Back to Journals » Advances in Medical Education and Practice » Volume 13
Millennials Medical Students Generation at the Crosswalks: Motivations and Attitudes Towards Study and Future Career – A Mixed-Method Study
Authors Gillissen A ![]() , Kochanek T
, Kochanek T ![]() , Zupanic M, Ehlers JP
, Zupanic M, Ehlers JP ![]()
Received 6 April 2022
Accepted for publication 22 September 2022
Published 17 October 2022 Volume 2022:13 Pages 1305—1319
DOI https://doi.org/10.2147/AMEP.S368128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Video abstract presented by Adrian Gillissen.
Views: 80
Adrian Gillissen,1 Tonja Kochanek,1 Michaela Zupanic,2 Jan P Ehlers1
1Institute for Didactics and Educational Research in Health Care, Department of Medicine, Faculty of Health, Witten/Herdecke University, Witten, Germany; 2Interprofessional and Collaborative Didactics in Medicine- and Health professions, Department of Medicine, Faculty of Health, Witten/Herdecke University, Witten, Germany
Correspondence: Adrian Gillissen, Institute for Didactics and Educational Research in Health Care, Department of Medicine, Faculty of Health, Witten/Herdecke University, Alfred-Herrhausen-Straße 50, Witten, 58455, Germany, Email [email protected]
Background and Objectives: The aim of this study was to investigate in the millennium medical student generation the influence of the curriculum (problem-based curriculum [PBC] vs science-based curriculum [SBC]), gender and semester level on medical students’ motives to study medicine, their attitudes toward their career and in this regard their view about their study condition in university.
Methods: Semi-structured qualitative interviews with 28 medical students were performed and analyzed using Mayring’s content analysis. Based on these results, a quantitative questionnaire for a nationwide survey was developed using a mixed-method-approach and send to most medical faculties in Germany. Data from n=1053 students entered statistical analysis.
Results: Humanistic ideals prevailed in the choice to enter medical school and to become a physician. PBC students were found to be significantly (p< 0.001) more idealistic and patient oriented, and they regard their curriculum more competitive than SBC-students (p< 0.001). A balanced work and family life is essential for all students but particularly important for the PBC – group, male and undergraduate students. The majority of students wanted to work with patients and omitted patient-distant line of work. Undergraduate SBC-students saw their studies as old-fashioned citing lack of patient contact (p< 0.001 compared to PBC), which eased in the graduate study part.
Conclusion: This study found major differences in student’s perceptions depending on curriculum type. PBC-students were more idealistic, and humanistic ideals prevailed in comparison to SBC. For both, close patient contact is essential in their training. Particularly for female students, lifestyle factors and a balanced work-life-integration outweigh career ambitiousness. This study offers an important insight to policy makers and educators to understand the motivation and perceptions of the millennial student generation regarding their studies and future career plans, which should be considered in educational policies.
Keywords: medical students, career expectations, perceptions
Introduction
Medical professionalism including professional behavior towards patients have been increasingly emphasized in medical school curricula. Good interpersonal skills, knowledge and empathy of healthcare professionals toward patients ultimately lead a positive impact on patient satisfaction, compliance to treatment and care outcomes.1–3 Besides humanistic reasoning and empathy, motivation is a determining factor to affect these professional skills, once it guides and sustains such goal-oriented activities.4,5 The Self-Determination Theory, distinguishes between the intrinsic motivation, when activities are based on genuine interest, and controlled motivation, when external factors are the main driving motivational force.6 Intrinsic motivated students have more deep study strategy, more self-study hours, better academic performance and lower exhaustion from studies.7 As an independent variable, motivation affects the choice of medicine and the specialty within medicine and intention to excel in medical study, and it can be manipulated by medical educators.8 Externally generated motives were associated with less favorable learning behaviors. Lower motivation leads more often to burnout, lower quality of live, self-efficacy and inferior test scores.9 Motivators for a career in health care are humanitarian ideals, societal views (job opportunities, prestige, job security), medical background of family members and scientific reasons (curiosity in scientific and medical knowledge, academia, specific medical subspecialities).10–12 Students’ motivation is based on the pursuit of different levels of needs following the Maslow’s hierarchy.13 Levels of student’s motivation has been investigated at different phases of medical education finding highest motivation scores in early semesters.14,15 Although education environment like educational contexts and teachers’ autonomy-support influence motivation levels, studies to compare students’ motivation in association with their curriculum type are rare and motivational processes are substantially undervalued in curriculum development.16–18 A Brazilian study comparing motivation of students from a traditional with those studying a reformed curriculum found significant higher motivation levels in the latter, which persisted over the whole study period.17 The switch away from the traditional curriculum reduced the medical students’ levels of anxiety, improved students’ metacognitive processing capacity and self-regulated learning skills.19,20 Knowing the different determinants and effects of motivation, educators can initiate interventions that motivate students to engage more successfully in their studies, resulting in more to positive outcomes not only profiting themselves but also their patients.16
For centuries, students in Germany were taught a traditional science-based curriculum (SBC), starting in the first 2 (undergraduate = preclinical part) years with courses such as physics, chemistry and anatomy, lacking direct patient contact. The notion for this diachronic founded approach is, that formal analytic reasoning which is integral to the natural sciences, should hold pride of place in the intellectual training of physicians.21 During the next (graduate = clinical part) 4 years patient contact intensifies stepwise. In the 80s, the private University Witten-Herdecke introduced a problem-based constructivist model instructional curriculum (PBC), which was around 2000s adapted also by some state universities.22 In there, medical students are introduced to early patient contact already in the undergraduate part of their study, learning communication skills and clinical examination in the pre-clinical years with the purpose of gaining early clinical experience in combination with basic medical knowledge. This gives the unique opportunity to build a comprehensive structural model for personal identity of the millennial medical student generation by identifying various compounding factors, which also includes the curriculum type how their motivation regarding aspects of medical professionalism is evolved. With this body of knowledge, a desirable professional identity in these students can be formulated.
Aim and Research Questions
This study investigated millennial medical students of all 12 semesters – beginning with the first year (undergraduate) to the final (6th) year (graduate) – perceptions on professionalism, their motives to study medicine and their career plans. The primary aim of this study was twice:
- The motives to study medicine and their view about their study condition in university.
- The individual conceptualizations as well as the expectations towards their studies in university and how they pursue their professional career in medicine.
The secondary aim of this study was to verify whether there are significant confounders, such as gender, study curriculum and semester levels respectively. Based on the existing literature, we expected to find differences in attitudes regarding gender and semester level.23–25
Methods
This study uses an exploratory sequential mixed-method design, in which the information collected in the first qualitative phase (phase A) was then integrated into the second phase (phase B) consisting of a quantitative internet-based survey to affirm or dismiss the results from the qualitative part quantitatively.26–28
Phase A
A thorough literature search was carried out to collect themes students relate to medical professionalism with the focus on students’ motives to study medicine, their motivations in medical studies and perceptions to become a medical doctor. We used the definition of medical professionalism as described elsewhere.29,30 The following themes were extracted:
- The motive to become a physician, specifics of their studies while being at their respective university,
- Learning habits as an undergraduate and graduate student,
- Their career expectations and future challenges,
- Their personal anticipation being an intern, and
- How to balance their private life with the intended career path.
Two focused think-aloud discussions among the authors were performed a) until an agreement regarding the extracted themes from the literature, and b) in order to test and adjust the interview guide appropriately. Ill-defined questions and redundancies were clarified, and the guide revised accordingly. Based on this consent procedure, a semi-structured interview template with four themes including six subcategories was constructed:
- Personal expectations regarding a) their time as a student and b) becoming a physician.
- Learning habits and challenges.
- Medical aspects (individual thoughts, error management).
- Digital medicine (individual notion, friend or foe in patient care).
