A range of outcome measures were used to determine the impacts of MBI on CMSP. Table 6 highlights the variability of six outcomes (pain, quality of life, depression, sleep quality, physical functioning, and mindfulness measures) measured in the nineteen included studies. While some studies used comparable instruments to measure outcomes, the constructs and data analysis methods were heterogeneous. Pain was measured across eighteen systematic reviews. Of these, six systematic reviews30,32,33,39,40,42 demonstrated negative outcomes, six17–19,31,34,36 demonstrated inconclusive outcomes and six37,38,41,43–45 reported positive outcomes. With regard to QoL, five systematic reviews18,30,31,37,43 showed inconclusive outcomes, two19,33 reported negative outcomes and three32,34,41 demonstrated positive outcomes. Depression was measured across ten systematic reviews. There were two studies each that reported negative31,37 and positive outcomes,34,43 and six systematic reviews30,32,33,36,39,41 that showed inconclusive outcomes. Sleep quality was measured across six systematic reviews, with three demonstrating negative outcomes31,37,42 and three reporting positive outcomes.18,30,33 Physical functioning was measured by eight systematic reviews. Of these, three showed negative35,36,42 and positive outcomes18,30,33 and in two reviews,31,32 the outcomes were inconclusive.
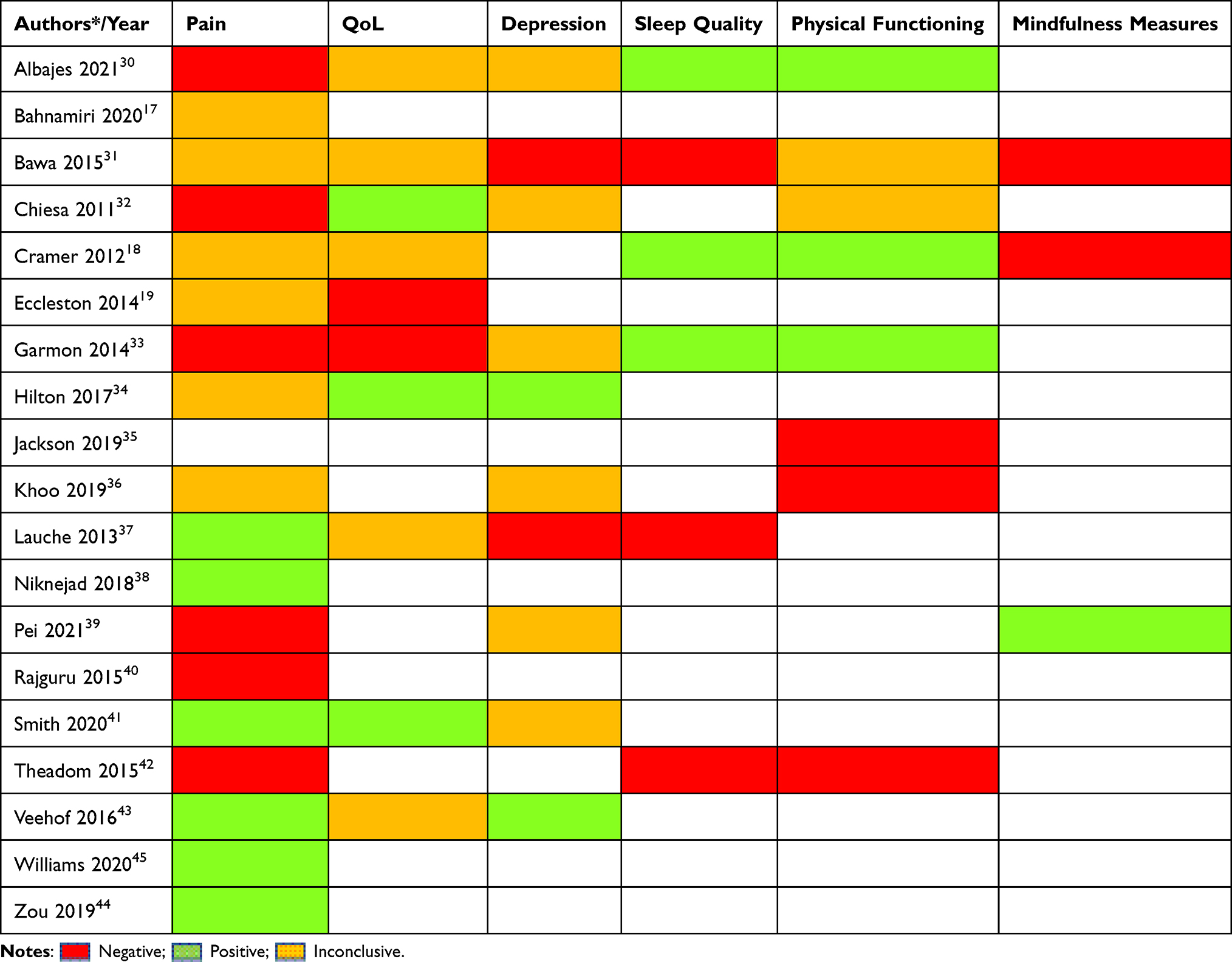 |
Table 6 Overview of Outcomes Reported in the Included Systematic Reviews |
Pain
Eighteen reviews17–19,30–34,36–45 measured the effect of MBI on various domains of pain, including pain intensity, perceived pain, pain interference, and pain acceptance. Studies that formed part of these reviews measured pain using psychometrically sound outcome measures (such as the Brief Pain Inventory and McGill Pain Questionnaire). Lauche et al37 (five studies), Niknejad et al38 (two studies), Smith and Langen41 (twelve studies), Veehof et al43 (twenty-eight studies), and Zou et al44 (seventeen studies), all reported that MBI were beneficial for pain. The studies included in these reviews collectively provided evidence of benefit. In addition to this, the review by Williams et al45 (six studies related to mindfulness) found that psychological interventions, of which mindfulness was an intervention, were beneficial in reducing pain. However, outcome data specific for mindfulness were not provided. Smith and Langen41 found that MBSR may provide relief from pain in the long-term. While the findings of Lauche et al37 were similar, these were confined to short-term relief in people with fibromyalgia. The findings by Zou et al44 also suggested there were long-term benefits for chronic low back pain when using mindful exercises (Tai Chi, Qigong, Yoga) compared to other non-active and active controls. Veehof et al43 reported a small effect size for pain intensity, and a moderate effect size for pain interference, compared with a waitlist, education/support group, CBT, or relaxation control. Niknejad et al38 also found statistically significant positive results in pain intensity and pain interference compared with a waitlist and a health education control.
