")
Back to Journals » Patient Related Outcome Measures » Volume 10
Mild-severe hemophilia B impacts relationships of US adults and children with hemophilia B and their families: results from the B-HERO-S study
Authors Cutter S, Guelcher C, Hunter S, Rotellini D , Dunn S , Cooper DL
Received 2 May 2019
Accepted for publication 29 July 2019
Published 16 August 2019 Volume 2019:10 Pages 257—266
DOI https://doi.org/10.2147/PROM.S214188
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Susan Cutter,1 Christine Guelcher,2 Susan Hunter,3 Dawn Rotellini,4 Spencer Dunn,5 David L Cooper6
1Penn Comprehensive Hemophilia and Thrombosis Program, Hospital of the University of Pennsylvania, Philadelphia, PA, USA; 2Comprehensive Hemostasis and Thrombosis Program, Children’s National Health System, Washington, DC, USA; 3Hemostasis and Thrombosis Center, University Hospitals Cleveland Medical Center, Cleveland, OH, USA; 4National Hemophilia Foundation, New York, NY, USA; 5Center for Comprehensive Care and Diagnosis of Inherited Bleeding Disorders, Orange, CA, USA; 6Novo Nordisk Inc., Plainsboro, NJ, USA
Correspondence: Susan Cutter
Penn Comprehensive Hemophilia and Thrombosis Program, Hospital of the University of Pennsylvania, 3400 Spruce St – 3 rd Fl Dulles, Philadelphia, PA 19104, USA
Tel +1 215 615 8007
Email [email protected]
Background: The B-HERO-S study evaluated the impact of mild to severe hemophilia B on the lives of affected adults and children. Here, we assessed the impact of hemophilia B on relationships.
Methods: US adults with hemophilia B and caregivers of affected children completed separate online surveys that included questions regarding impact of the disease on interpersonal relationships.
Results: Most (88%) of the 299 adults completing the survey had mild to moderate hemophilia B. Of those, 54% were married or in a long-term relationship, and 44% were single. Most adults (87%) reported that hemophilia affected their ability to form close relationships with partners or prospective partners; 35% were very/quite dissatisfied with the support received from a previous partner. Nearly all participants (98%) were very/quite satisfied with the support received from their current partner. Most were very/quite satisfied with the support from family (87%) and friends (96%). Most participants reported a negative reaction or experience as a result of disclosing their hemophilia (friend/colleague/employer, 76%/80%/82%, respectively). Of 150 caregivers of children with mostly mild to moderate hemophilia (74%), 89% were married or in a long-term relationship, and most felt very well/quite supported by their partner (98%) and family (92%). Most felt very/quite satisfied with the support of teachers (94%), children at school (80%), and other adults in regular contact (72%). Most caregivers reported negative experiences telling a friend (76%) or having their child tell a friend (69%) about the child’s hemophilia; 43% reported that their child was bullied because of his/her hemophilia.
Conclusion: Although the impact of severe hemophilia on relationships has been reported in HERO and other studies, B-HERO-S suggested that mild to moderate hemophilia B also significantly influences relationships of affected men/women and boys/girls, especially in disclosing their diagnosis, selecting a partner, and feeling bullied by peers/colleagues.
Keywords: support, partners, relationship satisfaction, caregivers, interpersonal relationships
Introduction
Hemophilia is a rare, X-linked, congenital bleeding disorder caused by a deficiency in coagulation factor VIII (hemophilia A) or factor IX (hemophilia B).1 Deficiency of coagulation factors results in repeated bleeds, often into joints, which can lead to hemophilic arthropathy.2 The pain and mobility impairment caused by hemophilic arthropathy can greatly affect health-related quality of life (HRQoL) of people with hemophilia.3,4
The international Hemophilia Experiences, Results, and Opportunities (HERO) study was designed to assess psychosocial issues and quantitatively measure HRQoL in people with hemophilia in 10 countries.5 Participants in this study were largely patients with hemophilia A (74%), and disease severity ranged from moderate to severe. In the HERO study, 1 of 3 participants reported that hemophilia had a negative impact on their ability to form close relationships, and many also reported having negative relationship experiences associated with their hemophilia.6 Despite acknowledging a negative impact of hemophilia on relationships, most participants described overall satisfaction with the support in their current relationships. Patients on some form of prophylaxis reported less satisfaction in relationships, suggesting that relationship issues may correlate with increased disease severity. However, the HERO study underrepresented patients with hemophilia B as well as patients with mild-moderate hemophilia.