Each category/subcategory consisted of one major questions given to the interviewees. Depending on the category up to seven adjunct questions were asked as a stimulus, if needed. The questions stimulated the respondents to talk freely. This safeguarded a systematic and comprehensive assessment of attitudes, apprehensions and expectations regarding the medical training. Although the interview touches broader issues, only aspects relevant for the above outlined research questions were included in this analysis. Using this methodological approach the semi-structured interview form for a thematic analysis was chosen, as described earlier.31
The first author conducted the semi-structured interviews between November 2019 and March 2020. The interviews took place face-to-face (n=9) at the University Witten-Herdecke and at the Kreiskliniken Reutlingen – Ermstalklinik, Germany, or over the phone (n=19). All interviews, which lasted about 30 minutes, were electronically audio recorded and transcribed verbatim (Table 1). All the quotations in this paper were translated into English language and were double-checked by back translation as described earlier.32 Reporting complied the consolidated criteria for reporting qualitative studies 32-item checklist (COREQ).33 Participants were students of various semesters in German medical faculties of private or state universities. The participants were selected consecutively by chance using in part snowball until theoretical saturation of the answers had been reached. The authors approached most participants by email, some personally by the authors, and some by phone.
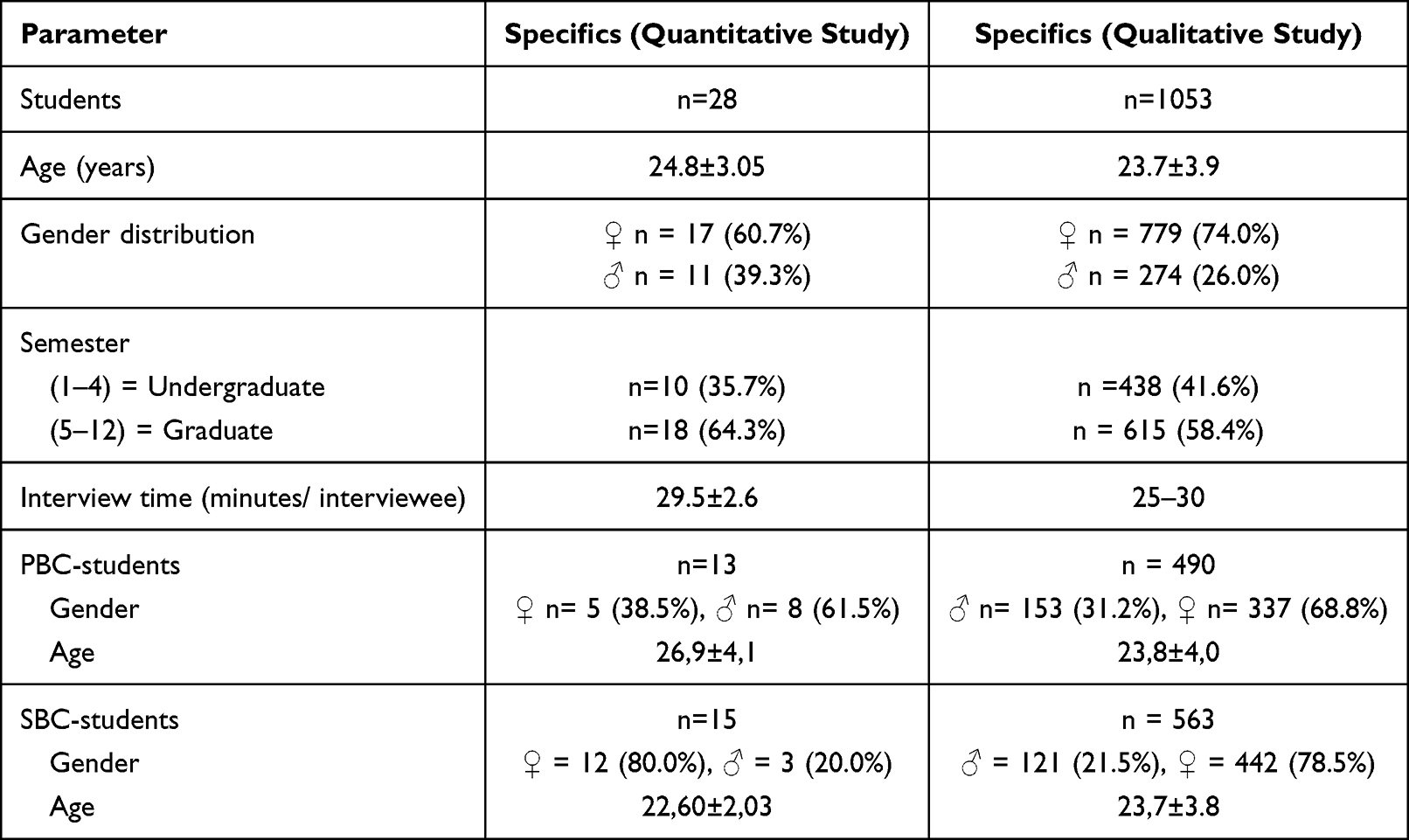 |
Table 1 Baseline Data of Interviewees. All Professions and Activities Lasted ≥6 Months. Direct Transition Means = No Time Lost Between High School Exam and Entering University |
The only inclusion criterion was, that students must be actively study medicine in one of the German universities. They studied in the German universities of Aachen, Bonn, Heidelberg, Rostock or Witten-Herdecke; 27 were Germans, one from Austria. The age of the interviewees was between 19 and 34 years (24.6±3.1).
Phase B
Mixed methods analytical techniques with a sequential exploratory strategy were used to collect qualitative data to identify key concepts subsequently measured in an online survey.34,35
Development of the Quantitative Survey Instrument
Every item that was mentioned in more than twice in the qualitative interviews of part A, was translated into a question. All questions were reviewed by the authors for content validity.36,37 This is seen as an objective judgment about the construct of an instrument, which indicates the instrument’s relevance to the study’s aim, how to express phrases, the wording of questions, and understanding the researcher’s intended concept.38,39 The items were then refined through another author’s group discussion, and the outcome was tested through a pilot study with 4 students from preclinical and clinical settings to understand how they perceive the subject of interest to finalize the list of items. Comments and suggestions were added, overlaps were avoided, resulting in the final construct of questions.
Response to the Qualitative Survey
The online survey was sent to all medical faculties in Germany from which most forwarded the survey invitation by email to about 80000 medical students. Each contained an invitation letter and an information sheet. As an incentive, we offered 280 Amazon vouchers each 25€ per completed survey which were distributed by way of a lottery.
Data Analysis
In Phase A, the quotations were first identified as expressions of a particular factor and further categorized into the sub-themes. To increase inter- and intra-coder reliability, the authors performed the analysis of the transcribed interviews independently. An inductive content analysis was performed using Mayring’s principles as also exploited by others.40,41 From the research question, a theoretical based definition of the aspects of analysis, main categories including sub categories were formulated, which leads to coding rules of those categories. The categories were collected in an open coding agenda using the software Quirkos (www.quirkos.com), and eventually revised and formative checked for reliability within the coding process in repetitive discussions until consensus was reached (investigator triangulation). Thus, individual phases and passages summarized into one code. The final working through the texts were again checked for reliability. Prototypical text passages, categorical definitions, and rules to discern the categories were formulated. The material was completed systematically step by step and revised within the process of analysis. Using this methodological approach, the authors followed quantitative inquiry approaches, which is also the cornerstone of grounded theory.42 However, instead of generating a formal theory, the intention of this qualitative content analysis was to use the results to develop a protocol, which was incorporated into a questionnaire of a quantitative inquiry (Phase B).
The authors developed a quotation tree during the transcription of the interviews, consisting of three main categories (Figure 1 Supplement):
- Students’ choice.
- Career options.
- Study related statements.
