Back to Journals » Advances in Medical Education and Practice » Volume 7
Mindful approach to University education
Authors Broggi F, Bomba M ![]() , Rimondini M, Mutti M, Pasta S, Ricci C, Tagliabue L, Valsecchi S, Monaco E, Neri F, Oggiano S, Nacinovich R
, Rimondini M, Mutti M, Pasta S, Ricci C, Tagliabue L, Valsecchi S, Monaco E, Neri F, Oggiano S, Nacinovich R ![]()
Received 31 December 2015
Accepted for publication 23 March 2016
Published 27 September 2016 Volume 2016:7 Pages 553—558
DOI https://doi.org/10.2147/AMEP.S103402
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Fiorenza Broggi,1 Monica Bomba,1 Michela Rimondini,2 Maura Mutti,1 Sara Pasta,1 Chiara Ricci,1 Luca Tagliabue,1 Silvia Valsecchi,1 Elide Monaco,1 Francesca Neri,1 Silvia Oggiano,2 Renata Nacinovich,1
1Department of Child and Adolescent Psychiatry, San Gerardo Hospital, University of Milano–Bicocca, Monza, 2Department of Clinical Psychology, University of Verona, Italy
Abstract: A mindful approach to education and training could improve students’ reflective capacities and have positive effects on clinical practice because it facilitates a helping relationship. The main aims of this study were to investigate whether participation in a mindful-based University training was associated with increases in mindfulness skills as measured by the 5-Facet M Questionnaire, and to present the Italian validation of the questionnaire. Sixty-seven students from the course Neuro and Psychomotor Therapy were enrolled. They filled in the self-administered 5-Facet M Questionnaire before and 1 month after a mindfulness-based training, focused on role-playing and followed by a feedback group discussion. The Italian version of the 5-Facet M Questionnaire had good psychometric properties. The pre- and post-training analysis showed a significant increase in the subscale ‘Observing’. Findings suggest that role-playing and feedback group sessions are valid tools to improve students’ mindfulness skills.
Keywords: mindfulness, role play, self-awareness, communication skills, insight, reflective capacities, feedback
Introduction
The practice of mindfulness refers to the use of the ability to focus one’s attention on the present experience, neither judgmentally nor in a condescending way.1–4 In fact, mindfulness is aimed at replacing day-to-day reactive, automatic, and destructive behaviors with aware and context-appropriate choices, through the acquisition of the following three fundamental abilities:
- Learning the ability to live in the present moment, instead of being caught up in the imagination of the future, or in the recrimination of the past.
- Learning to recognize thoughts for what they are and not consider them as matters of fact, to facilitate decentralization.
- Overcoming the tendency to avoid experiences, which is characterized by flight attitude and rejection of one’s own thoughts, emotions, and physical sensations. This goal is correlated with the awareness of being able to choose one’s own actions and the objectives to commit to.
Siegel explains how a mindful approach to education and training puts the students in the center, actively involving them in the learning process, enabling the teacher to join him/her as an active explorer in the student’s discovery journey.5,6
In clinical practice, mindful awareness and the empathic availability of the therapist to be mindfully present to all that arises as the object of the joint attention of the therapeutic experience can become a fundamental part of therapy. It can improve people’s lives and reduce suffering, thus facilitating a personal transformation that involves the three points of the triangle of well-being: coherent mind, empathic relationships, and neural integration.5
Joint attention starts the attunement, which can be considered the core of the therapeutic change: when we engage in a relationship with another person, we reciprocally focus our awareness on the elements of our minds and these elements become the shared center. When this union develops, we start to resonate with our reciprocal states and we get modified by the relationship with the other.5 The internal attunement that encourages the growth of the brain and the interpersonal attunement that catalyzes similar activation and neural growth promote integration. Therefore, for any kind of therapy to be effective, activation, growth, and neural integration must be facilitated, and coherence of the mind and stable empathy in the relationships must be promoted. This is the way in which therapy strengthens the triangle of well-being.5
The neuro and psychomotor therapist for children works in a therapeutic rehabilitation setting in which communication is mainly based on nonverbal language; therefore, he/she must be trained during his/her university studies to recognize the languages he/she will be using daily with children from an emotional and sensitivity point of view (look, facial expressions, posture, gestures, voice tone, voice, and prosody) and their tuning in to the communication. In order to properly relate to patients, therapists must learn how to act with awareness and attention in their daily clinical practice; for this purpose, a training program should provide the possibility of being observed and observing oneself in the rehabilitation therapeutic practice and of receiving a feedback about it from an external supervisor. This pathway should be followed slowly, safely, and respecting personal sensibilities.