The Bridging Hemophilia B Experiences, Results, and Opportunities Into Solutions (B-HERO-S) study was designed to evaluate the effects of mild, moderate, and severe hemophilia B on psychosocial issues and HRQoL for people with hemophilia and caregivers of affected children.7 The study predominantly examined those with mild to moderate disease severity. Importantly, the B-HERO-S study population included a large proportion of female adults responding as people with hemophilia (≤40% factor IX activity; n=86 [29%]). The study also included female caregivers who are carriers and may be symptomatic.8
To further define the impact of hemophilia B on interpersonal relationships for people with hemophilia, the B-HERO-S survey included questions about participants’ relationships with their families and other groups. This analysis defines the impact of hemophilia B disease burden on the relationships of adults and children with hemophilia.
Materials and methods
The B-HERO-S study methods were previously reported in detail.7 Briefly, the online cross-sectional study recruited patients through 3 hemophilia advocacy organizations (Coalition for Hemophilia B, Hemophilia Federation of America, and National Hemophilia Foundation) using email and social media. The study was approved by the Central Institutional Review Board (Quorum Review IRB, Seattle, WA, USA); the IRB waived informed consent for the study due to minimal risk criteria. Between September 24 and November 2, 2015, participants completed one of two distinct online surveys: one for adults with hemophilia B (aged ≥18 years) or one for caregivers of affected children (aged <18 years). The study included individuals with hemophilia B of any severity, with or without inhibitors, including women and caregivers of girls with hemophilia B.
Results
Respondent demographics and characteristics are summarized in Table 1. Overall, 54% of adults with hemophilia B were married or in a long-term relationship, and 44% were single. Most adults (87%) reported that hemophilia affected their ability to form close relationships with partners or prospective partners, while 12% reported no effect and 1% declined to answer. When asked how hemophilia affected their relationships, 56% reported being worried about the impact of their hemophilia in future years (Figure 1). Additionally, 45% stated that they were worried about being able to support a family in the future, and 42% were fearful of a partner’s/prospective partner’s reaction if they disclosed their hemophilia.