Likert scale questions (ranging from 0=decline/do not know to 7=completely agree), questions with a percent scale from 0 to 100 and questions with the option of three answers (do not know, false, fully agree) were used. An item was considered a “firm perception” when the mean response was within one-third of the lowest/highest possible answer scores. Statistical analysis was performed in the quantitative study part using SPSS (V27). Only complete data sets were analyzed. Data sets being prematurely terminated by the students were omitted. Descriptive statistics were used to summarize student demographic data. Cronbach’s alpha was calculated to assess internal consistency of categories of professional behavior in the students’ choice paragraph (Table 2). Mann–Whitney-U-Tests were used to compare the responses relating to perceptions. Group comparators were curriculum type, gender and semester levels. Pearson correlation coefficient was calculated to compare students’ socio-humanistic attitudes towards their intention to a career in medicine. For the determination of work schedule preferences between student groups, the Chi-Square test was used. A p-value of less than 0.05 was considered statistically significant.
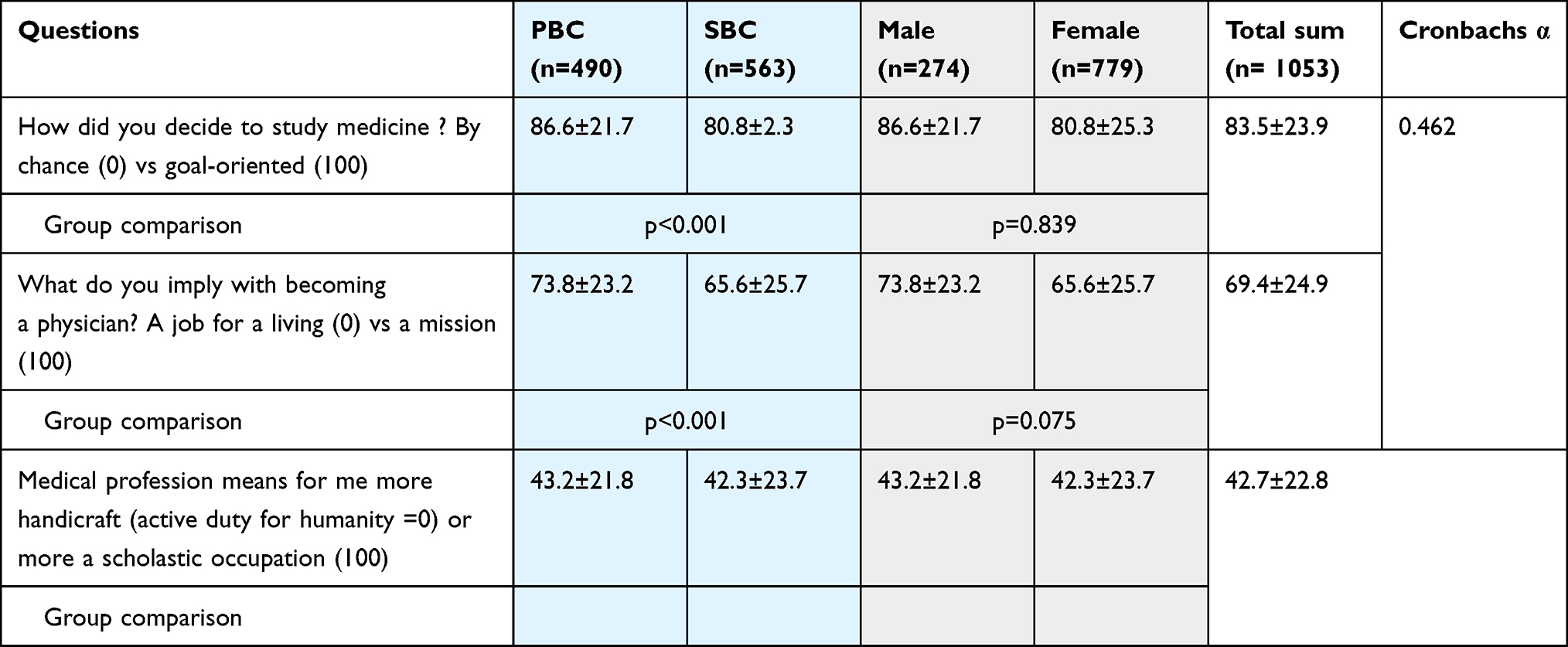 |
Table 2 Incentive to Study Medicine and Vision |
Ethics
Informed consent confirmed voluntarily participation of each individual participant at the beginning of the survey. All participants of the qualitative study part agreed to the audio recording, either verbally or in written form. By designating each student a code through a computerized assignment system, anonymity, confidentiality and data security was guaranteed. Prior to the first interview ethical approval for the study from the University Faculty of Medicine and Dentistry Committee for Ethics at the University Witten-Herdecke (#137/2919), Germany were obtained.
Results
For phase A 17 women and 11 men were recruited. Thirteen students came from a university with a problem-based curriculum (PBC) and 15 were taught with a science-based focus (SBC). In phase B 1053 questionnaires were analyzed. The response proportion was ca. 1.3%. In both study phases women prevailed which roughly represents the gender distribution in German medical schools (2020/2021: male 36.8%, female 63.2%, https://de.statista.com, July 02, 2022). Table 1 summarizes the baseline characteristics of all participants.
Student’s Choice
In the qualitative study part, social and humanistic reasoning prevailed as the major motive to study medicine, like wishing to help patients, to heal diseases, compassionateness besides the fascination of understanding the scientific foundation of underlying diseases. All of the students gave statements like.
“It is fascinating to work with humans, share their grief, and to deal with their emotions”.
Some patients expressed socio-economic centered motives like job security and broad professional job opportunities, or they were unable to give a concrete reason, had simply luck in the state-run distribution system or – in one case and due to an indecisiveness – medicine was chosen because “a close friend suggested it”.
On average 80% of students in the quantitative study part made their decision to become a physician goal oriented before applying for a place at a medical college (Table 2). 86.6±21.7% of PBC-students vs 80.8±21.3% of SBC-students (p<0.001) decided to study medicine in a goal-oriented manner. Although all students favor a humanistic reasons over economic motivations for becoming a physician, clearly PBC-students dominate in this reasoning over SBC-students (73.8±23.2% vs 65.6±25.7%, p<0.001, Table 2). For PBC-students medical profession is more an active duty for humanity than a scholastic occupation compared to the SBC-group (43.2±21.8 to 42.3±23.7, p<0.001, Table 2). We found no gender differences. When asked whether they perceived the medical profession primarily as a service for humans or as a somewhat detached scholarly activity, students had a quite balanced view although tending to the first. Pearson correlation coefficient revealed that goal-oriented modus operandi to apply for a place in medical college correlated significantly (although with a low correlation coefficient) with social and humanistic attitudes towards the profession. Factors like the desire for helping people and the ability to provide healing and support correlated clearly with social and humanistic attitude (depending on the comparison p<0.0001 or p=0.036, Table 3).