These findings are in stark contrast to reviews by Albajes et al30 (eleven studies), Chiesa et al32 (seven studies), Garmon et al33 (eleven studies), Pei et al39 (seven studies), Rajguru et al40 (six studies), and Theadom et al42 (three studies), who each reported no benefits of MBI for CMSP. While individual studies within these reviews may have reported some benefits, which may have contributed to small gains, collectively the authors highlight lack of sufficient and robust evidence to support MBI. For example, Albajes et al30 focused on psychological therapies for fibromyalgia and found eight studies that related to MBI. Of these, four studies assessed pain as an outcome with only one reporting positive outcomes.
Six reviews reported mixed results for the effectiveness of MBI for pain, including Bahnamiri et al17 (nine studies), Bawa et al31 (eight studies), Cramer et al18 (three studies), Eccleston et al19 (two studies), Hilton et al34 (thirty-eight studies), and Khoo et al36 (sixteen studies). Results were often mixed as MBI were reported to have an impact on one aspect of pain but not on another (such as a positive impact on perceived pain but no impact on pain intensity). The review by Bawa et al31 found a positive effect of MBI on perceived pain but no evidence of any benefit on pain intensity. In some instances, MBI were no better than other interventions (such as CBT), as highlighted by Khoo et al.36 In one review, Eccleston et al19 found that internet-delivered psychological therapies, which included MBI, reduced headache pain and non-headache related pain with a small effect size, although it was reported that there was insufficient evidence to make a firm conclusion. Similarly to Williams et al,45 we found that data specific to MBI was not able to be extracted separately. For these reasons, we found that Eccleston et al19 provided mixed evidence. The review by Bahnamiri et al17 reported positive benefits of MBI for chronic low back pain and found MBI reduced pain intensity in both the short-term and long-term when compared to inactive controls. However, Bahnmiri et al17 also showed that MBI reduced pain intensity as efficiently as CBT and there were no statistically significant differences between the two approaches; accordingly, these findings provided mixed evidence. The conflicting nature of the evidence-base, coupled with concerns about methodological quality and heterogeneity within the primary research, means an unequivocal finding about the effectiveness of MBI on pain cannot be made. Collectively, the literature provides mixed evidence regarding the effectiveness of MBI for pain.