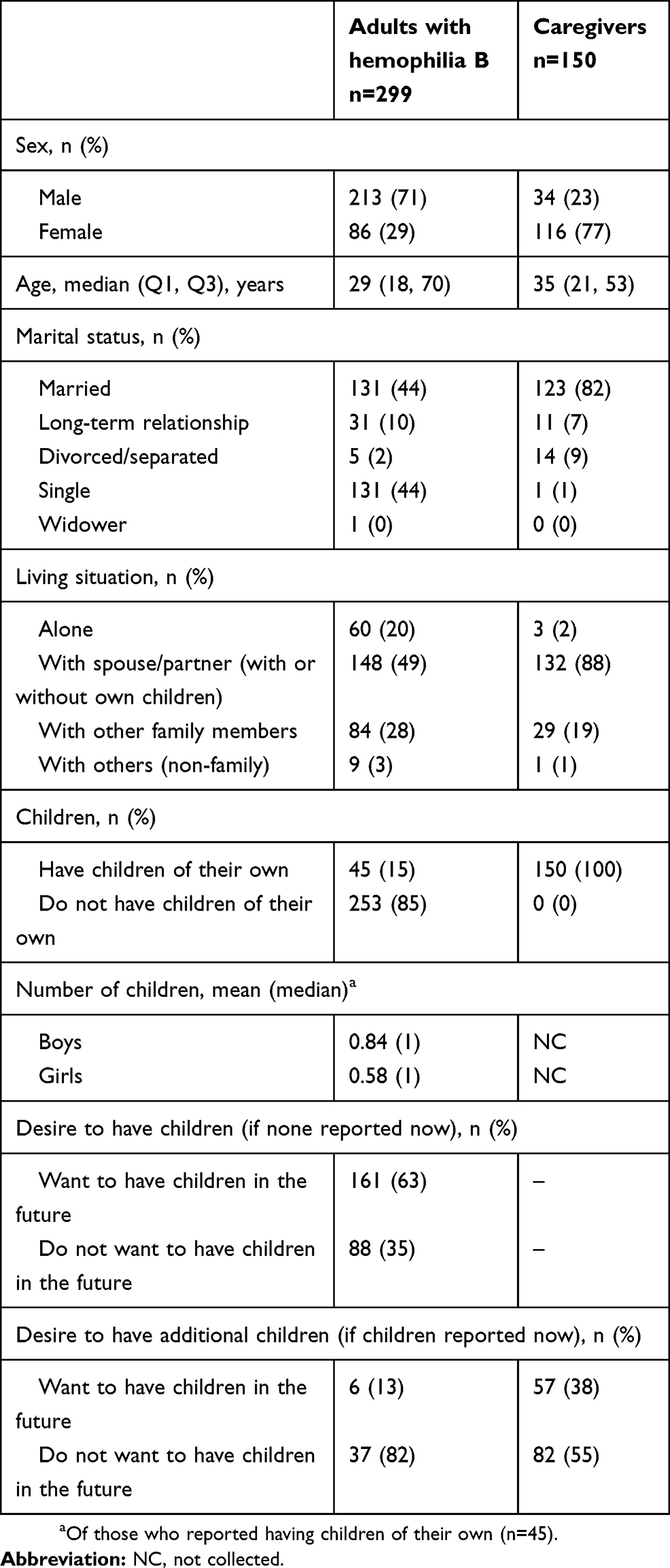 |
Table 1 Respondent demographics and characteristics |
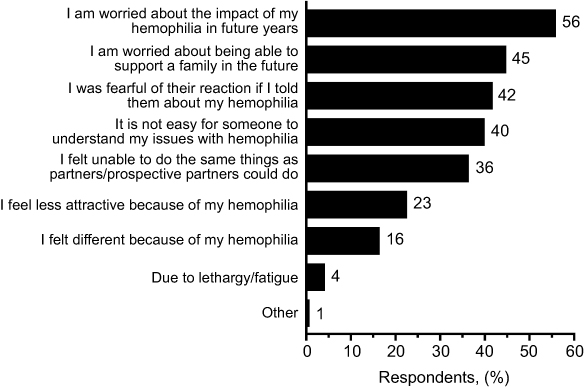 |
Figure 1 Adults with hemophilia B: impact of hemophilia on relationships. |
Nearly all participants (98%) were very or quite satisfied with the support received from their current partner (Figure 2). Primary reasons included “my partner takes the lead in providing financial security” (45%), “my partner really cares about me” (39%), and “our love for each other is very strong” (36%) (Figure 3). In contrast, only 56% of participants were very or quite satisfied with the support received from a previous partner (Figure 2). Ninety percent reported that their experiences in a prior relationship, both positive and negative, including the degree of support received, affected their decision to enter into a relationship with their current partner. Most were very/quite satisfied with the support from family (87%), friends (96%), colleagues at work/school (87%), and an employer/manager (90%) (Figure 2).
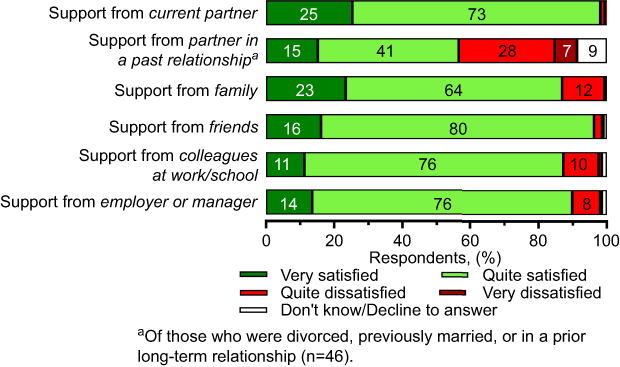 |
Figure 2 Adults with hemophilia B: degree of satisfaction with support regarding hemophilia. |
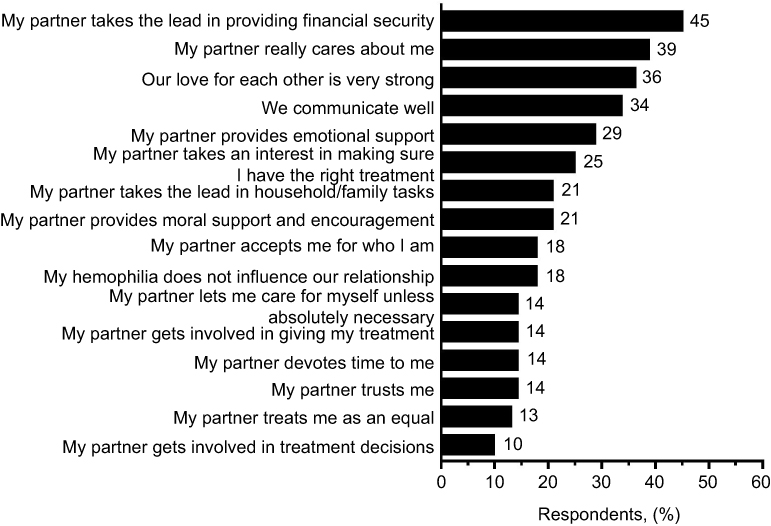 |
Figure 3 Adults with hemophilia B: reasons for satisfaction with current partner. |
Despite this support, most participants reported a negative reaction or experience as a result of disclosing their hemophilia to a friend (76%), colleague (80%), or employer (86%). Most also reported feeling bullied by peers (69%) or colleagues (66%) because of hemophilia. The majority noted that disclosing hemophilia affected current relationships with friends and colleagues (89% and 83%, respectively) (Figure 4). Past experiences with disclosure also affected which friends (77%) or colleagues (75%) they told about their hemophilia, and how or when they disclosed their hemophilia status to these individuals. Most participants stated that either a select few or most of their contacts know about their hemophilia, including friends (66%), colleagues (74%), employers/managers (72%), neighbors (74%), other contacts (80%), or social media contacts (82%) (Table S1). Most caregivers stated that either a select few or most of their contacts know about their child’s hemophilia, including the child’s friends (54%), children at school (60%), teachers (53%), neighbors (68%), other adults (80%), or social media contacts (72%).
