Back to Journals » Infection and Drug Resistance » Volume 16
Migratory Pulmonary Infiltrates in a B-Cell-Depleted COVID-19 Patient
Authors Zhu W ![]() , Xie T
, Xie T ![]() , Xu M, Chen R, Zhang T
, Xu M, Chen R, Zhang T
Received 3 October 2023
Accepted for publication 7 November 2023
Published 13 November 2023 Volume 2023:16 Pages 7205—7208
DOI https://doi.org/10.2147/IDR.S439795
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Wenyan Zhu,1 Tiange Xie,2 Mengru Xu,1 Ruxuan Chen,1 Ting Zhang1
1Department of Pulmonary and Critical Care Medicine, Peking Union Medical College Hospital, Chinese Academy of Medical Science and Peking Union Medical College, Beijing, People’s Republic of China; 2Department of General Practice, Peking Union Medical College Hospital, Chinese Academy of Medical Science and Peking Union Medical College, Beijing, People’s Republic of China
Correspondence: Ting Zhang; Ruxuan Chen, Email [email protected]; [email protected]
Background: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is still rampant around the world. Immunocompromised patients are prone to have long-term infection with coronavirus disease 2019 (COVID-19). However, it is difficult to decide on an appropriate treatment for persistent SARS-CoV-2 infection.
Case Presentation: We present a case of prolonged SARS-CoV-2 infection in a patient who had undergone B-cell depletion therapy. Chest computed tomography (CT) revealed notable migratory pulmonary infiltrates, and bronchoalveolar lavage fluid was positive for SARS-CoV-2 (day-120). The patient responded well to the combination treatment of antiviral medication, convalescent plasma, and corticosteroid.
Conclusion: When chest CT shows migratory pulmonary infiltrates in patients with recent COVID-19, it is necessary to be alert to the possibility of persistent SARS-CoV-2 infection, especially in B-cell-depleted immunocompromised patients. Once the diagnosis is confirmed, repeated antiviral therapy and intravenous convalescent plasma should be considered.
Keywords: SARS-CoV-2, migratory pulmonary infiltrates, B-cell depletion, antiviral therapy, convalescent plasma
Background
Coronavirus disease 2019 (COVID-19) results from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, leading to the ongoing worldwide pandemic. The most common computed tomography (CT) findings of COVID-19 pneumonia are peripheral ground-glass opacities (GGOs) and consolidation in severe cases, which might progressively evolve toward an organizing pneumonia pattern.1–3
Immunocompromised or immunodeficient patients are at high risk for viral and other opportunistic infections.4,5 B-cell-related humoral immunity plays a vital role in defending against virus infection and clearing viruses. Previous reports have suggested that patients with B-cell immunodeficiency caused by underlying diseases or drug therapy may develop prolonged and persistent SARS-CoV-2 infection.6,7 Obinutuzumab is an anti-CD-20 monoclonal antibody that mainly affects B cells. Consequently, patients receiving obinutuzumab have a reduced ability to elicit antibody responses after SARS-CoV-2 infection, enabling prolonged, active viral replication once infected.8
Here, we describe a B-cell-depleted COVID-19 patient after obinutuzumab therapy. His serial chest CT revealed rapidly changing migratory pulmonary infiltrates. To our knowledge, precious few cases9–11 have been reported concerning migratory pulmonary infiltrates in rituximab-treated patients with SARS-CoV-2 infection, and this is the first reported case of prolonged COVID-19 with notable migratory pulmonary infiltrates in a patient with previous obinutuzumab therapy.