A mindful approach facilitates child therapists to be able to actively listen to patients and to stay with them in the “here and now”. Moreover, students’ training programs aimed at building reflective and aware relationships positively influence clinical capacities, facilitating a correct helping relationship.5 In this study, we propose to introduce the role-playing approach in the training of child therapists in order to facilitate the acquisition of greater mindfulness skills, which could be later implemented in their daily practice. In fact, it is fundamental to build a training setting considering a physical and symbolic environment, with regard to space, time, and privileged relationships domains. It is something that refers to the way training is conducted by acting, to its “materiality”, as Massa said,7 which means giving attention to both the physical space, which helps in learning, as well as time, rhythms, and relationships, which might facilitate its development.
The aims of our research were as follows: 1) to assess the effectiveness of mindfulness-based role-playing and feedback group sessions in increasing the levels of mindfulness in an educational context, as measured by the Five-Facet Mindfulness Questionnaire8 (FFMQ); and 2) to validate the Italian version of the FFMQ.
Methods
Sample
Ethical approval was obtained from Ethics Committee of Milano Bicocca University, June 10, 2013. Role-playing is part of the personal training provided to students of the second and third years of the Childhood Neuro and Psychomotricity course at Milan Bicocca University, Italy. All the 43 students of the second and third years, 40 females (93%) and three males (7%), decided to participate in the study.
All participants signed an informed consent. Twenty-one were in the second year (20 females and one male), and 22 were third-year students (20 females and two males). The students had a mean age of 22.04 years.
The 43 subjects attending the second and the third years were randomly divided into eight groups of five to six participants, homogeneous per year of the course. These subjects underwent the role-play sessions; they were also asked to fill in the questionnaire to assess mindfulness skills (the Five-Facet Mindfulness Questionnaire). The group composition was not modified during the different stages of the study.
At the end of the role-play training, the students received a feedback in order to improve their awareness on their mindfulness skills. The results were not included in the assessment of the student’s academic curriculum and didn’t represent an academic evaluation.
Tools
Self-assessment Five-Facet Mindfulness Questionnaire
The Self-assessment Five-Facet Mindfulness Questionnaire (Five-Facet M Questionnaire)9 theoretically refers to the practice of mindfulness, which aims at replacing reactive, day-to-day automatic and destructive behaviors with aware and context-appropriate choices. This assessment tool measures all the five components of mindfulness: observing, describing, acting with awareness, nonjudging, and nonreactivity. It is a pen-and-paper questionnaire, self-administered, both individually. It is made up of 39 items, divided into five subscales, which measure the five elements of mindfulness: Observing (eight items, eg, “I realize when my mood starts to change”), Describing (eight items, eg, “I can easily put my feelings into words”), Acting with awareness (eight items, eg, “When I do things, my mind wanders off and I’m easily distracted”), Nonjudging (eight items, eg, “I tell myself I shouldn’t be feeling the way I’m feeling”), and Nonreactivity (seven items, eg, “Feel my emotions and feelings without having to react”).
Each item is measured on a five-point Likert scale, in which 1 corresponds to the answer “never or very rarely true” and 5 indicates “always or almost always true”. The sum of the scores for the items composing each scale represents the scale score, and the total score corresponds to the sum of the five scales’ subtotals. The final scores from Observing, Describing, Acting with awareness, and Non-judging can vary from 8 to 40, whereas the final score from the Non-reactivity scale is from seven to 35. The total score is made up of five subtotals, with a range from 39 to 195.
Translation procedure
The Italian version we used is derived from the translation of the original questionnaire written in English. Translation was done from the English version received by the author with her written permission to the use of the questionnaire. First, the Five-Facet M Questionnaire was translated into Italian by two independent linguistic experts, and this resulted in the development of versions A and B of the questionnaire. Then, both the linguistic experts discussed each item with the clinical experts, and version C was reached. This version C was then back-translated into English by two other linguistic experts. This step resulted in the version D. This version D was then compared with the original questionnaire and points of disagreement were discussed with clinical experts. Language was again modified and an Italian version E was created. This questionnaire was administered to ten students of the first year of the academic course for neuro and psychomotor therapy for children in order to assess the ease of understanding. They were encouraged to report any difficulty that they had faced in understanding any of the items. Wherever the students reported any difficulty, the issue was discussed with the linguistic experts and appropriate change was made to keep the language the closest possible to the original questionnaire. Finally, version F was created. This final version was used for this study.