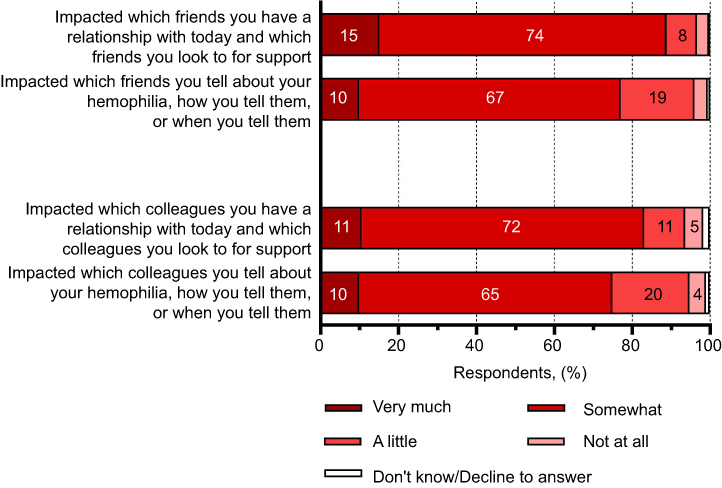 |
Figure 4 Adults with hemophilia B: experience with disclosing hemophilia to friends/colleagues and the impact on current relationships and approaches to disclosure. |
Of 150 caregivers, most cared for children with mild-moderate hemophilia (74%). Most caregivers reported either no impact (27%) or mixed positive/negative impact (49%) of their child’s hemophilia on his or her unaffected siblings (Figure 5). The negative impacts of hemophilia on unaffected siblings included that other children do not receive as much of the caregiver’s time as the child with hemophilia (45%), other children are prevented from doing what they want to do (39%), and other children have to take some responsibility in caring for their sibling with hemophilia (39%) (Figure S1). The positive impacts of hemophilia on unaffected siblings included that the children are closer because one of them has hemophilia (52%), the other children are more mature because of their sibling’s hemophilia (41%), and the other children have learned to share more easily (41%).
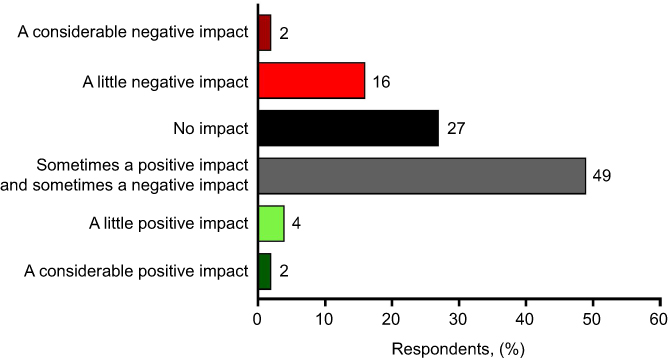 |
Figure 5 Caregivers: impact of child’s hemophilia on his/her unaffected siblings. |
Overall, 89% of caregivers were married or in a long-term relationship (Table 1), with most feeling very or quite satisfied with the support received from their partner (98%) and family (92%) (Figure 6). Most caregivers also felt very or quite satisfied with the support they received from others, including children at school (80%), teachers (94%), and other adults in regular contact (72%). Of caregivers dissatisfied with support from others, most noted that adults in regular contact are overprotective (59%) and do not know enough about hemophilia (56%). All (100%) reported that teachers at school do not know enough about hemophilia, and many (73%) reported that other children at school are overprotective (Table 2).