Case Presentation
On December 15, 2022, a 42-year-old male who had been treated with obinutuzumab on November 18, 2022, for primary immune thrombocytopenia developed a fever. His nasopharyngeal SARS-CoV-2 antigen test was positive. He had received three doses of COVID-19 vaccine (recombinant SARS-CoV-2 S-protein receptor-binding domain vaccine, ZF2001, China) in 2021. The body temperature became normal two days later and his nasopharyngeal SARS-CoV-2 antigen test turned negative. He developed cough and white sputum in January 2023. Chest CT performed on day-64 post-infection revealed multiple GGOs in both lungs, predominantly in the left lower lobe (Figure 1A). Follow-up CT (day-70) revealed that the original GGOs in the left lower lobe resolved, and multiple GGOs emerged in the left upper lobe (Figure 1B). On day-76, the patient was admitted to a local hospital. On physical examination, his body temperature was 38.6°C; blood pressure, 121/80 mmHg; pulse, 83 beats/min; respiratory rate, 19 breaths/min, and pulse oxygen saturation, 99% on room air. Laboratory tests showed a moderately elevated erythrocyte sedimentation rate (ESR) (42 mm/h), as well as a reduced lymphocyte count (400/μL). Other routine blood tests were within normal range. The nasopharyngeal swab was negative for the SARS-CoV-2 antigen. Moxifloxacin (day-76) and high-dose methylprednisolone (up to 80mg daily, day-81) were administered successively without obvious clinical remission. During this period, chest CT showed rapidly changing migratory pulmonary infiltrates (Figure 1C–F).
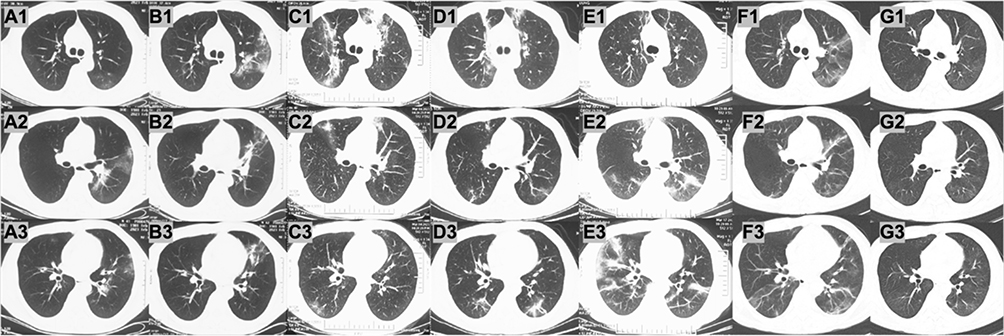 |
Figure 1 Chest CT (day-64, in (A)) revealed bilateral GGOs, predominantly in the left lower lobe. CT scans taken on day-70, day-79, day-85, day-92, and day-120 after COVID-19 onset (in B–F respectively) showed rapidly changing migratory pulmonary infiltrates consistent with organizing pneumonia. In (G) the CT scan showed the resolution of the pulmonary infiltrates on day-141. Supplementary note: A1, B1, C1, D1, E1, F1, and G1 are the chest CT at the bifurcation level of the trachea. A2, B2, C2, D2, E2, F2, and G2 are the chest CT at the level of right middle bronchus and left main bronchus. A3, B3, C3, D3, E3, F3, and G3 are the chest CT at the level of right middle bronchus. |
On day-120, he was transferred to our hospital because of the persistent fever and undiagnosed pulmonary infiltrates. Laboratory analysis showed an average lymphocyte count (1500/μL), while the peripheral blood B-cell count was zero. Blood eosinophil count, C-reaction protein (CRP), ESR, and rheumatoid factor were all within normal ranges. Antineutrophil cytoplasmic antibodies and antinuclear antibodies were negative. Blood and sputum cultures for bacteria and fungi were negative. No SARS-CoV-2 specific antibodies were detected in the serum. The nasopharyngeal SARS-CoV-2 antigen test was negative. However, the nasopharyngeal swab was positive for SARS-CoV-2 RNA (Cycle threshold, Ct value of 38.67), and bronchoalveolar lavage fluid (BALF) testing was also positive (Ct value of 31.72). The differential cell counts of BALF revealed remarkably lymphocytic inflammation (lymphocyte percentage 57.5%). Considering the possibility of secondary organizing pneumonia associated with prolonged SARS-CoV-2 infection, the patient received antiviral therapy (nirmatrelvir/ritonavir), infusion of convalescent plasma and oral methylprednisolone (up to 48 mg daily), resulting in rapid improvement of clinical symptoms. Chest CT (day-141) revealed significant dissipation of previous GGOs, and no new infiltrates were detected (Figure 1G).