Quality of Life
Ten reviews18,19,30–34,37,41,43 measured the effectiveness of MBI on Quality of life (QoL). Studies that formed these reviews measured QoL using various psychometrically tested outcome measures, such as the Short-form health survey (SF-36), and EuroQoL. Albajes et al30 identified that MBI might be beneficial for QoL-related outcomes. Of the seven studies included in the review by Albajes et al,30 six studies found significant benefits from the intervention, and one found a non-significant difference between the three treatment groups: MBSR, treatment as usual and Multicomponent intervention (FibroQoL). Bawa et al31 also found mixed results regarding the impact of MBI on QoL and concurred with Albajes et al30 that the effect of MBI was generally found to be equivalent to an active comparator. Overall, Albajes et al,30 Bawa et al,31 Cramer et al,18 Lauche et al,37 and Veehof et al43 all provided mixed or conflicting evidence of benefit. By contrast, Chiesa et al,32 Hilton et al,34 and Smith and Langen41 all reported significant improvements in QoL when MBI were compared to both active and inactive comparators. These comparators included treatment as usual, support groups, education, stress management, and waitlist controls. On the other hand, Eccleston et al,19 and Garmon et al,33 both reported that there was insufficient evidence to suggest that MBI improve QoL in people living with chronic pain. Collectively, the literature provides mixed evidence regarding the effectiveness of MBI on QoL.
Depression
Ten reviews30–34,36,37,39,41,43 measured the effectiveness of MBI for depression. Studies that formed these reviews measured depression using various psychometrically tested outcome measures, such as the Hospital Anxiety and Depression Scale, and the Beck Depression Inventory. Hilton et al,34 and Veehof et al,43 both identified that MBI were beneficial for depression as the studies included in the reviews collectively provided evidence of benefit. The review by Hilton et al34 reported positive effects when comparing MBI with different comparators (eg treatment as usual, support, education, stress management, waitlist control), finding that MBI significantly lowered depression scores, both post treatment and later after follow-up. This was in contrast to reviews by Bawa et al31 (6 studies), and Lauche et al37 (five studies), that collectively reported no benefits when MBI were compared to active and inactive controls,31 both in the short-term and long-term.37 While some individual studies included in these reviews did demonstrate small improvements in depression, collectively there was insufficient evidence to support the effectiveness of MBI.
Six reviews30,32,33,36,39,41 reported mixed findings. Khoo et al36 undertook a meta-analysis of three studies and reported a significant change in depression symptoms in favour of MBSR over controls; however, when MBSR was compared to CBT, the differences between treatments were no longer significant. While Albajes et al30 reported that ACT may be a promising intervention for depression based on percentages of success (eg 100% success rate for studies using ACT vs 67% success rate for MBI), an overall lack of robust data prevented a conclusive verdict. Chiesa et al32 reported that in three of four studies comparing MBI with wait list control, and one study comparing MBI to progressive muscle relaxation, MBI was found to be significantly more effective in improving depression. However, in two studies comparing MBI to active treatment (eg qigong, educational support group, cognitive behavioural therapy, educational group), the difference between treatments was not shown to be statistically significant. Garmon et al33 reported similarly mixed findings according to the type of control group. In two studies, MBI were found to be effective in reducing depression when compared with waitlist controls, but not when compared to active controls (eg education, multi-disciplinary pain intervention CBT). Data from two further studies38,42 that examined the effect of MBI on depression in chronic pain were not included, as MBI formed part of a battery of psychological interventions, and data for the specific effects of MBI on depression could not be separated. Collectively, the literature provides mixed evidence regarding the effectiveness of MBI on depression.
Sleep Quality
Six reviews18,30,31,33,37,42 measured the effectiveness of MBI on sleep quality. Sleep quality was assessed using a range of outcome measures, including the Pittsburgh Sleep Quality Index, Epworth Sleepiness Scale and Visual Analogue Scale. Albajes et al30 identified that MBI may be beneficial for sleep-related problems as the four studies included in their review collectively provided evidence of a significant improvement. These purported benefits were reported for a range of sleep parameters, including sleep quality, sleep problems, sleep disturbances and sleep latency. These findings were supported by Cramer et al18 and Garmon et al33 who included one and two studies respectively, with both reporting improvements in sleep quality. This was in contrast to reviews by Bawa et al31 (two studies), Lauche et al37 (two studies) and Theadom et al42 (one study), which reported no benefits of MBI on sleep quality. Collectively, the included reviews provide conflicting evidence regarding the effectiveness of MBI on sleep quality.