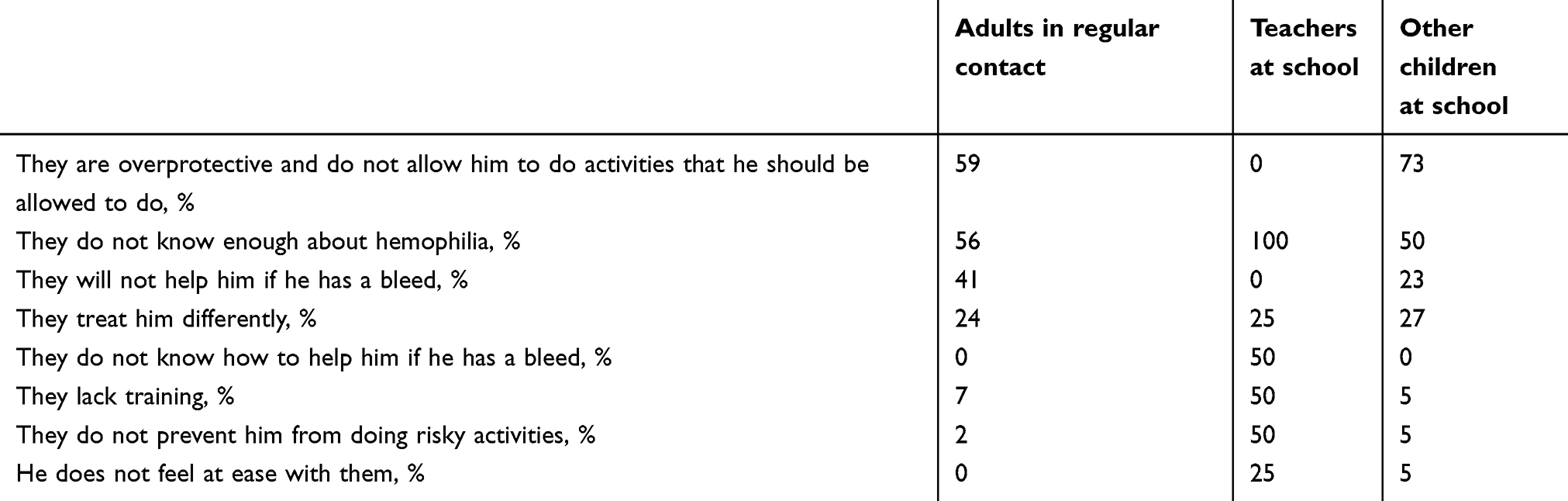 |
Table 2 Caregivers: reasons for dissatisfaction with relationships |
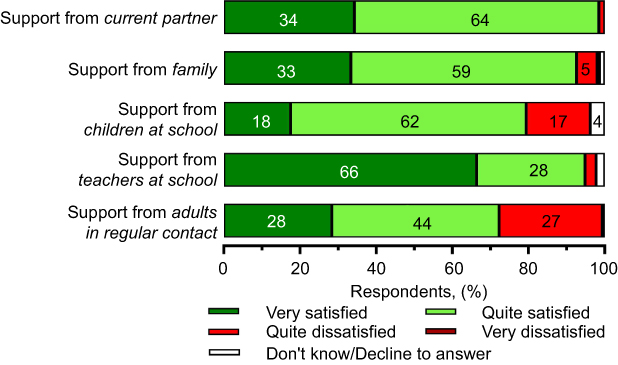 |
Figure 6 Caregivers: degree of satisfaction with support regarding their child’s hemophilia. |
Most caregivers (76%) reported ever having a negative reaction or negative experience as a result of telling a friend that their child has hemophilia, 69% reported that their child had a negative reaction or negative experience as a result of telling someone they had hemophilia, and 43% reported their child had been bullied as a result of having hemophilia.
Discussion
The HERO study previously found that while people with hemophilia report negative relationship experiences associated with their hemophilia, most are satisfied with the support they receive in their current relationships.6 The B-HERO-S study expanded on these findings by examining the seemingly contradictory reports of negative experiences and high relationship satisfaction. The B-HERO-S data suggest that for people with hemophilia, prior negative experiences inform their decisions in current relationships and may lead to greater relationship satisfaction. Very few respondents reported that all their social contacts know about their hemophilia, suggesting that most are selective about disclosing their hemophilia. Most people with hemophilia also reported that their previous experience of disclosing hemophilia to friends and colleagues had some impact on which friends and colleagues they currently have relationships with, as well as how they disclosed their hemophilia in these relationships. Thus, the prior negative experiences of people with hemophilia may encourage them to pursue relationships with individuals likely to be more supportive, leading to greater satisfaction in current personal and professional relationships. Consistent with this idea, most people with hemophilia stated that they are very or quite satisfied with the support from their current partner, while reporting less satisfaction with support from their previous partners. This suggests that based on prior negative experiences, people with hemophilia may seek partners who are more supportive of their hemophilia, thereby leading to a high rate of satisfaction with support from current partners.