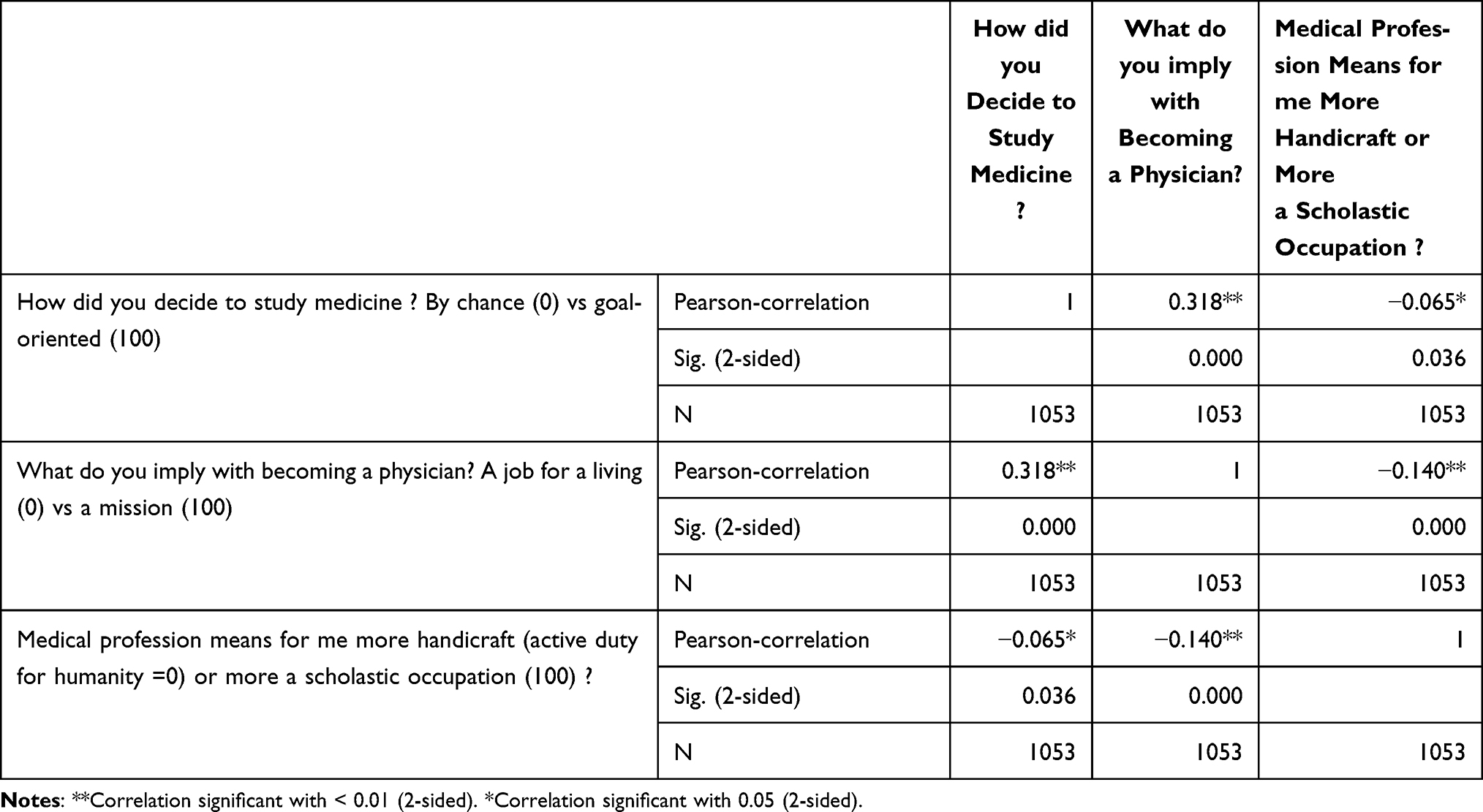 |
Table 3 Pearson Correlations Coefficient. There is a Strong Correlation Between the Decision to Become a Doctor, Socio-Humanistic Attitude Towards the Medical Profession and Empathy. Sig = Significance. Numbers in Parenthesis in the First Column = Rating Points Interviewees Could Give in Selected Question |
Career Options
Most students start medical school with some idea about a specialty choice and most of them articulated at least some preferences when specifically asked. Even those with a strong preference acknowledged that the career preference might be subject to change with further training.
After medical school, almost all graduates planned to start residency training in hospitals for learning purposes. Ultimately, most students from both groups saw their future in a private practice either as a general practitioner or as a specialized private practitioner (eg in psychiatry, pediatrics, dermatology). The following reasons were given: personal decision-making authority in contrast of staying low in “the food chain” when working in a hospital, better for family planning, lack of shift work, having free weekends, and relatively independence from others including a superordinate administration.
In the first years [after graduating] I definitely see myself in the clinic. To do really good medicine and to learn a lot. But I think it’s quite likely that I’ll switch to a private practice later on. (PBC, WH805)
Working in a team rather to be alone, care of challenging cases, and intense medical training provided in hospitals were reasons for that decision. The responses from the individual interviews nicely matched with the data from the qualitative study part. Students clearly preferred to do patient care, preferably in the hospital, but also as a family doctor in a practice (Likert scale about 5 vs about 4, Table 4). This was more noticeable in the PBC- and in the graduate student group choosing a Liker rating >5 (Table 4). Patient remote activities (eg laboratory work, pathology, pharmaceutical industry, government institutions) were from minor interest (Liker rating ≤3), although male students preferred those more, than female students (p<0.001). Differences between PBC/SBC or graduation level were not found (Table 4). These attitudes prevailed even when asked for their long-term (>15 years after graduation) career plans. An academic career is perceived as an equivalent option to working in a non-academic hospital or as a family doctor, although female students preferred the private practices (mean Likert scale 4.8±1.7 vs 5.3±1.5, p<0.01) because of the assumed and desired lower working hours (Table 4, Table 1 Supplement, Figure 1).
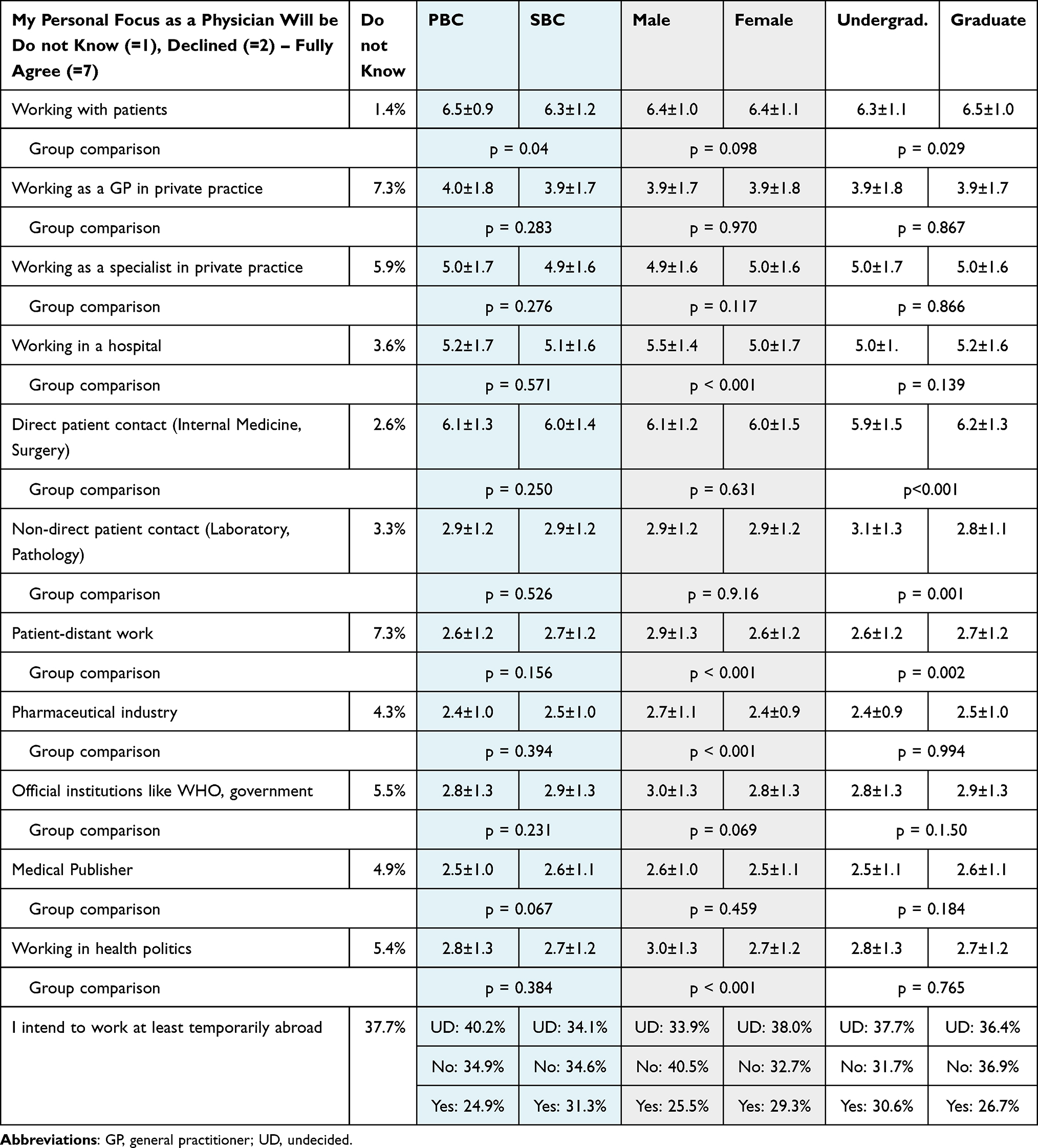 |
Table 4 Preferred Working Condition and Career Directly After Graduating from University |
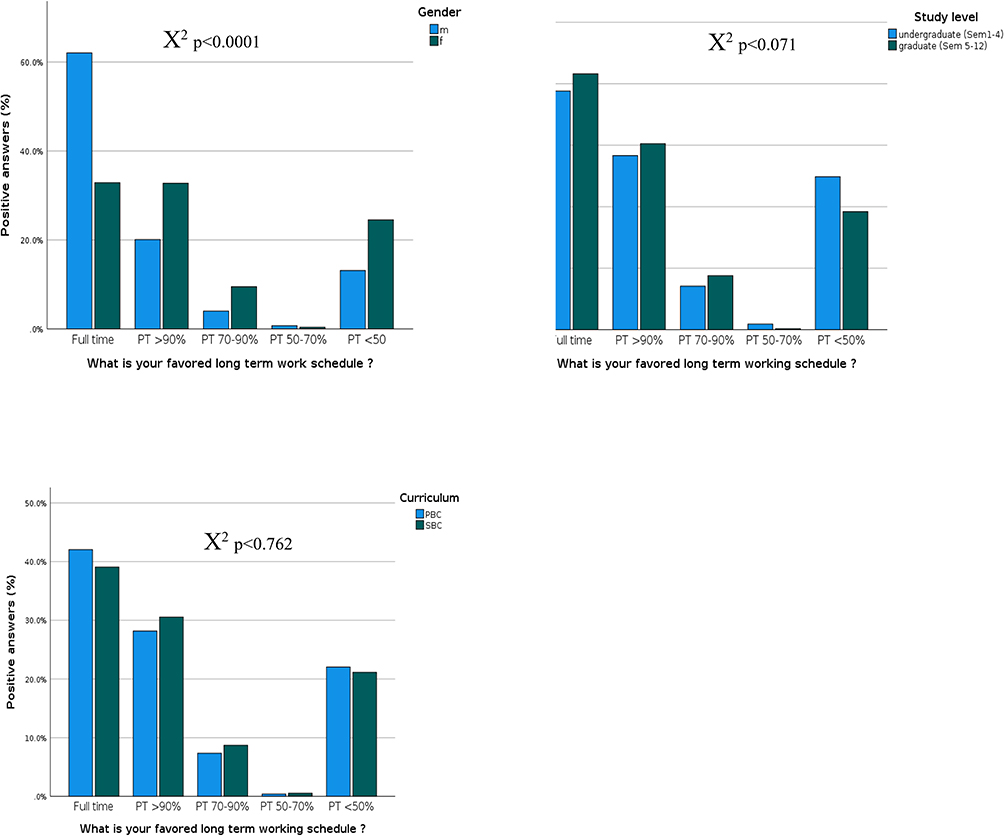 |
Figure 1 Men mostly favor full time job assignments while women prefer part time jobs in the long run. Regardless of curriculum type or study level about 20% favor part time jobs with <50% working schedules. Abbreviations: PT, part time; m, male; f, female; sem, semester; PBC, problem-based curriculum; SBC, science-based curriculum. |