Physical Functioning
Eight reviews18,30–33,35,36,42 measured the effectiveness of MBI on physical functioning. Studies that formed part of these reviews used various measures of physical functioning, such as the Short Physical Performance Battery and Roland Morris Disability Questionnaire. Albajes et al,30 Cramer et al,18 and Garmon et al,33 all identified that MBI were beneficial for physical functioning related problems as the eight unique studies (of which one study was repeated) included in the reviews collectively provided evidence of benefit. The review by Albajes et al reported positive benefits in the short to medium term (at twelve weeks) as well as long term (eighteen months). This contrasted with reviews by Jackson et al35 (fifteen studies), Khoo et al36 (fifteen studies), and Theadom et al42 (two studies), that collectively reported no benefits of MBI on physical functioning. While some of the individual studies included in these reviews did demonstrate small improvements in physical functioning, collectively there was insufficient evidence to support the effectiveness of MBI. Two reviews31,32 reported mixed findings. Bawa et al31 undertook a meta-analysis of five studies and reported a combined positive small effect size. This effect was particularly noticeable when MBI were compared to inactive controls, but not when compared with active controls. Collectively, the literature provides mixed evidence regarding the effectiveness of MBI on physical functioning.
Mindfulness Measures
Three reviews18,31,39 measured the effectiveness of MBI on measures of mindfulness. Studies that formed these reviews used an array of outcome measures, including the Mindful Attention and Awareness Scale (MAAS), Five Facet Mindfulness Questionnaire (FFMQ), and 14-item short form of the Freiburg Mindfulness Inventory (FMI). Pei et al39 (three studies) identified that MBCT increased mindfulness in the short-term. However, when these data underwent meta-analysis, there was limited evidence to suggest that MBCT has a positive impact on mindfulness when compared with non-MBCT in the short-term. This contrasted with reviews by Bawa et al31 (four studies), and Cramer et al18 (one study), that collectively reported no statistically significant benefits of MBI on mindfulness. However, Bawa et al31 suggest that the MAAS measurement tool used in three of the four studies included in their review may be inappropriate for use with novice meditators as it lacks the necessary sensitivity to measure changes in this population. Referring to MAAS as unidimensional, Bawa et al31 recommend that a multidimensional tool be used in future research, such as the FMI measurement tool. The review by Cramer et al18 included only one study. This study was also included in the review by Bawa et al.31 Both reviews are in agreeance regarding this study and so no additional data of importance was found. While some of the individual studies included in these reviews did support small improvements in mindfulness, the evidence was largely insufficient. Collectively, the literature provides mixed evidence regarding the effectiveness of MBI on mindfulness outcomes.
Summary of Results
An overview of the volume and direction of the evidence regarding the effectiveness of MBI for CMSP is illustrated in Figure 2. Overall, across the included systematic reviews and across all outcomes, the evidence remains mixed, and is therefore inconclusive.
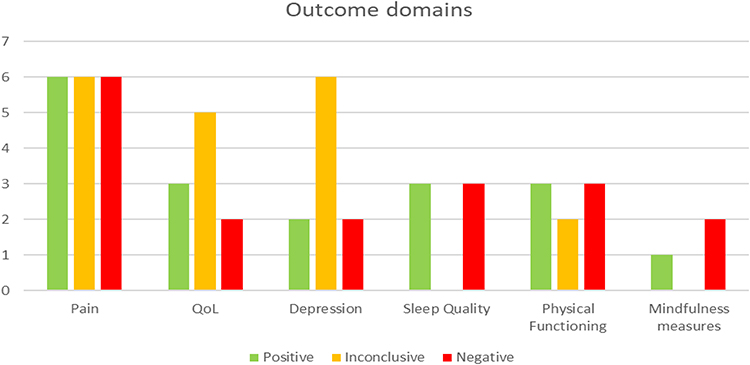 |
Figure 2 Overview of outcomes and results from the included systematic reviews. |
Discussion
This umbrella review set out to provide a synthesis of the best available research evidence regarding the effectiveness of MBI for adults suffering from CMSP. Given the rising popularity of MBI, and the plethora of research investigating the effectiveness of these techniques in recent decades, it is important to keep abreast of this evidence-base in order to adequately inform clinical practice, and to guide future research. While the available evidence for this umbrella review was predominantly low-quality and mixed, there are some outcomes for which MBI shows some promise (eg, pain, quality of life and depression).
An important finding of this review was the variability in the definitions of mindfulness reported across included studies. While there were some commonalities, there was also marked differences. For example, the review by Khoo et al36 defined mindfulness in the context of MBSR, that is as “a group-based intervention that focuses on building awareness and acceptance of moment-to-moment experiences, including physical discomfort and difficult emotions. Core components of MBSR include increasing awareness of one’s body, emotions, sensations, thoughts as well as learning self-regulation strategies and more adaptive responses to stress”. This definition suggests there is a fundamentally judgemental element to mindfulness practice where one becomes aware of a sensation or thought, acknowledges it, and employs adaptive strategies to alter their response to the sensation. However, Veehof et al43 defines mindfulness as “intentional and non-judgmental awareness. It can be conceptualized as a multifaceted construct, consisting of the facets: observe, describe, act with awareness, non-judge and non-react”. This definition suggests a non-judgemental, non-reactive approach to mindfulness. This appears to be in line with the standard definition for mindfulness within MBSR as originally coined by John Kabat-Zinn,11 which describes mindfulness as essentially non-judgemental. This is an important consideration as these varying philosophical approaches to MBI likely influence treatment approaches and hence outcomes.