Training program
The training on the use of verbal and nonverbal techniques, aimed at understanding children and help them during the therapy, had the main objective of improving the students’ levels of mindfulness by the following means:
- increasing the level of awareness of the subjects toward their emotions, thoughts, and automatisms;
- having them learn how to stick to the present moment, instead of being taken away by the anticipation of the future or mourning for the past;
- having them learn how to witness their thoughts for what they are.
The 43 students attending the second and the third years of the courses were divided into eight groups. Each group underwent two modules composed of a role-play session followed by a video feedback and a group discussion (Figure 1), for a total of 30 hours. The second module was proposed 30 days after the first one. The modules had the following structure: on the first day, before each role simulation, a briefing supervised by the coordinator took place, aimed at receiving information (place, goals) and thinking over the experience that the student was about to have. It is aimed at guiding someone toward an experience that is characterized by instructions, aims, and rules. This activates an anticipative reflection, creating a welcoming environment, which helps participants to find the courage to express their own fears and training deficiencies they think of having and to help them become more aware of their emotions and thoughts.10–13 After the briefing, each student was asked to alternatively play the role of the therapist, the patient, and the observer. Each subject within his/her own group played all the three roles. The role-playing allows the subjects to connect with their inner experience in a supportive and nonjudgmental context and aimed at improving the students’ verbal and nonverbal techniques: for instance, adapting the language content, structure, and tone to the child’s age and abilities and to different moments in the therapy; synchronizing the tone with the posture; modifying one’s look according to the changes in the play, the posture, and the tone; modifying one’s posture according to the child’s. At the end of each simulation, we proposed a debriefing in which the group met with the coordinator to analyze the experience, highlighting mistakes and accidents, detected both during the action and later on; additionally, retrospective thinking was facilitated, together with an intentional reviewing of what occurred.
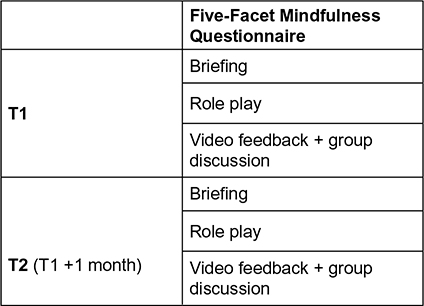 | Figure 1 Study design. |
On the second day, the group met to watch the videos of the five role plays. On the following day, all participants had a moment of personal reflection and they wrote what arose, both from the debriefing moments and from the group work. Finally, on the fourth day, the group met with the coordinator to share thoughts. This pattern was used also in the second module, for both years of the course.
Study design
All the subjects enrolled were given a numerical code.
The study is divided into two assessment phases (Figure 1).
- Time 1 (T1): the self-administered Five-Facet M Questionnaire is filled in by the students. Afterward, the first role play is presented. The experiences are video-recorded and, the following day, the video recordings are used by the students for the theoretical analysis.
- Time 2 (T2): after 1 month from T1, the second role play is presented.
Moreover, the second self-administered Five-Facet M Questionnaire is filled in on the same day, at the end of the role play (Figure 1).
Statistical analysis
The categorical variables are expressed in number and percentage, while the continuous variables are identified as mean and standard deviation (SD). To read the significance of a hypothesis test, the null hypothesis is rejected if the P-value is <5%.
To evaluate the presence of potential differences between second-year and third-year students at baseline, ie, at the start situation, a specific test was run to verify the differences between the samples, the t-test for independent samples, on the sociodemographic data together with the tests collected at T1. Because no significant differences were found between the two course years, we proceeded with the analysis of all data, considering the subjects as belonging to only one sample.
Reliability of the Five-Facet M Questionnaire was measured by calculating the Cronbach’s alpha. Pearson test was adopted to study the correlation between the subscales. To evaluate the Five-Facet M Questionnaire pre–post role play, the paired-samples t-test was used.
R-Statistical package was used for data analysis. A P-value ≥0.05 was considered to be statistically significant.
Results
Sociodemographic characteristics
No significant differences emerged among the 43 Italian subjects of different academic-class years (three males and 40 females) with regard to sociodemographic variables (Table 1).