Regardless of gender, curriculum type or graduate level 60% to 70% of the students preferred a well-adjusted balance of family, lifestyle, profession and business, although PBC-students (0–100 rating: PBC 39.3±24.7 vs SBC 34.5±22.8, p=0.01), male students (male 41.5±26.3 vs female 35.0±22.6, p=0.01) and undergraduate students (undergraduate 39.8±23.5 vs graduate 34.5±23.8, p<0.001, Table 2 Supplement) all rate the professional engagement over the work-life-balance significantly higher than their comparators respectively. Although indicating their earnestness to engage themselves in the medical field, >50% were unwilling to let their work dominate their private live. Family allegiance and sufficient spare time had a high priority (Table 2 Supplement). Other desired work specifications for of all interviewees were (rating in Liker scale ≥4.3): pleasure at work, good learning opportunities, adoption of responsibility and job security, but not necessarily high wages (Table 3 Supplement).
Study Related Statements
In the first part of this study, students expressed the desire to go deeper into the curriculum in order to get the best training and therefore the foremost foundation to become a good health professional. The SBC- but not the PBS-group expressed their concerns that the curriculum is too science-based and lacks practical bearing necessary for the management of patients.
… I wish, we had more practical courses, because we were taught from time to time in hospitals but without seeing patients. Otherwise we are standing somewhat shaky in front of real patients in medical clerkship.
The quantitative data confirmed that SBC-students regard PBC as clinically more applicable. Graduate students accented this notion particularly (p<0.001). Non-curricular study properties like socialization and fun are rated equally important to medical training in all groups, and women significantly prefer flexible study hours (p<0.001, Table 4 Supplement), which matches nicely with their higher ratings for a good work-life-balance (p<0.01, Table 2 Supplement) compared to their male counterparts.
Perceptions about different aspects of the study varied considerably between the three groups. While PBC is characterized by frequent patient interaction in undergraduate level, and students enjoy a holistic teaching approach, SBC students wished the same but perceived the first two study years as more clinically distant (0 = early patient contact to 100 = clinically distant rating: PBC 47.7±26.4 vs SBC 57.6±27.7, p<0.001), regard them comparably old fashioned (0 = old fashioned to 100 = modern: rating: PBC 67.0±23.0 vs SBC 47.0±22.5, p<0.001) and as a less competitive in medical training (rating: PBC competitiveness 72.1±21.7 vs SBC competitiveness 47.0±22.5, p<0.001). PBC-, male- and undergraduate students rated their relationship to the faculty significantly better than their respective counterparts (Table 5).