The variability in the definitions of MBI also seems to extend to the parameters of these interventions as shown in Table 4. Heterogeneity was found in session lengths, number of sessions, frequency of sessions and duration of treatments. For example, Garmon et al33 included body scan, sitting meditation, yoga, stretching and breathing, while Lauche et al37 included walking meditation and informal practice during activities of daily living as part of MBSR intervention parameters. Similarly, session duration and frequency in Lauche et al37 were 2–3.5 hours weekly for 8–10 sessions, with homework 30–40 min for 8–12 weeks, while Rajguru et al40 included 30–45 min weekly sessions with 30–45 min homework 5–6 days per week for 8 weeks. It is unknown why such heterogeneity exists in the literature given that many of these techniques have internationally standardised training programs, such as Transcendental Meditation® and MBSR. Indeed, the official curriculum guide for MBSR stipulates that MBSR should be conducted as an 8-week, 10 session course, which includes 31 hours of direct instruction.11 The content of each session is clearly outlined in this guide. Although the authors of the original guide welcome adaptation of new mindfulness systems, they do suggest the term MBSR only be used in line with such guides.11
An interesting finding from this umbrella review was that for all outcomes, MBI was shown to be more effective than inactive controls, but comparable to active controls, particularly when the active comparator was CBT. This was consistent across reviews that included both inactive and active controls, or active controls only. There are several possible explanations for this finding. First, it is possible that MBI has a positive effect on a range of outcomes in persons living with CMSP, when compared to no intervention. Second, as MBI reported in this review often included MBSR techniques, which share commonalities with CBT, it is not surprising that both interventions reported comparable findings. The comparable findings for MBI and CBT may have implications for practice. For example, as CBT is generally provided by qualified health professionals, MBI may be an easily accessible, cost-effective alternative to CBT given that MBI does not require specialist training and credentialing.46,47
Recent research using functional magnetic resonance imaging investigated the physiological mechanisms for potential benefits of MBI on pain.20 There was variation in the changes in the neural mechanisms of pain attenuation across those with varying levels of experience in mindfulness practice.20 Findings from the research indicate that in novice meditators, with less than 10 hours of practice, higher order regulation occurred across the orbitofrontal cortex and rostral anterior cingulate cortex (brain areas that are involved with the processing of pain), which regulated low-level neural targets in the thalamus and primary somatosensory cortex suggesting the activation of reappraisal mechanisms.20 Further to this, more experienced meditators, having practiced MBI for greater than 1000 hours, showed deactivation of the prefrontal cortex, and an increased activation in the somatosensory cortex which shows an increased ability to reduce appraisals of arising sensory events.20 It is suggested that these changes and differences in the neural activity across the differing experience levels of mindfulness practitioners may be due to neural plasticity, which is affected by practice frequency.20 The outcome of this is first a change in state mindfulness, the part of mindfulness that is controlled moment to moment, and a progression, amongst more experienced practitioners, towards a change in trait mindfulness, which is the normal, underlying level of mindfulness experienced by an individual, regardless of their deliberate control.20,21
While this umbrella review identified 19 reviews, which on face value seems to indicate a large body of evidence, there were concerns about the methodological quality of this evidence base. Using the AMSTAR 2 critical assessment tool, fifteen of the nineteen reviews were rated as critically low. This finding is not unique to this umbrella review and is shared by other research. For example, a recent qualitative content analysis reviewed the current literature related to both mindfulness and meditation, with the aim to develop a framework and guideline for reporting mindfulness and meditation research.48 The study reported that the underlying evidence base related to mindfulness and meditation was heterogeneous in terms of study designs, lacked comparisons or controls, lacked appropriate randomization, follow-up assessments, reporting of treatment dose, and consideration for potential biases.48 One way to address this shortcoming is through the use of reporting guidelines. The CONSORT (Consolidated Standards of Reporting Trials) statements are established reporting guidelines commonly used for studies reporting social and psychological interventions. The extension CONSORT-SPI 2018 has been recently proposed as a useful tool for the reporting of MBI; although, it does not currently provide specific guidance for meditation-based interventions.48 A further extension of this CONSORT statement may help improve the rigour, transparency, and consistency of reporting of interventions in future meditation research.