Discussion and Conclusions
Here, we reported a case of prolonged SARS-CoV-2 infection with migratory pulmonary infiltrates in a patient who had undergone B-cell depletion therapy. Serial CT scans revealed migratory opacities consistent with a pattern of organizing pneumonia (OP). In addition to OP, migratory pulmonary infiltrates are commonly seen in eosinophilic lung diseases (eg, chronic eosinophilic pneumonia, eosinophilic granulomatosis with polyangiitis, and drug-induced hypersensitivity syndrome), parasitic infestations, and alveolar hemorrhage. For our patient, eosinophilic lung diseases were excluded according to normal eosinophil counts in both BALF and serum. Pulmonary parasitosis and alveolar hemorrhage were excluded due to negative epidemiological history and non-bloody BALF. Organizing pneumonia is classified into cryptogenic OP (COP) and secondary OP (SOP). Secondary OP can be caused by various viral infections, including adenovirus, cytomegalovirus, herpes, human immunodeficiency virus, influenza, and Middle East respiratory syndrome coronavirus, perhaps via immune system stimulation by viral antigens.12 Given the prior findings9–11 that the duration of active SARS-CoV-2 replication was prolonged and migratory pulmonary infiltrates on imaging in patients previously treated with anti-CD20 monoclonal antibodies, such as rituximab, and that radiological features of OP were commonly seen in COVID-19 patients, we assumed that our patient developed SOP to SARS-CoV-2 infection after 120 days of onset.
For the management of SOP, it is essential to treat the cause of disease. Nirmatrelvir/ritonavir is an oral antiviral drug consisted of nirmatrelvir, a novel SARS-CoV-2 primary protease inhibitor targeting 3CLpro of SARS-CoV-2, plus ritonavir (for its action as an inhibitor of cytochrome P450 3A4 to decrease nirmatrelvir metabolism and increase its serum levels).13 A standard course of nirmatrelvir/ritonavir treatment is associated with a markedly reduced risk of progression to severe COVID-19 or mortality.13,14 But nirmatrelvir/ritonavir alone will not clear the virus. Whether a standard course of nirmatrelvir/ritonavir treatment is sufficient for patients with persistent viral infection needs further study. Given that nirmatrelvir/ritonavir can only suppress viral duplication, SARS-CoV-2 specific antibodies are necessary to achieve viral clearance. The convalescent plasma contains protective antibodies produced by COVID-19 patients, which could reduce the incidence of hospitalization and death when a sufficient dose is given to patients with a recent onset of symptoms and to those who do not have a sufficient antibody response to SARS-CoV-2 infection.15 Patients with B-cell-depletion may not be able to produce antibodies effectively, leading to the persistent replication of the virus. Combining antiviral therapy with COVID-19 convalescent plasma or COVID-19 immunoglobulin may be beneficial to virus clearance and disease improvement in these immunosuppressed patients. This approach has succeeded in treating our patient, and also partly demonstrates the prolonged low titer virus replication in his lungs. In patients hospitalized with COVID-19, dexamethasone resulted in lower 28-day mortality among those receiving either invasive mechanical ventilation or oxygen alone at randomization.16 However, there is no consensus on the dosage and course of corticosteroid use for patients with OP-like changes on chest CT. Further research is needed on the strategy of corticosteroid therapy in B-cell-depleted COVID-19 patients with SOP.
In conclusion, we describe a prolonged clinical course in an immunocompromised patient with B-cell depletion who developed migratory pulmonary infiltrates after infection with SARS-CoV-2 and improved after antiviral therapy, convalescent plasma, and corticosteroid therapy. Notably, COVID-19 should be included in the differential diagnosis of migratory pulmonary infiltrates, especially in patients with B-cell depletion, due to the incompetent humoral immunity and disability of protective antibodies production. Combined antiviral therapy and convalescent plasma therapy may be an effective strategy for prolonged SARS-CoV-2 infection in patients with B-cell-depletion, however, further studies are needed to confirm it. The rational use of corticosteroids, including initiation timing, optimal dosage, and duration, in such patients needs further investigation.
Abbreviations
BALF, bronchoalveolar lavage fluid; COVID-19, coronavirus disease 2019; CRP, C-reaction protein; COP, cryptogenic organizing pneumonia; CT, chest computed tomography; Ct, cycle threshold; ESR, erythrocyte sedimentation rate; GGOs, ground-glass opacities; OP, organizing pneumonia; SOP, secondary organizing pneumonia; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Ethics and Consent
The patient provided informed consent to publish their case details and any accompanying images. In our institution, ethical approval is waived for case reports.