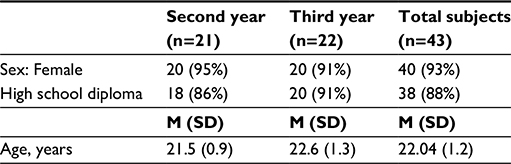 | Table 1 Sample description Abbreviations: M, mean; SD, standard deviation. |
Five-Facet M Questionnaire
In Table 2, the results of the analysis of internal consistency of the five scales of the Five-Facet M Questionnaire are described. The scales showed a good internal consistency, being well balanced and presenting an α-value between 0.77 and 0.89. Cronbach’s alpha of the total scale was 0.80.
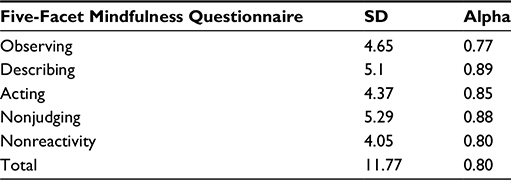 | Table 2 Analysis of inner consistency and SD of the self-administered Five-Facet Mindfulness Questionnaire Abbreviation: SD, standard deviation. |
In order to check the relation between the subscales, we used Pearson’s coefficient, which showed a low correlation between the five subscales of the Five-Facet Mindfulness Questionnaire (range: –0.16 to 0.30), indicating that they differentiate the areas studied sufficiently well. The results confirmed that the Italian version of the Five-Facet M Questionnaire also presented psychometric properties as good as the US version.8
Pre- and posttraining analysis
Five-Facet M Questionnaire
An analysis of the effect of the role-play approach on the score variance of the Five-Facet M Questionnaire was performed using the t-test for paired samples (Table 3).
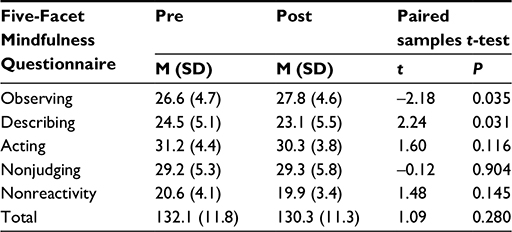 | Table 3 Effect of role play on mean scores and SD in the Five-Facet Mindfulness Questionnaire Abbreviations: M, mean; SD, standard deviation. |
We found a significant increase of the scores in the subscale Observing (P=0.035) and a decrease of the scores in the subscale Describing (P=0.031). In addition, there was a slight increase in the subscale Nonjudging, although not statistically significant. No other noteworthy changes in the Five-Facet M Questionnaire emerged.
Discussion
The purpose of this study was to evaluate whether a mindfulness-based training aimed at improving the communication skills of students of neuro and psychomotor therapy would increase the subjects’ mindfulness. In the training, we chose to use role plays and simulations because they have been shown to be effective and useful in training programs.14–17
The results of our study showed that improvements as assessed by the Five-Facet M Questionnaire were seen only in one item (Observing). Nevertheless, a slight increase in the subscale Nonjudging was found. These data may suggest that the subjects were probably starting a developmental shifting from a “top–down” modality of experiencing the world under the influence of prior learning and categories, to a “bottom–up” modality based on personal observation and mindfulness skills. Our hypothesis is that autoreflective capacity and awareness of the therapeutic relationship might emerge later on in the progress of the training, after the acquisition of the competence skills. In fact, in order to overcome the tendency to avoid experiences, a long and gradual training course is necessary.5
Siegel18 claims that the role of mindfulness awareness is to enable the mind to “discern” the nature of the mind itself, awakening the person and leading him/her to insights into which prejudices and emotional reactions are embodied in the thought and in the reflective answers, which cause inner distress. The training process to awareness may lead to achievement of mindful awareness.
This may allow the student to deactivate the automatisms, reducing the use of top–down modality and inducing a mindful approach to clinical experience.19
A limitation of this study is the relatively small sample. It would be useful to expand it in further studies.
Moreover, the experience of the role plays and of the feedback from the conductor were described in the students’ written reports as enabling major reflective skills and a deeper insight of their observational capacities. They reported how they struggled to be in the relationship with the patient without judging or immediately categorizing what they were observing. The following are some qualitative answers regarding the students’ first experience:
Seeing myself in the video, I noticed my postural rigidity and the stiffness in my voice when I addressed a fellow/patient, while playing the role of the therapist; this attitude had already been pointed out by the observers during the feedback. This made me think about how much anxiety related to what was going to happen prevented me from being emotionally attuned.