Strengths and Limitations of This Review
As the popularity of MBI increases, it is important to map and establish the evidence base of this practice. This review has mapped for the first time, the definitions of mindfulness as reported in systematic reviews. The methodology was also informed by best practice standards and was conducted in accordance with established protocols (PRISMA49 and JBI27). The evidence was synthesised using a well-established and widely used framework (NHMRC FORM framework).28 Nevertheless, as with any research, this umbrella review too has limitations. The search strategy was limited to reviews published in the English language, which may have possibly introduced language bias. There were also limitations that are inherent to umbrella reviews. For example, given that an umbrella review is a review of reviews, the primary focus is on the data reported within the systematic reviews and not on the data from the primary research studies included in those reviews. This means that it is often necessary to rely upon the interpretations of primary data that were made within the systematic reviews, which may or may not have been undertaken using a rigorous process. Another important limitation to consider is the differentiation between different types of pain (such as persistent and recurrent pain). The reviews included in this umbrella review often did not differentiate between persistent and recurrent pain (which may be common in musculoskeletal disorders). Given different types of pain may respond differently to MBIs, this lack of differentiation may have contributed to the mixed results.
Recommendations for Practice and Future Research
Based on the findings of our review, we propose three key recommendations. First, heterogeneity was found across several aspects of the practice and delivery of MBI in both primary and secondary research. We therefore recommend development and implementation of standardised protocols for MBI to ensure consistency in its application and facilitate comparison between research. Second, as mindfulness is used as an umbrella term that includes many different types of interventions, such as MBSR, ACT, and mindful exercise, further investigations of the differences in effect between the various types of MBI is recommended. These differences may provide a more nuanced understanding of the role of different MBI in different clinical contexts. Finally, while MBI was found to be comparable to CBT (and better than no treatment) for people with CMSP, caution is required in its application due to the generally low quality of the evidence. Further research is required to substantiate these findings through the use of standardised and replicable protocols.
Conclusion
The aim of this umbrella review was to synthesise the best available research evidence for the effectiveness of MBI for adults living with CMSP across a range of outcomes (pain, sleep quality, depression, quality of life, physical functioning, mindfulness), and to explore the parameters and methodologies used in the systematic reviews. Collectively, across the 19 included reviews, there was mixed results to support the effectiveness of MBI. A potential reason for these mixed results may be due to heterogeneity of parameters underpinning MBIs reported in the reviews including varying techniques, intensity, duration, and frequency. This, combined with concerns about methodological quality, means an unequivocal recommendation to support MBI for adults living with CMSP cannot be made and caution is required in interpreting these results. With increasing interest in the clinical use of MBI in the management of CMSP, development and testing of standardised protocols for MBI through further research is warranted.
Data Sharing Statement
All relevant data are within the paper and its supporting information files.
Acknowledgments
The authors would like to thank and acknowledge Lorien Delaney, Academic Librarian, University of South Australia, for generously providing guidance, feedback and validation of the search strategy used in this systematic review.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation. All authors gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
Disclosure
The authors have declared that no competing interests exist.
References
1. Blyth FM, Briggs AM, Schneider CH, Hoy DG, March LM. The global burden of musculoskeletal pain—where to from here? Am J Public Health. 2019;109(1):35–40. doi:10.2105/AJPH.2018.304747
2. Organization WH. Musculoskeletal health; 2022. Available from: https://wwwwhoint/news-room/fact-sheets/detail/musculoskeletal-conditionsPristupljeno.
3. Booth J, Moseley GL, Schiltenwolf M, Cashin A, Davies M, Hübscher M. Exercise for chronic musculoskeletal pain: a biopsychosocial approach. Musculoskeletal Care. 2017;15(4):413–421. doi:10.1002/msc.1191
4. Pomarensky M, Macedo L, Carlesso LC. Management of chronic musculoskeletal pain through a biopsychosocial lens. J Athl Train. 2022;57(4):312–318. doi:10.4085/1062-6050-0521.20
5. Hilty DM. Advancing science, clinical care and education: shall we update engel’s biopsychosocial model to a bio-psycho-socio-cultural model. Psychol Cogn Sci Open J. 2015;1(1):e1–e6. doi:10.17140/PCSOJ-1-e001
6. Flynn DM. Chronic musculoskeletal pain: nonpharmacologic, noninvasive treatments. Am Fam Physician. 2020;102(8):465–477.
7. Brown CA, Jones AK. Psychobiological correlates of improved mental health in patients with musculoskeletal pain after a mindfulness-based pain management program. Clin J Pain. 2013;29(3):233–244. doi:10.1097/AJP.0b013e31824c5d9f
8. Shafiei F, Amini FM. Efficacy of mindfulness-based stress reduction on reducing catastrophizing and pain intensity in patients suffering chronic musculoskeletal pain. J Anesth Pain. 2017;8(1):1–10.