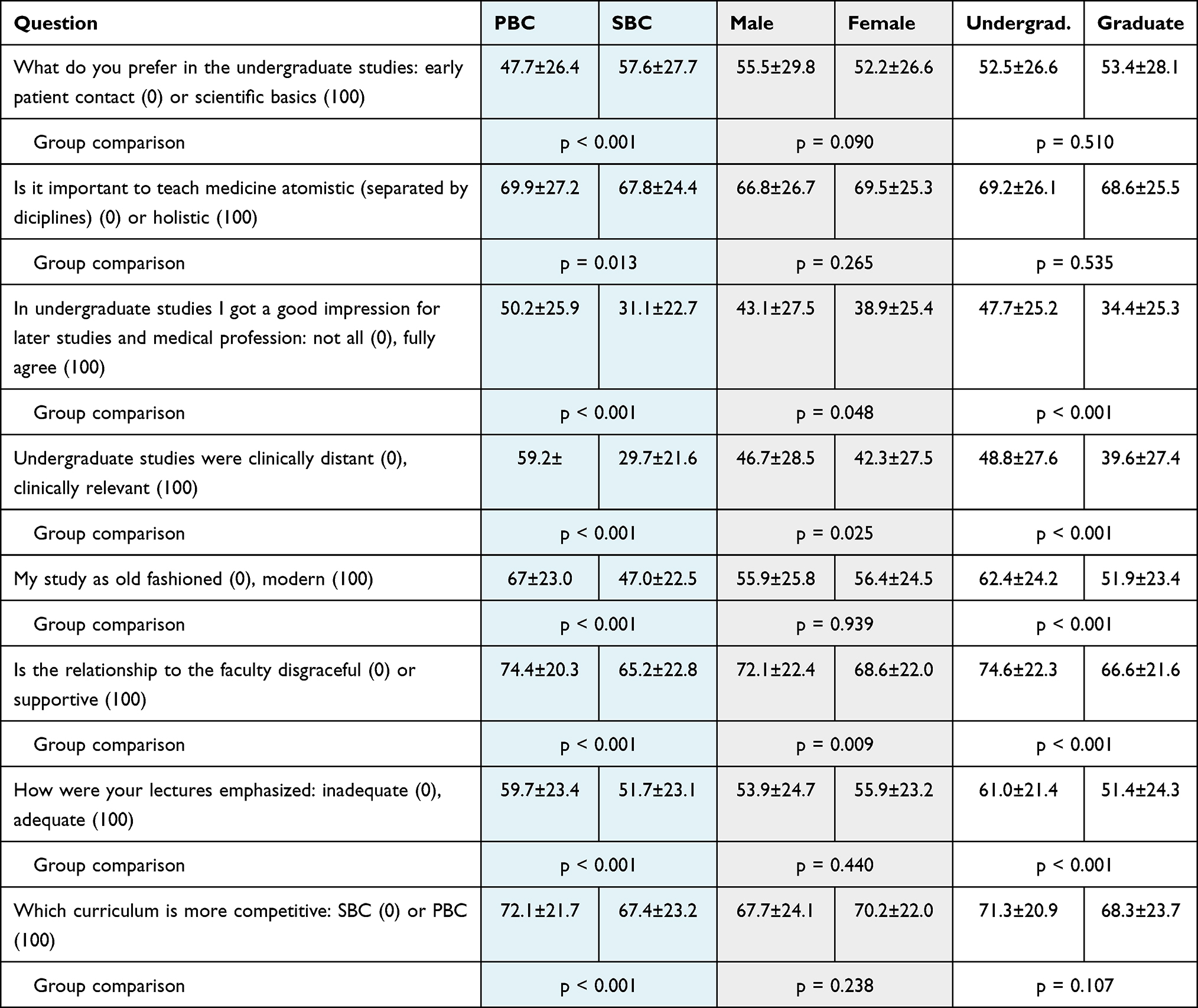 |
Table 5 Medical Students’ Perceptions Toward Their Studies as a Good or Bad Preparation for Becoming a Medical Doctor |
Discussion
This study consists of an exploratory part (phase A), which served as a template for a quantitative questionnaire (phase B) to explore the motivation of the millennials generation medical students towards key aspects of medical professionalism. The findings extracted from the second study phase validated the results from the first phase.27
Students’ Choice
Before the 19th century, women were considered unable to be doctors, which changed later gradually. In this study, women prevailed by almost 4:1 over men which is exceptionally high even compared to other recent surveys from developed countries. Many determining factors were cited for choosing the medical career such as interest in science and academia, social interest, but also socio-economic factors including flexible working hours and work independence, prestige, job and financial security, and interest in humanitarian topics.13,43,44 The qualitative part of this study validated this reasoning. The decision to study medicine was very much goal-oriented and had a strategic objective which has been reported earlier.45 In addition, this study found that PBC students had a significant higher intrinsic motivation to study medicine and associated their future engagement in healthcare more often with humanistic ideals than the SBC group. These perceptions was evenly distributed among sexes, which is in contrast to other studies stating higher motivation levels in females.46–48 Although speculative, these gender differences might be due to the heterogeneous study admission process for medical students in Germany. The admission is primarily based on high school GPA. But students can improve their acceptance chance with a cognitive test as well as an situational judgment tests and job experiences, which – however - are graded quite differently depending on the university.49,50 Once we recruited medical students in a nationwide survey, gender differences were probably diluted by this selection processes.
Medical students regard a balanced combination of academic workload as well as the absorption into a clinical environment with their private live essential for their well-being.51,52 An effective work–life balance protects against risks like anxiety, depression and stress.53 In this study, personal maturity, social contacts and pleasure at work were seen as equally important, and work–life-balance prevails over fascination for profession and career in PBC, male and undergraduate students even more than in the comparator groups respectively. However, when asked for their preferred working hours, more women than men wanted to work part time although a sizable proportion of men (39%) declined to work full time too, which is high in comparison to Japanese and Australian studies but similar to a surveys from Chicago and Germany.52,54–56
Career Options
The majority of the students from this study preferred direct patient contact for their future career path, which is in concordance with numerous studies in the past.57 This tendency increased in graduate level or with higher semester level.58 Male and female students expressed similar attitudes regarding the preferred work setting (GP, specialization), although the first favor hospital work at the beginning of their medical training more than the latter, the majority of all students aim for a private practice because of presumed flexible working hours as a GP. Curriculum or semester level had no influence on this attitude. In other European studies medical students’ career plans varies between becoming a family doctor (GP) or the desire to further specialize.59–62 Because students in the qualitative study part were undecided what subspeciality to choose and how they want to specialize in the future, claiming that they lacked the appropriate information or not having attended specific medical courses, we included questions of students’ attitudes of more general profession types like patient distant professions. Very clearly, a patient distant career option was not within the scope of almost all interviewees. Male students had in some of those professions statistically more positive attitudes than women. Tendency in favor of direct patient care in contrast to patient-distant careers mitigated even more with further study time. Working in the pharmaceutical industry or for a medical publisher was seen as least attractive. This aspect was only rarely investigated in the literature. But also job opportunities in eg pathology, in a laboratory or for administrative institutions (eg WHO) had a low priority and matched earlier reports.63,64
An academic career or research-oriented careers including entering a PhD program were seen as an equivalent options in this study. Significantly more PBC, male and undergraduate students expressed their interest in working in academia and research than their comparators. Besides non-minority status, male gender, lower debt at graduation, strong attitudes toward research at time of graduation, and greater social pressures also a patient – centered curriculum and study level are associated with a positive perception toward a career in medical research.65 Unexpectedly, less SBC-students wanted to pursue an academic career, which contradicted the results from the qualitative study part. In systematic reviews and a meta-analysis of 75 studies with almost 900,000 individuals performed in other developed countries, up to 80% of students expressed interested in academic work being higher than in this study.25,66
Study Related Statements
This study found significant differences between PBC and SBC students regarding their perceptions of the undergraduate study years. While PBC students enjoyed early patient contact and rate their relationships to faculty members high, SBC-students rated those first 2 year as old-fashioned, clinical distant and less competitive. These data hint a difference in students’ motivation depending on curriculum type. Studies studying the effect of different curriculum types on students’ motivations in studying medicine and learning are rare. Del-Ben et al (2019) found that students with the reformed curriculum (small group discussions, clinical activities with real patients, promoting active learning methods) had higher autonomous and controlled motivation than those of the traditional (science based, mainly lectures) curriculum.17 Clearly teaching methods can improve or weaken motivation levels. For example, the introduction of standardization in medical education, problem-based and learner-centered methodologies improved students’ cognitive and metacognitive processing.18
Limitations
This study has a few limitations: a) It covers a broad spectrum of different aspects regarded as important for professionalism building in medical students, but did not investigate each theme in depth as done as other investigations. b) The second part of the study was based on the results of the quantitative section omitting the use of validated questionnaires in specific areas of professionalism themes. c) The statements/questions may not reflect scientific clarity. The reason was that these statements and consequently the questions are based on the qualitative study part. This issue was addressed through a discussion of each item by the authors and by testing the questionnaire in a pilot study with students (see methods). d) although the questionnaire of the second study part was send to the majority of medical students in Germany, only a fraction replied bearing the risk of a selection bias. e) This study was carried out solely in Germany and as such not necessarily mirroring students’ perceptions in other countries or regions, although the comparison with comparable studies done in other developed countries revealed, depending on subthemes of professionalism, similar results.58,67
Conclusion
In this study for the first time to the authors’ knowledge, the influence of curriculum type, gender and educational level was investigated in parallel on professionalism forming in medical students. Important themes students were aware of, included their specific intention why they choose to study medicine, educational specifics of the curriculum, career expectations including thoughts of work-life-balance and attitudes towards becoming a “good doctor”. Students expressed clear thoughts about central aspects of medical professionalism also in undergraduate level, which matched with their focused strategy to get admitted to medical studies. Humanistic ideals prevailed in the choice to enter medical school and to become a physician. PBC students were found to be more idealistic and patient oriented as well as more “faculty supportive”. They consider their curriculum more competitive. Gender differences comprised on the acceptance of more working hours but also being more flexible in accepting a patient-distant line of work. Undergraduate SBC students saw their medical studies as old-fashioned citing lack of patient contact. This however, mitigated in the graduate study part. A balanced work, family and lifestyle was essential for all students. Predominantly women but also almost 40% of the men desired part-time engagements. Obviously, medical students who represent the coming generation of physicians have very distinctive thoughts about their medical training, their time in university, their professional career and achieving a satisfactory work-life effectiveness.