The B-HERO-S study also found that despite having mild to moderate hemophilia, most respondents reported negative previous relationship experiences associated with their disease. Several hemophilia-related challenges may cause negative experiences. For example, lack of public awareness about hemophilia can lead to bullying, overprotectiveness, or other negative experiences at school and with friends. The B-HERO-S study participants were predominantly people with mild to moderate hemophilia (88%), while HERO participants had moderate to severe hemophilia. This provided the opportunity to compare reported relationship issues among individuals with different disease severities. Surprisingly, most adult respondents with hemophilia B in the B-HERO-S study (87%) believed that hemophilia affected their ability to develop close relationships with past or prospective partners, compared with only 36% in the HERO study.6 This suggests that past negative relationship experiences are an important issue, at least for a segment of those affected with mild to moderate hemophilia. Although having more severe hemophilia would seem to have a greater negative impact on relationships, these individuals deal with the disease throughout their childhood, as it affects them more severely from a young age. This means that they also have action and treatment plans in place to manage their hemophilia and that they are accustomed to living with their symptoms. Individuals with severe hemophilia are also more likely to have additional support.7
In contrast, people with mild to moderate hemophilia and women with hemophilia have more variable symptoms, as well as variable times of symptom onset.7,8 Problems often develop during adolescence, coinciding with menarche or increased activity levels; therefore, the median age of diagnosis for patients with mild hemophilia is 14 years, while patients with moderate hemophilia are diagnosed around age 6, and those with severe hemophilia are diagnosed before the age of 1.7 This later onset of symptoms means that hemophilia management may be less familiar to those with mild to moderate hemophilia, leading to lower self-efficacy related to their disease and higher likelihood of relying on their hemophilia treatment center (HTC) for their care.7 Conversely, they may minimize their diagnosis and symptoms, resulting in less contact with their HTC, which might be further encouraged by patient/family perceptions around education about the typical course of “mild” hemophilia or labeling affected women with factor IX below 40% as “symptomatic carriers” instead of people with mild hemophilia. These individuals may have less preparedness in understanding and managing their diagnosis and be less connected with the broader hemophilia community. Lack of self-efficacy, understanding, and/or knowledge related to their hemophilia has the potential to negatively influence their partner relationships as well as their ability to fully consider issues related to disclosure. Further, potential for less frequent contact with HTCs may mean they are not as comfortable reaching out for support when relationship issues or other issues arise.
The issues raised in this study are particularly important as we consider the next generation of therapies for patients with severe hemophilia including those with inhibitors, who have up until this point been very engaged with their treatment centers and the community. As new prophylactic treatments including factor/non-factor products and gene therapy seek to move patients from a severe to mild phenotype, there is the potential that patients with infrequent bleeding will evolve their engagement with HTCs and the community to patterns similar to those of patients with mild hemophilia today. This creates the potential for problems to occur if planning around childhood transitions becomes less consistent, patients are lost in transition to adult centers, disclosure of hemophilia to friends/schools/colleagues/employers becomes less common, and lack of appreciation for bleeds or bleeding risk with surgery/procedures leads to unforeseen complications. Beyond the positive impact of new treatments on joint outcomes, lack of proactive engagement may paradoxically increase the psychosocial burden of hemophilia. In addition, families whose relatives have undergone gene therapy may lack awareness of their family history and risks related to bleeding complications. This may result in delayed diagnosis, complications, and negative outcomes, potentially reversing decades of progress related to hemophilia.
A limitation of this study is possible recruitment bias. Study participants were recruited by hemophilia B advocacy organizations, which may have resulted in enrollment of more severe patients who are more likely to seek support from and be involved in the hemophilia B community. However, when compared with data from the Community Counts HTC Populations Profile, the B-HERO-S study enrolled ~9% of eligible adults and children (449 respondents/5099 patients with hemophilia B in the United States).9 Additionally, individuals with mild to moderate hemophilia, including women with hemophilia, may have been more likely to respond as they were excluded from previous studies.5 Comparison of the US B-HERO-S study results in mostly mild-moderate hemophilia and the international HERO study results in moderate-severe hemophilia A and B may have additional limitations due to cultural nuances and differences. In addition, the data collected during the 2 surveys were similar but not identical.