9. Curtin KB. The Relationship Between Chronic Musculoskeletal Pain, Anxiety and Mindfulness: adjustments to the Fear-Avoidance Model of Chronic Pain [Ph.D.]. Ann Arbor: American University; 2017.
10. Siegel RD, Germer CK, Olendzki A. Mindfulness: what is it? Where did it come from? In: Clinical Handbook of Mindfulness. Springer; 2009:17–35.
11. Santorelli SF, Kabat-Zinn J, Blacker M, Meleo-Meyer F, Koerbel L. Mindfulness-based stress reduction (MBSR) authorized curriculum guide. In: Center for Mindfulness in Medicine, Health Care, and Society (CFM). University of Massachusetts Medical School; 2017.
12. Davidson RJ, Kabat-Zinn J, Schumacher J, et al. Alterations in brain and immune function produced by mindfulness meditation. Psychosom Med. 2003;65(4):564–570. doi:10.1097/01.PSY.0000077505.67574.E3
13. Zelazo PD, Lyons KE. The potential benefits of mindfulness training in early childhood: a developmental social cognitive neuroscience perspective. Child Dev Perspect. 2012;6(2):154–160. doi:10.1111/j.1750-8606.2012.00241.x
14. Blanck P, Perleth S, Heidenreich T, et al. Effects of mindfulness exercises as stand-alone intervention on symptoms of anxiety and depression: systematic review and meta-analysis. Behav Res Ther. 2018;102:25–35. doi:10.1016/j.brat.2017.12.002
15. la Cour P, Petersen M. Effects of mindfulness meditation on chronic pain: a randomized controlled trial. Pain Med. 2015;16(4):641–652. doi:10.1111/pme.12605
16. Vøllestad J, Nielsen MB, Nielsen GH. Mindfulness‐and acceptance‐based interventions for anxiety disorders: a systematic review and meta‐analysis. Br J Clin Psychol. 2012;51(3):239–260. doi:10.1111/j.2044-8260.2011.02024.x
17. Bahnamiri FA, Norouzi A, Reskati MH, Hosseini SH. Effectiveness of mindfulness-based interventions on pain intensity in patients with chronic low back pain: a systematic review. Iran J Psychiatry Behav Sci. 2020;14(4):1.
18. Cramer H, Haller H, Lauche R, Dobos G. Mindfulness-based stress reduction for low back pain. A systematic review. BMC Complement Altern Med. 2012;12(1):1–8. doi:10.1186/1472-6882-12-162
19. Eccleston C, Fisher E, Craig L, Duggan GB, Rosser BA, Keogh E. Psychological therapies (Internet‐delivered) for the management of chronic pain in adults. Cochrane Database Syst Rev. 2014;2:1.
20. Zeidan F, Baumgartner JN, Coghill RC. The neural mechanisms of mindfulness-based pain relief: a functional magnetic resonance imaging-based review and primer. Pain Rep. 2019;4:4. doi:10.1097/PR9.0000000000000759
21. Kiken LG, Garland EL, Bluth K, Palsson OS, Gaylord SA. From a state to a trait: trajectories of state mindfulness in meditation during intervention predict changes in trait mindfulness. Pers Individ Dif. 2015;81:41–46. doi:10.1016/j.paid.2014.12.044
22. Wang L-P, Jiang X-L, Wang L, Wang G-R, Bai Y-J, Morgan D. Barriers to and facilitators of research utilization: a survey of registered nurses in China. PLoS One. 2013;8(11):e81908. doi:10.1371/journal.pone.0081908
23. Treede R-D, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003. doi:10.1097/j.pain.0000000000000160
24. Higgins JP Cochrane handbook for systematic reviews of interventions version 5.0. 1. The Cochrane Collaboration; 2008. Available from: http://wwwcochrane-handbookorg.
25. EndNote [computer program]. Version EndNote X9. Philadelphia, PA: Clarivate; 2013.
26. Covidence system review software [computer program]. Melbourne, Australia; 2021.
27. Aromataris E, Fernandez R, Godfrey C, Holly C, Khalil H, Tungpunkom P. Chapter 10: umbrella reviews. In: JBI Manual for Evidence Synthesis. JBI; 2020.
28. Hillier S, Grimmer-Somers K, Merlin T, et al. FORM: an Australian method for formulating and grading recommendations in evidence-based clinical guidelines. BMC Med Res Methodol. 2011;11(1):1–8. doi:10.1186/1471-2288-11-23
29. Tsiros MD, Tian EJ, Shultz SP, et al. Obesity, the new childhood disability? An umbrella review on the association between adiposity and physical function. Obes Rev. 2020;21(12):e13121. doi:10.1111/obr.13121
30. Albajes K, Moix J. Psychological interventions in fibromyalgia: an updated systematic review. Mediterr J Clin Psychol. 2021;9(1):1.