Another student wrote: “Only after listening to the observers’ feedback, I realized that I was not able to change according to the child’s needs”. A third student said:
I was sure I had paid attention to the environment, I had been sensitive to changes and I had been able to focus on the other’s needs, but maybe when I started I was too confident and I realized that, though I tried to do well, I was emotionally absent.
Furthermore, at the end of the experience, a whole group of students reported as follows:
Playing the role of the therapist, the biggest difficulty was adjusting to the characteristics of the fellow who was playing the role of the child. These first experiences turned out to be fundamental to start to become aware of one’s own ability to feel, but we realized that the process of awareness needs to continue the role playing for a longer time.
The results seem to confirm the initial hypothesis regarding the possibility of training the student to relate with awareness and in a reflective way. This might have a positive effect on future clinical practice, guiding the therapist in establishing a correct relationship with the patient.
Siegel5 claims that a mindful approach is demonstrated to be an effective therapeutic approach and that the mindful position of the therapist plays a very important role in treatment effectiveness. Our research needs to be widened to a larger sample of students, but our first results supported the proposal of using a mindful approach while teaching future child neuro–psychomotor therapists. Moreover, students’ personal training experience should be measured and verified over time.
Going back to the main aims of this study, students’ degree of awareness evolves over a long period of time. A longer longitudinal study is needed to confirm the positive trend of the students’ acquisition of mindful skills, which represents a slow learning process, necessary to facilitate the growth of communicative skills.
Disclosure
The authors report no conflicts of interest in this work.
References
Brown KW, Ryan RM. The benefits of being present: mindfulness and its role in psychological well-being. J Pers Soc Psychol. 2003;84(4):822–848. | ||
Kabat J, Zinn J. Full Catastrophe Living: Using the Wisdom of Your Mind and Body to Face Stress, Pain and Illness. New York: Delacorte; 1990. | ||
Linehan MM. Cognitive of Borderline Personality Disorder. New York: Guilford; 1993. | ||
Marlatt GA, Kristeller JL. Mindfulness and Meditation in Integrative Spirituality into Treatment. Washington DC: American Psychological Association; 1999. | ||
Siegel D. The Mindful Brain: Reflection and Atonement in the Cultivation of Well-Being. New York City: WW Norton; 2007. | ||
Epstein R, Siegel DJ, Silberman J. Self-monitoring in clinical practice: a challenge for medical educators. J Contin Educ Health Prof. 2008;28(1):5–13. | ||
Massa R. La clinica della formazione. Milano: Franco Angeli; 1992. | ||
Baer RA, Smith GT, Lykins E, et al. Construct validity of the five facet mindfulness questionnaire in meditating and non meditating samples. Assessment. 2008;15(3):329–342. | ||
Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment method to explore facet of mindfulness. Assessment. 2006;13(1):27–45. | ||
Mezirow, J. Education for Perspective Transformation: Women’s Reentry Programs in Community Colleges. New York: Center for Adult Education, Teachers College, Columbia University, 1978. | ||
Fryer E, Arnold KR, Baile W, Tulsky J, Petracca F, Back A. Reflective teaching practices: an approach to teaching communication skills in a small group setting. Acad Med. 2006;81(7):638–644. | ||
Schön D. The Reflective Practitioner. New York: Basic Books; 1983. | ||
Schön D. Educating the Reflective Practitioner. San Francisco: Jossey-Bass; 1988. | ||
Chan CS, Wun YT, Cheung A, et al. Communication skill of general practitioners: any room for improvement? How much can it be improved? Med Educ. 2003;37(6):514–526. | ||
Croft P, White D, Wiskin C, Allan T. Evaluation by dentals students of a communication skills course using professional role-players in a UK school of dentistry. Eur J Dent Educ. 2005;9(1):2–9. | ||
Tiuraniemi J, Hatakka M, Keskinen E. Psychology students’ self-assessment of their professional skills: a Finnish case. Nord Psychol. 2008;60:267–282. | ||
Tiuraniemi J, Läärä R, Kyrö T, Lindeman S. Medical and psychology students’ self-assessed communication skills: a pilot study. Patient Educ Couns. 2011;83(2):152–157. | ||
Siegel D. The Developing Mind: How Relationships and the Brain Interact to Shape Who We Are. New York: Guilford; 2001. | ||
Baer RA. Mindfulness training as a clinical intervention: a conceptual and empirical review. Clin Psychol Sci Pract. 2003;10(2):125–143. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.