Conclusion
These data suggest that mild to moderate hemophilia B significantly affects the relationships of both males and females with hemophilia, children with hemophilia, and their caregivers. Although recruitment bias may limit quantitative conclusions, opportunities exist to more proactively counsel individuals with mild to moderate hemophilia B and their families to better navigate interpersonal relationships and disclosure and improve quality of life when they choose to engage with the HTC and community. As new prophylactic treatments seek to move patients with severe hemophilia to a mild phenotype, it is important to encourage continued close engagement to facilitate patients’ realistic understanding of these treatments and the potential risks of non-adherence to treatments, including the possible impact on their physical or psychosocial well-being.
Abbreviations
B-HERO-S, Bridging Hemophilia B Experiences, Results and Opportunities into Solutions; HERO, Hemophilia Experiences, Results and Opportunities; HRQoL, health-related quality of life; HTC, hemophilia treatment center.
Acknowledgment
The authors acknowledge the medical writing assistance of Melissa Priest, PhD, of ETHOS Health Communications in Yardley, Pennsylvania, which was supported financially by Novo Nordisk Inc., Plainsboro, New Jersey, in compliance with international Good Publication Practice guidelines.
Disclosure
SC has received honoraria from Novo Nordisk and Pfizer. CG reports personal fees from Novo Nordisk, Genentech, Octapharma, the National Hemophilia Foundation, Indiana Hemophilia, and Thrombosis Center outside the submitted work; she is also a Hemophilia Alliance Board member. SH reports personal fees from Novo Nordisk and grants from Cascade Hemophilia Consortium and MCHB, CDC outside the submitted work. DR is an employee of the National Hemophilia Foundation. The National Hemophilia Foundation has received grant funding from Novo Nordisk for the creation of educational workshops: HERO B. SD reports research funding from Bayer. DLC is an employee of Novo Nordisk. The authors report no other conflicts of interest in this work.
References
1. Srivastava A, Brewer AK, Mauser-Bunschoten EP, et al. Guidelines for the management of hemophilia. Haemophilia. 2013;19(1):e1–e47.
2. Luck JV
3. Forsyth AL, Witkop M, Lambing A, et al. Associations of quality of life, pain, and self-reported arthritis with age, employment, bleed rate, and utilization of hemophilia treatment center and health care provider services: results in adults with hemophilia in the HERO study. Patient Prefer Adher. 2015;9:1549–1560. doi:10.2147/PPA.S87659
4. Neufeld EJ, Recht M, Sabio H, et al. Effect of acute bleeding on daily quality of life assessments in patients with congenital hemophilia with inhibitors and their families: observations from the dosing observational study in hemophilia. Value Health. 2012;15(6):916–925. doi:10.1016/j.jval.2012.05.005
5. Forsyth AL, Gregory M, Nugent D, et al. Haemophilia Experiences, Results and Opportunities (HERO) study: survey methodology and population demographics. Haemophilia. 2014;20(1):44–51. doi:10.1111/hae.12239
6. Cassis FR, Buzzi A, Forsyth A, et al. Haemophilia Experiences, Results, and Opportunities (HERO) study: influence of haemophilia on interpersonal relationships as reported by adults with haemophilia and parents of children with haemophilia. Haemophilia. 2014;20(4):e287–e295. doi:10.1111/hae.12454
7. Buckner TW, Witkop M, Guelcher C, et al. Management of US men, women, and children with hemophilia and methods and demographics of the Bridging Hemophilia B Experiences, Results and Opportunities into Solutions (B-HERO-S) study. European Journal of Haematology. 2017;98(Suppl 86):5–17. doi:10.1111/ejh.12854
8. Plug I, Mauser-Bunschoten EP, Brocker-Vriends AH, et al. Bleeding in carriers of hemophilia. Blood. 2006;108(1):52–56. doi:10.1182/blood-2005-09-3879
9. Centers for Disease Control and Prevention. Community Counts - the HTC Population Profile. 2016. Available from: https://www.cdc.gov/ncbddd/hemophilia/communitycounts/data-community-counts.html. Accessed July 30, 2019.