31. Bawa FLM, Mercer SW, Atherton RJ, et al. Does mindfulness improve outcomes in patients with chronic pain? Systematic review and meta-analysis. Br J Gen Pract. 2015;65(635):e387–e400. doi:10.3399/bjgp15X685297
32. Chiesa A, Serretti A. Mindfulness-based interventions for chronic pain: a systematic review of the evidence. J Altern Complement Med. 2011;17(1):83–93. doi:10.1089/acm.2009.0546
33. Garmon B, Philbrick J, Daniel Becker M, John Schorling M, Padrick M, Goodman M. Mindfulness-based stress reduction for chronic pain: a systematic review. J Pain Manag. 2014;7(1):23.
34. Hilton L, Hempel S, Ewing BA, et al. Mindfulness meditation for chronic pain: systematic review and meta-analysis. Ann Behav Med. 2017;51(2):199–213. doi:10.1007/s12160-016-9844-2
35. Jackson W, Zale EL, Berman SJ, et al. Physical functioning and mindfulness skills training in chronic pain: a systematic review. J Pain Res. 2019;12:179. doi:10.2147/JPR.S172733
36. Khoo E-L, Small R, Cheng W, et al. Comparative evaluation of group-based mindfulness-based stress reduction and cognitive behavioural therapy for the treatment and management of chronic pain: a systematic review and network meta-analysis. Evid Based Ment Health. 2019;22(1):26–35. doi:10.1136/ebmental-2018-300062
37. Lauche R, Cramer H, Dobos G, Langhorst J, Schmidt S. A systematic review and meta-analysis of mindfulness-based stress reduction for the fibromyalgia syndrome. J Psychosom Res. 2013;75(6):500–510. doi:10.1016/j.jpsychores.2013.10.010
38. Niknejad B, Bolier R, Henderson CR, et al. Association between psychological interventions and chronic pain outcomes in older adults: a systematic review and meta-analysis. JAMA Intern Med. 2018;178(6):830–839. doi:10.1001/jamainternmed.2018.0756
39. Pei J-H, Ma T, Nan R-L, et al. Mindfulness-based cognitive therapy for treating chronic pain a systematic review and meta-analysis. Psychol Health Med. 2021;26(3):333–346. doi:10.1080/13548506.2020.1849746
40. Rajguru P, Kolber MJ, Garcia AN, Smith MT, Patel CK, Hanney WJ. Use of mindfulness meditation in the management of chronic pain: a systematic review of randomized controlled trials. Am J Lifestyle Med. 2015;9(3):176–184. doi:10.1177/1559827614522580
41. Smith SL, Langen WH. A systematic review of mindfulness practices for improving outcomes in chronic low back pain. Int JYoga. 2020;13(3):177.
42. Theadom A, Cropley M, Smith HE, Feigin VL, McPherson K. Mind and body therapy for fibromyalgia. Cochrane Database Syst Rev. 2015;4. doi:10.1002/14651858.CD001980.pub3
43. Veehof MM, Trompetter H, Bohlmeijer ET, Schreurs K. Acceptance-and mindfulness-based interventions for the treatment of chronic pain: a meta-analytic review. Cogn Behav Ther. 2016;45(1):5–31. doi:10.1080/16506073.2015.1098724
44. Zou L, Zhang Y, Yang L, et al. Are mindful exercises safe and beneficial for treating chronic lower back pain? A systematic review and meta-analysis of randomized controlled trials. J Clin Med. 2019;8(5):628. doi:10.3390/jcm8050628
45. Williams A, Fisher E, Hearn L, Eccleston C. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev. 2020;8. doi:10.1002/14651858.CD007407.pub4
46. Herman PM, Anderson ML, Sherman KJ, Balderson BH, Turner JA, Cherkin DC. Cost-effectiveness of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care among adults with chronic low-back pain. Spine. 2017;42(20):1511. doi:10.1097/BRS.0000000000002344
47. Cherkin DC, Sherman KJ, Balderson BH, et al. Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: a randomized clinical trial. JAMA. 2016;315(12):1240–1249. doi:10.1001/jama.2016.2323
48. Pilla D, Qina’au J, Patel A, et al. Toward a framework for reporting and differentiating key features of meditation-and mindfulness-based interventions. Mindfulness. 2020;11(11):2613–2628. doi:10.1007/s12671-020-01475-7
49. Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1–e34. doi:10.1016/j.jclinepi.2009.06.006
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.