This study offers in important insight to policy makers and educators to understand the motivation and perceptions of the millennial generation to accommodate educational policies in university and later with the beginning of medical training and specialization.
Ethics Approval and Consent to Participate
Every participant confirmed informal consent at the beginning of the survey. All participants of the qualitative study part agreed to the audio recording, either verbally or in written form. The study was performed in accordance with the Declarations of Helsinki. Confidentiality was warranted through an anonymization process. Ethical approval of the study was obtained prior to the first interview from the University Faculty of Medicine and Dentistry Committee for Ethics at the University Witten-Herdecke (# 137/2919).
Author Statements
All co-authors authorize Adrian Gillissen to submit the research article. A. Gillissen, T. Kochanek, M. Zupanic and J. Ehlers are the sole authors of the article and are legally able and entitled to submit the article and authorize Dove Medical Press (DMP) to publish the research article. We, the authors certify, that the research article is original, has not already been published in any other journal (medical, or otherwise) or is not currently under consideration for publication by another journal, and does not infringe any existing copyright or any other rights prescribed by law. The article contains nothing that is unlawful, defamatory, or which would, if published, constitute a breach of contract or of confidentiality. Due care, diligence and all other requisite investigations were carried out in the preparation of the research article to ensure its accuracy. To the best of our knowledge, all statements contained in it purporting to be factual are true and correct.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Kreiskliniken Reutlingen GmbH, Reutlingen, Germany. Grant No.: UW/H 11.540.
Disclosure
The authors declare that they have no competing interests.
References
1. Hojat M, Vergare M, Isenberg G, Cohen M, Spandorfer J. Underlying construct of empathy, optimism, and burnout in medical students. Int J Med Educ. 2015;6:12–16. doi:10.5116/ijme.54c3.60cd
2. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet Lond Engl. 2010;376(9756):1923–1958.
3. Birden H, Glass N, Wilson I, Harrison M, Usherwood T, Nass D. Defining professionalism in medical education: a systematic review. Med Teach. 2014;36(1):47–61.
4. Cui X, Ding N, Jiang N, Li H, Wen D. Preliminary study of the relationship between career choice motivation and understanding of professionalism in newly enrolled medical students in China: a cross-sectional study. BMJ Open. 2021;11(2):e041860.
5. Schulte-Uentrop L, Cronje JS, Zöllner C, Kubitz JC, Sehner S, Moll-Khosrawi P. Correlation of medical students’ situational motivation and performance of non-technical skills during simulation-based emergency training. BMC Med Educ. 2020;20(1):351.
6. Howard JL, Bureau J, Guay F, Chong JXY, Ryan RM. Student motivation and associated outcomes: a meta-analysis from self-determination theory. Perspect Psychol Sci J Assoc Psychol Sci. 2021;16(6):1300–1323.
7. Kusurkar RA, Ten Cate TJ, Vos CMP, Westers P, Croiset G. How motivation affects academic performance: a structural equation modelling analysis. Adv Health Sci Educ Theory Pract. 2013;18(1):57–69.
8. Kusurkar RA, Croiset G, Ten Cate TJ. Twelve tips to stimulate intrinsic motivation in students through autonomy-supportive classroom teaching derived from self-determination theory. Med Teach. 2011;33(12):978–982.
9. Lyndon MP, Henning MA, Alyami H, et al. Burnout, quality of life, motivation, and academic achievement among medical students: a person-oriented approach. Perspect Med Educ. 2017;6(2):108–114.
10. Khamees A, Awadi S, Al Sharie S, et al. Factors affecting medical student’s decision in choosing a future career specialty: a cross-sectional study. Ann Med Surg. 2022;74:103305.
11. Hao KA, Fu S, Islam S, et al. Medical student career choice: who is the influencer? J Surg Res. 2022;272:9–16.
12. Kusurkar RA, Ten Cate TJ, van Asperen M, Croiset G. Motivation as an independent and a dependent variable in medical education: a review of the literature. Med Teach. 2011;33(5):e242–e262.
13. Goel S, Angeli F, Dhirar N, Singla N, Ruwaard D. What motivates medical students to select medical studies: a systematic literature review. BMC Med Educ. 2018;18(1):16.
14. Kim KJ, Hwang JY, Kwon BS. Differences in medical students’ academic interest and performance across career choice motivations. Int J Med Educ. 2016;7:52–55.
15. Silva GMC, Da, Borges AR, Ezequiel O, da S, Lucchetti ALG, Lucchetti G. Comparison of students’ motivation at different phases of medical school. Rev Assoc Medica Bras. 2018;64(10):902–908.
16. Orsini C, Binnie VI, Wilson SL. Determinants and outcomes of motivation in health professions education: a systematic review based on self-determination theory. J Educ Eval Health Prof. 2016;13:19.
17. Del-Ben CM, Shuhama R, Costa MJ. Effect of changes to the formal curriculum on medical students’ motivation towards learning: a prospective cohort study. Sao Paulo Med J Rev Paul Med. 2019;137(2):112–118.
18. Kusurkar RA, Croiset G, Mann KV, Custers E, Ten Cate O. Have motivation theories guided the development and reform of medical education curricula? A review of the literature. Acad Med J Assoc Am Med Coll. 2012;87(6):735–743.
19. Zuardi AW, Prota FDG, Del-Ben CM. Reduction of the anxiety of medical students after curricular reform. Rev Bras Psiquiatr Sao Paulo Braz. 2008;30(2):136–138.
20. Turan S, Demirel O, Sayek I. Metacognitive awareness and self-regulated learning skills of medical students in different medical curricula. Med Teach. 2009;31(10):e477–e483.
21. Cooke M, Irby DM, Sullivan W, Ludmerer KM. American medical education 100 years after the Flexner report. N Engl J Med. 2006;355(13):1339–1344.
22. Kiessling C, Rotthoff T, Schnabel KP, Stosch C, Begenau J. 20 years of model curricula in German-speaking countries. GMS J Med Educ. 2019;36(5):Doc65.
23. Stockley AJ, Forbes K. Medical professionalism in the formal curriculum: 5th year medical students’ experiences. BMC Med Educ. 2014;14:259.
24. Monrouxe LV, Rees CE, Hu W. Differences in medical students’ explicit discourses of professionalism: acting, representing, becoming. Med Educ. 2011;45(6):585–602.
25. Janczukowicz J, Rees CE. Preclinical medical students’ understandings of academic and medical professionalism: visual analysis of mind maps. BMJ Open. 2017;7(8):e015897.
26. Onwuegbuzie AJ, Bustamante RM, Nelson JA. Mixed research as a tool for developing quantitative instruments. J Mix Methods Res. 2010;4(1):56–78.