Supplementary materials
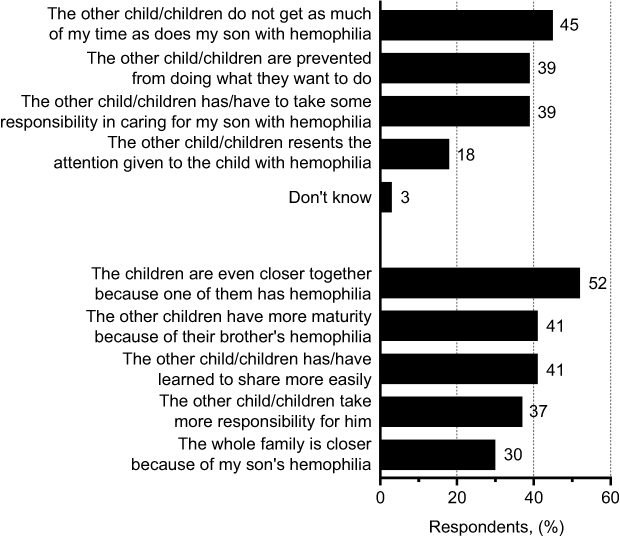 |
Figure S1 Caregivers: impact on siblings. |
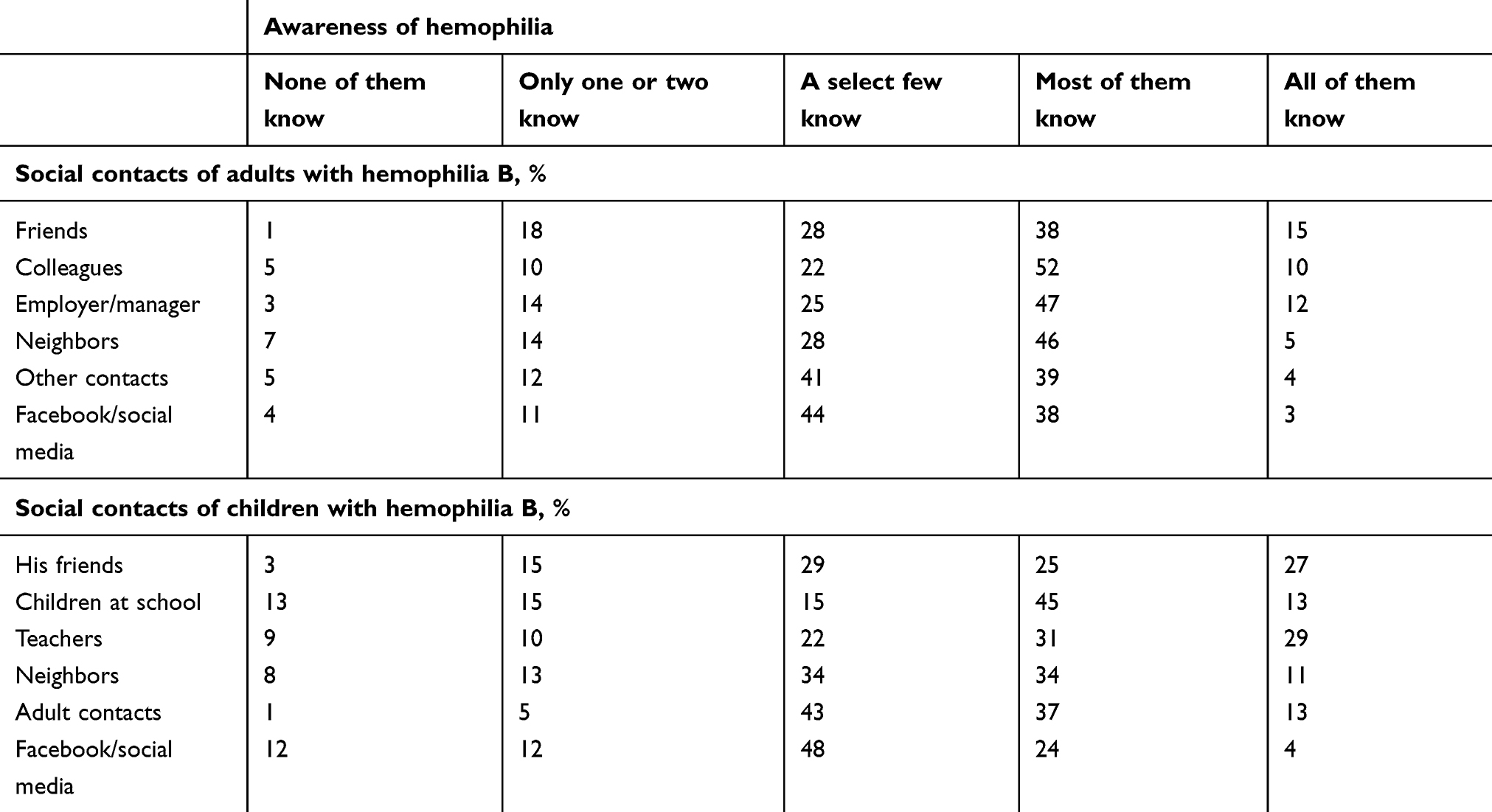 |
Table S1 Adults with hemophilia B and caregivers: awareness among social contacts of respondents’ hemophilia or respondents’ children’s hemophilia |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.