Acknowledgments
We would like to express our sincere gratitude and deep appreciation to Dr. Juhong Shi for her guidance and recommendations in this case report.
Funding
National High Level Hospital Clinical Research Funding (2022‑PUMCH‑A‑010).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kwee TC, Kwee RM. Chest CT in COVID-19: what the radiologist needs to know. Radiographics. 2022;42(1):E32. doi:10.1148/rg.219015
2. Yoon SH, Lee KH, Kim JY, et al. Chest radiographic and CT findings of the 2019 Novel Coronavirus Disease (COVID-19): analysis of nine patients treated in Korea. Korean J Radiol. 2020;21(4):494–500. doi:10.3348/kjr.2020.0132
3. Simpson S, Kay FU, Abbara S, et al. Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA - Secondary Publication. J Thorac Imaging. 2020;35(4):219–227. doi:10.1097/rti.0000000000000524
4. Manuel O, Estabrook M. RNA respiratory viral infections in solid organ transplant recipients: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant. 2019;33(9):e13511. doi:10.1111/ctr.13511
5. Waghmare A, Englund JA, Boeckh M. How I treat respiratory viral infections in the setting of intensive chemotherapy or hematopoietic cell transplantation. Blood. 2016;127(22):2682–2692. doi:10.1182/blood-2016-01-634873
6. Fung M, Babik JM. COVID-19 in immunocompromised hosts: what we know so far. Clin Infect Dis. 2021;72(2):340–350. doi:10.1093/cid/ciaa863
7. Brogna B, Bignardi E, Brogna C, et al. COVID-19 pneumonia in vaccinated population: a six clinical and radiological case series. Medicina. 2021;57(9):891. doi:10.3390/medicina57090891
8. Yasuda H, Tsukune Y, Watanabe N, et al. Persistent COVID-19 pneumonia and failure to develop anti-SARS-CoV-2 antibodies during rituximab maintenance therapy for follicular lymphoma. Clin Lymphoma Myeloma Leuk. 2020;20(11):774–776. doi:10.1016/j.clml.2020.08.017
9. John TM, Malek AE, Mulanovich VE, et al. Migratory pulmonary infiltrates in a patient with COVID-19 infection and the role of corticosteroids. Mayo Clin Proc. 2020;95(9):2038–2040. doi:10.1016/j.mayocp.2020.06.023
10. Santana ANC, Melo FX, Xavier FD, Amado VM. Migratory pulmonary infiltrates in a patient with COVID-19 and lymphoma. J Bras Pneumol. 2021;47(1):e20200528. doi:10.36416/1806-3756/e20200528
11. Ertesvåg NU, Sakkestad ST, Zhou F, et al. Persistent fever and positive PCR 90 days post-SARS-CoV-2 infection in a rituximab-treated patient: a case of late antiviral treatment. Viruses. 2022;14(8):1757. doi:10.3390/v14081757
12. Drakopanagiotakis F, Polychronopoulos V, Judson MA. Organizing pneumonia. Am J Med Sci. 2008;335(1):34–39. doi:10.1097/MAJ.0b013e31815d829d
13. Hammond J, Leister-Tebbe H, Gardner A, et al. Oral nirmatrelvir for high-risk, nonhospitalized adults with Covid-19. N Engl J Med. 2022;386(15):1397–1408. doi:10.1056/NEJMoa2118542
14. Najjar-Debbiny R, Gronich N, Weber G, et al. Effectiveness of paxlovid in reducing severe Coronavirus Disease 2019 and mortality in high-risk patients. Clin Infect Dis. 2023;76(3):e342–e349. doi:10.1093/cid/ciac443
15. Thompson MA, Henderson JP, Shah PK, et al. Association of convalescent plasma therapy with survival in patients with hematologic cancers and COVID-19. JAMA Oncol. 2021;7(8):1167–1175. doi:10.1001/jamaoncol.2021.1799
16. Horby P, Lim WS, Emberson JR, et al. Dexamethasone in hospitalized patients with Covid-19. N Engl J Med. 2021;384(8):693–704. doi:10.1056/NEJMoa2021436
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.