27. Pluye P, Hong QN. Combining the power of stories and the power of numbers: mixed methods research and mixed studies reviews. Annu Rev Public Health. 2014;35:29–45.
28. Onwuegbuzie AJ, Slate JR, Leech NL, Collins KM. Conducting mixed analyses: a general typology. Int J Mult Res Approaches. 2007;1(1):4–17.
29. Kirk LM. Professionalism in medicine: definitions and considerations for teaching. Proc Bayl Univ Med Cent. 2007;20(1):13–16.
30. Epstein RM, Hundert EM. Defining and assessing professional competence. JAMA. 2002;287(2):226–235.
31. Busse TS, Jux C, Kernebeck S, et al. Participatory design of an electronic cross-facility health record (ECHR) System for pediatric palliative care: a think-aloud study. Child Basel Switz. 2021;8(10):839.
32. Lombardo L, Ehlers J, Lutz G. Is your mind set? - how are intra- and interpersonal competences dealt with in medical education? A multi-professional qualitative study. BMC Med Educ. 2019;19(1):317.
33. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357.
34. Curry LA, Krumholz HM, O’Cathain A, Plano Clark VL, Cherlin E, Bradley EH. Mixed methods in biomedical and health services research. Circ Cardiovasc Qual Outcomes. 2013;6(1):119–123.
35. Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs-principles and practices. Health Serv Res. 2013;48(6 Pt 2):2134–2156.
36. Cronbach LJ, Meehl PE. Construct validity in psychological tests. Psychol Bull. 1955;52(4):281–302.
37. Feißt M, Hennigs A, Heil J, et al. Refining scores based on patient reported outcomes - statistical and medical perspectives. BMC Med Res Methodol. 2019;19(1):167.
38. Drost E. Validity and reliability in social science research. Educ Res Perspectives. 2011;38:105–124.
39. Yazdi-Feyzabadi V, Nakhaee N, Mehrolhassani MH, Naghavi S, Homaie Rad E. Development and validation of a questionnaire to determine medical orders non-adherence: a sequential exploratory mixed-method study. BMC Health Serv Res. 2021;21(1):136.
40. Mayring P. Qualitative Inhaltsanalyse. In: Mey G, Mruck K, editors. Handbuch Qualitative Forschung in der Psychologie: Band 2: Designs und Verfahren. Springer Fachmedien; 2020:495–511.
41. Rahm AK, Töllner M, Hubert MO, et al. Effects of realistic e-learning cases on students’ learning motivation during COVID-19. PLoS One. 2021;16(4):e0249425.
42. Tavakol M, Torabi S, Akbar Zeinaloo A. Grounded theory in medical education research. Med Educ Online. 2006;11(1):4607.
43. Pelaccia T, Viau R. Motivation in medical education. Med Teach. 2017;39(2):136–140.
44. Artino AR, La Rochelle JS, Durning SJ. Second-year medical students’ motivational beliefs, emotions, and achievement. Med Educ. 2010;44(12):1203–1212.
45. Wouters A. Effects of medical school selection on student motivation: a PhD thesis report. Perspect Med Educ. 2018;7(1):54–57.
46. Al Ansari AM, Kumar AP, AlSaleh AFF, Arekat MRK, Deifalla A. Validation of academic motivation scale among medical students using factor analysis and structural equation modeling: middle Eastern perspective. J Educ Health Promot. 2021;10:364.
47. Vallerand RJ, Pelletier LG, Blais MR, Briere NM, Senecal C, Vallieres EF. The academic motivation scale: a measure of intrinsic, extrinsic, and amotivation in education. Educ Psychol Meas. 1992;52(4):1003–1017.
48. Becker J, Burghaus D, Kappes K, et al. Warum Medizin studieren? [Why medicine? Analyzing students' motives for studying medicin] DMW - Dtsch Med Wochenschr. 2015;140(21):e207–e216.
49. Hampe W, Hissbach J, Kadmon M, Kadmon G, Klusmann D, Scheutzel P. Wer wird ein guter Arzt? Verfahren zur Auswahl von Studierenden der Human- und Zahnmedizin [Who will be a good physician? Admission procedures for medical and dental students]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2009;52(8):821–830.
50. Kelly ME, Patterson F, O’Flynn S, Mulligan J, Murphy AW. A systematic review of stakeholder views of selection methods for medical schools admission. BMC Med Educ. 2018;18(1):139.
51. Hancke K, Igl W, Toth B, Bühren A, Ditsch N, Kreienberg R. Work-life balance of German gynecologists: a web-based survey on satisfaction with work and private life. Arch Gynecol Obstet. 2014;289(1):123–129.
52. Takahashi K, Nin T, Akano M, Hasuike Y, Iijima H, Suzuki K. Views of Japanese medical students on the work-life balance of female physicians. Int J Med Educ. 2017;8:165–169.
53. Picton A. Work-life balance in medical students: self-care in a culture of self-sacrifice. BMC Med Educ. 2021;21(1):8.
54. Jerg-Bretzke L, Krüsmann P, Traue HC, Limbrecht-Ecklundt K. Was ihr wollt, Ergebnisse einer empirischen Bedarfsanalyse zur Verbesserung der Vereinbarkeit von Familie und Beruf bei Ärztinnen und Ärzten [What you will”: Results of an Empirical Analysis of the Need to Improve Work-life Balance for Physicians]. Gesundheitswesen Bundesverb Arzte Offentlichen Gesundheitsdienstes Ger. 2018;80(1):20–26.
55. Tolhurst HM, Stewart SM. Balancing work, family and other lifestyle aspects: a qualitative study of Australian medical students’ attitudes. Med J Aust. 2004;181(7):361–364.
56. Piotrowski M, Stulberg D, Egan M. Medical student interest in flexible residency training options. Fam Med. 2018;50(5):339–344.
57. Spencer J, Blackmore D, Heard S, et al. Patient-oriented learning: a review of the role of the patient in the education of medical students. Med Educ. 2000;34(10):851–857.
58. Pfarrwaller E, Voirol L, Piumatti G, et al. Students’ intentions to practice primary care are associated with their motives to become doctors: a longitudinal study. BMC Med Educ. 2022;22(1):30.
59. Heiligers PJM. Gender differences in medical students’ motives and career choice. BMC Med Educ. 2012;12:82.
60. Diderichsen S, Johansson EE, Verdonk P, Lagro-Janssen T, Hamberg K. Few gender differences in specialty preferences and motivational factors: a cross-sectional Swedish study on last-year medical students. BMC Med Educ. 2013;13:39.
61. Lefevre JH, Roupret M, Kerneis S, Karila L. Career choices of medical students: a national survey of 1780 students. Med Educ. 2010;44(6):603–612.
62. Soethout MBM, ten Cate OTJ. Beroepsvoorkeuren van studenten geneeskunde [Career preferences among medical students]. Ned Tijdschr Geneeskd. 2014;158:A6655.
63. Jajosky RP, Banks M, Jajosky AN. Concerns about the pathology job market dominate a popular online pathology forum and likely deterred American medical students from pursuing pathology residency. Heliyon. 2019;5(9):e02400.
64. Smith BR, Kamoun M, Hickner J. Laboratory medicine education at U.S. medical schools: a 2014 status report. Acad Med J Assoc Am Med Coll. 2016;91(1):107–112.
65. Krupat E, Camargo CA, Strewler GJ, Espinola JA, Fleenor TJ, Dienstag JL. Factors associated with physicians’ choice of a career in research: a retrospective report 15 years after medical school graduation. Adv Health Sci Educ Theory Pract. 2017;22(1):5–15.
66. Yang Y, Li J, Wu X, et al. Factors influencing subspecialty choice among medical students: a systematic review and meta-analysis. BMJ Open. 2019;9(3):e022097.
67. Magalhães E, Salgueira AP, Costa P, Costa MJ. Empathy in senior year and first year medical students: a cross-sectional study. BMC Med Educ. 2011;11:52.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.